 Bénédicte Billi1Paul Cholley2Vincent Grobost1Mélissa Clément3Virginie Rieu1Guillaume Le Guenno1
Bénédicte Billi1Paul Cholley2Vincent Grobost1Mélissa Clément3Virginie Rieu1Guillaume Le Guenno1 Hervé Lobbes1,4*
Hervé Lobbes1,4*- 1Service de Médecine Interne, Hôpital Estaing, Centre Hospitalier Universitaire de Clermont-Ferrand, Clermont-Ferrand, France
- 2Service de Radiologie, Hôpital Estaing, Centre Hospitalier Universitaire de Clermont-Ferrand, Clermont-Ferrand, France
- 3Service de Médecine Interne, Hôpital Henri Mondor, Aurillac, France
- 4Institut Pascal, Unité Mixte de Recherche (UMR) 6602, Centre National de la Recherche Scientifique, Université Clermont Auvergne, Clermont-Ferrand, France
Primary humoral deficiency and secondary B-cell depletion may lead to prolonged Sars-Cov-2 infection due to a decreased viral clearance. Prolonged infection is mainly driven by the lack of anti-Sars-Cov-2 immunoglobulin (IVIg) especially in patients with no vaccine response. Anti-spike immunoglobulin can be provided by infusion of convalescent patients’ plasma: recent studies highlighted that commercial immunoglobulin show high titers of neutralizing IgG. We conducted a single center retrospective cohort. We included 9 patients (6 males, median age 74 years old): one patient with X-linked agammaglobulinemia and 8 patients treated with rituximab (2 granulomatosis with polyangiitis, 1 neuromyelitis optica, 4 low grade B-cell lymphoma and 1 EBV post-transplant lymphoproliferative disorder). Mean serum globulin was 4 ± 1.6 g/L. 7/8 had received at least 3 doses of mRNA anti-Sars-Cov-2 vaccine (median 4) with no response (anti-Spike IgG 0 for 6 patients). In this specific population requiring oxygen therapy but no intensive care support, the administration of IVIg was well tolerated and provided a swift improvement of clinical status, a significant decrease of inflammation associated to the an improvement of radiological patterns. Our results suggest that immunoglobulin could be used as a salvage therapy as an alternative to convalescent plasma but highly stringent patient selection is required due to the worldwide shortage of IVIg.
1 Introduction
In patients with humoral deficiency, Covid-19 infection may be prolonged by a lack of viral clearance (1). It has been showed that the persistence of Sars-Cov-2 infection facilitates rapid viral evolution in immunocompromised patients (2). The usual care is based on the use of antiviral therapies or convalescent patients’ plasma carrying anti-Sars-Cov-2 antibodies (3). In a recent meta-analysis the use of convalescent plasma was associated with a significant decrease of mortality (4). The use of remdesivir as monotherapy or in combination with convalescent plasma (5) has been suggested for B cell-depleted patients, mostly in hematological malignancies. However, studies suggest that the use of remdesivir may lead to the emergence of multiresistant viral clones (6, 7).
Convalescent plasma is collected from patients who have recovered from Sars-Cov-2 infection (8). Convalescent plasma is polyclonal: the selection of plasma donor’s to provide a high load of neutralizing antibodies can be made on the titers of IgG and IgA (9) and some studies showed that plasma from vaccinated individuals provide a highly effective in vitro antiviral effect (10). Standard preparations of commercial IVIg contain > 98% of IgG: IgA and IgM are virtually absent whereas normal plasma contains about 72% of IgG, 17% of IgA and 10% of IgM (11). IVIg pre-pandemic commercial batches of IVIg was showed to contain cross-reactive Sars-Cov-2 receptor binding domain antibodies (12): as such, early clinical study suggested a potential benefit of IVIg for patients with severe COVID-19 (13). The spread of the disease lead to a progressive significant increase of Sars-Cov-2 antibodies in commercial IVIg batches (14–17) which may represent an alternative strategy to plasma (18) in immunocompromised patients.
2 Methods
We conducted a retrospective monocentric study in the Internal Medicine department of Clermont-Ferrand Estaing University Hospital from 01/01/2021 to 15/12/2023. The study was conducted in accordance with the Helsinki declaration and approved by local the Ethics Committee (International Review Board 00013412, “CHU de Clermont Ferrand IRB #1”, IRB number 2023-CF240) with compliance to the French policy of individual data protection. Inclusion criteria were adult immunocompromised patients characterized by: (i) primary or secondary B-cell depletion associated with reduction in serum immunoglobulin G (< 5 g/L), (ii) poor vaccine response or refusal of vaccination. Sars-Cov-2 infection was detected by PCR on nasopharyngeal swabs or by bronchoalveolar lavage.
3 Results
3.1 Baseline characteristics
Table 1 summarizes the characteristics of the population. We included 9 patients (6 males), median age 74 years old (min 20, max 86). 8/9 had secondary immunodeficiency associated with rituximab therapy: 3 patients were treated for autoimmune diseases (2 for granulomatosis with polyangiitis, 1 for neuromyelitis optica), 4 for low grade B-cell lymphoma, and 1 patient received various immunosuppressive drugs for pulmonary transplantation and rituximab for EBV associated Post-transplant lymphoproliferative disorder. The last patient (#9) was treated with low dose intravenous immunoglobulin for X-linked agammaglobulinemia (CD19 0/mm3).
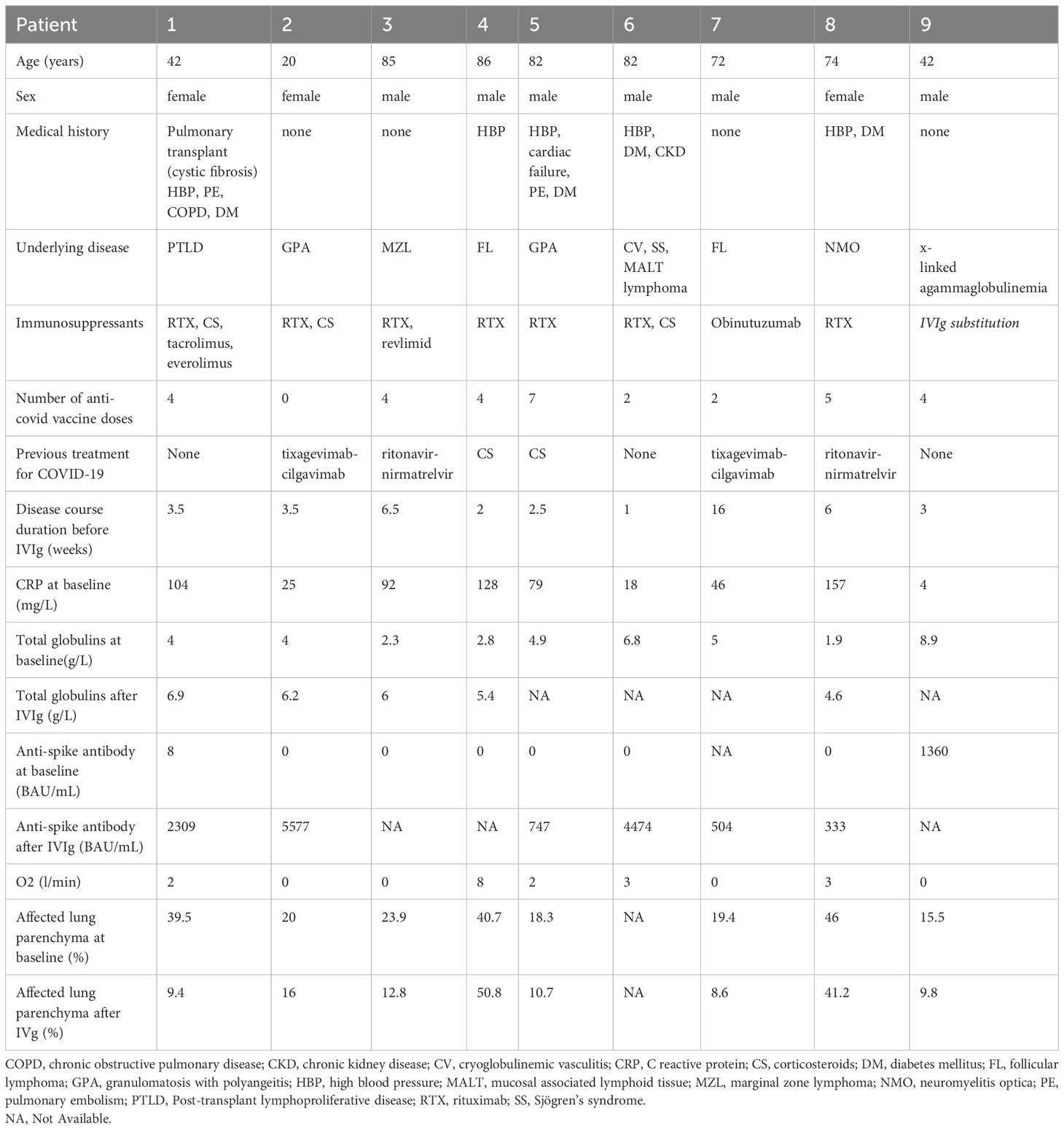
Table 1 Characteristics of adult immunocompromised patients with B-cell depletion and Sars-Cov2 infection treated by intravenous immunoglobulins.
Among the 8 patients with secondary immunodeficiency, mean baseline serum globulin was 4 ± 1.6 g/L. 7/8 had received at least 3 doses of mRNA anti-Sars-Cov-2 vaccine (median 4) with no response (anti-Spike IgG 0 for 6 patients). All strains were Omicron: the sub-variants were identified for 7/9 patients: 4 patients had BA.5 (22B) Omicron and 3 patients had XBB (22F) Omicron. For 2 patients, the sub-variants was not identifiable because of a too low viral load on the sample.
3.2 Treatment and clinical outcome.
All the patients were febrile, 55% required oxygen therapy. No patients required high flow oxygen or transfer to an intensive care unit. 66% received a treatment for COVID-19 prior to IVIg including nirmatrelvir-ritonavir (2/9, 22%), corticosteroids (2/9, 22%), and tixagevimab-cilgavimab (2/9, 22%). The IVIg infusion (CSL Behring Company, Privigen®) was administered 3.5 weeks (median) after positive Sars-Cov-2 PCR without any corticosteroids or antiviral treatment. 8 patients (including the patients treated for x-linked agammaglobulinemia) received a single dose of 1g/kg, one patient received a lower dosage (0.4 g/kg) because of chronic kidney disease.
Oxygen therapy was discontinued 4.5 days after IVIg infusion for each patient. The CRP significantly decreased 48 hours (34 ± 38 vs 72 mg ± 52 mg/L) and 7 to 10 days after IVIg injection (10 ± 12 mg/L, p < 0.001). Anti-spike IgG serology became positive for 6/8 patients (mean titer 2324 BAU, minimum 333 - maximum 5577). The delay between infection and IVIg initiation as well as previous treatment before IVIg for Sars-Cov-2 infection had no influence on the response to IVIg.
3.3 Radiological findings and pulmonary function test
A systematic centralized evaluation of the CT scan before and after IVIg was performed, using automated lung segmentation and quantitative measurements (Thoracic VCAR®, GE Health Care Corporation). A significant improvement of the CT scan was found 1 to 2 months after infusion: the percentage of affected parenchyma decreased from 28 ± 12% to 20 ± 16% (p = 0.03) and the number of lobes decreased from 4.5 ± 0.2 to 3.4 ± 1 (p = 0.01). Figure 1 shows representative changes of lung involvement before and after IVIg. Pulmonary function tests were available for 4 patients 3 months after IVIg: the forced vital capacity increased significantly for 2 patients (mean increase 425 mL (15%), p=0.02), while one patient remained stable (initially normal values) and one patient experienced alteration of her tests due to chronic graft rejection.
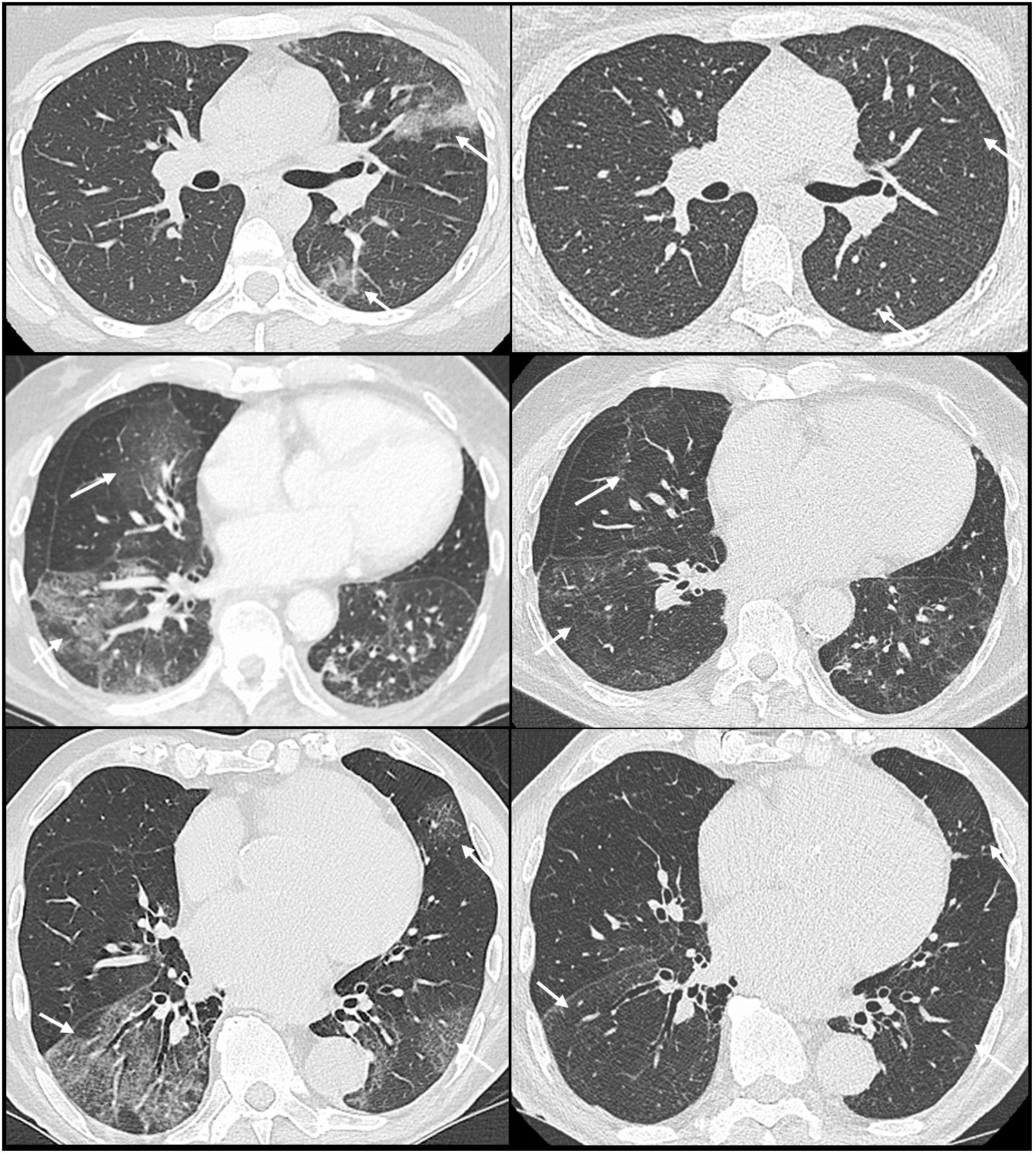
Figure 1 CT scan before (left) and after (right) intravenous immunoglobulin in immunocompromised patients with COVID-19 showing clear reduction in ground-glass opacities (arrows).
3.4 Clinical long-term outcomes
One patient discontinued rituximab treatment because of the stability of his follicular lymphoma. For the 7 remaining patients, the immunosuppressive therapy was not modified. One patient (#5) died 3 months after IVIg of a bacterial infection in a depressive geriatric background. Immediate IVIg tolerance was good for all the patients: no patients experienced adverse events.
At the last follow-up visit (median 5 months, minimum 3 - maximum 39 months), 3 patients were still receiving immunoglobulin substitution: patient #2 received subcutaneous immunoglobulin, whereas patient #7 and patient #9 received monthly IVIg.
Two patients (#2 and #3) experienced during the follow-up period a benign new Sars-Cov-2 infection (fever with no oxygen requirement), treated by ritonavir-nirmatrelvir. The other patients experienced no further sars-Cov-2 infection.
3.5 Comparison to patients treated by convalescent plasma therapy
During the same period, 6 immunocompromised patients (5 men, 1 woman; median age 63 years old) with no vaccine response (undetectable anti-spike antibodies despite 2 to 4 doses of vaccine) were treated by convalescent plasma therapy for COVID-19. Three patients received rituximab and various immunosuppressive drugs for autoimmune diseases (IgG4 related disease, warm autoimmune hemolytic anemia and polyangiitis microscopic) and 3 patients received rituximab (n=2) or obinutuzumab for low grade lymphoma (mantle cell lymphoma, follicular lymphoma and chronic lymphocytic leukemia). Only one patient required oxygen therapy before convalescent plasma infusion.
The Table 2 shows the main features of the two groups. No difference were statistically significative in term of age, sex, BMI or comorbidity (high blood pressure or diabetes mellitus). Two patients treated with convalescent plasma experienced transient worsening after the infusion (fever, increase of CRP), and one patient required additional treatment with corticosteroids. All patients finally recovered and experienced a favorable long term outcome. The statistical analysis is hampered by the low size sample of both groups: we found a greater decrease of CRP 48 hours after IVIg than in plasma group but the difference did not reach statistical significance.
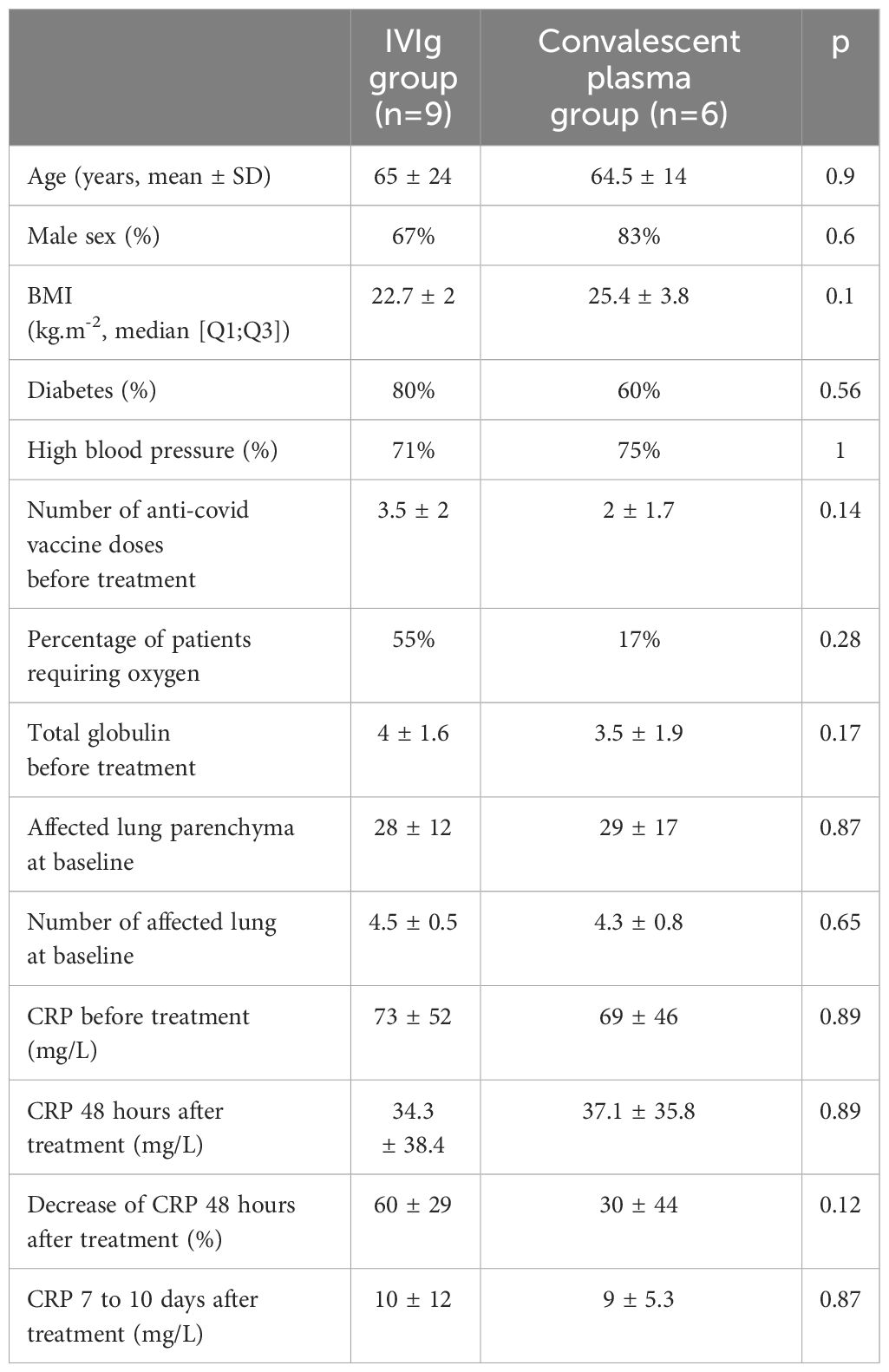
Table 2 Comparison of patients treated with IVIg or convalescent plasma for prolonged COVID-19.
4 Discussion
Early administration of IVIg in immunocompromised patients with B-cell depletion for the treatment of Sars-Cov-2 infection led to swift clinical, radiological and biological improvement. In our cohort, 6/9 patients had experienced the failure of a previous therapy for COVID-19 infection. A single dose of IVIg was used, without concomitant antiviral or cortisoteroid, with a good tolerance profile. Despite the lack of specific anti-Sars-Cov-2 antibodies, Xie et al. reported in 2020 a potential benefit of IVIg in severe COVID-19 (19), that may be due to the presence of cross-reactive Sars-Cov-2 receptor binding domain antibodies (12). In a retrospective case-control study in intensive care units, an increase of mortality was found in patients receiving IVIg (20) and in a multicenter retrospective study, no clear benefit of IVIg on hospitalization duration, mechanical ventilation or mortality rate was reported (21). A meta-analysis found similar results arguing against the use of IVIg (22): however, most studies of IVIg in COVID-19 have included critically-ill patients in intensive care units, most of them requiring mechanical ventilation.
Our population was very specific, as we included patients with B-cell immunodeficiency with severe impairment of globulin levels and no protective levels of IgG-anti-spike antibodies. Our results cannot be extended to severe patients admitted in intensive care units. The good tolerance profile and swift efficacy obtained suggest that IVIg could be used as a salvage therapy if convalescent plasma is not available. The transmission of IgG anti-Sars-COV2 has been clearly showed in X-linked agammaglobulinemic patients receiving IVIg (23), supporting the potential efficacy of IVIg administration as pre-exposure prophylaxis in immunocompromised patients especially as commercial batches contain increasing titers of neutralizing anti-Sars-Cov-2 IgG (24) but further studies are required to support the interest of this strategy. Nevertheless, the current shortage of IVIg dictates an extremely rigorous selection of patients eligible for this treatment.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was approved by local Ethics Committee (IRB00013412, “CHU de Clermont Ferrand IRB #1”, IRB number 2023-CF240) with compliance to the French policy of individual data protection.
Author contributions
BB: Formal analysis, Investigation, Writing – original draft. PC: Formal analysis, Investigation, Writing – original draft. VG: Conceptualization, Formal analysis, Writing – review & editing. MC: Conceptualization, Formal analysis, Writing – review & editing. VR: Conceptualization, Formal analysis, Writing – review & editing. GL: Conceptualization, Formal analysis, Methodology, Writing – review & editing. HL: Conceptualization, Investigation, Project administration, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chan M, Linn MMN, O’Hagan T, Guerra-Assunção JA, Lackenby A, Workman S, et al. Persistent SARS-coV-2 PCR positivity despite anti-viral treatment in immunodeficient patients. J Clin Immunol. (2023) 43:1083–92. doi: 10.1007/s10875-023-01504-9
2. Hettle D, Hutchings S, Muir P, Moran E. Persistent SARS-CoV-2 infection in immunocompromised patients facilitates rapid viral evolution: Retrospective cohort study and literature review. Clin Infect Pract. (2022) 16:100210. doi: 10.1016/j.clinpr.2022.100210
3. Franchini M, Casadevall A, Senefeld JW, Joyner MJ, Sullivan DJ, Focosi D. Recommendations on the use of COVID-19 convalescent plasma to treat immunocompromised patients. Semin Thromb Hemost. (2023). doi: 10.1055/s-0043-1776876
4. Senefeld JW, Franchini M, Mengoli C, Cruciani M, Zani M, Gorman EK, et al. COVID-19 convalescent plasma for the treatment of immunocompromised patients: A systematic review and meta-analysis. JAMA Network Open. (2023) 6:e2250647. doi: 10.1001/jamanetworkopen.2022.50647
5. Weinbergerova B, Mayer J, Kabut T, Hrabovsky S, Prochazkova J, Kral Z, et al. Successful early treatment combining remdesivir with high-titer convalescent plasma among COVID-19-infected hematological patients. Hematological Oncol. (2021) 39:715–20. doi: 10.1002/hon.2908
6. Martinot M, Jary A, Fafi-Kremer S, Leducq V, Delagreverie H, Garnier M, et al. Emerging RNA-dependent RNA polymerase mutation in a remdesivir-treated B-cell immunodeficient patient with protracted coronavirus disease 2019. Clin Infect Dis. (2021) 73:e1762–5. doi: 10.1093/cid/ciaa1474
7. Heyer A, Günther T, Robitaille A, Lütgehetmann M, Addo MM, Jarczak D, et al. Remdesivir-induced emergence of SARS-CoV2 variants in patients with prolonged infection. Cell Rep Med. (2022) 3(9):100735. doi: 10.1016/j.xcrm.2022.100735
8. Bloch EM, Shoham S, Casadevall A, Sachais BS, Shaz B, Winters JL, et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J Clin Invest. (2020) 130:2757–65. doi: 10.1172/JCI138745
9. Acosta-Ampudia Y, Monsalve DM, Rojas M, Rodríguez Y, Gallo JE, Salazar-Uribe JC, et al. COVID-19 convalescent plasma composition and immunological effects in severe patients. J Autoimmun. (2021) 118:102598. doi: 10.1016/j.jaut.2021.102598
10. Sullivan DJ, Franchini M, Joyner MJ, Casadevall A, Focosi D. Analysis of anti-SARS-CoV-2 Omicron-neutralizing antibody titers in different vaccinated and unvaccinated convalescent plasma sources. Nat Commun. (2022) 13:6478. doi: 10.1038/s41467-022-33864-y
11. Gonzalez-Quintela A, Alende R, Gude F, Campos J, Rey J, Meijide LM, et al. Serum levels of immunoglobulins (IgG, IgA, IgM) in a general adult population and their relationship with alcohol consumption, smoking and common metabolic abnormalities. Clin Exp Immunol. (2008) 151:42–50. doi: 10.1111/j.1365-2249.2007.03545.x
12. Ahn TS, Han B, Krogstad P, Bun C, Kohn LA, Garcia-Lloret MI, et al. Commercial immunoglobulin products contain cross-reactive but not neutralizing antibodies against SARS-CoV-2. J Allergy Clin Immunol. (2021) 147:876–7. doi: 10.1016/j.jaci.2020.12.003
13. Wang G, He Z, Wu F, Ge Z, Zhu J, Chen Z. IgG response to spike protein of SARS-CoV-2 in healthy individuals and potential of intravenous IgG as treatment for COVID-19. Virol J. (2022) 19:186. doi: 10.1186/s12985-022-01921-z
14. Jordan SC, Berg A, Shin B, Vo A, Ammerman N, Zhang R. Intravenous immunoglobulin contains high-titer neutralizing IgG antibodies to SARS-CoV-2. Am J Transplant. (2022) 22:2484–5. doi: 10.1111/ajt.17086
15. Park HJ, Alcover KC, Wang Q, Gada SM. SARS-coV-2 antibody longitudinal profile of immune globulin preparations. Mil Med. (2022) 29:usac192. doi: 10.1093/milmed/usac192
16. Volk A, Covini-Souris C, Kuehnel D, De Mey C, Römisch J, Schmidt T. SARS-coV-2 neutralization in convalescent plasma and commercial lots of plasma-derived immunoglobulin. BioDrugs. (2022) 36:41–53. doi: 10.1007/s40259-021-00511-9
17. Bloch EM, Focosi D, Shoham S, Senefeld J, Tobian AAR, Baden LR, et al. Guidance on the use of convalescent plasma to treat immunocompromised patients with coronavirus disease 2019. Clin Infect Dis. (2023) 76:2018–24. doi: 10.1093/cid/ciad066
18. Romero C, Díez J-M, Gajardo R. Anti-SARS-CoV-2 antibodies in healthy donor plasma pools and IVIG products—an update. Lancet Infect Dis. (2022) 22:19. doi: 10.1016/S1473-3099(21)00755-6
19. Xie Y, Cao S, Dong H, Li Q, Chen E, Zhang W, et al. Effect of regular intravenous immunoglobulin therapy on prognosis of severe pneumonia in patients with COVID-19. J Infect. (2020) 81:318–56. doi: 10.1016/j.jinf.2020.03.044
20. Ali HS, Elshafei MS, Saad MO, Mitwally HA, Al Wraidat M, Aroos A, et al. Clinical outcomes of intravenous immunoglobulin therapy in COVID-19 related acute respiratory distress syndrome: a retrospective cohort study. BMC Pulmonary Med. (2021) 21:354. doi: 10.1186/s12890-021-01717-x
21. Salehi M, Barkhori Mehni M, Akbarian M, Fattah Ghazi S, Khajavi Rad N, Moradi Moghaddam O, et al. The outcome of using intravenous immunoglobulin (IVIG) in critically ill COVID-19 patients’: a retrospective, multi-centric cohort study. Eur J Med Res. (2022) 27:18. doi: 10.1186/s40001-022-00637-8
22. Kwapisz D, Bogusławska J. Intravenous immunoglobulins (IVIG) in severe/critical COVID-19 adult patients. BioMed Pharmacother. (2023) 163:114851. doi: 10.1016/j.biopha.2023.114851
23. Raphael A, Shamriz O, Tvito A, Magen S, Goldberg S, Megged O, et al. SARS-CoV-2 spike antibody concentration in gamma globulin products from high-prevalence COVID-19 countries are transmitted to X-linked agammaglobulinemia patients. Front Immunol. (2023) 14:1156823. doi: 10.3389/fimmu.2023.1156823
Keywords: SARS-CoV-2, immunodeficiency, B-cell depletion, rituximab, intravenous immunoglobulin
Citation: Billi B, Cholley P, Grobost V, Clément M, Rieu V, Le Guenno G and Lobbes H (2024) Intravenous immunoglobulins for the treatment of prolonged COVID-19 in immunocompromised patients: a brief report. Front. Immunol. 15:1399180. doi: 10.3389/fimmu.2024.1399180
Received: 11 March 2024; Accepted: 08 April 2024;
Published: 19 April 2024.
Edited by:
Valentina Mazzotta, National Institute for Infectious Diseases Lazzaro Spallanzani (IRCCS), ItalyReviewed by:
Ann Auma, Case Western Reserve University, United StatesSuresh D. Sharma, United States Department of Health and Human Services, United States
Copyright © 2024 Billi, Cholley, Grobost, Clément, Rieu, Le Guenno and Lobbes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hervé Lobbes, aGxvYmJlc0BjaHUtY2xlcm1vbnRmZXJyYW5kLmZy