
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 19 August 2024
Sec. Multiple Sclerosis and Neuroimmunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1454474
This article is part of the Research Topic Neuroanatomical and Molecular Biomarkers for Multiple Sclerosis Progression and Therapeutic Response View all 3 articles
 Raquel Sainz-Amo1,2†
Raquel Sainz-Amo1,2† Alexander Rodero Romero2†
Alexander Rodero Romero2† Enric Monreal1†
Enric Monreal1† Juan Luis Chico García1
Juan Luis Chico García1 José Ignacio Fernández Velasco2
José Ignacio Fernández Velasco2 Noelia Villarrubia2Jose Luis Veiga González2
Noelia Villarrubia2Jose Luis Veiga González2 Susana Sainz de la Maza1Fernando Rodríguez Jorge1
Susana Sainz de la Maza1Fernando Rodríguez Jorge1 Jaime Masjuan1
Jaime Masjuan1 Lucienne Costa-Frossard1
Lucienne Costa-Frossard1 Luisa María Villar2*
Luisa María Villar2*Introduction: Alemtuzumab is a highly effective pulsed immune reconstitution therapy for multiple sclerosis (MS).
Aim: To evaluate serum neurofilament light chain (sNfL) and serum glial fibrillary acidic protein (sGFAP) in patients with relapsing-remitting MS who have been treated with Alemtuzumab over the course of 2 years.
Methods: This prospective study involved MS patients treated with Alemtuzumab at a referral MS center. Both sNfL and sGFAP were analyzed at baseline and then again at 6, 12, and 24 months post-treatment using the single molecule array (SiMoA) technique. We also recruited matched healthy controls (HCs) for comparison.
Results: The study included 46 patients (with a median age of 34.2 [Interquartile range (IQR), 28.7–42.3] years, 27 of which were women [58%]) and 76 HCs. No differences in demographic characteristics were observed between patients and HC. The median disease duration was 6.22 (IQR, 1.56–10.13) years. The median annualized relapse rate before treatment was 2 (IQR, 1–3). At baseline, sNfL and sGFAP levels were higher in MS patients (median of 18.8 [IQR, 10.7–52.7] pg/ml and 158.9 [IQR, 126.9–255.5] pg/ml, respectively) when compared to HC (6.11 [IQR, 2.03–8.54] pg/ml and 91.0 [72.6–109] pg/ml, respectively) (p<0.001 for both comparisons). The data indicates that 80% of patients had high (≥10 pg/ml) sNfL values at baseline. We observed a significant decrease in sNfL levels at 6 (65%, p = 0.02), 12 (70.8%, p<0.001), and 24 (78.1%, p<0.001) months. sNfL reached similar levels to HC only after 24 months of Alemtuzumab treatment. During the follow-up period, no changes were identified in the sGFAP values.
Conclusion: Alemtuzumab leads to the normalization of sNfL values in MS patients after 2 years of treatment, with no apparent effect on sGFAP values.
Serum biomarkers have emerged as a useful tool in multiple sclerosis (MS), especially since the establishment of fourth-generation immune assays over the past decade (1, 2). Neurofilaments are cytoskeletal proteins whose release into CSF and blood is a quantitative measure of neuronal injury (3). Serum neurofilament light chain (sNfL) in MS has been validated as a biomarker for clinical and radiological inflammation and as a predictor of disease worsening (4–7).
Serum glial fibrillary acidic protein (sGFAP) is the main intermediate filament of astrocytes (8). sGFAP has been suggested as a biomarker to detect progressive MS and disability deterioration separate from inflammation (9–12). The combination of both biomarkers seems to enhance predictive accuracy (9, 10).
Alemtuzumab, a humanized monoclonal antibody, is a significant figure among the current pulsed immune reconstitution therapies. It works by binding to CD52, leading to a substantial reduction in autoreactive T and B-lymphocytes (13). This action paves the way for a new immune cell population, which is less likely to launch an immunological attack on the central nervous system (CNS) (14–17). The effectiveness of Alemtuzumab has been proven through rigorous clinical investigations, including phase II (CAMMS223) and phase III (CARE-MS I & II) trials, as well as observational studies with patients suffering from highly active disease (18–21).
The impact of Alemtuzumab on both sNfL and sGFAP levels has begun to be studied (22), but the evidence is limited.
We aimed to evaluate sNfL and sGFAP in patients with relapsing-remitting MS (RRMS) treated with Alemtuzumab over 2 years and to compare their values with a cohort of matched healthy controls (HCs). In addition, we intended to analyze the relationship between sNfL and sGFAP values and changes in disease course in terms of no evidence of disease activity-3 (NEDA-3), risk of relapse-associated worsening (RAW), and progression independent of relapse activity (PIRA).
This was an observational study with prospective data collection, aligning with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Patients were recruited for the study at the Hospital Universitario Ramón y Cajal in Madrid, Spain. We consecutively enrolled patients with RRMS who began Alemtuzumab treatment between July 2015 and January 2022. These patients were followed until January 31, 2024. Both treatment-naïve and previously treated patients with one or more disease-modifying therapies (DMTs) were included. A wash-out period of four weeks was established for patients previously treated with monoclonal antibodies or fingolimod. No wash-out period was used for other drugs. Age, sex, and body mass index matched HCs were recruited between August 2023 and February 2024.
The study received approval from the Hospital Universitario Ramón y Cajal ethics committee, and all patients, along with HC, signed an informed consent prior to participation. Anonymized data, which support the findings of this study, will be available to any qualified investigator upon reasonable request for 3 years following the publication of the study.
Patients received 60 mg of Alemtuzumab intravenously for five consecutive days. After 12 months, they were given a repeated dose of 36 mg intravenously over three consecutive days. Additional doses of 36 mg of Alemtuzumab were utilized at the signs of new disease activity, such as a relapse or the detection of new, enlarging, or contrast-enhancing MRI lesions. Premedication with 1000 mg of intravenous methylprednisolone, an oral antihistamine, paracetamol, and omeprazole was given. Furthermore, patients received prophylactic treatments with acyclovir and trimethoprim/sulfamethoxazole.
Demographic, clinical, and radiological variables were collected at baseline. Experienced neurologists conducted all EDSS evaluations at least every 3 months and additional examinations in the event of a relapse. A baseline MRI was taken within a month prior to the start of treatment in accordance with established clinical protocols. Subsequent control MRI studies were done annually.
Patient blood specimens were collected just before initiating Alemtuzumab treatment and again at 6, 12, and 24 months after that. Serum sample aliquots were procured and stored at -80° until they were processed.
sNfL and sGFAP were quantified using an SR-X instrument (Quanterix, Lexington, MA) with the single molecule array (SIMOA) technique (Quanterix, Billerica, MA). We employed the NF-light Advantage Kit (Quanterix, Billerica, MA) and the Serum GFAP Discovery Kit (Quanterix, Billerica, MA), respectively, following the manufacturer’s instructions. The mean inter- and intra-assay coefficients equaled 6% and 7% for sNfL and 6% and 10% for sGFAP, respectively. The research team handling the evaluation of the serum samples remained unaware of the clinical data.
We applied the revised 2017 McDonald criteria for patient diagnosis (23). Disability was assessed using the EDSS score (24). Confirmed disability worsening was defined as an increase of at least 1.5 points in the EDSS if the baseline score was 0, a rise of at least 1 point if the previous EDSS was between 1 and 5, and a minimum 0.5 point increase for patients with a baseline EDSS of 5.5 or higher (25). NEDA-3 was defined as the absence of relapses, disability worsening, and new and/or enlarged T2 lesions or gadolinium-enhancing lesions on MRI (26). Conversely, patients experiencing either a relapse, MRI activity or an exacerbation of neurological disability were classified as having evidence of disease activity-3 (EDA-3). RAW and PIRA were defined as previously described (27).
The cut-off applied for sNfL and sGFAP levels was established at the 90th percentile value of the corresponding HC, which was 10 pg/ml for sNfL and 140 pg/ml for sGFAP, in line with the benchmarks used in previous studies (5, 7, 28).
Descriptive analyses were summarized using absolute and relative proportions for categorical variables, and differences were examined using either a χ² or Fisher’s exact test. The median with an interquartile range (IQR) was employed to describe continuous variables, and associations between groups were evaluated using the Kruskal-Wallis and Mann Whitney-U tests. We performed statistical analyses using the GraphPad Prism 9.0 software (GraphPad Prism Inc., San Diego, CA). All tests were two-tailed, and a significance level of P < 0.05 was deemed significant.
We incorporated 46 patients (27 women (58%)) into the study, for a combined total of 77 (Figure 1), all of whom initiated Alemtuzumab in a single referral MS center. Table 1 displays the clinical and demographic data of the cohort, as well as their matched HC.
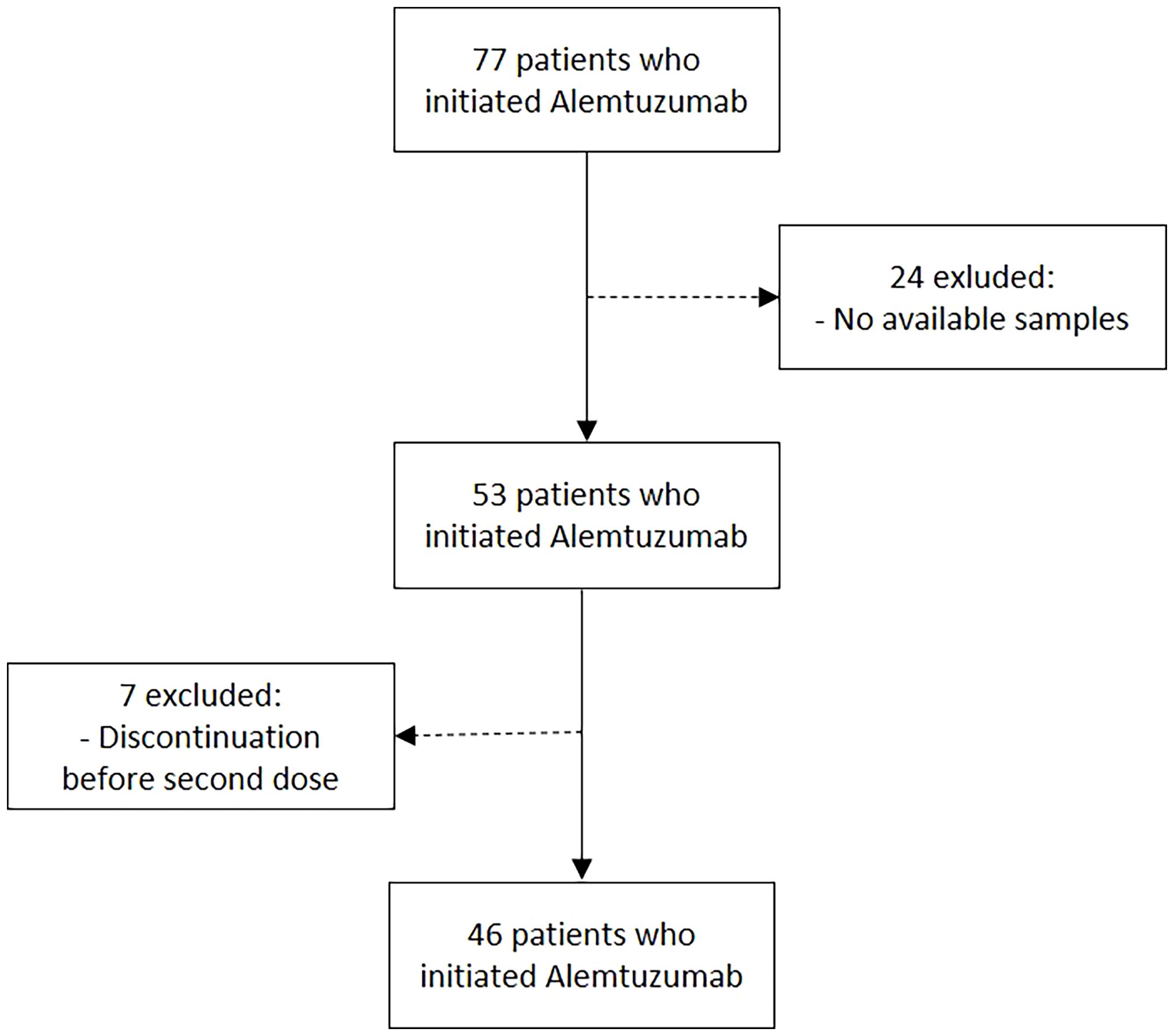
Figure 1. Flowchart of patients included.
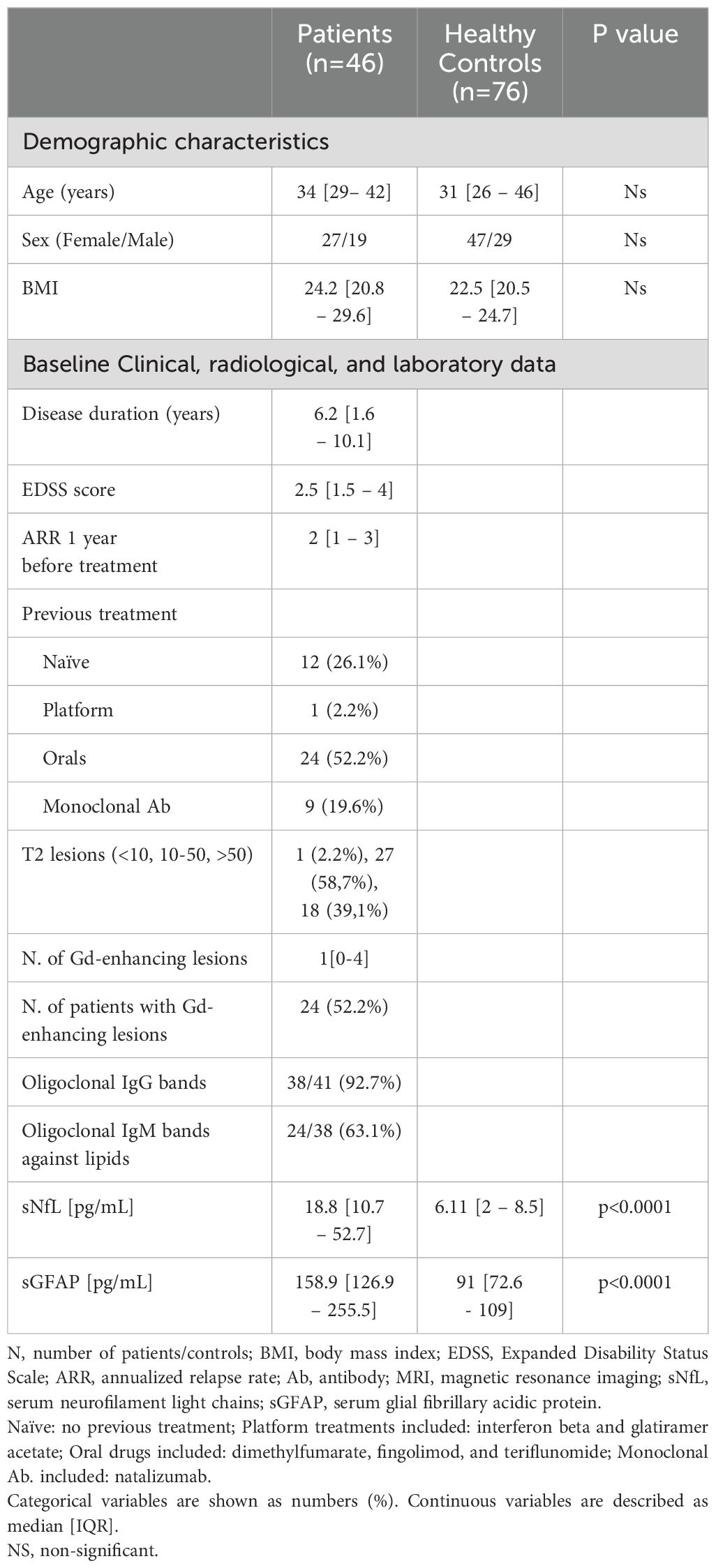
Table 1. Baseline data.
The median age (IQR) of Alemtuzumab-treated patients was 34.2 (28.7–42.3) years. The disease duration at the onset of Alemtuzumab was 6.2 (1.6–10.1) years. Twelve patients (26.1%) were naïve, and 34 (73.9%) switched from other DMTs due to lack of efficacy (24, 52.2%) or safety concerns (10, 21.7%). The annualized relapse rate (ARR) the year prior to treatment initiation was 2 (1–3). Eighteen patients (39.1%) had more than 50 lesions in their baseline MRI, while 24 (52.2%) had gadolinium-enhancing lesions.
The values of sNfL and sGFAP were higher at baseline in MS patients compared to HC (p<0.001 for both comparisons).
A substantial decrease in sNfL levels was observed at 6 (65%, p = 0.02), 12 (70.8%, p<0.001), and 24 months (78.1%, p<0.001). sNfL levels were akin to those of the HC only after 24 months of Alemtuzumab treatment (Figure 2). No changes in sGFAP values were identified during the follow-up period (Figure 2).
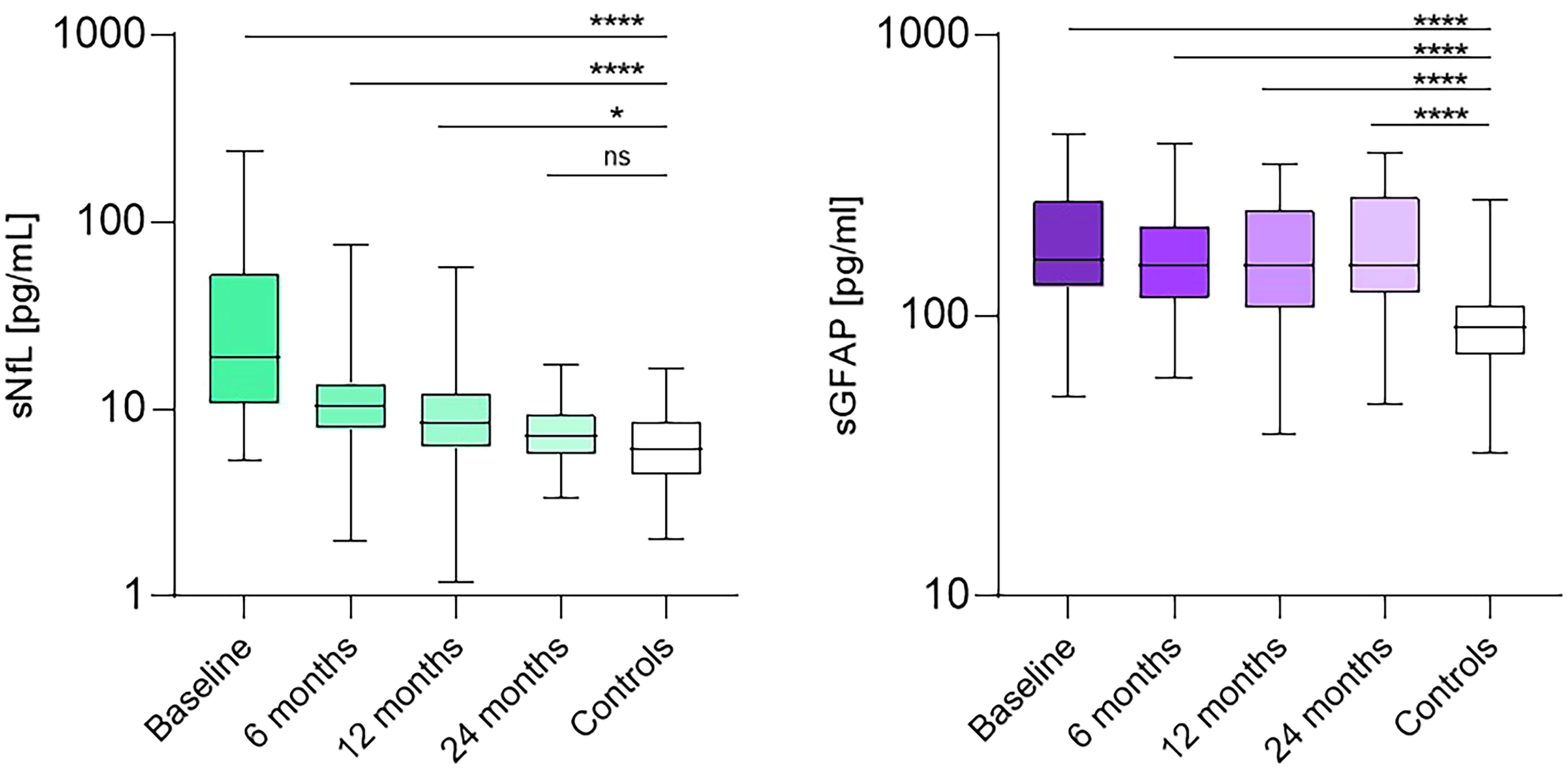
Figure 2. sNfL (pg/ml) values of controls and patients at baseline and after 6, 12, 24 months of treatment. sGFAP (pg/ml) values of controls and patients at baseline and after 6, 12, and 24 months of treatment. NS, non-significant, ****: p<0.0001, *: p<0.01.
We did not find differences in sNfL and SGFAP values between naïve and previously treated patients neither at baseline nor at 6, 12, 24 months. Likewise, we did not find differences between sexes (Supplementary Table 1).
Thirty-seven patients (80%) exhibited high (≥10 pg/ml) sNfL values at baseline. Patients presenting these high sNfL values had a higher number of gadolinium-enhancing lesions at baseline (median 1 [IQR 0 – 5] vs. 0 [0 – 0.75] p = 0.02).
Patients with high sNfL at the baseline had a greater number of new T2 lesions in the MRI performed after the first year of treatment (1 [0–2] vs. 0 [0-0], p=0.006). Similarly, NEDA-3 (44.2% vs. 88.9%, p=0.02) was achieved by a smaller proportion of these patients during the first year. However, these differences dissipated in the following years of follow-up (39.4% vs 78%, p=0.06 after second year).
We next analyzed the risks associated with RAW and PIRA. Median [IQR] follow-up time was 5.8 years [4.8-7.7], 76% of patients were followed up for at least five years. No significant differences were noted between patients with high sNfL at baseline and those with lower values concerning the risk of RAW (HR 0.3 [0.04 – 2.1], p=0.2). However, throughout the follow-up, no patients with low sNfL experienced either RAW or PIRA. In contrast, for the 27 patients with high sNfL who were followed 5 years post-Alemtuzumab administration, the cumulative incidences of RAW and PIRA were 15% and 14.4%, respectively. Baseline sGFAP levels served as a differentiating factor for patients who encountered RAW during follow-up, as they exhibited lower values compared to those suffering from PIRA (99 [79–123] vs. 178 [147–276], p = 0.02). Furthermore, patients with higher sGFAP values demonstrated a tendency for an increased risk of PIRA over time (HR 3.7 [0.5–27.5], p = 0.2) (Figure 3).
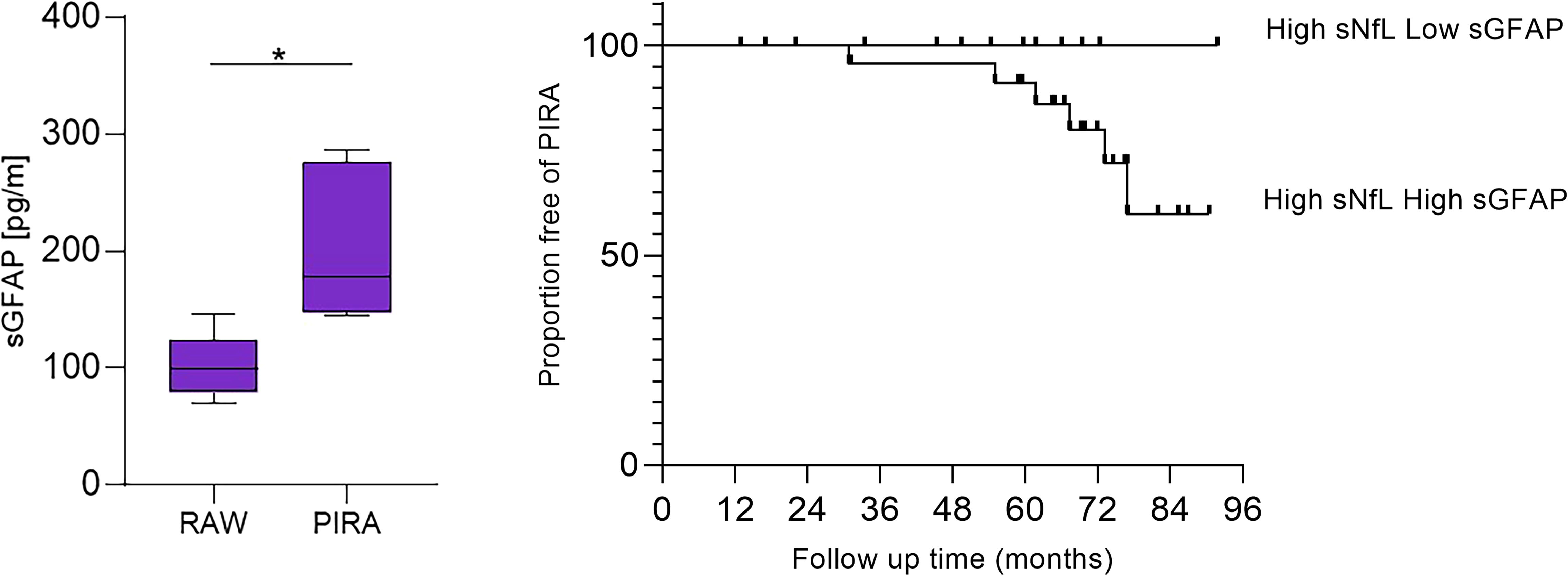
Figure 3. Comparison of baseline sGFAP (pg/ml) values in patients with high sNfL (pg/ml). Kaplan-Meier comparing time to PIRA in patients with high sNfL (pg/ml) who had high versus low sGFAP (pg/ml). *: p=0.02.
sNfL levels indicate acute axonal damage and are associated with acute inflammatory activity seen as clinical relapses or T2-weighted or contrast-enhancing lesions (29). These levels can be used as a biomarker for monitoring inflammation (5) and disease progression (7). Combining sNfL levels with sGFAP might enhance the ability to identify patients at risk of disease progression (10).
The early administration of high-efficacy DMTs (HE-DMTs) in patients with high sNfL levels has been associated with no disability worsening (7). However, there are only a few studies focused on the analysis of sNfL values over time in patients who have started on a specific HE-DMT. Additionally, there are even fewer studies that analyze both sNfL and sGFAP.
We aimed to explore the role of both biomarkers in a cohort of highly active patients treated with Alemtuzumab. First, we analyzed sNFL and sGFAP over 2 years and compared the values to a cohort of matched HCs. We observed that sNfL decreased progressively, as described in other cohorts (22, 30–33), but did not reach similar values to those of the HC until a follow-up of two years. A reduction in sNfL was also described two years after alemtuzumab initiation in other cohort of patients treated with alemtuzumab who showed moderate levels at treatment onset (22). We could show that results are similar in a more active cohort with clearly higher baseline sNfL values. Likewise, a clear decrease of sNfL was observed in the Alemtuzumab arm of the CARE-MS I study (27), this decrease was higher compared with patients treated with Interferon-beta-1a. In our cohort we also see a decrease in sNfL values until the normalization is reached and there is no difference with HCs. Higher baseline sNfL values were associated with higher T2 lesion load, as we describe in our cohort.
By contrast, in patients with high sGFAP levels at treatment initiation these levels remained stable over time and were higher than those of HC, which confirms previous findings in which symptomatic controls were used as control group (22).
Alemtuzumab eliminates the abnormal B and T cells (13) and let the immune system to reconstitute a normal lymphocyte response. This seems to work very efficiently in patients who have not an intrathecal activation of the innate immune response, reflected by the high sGFAP values. By contrast, in patients with increased sGFAP values a trend to a higher risk of PIRA was observed, despite the normalization of sNfL. The association of sGFAP with high risk of disability progression was already described (10). Our data strongly suggest that normalization of sGFAP values it crucial for avoiding disease progression in MS.
We examined whether baseline sNfL was associated with an increase in disability over time. We set a cut-off value of 10 pg/mL for sNfL and 140 pg/mL for sGFAP based on the 90th percentile of our population of matched HCs. Patients with elevated sNfL displayed more clinical and radiological activity during the initial year. However, these differences were not apparent in the following years. Along with the normalization of sNfL, this information emphasizes the effectiveness of Alemtuzumab in managing axonal damage and inflammation.
No patient with low sNfL values demonstrated RAW or PIRA during follow-up. Additionally, high levels of sGFAP in this patient group were associated with a trend toward a higher risk of PIRA. These data suggest that astrogliosis (34) may remain active despite Alemtuzumab treatment and contribute to patient disability worsening independent of relapses.
The primary limitation of our study was the reduced sample size. These findings should be validated in larger, multicenter cohorts.
In conclusion, we observed a normalization of sNfL levels at follow-up, while sGFAP concentrations remained unchanged. This suggests that Alemtuzumab reduces acute axonal damage but has little or no effect on astrogliosis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comite ético de Investigación clínica GAE Ramon y Cajal Area 4. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
RA: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Visualization. AR: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Visualization. EM: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Visualization. JG: Formal analysis, Writing – review & editing. JG: Writing – review & editing. NV: Writing – review & editing. JV: Writing – review & editing. Sd: Writing – review & editing. FJ: Writing – review & editing. JM: Writing – review & editing. LC: Writing – review & editing. LV: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants RD21/0002/0053 from La Red Española de Enfermedades Inflamatorias (REI) and PI21/00828, integrated in the Plan Estatal I+D+i, cofunded by Insti-tuto de Salud Carlos III (ISCIII)-Subdirección General de Evaluación and Fondo Europeo de Desarrollo Regional (FEDER; “Otra manera de hacer Europa”).
Authors acknowledge the nurses Silvia Morel and Ana María Pérez Macias, MSc (Neurology Dept, Ramón y Cajal University Hospital, Madrid, Spain), for their help in obtaining the blood samples, and the technician Sonia Ortega (Inmunology Dept, Ramón y Cajal University Hospital, Madrid, Spain) for her technical support.
RS-A reported receiving research travel support from Roche and Janssen outside the submitted work. EM reported receiving research grants, travel support, or honoraria for speaking engagements from Biogen, Sanofi, Merck, Novartis, Almirall, Roche, Bristol Myers Squibb, and Janssen outside the submitted work. JF reported receiving research travel support from Roche and Janssen outside the submitted work. SM reported receiving personal fees from Almirall, Bristol Myers Squibb, and Teva outside the submitted work and receiving compensation for lectures or travel expenses from Merck Serono, Biogen, Sanofi Genzyme, Roche, Janssen, and Novartis. JC reported receiving personal fees from Sanofi outside the submitted work and receiving speaker honoraria from Biogen Idec and Sanofi. FR reported receiving personal fees from Sanofi outside the submitted work and receiving speaker honoraria from Biogen Idec and Sanofi. LF reported receiving speaker fees and travel support and/or serving on advisory boards for Biogen, Sanofi, Merck, Bayer, Novartis, Roche, Teva, Celgene, Ipsen, Biopas, Bristol Myers Squibb, Janssen, and Almirall. LV reported receiving grants and personal fees from Merck, Roche, Sanofi Genzyme, Bristol Myers Squibb, Celgene, Biogen, and Novartis outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1454474/full#supplementary-material
1. Khalil M, Teunissen CE, Otto M, Piehl F, Sormani MP, Gattringer T, et al. Neurofilaments as biomarkers in neurological disorders. Nat Rev Neurol. (2018) 14:577–89. doi: 10.1038/s41582-018-0058-z
2. Petzold A. Glial fibrillary acidic protein is a body fluid biomarker for glial pathology in human disease. Brain Res. (2015) 1600:17–31. doi: 10.1016/j.brainres.2014.12.027
3. Gafson AR, Jiang X, Shen C, Kapoor R, Zetterberg H, Fox RJ, et al. Serum neurofilament light and multiple sclerosis progression independent of acute inflammation. JAMA Netw Open. (2022) 5:e2147588. doi: 10.1001/jamanetworkopen.2021.47588
4. Disanto G, Barro C, Benkert P, Naegelin Y, Schädelin S, Giardiello A, et al. Serum Neurofilament light: A biomarker of neuronal damage in multiple sclerosis. Ann Neurol. (2017) 81:857–70. doi: 10.1002/ANA.24954
5. Benkert P, Meier S, Schaedelin S, Manouchehrinia A, Yaldizli Ö, Maceski A, et al. Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurol. (2022) 21:246–57. doi: 10.1016/S1474-4422(22)00009-6
6. Thebault S, Abdoli M, Fereshtehnejad SM, Tessier D, Tabard-Cossa V, Freedman MS. Serum neurofilament light chain predicts long term clinical outcomes in multiple sclerosis. Sci Rep. (2020) 10. doi: 10.1038/S41598-020-67504-6
7. Monreal E, Fernández-Velasco JI, García-Sánchez MI, Sainz de la Maza S, Llufriu S, Álvarez-Lafuente R, et al. Association of serum neurofilament light chain levels at disease onset with disability worsening in patients with a first demyelinating multiple sclerosis event not treated with high-efficacy drugs. JAMA Neurol. (2023) 80:397–403. doi: 10.1001/JAMANEUROL.2023.0010
8. Yang Z, Wang KK. Glial fibrillary acidic protein: from intermediate filament assembly and gliosis to neurobiomarker. Trends Neurosci. (2015) 38:364–74. doi: 10.1016/j.tins.2015.04.003
9. Barro C, Healy BC, Liu Y, Saxena S, Paul A, Polgar-Turcsanyi M, et al. Serum GFAP and nfL levels differentiate subsequent progression and disease activity in patients with progressive multiple sclerosis. Neurology(R) Neuroimmunol Neuroinflamm. (2022) 10. doi: 10.1212/NXI.0000000000200052
10. Meier S, Willemse EAJ, Schaedelin S, Oechtering J, Lorscheider J, Melie-Garcia L, et al. Serum glial fibrillary acidic protein compared with neurofilament light chain as a biomarker for disease progression in multiple sclerosis. JAMA Neurol. (2023) 80:287–97. doi: 10.1001/JAMANEUROL.2022.5250
11. Abdelhak A, Foschi M, Abu-Rumeileh S, Yue JK, D'Anna L, Huss A, et al. Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat Rev Neurol. (2022) 18:158–72. doi: 10.1038/s41582-021-00616-3
12. Högel H, Rissanen E, Barro C, Matilainen M, Nylund M, Kuhle J, et al. Serum glial fibrillary acidic protein correlates with multiple sclerosis disease severity. Mult Scler. (2020) 26:210–9. doi: 10.1177/1352458518819380
13. Ruck T, Bittner S, Wiendl H, Meuth SG. Alemtuzumab in multiple sclerosis: mechanism of action and beyond. Int J Mol Sci. (2015) 16:16414–39. doi: 10.3390/ijms160716414
14. Cox AL, Thompson SA, Jones JL, Robertson VH, Hale G, Waldmann H, et al. Lymphocyte homeostasis following therapeutic lymphocyte depletion in multiple sclerosis. Eur J Immunol. (2005) 35:3332–42. doi: 10.1002/eji.200535075
15. Jones JL, Phuah CL, Cox AL, Thompson SA, Ban M, Shawcross J, et al. IL-21 drives secondary autoimmunity in patients with multiple sclerosis, following therapeutic lymphocyte depletion with Alemtuzumab (Campath-1H). J Clin Invest. (2009) 119:2052–61. doi: 10.1172/JCI37878
16. Thompson SA, Jones JL, Cox AL, Compston DA, Coles AJ. B-cell reconstitution and BAFF after Alemtuzumab (Campath-1H) treatment of multiple sclerosis. J Clin Immunol. (2010) 30:99–105. doi: 10.1007/s10875-009-9327-3
17. Havari E, Turner MJ, Campos-Rivera J, Shankara S, Nguyen TH, Roberts B, et al. Impact of Alemtuzumab treatment on the survival and function of human regulatory T cells in vitro. Immunology. (2014) 141:123–31. doi: 10.1111/imm.12178
18. Ziemssen T, Thomas K. Alemtuzumab in the long-term treatment of relapsing-remitting multiple sclerosis: an update on the clinical trial evidence and data from the real world. Ther Adv Neurol Disord. (2017) 10:343–59. doi: 10.1177/1756285617722706
19. Havrdova E, Arnold DL, Cohen JA, Hartung HP, Fox EJ, Giovannoni G, et al. Alemtuzumab CARE-MS I 5-year follow-up: durable efficacy in the absence of continuous MS therapy. Neurology. (2017) 89:1107–16. doi: 10.1212/WNL.0000000000004313
20. Coles AJ, Cohen JA, Fox EJ, Giovannoni G, Hartung HP, Havrdova E, et al. Alemtuzumab CARE-MS II 5-year follow-up: efficacy and safety findings. Neurology. (2017) 89:1117–26. doi: 10.1212/WNL.0000000000004354
21. Ziemssen T, Bass AD, Berkovich R, Comi G, Eichau S, Hobart J, et al. Efficacy and safety of Alemtuzumab through 9 years of follow-up in patients with highly active disease: post hoc analysis of CARE-MS I and II patients in the TOPAZ extension study. CNS Drugs. (2020) 34:973–88. doi: 10.1007/s40263-020-00749-x
22. Sandgren S, Novakova L, Nordin A, Axelsson M, Malmeström C, Zetterberg H, et al. A five-year observational prospective mono-center study of the efficacy of Alemtuzumab in a real-world cohort of patients with multiple sclerosis. Front Neurol. (2023) 14:1265354. doi: 10.3389/fneur.2023.1265354
23. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
24. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. (1983) 33:1444–52. doi: 10.1212/WNL.33.11.1444
25. Weinshenker BG, Issa M, Baskerville J. Meta-analysis of the placebo-treated groups in clinical trials of progressive MS. Neurology. (1996) 46:1613–9. doi: 10.1212/WNL.46.6.1613
26. Giovannoni G, Turner B, Gnanapavan S, Offiah C, Schmierer K, Marta M. Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Mult Scler Relat Disord. (2015) 4:329–33. doi: 10.1016/j.msard.2015.04.006
27. Lublin FD, Häring DA, Ganjgahi H, Ocampo A, Hatami F, Čuklina J, et al. How patients with multiple sclerosis acquire disability. Brain. (2022) 145:3147–316. doi: 10.1093/BRAIN/AWAC016
28. Tybirk L, Hviid CVB, Knudsen CS, Parkner T. Serum GFAP - reference interval and preanalytical properties in Danish adults. Clin Chem Lab Med. (2022) 60:1830–8. doi: 10.1515/CCLM-2022-0646
29. Thebault S, Bose G, Booth R, Freedman MS. Serum neurofilament light in MS: The first true blood-based biomarker? Mult Scler. (2022) 28:1491–7. doi: 10.1177/1352458521993066
30. Nötzel M, Werder LI, Ziemssen T, Akgün K. Ella versus simoa serum neurofilament assessment to monitor treatment response in highly active multiple sclerosis patients. Int J Mol Sci. (2022) 23:12361. doi: 10.3390/ijms232012361
31. Delcoigne B, Manouchehrinia A, Barro C, Benkert P, Michalak Z, Kappos L, et al. Blood neurofilament light levels segregate treatment effects in multiple sclerosis. Neurology. (2020) 94:e1201–12. doi: 10.1212/WNL.0000000000009097
32. Akgün K, Kretschmann N, Haase R, Proschmann U, Kitzler HH, Reichmann H, et al. Profiling individual clinical responses by high-frequency serum neurofilament assessment in MS. Neurol Neuroimmunol Neuroinflamm. (2019) 6:e555. doi: 10.1212/NXI.0000000000000555
33. Kuhle J, Daizadeh N, Benkert P, Maceski A, Barro C, Michalak Z, et al. Sustained reduction of serum neurofilament light chain over 7 years by Alemtuzumab in early relapsing-remitting MS. Mult Scler. (2022) 28:573–82. doi: 10.1177/13524585211032348
Keywords: alemtuzumab, sNfL, sGFAP, multiple sclerosis, SiMoA
Citation: Sainz-Amo R, Rodero Romero A, Monreal E, Chico García JL, Fernández Velasco JI, Villarrubia N, Veiga González JL, Sainz de la Maza S, Rodríguez Jorge F, Masjuan J, Costa-Frossard L and Villar LM (2024) Effect of alemtuzumab over sNfL and sGFAP levels in multiple sclerosis. Front. Immunol. 15:1454474. doi: 10.3389/fimmu.2024.1454474
Received: 25 June 2024; Accepted: 05 August 2024;
Published: 19 August 2024.
Edited by:
Tjalf Ziemssen, University Hospital Carl Gustav Carus, GermanyReviewed by:
Nuria Álvarez-Sánchez, St Michael’s Hospital, CanadaCopyright © 2024 Sainz-Amo, Rodero Romero, Monreal, Chico García, Fernández Velasco, Villarrubia, Veiga González, Sainz de la Maza, Rodríguez Jorge, Masjuan, Costa-Frossard and Villar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luisa María Villar, bHVpc2FtYXJpYS52aWxsYXJAc2FsdWQubWFkcmlkLm9yZw==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.