 Fiorella D’Auria1*†§
Fiorella D’Auria1*†§ Luciana Valvano2†§
Luciana Valvano2†§ Giovanni Calice3*
Giovanni Calice3* Vittoria D’Esposito4
Vittoria D’Esposito4 Serena Cabaro4
Serena Cabaro4 Pietro Formisano4
Pietro Formisano4 Gabriella Bianchino1
Gabriella Bianchino1 Antonio Traficante1Antonella Bianculli5Grazia Lazzari5
Antonio Traficante1Antonella Bianculli5Grazia Lazzari5 Teodora Statuto2‡Luciana Rago5‡
Teodora Statuto2‡Luciana Rago5‡- 1Laboratory of Clinical Pathology, Centro di Riferimento Oncologico della Basilicata (IRCCS-CROB), Rionero in Vulture, Italy
- 2Laboratory of Clinical Research and Advanced Diagnostics, Centro di Riferimento Oncologico della Basilicata (IRCCS-CROB), Rionero in Vulture, Italy
- 3Laboratory of Preclinical and Translational Research, Centro di Riferimento Oncologico della Basilicata (IRCCS-CROB), Rionero in Vulture, Italy
- 4Università degli Studi di Napoli “Federico II”, Department of Translational Medical Sciences, Napoli, Italy
- 5Radiotherapy Unit, Centro di Riferimento Oncologico della Basilicata (IRCCS-CROB), Rionero in Vulture, Italy
Background: The other side of radiotherapy (RT), in addition to the cytotoxic effect, is the ability to modulate the immune system in terms of activation or suppression, also depending on the dose and fractionation delivered. This immune RT effect can be detected both locally in the irradiated tumor site and in the peripheral blood. The aim of this study was to assess the consequence of pelvic irradiation on peripheral immune cells and cytokine secretions in localized prostate cancer (PC) patients undergoing pelvic irradiation with a simultaneous moderately hypofractionated prostate/prostate bed boost by Volumetric Modulated Arc Therapy (VMAT). Furthermore, we analyzed whether there was a correlation between these peripheral immune parameters and acute and late genitourinary (GU) and gastrointestinal (GI) toxicity.
Methods: Thirty-eight PC patients were treated with pelvis irradiation (dose per fraction 1.8 Gy) and simultaneous hypofractionated (median dose per fraction: 2.7 Gy) prostate/prostate bed boost. A longitudinal analysis was performed for 12 months on peripheral blood to assess changes in 9 different lymphocyte subpopulations by flow cytometry and 10 circulating cytokines by Multiplex Luminex assay and ELISA.
Results: Our analysis revealed that basal IFN-γ serum values were significantly lower in the definitive (curative intent for patients with prostate) patient group respect to the post-operative one. All the lymphocyte subsets and IFN-α, IFN-β and Il-2 peripheral concentrations displayed significant variations between the different time points considered. The immune cell population that suffers the greatest RT toxicity in the blood was B lymphocyte. We found an interesting correlation between basal TGF-β1 and late GU toxicity. In particular, TGF-β1 concentrations before RT were significantly higher in patients that experienced grade 2-3 of late GU toxicity, respect to grade 0-1. Exploring possible correlations between some clinical/biological findings and radiation planning parameters, we found no statistical significance.
Conclusions: Our study analyzed, in the context of hypofractionated radiotherapy in prostate cancer, different parameters of the peripheral immune system. We have highlighted longitudinally the peripheral behavior of the different lymphocyte subpopulations and of a group of 10 cytokines during the first year after RT. One of the analyzed cytokines, such as TGF-β1, has proven to be promising predictive factor of severe late GU toxicity.
Introduction
Radiotherapy (RT) is one of the anti-tumor therapeutic strategies in different types of cancers, thanks to its property of killing neoplastic cells by irreparable damage induced to DNA. In addition to the classical role of RT, recently, its possible ability to modulate the immune system’s response against tumors has also been much studied (1–11). The local immunomodulatory RT effects can be immune-stimulatory but, in contrast, also immune-suppressive, also based on the dose and fractionation delivered (7, 12). As regards the circulating immune cells, lymphocytes (particularly B cells) are more sensitive to radiation respect to myeloid cells (7).
With these premises, preclinical (13–15) and clinical studies (16, 17) on the possible combination of the best RT dose and fraction with immunotherapy have emerged.
Studying how different RT doses and schedules can act on the patient immune system is important to be able to design therapeutic combinations of RT with immunomodulatory agents in the future.
Although improved modern radiotherapy techniques target tumor tissues more precisely, normal cells in the surrounding tissues can still be damaged (18). The RT effects on the immune system can be different: induction of immunogenic cell death, activation of dendritic cells, reduction of Treg cells in the tumor microenvironment, increased expression of tumor-associated antigens, activation of tumor-specific T lymphocytes, increased production of pro-inflammatory cytokines (5, 19). RT-induced acute phase of inflammation, which in some patients does not resolve and results in a state of chronic inflammation, may contribute to the development of fibrosis in normal tissues surrounding the tumor and therefore of late toxicity (7, 20, 21).
With these assumptions, the aim of our work was to assess the consequence of hypofractionated RT on prostate/prostate bed with concomitant prophylactic irradiation of the pelvis, on peripheral immune cells and cytokine secretions in localized prostate cancer patients. Furthermore, we looked, among the components of the immune system studied, which could be a predictive factor for RT toxicity, since it is an important aspect for clinicians.
Methods
Patients’ characteristics
Thirty-eight prostate cancer patients were prospectively enrolled in our single-institutional study between April 2020 and November 2021. The study was examined and approved by the local ethics committee (Comitato Etico Unico Regionale per la Basilicata, approval number 20170016087) and therefore conducted in accordance with the ethical principles of the Declaration of Helsinki. All enrolled patients were treated according to our Institutional guidelines. In particular, 17 patients underwent definitive moderately hypofractionated RT and 21 patients underwent post-operative moderately hypofractionated RT. Table 1 reports the details of the doses and fractionations used for the two groups of patients. Hormone therapy was prescribed to 26 patients (Table 2). Median duration time of the hormone therapy was 24 months for both groups of patients (definitive range: 12-54 months; post-operative range: 6–36 months).
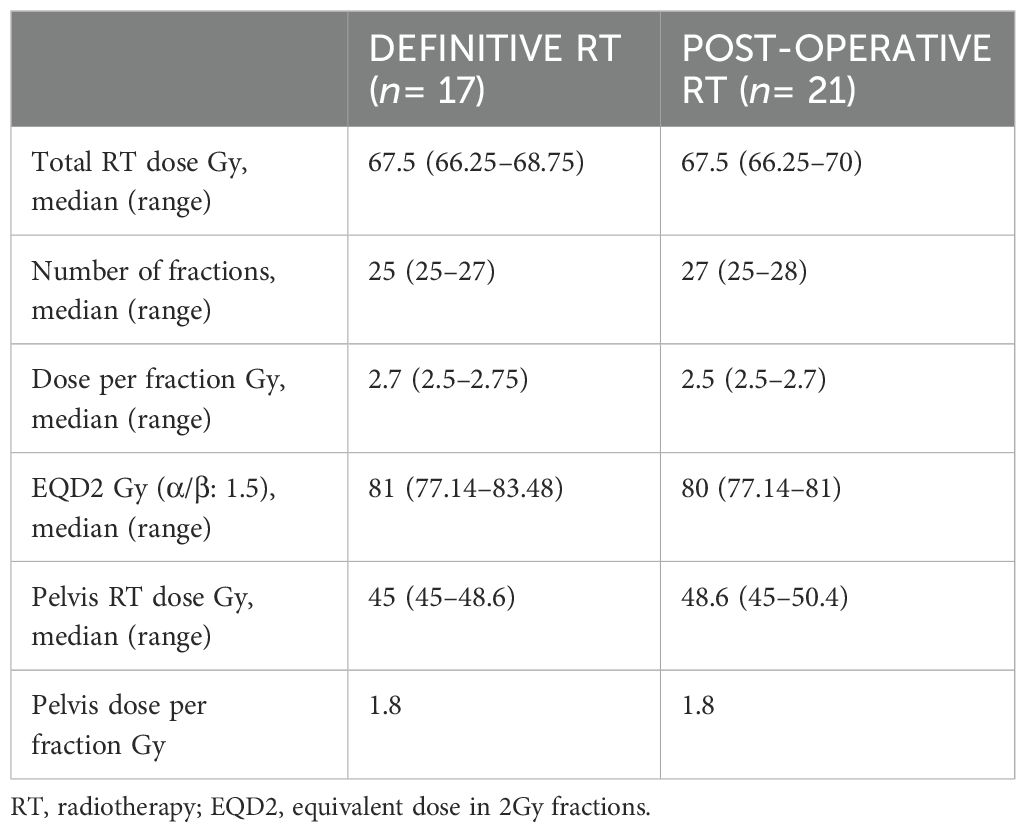
Table 1. Doses and fractionations.
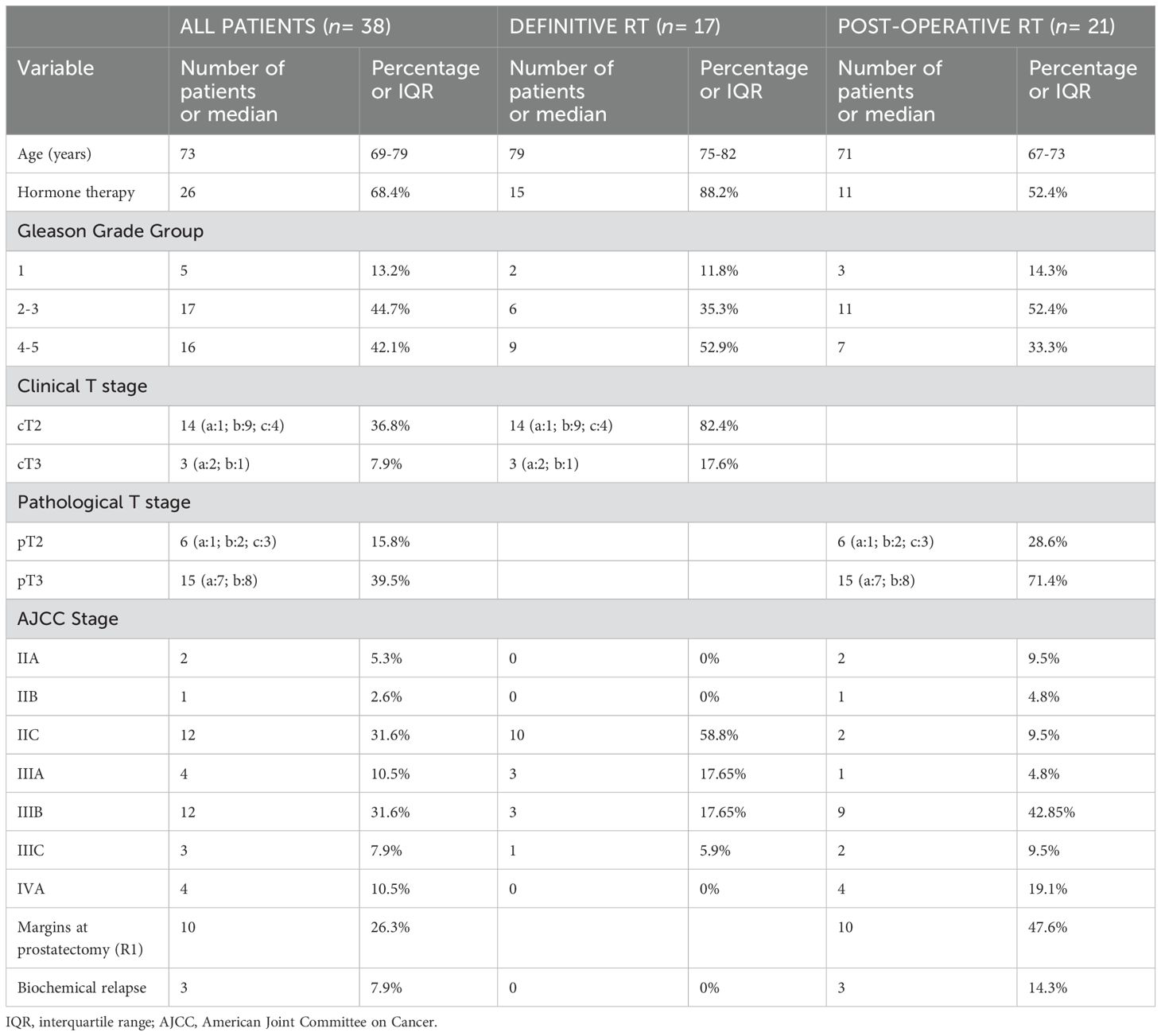
Table 2. Patient characteristics.
Target volumes were: prostate + seminal vesicles + pelvis for definitive RT; prostate bed + pelvis for post-operative RT. For both RT treatments, patients received a daily dose of 1.8 Gy to the pelvis and a simultaneous integrated boost (SIB), with median dose per fraction of 2.7 Gy (2.5-2.75), to the prostate/prostate bed. For the cranial limit of the pelvis, the right and left common iliac lymph nodes were included. Both groups were treated by Volumetric Modulated Arc therapy (VMAT).
Peripheral blood was collected before RT (t0), at the end of RT (t1), at follow-up time of 3 (t2), 6 (t3) and 12 months (t4) after the end of RT, respectively for 37, 38, 34, 33 and 28 patients.
At the above mentioned time points, absolute counts of white blood cells (WBC) and lymphocytes (ALC) were determined with a Beckman Coulter DXH800.
The genitourinary (GU) and gastrointestinal (GI) RT toxicity of the patients was recorded taking into account the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. For acute toxicity, we considered the events that occurred in the 120 days following the start of RT. The patients were subjected to the IPSS (International Prostate Symptom Score) questionnaire (22) for an objective evaluation of their urinary symptoms due to the prostatic disease.
Flow cytometry
For flow cytometry analysis, fluorescence-labeled antibodies were mixed with 100 µl of peripheral blood and incubated for 15 min in the dark. The antibody combinations were CD3-FITC/CD16CD56-PE/CD45-PerCP/CD8-PE-Cy7/CD4-APC/CD19-APC-Cy7; CD127-PE/CD4-PerCP/CD25-PE-Cy7/CD45-APC-Cy7. For each combination, 50,000 to 100,000 CD45-positive cells were analyzed. The peripheral blood lymphocyte subpopulations considered for this study are previously described (8, 23). The gating strategy is shown in Supplementary Figures 1 and 2. The absolute number of each cell subpopulation was obtained using the percentage and the ALC values.
Cytokines
Serum samples were tested to quantify 9 human cytokines (IFN-α, IFN-β, IFN-γ, IL-1β, IL-2, IL-6, IL-8, IL-10, TNF-α) with Multiplex Luminex assay kit (R&D Systems) on Luminex 200 System and TGF-β1 by ELISA (R&D Systems).
Statistical analysis
We have checked the normal distribution of all variable values by Shapiro–Wilk’s normality method. Since not all data had a normal course, we chose to represent them by median and interquartile range (IQR) and to apply the non-parametric statistical Kruskal–Wallis test and Wilcoxon rank sum test. Correlation was evaluated by Spearman’s rank method. Statistical significance was established on p-value<0.05. All the statistical analyses were performed by R software and CRAN packages (24); customized images were processed by the ggpubr package (25).
Results
Patient characteristics are reported in Table 2. Baseline data of cell population and cytokine concentrations are summarized in Table 3. With a median follow-up of 36 months (range 24-50), three patients (7.9%) experienced biochemical relapse, all in the post-operative RT setting. Only one patient (2.6%) died due to a second neoplasm.
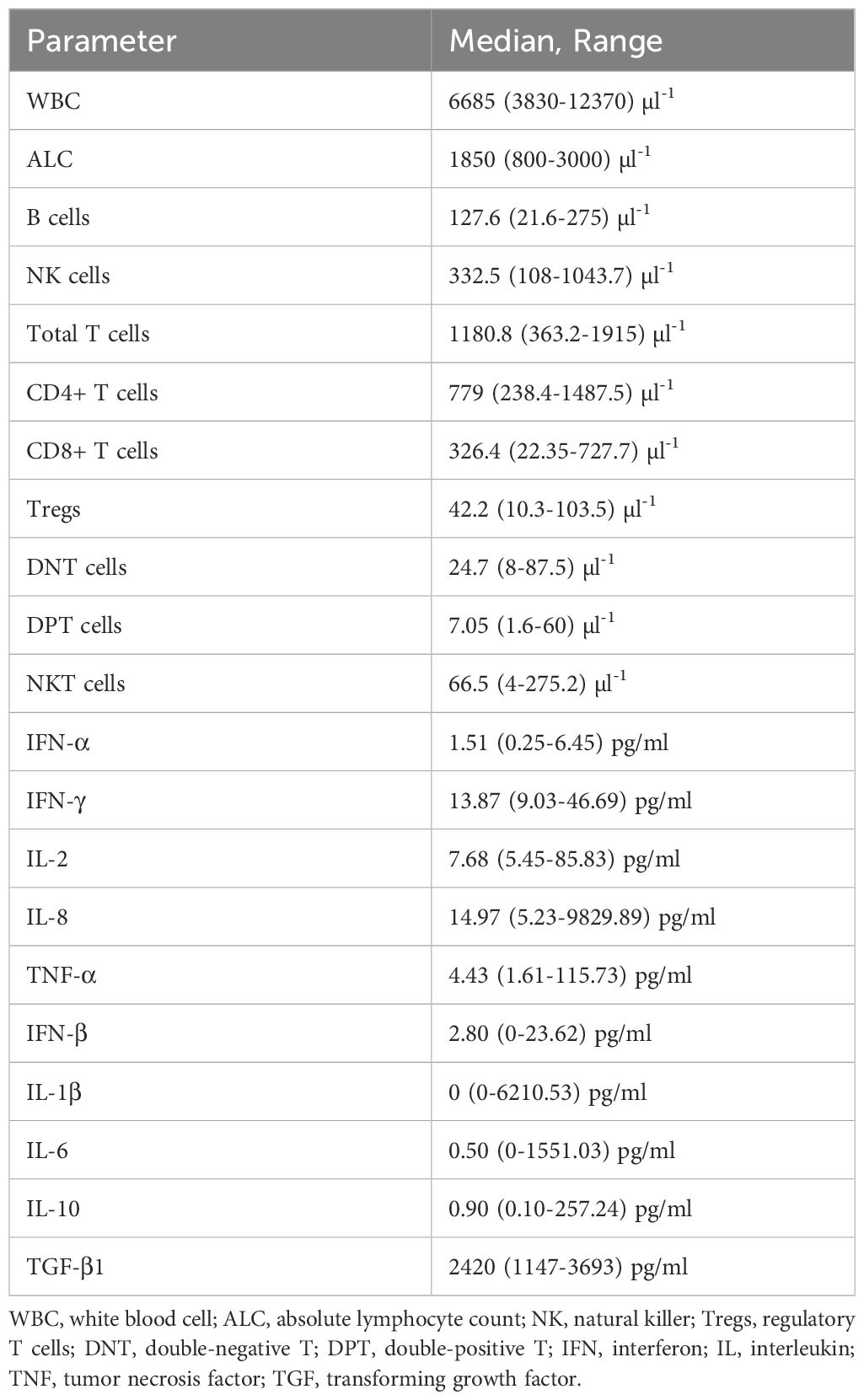
Table 3. Cell populations and cytokines values at baseline.
Correlation of baseline values with patient characteristics
We analyzed whether the baseline values of the different cell types and cytokines were influenced by: age, Gleason score, AJCC stage, TNM group, and type of RT (definitive or post-operative). We found that the only parameter significantly correlated with age was DNT value (p-value: 0.014, rho: -0.399). As regards the treatment, basal serum concentration of IFN-γ was significantly lower in definitive patients group (median: 12.7 pg/ml; IQR: 12.1-14.3 pg/ml) respect to post-operative one (median: 13.9 pg/ml; IQR: 13.9-18.7 pg/ml) (p-value: 0.039). We did not find any other influence of the variables considered on the values of the lymphocyte subtypes and cytokines.
Changes in lymphocyte subpopulations and cytokines over time
The different peripheral lymphocyte populations considered were: total T cells (CD3+), CD4+ T cells (CD3+ CD4+ CD8-), CD8+ T cells (CD3+ CD8+ CD4-), regulatory T cells (Tregs) (CD4+ CD25+ CD127low/-), DNT cells (CD3+ CD4- CD8- CD16/CD56-), DPT cells (CD3+ CD4+ CD8+), NKT cells (CD3+ CD16/CD56+), NK cells (CD3- CD16/CD56+) and B cells (CD19+) (Supplementary Figures 1, 2). The concentrations (cells/µl) of all these immune cell subtypes vary significantly (p-value<0.001) during the time points considered (Figure 1). In particular, they have a noticeable decrease at the end of RT (t1) compared to baseline (t0) and then tend to increase gradually during the following 12 months, without however reaching pre-RT values. Only NK cells return to initial values 12 months (t4) after the end of RT (t0 median: 332.5 cells/µl, IQR: 220.4-434.7; t4 median: 318.8 cells/µl, IQR: 222.9-532.9, p-value=0.848) and for B cells at time t4 the difference with the values at t0 is no longer statistically significant (p-value=0.124). Total T and CD4+ T cells have the slowest recovery after RT, in fact at t4 they do not even reach 50% of the t0 values (p-value<0.001). The greatest RT toxicity is experienced by B-lymphocytes, which are reduced by approximately 90% at t1 compared to t0 (t1 median: 11.8 cells/µl, IQR: 7.6-16.5; t0 median: 127.6 cells/µl, IQR: 95.9-168.1, p-value<0.001).
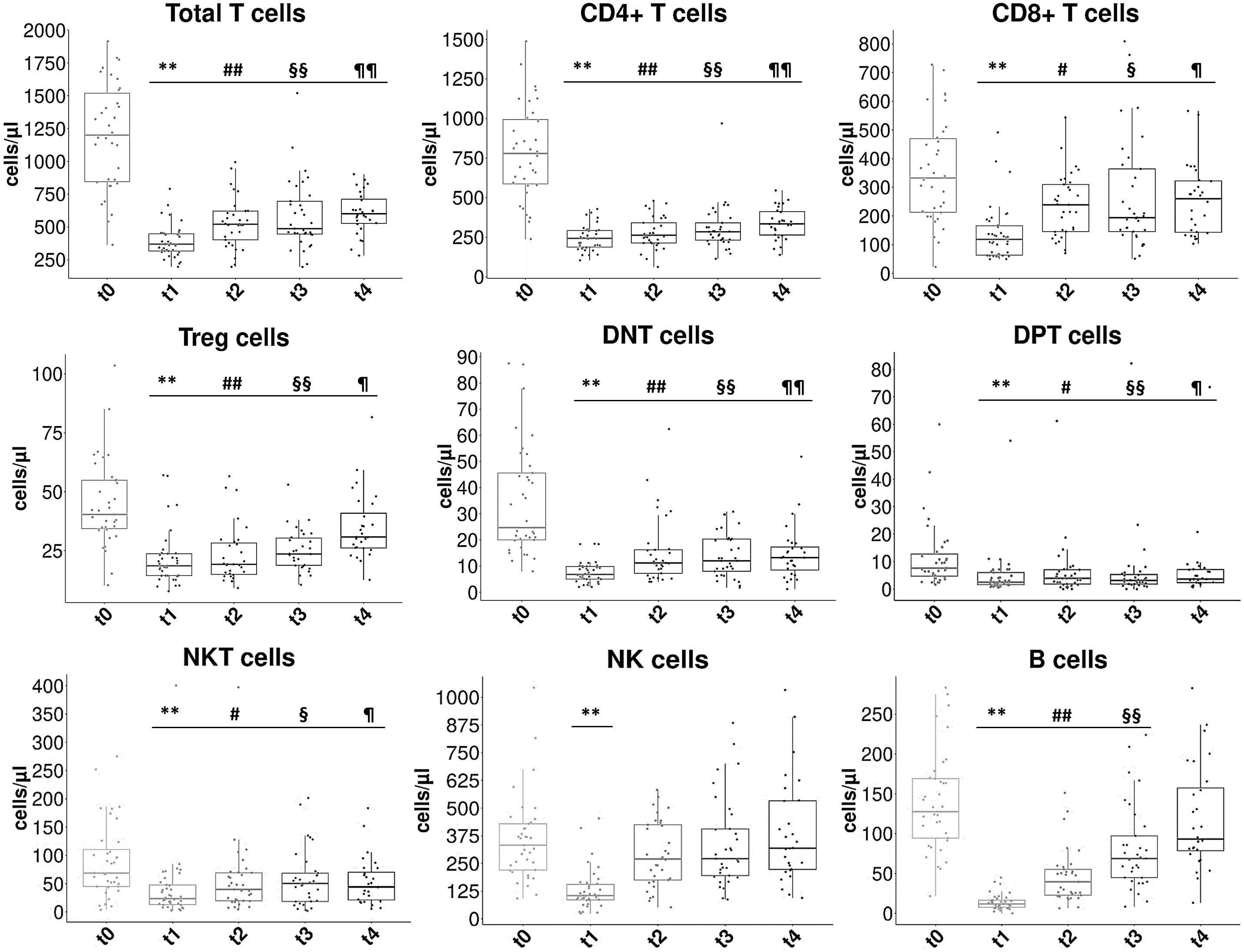
Figure 1. Concentration changes of lymphocyte subpopulations at the different time points considered. The box plots show the concentration values (in cells/µl) of the different peripheral lymphocyte subpopulations at the five considered time points: t0= pre-RT, t1= end of RT, t2= 3 months after RT, t3= 6 months after RT, t4= 12 months after RT. Statistical symbols (multiple comparison): **t1 vs t0 p<0.001; #t2 vs t0 p<0.05; ##t2 vs t0 p<0.001; §t3 vs t0 p< 0.05; §§t3 vs t0 p< 0.001; ¶t4 vs t0 p<0.05; ¶¶t4 vs t0 p<0.001.
Regarding serum cytokines, the concentrations of IFN-α, Il-2 and IFN-β changed significantly (p-value<0.05) between the different time points considered (Figure 2). In particular, we found reduction of IFN-α values for all time points respect to t0 (p-value<0.05), significant reduction of IL-2 respect to t0 at t2 and t3 time points and slight subsequent increase, and IFN-β clear reduction in value at time points t3 (p-2value<0.05) and t4 (not statistically significant) respect to t0.
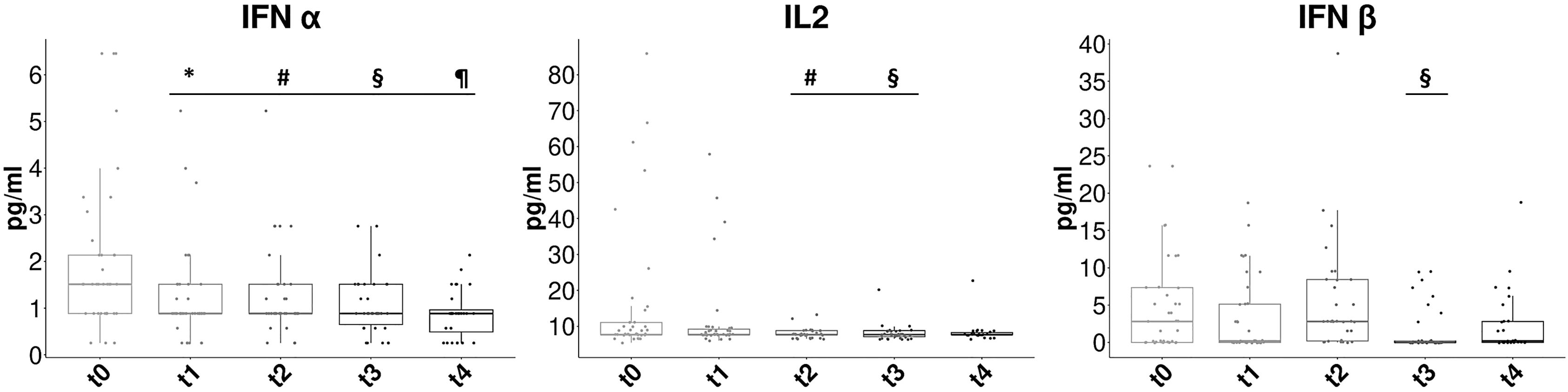
Figure 2. Concentration changes of cytokines at the different time points considered. The box plots show the concentration values (in pg/ml) of the serum cytokines at the five considered time points: t0= pre-RT, t1= end of RT, t2= 3 months after RT, t3= 6 months after RT, t4= 12 months after RT. We show only the value time series that have significant variation (Kruskal-Wallis p<0.05). Statistical symbols (multiple comparison): *t1 vs t0 p<0.05; #t2 vs t0 p<0.05; §t3 vs t0 p< 0.05; ¶t4 vs t0 p<0.05.
Correlations between cytokines and lymphocyte subpopulations
We investigated the possible correlation between some of the cytokines tested and the lymphocyte subtypes biologically related to them (total T cells and other T cell subsets). At the end of RT, we found a negative significant correlation between CD8+ T cells and IL-2 values (p-value: 0.037, rho: -0.338). No other significant correlation was found (Table 4).
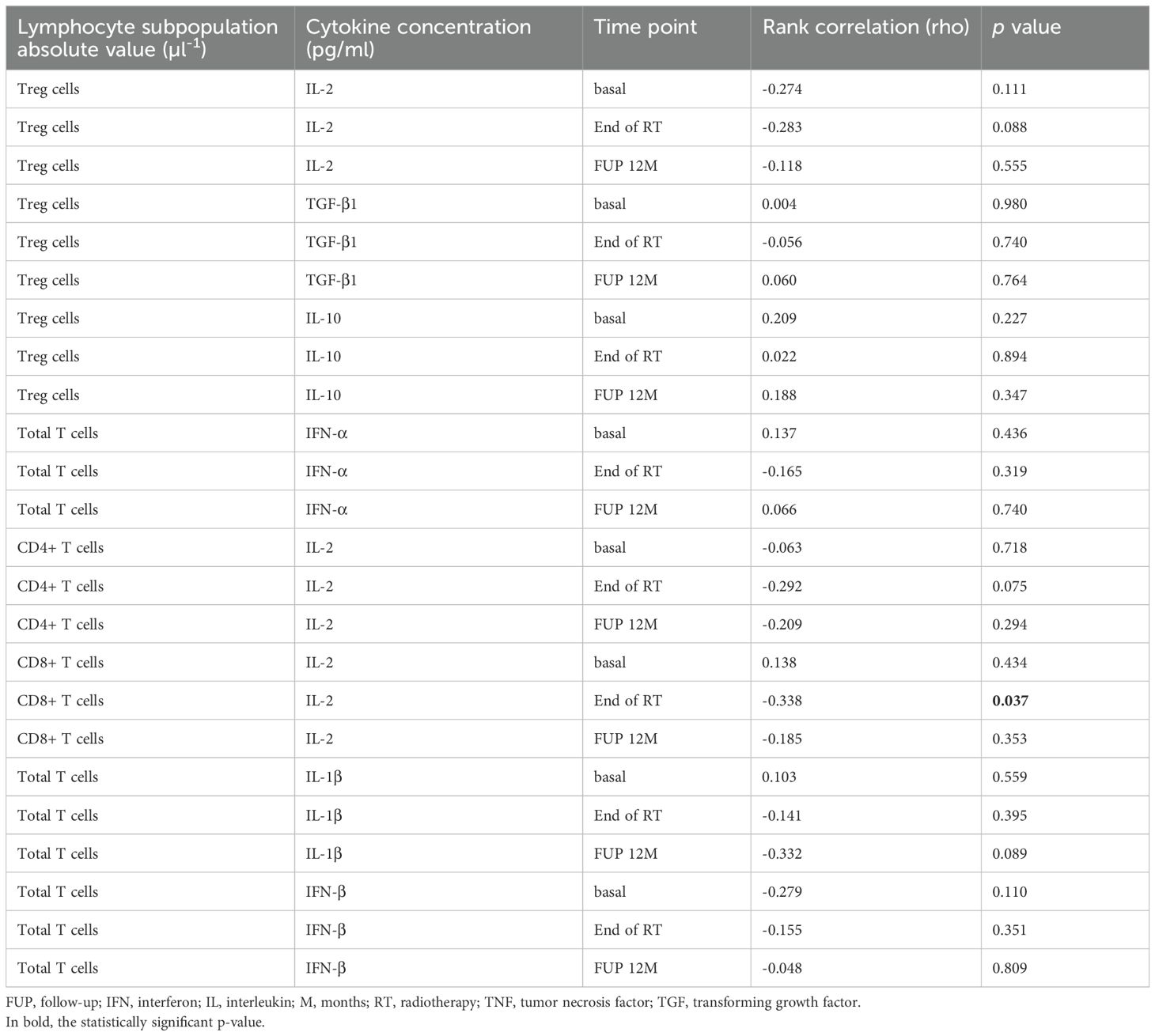
Table 4. Correlation between peripheral T lymphocyte subpopulation values and serum cytokine concentrations.
Toxicity data and correlation with TGF-β1 basal levels
In Table 5, we summarize the GU and GI toxicity (acute and late) associated to the RT treatment that we recorded during the follow up time of the patients.
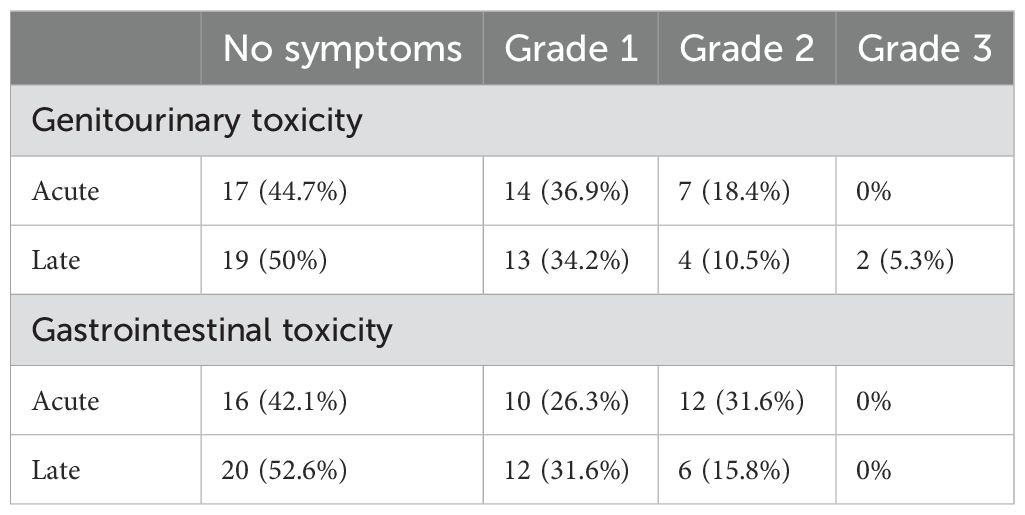
Table 5. RT toxicity data of the patients.
We tested whether there was a correlation between the severity of late GU and GI toxicity and baseline values of lymphocyte subpopulations and cytokines. In the late GU toxicity setting, we found that TGF-β1 was significantly higher in grade 2-3 (median: 3082 pg/ml, IQR: 2843-3352) than in grade 0-1 (median: 2337 pg/ml, IQR: 2076-2613) (p-value: 0.039) (Figure 3). We did not find the same statistically significant difference for late GI toxicity, where the values for the group grade 0-1 (median: 2409 pg/ml, IQR: 2113-2843) and grade 2-3 (median: 2441 pg/ml, IQR: 2052-2601) were comparable. There wasn’t a correlation between TGF-β1 basal values and GU or GI acute toxicity grades. No other baseline parameters were significantly correlated with the higher late GU or GI toxicity grades.
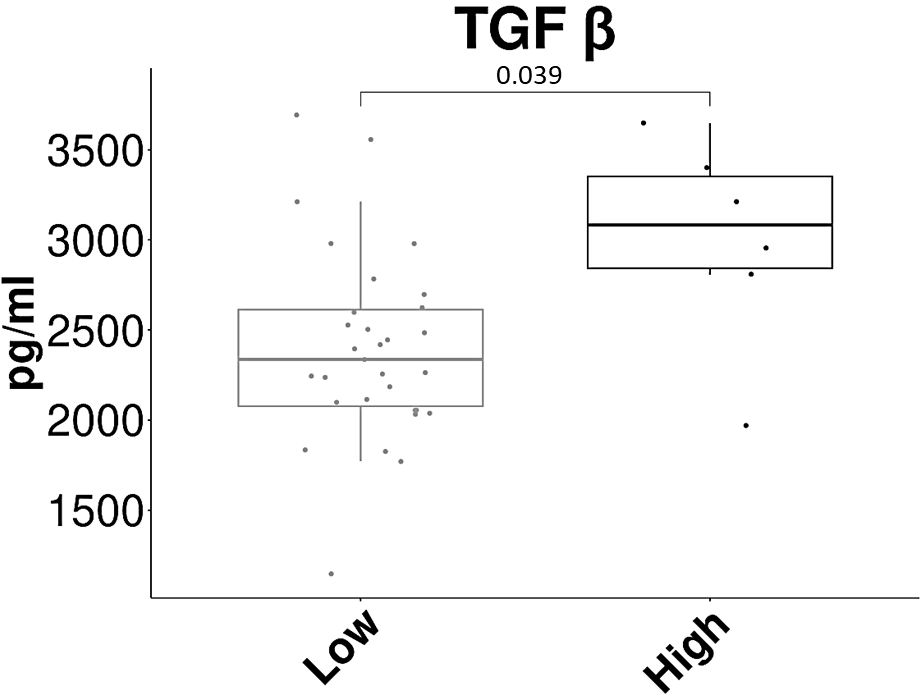
Figure 3. Correlation between TGF-β1 basal concentration and late genitourinary toxicity. The box plot shows the basal concentration values (in pg/ml) of serum TGF-β1 in the two groups of patients: Low= grade 0-1 of late GU toxicity, High= grade 2-3 of late GU toxicity.
Radiation planning parameters vs clinical and biological data
Since B-lymphocytes are those cells that suffer the greatest grade of RT toxicity, we evaluated if the ratios of B cell concentrations at the concentrations at t1, t2 and t4 compared to t0 correlated with the volumes (in cm3) of the pelvis irradiated and with the mean dose (in Gy) of radiation received by the pelvis. We did not find any statistically significant correlation (data not shown).
We then considered whether values of pelvis irradiated volumes and pelvis RT mean dose had a correlation with the results of the IPSS questionnaire at 3 and 24 months after RT, grouping patients into mildly or moderately/severely symptomatic. Again, we found no significant correlation.
Discussion
The immune system has recently been much studied in the field of RT. This interest is driven both by the attempt to better explain the effects of RT on immune cells and by the search for possible predictive factors of response or toxicity. In our case, we focused on the study of the peripheral variations of some parameters of the immune system in prostate cancer patients subjected to hypofractionated RT. The study of the trend of lymphocyte subpopulations following RT is present in literature in various types of cancer (1, 2, 8, 26–32).
Speaking specifically about RT for prostate cancer (PC), Eckert et al. observed, in 18 patients, that during the course of standard RT, the percentage of peripheral blood T cells, CD8+ and naïve CD4+ T cells and B cells decreased while regulatory T and NK cells increased (1).
A further study on a group of 33 PC patients found that definitive (curative intent for patients with prostate) or salvage (administered for post-prostatectomy biochemical relapse) RT cause similar effects and, in particular, that B-lymphocytes are more sensitive to both types of RT respect to T and NK cells (33).
In our previous work, we found that in PC patient’s peripheral immune cell subpopulation values decreased significantly at the end of RT, but less in the hypofractionation group than in the conventional one. Also the other smaller subgroups of T cell populations, double-negative T (DNT), double-positive T (DPT), and NKT cells significantly decreased at the end of RT with a slight tendency to recover during follow up, particularly in the hypofractionation group (8).
In a recent work of Palermo et al. (9), in accordance with our aforementioned data, total B and T cells decreased and conventional fractionated RT had a worse long-term effect on immune cells.
Another important aspect not to be underestimated is the RT cytotoxic effect on the various immune cell populations present in the lymph nodes draining the tumor which, based on the different therapeutic schemes, can be irradiated simultaneously with the tumor (34). These lymph nodes, in fact, are a very important site for the development of adaptive anti-tumor immunity.
The peculiarity of our work is that of having considered the variation in the concentration of the different peripheral blood lymphocyte subpopulations, contrary to most existing publications, which consider percentage values. In line with data from our previous work (8), we found that the concentration of B-lymphocytes is the one that undergoes the greatest decrease following RT. This data is in line with what has previously been reported in literature also for breast cancer (2, 32), gynecologic neoplasms (28) and prostate cancer (1, 29, 33). B cells slowly tend to rise during follow-up but, 12 months after RT, they do not reach the basal values. The other lymphocyte subpopulations also have the same trend, except for NK cells that are the only ones to return to pre-RT values at 12 months follow up after RT. This trend is also found in other types of carcinomas treated with radiotherapy (32, 35).
As already known, RT can also have a significant effect on cytokine release (21). Some of them, such as IL-1β, IL-6, IL-8, IFN-γ, and TNF-α, have a pro-inflammatory role, others, such as IL-10 and TGF-β, an immuno-modulatory function (21).
As regards proinflammatory cytokines, many studies reported an increase in circulating levels during RT. In particular, IL-6 increases during radiotherapy for PC and is also associated with acute genitourinary toxicity (4). In another study (36), IL-6 and also IFN-gamma increased during prostate intensity-modulated radiation therapy (IMRT) and IL-2 and IL-1 levels were correlated to GI and GU toxicity.
In a study of 18 PC patients, Singh J et al. found an association, not statistically significant, between TNF-α, IL-6 and TGF-β1 levels and the severity of GU and GI toxicity (5).
In a group of 39 localized or locally advanced PC patients undergoing RT, Kopcalic K et al. found that circulating levels of IL-6 correlated with fatigue and TGF-β1 with GU toxicity (37).
Regarding the analysis of cytokines in our work, we found a significantly different basal concentration of IFN-γ between definitive and post-operative patients. The correlation between the presence of the prostate and the concentration of IFN-γ was reported also in the study of Stanojkovic et al. (4). In their study, however, the concentration was higher in the definitive group than in the post-operative one. The same authors identified a correlation between higher concentrations of IL-6 and higher degrees of acute GU toxicity. As far as we are concerned, we did not find any correlation between serum IL-6 levels, basal or post-RT, and the other variables considered. Among all 10 cytokines analyzed, we found an interesting correlation between TGF-β1 basal serum values and late GU toxicity, an insidious RT effect feared by clinicians. In various works, on the prostate as well as on lung or breast cancer (15, 38, 39), the correlation between TGF-β and RT toxicity has been studied. In particular, in PC patients, Kopcalic et al. found a statistically significant correlation (p=0.036) between pre-treatment serum TGF-β1 concentration and the higher grades of acute GU toxicity (37). In locally advanced lung cancer, it was observed that at the time of 30-48 Gy irradiation, higher changes of serum TGF-β compared to baseline were correlated with higher degrees of radiation-induced lung injury (38). In stage 0-1 breast cancer patients, the mean TGF-β1 serum levels pre-accelerated hypofractionated partial breast irradiation correlate with the development of moderate to severe radiation-induced fibrosis (39). In our group of PC patients, serum TGF-β1 median concentration was significantly higher in patients who developed grades 2-3 of late GU toxicity than in those with grades 0-1.
One of our limitations is the small size of our group of patients, especially the 12-month time point for which we were only able to collect samples from 28 patients. This could probably also influence the non-statistically significant variation over time for many of the cytokines considered.
As regards the analysis of the effects of hypofractionated RT on the immune system in PC, this work longitudinally analyzes in detail the peripheral concentration changes of the different populations of immune cells within a year from the end of radiotherapy. We show which populations suffer the greatest toxicity (B cells), which recover the slowest (total T and CD4+ T cells) and in any case does not reach baseline levels at one year and which, one year after RT, manages to return to initial values (NK cells). Furthermore, very important information for clinicians, we highlight how baseline serum values of the cytokine TGF-β1 can be a potential predictive marker of severe late genitourinary toxicity.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comitato Etico Unico Regionale per la Basilicata. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FDA: Data curation, Formal analysis, Investigation, Writing – original draft. LV: Data curation, Investigation, Writing – review & editing. GC: Formal analysis, Software, Writing – review & editing. VDE: Investigation, Writing – review & editing. SC: Investigation, Writing – review & editing. PF: Supervision, Writing – review & editing. GB: Resources, Writing – review & editing. AT: Supervision, Writing – review & editing. AB: Methodology, Writing – review & editing. GL: Supervision, Writing – review & editing. TS: Data curation, Formal analysis, Writing – review & editing. LR: Resources, Conceptualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Italian Ministry of Health - Ricerca Corrente 2024.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1457839/full#supplementary-material
References
1. Eckert F, Schaedle P, Zips D, Schmid-Horch B, Rammensee HG, Gani C, et al. Impact of curative radiotherapy on the immune status of patients with localized prostate cancer. Oncoimmunology. (2018) 7:e1496881. doi: 10.1080/2162402X.2018.1496881
2. Yuan C, Wang Q. Comparative analysis of the effect of different radiotherapy regimens on lymphocyte and its subpopulations in breast cancer patients. Clin Transl Oncol. (2018) 20:1219–25. doi: 10.1007/s12094-018-1851-2
3. Lhuillier C, Rudqvist NP, Elemento O, Formenti SC, Demaria S. Radiation therapy and anti-tumor immunity: exposing immunogenic mutations to the immune system. Genome Med. (2019) 11:40. doi: 10.1186/s13073-019-0653-7
4. Stanojković TP, Matić IZ, Petrović N, Stanković V, Kopčalić K, Besu I, et al. Evaluation of cytokine expression and circulating immune cell subsets as potential parameters of acute radiation toxicity in prostate cancer patients. Sci Rep. (2020) 10:19002. doi: 10.1038/s41598-020-75812-0
5. Singh J, Sohal SS, Ahuja K, Lim A, Duncan H, Thachil T, et al. Investigation of circulatory cytokines in patients undergoing intensity-modulated radiotherapy (IMRT) for adenocarcinoma of the prostate and association with acute RT-induced toxicity: A prospective clinical study. Cytokine. (2020) 131:155108. doi: 10.1016/j.cyto.2020.155108
6. Wang Q, Li S, Qiao S, Zheng Z, Duan X, Zhu X. Changes in T lymphocyte subsets in different tumors before and after radiotherapy: A meta-analysis. Front Immunol. (2021) 12:648652. doi: 10.3389/fimmu.2021.648652
7. Cytlak UM, Dyer DP, Honeychurch J, Williams KJ, Travis MA, Illidge TM. Immunomodulation by radiotherapy in tumour control and normal tissue toxicity. Nat Rev Immunol. (2022) 22:124–38. doi: 10.1038/s41577-021-00568-1
8. D’Auria F, Statuto T, Rago L, Montagna A, Castaldo G, Schirò I, et al. Modulation of peripheral immune cell subpopulations after rapidArc/moderate hypofractionated radiotherapy for localized prostate cancer: findings and comparison with 3D conformal/conventional fractionation treatment. Front Oncol. (2022) 12:829812. doi: 10.3389/fonc.2022.829812
9. Palermo B, Bottero M, Panetta M, Faiella A, Sperduti I, Masi S, et al. Stereotactic ablative radiation therapy in 3 fractions induces a favorable systemic immune cell profiling in prostate cancer patients. Oncoimmunology. (2023) 12:2174721. doi: 10.1080/2162402X.2023.2174721
10. Koukourakis IM, Tiniakos D, Kouloulias V, Zygogianni A. The molecular basis of mmune-radiotherap. Int J Radiat Biol. (2023) 99:715–36. doi: 10.1080/09553002.2023.2144960
11. Carvalho HA, Villar RC. Radiotherapy and immune response: the systemic effects of a local treatment. Clinics. (2018) 73 Suppl 1:e557s. doi: 10.6061/clinics/2018/e557s
12. Romano E, Honeychurch J, Illidge TM. Radiotherapy-immunotherapy combination: how will we bridge the gap between pre-clinical promise and effective clinical delivery? Cancers. (2021) 13:457. doi: 10.3390/cancers13030457
13. Formenti SC, Demaria S. Future of radiation and immunotherapy. Int J Radiat Oncol Biol Phys. (2020) 108:3–5. doi: 10.1016/j.ijrobp.2020.04.034
14. Mondini M, Levy A, Meziani L, Milliat F, Deutsch E. Radiotherapy-immunotherapy combinations-perspectives and challenges. Mol Oncol. (2020) 14:1529–37. doi: 10.1002/1878-0261.12658
15. Dewan MZ, Galloway AE, Kawashima N, Dewyngaert JK, Babb JS, Formenti SC, et al. Fractionated but not single-dose radiotherapy induces an immune-mediated abscopal effect when combined with anti-CTLA-4 antibody. Clin Cancer Res. (2009) 15:5379–88. doi: 10.1158/1078-0432.CCR-09-0265
16. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N Engl J Med. (2018) 379:2342–50. doi: 10.1056/NEJMoa1809697
17. Theelen WSME, Peulen HMU, Lalezari F, van der Noort V, de Vries JF, Aerts JGJV, et al. Effect of pembrolizumab after stereotactic body radiotherapy vs pembrolizumab alone on tumor response in patients with advanced non-small cell lung cancer: results of the PEMBRO-RT phase 2 randomized clinical trial. JAMA Oncol. (2019) 5:1276–82. doi: 10.1001/jamaoncol.2019.1478
18. De Ruysscher D, Niedermann G, Burnet NG, Siva S, Lee AWM, Hegi-Johnson F. Radiotherapy toxicity. Nat Rev Dis Primers. (2019) 5:13. doi: 10.1038/s41572-019-0064-5
19. Van Limbergen EJ, De Ruysscher DK, Pimentel VO, Marcus D, Berbee M, Hoeben A, et al. Combining radiotherapy with immunotherapy: the past, the present and the future. Br J Radiol. (2017) 90:20170157. doi: 10.1259/bjr.20170157
20. Balázs K, Antal L, Sáfrány G, Lumniczky K. Blood-derived biomarkers of diagnosis, prognosis and therapy response in prostate cancer patients. J Pers Med. (2021) 11:296. doi: 10.3390/jpm11040296
21. Di Maggio FM, Minafra L, Forte GI, Cammarata FP, Lio D, Messa C, et al. Portrait of inflammatory response to ionizing radiation treatment. J Inflamm. (2015) 12:14. doi: 10.1186/s12950-015-0058-3.21
22. Barry MJ, Fowler FJ Jr, O’Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. (1992) 148:1549–57. doi: 10.1016/s0022-5347(17)36966-5
23. Valvano L, Nozza F, D’Arena G, D'Auria F, De Luca L, Pietrantuono G, et al. Preliminary analysis of double-negative T, double-positive T, and natural killer T-like cells in B-cell chronic lymphocytic leukemia. Cancer Med. (2023) 12:13241–55. doi: 10.1002/cam4.6015
24. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Available at: https://www.R-project.org/.
25. Kassambara A. ggpubr: ‘ggplot2’ Based publication ready plots (2019). Available online at: https://CRAN.R-project.org/package=ggpubr (Accessed May 05, 2024).
26. Raben M, Walach N, Galili U, Schlesinger M. The effect of radiation therapy on lymphocyte subpopulations in cancer patients. Cancer. (1976) 37:1417–21. doi: 10.1002/1097-0142(197603)37:3<1417::aid-cncr2820370324>3.0.co;2-n
27. Rand RJ, Jenkins DM, Bulmer R. T and B lymphocytes sub-populations following radiotherapy for invasive squamous cell carcinoma of the uterine cervix. Clin Exp Immunol. (1978) 33:159–65.
28. Lissoni P, Meregalli S, Bonetto E, Mancuso M, Brivio F, Colciago M, et al. Radiotherapy-induced lymphocytopenia: changes in total lymphocyte count and in lymphocyte subpopulations under pelvic irradiation in gynecologic neoplasms. J Biol Regul Homeost Agents. (2005) 19:153–8.
29. Johnke RM, Edwards JM, Kovacs CJ, Evans MJ, Daly BM, Karlsson UL, et al. Response of T lymphocyte populations in prostate cancer patients undergoing radiotherapy: influence of neoajuvant total androgen suppression. Anticancer Res. (2005) 25:3159–66.
30. Li H, Yu H, Lan S, Zhao D, Liu Y, Cheng Y. Aberrant alteration of circulating lymphocyte subsets in small cell lung cancer patients treated with radiotherapy. Technol Cancer Res Treat. (2021) 20:15330338211039948. doi: 10.1177/15330338211039948
31. Verastegui EL, Morales RB, Barrera-Franco JL, Poitevin AC, Hadden J. Long-term immune dysfunction after radiotherapy to the head and neck area. Clin Trial. (2003) 3:1093–104. doi: 10.1016/s1567-5769(03)00013-4
32. Sage EK, Schmid TE, Sedelmayr M, Gehrmann M, Geinitz H, Duma MN, et al. Comparative analysis of the effects of radiotherapy versus radiotherapy after adjuvant chemotherapy on the composition of lymphocyte subpopulations in breast cancer patients. Radiother Oncol. (2016) 118:176–80. doi: 10.1016/j.radonc.2015.11.016
33. Sage EK, Schmid TE, Geinitz H, Gehrmann M, Sedelmayr M, Duma MN, et al. Effects of definitive and salvage radiotherapy on the distribution of lymphocyte subpopulations in prostate cancer patients. Strahlenther Onkol. (2017) 193:648–55. doi: 10.1007/s00066-017-1144-7
34. Koukourakis MI, Giatromanolaki A. Tumor draining lymph nodes, immune response, and radiotherapy: Towards a revisal of therapeutic principles. Biochim Biophys Acta Rev Cancer. (2022) 1877:188704. doi: 10.1016/j.bbcan.2022.188704
35. Dovsak T, Ihan A, Didanovič V, Kansky A, Verdenik M, Hren NI., et al. Effect of surgery and radiotherapy on complete blood count, lymphocyte subsets and inflammatory response in patients with advanced oral cancer. BMC Cancer. (2018) 18:235. doi: 10.1186/s12885-018-4136-9
36. Christensen E, Pintilie M, Evans KR, Lenarduzzi M, Ménard C, Catton CN, et al. Longitudinal cytokine expression during IMRT for prostate cancer and acute treatment toxicity. Clin Cancer Res. (2009) 15:5576–83. doi: 10.1158/1078-0432.CCR-09-0245
37. Kopčalić K, Matić IZ, Besu I, Stanković V, Bukumirić Z, Stanojković TP, et al. Circulating levels of IL-6 and TGF-β1 in patients with prostate cancer undergoing radiotherapy: associations with acute radiotoxicity and fatigue symptoms. BMC Cancer. (2022) 22:1167. doi: 10.1186/s12885-022-10255-6.37
38. Seto Y, Kaneko Y, Mouri T, Shimizu D, Morimoto Y, Tokuda S, et al. Changes in serum transforming growth factor-beta concentration as a predictive factor for radiation-induced lung injury onset in radiotherapy-treated patients with locally advanced lung cancer. Transl Lung Cancer Res. (2022) 11:1823–34.38. doi: 10.21037/tlcr-22-229
39. Boothe DL, Coplowitz S, Greenwood E, Barney CL, Christos PJ, Parashar B, et al. Transforming growth factor β-1 (TGF-β1) is a serum biomarker of radiation induced fibrosis in patients treated with intracavitary accelerated partial breast irradiation: preliminary results of a prospective study. Int J Radiat Oncol Biol Phys. (2013) 87:1030–6. doi: 10.1016/j.ijrobp.2013.08.045
Keywords: radiotherapy, prostate cancer, hypofractionation, toxicity, immune cells, cytokines
Citation: D’Auria F, Valvano L, Calice G, D’Esposito V, Cabaro S, Formisano P, Bianchino G, Traficante A, Bianculli A, Lazzari G, Statuto T and Rago L (2024) Hypofractionated radiotherapy with simultaneous integrated boost for localized prostate cancer patients: effects on immune system and prediction of toxicity. Front. Immunol. 15:1457839. doi: 10.3389/fimmu.2024.1457839
Received: 01 July 2024; Accepted: 08 October 2024;
Published: 28 October 2024.
Edited by:
Giandomenico Roviello, University of Firenze, ItalyReviewed by:
Rodney Macedo Gonzales, Columbia University, United StatesFrancolini Giulio, University of Florence, Italy
Copyright © 2024 D’Auria, Valvano, Calice, D’Esposito, Cabaro, Formisano, Bianchino, Traficante, Bianculli, Lazzari, Statuto and Rago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fiorella D’Auria, ZmlvcmUuZGF1cmlhQHZpcmdpbGlvLml0; Giovanni Calice, Z2lvdmFubmkuY2FsaWNlQGNyb2IuaXQ=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
§ORCID: Fiorella D’Auria, orcid.org/0000-0002-3030-1651
Luciana Valvano, orcid.org/0000-0002-6382-7318