
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 05 June 2024
Sec. Cancer Immunity and Immunotherapy
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1383125
This article is part of the Research Topic Immunology and Immunotherapy of Skin Cancer View all 15 articles
 Johanna Matull1,2
Johanna Matull1,2 Jan-Malte Placke1
Jan-Malte Placke1 Georg Lodde1
Georg Lodde1 Anne Zaremba1
Anne Zaremba1 Jochen Utikal3,4,5
Jochen Utikal3,4,5 Patrick Terheyden6
Patrick Terheyden6 Claudia Pföhler7
Claudia Pföhler7 Rudolf Herbst8
Rudolf Herbst8 Alexander Kreuter2Julia Welzel9Julia Kretz1Inga Möller1
Alexander Kreuter2Julia Welzel9Julia Kretz1Inga Möller1 Antje Sucker1
Antje Sucker1 Annette Paschen1
Annette Paschen1 Elisabeth Livingstone1
Elisabeth Livingstone1 Lisa Zimmer1Eva Hadaschik1
Lisa Zimmer1Eva Hadaschik1 Selma Ugurel1
Selma Ugurel1 Dirk Schadendorf1,10,11Carl Maximilian Thielmann1†Klaus Georg Griewank1*†
Dirk Schadendorf1,10,11Carl Maximilian Thielmann1†Klaus Georg Griewank1*†Background: Screening for gene mutations has become routine clinical practice across numerous tumor entities, including melanoma. BAP1 gene mutations have been identified in various tumor types and acknowledged as a critical event in metastatic uveal melanoma, but their role in non-uveal melanoma remains inadequately characterized.
Methods: A retrospective analysis of all melanomas sequenced in our department from 2014–2022 (n=2650) was conducted to identify BAP1 mutated samples. Assessment of clinical and genetic characteristics was performed as well as correlations with treatment outcome.
Results: BAP1 mutations were identified in 129 cases and distributed across the entire gene without any apparent hot spots. Inactivating BAP1 mutations were more prevalent in uveal (55%) compared to non-uveal (17%) melanomas. Non-uveal BAP1 mutated melanomas frequently exhibited UV-signature mutations and had a significantly higher mutation load than uveal melanomas. GNAQ and GNA11 mutations were common in uveal melanomas, while MAP-Kinase mutations were frequent in non-uveal melanomas with NF1, BRAF V600 and NRAS Q61 mutations occurring in decreasing frequency, consistent with a strong UV association. Survival outcomes did not differ among non-uveal melanoma patients based on whether they received targeted or immune checkpoint therapy, or if their tumors harbored inactivating BAP1 mutations.
Conclusion: In contrast to uveal melanomas, where BAP1 mutations serve as a significant prognostic indicator of an unfavorable outcome, BAP1 mutations in non-uveal melanomas are primarily considered passenger mutations and do not appear to be relevant from a prognostic or therapeutic perspective.
Melanoma, a highly aggressive skin cancer with poor prognosis once metastasized, leads to approximately 55,500 deaths annually worldwide (1). Treatment options for advanced disease were limited for decades, but therapeutic breakthroughs, such as the introduction of immune checkpoint inhibitors (ICI) and targeted therapies (TT), have significantly improved progression-free and overall survival rates. Essential to their development was a better understanding of tumor immunology, genetics, and the widespread use of high-throughput sequencing in clinical routine (2).
Melanoma exhibits one of the highest mutation frequencies among all cancers, with a particularly diverse range of genetic alterations (2, 3). The Cancer Genome Atlas has proposed a genetic classification of melanoma into four subtypes based on mutations in BRAF, NRAS, NF1 and triple-wild-type melanomas (4). While some mutations have clear therapeutic implications, such as BRAF V600E, the clinical relevance of the majority of identified mutations remains poorly defined.
Mutations in the BRCA-1 associated protein 1 (BAP1) gene were recognized as relevant in various cancer types, including uveal melanoma, mesothelioma and renal cell carcinoma. BAP1 is a ubiquitin carboxy-terminal hydrolase encoded by the BAP1 gene, located on the short arm of chromosome 3. It was discovered by Jensen and colleagues in 1998 for its ability to bind to BRCA-1 and enhance its tumor suppressive activity (5, 6).
Over the years, BAP1 has been found to act independently as a tumor suppressor through its de-ubiquinating activity, which regulates target genes involved in transcription, cell cycle control, DNA damage repair, apoptosis, and cell metabolism (7). Germline BAP1 mutations cause the BAP1 predisposition syndrome (BAP1-TPDS), associated with a high susceptibility to various malignancies, such as uveal melanoma, malignant mesothelioma, cutaneous melanoma, renal cell carcinoma, and other tumors (8).
BAP1 inactivation is strongly linked to a higher metastatic risk and poor prognosis in uveal melanoma, mutated in 84% of metastatic cases (9, 10). However, in non-uveal melanoma, the role of BAP1 in tumorigenesis and its prognostic significance, particularly in cutaneous melanoma, has been controversial. Low BAP1 mRNA expression levels were reported to be associated with worse survival in some cutaneous melanoma patient cohorts, while in others, low BAP1 mRNA expression was associated with better overall survival (11, 12).
Current research suggests that loss of BAP1 may have a growth-sustaining effect, making it a potential therapeutic target (13). This study aims to further understand the role of BAP1 and its implications on clinical course in non-uveal and uveal melanoma by examining a multicenter cohort and correlating clinical and survival information in the respective patients.
The next-generation sequencing reports from a total of 2650 melanoma patients analyzed at the Department of Dermatology, University Hospital Essen, were reviewed to identify patients harboring BAP1 mutations (n=129). Of those, 60 tissue samples and related clinical data were obtained from the Westdeutsche Biobank Essen (11–4715-BO), and 69 from the prospective multicenter translational study Tissue Registry in Melanoma (ADOREG/TRIM; NCT05750511; CA209–578; 15–6566-BO) conducted by the German Dermatological Cooperative Oncology Group. Existing data of BAP1 wildtype melanoma samples (n=1215) were analyzed for comparison of mutational load and mutation types. Tumors were classified as per the American Joint Committee on Cancer (AJCC 8th) staging system (14). Histological evaluation was carried out by local board-certified dermatopathologists. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee of the University of Duisburg-Essen (ethics approval no. 21–9873-BO).
Formalin-fixed, paraffin-embedded (FFPE) specimens were prepared in 10 μm sections and deparaffinized according to standard procedures. After airdrying, the tumor tissue was manually macrodissected from sections (15). Genomic DNA was isolated applying the QIAamp DNA Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions.
Sequencing was performed using a 30-gene custom amplicon-based panel as previously described, covering known melanoma-related gene mutations including BAP1 (Supplementary Table 1) (16).
To eliminate questionable low frequency background mutation calls, mutations were reported only if ≥ 10 reads reported the mutated variant, coverage of the mutation site was ≥ 30 reads and the frequency of mutated reads was ≥ 10%. The average read coverage of the targeted area achieved in the study was 1773x. All samples were sequenced using an Illumina MiSeq and analyzed with the same software (CLC) by the same team over the past eight years. In 2018, there was a transition from PCR-based amplification to an oligo-capture-based technique by Integrated DNA Technologies (IDT).
Associations between covariates were investigated using chi-squared and Fisher’s exact tests as indicated. Continuous variables are presented as mean with standard deviation or as median with range, as appropriate. Categorical variables are presented as counts and percentages. Survival data were analyzed using the Kaplan-Meier method with log-rank testing. Progression-free survival (PFS) was calculated from date of systemic treatment initiation to date of progression, or death. Censoring occurred upon change of therapeutic regimen or date of last follow-up.
Overall survival (OS) was calculated from the first date of stage IV diagnosis or start of ICI/TT therapy until death or last patient contact (censored observation), respectively. Tests with P-values less than.05 were considered statistically significant. Statistical analyses were performed using Microsoft Excel, GraphPad Prism (version 9), SPSS 27.0 (IBM Corp., Armonk NY, USA), R (R version 4.0.3 (2020–10-10)) and RStudio (17).
Among a cohort of 2650 melanoma patients, 129 patients harboring a BAP1 mutation (BAP1mut) were identified and included in this study. Of those, 116 (89.9%) cases were categorized as non-uveal melanoma (NUM) based on the origin of the primary tumor (cutaneous (n=98), mucosal (n=6), meningeal (n=1), or occult (n=11)). Two additional cases with missing primary location information were considered NUM based on mutational pattern. Eleven (8.5%) cases were of uveal origin.
In the non-uveal melanoma subgroup (n=118) median age at first diagnosis was 60 years (range 22–82) and 65.3% (n=77) patients were male (Table 1). In patients with cutaneous melanoma and documented primary (n=45), the most common reported localization was the lower extremity (n=16; 35.6%). Trunk, head and neck and upper extremity were less frequent (n=13; n=12; n=4, respectively).
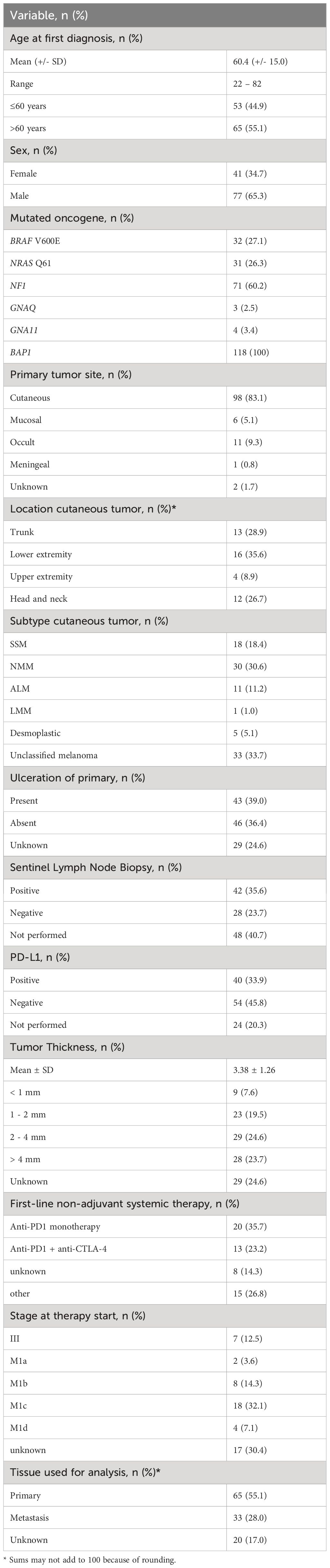
Table 1 Clinical characteristics of patients with BAP1mut non-uveal melanoma (n=118).
Of all patients receiving systemic therapy (n=56), anti-PD-1 monotherapy was most frequently administered as first-line treatment (20 cases, 35.7%). CTLA4/PD-1 blockade and BRAF/MEK targeted therapy was less common (13 and 8 cases, respectively). In 15 cases (26.8%) other therapeutic regimens were used including chemotherapy-based regimens, anti-CTLA-4 monotherapy, BRAF inhibitor monotherapy and combination therapy of anti-PD1 and BRAF/MEK inhibitors.
Activating mutations in BRAF V600, NRAS Q61 or mutations in NF1 were detected in 32 (27.1%), 31 (26.3%) and 71 (60.2%) samples, respectively. Activating mutations in GNAQ/GNA11 genes were less common with mutations in 3 and 4 samples (2.5% and 3.4%, respectively) (Figure 1A, Supplementary Table 2). BAP1 mutations were inactivating frameshift or nonsense (hereafter abbreviated and termed “INAC”) in 16.9% (n=20) of cases.

Figure 1 Characteristics of BAP1mut melanoma. Distribution of activating gene mutations in BAP1mut non-uveal (left) and uveal (right) melanoma tumor samples (A). Left: BAP1mut melanoma harbored more mutations than BAP1wtmelanoma. Middle: Within the group of BAP1mut melanoma, non-uveal tumors exhibited higher mutation numbers than tumors of uveal origin. Right: Non-uveal BAP1mut tumors from cutaneous sites showed the highest number of mutations compared with tumors of uveal origin and mucosal, meningeal or occult origin (subsumed as “other”) (B). Uveal BAP1mut tumor samples exhibited the lowest amount of C>T substitutions compared to both non-uveal BAP1mut and BAP1wt melanomas (C). Statistical tests were performed using Welch’s t test and Dunnett’s test. Data is shown as mean ± SEM. *p < 0.05, ****p < 0.0001.
In this subgroup, 5 patients were female and 6 were male. Median age at diagnosis was 65 years (range 43–84) (Table 2). Neither age at first diagnosis nor sex differed significantly between NUM and uveal melanoma subgroup (Table 3).
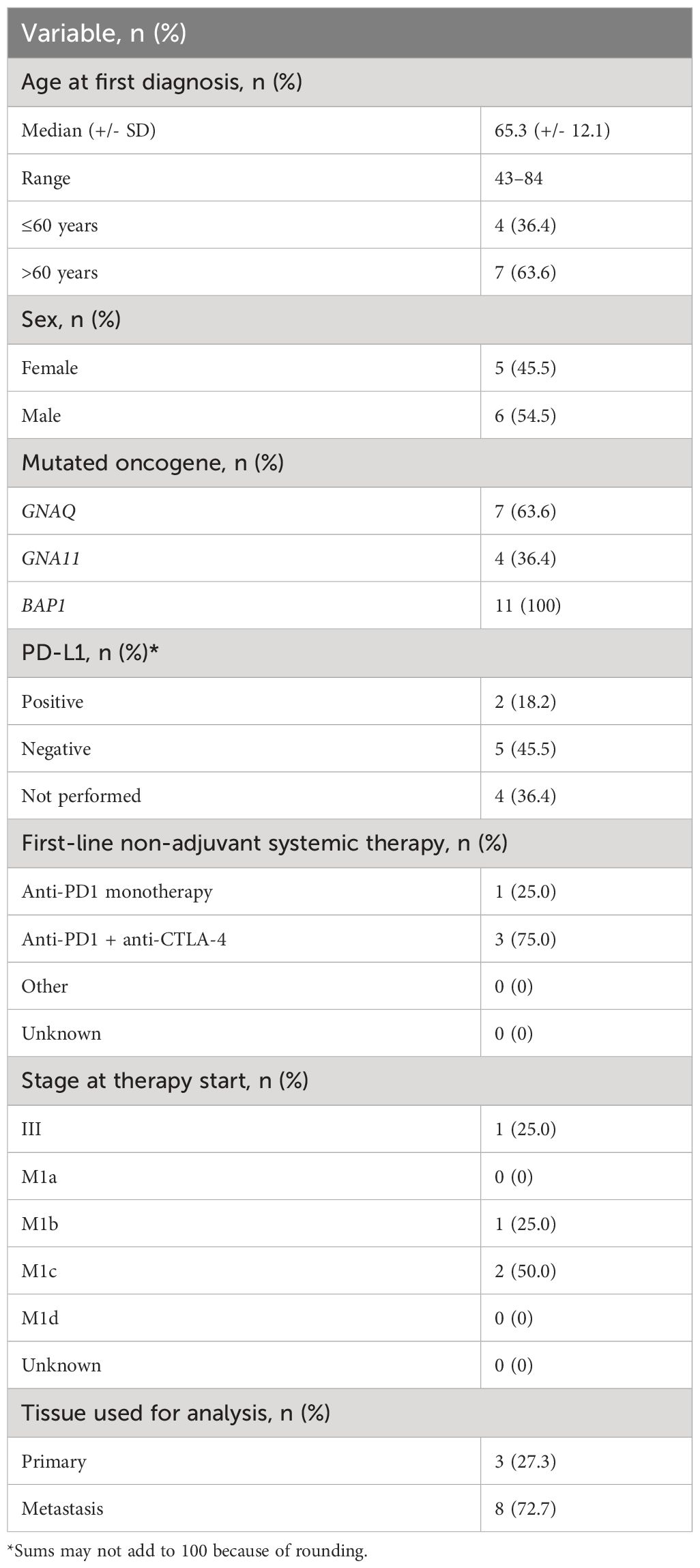
Table 2 Clinical characteristics of patients with BAP1mut uveal melanoma (n=11).
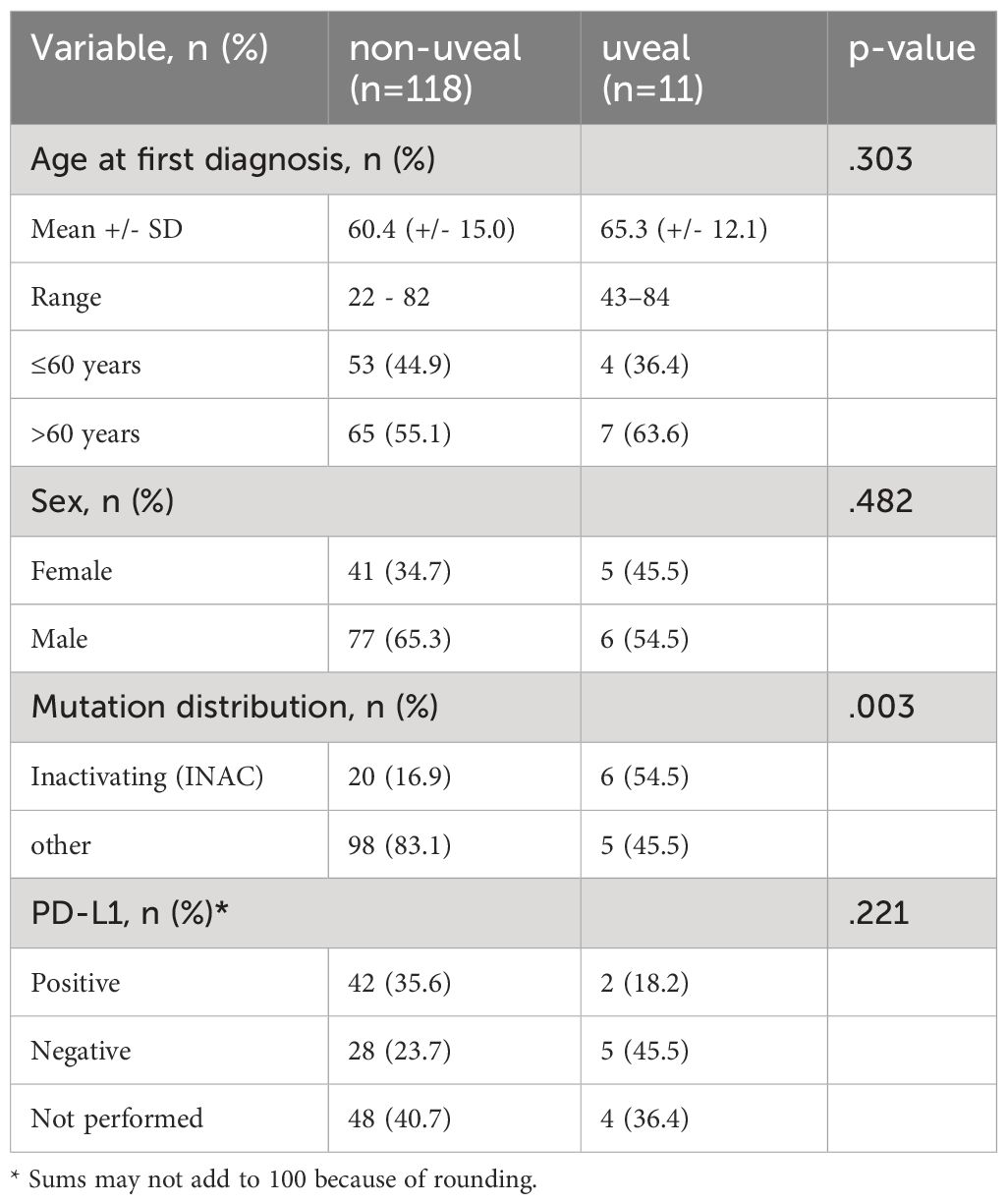
Table 3 Comparison of clinical characteristics between BAP1mut non-uveal and uveal melanoma patients.
Combined CTLA4/PD-1 blockade was administered in 3 of 4 cases as first-line non-adjuvant systemic therapy.
No BRAF, NRAS or NF1 mutations were detected in uveal melanoma samples. GNAQ and GNA11 mutations were regularly present with mutations in 7 (63.6%) and 3 samples (27.3%), respectively. BAP1 mutations were detected in all 11 samples with 54.5% inactivating mutations (n=6).
271 BAP1 mutations were identified in the 129 examined samples (Supplementary Table 4). Non-uveal melanomas frequently harbored more than one BAP1 mutation (n=54, 45.8%), while only 3 samples of uveal origin (27.3%) harbored two or more (Supplementary Table 5). Mutations in BAP1 were distributed equally without clustering or hotspots. The primary catalytic domain of BAP1 protein harbored both inactivating and missense mutations (Figure 2). Uveal melanomas harbored significantly more inactivating (frameshift or nonsense) mutations than non-uveal (54.5% and 16.9%, p=0.003).
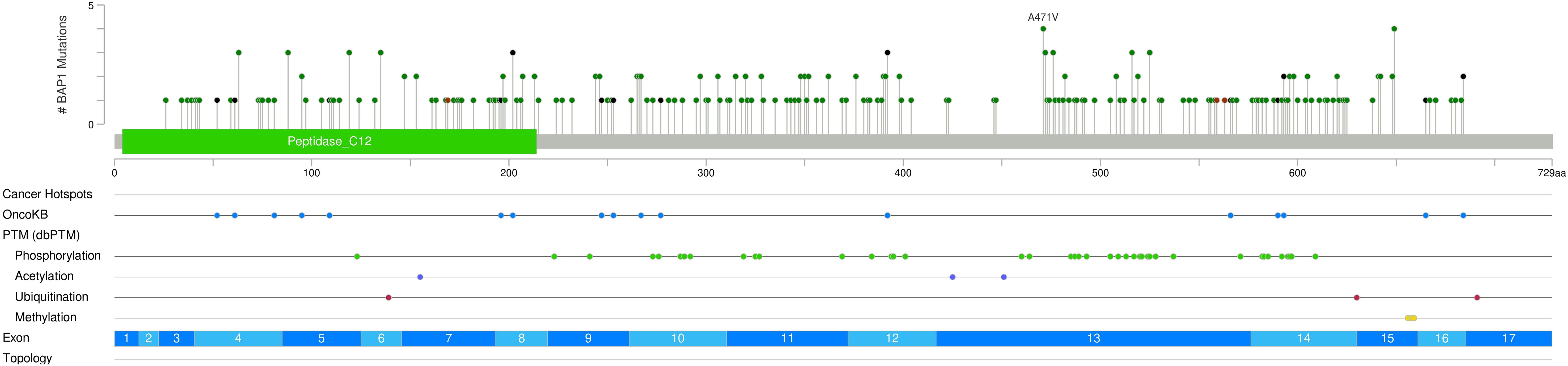
Figure 2 Lollipop mutation graph demonstrates the distribution of mutations throughout the BAP1 gene with missense mutations shown in green, inactivating (Nonsense or frame-shift mutations) in black, and frameshift mutations in brown.
Mutations in other genes were identified in 117 NUM tumor samples (97.5%). BRAF mutations were found in more than half of the cases (n=62, 53.4%) with activating V600E and V600K mutations in 32 (27.1%) and 3 samples (2.5%), respectively. NRAS mutations were found in 54 samples (45.8%), of which 33 (28.0%) were activating Q61/G12 mutations. KRAS mutations were less frequent with 5 activating mutations (4.2, 1 G12V, 3 G12D, 1 G13S). NF1 mutations were present in 71 samples (60.2%) and activating TERT-promoter mutations in 54 samples (45.8%) (Supplementary Table 4). Other frequently mutated genes included ARID1A (65.3%), ARID2 (59.3%), and SMARCA4 (58.5%). Less frequent mutations were reported in various genes including SF3B1, KIT, TERT, TP53, WT1, PIK3CA, FBXW7, GNA11, CTNNB1, PIK3R1, MAP2K1, MITF, IDH1, MAP2K2, GNAQ, PTEN, EZH1, RAC1 and CDK4 (Figure 3).
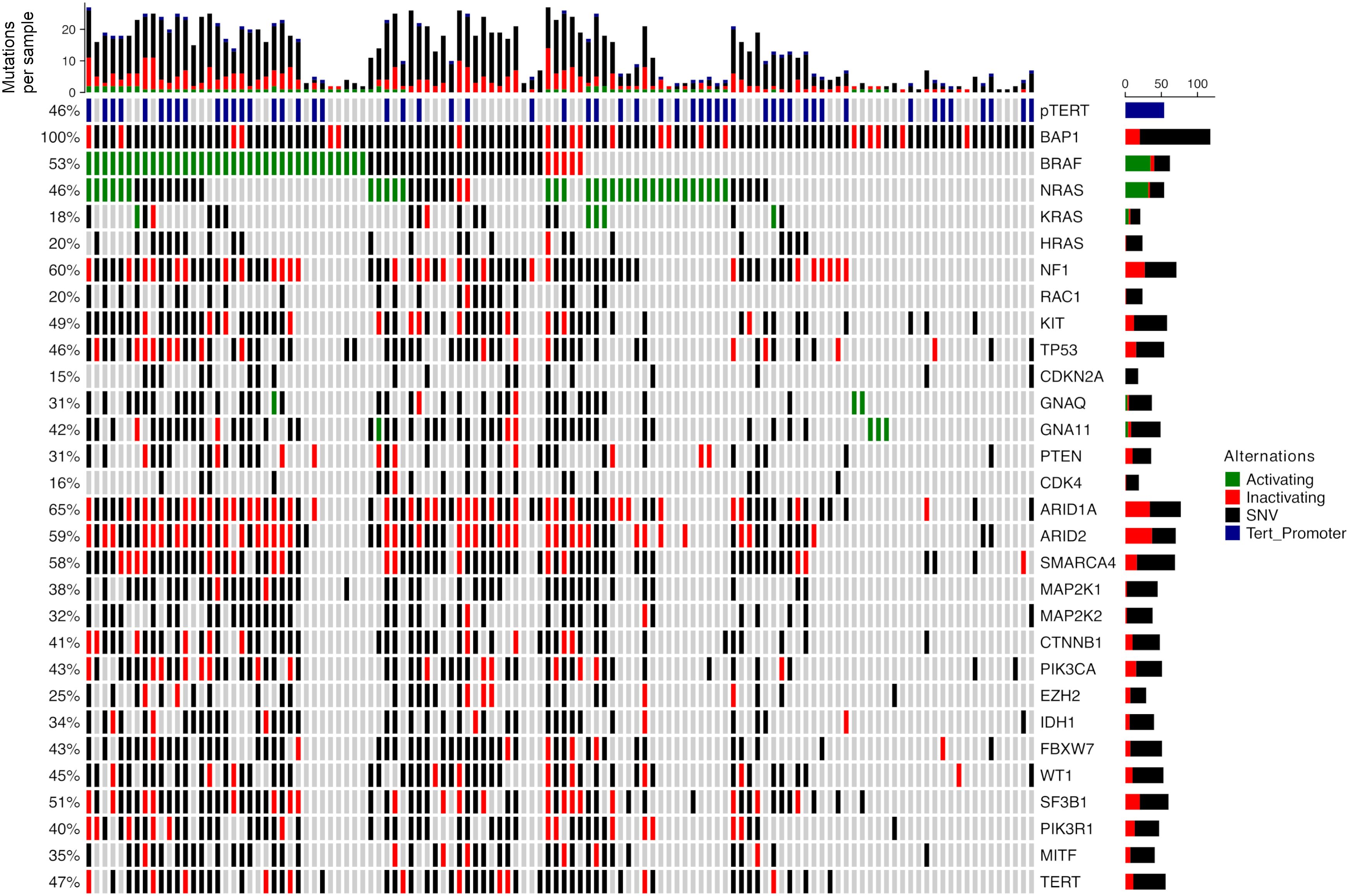
Figure 3 Mutation distribution in BAP1mut non-uveal melanoma. Green: mutations known or assumed to be activating. Red: loss of function mutations. Blue: known activating mutations in the TERT promoter region.
No BRAF, NRAS, NF1 or TERT promoter mutations were detected, though all tumor samples harbored additional mutations (Figure 4). GNAQ and GNA11 mutations were frequent with 7 (63.6%) and 4 mutations (36.4%) and predominantly activating (100% of GNAQ mutations and 75% of GNA11). Mutations affecting codon 209 in GNAQ were Q209L (n=3), Q209P (n=2) and Q209R (n=1). One sample harbored an activating R183Q mutation. In GNA11 all codon 209 mutations were Q209L (n=2). One sample harbored an activating R183C mutation in Exon 4. More than half of detected BAP1 mutations were found to be inactivating. Rarer mutations identified were SF3B1, ARID1A, and SMARCA4.
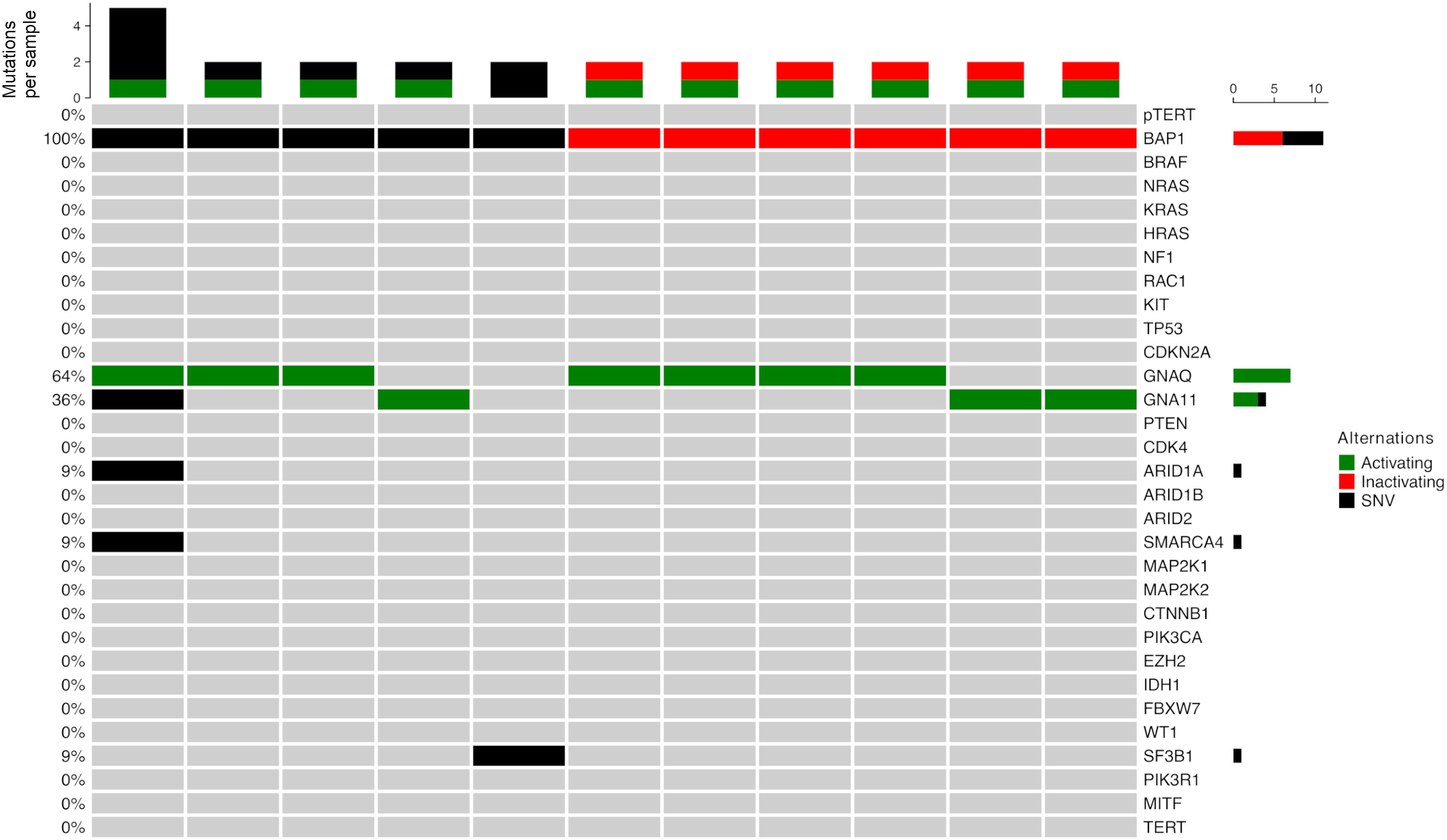
Figure 4 Mutation distribution in BAP1mut uveal melanoma. Green: mutations known or assumed to be activating. Red: loss of function mutations.
BAP1mut melanomas (n=129) exhibited a significantly higher number of mutations compared to BAP1wt melanomas (n=1215) with 33.1 versus 4.1 mutations per sample. Within the group of BAP1mut melanomas, uveal melanomas demonstrated lower mutation frequencies compared to BAP1mut NUM (3.3 mutations versus 35.9 mutations per sample). Upon subgroup analysis of the non-uveal BAP1mut cohort, cutaneous melanomas exhibited a higher mutational load compared to those of mucosal, meningeal, or occult origin (mean 39.5 and 18.2 mutations per sample, respectively) (Figure 1B).
BAP1mut NUM showed significantly more C>T alterations than BAP1wt melanomas. Uveal BAP1mut tumor samples were found to exhibit the lowest amount of C>T substitutions compared to both non-uveal BAP1mut and BAP1wt melanomas (Figure 1C).
Survival analysis showed a median overall survival time of 38.0 months for all included patients with stage lV BAP1mut tumors with matching survival data (n=81). Comparison of OS between patients with BAP1mut uveal and non-uveal melanoma revealed a longer survival for those with NUM, though nonsignificant (41.2 and 44.7, respectively, p=0.26) (Figure 5A).
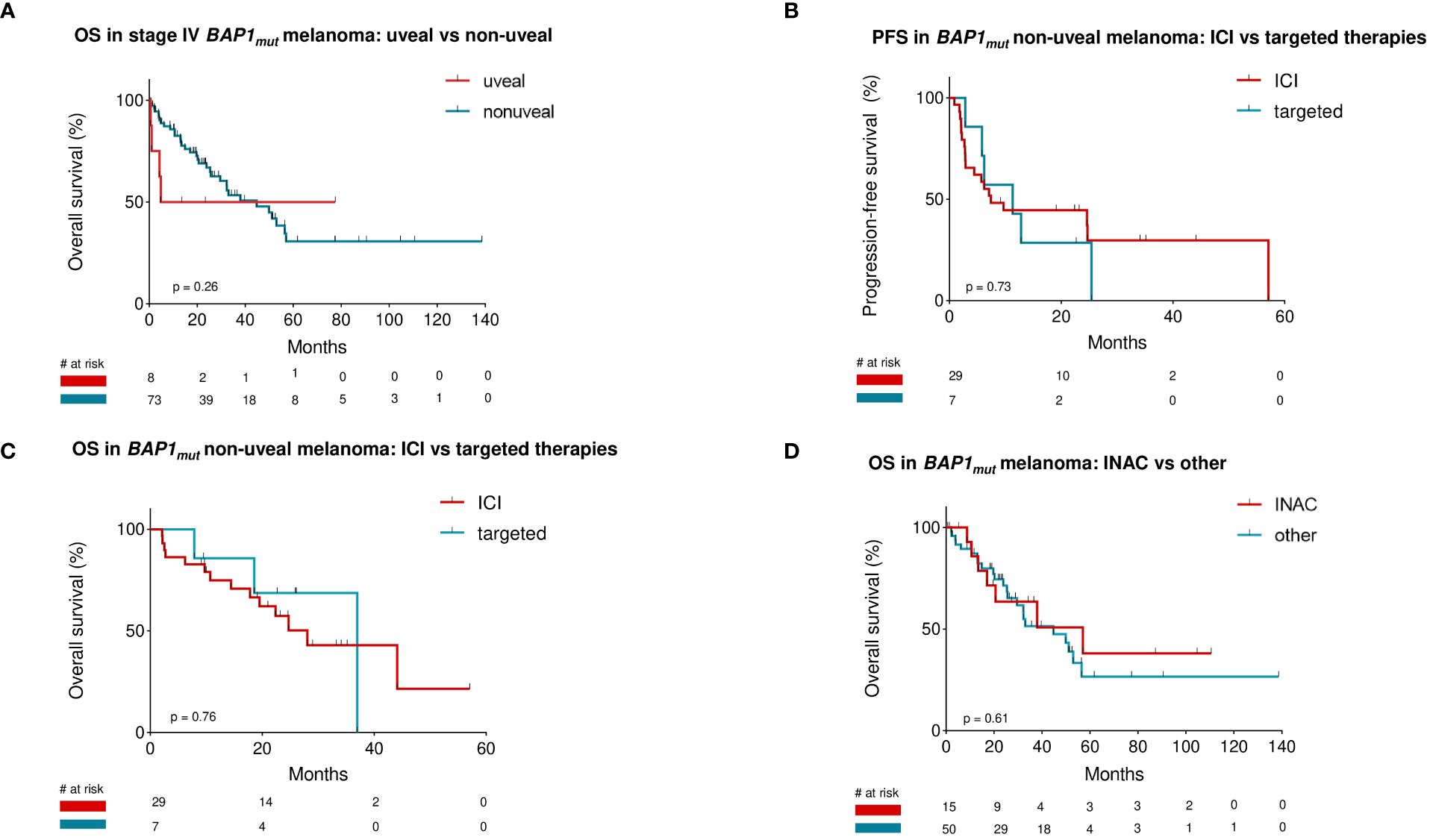
Figure 5 Patients with stage IV BAP1mut non-uveal melanoma (n=73) did not show a difference in overall survival compared to patients with stage IV BAP1mut uveal melanoma (n=8) (A). Survival rates of BAP1mut non-uveal melanoma patients receiving immunotherapy as first non-adjuvant therapy compared to those receiving targeted therapies showed no significant difference in either progression-free or overall survival (B, C). Patients with inactivating BAP1 mutations did not differ in overall survival compared to those with other mutation types (D).
Survival rates of NUM patients receiving immunotherapy as first non-adjuvant therapy (n=29) were 7.4 (mPFS) and 28.1 months (mOS), respectively. Patients receiving targeted therapies (n=7) as first-line therapy had a mPFS of 11.3 and mOS of 37.0 months. Comparison of survival rates between ICI-cohort and TT-cohort did not show any significant difference in either PFS or OS: p=0.73 and p=0.76, respectively (Figures 5B, C).
Further analysis of OS in patients with stage lV BAP1mut NUM depending on mutation-type showed a median OS of 57.0 months for patients with inactivating BAP1 mutations (n=15) and 44.7 months for those with other mutation-types (n=50). The observed difference was not statistically significant (p=0.61) (Figure 5D).
A case-by-case analysis for uveal melanoma patients was performed to evaluate treatment response (Supplementary Table 3). All patients with first-line non-adjuvant systemic therapy received ICI-based regimens (n=4). Treatment response to ICI was progressive disease in three patients (75%). One patient (25%) exhibited a partial response (this tumor harbored a GNA11 R183C and a BAP1 R385* mutation, Supplementary Table 3).
In seven cases BAP1mut non-uveal tumors were identified harboring activating GNAQ or GNA11 mutations. Four tumors were of cutaneous origin, two occult and one melanocytoma of the central nervous system. Therapies were diverse and follow-up data incomplete (Supplementary Table 2).
Our study aimed to investigate the genetic characteristics of BAP1mut melanoma based on a cohort of 129 uveal and non-uveal melanoma patient cases, and to correlate these with clinicopathological data and outcomes.
To the best of our knowledge, this study is the largest to date investigating BAP1mut non-uveal melanoma and contains the most detailed genetic analysis of this melanoma subtype.
Among BAP1mut non-uveal melanoma cases, we observed a predominance of nodular melanoma as the most prevalent histopathological subtype, and a skewed distribution of tumor thickness towards thicker tumors. This finding is noteworthy as superficial spreading melanomas typically represent the prevailing subtype in Western countries (18). Mucosal and uveal melanomas were overrepresented compared to BAP1wt cohorts, fitting existing data (9, 19–22).
Mutation patterns varied substantially between non-uveal and uveal samples. Uveal BAP1mut melanomas exhibited significantly lower numbers of accompanying mutations and no evidence of UV-induced mutagenesis (23). In contrast, non-uveal BAP1mut melanomas had a higher mutational burden and number of UV-signature mutations (C>T/CC>>TT transitions) than BAP1wt melanomas, indicating preferential tumor occurrence in sun-exposed skin (20).
Analysis of uveal BAP1mut samples revealed a significantly lower total number of mutations, lacking common cutaneous driver mutations, while harboring known uveal melanoma driver mutations (10, 23). Genomic patterns of BAP1mut non-uveal melanomas differed substantially from those of uveal origin in terms of mutational load and driver oncogenes: NF1, BRAF, and NRAS mutations were frequent, often with numerous co-mutations. NF1 was the most common concomitant mutation. High mutation numbers and frequent NF1 mutations may suggest that BAP1mut non-uveal melanomas tend to be hypermutated tumors (24, 25). Previous reports on BAP1mut cutaneous melanocytic tumors have indicated higher frequencies of concurrent BRAF V600E mutations compared to our cohort (26). It will be interesting to see if other, larger studies can validate this finding.
BAP1 mutations are associated with poor prognosis in uveal melanoma, but their prognostic value in non-uveal melanoma remains controversial (10, 27, 28). Recent studies have shown that BAP1 mutations are associated with an inflammatory tumor microenvironment and increased immune cell infiltration, suggesting a potential role as a predictive biomarker for immunotherapy response (6, 29–32). Furthermore, it is well-documented that BAP1 mutations in uveal melanoma strongly correlate with BAP1 expression in immunohistochemical staining (33). However, we did not observe a significant difference in overall survival of stage lV non-uveal melanoma patients harboring BAP1 mutations compared to published BAP1 wildtype cohorts (16, 24). Within the cohort of uveal melanoma, a case-by-case analysis of four patients revealed a poor response to immunotherapy, consistent with previous studies, showing low efficacy of anti-PD-1 and anti-CTLA-4 therapies in uveal melanoma (9, 34). Overall survival independent of treatment in uveal melanoma patients, calculated from the initial diagnosis of stage IV, was relatively long compared to other cohorts of metastatic uveal melanoma patients reported previously (35). We believe this is partly due to selection bias, likely caused by the small number of patients with metastatic uveal melanoma treated in our department.
Although very rare, non-uveal melanoma with a uveal melanoma gene mutation signature can occur. These entities, termed “blue-nevus like melanoma” if cutaneous, or “primary central nervous system melanoma” if derived from the central nervous system, behave similarly to uveal melanoma (36). Our cohort encompassed seven cases; however, limited case number and follow-up did not allow a representative comparison. In these tumors, BAP1 mutations should not be seen as passenger mutations but relevant markers of metastasis and prognosis (37, 38).
Our study has certain limitations. We conducted sequencing on both primary tumors and metastases, and our assay may not have detected deletions involving entire exons, potentially resulting in missed identification of BAP1 alterations in some patients. Due to the retrospective study design and long data collection period as well as advances in sequencing technology over the years, there might be variations in the mutation detection rate or characterization accuracy over time. In addition, changes in treatment standards have occurred, making the interpretation of survival analysis challenging for this study. The cohort we analyzed was heterogeneous and consisted of various types of melanoma, including cutaneous, mucosal, occult, and meningeal melanoma. Furthermore, due to the retrospective nature of this study, we did not have access to comprehensive immunohistochemical staining for this cohort, which could have provided additional information, such as whether loss of protein expression is a good surrogate for BAP1 mutation status in non-uveal melanoma, as has been well demonstrated for uveal melanoma.
Although our findings are based on the largest cohort of BAP1mut non-uveal melanomas to date, larger, preferably prospective studies are needed to validate our results.
Our analysis demonstrates that, except for rare cases such as non-uveal melanomas exhibiting a uveal melanoma mutation signature and cases involving germline mutations, where BAP1 mutations are associated with poor prognosis or familial predisposition syndromes, respectively, BAP1 mutations in non-uveal melanomas are typically passenger mutations. These mutations are predominantly found in heavily mutated tumors and do not appear to have any significant prognostic or therapeutic value.
The data analyzed in this study is subject to the following licenses/restrictions: The data underlying this article will be shared on reasonable request to the corresponding author. Requests to access these datasets should be directed toa2xhdXMuZ3JpZXdhbmtAdWstZXNzZW4uZGU=.
The studies involving humans were approved by ethics committee of the University of Duisburg-Essen (ethics approval no. 21-9873-BO). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by- product of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
JM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. J-MP: Data curation, Writing – review & editing. GL: Writing – review & editing. AZ: Writing – review & editing. JU: Data curation, Writing – review & editing. PT: Data curation, Writing – review & editing. CP: Data curation, Writing – review & editing. RH: Data curation, Writing – review & editing. AK: Data curation, Writing – review & editing. JW: Data curation, Writing – review & editing. JK: Data curation, Writing – review & editing. IM: Data curation, Writing – review & editing. AS: Data curation, Writing – review & editing. AP: Data curation, Writing – review & editing. EL: Data curation, Writing – review & editing. LZ: Data curation, Writing – review & editing. EH: Data curation, Writing – review & editing. SU: Data curation, Writing – review & editing. DS: Data curation, Writing – review & editing. CT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing. KG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was in part supported by Bristol Myers Squibb for the multicenter translational study “Tissue Registry in Melanoma” (TRIM) within the framework of the skin cancer registry ADOREG of the German Dermatologic Cooperative Oncology Group (DeCOG). J-MP was supported by the DFG (German Research Foundation)funded Clinician Scientist Program of the University Medicine Essen Clinician Scientist Academy (UMEA) (FU 356/12-1).
The authors are indebted to all patients and their relatives. Human biological samples and related data were obtained from the Westdeutsche Biobank Essen (11–4715-BO, n=60), and from the prospective multicenter translational study Tissue Registry in Melanoma (ADOREG/TRIM; NCT05750511; CA209–578; 15–6566-BO, n=69) conducted by the German Dermatological Cooperative Oncology Group (DeCOG).
JM: Declares travel support from Bristol Myers Squibb, Novartis and Sun Pharmaceutical Industries, outside the submitted work. J-MP: served as consultant and/or has received honoraria from Bristol-Myers Squibb, Novartis, Sanofi and received travel support from Bristol-Myers Squibb, Novartis, Pierre Fabre and Therakos, outside the submitted work. GL: Declares travel support from Sun Pharma, outside the submitted work. AZ: Declares travel support from Novartis, Sanofi Grenzyme, and Bristol-Myers Squibb, outside the submitted work. JU: Is on the advisory board or has received honoraria and travel support from Amgen, Bristol Myers Squibb, GSK, Immunocore, LeoPharma, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche, Sanofi outside the submitted work. PT: served as consultant and/or received honoraria form Almirall, Bristol Myers Squibb, Biofrontera, Curevac, Kyowa Kirin, Merck, Merck Sharp & Dohme, Novartis, Pierre-Fabre, Roche, Sanofi, 4SC, and travel support from Bristol Myers Squibb outside the submitted work. CP: Received honoraria speaker honoraria and advisory-board honoraria and travel support from BMS, MSD, Novartis, Merck Serono, Pierre Fabre, Sunpharma, AbbVie, LEO, and Kyona Kirin, outside the submitted work. RH: Is an employee of Helios Kliniken Erfurt GmbH. JW: Received honoraria and travel support from Almirall, Bristol Myers Squibb, Novartis, Pierre Fabre and Merck Sharp & Dohme, outside the submitted work. EL: Served as consultant and/or has received honoraria from Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, Sanofi, Sunpharma, Takeda and travel support from Bristol-Myers Squibb, Pierre Fabre, Sunpharma and Novartis, outside the submitted work. LZ: Served as consultant and/or has received honoraria from Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, Sunpharma and Sanofi; Research funding to institution: Novartis; travel support from Merck Sharp & Dohme, Bristol- Myers Squibb, Amgen, Pierre-Fabre, Sunpharma and Novartis, outside the submitted work. SU: Research support from Bristol Myers Squibb and Merck Serono; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Merck Serono, and Novartis; meeting and travel support from Almirall, Bristol-Myers Squibb, IGEA Clinical Biophysics, Merck Sharp & Dohme, Novartis, Pierre Fabre, and Sun Pharma, outside the submitted work. DS: Reports personal fees and non-financial support from Roche/Genentech, grants, personal fees, non-financial support and other from BMS, personal fees from Merck Sharp & Dohme, personal fees and non-financial support from Merck Serono, grant, personal fees and non-financial support from Amgen, personal fees from Immunocore, personal fees from Incyte, personal fees from 4SC, personal fees from Pierre Fabre, personal fees and non-financial support from Sanofi/Regeneron, personal fees from Array BioPharma, personal fees from Pfizer, personal fees from Philogen, personal fees from Regeneron, personal fees from Nektar, personal fees from Sandoz, grants, personal fees and non-financial support from Novartis, personal fees and non-financial support from SunPharma, Replimune, Helsinn, OncoSec and InFlaRx outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1383125/full#supplementary-material
1. Schadendorf D, van Akkooi ACJ, Berking C, Griewank KG, Gutzmer R, Hauschild A, et al. Melanoma. Lancet. (2018) 392:971–84. doi: 10.1016/S0140–6736(18)31559–9
2. Davis EJ, Johnson DB, Sosman JA, Chandra S. Melanoma: What do all the mutations mean? Cancer. (2018) 124:3490–9. doi: 10.1002/cncr.31345
3. Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV, et al. Signatures of mutational processes in human cancer. Nature. (2013) 500:415–21. doi: 10.1038/nature12477
4. Cancer Genome Atlas N. Genomic classification of cutaneous melanoma. Cell. (2015) 161:1681–96. doi: 10.1016/j.cell.2015.05.044
5. Jensen DE, Proctor M, Marquis ST, Gardner HP, Ha SI, Chodosh LA, et al. BAP1: a novel ubiquitin hydrolase which binds to the BRCA1 RING finger and enhances BRCA1-mediated cell growth suppression. Oncogene. (1998) 16:1097–112. doi: 10.1038/sj.onc.1201861
6. Louie BH, Kurzrock R. BAP1: Not just a BRCA1-associated protein. Cancer Treat Rev. (2020) 90:102091. doi: 10.1016/j.ctrv.2020.102091
7. Wang A, Papneja A, Hyrcza M, Al-Habeeb A, Ghazarian D. Gene of the month: BAP1. J Clin Pathol. (2016) 69:750–3. doi: 10.1136/jclinpath-2016–203866
8. Rai K, Pilarski R, Cebulla CM, Abdel-Rahman MH. Comprehensive review of BAP1 tumor predisposition syndrome with report of two new cases. Clin Genet. (2016) 89:285–94. doi: 10.1111/cge.12630
9. Yang J, Manson DK, Marr BP, Carvajal RD. Treatment of uveal melanoma: where are we now? Ther Adv Med Oncol. (2018) 10:1758834018757175. doi: 10.1177/1758834018757175
10. Decatur CL, Ong E, Garg N, Anbunathan H, Bowcock AM, Field MG, et al. Driver mutations in uveal melanoma: Associations with gene expression profile and patient outcomes. JAMA Ophthalmol. (2016) 134:728–33. doi: 10.1001/jamaophthalmol.2016.0903
11. Kumar R, Taylor M, Miao B, Ji Z, Njauw JC, Jonsson G, et al. BAP1 has a survival role in cutaneous melanoma. J Invest Dermatol. (2015) 135:1089–97. doi: 10.1038/jid.2014.528
12. Liu-Smith F, Lu Y. Opposite roles of BAP1 in overall survival of uveal melanoma and cutaneous melanoma. J Clin Med. (2020) 9:411. doi: 10.3390/jcm9020411
13. Luo X, Xu Y, Li Y, Zhang G, Huang S, Liu X, et al. BAP1 deletion abrogates growth and metastasis of murine cutaneous melanoma. Melanoma Res. (2021) 31:119–29. doi: 10.1097/CMR.0000000000000714
14. Keung EZ, Gershenwald JE. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: implications for melanoma treatment and care. Expert Rev Anticancer Ther. (2018) 18:775–84. doi: 10.1080/14737140.2018.1489246
15. Griewank KG, Westekemper H, Murali R, Mach M, Schilling B, Wiesner T, et al. Conjunctival melanomas harbor BRAF and NRAS mutations and copy number changes similar to cutaneous and mucosal melanomas. Clin Cancer Res. (2013) 19:3143–52. doi: 10.1158/1078–0432.CCR-13–0163
16. Thielmann CM, Matull J, Roth S, Placke JM, Chorti E, Zaremba A, et al. Genetic and clinical characteristics of ARID1A mutated melanoma reveal high tumor mutational load without implications on patient survival. Cancers (Basel). (2022) 14:2090. doi: 10.3390/cancers14092090
17. Team RC. R: A language and environment for statistical computing. R foundation for statistical computing. (Vienna). (2010).
18. Elder DE, Bastian BC, Cree IA, Massi D, Scolyer RA. The 2018 world health organization classification of cutaneous, mucosal, and uveal melanoma: Detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch Pathol Lab Med. (2020) 144:500–22. doi: 10.5858/arpa.2019-0561-RA
19. Murali R, Wilmott JS, Jakrot V, Al-Ahmadie HA, Wiesner T, McCarthy SW, et al. BAP1 expression in cutaneous melanoma: a pilot study. Pathology. (2013) 45:606–9. doi: 10.1097/PAT.0b013e3283653818
20. Anderson WF, Pfeiffer RM, Tucker MA, Rosenberg PS. Divergent cancer pathways for early-onset and late-onset cutaneous Malignant melanoma. Cancer. (2009) 115:4176–85. doi: 10.1002/cncr.24481
21. McLaughlin CC, Wu XC, Jemal A, Martin HJ, Roche LM, Chen VW. Incidence of noncutaneous melanomas in the U.S. Cancer. (2005) 103:1000–7. doi: 10.1002/cncr.20866
22. Song H, Wang L, Lyu J, Wu Y, Guo W, Ren G. Loss of nuclear BAP1 expression is associated with poor prognosis in oral mucosal melanoma. Oncotarget. (2017) 8:29080–90. doi: 10.18632/oncotarget.16175
23. Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature. (2002) 417:949–54. doi: 10.1038/nature00766
24. Thielmann CM, Chorti E, Matull J, Murali R, Zaremba A, Lodde G, et al. NF1-mutated melanomas reveal distinct clinical characteristics depending on tumour origin and respond favourably to immune checkpoint inhibitors. Eur J Cancer. (2021) 159:113–24. doi: 10.1016/j.ejca.2021.09.035
25. Cirenajwis H, Lauss M, Ekedahl H, Torngren T, Kvist A, Saal LH, et al. NF1-mutated melanoma tumors harbor distinct clinical and biological characteristics. Mol Oncol. (2017) 11:438–51. doi: 10.1002/1878–0261.12050
26. Piris A, Mihm MC Jr., Hoang MP. BAP1 and BRAFV600E expression in benign and Malignant melanocytic proliferations. Hum Pathol. (2015) 46:239–45. doi: 10.1016/j.humpath.2014.10.015
27. Harbour JW, Onken MD, Roberson ED, Duan S, Cao L, Worley LA, et al. Frequent mutation of BAP1 in metastasizing uveal melanomas. Science. (2010) 330:1410–3. doi: 10.1126/science.1194472
28. Ewens KG, Kanetsky PA, Richards-Yutz J, Purrazzella J, Shields CL, Ganguly T, et al. Chromosome 3 status combined with BAP1 and EIF1AX mutation profiles are associated with metastasis in uveal melanoma. Invest Ophthalmol Vis Sci. (2014) 55:5160–7. doi: 10.1167/iovs.14–14550
29. Hirsch TZ, Negulescu A, Gupta B, Caruso S, Noblet B, Couchy G, et al. BAP1 mutations define a homogeneous subgroup of hepatocellular carcinoma with fibrolamellar-like features and activated PKA. J Hepatol. (2020) 72:924–36. doi: 10.1016/j.jhep.2019.12.006
30. Shrestha R, Nabavi N, Lin YY, Mo F, Anderson S, Volik S, et al. BAP1 haploinsufficiency predicts a distinct immunogenic class of Malignant peritoneal mesothelioma. Genome Med. (2019) 11:8. doi: 10.1186/s13073–019-0620–3
31. Ladanyi M, Sanchez Vega F, Zauderer M. Loss of BAP1 as a candidate predictive biomarker for immunotherapy of mesothelioma. Genome Med. (2019) 11:18. doi: 10.1186/s13073–019-0631–0
32. Spencer KR, Wang J, Silk AW, Ganesan S, Kaufman HL, Mehnert JM. Biomarkers for immunotherapy: current developments and challenges. Am Soc Clin Oncol Educ Book. (2016) 35:e493–503. doi: 10.1200/EDBK_160766
33. Koopmans AE, Verdijk RM, Brouwer RW, van den Bosch TP, van den Berg MM, Vaarwater J, et al. Clinical significance of immunohistochemistry for detection of BAP1 mutations in uveal melanoma. Mod Pathol. (2014) 27:1321–30. doi: 10.1038/modpathol.2014.43
34. Heppt MV, Amaral T, Kahler KC, Heinzerling L, Hassel JC, Meissner M, et al. Combined immune checkpoint blockade for metastatic uveal melanoma: a retrospective, multi-center study. J Immunother Cancer. (2019) 7:299. doi: 10.1186/s40425–019-0800–0
35. Rodriguez-Vidal C, Fernandez-Diaz D, Fernandez-Marta B, Lago-Baameiro N, Pardo M, Silva P, et al. Treatment of metastatic uveal melanoma: Systematic review. Cancers (Basel). (2020) 12:2557. doi: 10.3390/cancers12092557
36. Griewank KG, Muller H, Jackett LA, Emberger M, Moller I, van de Nes JA, et al. SF3B1 and BAP1 mutations in blue nevus-like melanoma. Modern pathology: an Off J United States Can Acad Pathology Inc. (2017) 30:928–939. doi: 10.1038/modpathol.2017.23
37. Smit KN, Jager MJ, de Klein A, Kiliҫ E. Uveal melanoma: Towards a molecular understanding. Prog Retin Eye Res. (2020) 75:100800. doi: 10.1016/j.preteyeres.2019.100800
38. Griewank KG, Koelsche C, van de Nes JAP, Schrimpf D, Gessi M, Moller I, et al. Integrated genomic classification of melanocytic tumors of the central nervous system using mutation analysis, copy number alterations, and DNA methylation profiling. Clin Cancer Res. (2018) 24:4494–504. doi: 10.1158/1078–0432.CCR-18–0763
Keywords: BAP1, non-uveal melanoma, uveal melanoma, mutation profiling, immunotherapy
Citation: Matull J, Placke J-M, Lodde G, Zaremba A, Utikal J, Terheyden P, Pföhler C, Herbst R, Kreuter A, Welzel J, Kretz J, Möller I, Sucker A, Paschen A, Livingstone E, Zimmer L, Hadaschik E, Ugurel S, Schadendorf D, Thielmann CM and Griewank KG (2024) Clinical and genetic characteristics of BAP1-mutated non-uveal and uveal melanoma. Front. Immunol. 15:1383125. doi: 10.3389/fimmu.2024.1383125
Received: 06 February 2024; Accepted: 07 May 2024;
Published: 05 June 2024.
Edited by:
Francesco Sabbatino, University of Salerno, ItalyReviewed by:
Mizue Terai, Thomas Jefferson University, United StatesCopyright © 2024 Matull, Placke, Lodde, Zaremba, Utikal, Terheyden, Pföhler, Herbst, Kreuter, Welzel, Kretz, Möller, Sucker, Paschen, Livingstone, Zimmer, Hadaschik, Ugurel, Schadendorf, Thielmann and Griewank. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Klaus Georg Griewank, a2xhdXMuZ3JpZXdhbmtAdWstZXNzZW4uZGU=
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.