
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 23 April 2024
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1379611
 Elisa Chapuis1,2
Elisa Chapuis1,2 Elodie Bousquet3
Elodie Bousquet3 Jean-François Viallard1,4Benjamin Terrier5
Jean-François Viallard1,4Benjamin Terrier5 Zahir Amoura6Veronica Batani7Antoine Brézin8
Zahir Amoura6Veronica Batani7Antoine Brézin8 Patrice Cacoub9
Patrice Cacoub9 Marco Caminati10Thibaud Chazal11Cloé Comarmond12
Marco Caminati10Thibaud Chazal11Cloé Comarmond12 Isabelle Durieu13Mikael Ebbo1,14Maximilien Grall15Emmanuel Ledoult1,16Laura Losappio17
Isabelle Durieu13Mikael Ebbo1,14Maximilien Grall15Emmanuel Ledoult1,16Laura Losappio17 Irene Mattioli18
Irene Mattioli18 Arsène Mékinian19Roberto Padoan20
Arsène Mékinian19Roberto Padoan20 Francesca Regola21Jan Schroeder18Lior Seluk22Ludovic Trefond1,23Michael E. Wechsler22
Francesca Regola21Jan Schroeder18Lior Seluk22Ludovic Trefond1,23Michael E. Wechsler22 Guillaume Lefevre1,24
Guillaume Lefevre1,24 Jean-Emmanuel Kahn1,25
Jean-Emmanuel Kahn1,25 Pascal Sève26
Pascal Sève26 Matthieu Groh1,27* for the French Referral Center for Hypereosinophilic Syndromes (CEREO) and European Eosinophilic Granulomatosis with Polyangiitis Study Group (EESG)
Matthieu Groh1,27* for the French Referral Center for Hypereosinophilic Syndromes (CEREO) and European Eosinophilic Granulomatosis with Polyangiitis Study Group (EESG)Introduction: Eosinophils have widespread procoagulant effects. In daily practice, eosinophil-related cardiovascular toxicity consists of endomyocardial damage, eosinophilic vasculitis and arterial or venous thrombosis. Here we aim to report on the clinical features and treatment outcomes of patients with unexplained ophthalmic vascular manifestations and eosinophilia.
Methods: We conducted a retrospective, multicenter, observational study and a literature review of patients with eosinophilia (≥0.5 x109/L) and concomitant ophthalmic vascular manifestations independent of the underlying eosinophilic disease but with no alternative cause for ophthalmic manifestations.
Results: Fifty-seven patients were included (20 from the observational study and 37 from the literature review). Ophthalmic vascular features were the initial manifestation of eosinophil-related disease in 34 (59%) patients and consisted of 29 central retinal artery occlusions, six branch retinal artery occlusions, five central retinal vein occlusions, two branch retinal vein occlusions, seven retinal vasculitides, two retinal vasospasms, 12 Purtscher’s retinopathies, 13 anterior ischemic optic neuropathies and two posterior ischemic optic neuropathies. The median [IQR] absolute eosinophil count at onset of ophthalmic vascular manifestations was 3.5 [1.7-7.8] x109/L. Underlying eosinophil-related diseases included eosinophilic granulomatosis with polyangiitis (n=32), clonal hypereosinophilic syndrome (HES) (n=1), idiopathic HES (n=13), lymphocytic HES (n=2), adverse drug reactions (n=3), parasitosis (n=2), polyarteritis nodosa (n=1), IgG4-related disease (n=1), eosinophilic fasciitis (n=1) and primary sclerosing cholangitis (n=1). Other extra-ophthalmologic arterial or venous thromboses related to eosinophilia were reported in four (7%) and nine (16%) patients, respectively. Visual prognosis was poor: only eight (10%) patients achieved full recovery of ophthalmologic symptoms. After a median follow-up of 10.5 [1-18] months, one patient (3%) had a recurrence of an ophthalmic vascular manifestation, and three patients (10%) had a recurrence of other vascular symptoms (deep vein thrombosis in two and pulmonary embolism in one patient). At the time of recurrence, absolute eosinophil counts were above 0.5 x109/L in all cases (n=4).
Discussion: This study broadens the spectrum of vascular manifestations associated with hypereosinophilia by adding ophthalmic vascular manifestations. In patients with ophthalmological vascular manifestations and hypereosinophilia, aggressive treatment of the underlying pathology (and normalization of blood count) should be implemented.
Blood and/or tissue eosinophilia is a hallmark feature of multiple allergic, infectious, inflammatory, and neoplastic disorders (1). Eosinophils have widespread effects. These include the production of procoagulant phospholipids and the production of tissue factor and activated factor XII, both of which promote the genesis of thrombin (2–4). Eosinophils also release major basic protein (MBP, which contributes to platelet activation) (5, 6), eosinophilic cationic protein, eosinophil peroxidase and platelet activation factor, all of which foster thrombus formation (7, 8). According to the latest International Cooperative Working Group on Eosinophil Disorders (ICOG-Eo), both venous and/or arterial thromboses occurring in patients with absolute eosinophil counts (AEC) > 1.5 x109/L are Hypereosinophilic Syndrome (HES)-defining features (9).
In daily practice, cardiovascular manifestations related to the toxicity of eosinophils mainly consist of eosinophilic myocarditis, endomyocardial fibrosis, endocardial thrombi (with potential systemic emboli) (10), venous thromboembolism (11), and eosinophilic vasculitis in patients with idiopathic HES (12, 13) Eosinophilia can also be associated with organ and/or life-threatening manifestations e.g., thromboangiitis obliterans-like disease (14, 15), coronary vasospasm (16) or ischemic strokes of border zone distribution (17), all of which can have poor outcomes (18). To date, ophthalmic vascular manifestations (e.g. central retinal artery occlusion (CRAO), Purtscher’s retinopathy, central retinal vein occlusion (CRVO) or ischemic optic neuropathy (ION)) have seldom been reported in the setting of eosinophil-associated disorders, consisting mostly of case reports or small case series (19–22). Hence, the management of such patients is not standardized.
Here, we aim to report on the clinical picture and treatment outcomes of patients with ophthalmic vascular manifestations and eosinophilia, and ultimately to provide a data-driven practical therapeutic algorithm.
We conducted a retrospective, multicenter, observational study. Centers involved in the French National Reference Center for HES (CEREO) and in the European Eosinophilic Granulomatosis with Polyangiitis study group as well as 1 US center of EGPA expertise (National Jewish Health, NJH) were queried to identify patients with: (i) at least one episode of ophthalmic vascular manifestation (CRAO, branch retinal artery occlusion (BRAO), CRVO, branch retinal vein occlusion (BRVO), Purtscher’s retinopathy, retinal vasculitis or ION); (ii) concomitant absolute eosinophilia count (AEC) ≥ 0.5 x109/L when the ophthalmic vascular manifestation occurred. Exclusion criteria were the presence of any condition, comorbidity or concomitant treatment leading to thrombophilia (either constitutional or acquired), cardiac embolism, rhythmic heart disease, tight carotid stenosis (NASCET ≥70%) homolateral to the retinal involvement or other causes of Purtscher’s retinopathy (e.g. acute pancreatitis, head trauma or thrombotic microangiopathy), ION (e.g. giant cell arteritis) as well as the presence of anti-myeloperoxydase (MPO) anti-neutrophil cytoplasmic autoantibodies. A comprehensive list of exclusion criteria is provided in the Supplementary Appendix.
The PUBMED database was searched for English-language publications released up to April 2023, using the following combination of MeSH terms: (i) ‘hypereosinophilic syndrome’ (or any term referring to a condition embedded within the spectrum of clonal, reactive (including lymphocytic HES, drug-induced or paraneoplastic eosinophilia) and idiopathic HES (including single-organ and systemic eosinophil-associated diseases)); (ii) and a MeSH term referring to an ophthalmic vascular manifestation (e.g., retinal artery occlusion, retinal vein occlusion, retinal vasculitis, retinal diseases, optic neuropathy). Reference lists from selected publications were screened for additional relevant studies.
All cases were reviewed by the investigators (EC, MG) considering the entire follow-up. Using a standardized de-identified case report form, demographic (including cardiovascular and venous thromboembolism risk factors), clinical, laboratory and imaging findings at the time of the ophthalmic vascular manifestation as well as during follow-up were collected. For each patient, the underlying process underpinning blood hypereosinophilia was assessed according to the International COoperative study Group on Eosinophil disorders (ICOG-Eo) terminology (9) and thus considered as either clonal (i.e. neoplastic, including FIP1L1::PDGFRA myeloid neoplasm with eosinophilia), reactive (including all conditions that lead to the production of type 2 inflammation-related cytokines and thereby to non-clonal HE), overlapping (when embodied within the spectrum of autoimmune diseases, e.g. MPO ANCA-negative EGPA (23), IgG4-related disease (24), or eosinophilic fasciitis (25)), or idiopathic.
For patients with ≥ 3 months of follow-up, and after exclusion of patients with single-flare eosinophilia (parasitosis and drug-induced eosinophilia), studied outcomes included visual acuity at last follow-up, the recurrence of either ophthalmic or extra-ophthalmologic vascular events, the occurrence of ophthalmic complications (e.g. retinal neovascularization, intravitreal hemorrhage or neovascular glaucoma), and death. Full ophthalmic recovery was defined as the resolution of ophthalmologic symptoms (full correction of visual acuity, visual field normalization, no recurrence of transient monocular blindness). Partial recovery was defined as partial improvement in visual acuity and/or visual field.
Patient characteristics are reported as median [interquartile] ([IQR]) and frequency (percentage) for continuous and categorical variables, respectively. Visual acuity was converted into the log of the minimum angle of resolution (logMAR). Patient subsets were differentiated based on the subtype of vascular manifestation (arterial involvement vs. venous thrombosis vs. Purtscher’s retinopathy). Visual outcomes were compared using the Chi-squared test and continuous variables were compared using the Kruskal Wallis test.
All methods were carried out in accordance with relevant guidelines and regulations (i.e. the Good Clinical Practice protocol, the Declaration of Helsinki principles and the MR004 French legislation regarding observational retrospective studies) and this study was approved by the independent ethics committee of Foch Hospital (IRB00012437, approval number 23-03-04).
One hundred and twenty-three patients were screened through the CEREO, EESG and NJH databases, and 55 case reports (corresponding to 56 patients) treated for eosinophilia and concomitant ophthalmic vascular manifestations were identified through the literature review. Overall, 57 patients fulfilled inclusion criteria (20 from the observational study and 37 from the literature review, Figure 1). Their main characteristics are reported in Table 1. Thirty-two (56%) were male and their median age at ophthalmic manifestation onset was 54 [44-65] years. Thirty-six (58%) had at least one cardiovascular risk factor, three (5%) had a prior history of cardiovascular disease and four (7%) had a prior history of venous thromboembolism. Among the 55 patients with available data, only one (2%) developed ophthalmic vascular involvement despite ongoing treatment with both antiplatelets and anticoagulants.

Figure 1 Flow-chart showing the search strategy and inclusion/exclusion criteria for the study population.
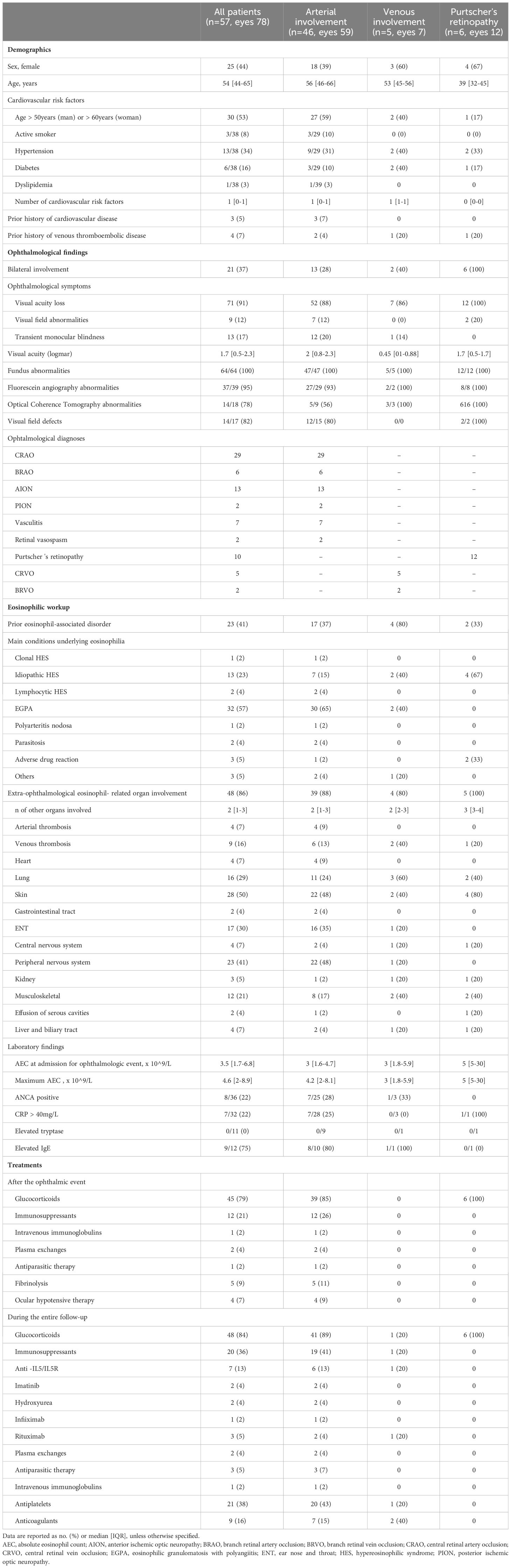
Table 1 Baseline demographic, clinical, biological and treatment features of patients with ophtalmic vascular manifestations and eosinophilia.
Ophthalmologic symptoms were the initial eosinophil-related organ involvement in 34 (59%) patients, while 23 (41%) had already been diagnosed with a prior eosinophil-associated disease, including 17 (30%) who were currently treated with systemic corticosteroids at the time of ophthalmic vascular involvement and four (7%) who had prior eosinophil-related venous thromboembolism. Among the seven patients with available data, the median delay between eosinophil-related first manifestation and ophthalmic symptoms was 36 [15-96] months. The median AEC at onset of ophthalmic vascular manifestation was 3.5 [1.7-6.8] x109/L. Among the 40 patients (70%) with available data, the median peak AEC during follow-up was 4.6 [2-8.9] x109/L, including 37 (92%) patients with hypereosinophilia > 1.5 x109/L (i.e. the HES-defining threshold). Among the 48 patients with extra-ophthalmologic eosinophil-related organ involvement, the median number of organs involved was two [1-3], consisting mostly of peripheral nervous system (n=23), skin (n=28), lung (n=16), ENT (n=17) and musculoskeletal (n=12) manifestations. Of note, four (7%) patients reported features of arterial thrombosis (ischemic stroke n=2, acute coronary syndrome and gastrointestinal tract ischemia, a single patient each), nine (16%) of venous thromboembolism (pulmonary embolism n=4, lower limb deep venous thrombosis n=3, inferior vena cava thrombosis, pulmonary vein thrombosis, a single patient each), and four (7%) had eosinophilic myocarditis. Among the 13 thrombotic manifestations, seven occurred concomitantly with ophthalmic vascular manifestations. Eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg-Strauss syndrome) was the leading cause driving eosinophilia (n=32, 57%). Other associated conditions included STAT5A-associated chronic eosinophilic leukemia (n=1, 2%), lymphocytic (n=2, 4%), idiopathic (n=13, 23%), reactive (n=5, 7% including three drug adverse reactions and two parasitosis) HES as well as overlapping diseases (n=4, 7%, consisting of polyarteritis nodosa, IgG4-related disease, sclerosing cholangitis and eosinophilic fasciitis, a single patient each).
Ocular involvement was bilateral in 21 patients (37%), and in the remaining patients there was no predominant eye involved. Ophthalmic vascular manifestations included CRAO (n= 24 patients, 29 eyes), BRAO (n= 5 patients, 6 eyes), CRVO (n= 3 patients, 5 eyes), BRVO (n= 2 patients, 2 eyes), retinal vasculitis (n= 5 patients, 7 eyes), retinal vasospasm evidenced upon fluorescein angiography (one patient with bilateral involvement), Purtscher’s retinopathy (n=6 patients, 12 eyes), anterior ischemic optic neuropathy (n= 10 patients, 13 eyes) and posterior ischemic optic neuropathy (n=2 patients with unilateral involvement). Ocular symptoms (present in all patients but one) consisted of vision loss (53 patients, 71 eyes), transient monocular blindness (11 patients, 13 eyes) and visual field abnormalities (7 patients, 9 eyes). The median visual acuity at diagnosis was 1.7 [0.5-2.3] logmar. In all eyes with available data (n=64 eyes), fundus examination was always abnormal (fundus data of the 2 patients with posterior ischemic optic neuropathy were not available). Among the 39 fluorescein angiographies that were performed, imaging findings were abnormal and concordant with the clinical diagnoses suspected upon fundus examination in 37 (95%) cases. Figure 2 illustrates the retinal imaging finding of a patient with CRAO in the left eye. Among the 28 patients with imaging of supra-aortic arteries, 8 (29%) had evidence of mild (NASCET < 70%) ipsilateral carotid artery atheroma. Of note, among the 22 patients with available concomitant brain imaging (cerebral MRI or injected TDM), cerebral ischemic events were reported in two (5%) cases.
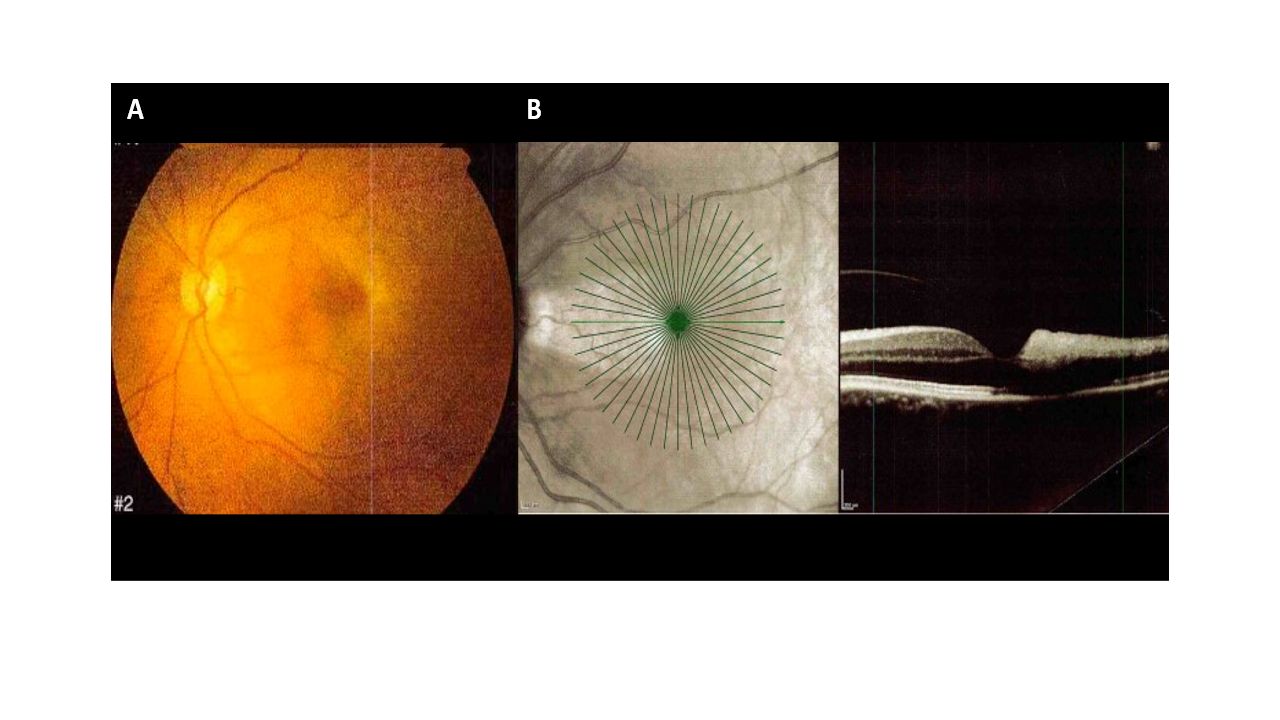
Figure 2 Color fundus photography and spectral domain optical coherence tomography (SD-OCT) of a 43-year-old woman with eosinophilia and central retinal artery occlusion (CRAO) in the left eye. (A) Color fundus photography illustrates a retinal whitening of the posterior pole indicative of a CRAO with preservation of the cilioretinal artery. (B) SD-OCT shows hyperreflectivity in the temporal middle and inner retinal layer hyperreflectivity consistent with CRAO and cilioretinal artery sparing.
At the acute phase, forty-five (79%) patients received systemic corticosteroids (oral corticosteroids, n=23; intravenous corticosteroids n=22; starting doses ranging from 10mg to 1mg/kg/day of prednisone or equivalent before gradual tapering). Twelve (21%) patients received immunosuppressants, including cyclophosphamide (n=8), azathioprine (n=3) and methotrexate (n=1). Fibrinolytic agents and ocular hypotensive therapy were prescribed in five (9%) and four (7%) patients, respectively, while nine (16%) and 21 (38%) patients received long-term anticoagulants or antiplatelets, respectively. Other treatments consisted of antiparasitic drugs (n=1), plasma exchanges (n=2) and intravenous immunoglobulins (n=1).
During follow-up, other treatments included imatinib (n=2), hydroxyurea (n=2) and infliximab (n=1).
Full details of patients' outcomes are provided in Table 2. Among the 50 (88%) patients with available follow-up data (including 30 with more than three months of follow-up), the median follow-up after the initial ophthalmic vascular manifestation was 10.5 [1-18] months. One (3%) patient had a recurrence of ophthalmic vascular manifestation (CRVO) and three (10%) patients had another vascular event (lower limb deep vein thrombosis n=2, pulmonary embolism n=1). In all cases, AEC was above 0.5 x109/L at time of recurrence. At last follow-up, only six patients (12%) achieved full recovery. Sixteen patients (32%) achieved partial recovery, 23 patients (46%) stabilized once under treatment, while the condition of the remaining five patients (10%) worsened despite therapy. By comparison with patients with arterial involvement, the rate of ophthalmic recovery was higher in patients with either Purtscher’s retinopathy or venous involvement (recovery achieved in 8/10 eyes with Purtscher’s retinopathy and in 4/5 eyes with venous involvement vs 18/53 eyes with arterial involvement, p=0.019). Patients with venous involvement or Purtscher’s retinopathy had a better visual acuity at last follow-up than patients with arterial involvement (median logmar 0 [0-0], 1 [0-2.3] and 0.5 [0.2-0.8] for patients with venous, arterial involvement and Purtscher’s retinopathy respectively; p= 0.038). Of note, the levels of baseline absolute eosinophil counts did not correlate with long-term visual outcomes, and there were no significant differences regarding the final visual acuities of patients who received antiplatelets vs. anticoagulants as well as in patients who received only corticosteroids vs. those who received both corticosteroids and immunosuppressants (data not shown).
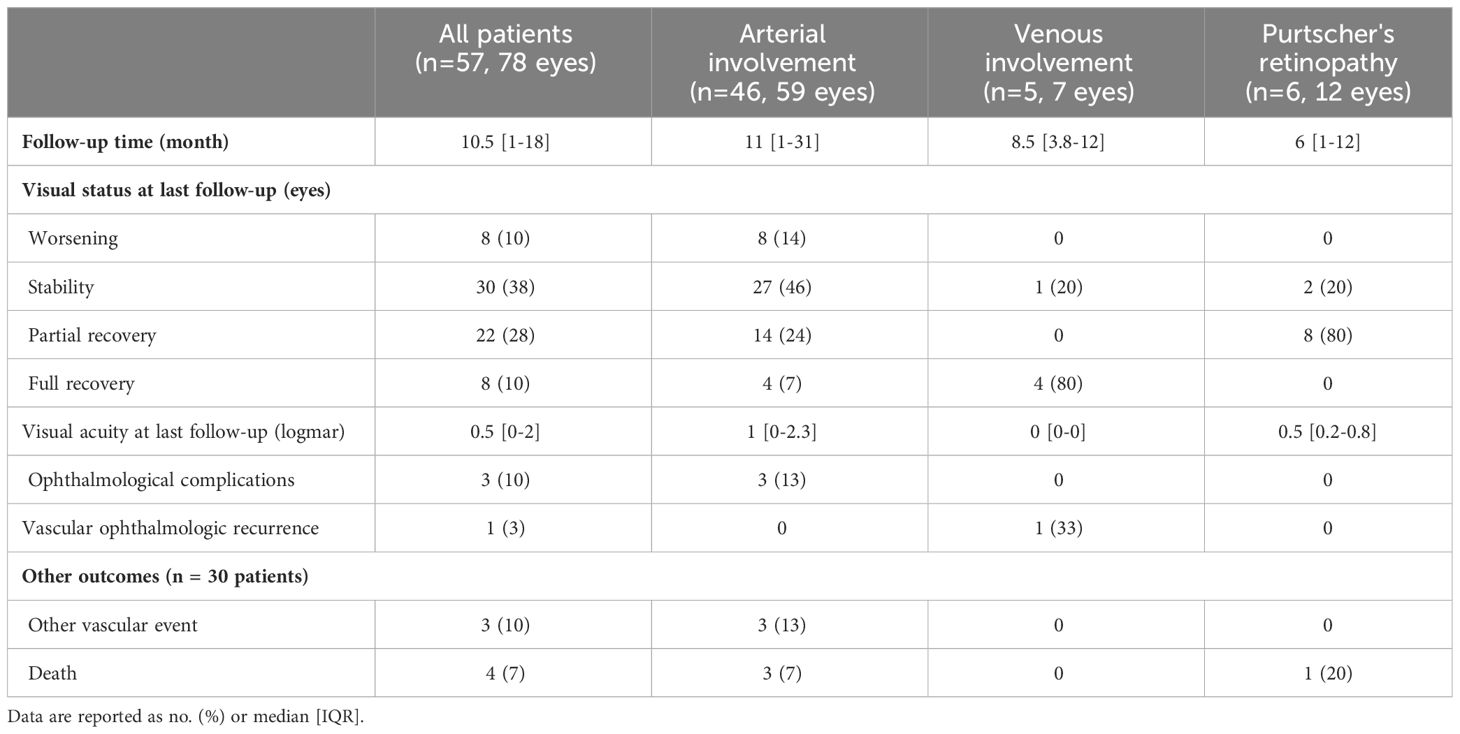
Table 2 Outcomes of patients with ophthalmic vascular manifestations and eosinophilia.
Three (10%) patients developed retinal neovascularization with subsequent intravitreal hemorrhage during follow-up. During follow-up, four patients died of pulmonary infection, MRSA-induced septic shock, endomyocardial fibrosis and hepatitis (a single patient each). Both patients who died of sepsis were treated by systemic corticosteroids (in addition to methotrexate or mepolizumab, a single patient each).
Thirty-two (57%) patients fulfilled MIRRA and/or ACR criteria for EGPA (all without MPO-ANCA). In the latter patients, ophthalmic vascular manifestations consisted of CRAO (17 patients, 21 eyes), BRAO (a single patient with unilateral involvement), AION (8 patients, 11 eyes), PION (a single patient with unilateral involvement), retinal vasculitis (3 patients, 4 eyes), CRVO (a single patient with bilateral involvement) and BRVO (a single patient with unilateral involvement). It was noteworthy that no patient with EGPA had Purtscher’s retinopathy. Extra-ophthalmic vascular manifestations included both eosinophilic-driven (e.g. eosinophilc myocarditis or central nervous system involvement, a single patient each) and vasculitic (e.g. mononeuritis multiplex n=18 patients and purpura, n=12 patients) manifestations. Among the 19 patients with available data, only five (26%) had mild elevation of C-reactive protein (CRP) levels (<40mg/L).
The visual prognosis of EGPA patients was poor and the median final visual acuity was 2 [0.1-2.4] logmar. Among the fourteen patients with at least three months of follow-up, only one patient recovered completely and three achieved partial recovery, whereas two patients worsened and eight had a stability of their visual acuity. Moreover, three patients (21%) had a new vascular event during follow-up (lower limb deep vein thrombosis, n=2; pulmonary embolism, n=1). None of the 32 EGPA patients died during follow-up.
Recent advances have led to the better understanding of the mechanisms driving the pro-coagulant effects of eosinophils (26), and reported cases of arterial and venous thrombotic manifestations related to eosinophilia have increased (11, 15–17, 19). Likewise, the spectrum of eosinophilia-related cardiovascular toxicity has now broadened beyond the scope of eosinophilic cardiomyopathy (10). Some studies have recently highlighted peculiar phenotypes e.g., thromboangiitis obliterans-like disease (14), eosinophilia-associated coronary vasospasm (16) or ischemic strokes of border zone distribution (17). Here, we shed further light on the diversity of eosinophil-induced vascular symptoms and report on various ophthalmic vascular manifestations occurring within the full-spectrum of eosinophil-related diseases, either as first disease manifestation or during follow-up.
Intracardiac thrombus and peripheral arterial emboli were the main features reported in the review of HES-related cardiovascular manifestations reported by Ogbogu et al (10). Likewise, in the main series of patients with HES, ophthalmic vascular manifestations have rarely been reported (19, 27, 28), and mostly consist of case reports or small case series (20–22). In their 2019 review of 189 patients with idiopathic eosinophilic vasculitis, Lefevre et al. reported on only one case of CRAO and one case of retinal vasculitis (12). Among 151 patients with FIP1L1::PDGFRA-related HES, only one case of CRAO was reported (19) and in another series of 26 patients with CD3-CD4+ lymphocytic HES, none presented with ophthalmic symptoms (27). Dupilumab-induced Purtscher’s retinopathy with eosinophilia reported herein is in line with dupilumab-induced eosinophilic vasculitis that our group has previously reported (29). EGPA is the only eosinophil-associated disease for which ophthalmic vascular manifestations have been more extensively depicted, with predominant arterial involvement and poor visual prognosis despite treatment with corticosteroids (30, 31).
Here, we report on a wide variety of ophthalmic vascular manifestations related to eosinophil-associated disorders, that clustered into three main clinical pictures (i.e. arterial or venous retinal occlusions and Purtscher’s retinopathy), with one in three patients having bilateral involvement. There was no clear correlation between the clinical picture and underlying eosinophil-related diseases, supporting the fact that eosinophilia, whatever its cause, can lead to ophthalmologic vascular toxicity. Nevertheless, both clonal and lymphocytic HES were rare (one and two patients respectively), and EGPA was never reported in the setting of Purtscher’s retinopathy. Strikingly, other (and most often concomitant) extra-ophthalmologic vascular manifestations related to eosinophilia were reported in up to 15% of patients, including organ or life-threatening events e.g., ischemic strokes, acute coronary syndrome, gastrointestinal tract ischemia, or inferior vena cava thrombosis. Although skin, lung and gastrointestinal symptoms are the most frequent manifestations of HES, the latter is a multifaceted disease and some patients have prominent vascular manifestations, including catastrophic antiphospholipid syndrome-like presentation (11). As expected (32–35), the visual prognosis was poor (with only six patients achieving full recovery and significant loss of visual acuity at last follow-up), especially in patients with ION or CRAO.
In this series, patients had few cardiovascular risk factors and no major risk factor for venous thromboembolism, suggesting that their ophthalmic manifestations indeed were the consequence of eosinophil-related toxicity. There is strong evidence substantiating the procoagulant effects of eosinophils and their direct toxicity on the vascular endothelium. First, injury-induced venous thrombosis is drastically reduced in both eosinophil-deficient and eosinophil-depleted mice (2). Moreover, eosinophils are potent producers of tissue factor (2–4), can produce procoagulant phospholipids and activate factor XII, which both stimulate the intrinsic coagulation pathway (2). Eosinophils also release major basic protein (MBP), a cationic protein that binds to thrombomodulin and thereby impairs its anticoagulant effects (5, 6). Likewise, the discharge of cytotoxic granules and pro-inflammatory mediators increases vascular permeability and induce endothelial damage, both of which contribute to a procoagulant state (26). Eosinophil extracellular DNA traps also promote platelet activation (36, 37). Lastly, since EGPA accounted for more than half of underlying eosinophil-related diseases, it is likely that underlying vasculitis also contributes to the clinical picture. Nevertheless, patients tested positive for MPO-ANCA were excluded from the study, and only a minority of patients had histologic evidence (or strong clinical surrogates) of vasculitis. Moreover, inflammatory markers tended to be low, suggesting a direct pathogenic role of eosinophils rather than systemic vasculitis (12).
As eosinophils seem to have a prominent role in the genesis of ophthalmic vascular manifestations, prompt initiation of eosinophil-targeted treatments is advisable to curb the deleterious pathophysiological process and to prevent the advent of other manifestations related to eosinophilia-related vascular toxicity. Corticosteroids are the cornerstone of the management of most eosinophilia-associated diseases (38–40). Here, 84% of patients received corticosteroids, which are rapidly effective in most cases (91%) except in a very limited number of well-defined conditions, including drug-hypersensitivity, clonal HES, and paraneoplastic eosinophilia (18). The use of corticosteroids has also seldom been reported in Purtscher’s retinopathy or CRVO, as evidence is lacking (33, 35). Although more than one third of patients received immunosuppressants, it should be emphasized that, in both HES and EGPA, there is no evidence that the adjunction of either cytotoxic drugs or anti-interleukin 5 biologics to corticosteroids is superior to corticosteroids alone at the acute phase (38, 40). Nevertheless, as mepolizumab has demonstrated clinical efficacy and substantial steroid-sparing effect in both EGPA and HES, it is likely that such treatment is beneficial on the long run in patients with high dose steroid dependency and/or steroid-related side effects (41–43).
CRAO presents a significant challenge in ophthalmology, as it often leads to irreversible retinal damage within four hours of the retinal artery occlusion. Unfortunately, there is currently no established treatment or evidence-based therapy available for non-arteritic CRAO. Numerous approaches have been attempted with the goal of dislodging emboli and enhancing retinal blood flow through various procedures, such as ocular massage, intraocular pressure reduction, isovolemic hemodilution, anticoagulation, and intraarterial fibrinolysis. These interventions have yielded poor visual outcomes (44, 45). Conversely, a strict management of cardiovascular risk factors is encouraged to manage CRVO (41), and there is no standard of treatment for Purtscher’s retinopathy (35). Overall, both anticoagulants (at the acute phase) and antiplatelets (on the long run) were also frequently prescribed. As the only recurrence of ophthalmic vascular manifestation occurred in a patient with persistent eosinophilia, long-term normalization of AEC (thanks to treatment of the underlying condition) is advisable and is likely to prevent the recurrence of vascular manifestations. Of note is that in venous thromboembolism related to eosinophilia, we have previously demonstrated that anticoagulants could be safely withdrawn once complete hematological response was obtained in the long run. A suggested algorithm for the management of eosinophil-associated vascular ophthalmic involvement is provided in Figure 3.

Figure 3 Suggested algorithm for the management of eosinophil-related ophthalmic vascular manifestations. HE, hypereosinophilia; CRAO, central retinal artery occlusion; BRAO, branch retinal artery occlusion; AION, anterior ischemic optic neuropathy; PION, posterior ischemic optic neuropathy; CRVO, central retinal vein occlusion; BRVO, branch retinal vein occlusion; GCA, giant cell arteritis.
This study has several drawbacks, including missing data and lack of standardized management within centers. Next, little follow-up data was available from the cases retrieved from the literature review, which possibly led to an underestimation of the risk of recurrence. Lastly, given the retrospective design of the study, we were unable to assess whether, besides AEC, other biological parameters (including markers of eosinophil activation and degranulation) could also correlate with outcomes.
Regardless of these limitations, this study – the first longitudinal analysis dedicated to ophthalmic vascular manifestations occurring during eosinophil-related diseases – emphasizes the fact that eosinophilia (whatever the underlying disease) can lead to ophthalmic vascular toxicity. It provides useful data for both ophthalmologists and physicians involved in the field of eosinophil-related disorders and suggests that, in a subset of patients with otherwise unexplained ophthalmic vascular manifestation and eosinophilia, long-term normalization of AEC is advisable to prevent the recurrence of vascular manifestations. Further large-scale studies are needed to confirm these preliminary findings, and collaborative endeavors are welcome.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by independent ethics committee of Foch Hospital (IRB00012437, approval number 23-03-04). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
EC: Formal analysis, Investigation, Writing – original draft, Writing – review & editing, Conceptualization, Methodology. EB: Writing – review & editing, Conceptualization, Data curation, Investigation. JV: Data curation, Writing – review & editing. BT: Data curation, Writing – review & editing. ZA: Data curation, Writing – review & editing. VB: Data curation, Writing – review & editing. AB: Data curation, Writing – review & editing. PC: Visualization, Writing – review & editing, Data curation. MC: Data curation, Writing – review & editing, Validation. TC: Writing – review & editing. CC: Writing – review & editing. ID: Data curation, Writing – review & editing. ME: Data curation, Writing – review & editing. MGra: Data curation, Writing – review & editing. EL: Data curation, Writing – review & editing. LL: Data curation, Writing – review & editing. IM: Data curation, Writing – review & editing. AM: Data curation, Writing – review & editing. RP: Data curation, Writing – review & editing. FR: Data curation, Writing – review & editing. JS: Data curation, Writing – review & editing. LS: Data curation, Writing – review & editing. LT: Data curation, Writing – review & editing. MW: Data curation, Writing – review & editing. GL: Data curation, Writing – review & editing. JK: Data curation, Writing – review & editing. PS: Data curation, Writing – review & editing. MGro: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AVM declared a shared parent affiliation with the author LL to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1379611/full#supplementary-material
1. Groh M, Lefèvre G, Ackermann F, Étienne N, Kahn J-E. [Hypereosinophilic syndromes]. Rev Prat. (2019) 69:767–73.
2. Uderhardt S, Ackermann JA, Fillep T, Hammond VJ, Willeit J, Santer P, et al. Enzymatic lipid oxidation by eosinophils propagates coagulation, hemostasis, and thrombotic disease. J Exp Med. (2017) 214:2121–38. doi: 10.1084/jem.20161070
3. Cugno M, Marzano AV, Lorini M, Carbonelli V, Tedeschi A. Enhanced tissue factor expression by blood eosinophils from patients with hypereosinophilia: A possible link with thrombosis. PloS One. (2014) 9:e111862. doi: 10.1371/journal.pone.0111862
4. Moosbauer C, Morgenstern E, Cuvelier SL, Manukyan D, Bidzhekov K, Albrecht S, et al. Eosinophils are a major intravascular location for tissue factor storage and exposure. Blood. (2006) 109:995–1002. doi: 10.1182/blood-2006-02-004945
5. Mukai HY, Ninomiya H, Ohtani K, Nagasawa T, Abe T. Major basic protein binding to thrombomodulin potentially contributes to the thrombosis in patients with eosinophilia. Br J Hematol. (1995) 90:892–9. doi: 10.1111/j.1365-2141.1995.tb05211.x
6. Slungaard A, Vercellotti GM, Tran T, Gleich GJ, Key NS. Eosinophil cationic granule proteins impair thrombomodulin function. A potential mechanism for thromboembolism in hypereosinophilic heart disease. J Clin Invest. (1993) 91:1721–30. doi: 10.1172/JCI116382
7. Rohrbach M, Wheatley C, Slifman N, Gleich G. Activation of platelets by eosinophil granule proteins. J Exp Med. (1990) 172:1271–4. doi: 10.1084/jem.172.4.1271
8. Ojima-Uchiyama A, Masuzawa Y, Sugiura T, Waku K, Fukuda T, Makino S. Production of platelet-activating factor by human normodense and hypodense eosinophils. Lipids. (1991) 26:1200–3. doi: 10.1007/BF02536531
9. Valent P, Klion AD, Roufosse F, Simon D, Metzgeroth G, Leiferman KM, et al. Proposed refined diagnostic criteria and classification of eosinophil disorders and related syndromes. Allergy. (2023) 78:47–59. doi: 10.1111/all.15544
10. Ogbogu P, Rosing DR, Horne MK. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol Allergy Clin North Am. (2007) 27:457–75. doi: 10.1016/j.iac.2007.07.001
11. Réau V, Vallée A, Terrier B, Plessier A, Abisror N, Ackermann F, et al. Venous thrombosis and predictors of relapse in eosinophil-related diseases. Sci Rep. (2021) 11:6388. doi: 10.1038/s41598-021-85852-9
12. Lefèvre G, Leurs A, Gibier J-B, Copin M-C, Staumont-Sallé D, Dezoteux F, et al. “Idiopathic eosinophilic vasculitis”: another side of hypereosinophilic syndrome? A comprehensive analysis of 117 cases in asthma-free patients. J Allergy Clin Immunol: In Pract. (2020) 8:1329–1340.e3. doi: 10.1016/j.jaip.2019.12.011
13. Maronese CA, Derlino F, Moltrasio C, Cattaneo D, Iurlo A, Marzano AV. Neutrophilic and eosinophilic dermatoses associated with hematological Malignancy. Front Med (Lausanne). (2024) 10:1324258. doi: 10.3389/fmed.2023.1324258
14. Rohmer J, Groh M, Samson M, London J, Jachiet M, Rouzaud D, et al. Distal ischemia as the initial presentation of hypereosinophilic syndrome-related arterial involvement: A case study and literature review. Autoimmun Rev. (2019) 18:828–30. doi: 10.1016/j.autrev.2019.06.004
15. Johnston AM, Woodcock BE. Acute aortic thrombosis despite anticoagulant therapy in idiopathic hypereosinophilic syndrome. J R Soc Med. (1998) 91:492–3. doi: 10.1177/014107689809100912
16. Groh M, Pineton de Chambrun M, Georges J-L, Panel K, Lefèvre G, Kahn J-E, et al. Recurrent cardiac arrest due to eosinophilia-related coronary vasospasm successfully treated by benralizumab. J Allergy Clin Immunol: In Pract. (2021) 9:3497–3499.e1. doi: 10.1016/j.jaip.2021.04.067
17. Tennenbaum J, Groh M, Venditti L, Campos-Gazeau F, Chalayer E, De Broucker T, et al. FIP1L1-PDGFRA-associated hypereosinophilic syndrome as a treatable cause of watershed infarction. Stroke. (2021) 52(10):e605–9. doi: 10.1161/STROKEAHA.121.034191
18. Gaillet A, Bay P, Péju E, Ait-Oufella H, Azoulay E, Benchabane N, et al. Epidemiology, clinical presentation, and outcomes of 620 patients with eosinophilia in the intensive care unit. Intensive Care Med. (2023) 49:291–301. doi: 10.1007/s00134-022-06967-9
19. Rohmer J, Couteau-Chardon A, Trichereau J, Panel K, Gesquiere C, Ben Abdelali R, et al. Epidemiology, clinical picture and long-term outcomes of FIP1L1-PDGFRA-positive myeloid neoplasm with eosinophilia: Data from 151 patients. Am J Hematol. (2020) 95:1314–23. doi: 10.1002/ajh.25945
20. Chaine G, Davies J, Kohner EM, Hawarth S, Spry CJF. Ophthalmologic abnormalities in the hypereosinophilic syndrome. Ophthalmology. (1982) 89:1348–56. doi: 10.1016/S0161-6420(82)34625-4
21. Gupta OP, Zegere E, Maguire JI. Purtscher-like retinopathy associated with primary hypereosinophilic syndrome. Retin cases Brief Rep. (2009) 3:193–6. doi: 10.1097/ICB.0b013e318162b14d
22. Farcet JP, Binaghi M, Kuentz M, Merlier JF, Mayaud C, Nebout T, et al. A hypereosinophilic syndrome with retinal arteritis and tuberculosis. Arch Internal Med. (1982) 142:625–7. doi: 10.1001/archinte.1982.00340160205034
23. Grayson PC, Ponte C, Suppiah R, Robson JC, Craven A, Judge A, et al. 2022 American College of Rheumatology/European alliance of associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Arthritis Rheumatol. (2022) 74:386–92. doi: 10.1002/art.41982
24. Umehara H, Okazaki K, Kawa S, Takahashi H, Goto H, Matsui S, et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. (2021) 31:529–33. doi: 10.1080/14397595.2020.1859710
25. Jinnin M, Yamamoto T, Asano Y, Ishikawa O, Sato S, Takehara K, et al. Diagnostic criteria, severity classification and guidelines of eosinophilic fasciitis. J Dermatol. (2018) 45:881–90. doi: 10.1111/1346-8138.14160
26. Khoury P, Grayson PC, Klion AD. Eosinophils in vasculitis: characteristics and roles in pathogenesis. Nat Rev Rheumatol. (2014) 10:474–83. doi: 10.1038/nrrheum.2014.98
27. Carpentier C, Verbanck S, Schandené L, Heimann P, Trépant A-L, Cogan E, et al. Eosinophilia associated with CD3–CD4+ T cells: characterization and outcome of a single-center cohort of 26 patients. Front Immunol. (2020) 11:1765. doi: 10.3389/fimmu.2020.01765
28. Ogbogu PU, Bochner BS, Butterfield JH, Gleich GJ, Huss-Marp J, Kahn JE, et al. Hypereosinophilic syndromes: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol. (2009) 124:1319–25.e3. doi: 10.1016/j.jaci.2009.09.022
29. Descamps V, Deschamps L, El Khalifa J, Groh M, Gibier J-B, Lefèvre G, et al. Eosinophilic vasculitis associated with persistent dupilumab-induced hypereosinophilia in severe asthma. Respir Med Res. (2021) 79:100821. doi: 10.1016/j.resmer.2021.100821
30. Takanashi T, Uchida S, Arita M, Okada M, Kashii S. Orbital inflammatory pseudotumor and ischemic vasculitis in Churg-Strauss syndrome: Report of two cases and review of the literature11The authors have no proprietary interest in any aspect of this study. Ophthalmology. (2001) 108:1129–33. doi: 10.1016/S0161-6420(01)00557-7
31. Akella SS, Schlachter DM, Black EH, Barmettler A. Ophthalmic eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome): A systematic review of the literature. Ophthalmic Plast Reconstruct Surg. (2019) 35:7. doi: 10.1097/IOP.0000000000001202
32. Madike R, Cugati S, Chen C. A review of the management of central retinal artery occlusion. Taiwan J Ophthalmol. (2022) 12:273–81. doi: 10.4103/2211-5056.353126
33. Blair K, Czyz CN. Central retinal vein occlusion. In: StatPearls. Treasure Island, Florida, United States of America: StatPearls Publishing (2023).
34. Luneau K, Newman NJ, Biousse V. Ischemic optic neuropathies. Neurologist. (2008) 14:341–54. doi: 10.1097/NRL.0b013e318177394b
35. Tripathy K, Patel BC. Purtscher retinopathy. In: StatPearls. Treasure Island, Florida, United States of America: StatPearls Publishing (2023).
36. Marx C, Novotny J, Salbeck D, Zellner KR, Nicolai L, Pekayvaz K, et al. Eosinophil-platelet interactions promote atherosclerosis and stabilize thrombosis with eosinophil extracellular traps. Blood. (2019) 134:1859–72. doi: 10.1182/blood.2019000518
37. Ueki S, Melo RCN, Ghiran I, Spencer LA, Dvorak AM, Weller PF. Eosinophil extracellular DNA trap cell death mediates lytic release of free secretion-competent eosinophil granules in humans. Blood. (2013) 121:2074–83. doi: 10.1182/blood-2012-05-432088
38. Groh M, Rohmer J, Etienne N, Abou Chahla W, Baudet A, Chan Hew Wai A, et al. French guidelines for the etiological workup of eosinophilia and the management of hypereosinophilic syndromes. Orphanet J Rare Dis. (2023) 18:100. doi: 10.1186/s13023-023-02696-4
39. Klion AD. How I treat hypereosinophilic syndromes. Blood. (2015) 126:1069–77. doi: 10.1182/blood-2014-11-551614
40. Emmi G, Bettiol A, Gelain E, Bajema IM, Berti A, Burns S, et al. Evidence-Based Guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev. Rheumatol. (2023) 19:378–93. doi: 10.1038/s41584-023-00958-w
41. Nicholson L, Talks SJ, Amoaku W, Talks K, Sivaprasad S. Retinal vein occlusion (RVO) guideline: executive summary. Eye (Lond). (2022) 36:909–12. doi: 10.1038/s41433-022-02007-4
42. Howard RC, Welch MN, Hager AC, Zumbro DS. Purtscher-like retinopathy and primary hypereosinophilic syndrome association. Retin cases Brief Rep. (2012) 6:273–7. doi: 10.1097/ICB.0b013e318228e32b
43. Fong A, Ahmed S, Ramalingam S, Brown RM, Harper L, Mollan SP. Eosinophilic granulomatosis with polyangiitis presenting as unilateral acute anterior ischemic optic neuropathy. Neuroophthalmology. (2021) 45:109–16. doi: 10.1080/01658107.2020.1761402
44. Schumacher M, Schmidt D, Jurklies B, Gall C, Wanke I, Schmoor C, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. (2010) 117:1367–1375.e1. doi: 10.1016/j.ophtha.2010.03.061
Keywords: eosinophilia, hypereosinophilic syndrome, eosinophilic granulomatosis with polyangiitis, retinal artery occlusion, retinal vein occlusion, retinal vasculitis, optic neuropathy
Citation: Chapuis E, Bousquet E, Viallard J-F, Terrier B, Amoura Z, Batani V, Brézin A, Cacoub P, Caminati M, Chazal T, Comarmond C, Durieu I, Ebbo M, Grall M, Ledoult E, Losappio L, Mattioli I, Mékinian A, Padoan R, Regola F, Schroeder J, Seluk L, Trefond L, Wechsler ME, Lefevre G, Kahn J-E, Sève P and Groh M (2024) Ophthalmic vascular manifestations in eosinophil-associated diseases: a comprehensive analysis of 57 patients from the CEREO and EESG networks and a literature review. Front. Immunol. 15:1379611. doi: 10.3389/fimmu.2024.1379611
Received: 31 January 2024; Accepted: 04 April 2024;
Published: 23 April 2024.
Edited by:
Chris Wincup, King’s College Hospital NHS Foundation Trust, United KingdomReviewed by:
Shinji Izuka, The University of Tokyo, JapanCopyright © 2024 Chapuis, Bousquet, Viallard, Terrier, Amoura, Batani, Brézin, Cacoub, Caminati, Chazal, Comarmond, Durieu, Ebbo, Grall, Ledoult, Losappio, Mattioli, Mékinian, Padoan, Regola, Schroeder, Seluk, Trefond, Wechsler, Lefevre, Kahn, Sève and Groh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthieu Groh, bS5ncm9oQGhvcGl0YWwtZm9jaC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.