 Loredana Ungureanu1,2
Loredana Ungureanu1,2 Alina Florentina Vasilovici1,2*Salomea-Ruth Halmágyi1,3Ioana Irina Trufin3
Alina Florentina Vasilovici1,2*Salomea-Ruth Halmágyi1,3Ioana Irina Trufin3 Adina Patricia Apostu1,3
Adina Patricia Apostu1,3 Simona Corina Şenilă1,2
Simona Corina Şenilă1,2- 1Department of Dermatology, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania
- 2Department of Dermatology, Emergency County Hospital, Cluj-Napoca, Romania
- 3Department of Dermatology, Clinical Hospital of Infectious Diseases, Cluj-Napoca, Romania
Melanoma is the most severe form of skin cancer with an incidence that is increasing all over the world. Melanoma cells derive from normal melanocytes and share different melanocyte-specific antigens, the same antigens against which an immune reaction develops in vitiligo, a skin disease characterized by autoimmune-mediated melanocyte destruction. The purpose of this review is to present the autoimmune-mediated melanocyte destruction associated with melanoma development, progression and treatment. Patients with vitiligo seem to have a lower chance of developing melanoma. On the other hand, patients with melanoma can develop depigmented lesions even at distant sites from the primary tumor, defined as melanoma-associated leukoderma (MAL). Drug-associated leukoderma (DAL) was also described in melanoma patients treated with immunotherapy or targeted therapy and it seems to be a favorable prognostic factor. Clinically, MAL and DAL can be diagnosed as vitiligo and there are few differences between these three entities. In this review, the incidence of DAL in melanoma patients treated with different therapies was researched in the literature and patient outcome was recorded, with studies showing a prolonged disease-free survival in melanoma patients with DAL, treated with immune checkpoint inhibitors. Further studies are however needed to understand the dynamics of autoimmune-mediated melanocyte destruction.
1 Introduction
Melanoma, the malignant tumor derived from melanocytes, is the most threatening form of skin tumors, with a continuously increasing incidence all over the world (1, 2). Although it represents less than 5% of all skin cancers, melanoma is responsible for the greatest number of skin cancer-related deaths worldwide (3). Due to the high mutational burden, melanoma is an immunogenic tumor, which is highlighted by its ability to undergo spontaneous regression and also immunotherapy-induced regression (3–7). Cancer immunity relies on the recognition of antigens by the host’s immune system. A large number of melanoma antigens that are recognized by the immune system have been described, more than for any other cancer (5). Melanoma-specific cytotoxic T lymphocytes have been observed both in the skin that surrounds the tumor and in the patient’s blood. Melanoma antigens that can be recognized by T-cells are classified as follows: (a) tumor-specific neo-antigens derived from DNA mutations, (b) cancer-germline antigens, which are tumor-specific shared antigens (3), melanocyte-specific differentiation antigens (e.g. gp100, MART-1, tyrosinase, TRP-1, TRP-2) and (4) other antigens such as viral antigens or overexpressed proteins (8). Melanoma cells originate from normal melanocytes, which explain why these two types of cells share many melanocyte antigens that are expressed by melanocytes in the skin of healthy donors, in the healthy skin of vitiligo patients and by tumor cells in melanoma patients (9). Melanocyte-specific antigens are proteins, and peptides that derive from them can be recognized by antigen-specific CD8+ T cells, and high levels of melanocyte-specific CD8+ T cells can be detected in the blood and among tumor-infiltrating lymphocytes in melanoma, as well as in patients with vitiligo (9).
Vitiligo is an autoimmune skin disease characterized by circumscribed or generalized depigmentation of the skin and mucosa, as a result of autoimmune-mediated melanocyte destruction (10). The importance of autoimmunity is highlighted by the frequent association with other autoimmune disorders and especially by the presence of autoantibodies against melanocyte differentiation antigens in the blood of a significantly higher percentage of patients with vitiligo compared with healthy individuals (5). Moreover, circulating melanocyte-specific CD8+ T cells, as well as infiltrates of T cells at the margins of active lesions have been described in most patients (11).
The present review aims at providing an overview of autoimmune-mediated melanocyte destruction that can appear in association with melanoma, from the risk of developing melanoma to melanoma prognosis and response to therapy. In order to assess the incidence of patients treated with different therapies that developed MAL, we researched the literature (PubMed) using these terms: “vitiligo melanoma treatment”, “vitiligo melanoma immunotherapy”, “vitiligo melanoma anti-PD1 therapy”. Only articles in English were selected and duplicates were excluded.
2 Autoimmune-mediated melanocyte destruction and the risk of developing melanoma
Due to the absence of melanin in depigmented lesions and secondary to incidental and therapeutic UV light exposure, concerns were raised about the development of skin cancer, especially melanoma, in vitiligo patients. However, genetic studies suggested a lower susceptibility of developing melanoma in patients with vitiligo (12). A genome-wide association study in patients with vitiligo showed significant associations between vitiligo and several genes that regulate immunity (13). Vitiligo was associated with a polymorphism in the gene that codes the main enzyme involved in melanin synthesis, tyrosinase (TYR gene). Interestingly, the TYR allele that confers risk for vitiligo is protective against melanoma, suggesting that strong anti-tyrosinase expression protects vitiligo patients against melanoma (13). Moreover, in a meta-analysis conducted by Liu et al. human-leukocyte antigen – A2 proved to be the protective allele against melanoma development, and at the same time the risk allele for vitiligo development (14). According to Wu et al. the inverse relationship might indicate that different or opposed biological pathways mediate vitiligo and skin cancer, meaning that an enhanced immune activity against melanoma can appear in vitiligo (12).
Epidemiological studies showed inconsistent results. Lindelof et al. found that vitiligo patients have a lower risk of developing melanoma (15). Teulings et al. found a threefold lower probability of developing melanoma in vitiligo patients in a retrospective comparative cohort study (16). In a study that included 10.040 patients with vitiligo, Paradisi et al. showed that they were 4 time less likely to develop melanoma compared with controls, the difference being highly statistically significant (17). Jorgensen et al. conducted a population-based study including 2,339 subjects with vitiligo and 23,293 controls, but their study showed no significant difference in what concerns the risk of cutaneous melanoma (18). Kim et al. showed that in Korean vitiligo population, the risk of melanoma is increased; however, skin cancer incidence in Korean patients was much lower than in their white counterparts (19). The latest and largest European study that included 15,156 vitiligo cases showed that vitiligo is associated with a substantially lower risk of new-onset skin cancer, for both melanoma and non-melanoma skin cancer (20).
Multiple mechanisms were proposed to explain the negative association between vitiligo and melanoma, including the use of sunscreens, the role of anti-melanocyte immune response in vitiligo, the absence of melanocytes in vitiligo lesions, and the overproduction of proinflammatory cytokines that stimulates the production of superoxide dismutase and glutathione peroxidase, thus reducing the risk of melanoma (21, 22).
3 Spontaneous autoimmune-mediated melanocyte destruction in melanoma
The development of depigmented lesions in melanoma patients has been reported for the first time more than 45 years ago, and confirmed by case reports, small patient series and a few studies (15, 23–31). Four patterns of depigmented lesions have been described in melanoma: (a) areas of depigmentation confined to the primary lesion, suggesting spontaneous regression, (b) areas of depigmentation around the primary tumor, (c) areas of depigmentation around benign melanocytic nevi (halo phenomenon), and (d) widespread hypomelanosis occurring at distant sites from the primary tumor (melanoma associated leukoderma - MAL) (24). The four types of depigmentation are not mutually exclusive and can occur simultaneously (24).
MAL occurs spontaneously in a fraction of melanoma patients, before or after the detection of melanoma (32). Quaglino et al. conducted a prospective cohort study on 2,954 patients of all stages with melanoma and found a 2.8% prevalence of melanoma-associated vitiligo, higher than the prevalence of vitiligo in the general population (33). The authors also showed that melanoma patients with MAL have a higher frequency of immune-mediated manifestations than melanoma patients without MAL, although MAL is less likely to be associated with autoimmune conditions than vitiligo (33). Quaglino et al. showed that depigmented lesions can appear before melanoma diagnosis, after surgical excision, after locoregional metastases, or after distant metastases (33).
The differences and similarities between MAL and vitiligo regarding clinical presentation are not very well defined, the literature being contradictory (Table 1). Studies show that the age at onset was significantly higher in patients with MAL than in vitiligo patients (32). A positive family history of vitiligo is reported in some studies, while in others a positive history was absent in all cases (24, 32, 34). Quaglino et al. found a symmetrical, bilateral distribution in the majority of patients, similar to that in vitiligo (33). Hartmann et al. found a symmetrical distribution pattern in 75% of MAL patients and no correlation between the distribution of the hypopigmentation and the location of the primary tumor (34). On the other hand, Koh et al. and Nordlund et al. showed that MAL is mostly characterized by hypopigmented macules with irregularly shaped border and confetti-like appearance, different from well-demarcated white macules in vitiligo (24, 25). Moreover, equal distribution among men and women, distribution on sun-exposed areas and multiple flecked depigmented macules were also described as clinical features that are distinct from vitiligo (35, 36).
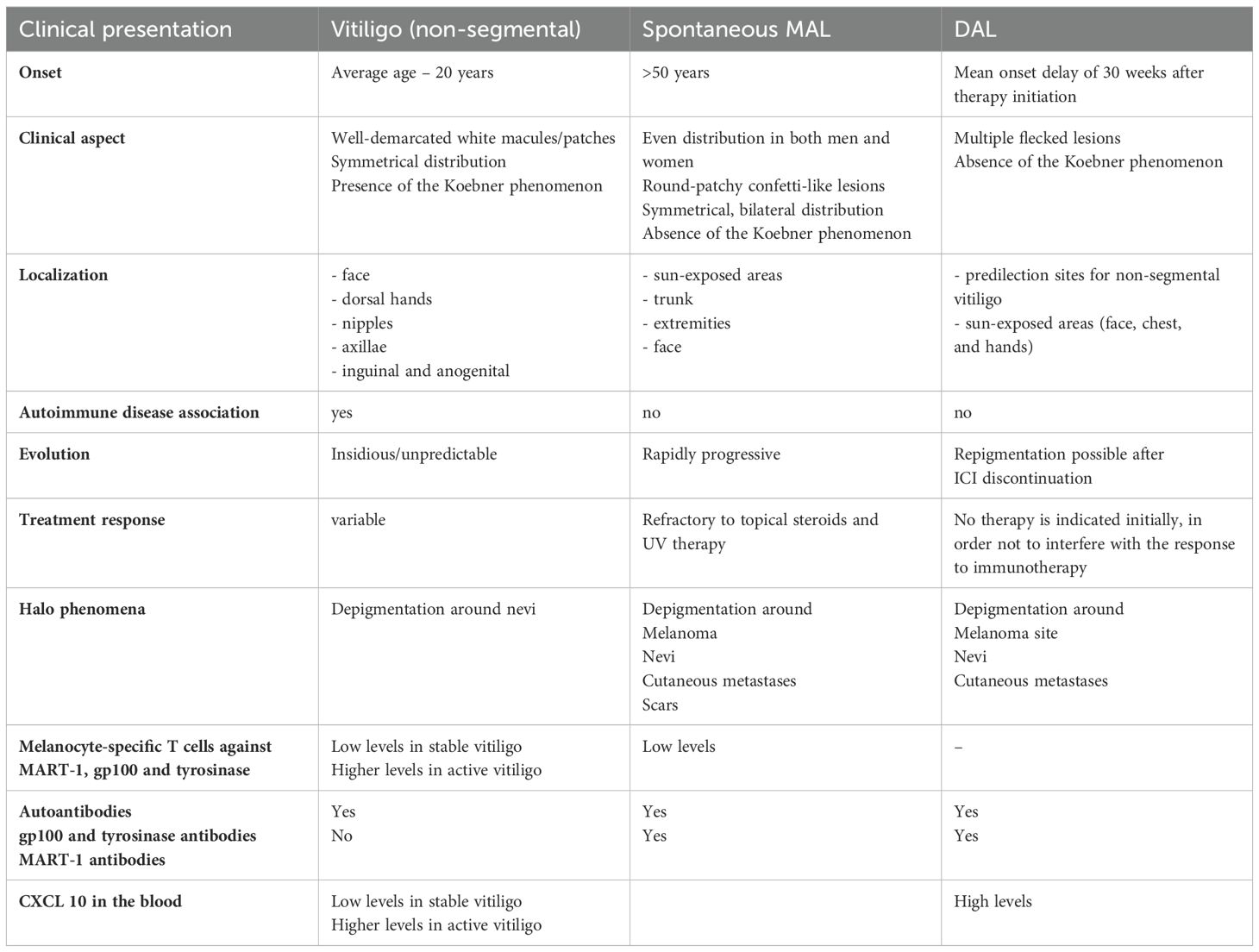
Table 1. Clinical aspect of vitiligo, MAL and DAL.
Lommerts et al. conducted a study to assess whether experts in the field can distinguish between MAL and vitiligo, and to assess if discriminative features can be identified. The authors showed that even experts cannot clearly differentiate between MAL and vitiligo only based on photographs, no significant differences being identified in the clinical presentation. As a consequence, a total body skin examination should be performed in all patients with seemingly typical vitiligo, especially if the age of onset is higher (32).
Teulings et al. retrospectively analyzed the clinical presentation, type of depigmentation and disease course of patients who developed MAL within one year before the detection of a primary melanoma or within 3 years before the detection of melanoma metastases with an unknown primary tumor, and identified seven patients initially diagnosed with non-segmental vitiligo as having MAL (37). They were older Caucasian patients, with sudden onset of rapidly progressive skin depigmentation on non-typical vitiligo predilection sites with median to sharp demarcations and often consisting of round patchy confetti-like lesions, mostly symmetrically scattered over the trunk, extremities and/or face; lesions were generally refractory to topical steroids and UV therapy (37). The authors emphasize that special attention should be given to older Caucasian patients presenting with late onset, rapidly progressing atypical vitiligo-like depigmentation refractory to standard treatment (37).
In some cases, the appearance of depigmented lesions revealed a regressing melanoma (31). Moreover, two cases of melanoma developing within a depigmented patch were recently described, suggesting that clinicians should be cautious in the presence of a new, solitary, vitiligo-like patch in a patient with no risk factors for vitiligo (38).
Hartmann et al. failed to show histological and immunohistological differences between MAL and vitiligo. No differences were described regarding the number of epidermal melanocytes and dendritic cells or the inflammatory infiltrate in terms of characteristics or composition (34).
Multiple studies showed that MAL is associated with a favorable prognosis (6, 33, 37, 39). Quaglino et al. found no statistically significant difference regarding disease free survival (DFS) in stage I-II patients based on the presence of MAL. On the other hand, MAL was associated with a significantly higher overall survival and DFS in stage III-IV melanoma patients, independent of treatment, with no difference in survival according to the time onset of MAL (33).
It is hypothesized that MAL is caused by anti-melanoma immunity targeting normal and malignant melanocytes, due to the presence of melanocyte differentiation antigens on both cells. Teulings at al. studied the immunological differences in patients with MAL and vitiligo. They found specific T cells against MART-1, gp100 and tyrosinase in the blood of both patients with MAL and vitiligo, although low levels were detected in MAL and stable vitiligo, while more melanocyte specific T cells were found in active vitiligo. Autoantibodies against gp100 and tyrosinase were found in both diseases, but MART-1 antibodies were only present in patients with MAL (40).
Palermo et al. found that melanocyte specific T cell response differs qualitatively, not quantitatively in melanoma and vitiligo. They did not find significant differences in the precursor frequencies of Melan-A-specific cytotoxic T lymphocytes, nor in their status of activation. However, they documented a higher receptor affinity of melanocyte T cells from vitiligo. Moreover, only T cells from vitiligo patients were capable of efficient TCR downregulation and IFN-γ production in response to HLA-matched melanoma cells, emphasizing that the receptor affinity difference is physiologically relevant (41).
Vitiligo patients have an increased frequency of halo nevi, while multiple halo nevi might predispose to the onset of vitiligo (42). Halo phenomena have been described in melanoma patients, not only around melanoma and benign nevi, but also around cutaneous metastases and scars in patients with MAL, but its significance is not fully understood (33, 43, 44).
4 Therapy-induced autoimmune-mediated melanocyte destruction in melanoma
4.1 Immunotherapy-induced autoimmune-mediated melanocyte destruction in melanoma
Teulings et al. conducted a systematic review of 137 studies including 5,737 patients with stage III to IV melanoma treated with immunotherapy between 1995 and 2013, and found a pooled incidence of drug-associated leukoderma (DAL) of 3.4% (45). Their review suggested that patients with melanoma that develop DAL have a two-fold decreased risk of disease progression and a four-fold decreased risk of death compared with patients without DAL, suggesting that DAL is a clinical marker for effective anti-melanoma immunity and clinical outcome (45). Various immunotherapies were studied in the review coordinated by Teulings, including general stimulation with interferon-α (IFN- α) or interleukin-2 (IL-2), a modified oncolytic virus, and immune check-point inhibitors, the last being the standard immunotherapy for melanoma nowadays (45).
4.1.1 Immune checkpoint inhibitors
ICI, namely anti-cytotoxic T-lymphocytes antigen-4 (CTLA-4) and programmed cell death (PD)-1 inhibitors, act by upregulating the anti-tumor immune response, enhancing T-cell activation (46).
DAL can occur in up to 2-25% of patients treated with ICI for melanoma, generally occurring at higher rates after anti-PD-1 therapy compared with CTLA-4 inhibition, with a mean onset delay of 30 weeks after therapy initiation (32, 37, 44, 45, 47, 48). The appearance of DAL after ICI is significantly associated with favorable prognosis in multiple studies (45, 48–50). In patients treated with anti-PD-1 agents, DAL is independently associated with a better response rate and better overall survival (49, 51).
Larsabal et al. found that DAL occurring in patients receiving anti-PD-1 therapies is clinically different from vitiligo. Accordingly, no family history of vitiligo, thyroiditis or other autoimmune disorders is reported, and the Koebner phenomenon is absent. Moreover, depigmented lesions can occur on predilection sites for non-segmental vitiligo, but also on sun-exposed areas (face, chest and hands) (Table 1) (52). Lommerts et al. demonstrated, however, the lack of clear discriminative features between DAL and non-segmental vitiligo, both clinically and histologically (32).
Depigmented lesions were also described around primary melanoma sites and around cutaneous metastases, and the concomitant presence of leucotrichia, as well as halo nevi, was also documented (32, 49). Rarely, DAL can be associated with autoimmune bilateral diffuse granulomatous uveitis during or after ICI (53). After the discontinuation of ICI, repigmentation can occur, but it usually resides (46). Matsuya et al. tried to evaluate the correlation between DAL dynamics and clinical efficacy of anti-PD-1 antibodies. They found that DAL expansion and grade 2 DAL (depigmented lesions affecting more than 10% of body surface) showed no improvement in treatment response, but were associated with prolonged progression-free survival and a trend for prolonged overall survival (54).
Hua et al. performed skin biopsies from depigmented lesions developed during pembrolizumab therapy and observed a dermal inflammatory infiltrate composed of T cells and the disappearance of melanocytes (49). Freeman-Keller proposed that PD-1 mediates tolerance to melanosomal proteins, and inhibition of PD-1 activity leads to autoimmune depigmentation (55). Le Gal et al. demonstrated that CD8+ T-cells are the main effector cells that recognize melanocyte differentiation antigens, being present in both tumor and DAL tissue (56). Schumacher et al. showed that neoantigen-specific T-cells are important active ingredients for successful immunotherapy (57), however in patients with low neoantigens, the immunity against melanocyte differentiation antigens is relevant in rescuing suboptimal immune activation (58). Lo et al. found that patients with low melanoma neoantigen burden that responded to ICI had tumors with higher expression of pigmentation-related genes. Moreover, expansion of peripheral blood CD8+ T cells against melanocyte specific antigens was observed only in patients who responded to ICI (59). Altogether, patients that respond to ICI despite low neoantigen load have an expansion of CD8+ T cell response against melanocyte specific antigens, which can also attack normal melanocytes leading to DAL, while responding patients that do not develop DAL may have effective neo-antigen immunity (46, 58).
Carbone et al. analyzed T cell subsets from the peripheral blood of metastatic melanoma patients undergoing anti-PD-1 therapy and skin biopsies collected from those who developed DAL, and sequenced T cell receptor (TCR) cells derived from biopsies of DAL and primary melanoma of the same patient (59). DAL development was associated with blood reduction of CD8+ mucosal-associated invariant T (MAIT), T helper (h) 17, natural killer (NK) CD56bright, and T regulatory (T-reg) cells. A high amount of IL17-A expressing cells in DAL biopsies was also documented, suggesting a possible migration of Th17 cells from the blood in depigmented lesions. Interestingly, in most of the cases, they found different TCR sequences between DAL and primary tumor, but shared TCR sequences between DAL and metastatic tissue of the same patient (59). They concluded that T-cell response against normal melanocytes, which leads to DAL, is mediated by T-cell clones targeting metastatic tissues, rather than reactivation of specific T-cell clones infiltrating primary melanoma. Altogether, anti-PD-1 therapy seems to induce a de novo immune response, triggered by the presence of metastatic tissue (59).
There are conflicting reports regarding the humoral response in ICI-induced DAL. Development of antibodies can occur secondarily to T-cell melanoma cell destruction and antigen release. As mentioned before, Teulings et al. showed that autoantibodies directed against gp100 and tyrosinase were found in both vitiligo and DAL, but MART-1 antibodies were only present in patients with DAL (40). Moreover, Larsabal et al. found higher levels of the chemokine CXCL10 in the blood of melanoma patients developing DAL after ICI compared with vitiligo patients and healthy controls (52). However, higher amounts of CXCL10 were found in active vitiligo, suggesting that reported differences between ICI-induced DAL and active vitiligo could be less significant (60).
Although DAL is considered an adverse effect of ICI therapy, treatment can be continued as DAL is associated with better survival and better response rates. Local or systemic immunosuppression is not recommended, as it may hypothetically decrease the response to ICI therapy. However, local treatment can be considered if DAL persists after extended discontinuation of immunotherapy (46).
The incidence of DAL in melanoma patients using different therapies is summarized in Table 2.
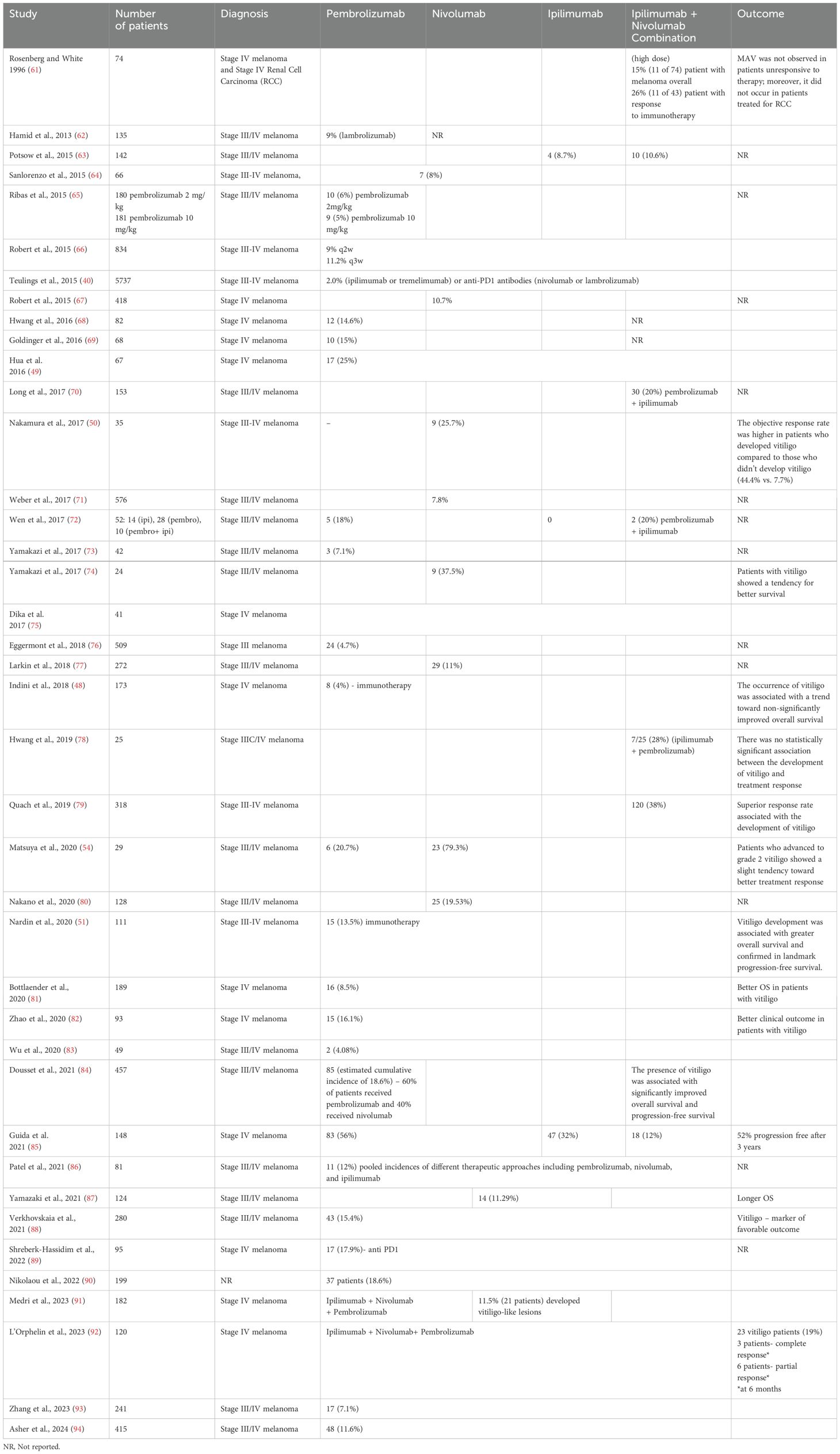
Table 2. Incidence of DAL in melanoma patients treated with different therapies.
Taking into account that not all melanoma patients respond to ICI, there is an increased need to identify some biomarkers that could predict treatment response and further research on the significance of DAL is also required to help determine its predictive value.
4.2 Targeted therapy-induced autoimmune-mediated melanocyte destruction in melanoma
Recently, DAL has also been described in patients treated with targeted therapies, being associated with better prognosis (95, 96). Ramondetta et al. hypothesized that targeted therapy-induced DAL can be explained by the effect on immune system cells related to the blockage of cancer cells by BRAF and MEK (95). Clinically, in contrast to classical vitiligo, which mainly involves the genitalia, wrists and perioral region, drug-induced DAL is localized on sun-exposed areas (face, neck, hands and arms). In the same study, the authors tried to classify drug-induced leukoderma according to the European Guidelines for the management of vitiligo, and found that the most frequent subtype is the non-segmental form (71.4%), particularly the generalized (40%) and acrofacial (40%) forms. In contrast, the distribution of spontaneous MAL was non-segmental, with a prevalence of the focal form (96).
5 Conclusions
Autoimmune-mediated melanocyte destruction in melanoma has many faces, starting with disease predisposition and continuing with diagnosis, prognosis and treatment response. Further studies are needed in order to better characterize the clinical picture, the differences and similarities between MAL and vitiligo, the differences and similarities between MAL and DAL. Moreover, understanding the mechanism of concomitant autoimmune destruction of normal and malignant melanocytes could help select patients with an increased likelihood of therapeutic response, especially after ICI. Treatment options for depigmented lesions in DAL and the risk of decreasing the response to melanoma therapy in these patients also require further studies.
Author contributions
LU: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AV: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. S-RH: Data curation, Resources, Writing – original draft, Writing – review & editing. IT: Data curation, Resources, Writing – original draft, Writing – review & editing. AA: Data curation, Resources, Visualization, Writing – original draft, Writing – review & editing. SS: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. (2024) 74:12–49. doi: 10.3322/caac.21820
3. Maio M. Melanoma as a model tumor for immuno-oncology. Ann Oncol. (2012) 23 Suppl 8:viii10–4. doi: 10.1093/annonc/mds257
4. Mukherji B. Immunology of melanoma. Clin Dermatol. (2013) 31:156–65. doi: 10.1016/j.clindermatol.2012.08.017
5. Uchi H, Stan R, Turk MJ, Engelhorn ME, Rizzuto GA, Goldberg SM, et al. Unraveling the complex relationship between cancer immunity and autoimmunity: lessons from melanoma and vitiligo. Adv Immunol. (2006) 90:215–41. doi: 10.1016/S0065-2776(06)90006-6
6. Motofei IG. Melanoma and autoimmunity: spontaneous regressions as a possible model for new therapeutic approaches. Melanoma Res. (2019) 29:231–6. doi: 10.1097/CMR.0000000000000573
7. Motofei IG. Malignant melanoma: autoimmunity and supracellular messaging as new therapeutic approaches. Curr Treat Options Oncol. (2019) 20:45. doi: 10.1007/s11864-019-0643-4
8. Ohta S, Misawa A, Kyi-Tha-Thu C, Matsumoto N, Hirose Y, Kawakami Y. Melanoma antigens recognized by T cells and their use for immunotherapy. Exp Dermatol. (2023) 32:297–305. doi: 10.1111/exd.14741
9. Wankowicz-Kalinska A, Le Poole C, van den Wijngaard R, Storkus WJ, Das PK. Melanocyte-specific immune response in melanoma and vitiligo: two faces of the same coin? Pigment Cell Res. (2003) 16:254–60. doi: 10.1034/j.1600-0749.2003.00038.x
10. Feng Y, Lu Y. Advances in vitiligo: Update on therapeutic targets. Front Immunol. (2022) 13:986918. doi: 10.3389/fimmu.2022.986918
11. Boehncke WH, Brembilla NC. Autoreactive T-lymphocytes in inflammatory skin diseases. Front Immunol. (2019) 10:1198. doi: 10.3389/fimmu.2019.01198
12. Wu W, 23 and Me Research Team, Amos CI, Lee JE, Wei Q, Sarin KY, et al. Inverse relationship between vitiligo-related genes and skin cancer risk. J Invest Dermatol. (2018) 138:2072e5. doi: 10.1016/j.jid.2018.03.1511
13. Jin Y, Birlea SA, Fain PR, Gowan K, Riccardi SL, Holland PJ, et al. Variant of TYR and autoimmunity susceptibility loci in generalized vitiligo. N Engl J Med. (2010) 362:1686–97. doi: 10.1056/NEJMoa0908547
14. Liu JB, Li M, Chen H, Zhong SQ, Yang S, Du WD, et al. Association of vitiligo with HLA-A2: a meta-analysis. J Eur Acad Dermatol Venereol. (2007) 21:205–13. doi: 10.1111/j.1468-3083.2006.01899.x
15. Lindelof B, Hedblad MA, Sigurgeirsson B. On the association between vitiligo and Malignant melanoma. Acta Derm Venereol. (1998) 78:483–4. 38. doi: 10.1080/000155598442944
16. Teulings HE, Overkamp M, Ceylan E, Nieuweboer-Krobotova L, Bos JD, Nijsten T, et al. Decreased risk of melanoma and nonmelanoma skin cancer in patients with vitiligo: a survey among 1307 patients and their partners. Br J Dermatol. (2013) 168:162–71. doi: 10.1111/bjd.12111
17. Paradisi A, Tabolli S, Didona B, Sobrino L, Russo N, Abeni D. Markedly reduced incidence of melanoma and nonmelanoma skin cancer in a nonconcurrent cohort of 10,040 patients with vitiligo. J Am Acad Dermatol. (2014) 71:1110–6. doi: 10.1016/j.jaad.2014.07.050
18. Jørgensen MG, Toyserkani NM, Egeberg A, Sørensen JA. Risk of skin cancer in patients with vitiligo in Denmark: a nationwide cohort study. JAAD Int. (2020) 1:31e8. doi: 10.1016/j.jdin.2020.03.004
19. Kim HS, Kim HJ, Hong ES, Kim KB, Lee JD, Kang TU, et al. The incidence and survival of melanoma and nonmelanoma skin cancer in patients with vitiligo: a nationwide population-based matched cohort study in Korea. Br J Dermatol. (2020) 182:907–15. doi: 10.1111/bjd.18247
20. Ferguson J, Eleftheriadou V, Nesnas J. Risk of melanoma and nonmelanoma skin cancer in people with vitiligo: United Kingdom population-based cohort study. J Invest Dermatol. (2023) 143:2204–10. doi: 10.1016/j.jid.2023.04.013
21. Hammoud SM, Kruis RW, Sigurdsson V. Prediction of the occurrence of melanoma and non-melanoma skin cancer in patients with vitiligo. Acta Derm Venereol. (2016) 96:106–7. doi: 10.2340/00015555-2179
22. Rodrigues M. Skin cancer risk (Nonmelanoma skin cancers/melanoma) in vitiligo patients. Dermatol Clin. (2017) 35:129–34. doi: 10.1016/j.det.2016.11.003
23. Goldman L, Wilson RG, Glasgow R, Richfield R. Perilesional leucoderma in metastatic melanoma. The use of the Wood’s light for early detection of this rare reaction. Acta Derm Venereol. (1967) 47:369–72.
24. Koh HK, Sober AJ, Nakagawa H, Albert DM, Mihm MC, Fitzpatrick TB. Malignant melanoma and vitiligo-like leukoderma: an electron microscopic study. J Am Acad Dermatol. (1983) 9:696–708. doi: 10.1016/s0190-9622(83)70183-0
25. Nordlund JJ, Kirkwood JM, Forget BM, Milton G, Albert DM, Lerner AB. Vitiligo in patients with metastatic melanoma: a good prognostic sign. J Am Acad Dermatol. (1983) 9:689–96. doi: 10.1016/s0190-9622(83)70182-9
26. Barrie`re H, Litoux P, Le Lay M, Bureau B, Stalder JF, Dreno B. Cutaneous achromia and Malignant melanoma. Ann Dermatol Venereol. (1984) 111:991–6.
27. Bystryn JC, Rigel D, Friedman RJ, Kopf A. Prognostic significance of hypopigmentation in Malignant melanoma. Arch Dermatol. (1987) 123:1053–5. doi: 10.1001/archderm.1987.01660320095019
28. Schallreuter KU, Levenig C, Berger J. Vitiligo and cutaneous melanoma. A Case study Dermatologica. (1991) 183:239–45. doi: 10.1159/000247693
29. Cui J, Bystryn JC. Melanoma and vitiligo are associated with antibody responses to similar antigens on pigment cells. Arch Dermatol. (1995) 131:314–8. doi: 10.1001/archderm.1995.01690150078015
30. Garbelli S, Mantovani S, Palermo B, Giachino C. Melanocyte-specific, cytotoxic T cell responses in vitiligo: the effective variant of melanoma immunity? Pigment Cell Res. (2005) 18:234–42. doi: 10.1111/j.1600-0749.2005.00244
31. Arpaia N, Cassano N, Vena GA. Regressing cutaneous Malignant melanoma and vitiligo-like depigmentation. Int J Dermatol. (2006) 45:952–6. doi: 10.1111/j.1365-4632.2004.02468.x
32. Lommerts JE, Teulings HE, Ezzedine K, van Geel N, Hartmann A, Speeckaert R, et al. Melanoma associated leukoderma and vitiligo cannot be differentiated based on blinded assessment by experts in the field. J Am Acad Dermatol. (2016) 75:1198–204. doi: 10.1016/j.jaad.2016.07.060
33. Quaglino P, Marenco F, Osella-Abate S, Cappello N, Ortoncelli M, Salomone B, et al. Vitiligo is an independent favorable prognostic factor in stage III and IV metastatic melanoma patients: results from a single-institution hospital-based observational cohort study. Ann Oncol. (2010) 21:409–14. doi: 10.1093/annonc/mdp325
34. Hartmann A, Bedek C, Keikavoussi P, Becker JC, Hamm H, Brocker EB. Vitiligo and melanoma-associated hypopigmentation (MAH): Shared and discriminative features. J Dtsch Dermatol Ges. (2008) 6:1053–9. doi: 10.1111/j.1610-0387.2008.06755.x
35. Naveh H, Rao UNM, Butterfield LH. Melanoma-associated leukoderma-immunology in black and white? Pigment. Cell Melanoma Res. (2013) 26:796–804. doi: 10.1111/pcmr.12161
36. Saleem MD, Oussedik E, Schoch JJ, Berger AC, Picardo M. Acquired disorders with depigmentation: A systematic approach to vitiliginoid conditions. J Am Acad Dermatol. (2019) 80:1215–31. doi: 10.1016/j.jaad.2018.03.063
37. Teulings HE, Lommerts JE, Wolkerstorfer A, Nieuweboer-Krobotova L, Luiten RM, Bekkenk MW, et al. Vitiligo-like depigmentations as the first sign of melanoma: a retrospective case series from a tertiary vitiligo center. Br J Dermatol. (2017) 176:503–6. doi: 10.1111/bjd.14790
38. Francisco G, Rao BK, Victor FC. Two reports of Malignant melanoma arising within vitiligo-like depigmented patch. JAAD Case Rep. (2018) 4:573–5. doi: 10.1016/j.jdcr.2018.05.008
39. Rodrìguez-Cuevas S, Lòpez-Chavira A, Zepeda del Rio G, Cuadra-Garcia I, Fernàndez-Diez J. Prognostic significance of cutaneous depigmentation in Mexican patients with Malignant melanoma. Arch Med Res. (1998) 29:155–8.
40. Teulings HE, Willemsen KJ, Glykofridis I, Krebbers G, Komen L, Kroon MW, et al. The antibody response against MART-1 differs in patients with melanoma-associated leucoderma and vitiligo. Pigment Cell Melanoma Res. (2014) 27:1086–96. doi: 10.1111/pcmr.12294
41. Palermo B, Garbelli S, Mantovani S, Scoccia E, Da Prada G, Bernabei P, et al. Qualitative difference between the cytotoxic T Lymphocyte responses to melanocyte antigens in melanoma and vitiligo. Eur J Immunol. (2005) 35:3153–62. doi: 10.1002/eji.200535110
42. Yang Y, Li S, Zhu G, Zhang Q, Wang G, Gao T, et al. A similar local immune and oxidative stress phenotype in vitiligo and halo nevus. J Dermatol Sci. (2017) 87:50–9. doi: 10.1016/j.jdermsci.2017.03.008
43. Vyas R, Selph J, Gerstenblith MR. Cutaneous manifestations associated with melanoma. Semin Oncol. (2016) 43:384–9. doi: 10.1053/j.seminoncol.2016.02.031
44. Failla CM, Carbone ML, Fortes C, Pagnanelli G, D'Atri S. Melanoma and vitiligo: in good company. Int J Mol Sci. (2019) 20:5731. doi: 10.3390/ijms20225731
45. Teulings HE, Limpens J, Jansen SN, Zwinderman AH, Reitsma JB, Spuls PI, et al. Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: a systematic review and meta-analysis. J Clin Oncol. (2015) 33:773–81. doi: 10.1200/JCO.2014.57.4756
46. Lommerts JE, Bekkenk MW, Luiten RM. Vitiligo induced by immune checkpoint inhibitors in melanoma patients: an expert opinion. Expert Opin Drug Saf. (2021) 20:883–8. doi: 10.1080/14740338.2021.1915279
47. Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. (2018) 19:345–61. doi: 10.1007/s40257-017-0336-3
48. Indini A, Di Guardo L, Cimminiello C, Prisciandaro M, Randon G, De Braud F, et al. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic melanoma. J Cancer Res Clin Oncol. (2019) 145:511–21. doi: 10.1007/s00432-018-2819-x
49. Hua C, Boussemart L, Mateus C, Routier E, Boutros C, Cazenave H, et al. Association of vitiligo with tumor response in patients with metastatic melanoma treated with pembrolizumab. JAMA Dermatol. (2016) 152:45–51. doi: 10.1001/jamadermatol.2015.2707
50. Nakamura Y, Tanaka R, Asami Y, Teramoto Y, Imamura T, Sato S, et al. Correlation between vitiligo occurrence and clinical benefit in advanced melanoma patients treated with nivolumab: A multi-institutional retrospective study. J Dermatol. (2017) 44:117–22. doi: 10.1111/jde.2017.44.issue-2
51. Nardin C, Jeand’heur A, Bouiller K, Valnet-Rabier MB, Dresco F, Castagna J, et al. Vitiligo under anti-programmed cell death-1 therapy is associated with increased survival in melanoma patients. J Am Acad Dermatol. (2020) 82:770–2. doi: 10.1111/1346-8138.13520
52. Larsabal M, Marti A, Jacquemin C, Rambert J, Thiolat D, Dousset L, et al. Vitiligo-like lesions occurring in patients receiving anti-programmed cell death-1 therapies are clinically and biologically distinct from vitiligo. J Am Acad Dermatol. (2017) 76:863–70. doi: 10.1016/j.jaad.2016.10.044
53. Fujimura T, Kambayashi Y, Tanita K, Sato Y, Hidaka T, Otsuka A, et al. HLA-DRB1*04:05 in two cases of Vogt-Koyanagi-Harada disease-like uveitis developing from an advanced melanoma patient treated by sequential administration of nivolumab and dabrafenib/trametinib therapy. J Dermatol. (2018) 45:735–7. doi: 10.1111/1346-8138.14273
54. Matsuya T, Nakamura Y, Matsushita S, Tanaka R, Teramoto Y, Asami Y, et al. Vitiligo expansion and extent correlate with durable response in anti-programmed death 1 antibody treatment for advanced melanoma: A multi-institutional retrospective study. J Dermatol. (2020) 47:629–35. doi: 10.1111/1346-8138.15345
55. Freeman-Keller M, Kim Y, Cronin H, Richards A, Gibney G, Weber JS. Nivolumab in resected and unresectable metastatic melanoma: characteristics of immune-related adverse events and association with outcomes. Clin Cancer Res. (2016) 22:886–94. doi: 10.1158/1078-0432.CCR-15-1136
56. Le Gal FA, Avril MF, Bosq J, Lefebvre P, Deschemin JC, Andrieu M, et al. Direct evidence to support the role of antigen-specific CD8(+) T cells in melanoma-associated vitiligo. J Invest Dermatol. (2001) 117:1464–70. doi: 10.1046/j.0022-202x.2001.01605.x
57. Schumacher TN, Schreiber RD. Neoantigens in cancer immunotherapy. Science. (2015) 348:69–74. doi: 10.1126/science.aaa4971
58. Lo JA, Kawakubo M, Juneja VR, Su MY, Erlich TH, LaFleur MW, et al. Epitope spreading toward wild-type melanocyte-lineage antigens rescues suboptimal immune checkpoint blockade responses. Sci Transl Med. (2021) 13:eabd8636. doi: 10.1126/scitranslmed.abd8636
59. Carbone ML, Capone A, Guercio M, Reddel S, Silvestris DA, Lulli D, et al. Insight into immune profile associated with vitiligo onset and anti-tumoral response in melanoma patients receiving anti-PD-1 immunotherapy. Front Immunol. (2023) 14:1197630. doi: 10.3389/fimmu.2023.1197630
60. Wang XX, Wang QQ, Wu JQ, Jiang M, Chen L, Zhang CF, et al. Increased expression of CXCR3 and its ligands in patients with vitiligo and CXCL10 as a potential clinical marker for vitiligo. Br J Dermatol. (2016) 174:1318–26. doi: 10.1111/bjd.14416
61. Rosenberg SA, White DE. Vitiligo in patients with melanoma: normal tissue antigens can be targets for cancer immunotherapy. J Immunother Emphasis Tumor Immunol. (1996) 19:81–4. doi: 10.1097/00002371-199601000-00009
62. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med. (2013) 369:134–44. doi: 10.1056/NEJMoa1305133
63. Postow MA, Chesney J, Pavlick AC, Robert C, Grossmann K, McDermott D, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. (2015) 372:2006–17. doi: 10.1056/NEJMoa1414428
64. Sanlorenzo M, Vujic I, Daud A, Algazi A, Gubens M, Luna SA, et al. Pembrolizumab cutaneous adverse events and their association with disease progression. JAMA Dermatol. (2015) 151:1206–12. doi: 10.1001/jamadermatol.2015.1916
65. Ribas A, Puzanov I, Dummer R, SChadendorf D, Hamid O, Robert C, et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomized, controlled, phase 2 trial. Lancet Oncol. (2015) 16:908–18. doi: 10.1016/S1470-2045(15)00083-2
66. Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, et al. KEYNOTE-006 investigators. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med. (2015) 372:2521–32. doi: 10.1056/NEJMoa1503093
67. Robert C, Long GV, Brady B, Dutriaux C, Maio M, Mortier L, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. (2015) 372:320–30. doi: 10.1056/NEJMoa1412082
68. Hwang SJ, Carlos G, Wakade D, Byth K, Kong BY, Chou S, et al. Cutaneous adverse events (AEs) of anti-programmed cell death (PD)-1 therapy in patients with metastatic melanoma: A single-institution cohort. J Am Acad Dermatol. (2016) 74:455–61. doi: 10.1016/j.jaad.2015.10.029
69. Goldinger SM, Stieger P, Meier B, Micaletto S, Contassot E, French LE, et al. Cytotoxic cutaneous adverse drug reactions during anti-PD-1 therapy. Clin Cancer Res. (2016) 22:4023–9. doi: 10.1158/1078-0432.CCR-15-2872
70. Long GV, Atkinson V, Cebon JS, Jameson MB, Fitzharris BM, McNeil CM, et al. Standard-dose pembrolizumab in combination with reduced-dose ipilimumab for patients with advanced melanoma (KEYNOTE-029): an open-label, phase 1b trial. Lancet Oncol. (2017) 18:1202–10. doi: 10.1016/S1470-2045(17)30428-X
71. Weber JS, Hodi FS, Wolchok JD, Topalian SL, SChadendorf D, Larkin J, et al. Safety profile of nivolumab monotherapy: A pooled analysis of patients with advanced melanoma. J Clin Oncol. (2017) 35:785–92. doi: 10.1200/JCO.2015.66.1389
72. Wen X, Ding Y, Li J, Zhao J, Peng R, Li D, et al. The experience of immune checkpoint inhibitors in Chinese patients with metastatic melanoma: a retrospective case series. Cancer Immunol Immunother. (2017) 66:1153–62. doi: 10.1007/s00262-017-1989-8
73. Yamazaki N, Takenouchi T, Fujimoto M, Ihn H, Uchi H, Inozume T, et al. Phase 1b study of pembrolizumab (MK-3475; anti-PD-1 monoclonal antibody) in Japanese patients with advanced melanoma (KEYNOTE-041). Cancer Chemother Pharmacol. (2017) 79:651–60. doi: 10.1007/s00280-016-3237-x
74. Yamazaki N, Kiyohara Y, Uhara H, Uehara J, Fujimoto M, Takenouchi T, et al. Efficacy and safety of nivolumab in Japanese patients with previously untreated advanced melanoma: A phase II study. Cancer Sci. (2017) 108:1223–30. doi: 10.1111/cas.13241
75. Dika E, Ravaioli GM, Fanti PA, Piraccini BM, Lambertini M, Chessa MA, et al. Cutaneous adverse effects during ipilimumab treatment for metastatic melanoma: a prospective study. Eur J Dermatol. (2017) 27:266–70. doi: 10.1684/ejd.2017.3023
76. Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD, Schmidt H, et al. Prolonged survival in stage III melanoma with ipilimumab adjuvant therapy. N Engl J Med. (2016) 375:1845–55. doi: 10.1056/NEJMoa1611299
77. Larkin J, Minor D, D'Angelo S, Neyns B, Smylie M, Miller WH Jr, et al. Overall survival in patients with advanced melanoma who received nivolumab versus investigator's choice chemotherapy in checkMate 037: A randomized, controlled, open-label phase III trial. J Clin Oncol. (2018) 36:383–90. doi: 10.1200/JCO.2016.71.8023
78. Hwang SJE, Park JJW, Wakade D, Chou S, Byth K, Fernandez-Penas P. Cutaneous adverse events of anti-programmed death 1 antibodies combined with anti-cytotoxic T-lymphocyte-associated protein 4 therapy use in patients with metastatic melanoma. Melanoma Res. (2019) 29:172–7. doi: 10.1097/CMR.0000000000000518
79. Quach HT, Dewan AK, Davis EJ, Ancell KK, Fan R, Ye F, et al. Association of anti-programmed cell death 1 cutaneous toxic effects with outcomes in patients with advanced melanoma. JAMA Oncol. (2019) 5:906–8. doi: 10.1001/jamaoncol.2019.0046
80. Nakano E, Takahashi A, Namikawa K, Muto Y, Jinnai S, Kage Y, et al. Correlation between cutaneous adverse events and prognosis in patients with melanoma treated with nivolumab: A single institutional retrospective study. J Dermatol. (2020) 47:622–8. doi: 10.1111/1346-8138.15309
81. Bottlaender L, Amini-Adle M, Maucort-Boulch D, Robinson P, Thomas L, Dalle S. Cutaneous adverse events: a predictor of tumor response under anti-PD-1 therapy for metastatic melanoma, a cohort analysis of 189 patients. J Eur Acad Dermatol Venereol. (2020) 34:2096–105. doi: 10.1111/jdv.16311
82. Zhao JJ, Wen XZ, Ding Y, Li DD, Zhu BY, Li JJ, et al. Association between immune-related adverse events and efficacy of PD-1 inhibitors in Chinese patients with advanced melanoma. Aging (Albany NY). (2020) 12:10663–75. doi: 10.18632/aging.103285
83. Wu CE, Yang CK, Peng MT, Huang PW, Chang CF, Yeh KY, et al. The association between immune-related adverse events and survival outcomes in Asian patients with advanced melanoma receiving anti-PD-1 antibodies. BMC Cancer. (2020) 20:1018. doi: 10.1186/s12885-020-07508-7
84. Dousset L, Pacaud A, Barnetche T, Kostine M, Dutriaux C, Pham-Ledard A, et al. Analysis of tumor response and clinical factors associated with vitiligo in patients receiving anti-programmed cell death-1 therapies for melanoma: A cross-sectional study. JAAD Int. (2021) 5:112–20. doi: 10.1016/j.jdin.2021.09.002
85. Guida M, Strippoli S, Maule M, Quaglino P, Ramondetta A, Chiaron Sileni V, et al. Immune checkpoint inhibitor associated vitiligo and its impact on survival in patients with metastatic melanoma: an Italian Melanoma Intergroup study. ESMO Open. (2021) 6:100064. doi: 10.1016/j.esmoop.2021.100064
86. Patel AB, Farooq S, Welborn M, Amaria RN, Chon SY, Diab A, et al. Cutaneous adverse events in 155 patients with metastatic melanoma consecutively treated with anti-CTLA4 and anti-PD1 combination immunotherapy: Incidence, management, and clinical benefit. Cancer. (2022) 128:975–83. doi: 10.1002/cncr.34004
87. Yamazaki N, Takenouchi T, Nakamura Y, Takahashi A, Namikawa K, Kitano S, et al. Prospective observational study of the efficacy of nivolumab in Japanese patients with advanced melanoma (CREATIVE study). Jpn J Clin Oncol. (2021) 51:1232–41. doi: 10.1093/jjco/hyab064
88. Verkhovskaia S, Di Pietro FR, Mastroeni S, Carbone ML, Abeni D, Morese R, et al. Vitiligo-like leukoderma as an indicator of clinical response to immune checkpoint inhibitors in late-stage melanoma patients. J Cancer Res Clin Oncol. (2022) 148:2529–38. doi: 10.1007/s00432-021-03811-3
89. Shreberk-Hassidim R, Aizenbud L, Lussheimer S, Thomaidou E, Bdolah-Abram T, Merims S, et al. Dermatological adverse events under programmed cell death-1 inhibitors as a prognostic marker in metastatic melanoma. Dermatol Ther. (2022) 35:e15747. doi: 10.1111/dth.15747
90. Nikolaou VA, Apalla Z, Carrera C, Fattore D, Sollena P, Riganti J, et al. Clinical associations and classification of immune checkpoint inhibitor-induced cutaneous toxicities: a multicenter study from the European Academy of Dermatology and Venereology Task Force of Dermatology for Cancer Patients. Br J Dermatol. (2022) 187:962–9. doi: 10.1111/bjd.21781
91. Medri M, Savoia F, Foca F, Miserocchi A, Quaglino P, Rubatto M, et al. A retrospective observational study on cutaneous adverse events induced by immune checkpoint inhibitors. Ital J Dermatol Venerol. (2023) 158:437–44. doi: 10.23736/S2784-8671.23.07542-4
92. L'Orphelin JM, Cassecuel J, Kandolf L, Harwood CA, Tookey P, Junejo MH, et al. And European Association of Dermato-Oncology. Cutaneous manifestations induced by check point inhibitors in 120 melanoma patients-The European MelSkinTox study. J Eur Acad Dermatol Venereol. (2023) 7:1606–15. doi: 10.1111/jdv.19112
93. Zhang S, Tang K, Wan G, Nguyen N, Lu C, Ugwu-Dike P, et al. Cutaneous immune-related adverse events are associated with longer overall survival in advanced cancer patients on immune checkpoint inhibitors: A multi-institutional cohort study. J Am Acad Dermatol. (2023) 88:1024–32. doi: 10.1016/j.jaad.2022.12.048
94. Asher N, Bar-Hai N, Ben-Betzalel G, Stoff R, Grynberg S, Schachter J, et al. Exploring the clinical significance of specific immune-related adverse events in melanoma patients undergoing immune checkpoint inhibitor therapy. Melanoma Res. (2024) 34:439–49. doi: 10.1097/CMR.0000000000000985
95. Ramondetta A, Ribero S, Conti L, Fava P, Marra E, Broganelli P, et al. Clinical and pathological relevance of drug induced vitiligo in patients treated for metastatic melanoma with anti-PD1 or BRAF/MEK inhibitors. Acta Derm Venereol. (2020) 100:adv00001. doi: 10.2340/00015555-3319
Keywords: melanoma, autoimmunity, melanocytes, vitiligo, melanoma-associated leukoderma, immunotherapy, targeted therapy
Citation: Ungureanu L, Vasilovici AF, Halmágyi S-R, Trufin II, Apostu AP and Şenilă SC (2024) The many faces of autoimmune-mediated melanocyte destruction in melanoma. Front. Immunol. 15:1417273. doi: 10.3389/fimmu.2024.1417273
Received: 14 April 2024; Accepted: 16 September 2024;
Published: 03 October 2024.
Edited by:
Monica Neagu, Victor Babes National Institute of Pathology (INCDVB), RomaniaReviewed by:
Cristina M. Failla, Institute of Immaculate Dermatology (IRCCS), ItalyWeinan Guo, Air Force Medical University, China
Copyright © 2024 Ungureanu, Vasilovici, Halmágyi, Trufin, Apostu and Şenilă. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alina Florentina Vasilovici, YWxpbmFfbGV0Y2FAeWFob28uY29t