
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol., 24 July 2024
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1397103
This article is part of the Research TopicCase Reports in Autoimmune and Autoinflammatory DisordersView all 42 articles
 Ana Teodósio Chícharo1,2*†
Ana Teodósio Chícharo1,2*† Mónica Rebelo3†Ana Rita Lopes1,4Maria João Saavedra1,4Maria Filipa Paramés5Ana Rita Araújo3
Mónica Rebelo3†Ana Rita Lopes1,4Maria João Saavedra1,4Maria Filipa Paramés5Ana Rita Araújo3 Ana Rita Cruz-Machado1,4Luísa Pinto6‡
Ana Rita Cruz-Machado1,4Luísa Pinto6‡ Susana Capela1,4‡
Susana Capela1,4‡Fetal autoimmune atrioventricular block (AVB) is a rare but potentially life-threatening condition. It results from the passage of maternal anti-SSA/Ro or Anti SSB/La auto-antibodies into the fetal circulation, leading to inflammation and fibrosis of the AV node and often to irreversible damage. Besides AVB, these antibodies can also cause cardiomyopathies, but there is no evidence linking them to tachyarrhythmias. We present the case of a patient with significant risk factors for fetal AVB: a prior history of hydrops fetalis, high anti-SSA/Ro antibody levels and hypothyroidism. In this case, the use of dexamethasone and intravenous immunoglobulin may have contributed to reversing the first-degree atrioventricular block detected at 19 weeks of gestation. Additionally, at 21 weeks, the fetus developed a tachyarrhythmia that needed treatment with flecainide. Soon after the birth, the newborn underwent ECG Holter and Wolff-Parkinson-White Syndrome (WPWS) was diagnosed. To our knowledge, the coexistence of fetal AVB and WPWS has never been described.
Fetal autoimmune AVB is amongst the manifestations collectively referred to as neonatal lupus. Fetal AVB results from the passage of maternal anti-SSA/Ro and/or anti-SSB/La auto-antibodies into the fetal circulation, leading to inflammation and fibrosis of the atrioventricular node, often causing irreversible damage. Fetal AVB occurs in 2–5% of pregnancies in women with anti-SSA/Ro and/or anti-La/SSB antibodies, but the rate in subsequent gestations may be as high as 17% (1). Thyroid pathology also increases the risk of fetal AVB in mothers with anti-SSA/Ro antibodies. On the other hand, WPWS is a congenital heart condition that occurs in 0.1% of neonates (2). It is characterized by an abnormal electrical pathway between the atria and ventricles that leads to tachycardia. To the best of our knowledge, there is only one other case in the literature describing WPWS in a newborn with neonatal lupus (3). Herein, we present a unique case of coexistence of immune AVB and WPWS in the offspring of a woman with anti-SSA/Ro antibodies, underlining the diagnostic and therapeutic challenges faced throughout pregnancy.
We present the case of a 29-year-old Caucasian female with hypothyroidism, medicated and controlled with levothyroxine 37.5 µg/day. She had a normal body mass index (20.4 kg/m2) and denied toxic habits. Her family history was irrelevant. She denied previous surgeries and other physical or mental issues. She got pregnant for the first time in the beginning of 2022. This pregnancy, desired and planned, was uneventful until 21 weeks of gestation (WG), when the routine obstetric ultrasound identified a severe hydrops fetalis. The fetal echocardiogram revealed a third-degree AVB (atrial heart rate 140 bpm, ventricular heart rate 47 bpm). Initial laboratory results showed positive antinuclear antibodies (titer 1:1280) with strongly positive anti-SSA/SSB antibodies. At this point, the couple was informed of the poor prognosis of the situation and medical termination of pregnancy was performed at 23 WG.
At this time, the patient’s concerns were tied to her desire to become a mother and the fear of the recurrence of this situation. She was subsequently referred to preconceptional counseling at our rheumatology/obstetrics multidisciplinary clinic in a tertiary hospital, that took place in July of 2022.
A comprehensive medical history revealed that the patient had been experiencing chilblains, fatigue and sporadic mechanical arthralgia over the past two years. She denied symptoms such as sicca syndrome, oral ulcers, alopecia, skin lesions, Raynaud phenomenon, fever, weight loss or any other symptoms of connective tissue disease. Physical examination yielded unremarkable findings. A more detailed laboratory work-up revealed high anti-SSA/Ro titers. Anti-dsDNA and antiphospholipid antibodies were negative. Inflammatory parameters (erythrocyte sedimentation rate and C-reactive protein), complement levels (C3 and C4 levels) and thyroid function were normal. No significant changes were detected through capillaroscopy, salivary gland ultrasound or biopsy. Echocardiogram and thoracic CT also showed no remarkable findings.
Given her intention to conceive again, preconception counseling was provided, which involved a discussion about the increased risk of AVB in the subsequent gestation (up to 17% according to international series) (1). She was advised to seek care at a high-risk pregnancy clinic, with multidisciplinary appointments and a recommendation to undergo weekly fetal echocardiograms starting at 16 WG. Additionally, she was prescribed hydroxychloroquine at a dose of 400mg/day.
Six months later, the patient became pregnant again and received care at our obstetric-rheumatology unit. She reported no symptoms. The routine first trimester ultrasound showed no abnormalities. The risk of preeclampsia, assessed by a score that includes clinical data, blood pressure, Doppler of the uterine arteries and laboratory results [pregnancy-associated plasma protein-A (PAPP-A) and placental growth factor (PlGF)], revealed a low risk. Anti-SSA/Ro titers remained high [anti-Ro52 4236 UQ CU (chemiluminescent units); anti-Ro60 >27496 UQ CU], while anti-SSB/La was slightly above the normal range (7.4 UQ; cut-off 5 UQ). As programmed, weekly fetal echocardiograms were initiated at 16 WG.
At 19 WG, the patient reported extreme fatigue, without dyspnea, thoracic pain or other symptoms. Two consecutive fetal echocardiograms revealed a prolonged mechanical PR interval (150-157 msec), suggestive of a first-degree AVB (Figure 1), with no structural or functional heart disease. Given her high-risk profile (previous hydrops fetalis, hypothyroidism and high levels of anti-SSA/Ro antibodies), it was decided to initiate dexamethasone 8 mg/day (together with calcium and vitamin D3 supplementation) and intravenous immunoglobulin (IVIG) at a dose of 1 g/Kg (4). The Nephrology team was consulted at this point to consider plasmapheresis if the heart block progressed to second degree. Fortunately, four days later, the first-degree fetal AVB had reversed (PR interval 116-130 msec) and anti-SSA antibody titers had decreased [anti-Ro52 1232 FLU (fluorescence units); anti-Ro60 15647 FLU]. For the first time, complement consumption was noted (C4 4 mg/dl), probably related to the IVIG therapy, as the patient dramatically improved her fatigue (5). The IVIG perfusions were maintained twice a week and dexamethasone was gradually tapered down to 4 mg/day.
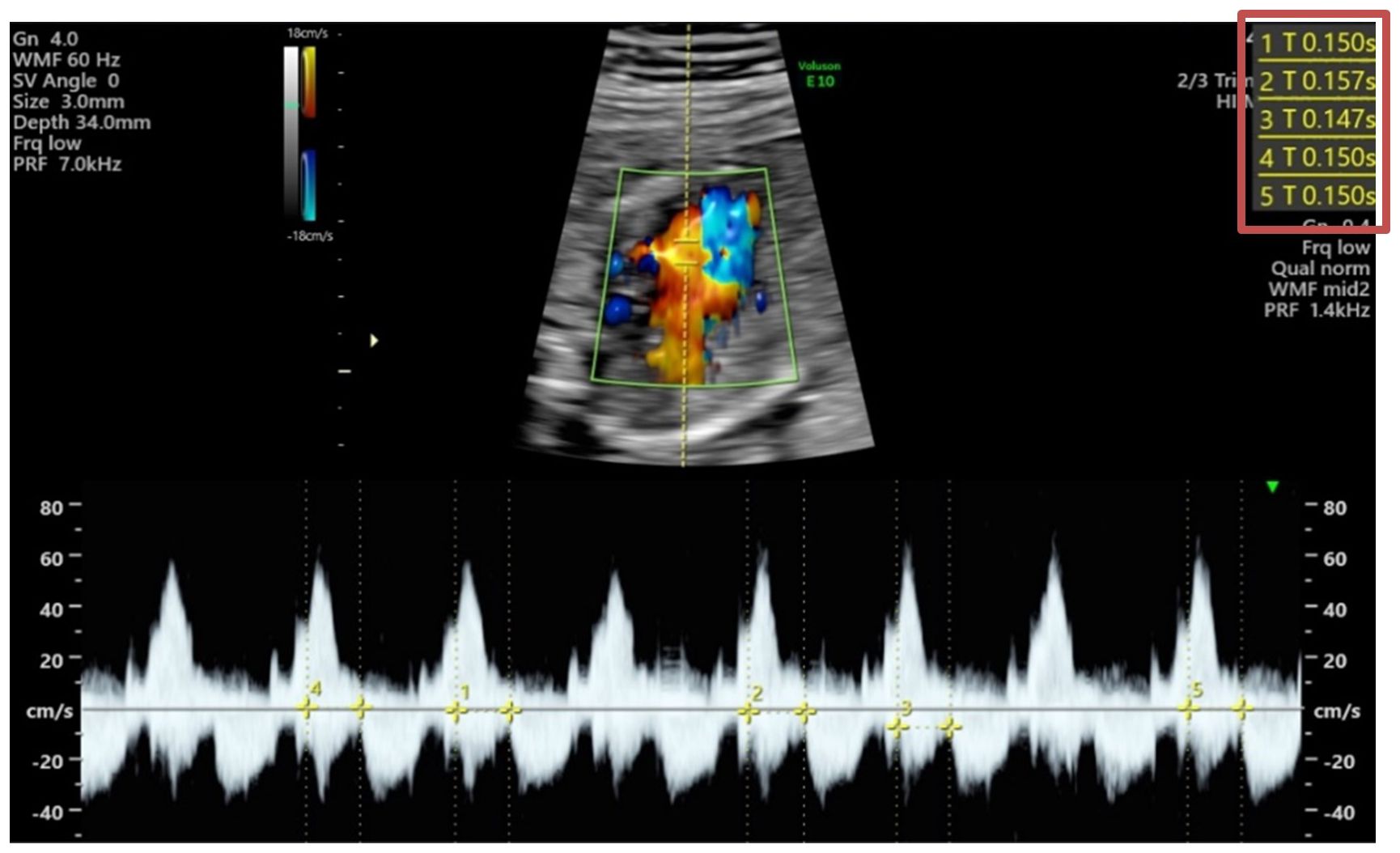
Figure 1 Fetal echocardiogram (2D image with color Doppler and flow Doppler) at 19 weeks of gestation, showing a prolongation of mechanical PR interval. On the top right corner of the image are presented the different measurements: 150, 157, 147, 150, 150 milliseconds.
At 21 WG, a fetal echocardiogram revealed short periods of paroxysmal supraventricular tachycardia (fetal heart rate 260 bpm; normal PR interval 124-129 msec) (Figure 2). The patient was initially advised with general measures, such as ensuring adequate hydration, and avoiding stimulants and anxiety-inducing situations. However, at 22 WG, a subsequent fetal echocardiogram showed that the fetus was in supraventricular tachycardia, with only small periods in sinus rhythm, and a small pericardial effusion was noted. Flecainide at a dose of 100 mg every 8 hours was introduced at this point. Despite being the safest antiarrhythmic choice regarding the risk of bradycardia, the patient and the fetus remained under close monitoring. After 3 weeks (6 perfusions) of IVIG, this therapy was discontinued, as tachyarrhythmias in children potentially triggered by this drug were reported in the literature (6, 7). Complement levels of C4 remained low throughout the IVIG therapy (from 19-21 WG) and returned to normal range in the beginning of third trimester. Dexamethasone was stopped at 28 WG, considering serial normal fetal echocardiograms. Flecainide was continued throughout pregnancy with dose adjustments based on serum drug levels.
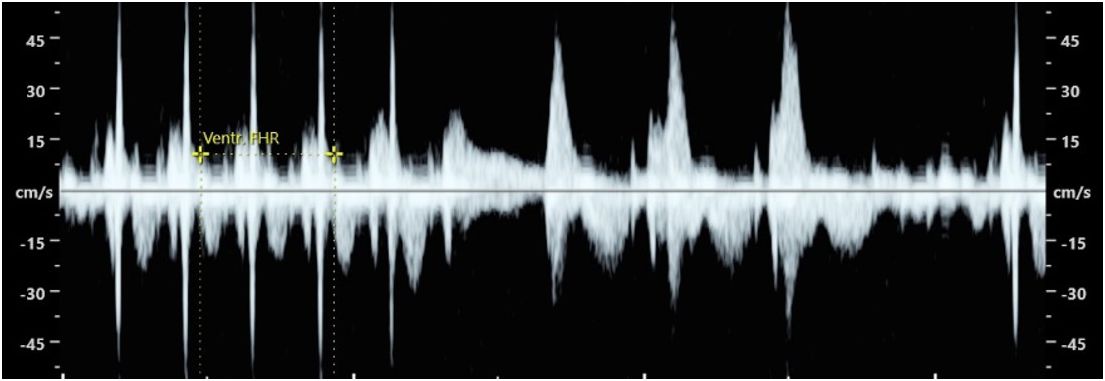
Figure 2 Fetal echocardiogram (Flow Doppler) at 21 weeks of gestation, revealing fetal supraventricular tachycardia alternating with sinus rhythm (a more explicit video is presented in Supplementary Material).
At 37 WG, the patient reported extreme fatigue and antibody titers increased once again (anti-Ro52 695 FLU; anti-Ro60 8498 FLU). Due to the similarity of the clinical presentation to what occurred at 19 WG, it was decided to repeat IVIG infusion before delivery. This also aimed to enhance immunomodulation in the newborn. Once again, the extreme fatigue resolved with this medication.
At 38 WG, she went into labor after spontaneous rupture of membranes and a vacuum extraction was performed. A healthy female baby weighing 2490g (percentile 5.2) was bornshowing no rash, cytopenia, hepatic dysfunction or any other manifestation of neonatal lupus. The neonate was started on propranolol due to the previous in utero tachyarrhythmia. At 1 month-old, a Holter monitoring revealed a short PR interval and a slurred QRS complex, consistent with WPWS (Figure 3).
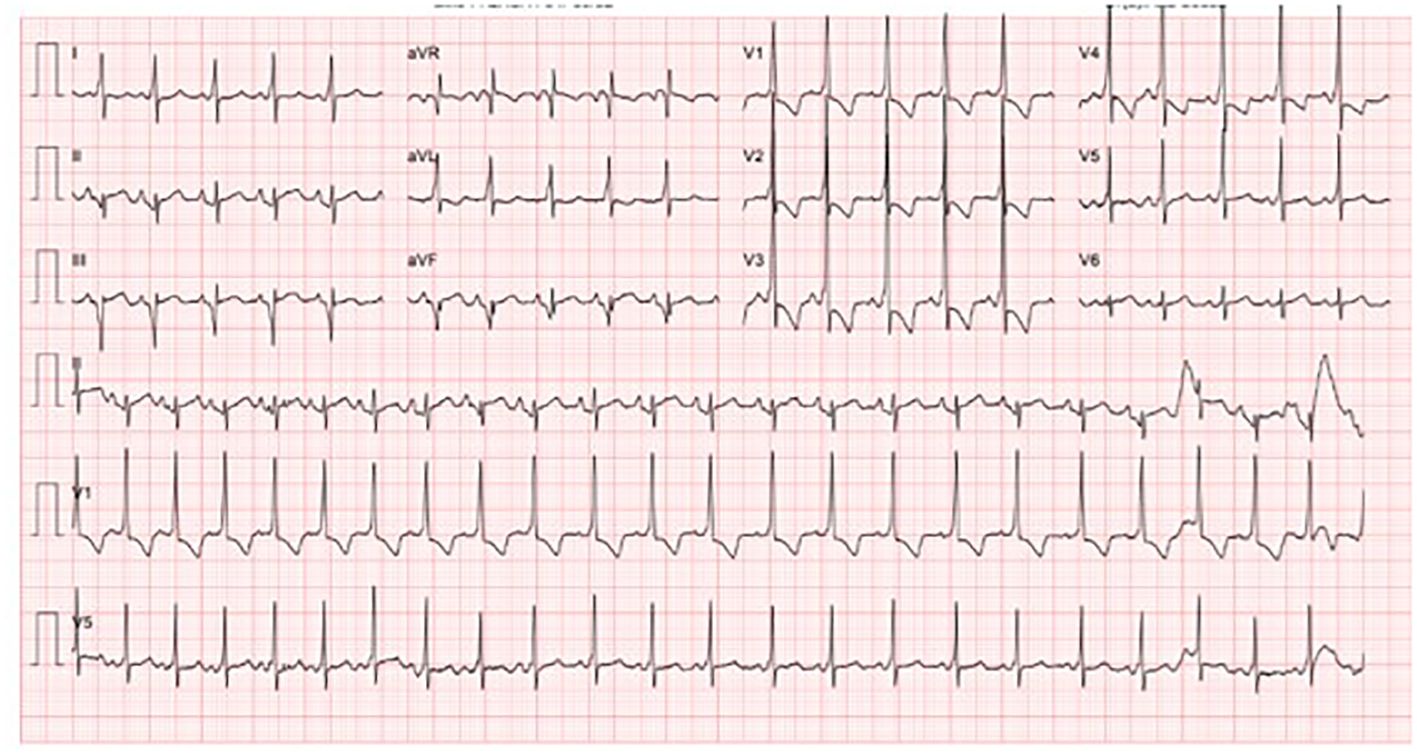
Figure 3 Holter of the newborn at 1 month-old. It. It is noticeable a short PR interval and a slurred QRS complex (delta wave) compatible with a Wolf-Parkinson-White Syndrome.
In June of 2024, the baby is now 10 months old and exhibits normal psychomotor development. The child is still under antiarrhythmic treatment, which will be maintained until she reaches one year of age. Regular follow-up appointments with pediatric cardiology are ongoing, and no new episodes of rhythm alteration were identified so far. Figure 4 illustrates the timeline of events, from the beginning of pregnancy until the postpartum period.
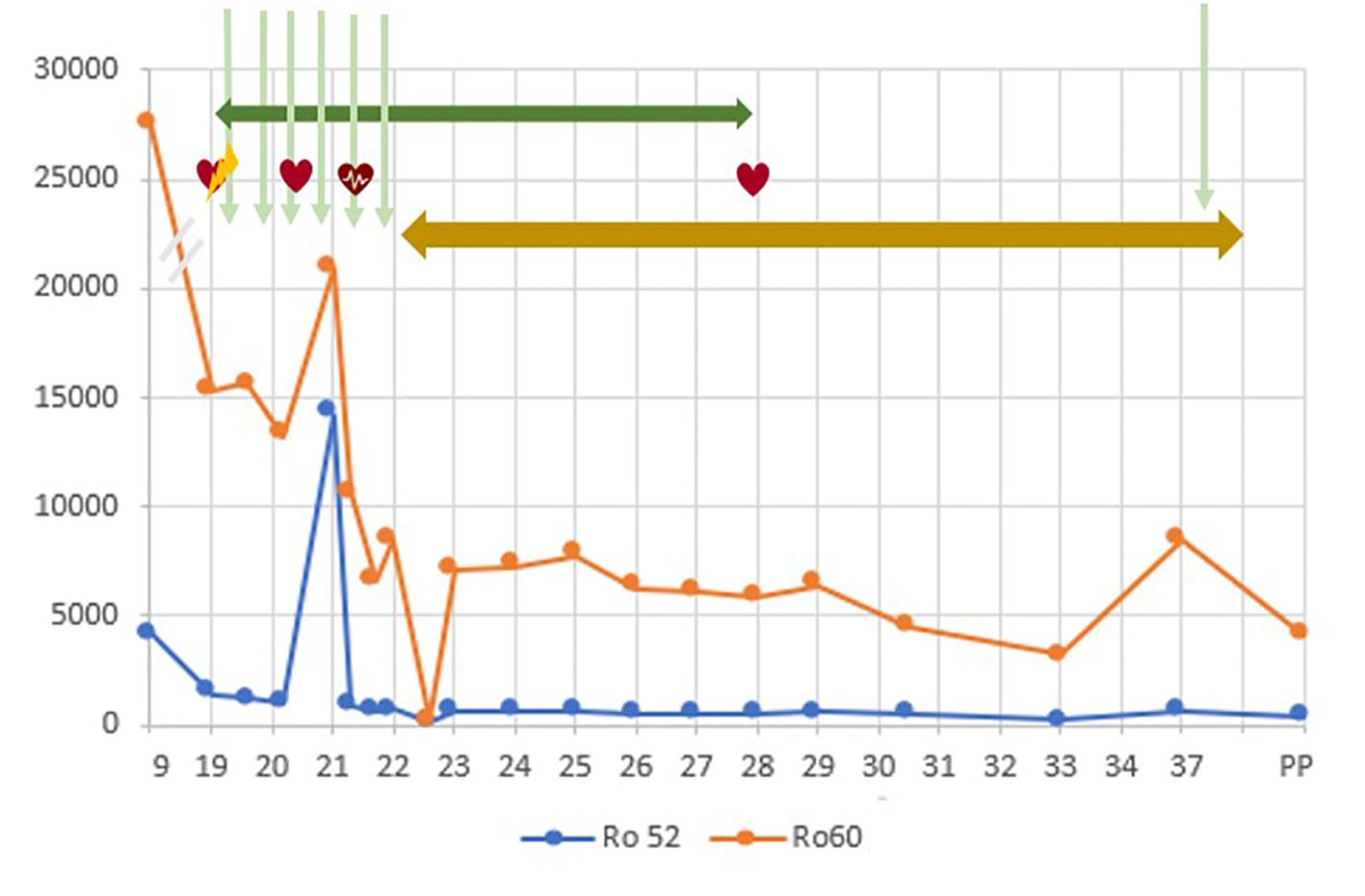
Figure 4 Timeline of events, from the beginning of pregnancy until the postpartum period. In X axis, the weeks of gestation. In Y axis, units of anti-SSA/Ro antibodies (at 9 WG, in UQ; from 19 WG on in FLU units). The blue line represents the Ro52 levels and the orange line represents the Ro60 levels. PP, postpartum
 First degree AV block
First degree AV block
 Sinus rhythm
Sinus rhythm
 Supraventricular tachycardia
Supraventricular tachycardia
 Intravenous immunoglobulin
Intravenous immunoglobulin
 Dexamethasone
Dexamethasone
 Flecainide
Flecainide
Neonatal lupus erythematosus (NLE) encompasses several fetal and child manifestations associated with maternal anti-Ro/SSA and, less frequently, anti-La/SSB auto-antibodies. This condition may affect children born to mothers with a pre-existing connective tissue disorder, primarily Sjogren’s syndrome or systemic lupus erythematosus. However, most cases are documented in asymptomatic antibody carriers (8). Manifestations linked to these antibodies include rash (in approximately 10%), transient cytopenia (around 20%) and mild transaminases elevation (approximately 30%). These complications resolve spontaneously as maternal antibodies disappear from the baby´s circulation (9). The most concerning manifestation associated with these antibodies is autoimmune congenital heart block, which may result in irreversible fetal complications and death. Anti-SSA/SSB antibodies can cross the placental barrier as early as week 11 of gestation, causing damage to fetal conduction tissues through inflammation, calcification and fibrosis, ultimately blocking signal conduction at the AV node (10).
To prevent AVB, the 2020 American College of Rheumatology Guidelines for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases recommends hydroxychloroquine during pregnancy for all women with anti-SSA/Ro and/or anti-SSB/La antibodies (10). Studies have indicated that exposure to hydroxychloroquine during fetal development may reduce the recurrence of congenital heart block by more than 50% (11, 12). This protective effect is attributed to hydroxychloroquine’s ability to inhibit Toll-like receptor 7 stimulation, preventing a cascade of events that lead to the secretion of pro-inflammatory substances and subsequent cardiac fibrosis (13, 14). Despite limited data, the safety profile of hydroxychloroquine makes it a favorable option.
Pregnant women with positive anti-SSA/Ro antibodies and a history of a previous infant with congenital heart block or other NLE manifestations should be referred for fetal heart evaluation by a pediatric cardiologist (10). Fetal cardiac conduction intervals, particularly the AV interval, should be closely monitored. American guidelines for the management of reproductive health in rheumatic diseases recommend weekly fetal echocardiography starting at weeks 16–18 and continuing up to week 26 in these high-risk patients with a previous fetal AVB (15).
Fetal AVB is considered a dynamic condition where lower-degree AVB can spontaneously revert or, on the other hand, progress to a higher-degree AVB within 24 hours (15). Treatment of fetal first-degree AVB is controversial but, recognizing that once third-degree AVB is installed the damage is irreversible, it is still recommended by international guidelines (10).
Regarding complete or third-degree AVB, no therapy has shown to improve mortality and morbidity rates associated with this condition. However, concerning incomplete AVB, the optimal pharmacological approach remains a matter of debate and an individual choice of the multidisciplinary clinic, based on local experience and available treatments. Various therapeutic interventions have been reported, mostly in single cases or small series, including corticosteroids, IVIG, plasmapheresis, beta-adrenergic agents, B cell depletion therapies, immunosuppressive agents and hydroxychloroquine (8).
According to American College of Rheumatology Guidelines for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases, if first or second-degree heart block are detected in a fetal echocardiogram, a brief course of dexamethasone is recommended (15). As a fluorinated steroid, dexamethasone can cross the placenta, exerting its effects on the developing fetus (8). Considering corticosteroids have anti-inflammatory effects, maternal administration of dexamethasone might prevent fetal AVB progression to a higher degree by mitigating the inflammatory response and potentially preventing the establishment of fibrosis of the conduction system. There may be a potential “window of opportunity” for treatment, before fibrosis is installed. Nevertheless, there are concerns about prolonged fetal exposure to corticosteroids, as it may lead to fetal growth restriction, oligohydramnios and potential long-term neurodevelopmental effects (16).
Regarding treatment with IVIG, the evidence is controversial and there is no standardized regimen. Some studies have concluded that IVIG in a dose of 400 mg/kg was ineffective as prophylactic therapy for preventing fetal AVB in high-risk pregnancies (17, 18). However, contrasting evidence suggests that IVIG may prevent the progression of immune-mediated fetal AVB by decreasing maternal serum antibody levels and potentially inhibiting the transfer of pathogenic anti-Ro/La antibodies across the placenta (19). This hypothesis is supported by murine model studies, case reports and small series using IVIG at a dose of 1mg/kg at different gestation timings (4, 20–22).
Our case report describes a patient with three significant risk factors for fetal AVB: a prior history of hydrops fetalis, high anti-SSA/Ro antibody levels and hypothyroidism. In a subsequent pregnancy, under hydroxychloroquine, a first degree AVB [PR interval of ≥150 msec (21)] was detected in a routine fetal echocardiogram at 19 WG, during an episode of extreme fatigue of the mother. At this point, the additional use of dexamethasone and IVIG might have contributed to revert the AVB, as there was a gradual reduction of maternal antibody titers and improvement in maternal symptoms. The unexpected turn of events occurred with the onset of fetal tachyarrhythmia starting at 21 WG, leading to the discontinuation of IVIG, due to concerns about its potential iatrogenic effect, and to the introduction of flecainide. In this case, starting antiarrhythmic therapy was a crucial but difficult decision, due to the potential of eliciting an AV block, a feared complication since the beginning of pregnancy. Only after birth the cause of the fetal tachyarrhythmia was identified: a concomitant WPWS diagnosis in the newborn detected by Holter.
As far as we are aware, there is only one other manuscript describing a case of NLE concomitant with WPWS. This Thai paper describes a case series of 6 newborns with NLE, all exhibiting cutaneous manifestations. Among them, one newborn had abnormal electrocardiogram changes compatible with WPWS, while no heart blocks were described (3).
Uncertainty remains regarding whether this occurrence of WPWS could potentially be another manifestation of the presence of anti-SSA/Ro antibodies, or merely a coincidental event with significant therapeutic implications.
This case highlights the importance of a multidisciplinary approach in evaluating and surveilling pregnant women with anti-SSA/SSB antibodies before, during, and after pregnancy. Prenatal management holds crucial clinical implications regarding fetal prognosis. Early detection of a fetal AVB can provide a “window of opportunity” to reverse the situation. Prompt intervention in an incomplete AVB can optimize fetal-maternal outcomes and mitigate the risks associated with autoimmune-mediated fetal AVB. However, there is a need for further research to establish clear protocols for the management of incomplete heart block in fetuses of mothers with positive anti-SSA/SSB antibodies. The additional diagnosis of WPWS in the newborn increased the complexity of this case.
“At 19 weeks of gestation, during my fourth fetal echocardiogram, a first-degree AV block was detected. This was my biggest fear, due to my SSA antibodies and past experience. Later in pregnancy, fetal tachyarrhythmia was also identified. The medical team (rheumatology, cardiology, and obstetrics) overseeing my care acted promptly to reverse the situation and stabilize the baby’s cardiac health, always explaining all procedures and their possible side effects. I remained well throughout the treatments, diligently following all medical advice, hoping for a happy outcome. Each treatment was accompanied by some anxiety, fearing that the SSA antibody levels would rise again and affect the baby. However, with the support of my family and the medical team, I felt confident and secure that this situation represented a challenge we would overcome, and that we would have our baby in our arms. Every week was a victory for all of us. At 38 weeks, Mara decided to be born beautiful and healthy”.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AC: Writing – original draft, Writing – review & editing. MR: Writing – review & editing. AL: Writing – review & editing. MS: Writing – review & editing. MP: Writing – review & editing. AA: Writing – review & editing. AC: Writing – review & editing. LP: Writing – review & editing. SC: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1397103/full#supplementary-material
Supplementary Material | We attach a short video of the fetal echocardiogram at 21 weeks of gestation, showing fetal supraventricular tachycardia alternating with sinus rhythm.
1. Llanos C, Izmirly PM, Katholi M, Clancy R, Friedman D, Kim M, et al. Recurrence rates of cardiac manifestations associated with neonatal lupus and maternal/fetal risk factors. Arthritis Rheum. (2009) 60:3091–7. doi: 10.1002/art.24768
2. Paerregaard M, Kock J, Pihl C, Pietersen A, Iversen KK, Bundgaard H, et al. The prevalence of Wolff-Parkinson-White syndrome in newborns – results from a large general population study. Eur Heart J. (2020) 41:ehaa946.3203. doi: 10.1093/ehjci/ehaa946.3203
3. Chunharas A, Nuntnarumit P, Hongeng S, Chaunsumrit A. Neonatal lupus erythematosus: clinical manifestations and management. J Med Assoc Thai. (2002) 85 Suppl 4:S1302–8.
4. Zhao L, Zhou Y, Wang C, Li Y, Zhu Q, Hua Y, et al. Successful prevention of fetal autoimmune-mediated heart block by combined therapies with hydroxychloroquine and intravenous immunoglobulin: A case report. Front Cardiovasc Med. (2021) 8:759260. doi: 10.3389/fcvm.2021.759260
5. Machimoto T, Guerra G, Burke G, Fricker F, Colona J, Ruiz P, et al. Effect of IVIG administration on complement activation and HLA antibody levels. Transpl Int. (2010) 23:1015–22. doi: 10.1111/j.1432-2277.2010.01088.x
6. Savasan S, Tuzcu V, Warrier I, Karpawich P. Cardiac rhythm abnormalities during intravenous immunoglobulin G infusion for treatment of thrombocytopenia. J Pediatr Hemat. (1997) 19(3):254–7. doi: 10.1097/00043426-199705000-00015
7. Guo Y, Tian X, Wang X, Xiao Z. Adverse effects of immunoglobulin therapy. Front Immunol. (2018) 9:1299. doi: 10.3389/fimmu.2018.01299
8. Brucato A, Tincani A, Fredi M, Breda S, Ramoni V. Should we treat congenital heart block with fluorinated corticosteroids? Autoimmun Rev. (2017) 16:1115–8. doi: 10.1016/j.autrev.2017.09.005
9. Wahren-Herlenius M, Sonesson SE, Clowse ME. Neonatal lupus erythematosus. In: Wallace D, Hahn B, editors. Dubois’ lupus erythematosus and related syndromes, 8th ed. Saunders, Philadelphia (2012). p. 464–72.
10. Liao H, Tang C, Qiao L, Zhou K, Hua Y, Wang C, et al. Prenatal management strategy for immune-associated congenital heart block in fetuses. Front Cardiovasc Med. (2021) 8:644122. doi: 10.3389/fcvm.2021.644122
11. Izmirly PM, Costedoat-Chalumeau N, Pisoni CN, Khamashta MA, Kim MY, Saxena A, et al. Maternal use of hydroxychloroquine is associated with a reduced risk of recurrent anti-SSA/Roantibody– associated cardiac manifestations of neonatal lupus. Circulation. (2012) 126:76–82. doi: 10.1161/CIRCULATIONAHA.111.089268
12. De Carolis S, Garufi C, Garufi E, De Carolis MP, Botta A, Tabacco S, et al. Autoimmune congenital heart block: A review of biomarkers and management of pregnancy. Front Pediatr. (2020) 8:607515. doi: 10.3389/fped.2020.607515
13. Barsalou J, Jaeggi E, Laskin CA, Brown P, Tian SY, Hamilton RM, et al. Prenatal exposure to antimalarials decreases the risk of cardiac but not non-cardiac neonatal lupus: a single-centre cohort study. Rheumatology. (2017) 56:1552–9. doi: 10.1093/rheumatology/kex191
14. Derdulska JM, Rudnicka L, Szykut-Badaczewska A, Mehrholz D, Nowicki RJ, Baranska-Rybak W, et al. Neonatal lupus erythematosus - practical guidelines. J Perinat Med. (2021) 49:529–38. doi: 10.1515/jpm-2020-0543
15. Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, et al. 2020 American college of rheumatology guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Care Res (Hoboken). (2020) 72:461–88. doi: 10.1002/acr.24130
16. Huić M. Maternal and fetal effects of antenatal exposure to corticosteroids. Croatian Med J. (2013) 54:564–70. doi: 10.3325/cmj.2013.54.564
17. Pisoni CN, Brucato A, Ruffatti A, Espinosa G, Cervera R, Belmonte-Serrano M, et al. Failure of intravenous immunoglobulin to prevent congenital heart block: findings of a multicenter, prospective, observational study. Arthritis Rheum. (2010) 62:1147–52. doi: 10.1002/art.27350
18. Friedman DM, Llanos C, Izmirly PM, Brock B, Byron J, Copel J, et al. Evaluation of fetuses in a study of intravenous immunoglobulin as preventive therapy for congenital heart block: results of a multicenter, prospective, open-label clinical trial. Arthritis Rheum. (2010) 62:1138–46. doi: 10.1002/art.27308
19. Sakthiswary R, D'Cruz D. Intravenous immunoglobulin in the therapeutic armamentarium of systemic lupus erythematosus: a systematic review and meta-analysis. Medicine. (2014) 93:e86. doi: 10.1097/MD.0000000000000086
20. Yu Y, Du L, Pan J, Zheng J, Chen A, Chen L. A 10-year retrospective study of neonatal lupus erythematous in China. Asian Pac J Allergy. (2016) 34:174–8. doi: 10.12932/AP0671.34.2.2016
21. Friedman DM, Kim MY, Copel JA, Llanos C, Davis C, Buyon JP. Prospective evaluation of fetuses with autoimmune-associated congenital heart block followed in the PR Interval and Dexamethasone Evaluation (PRIDE) Study. Am J Cardiol. (2009) 103:1102–6. doi: 10.1016/j.amjcard.2008.12.027
Keywords: case report, fetal atrio-ventricular block, congenital heart block, Wolff-Parkinson-White syndrome, pregnancy, anti-SSA/Ro antibodies
Citation: Chícharo AT, Rebelo M, Lopes AR, Saavedra MJ, Paramés MF, Araújo AR, Cruz-Machado AR, Pinto L and Capela S (2024) Dual challenge inside the womb: a case report of concomitant fetal atrio-ventricular block associated with maternal anti-SSA antibodies and fetal tachyarrhythmia diagnosed as Wolff-Parkinson-White syndrome after birth. Front. Immunol. 15:1397103. doi: 10.3389/fimmu.2024.1397103
Received: 06 March 2024; Accepted: 08 July 2024;
Published: 24 July 2024.
Edited by:
Gian Marco Ghiggeri, Giannina Gaslini Institute (IRCCS), ItalyReviewed by:
Michele Brignole, Italian Auxological Institute (IRCCS), ItalyCopyright © 2024 Chícharo, Rebelo, Lopes, Saavedra, Paramés, Araújo, Cruz-Machado, Pinto and Capela. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Teodósio Chícharo, YW5hdHpjaGljaGFyb0BnbWFpbC5jb20=
†These authors share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.