 Cláudia Chaves1
Cláudia Chaves1 Renata Puppin Zandonadi2
Renata Puppin Zandonadi2 António Raposo3*
António Raposo3* Eduardo Yoshio Nakano4
Eduardo Yoshio Nakano4 Fernando Ramos5,6
Fernando Ramos5,6 Priscila Farage7
Priscila Farage7 Edite Teixeira-Lemos8*
Edite Teixeira-Lemos8*- 1ESSV, Centre for Studies in Education and Innovation (CI&DEI), Polytechnic University of Viseu, Viseu, Portugal
- 2Faculty of Health Sciences, Nutrition Department, University of Brasília, Brasília, Brazil
- 3CBIOS (Research Center for Biosciences and Health Technologies), Universidade Lusófona de Humanidades e Tecnologias, Lisboa, Portugal
- 4Department of Statistics, University of Brasília, Brasília, Brazil
- 5Faculty of Pharmacy, University of Coimbra, Coimbra, Portugal
- 6Associated Laboratory for Green Chemistry (LAQV) of the Network of Chemistry and Technology (REQUIMTE), Porto, Portugal
- 7Faculty of Nutrition, Federal University of Goiás, Goiânia, Brazil
- 8CERNAS Research Centre, Polytechnic University of Viseu, Viseu, Portugal
Objective: This study aimed to compare the 36-Item Short Form Survey Instrument version 2 (SF-36-v2) (generic) and Celiac Disease Questionnaire (CDQ) (specific) questionnaires used to evaluate the quality of life (QoL) in celiac Portuguese adult individuals.
Methods: This cross-sectional study used non-probabilistic sampling based on Portuguese celiac patients who accessed the online survey in 2022. The online data collection used a self-reported instrument composed of three parts: (i) socioeconomic, health, and gluten-free diet (GFD) adherence questions; (ii) SF-36 v2 – Portuguese version (generic questionnaire) and (iii) Celiac Disease Questionnaire (CDQ) (specific questionnaire).
Results: A total of 234 individuals who accessed the survey completed the questionnaire. Seven of the eight SF-36 domains positively correlated to the specific questionnaire CDQ. The “General Health” domain (domain 4) showed a negative correlation with the CDQ. Differences in content between the two instruments might be able to explain this finding since the CDQ explores issues regarding the specificities of celiac disease (CD) and the lifelong GFD burden. About half of the sample from this study displayed poor diet adherence, it is possible that the SF-36 could not reflect the impact of CD treatment - the complete elimination of gluten from the diet - on patients’ health. Therefore, this issue should be carefully evaluated in future research.
Conclusion: Specific validated questionnaires for CD individuals, such as the CDQ, contemplate social, economic, and clinical variables that permeate the patient’s life context. Therefore, these instruments may be more suitable for evaluating QoL in this public. However, using a general questionnaire such as the SF-36 would be indicated for comparing QOL between celiac patients and the general population or even between CD and other disease individuals. In this case, we recommend assessing GFD compliance for control parallelly.
1 Introduction
For Celiac disease (CD) is a permanent autoimmune disorder triggered by gluten ingestion by genetically predisposed individuals, affecting approximately 1% of the worldwide population (1, 2). CD is considered a public health problem and may cause malabsorption, leading to nutritional deficiencies, liver and bone diseases, gastrointestinal symptoms, growth deficiency, or several other consequences (1, 3, 4).
Until now, the only safe treatment for CD is a life-long gluten-free diet (GFD) (1, 3) and usually, GFD compliance improves the quality of life (QoL) in most of CD patients due to symptom remission, nutritional deficiencies and other CD-related health consequences avoidance, and mortality reduction. However, multiple factors influence GFD compliance, such as acceptance, access, availability, and cost of gluten-free products; dietary restrictions; socialization difficulties; and economic burden, among others, potentially negatively impacting CD QoL (5–9). In this sense, CD is considered a chronic condition that affects patients’ QoL as other chronic diseases (5–8) and, to achieve optimal health, it is essential to understand the individual’s perception of QoL (10). In chronic conditions, it is crucial to evaluate the impact of patients’ health conditions on their ability to live a fulfilling life and promote public policies to minimize the physical, emotional, and social burden on the patient (11, 12).
Studies have explored CD patients’ QoL perceptions using generic and specific questionnaires developed for celiac patients (13–22). The use of a specific questionnaire is important to comprehend aspects related to the celiacs’ QoL, mental health, well-being, and the economic and social aspects caused by this chronic condition and their lifelong dietary and lifestyle changes (11, 23). However, the use of a general questionnaire such as Short Form-36 (SF-36) may allow comparison among individuals with different chronic diseases or healthy individuals (24–27). The SF-36 is a widely recognized questionnaire designed to assess an individual’s health-related quality of life and functional abilities and is highly used as a generic instrument in gastroenterology (13, 28–30). Comprising 36 items that explore eight different aspects of QoL, it offers a detailed evaluation of physical functioning, limitations in daily activities due to physical health issues, pain levels, overall health perception, energy levels, social functioning, limitations in activities due to emotional problems, and mental health.
Considering the specific questionnaires to measure CD patients’ QoL, the Celiac Disease Questionnaire (CDQ) is broadly applied (11, 23) that used SF-36 in its validation process (13). CDQ was developed, validated and applied in Germany (2006) and later, it was translated and applied in several European and Extra-European countries (5, 6, 15, 23, 31–43). In Portugal, a study translated and validated the CDQ into Portuguese (41) and our previous study evaluated the quality of life (QoL) perception among Portuguese celiac patients using this Portuguese version of CDQ (42). Furthermore, a separate study conducted in Portugal utilized the general questionnaire SF-36 to assess the perception of QoL in a sample of 195 Portuguese celiacs regarding compliance with a gluten-free diet (GFD) (44). However, no study has compared a generic (SF-36) and a specific (CDQ) questionnaire to evaluate the perception of QoL among Portuguese celiac patients.
Therefore, this study aimed to compare the SF-36 v2 (generic) and CDQ (specific) questionnaires used to evaluate the QoL in celiac Portuguese adult individuals. The study is justified by the need to understand the differences between specific and generic questionnaires and how they could impact the evaluation of QoL in CD.
2 Materials and methods
2.1 Study design and instruments
This cross-sectional study used non-probabilistic sampling based on Portuguese celiac patients who accessed the online survey in 2022. The online data collection method was chosen due to the pandemic caused by SARS-CoV-2, making it impossible to use face-to-face interviews. In addition, it is considered a productive and cheap method to enroll participants and reach a more extensive sample (45, 46). The instrument was composed of 3 parts: (i) socioeconomic, health and GFD adherence questions; (ii) the SF-36 v2– Portuguese version (generic questionnaire) and (iii) CDQ (specific questionnaire) (5). The CDQ is a specific questionnaire to evaluate CD patients’ QoL. It was developed by Häuser et al. (5) and validated in Portugal by Lobão et al. (41). This questionnaire comprises 28 items divided into 4 domains (emotions, gastrointestinal symptoms, concerns, and social) evaluated by 7-point scale (from “1” - worst QoL perception to “7” - best QoL perception). The QoL general instrument used was the SF-36 v2 Portuguese version, validated in Portugal. It is an adaptation of the SF-36, which generates a physical component summary (PCS) and a mental one (MCS). This questionnaire has 36 items divided into 8 domains (1. Physical functioning, 2. Role limitations due to physical health, 3. Pain, 4. General Health, 5. Energy/fatigue, 6. Social functioning, 7. Role limitations due to emotional problems, 8. Emotional well-being) (47). It is a widely used generic, coherent, and easily administered QoL questionnaire.
We also collected sociodemographic characteristics (gender, age, marital status, educational level) and clinical variables (age at CD diagnosis, GFD compliance, use of antidepressants). The GDF compliance was self-reported since we do not have a validated instrument to evaluate GFD compliance in Portugal. Considering data collection occurred during the COVID-19 pandemic, it was not possible to validate a new instrument to evaluate it since the laboratory tests were limited. Therefore, we opt to use self-reported GFD compliance, as performed in other studies (34, 39, 48–52). Participants chose the option that best characterized their current diet regarding the question: “Do you follow a gluten-free diet?”. The response options were: 1) Never; 2) Rarely; 3) Sometimes; 4) Almost always (most of the time); 5) Always. Strict GDF compliance was considered for those who self-reported always adhering to a GFD whereas all others considered “gluten-exposed”. All the participants filled out both questionnaires.
2.2 Participants and ethics
The online instrument was inserted in the SurveyMonkey® online platform. Individuals were invited to participate in the study by the Portuguese Celiac Association (Associação Portuguesa de Celíacos - APC) or via social media posting the link from February to May 2022. The inclusion criteria were as follows: a) Individuals aged >18 years diagnosed with celiac disease (CD) underwent a comprehensive diagnostic process, including clinical, serological, and histopathological assessments (specifically high upper digestive endoscopy with duodenal biopsies), along with genetic testing (HLA DQ2 and DQ8 analysis), in line with the ESsCD guideline (53). This criterion encompasses adults initially diagnosed with CD during childhood, adhering to the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) criteria (54)) and b) Participants were residents of Portugal and affiliated with the Portuguese Celiac Association (Associação Portuguesa de Celíacos - APC). After reading all the information about the study, those diagnosed with CD who agreed to participate accessed the questionnaire items. Those who disagreed were driven to the final page, acknowledging their time. All 234 individuals who signed the consent form to participate in the study completed the questionnaire.
The research followed the American Psychological Association (APA) Ethical Guidelines for Research involving Human Subjects. The participants were informed about the study’s scope, signed the informed consent form, and were not compensated for their participation. The Polytechnic University of Viseu Ethics Committee approved the ethical aspects of this study (n.° 59/SUB/2021 - 26th July 2021).
2.3 Statistical analysis
Data were extracted from the SurveyMonkey® platform and evaluated using International Business Machines Corporation (IBM) Statistical Package for the Social Sciences (SPSS) Statistics, version 22 (Armonk, NY: IBM Corp). The statistical analysis considered the CDQ and SF-36 scores.
Descriptive statistics were performed as mean and standard deviation for SF-36 subscales. Student’s t-test, Analysis of Variance (ANOVA) and Tukey’s posthoc test were used to compare the SF-36 and the variables of interest. The tests considered two-tailed hypotheses and a significance level of 5%. The association between the CDQ and SF-36 V2 was verified using Spearman’s correlation.
3 Results
A total of 234 individuals accepted to participate in the study and completed the questionnaire. The questionnaire was virtually applied, and all individuals who accessed it completed it. Table 1 shows data from the SF-36 domains subcategorized by sex, age, age at diagnosis, education, marital status, and diet. Males showed better scores for SF-36 domain 1 (Physical functioning), domain 2 (Role limitations due to physical health) and domain 7 (Role limitations due to emotional problems), and lower scores for domains 4 (General Health) and 5 (Energy/fatigue). Age differed only for domain 2 (Role limitations due to physical health), in which those > 40 y/o had better scores. Age at diagnosis differed only for domains 5 (Energy/fatigue), in which > 20 y/o at CD diagnosis had better scores and 6 (Social functioning) in which up to 20 y/o at CD diagnosis had better scores. Considering the educational level, participants with the highest educational level presented lower scores for domains 1, 2, 3, 6 and 7. Patients living alone presented lower scores for domain 1. Those following a GFD presented lower scores for D1, 2, 6, and 7 and the best score for D5 (Energy/fatigue). The use of antidepressants did not influence the SF-36 domains.
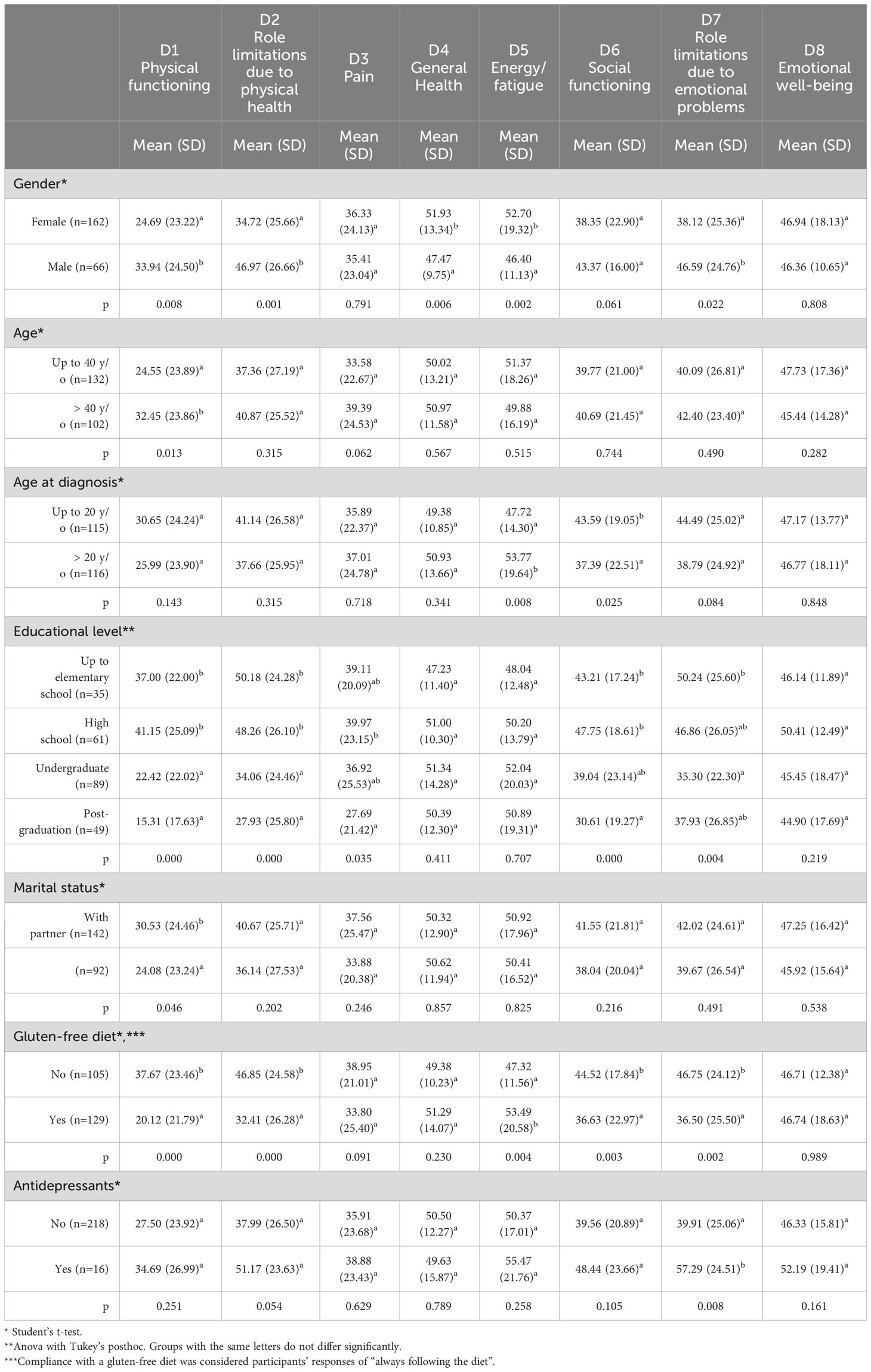
Table 1 SF-36 domains analyzed with subcategories based on sex, age groups, age at diagnosis of the condition, educational attainment, marital status, and dietary habits (n=234).
The CDQ domains’ maximum scores can be 49 and 196 in total. Table 2 shows that our sample presented the lowest score for social and gastrointestinal CDQ domains (23.03 ± 9.53 and 25.12 ± 8.81, respectively). Evaluating the associations, the SF-36 Domain 4 (general health) presented a negative association with all CDQ domains (Table 2). All the other domains showed positive associations with the CDQ.
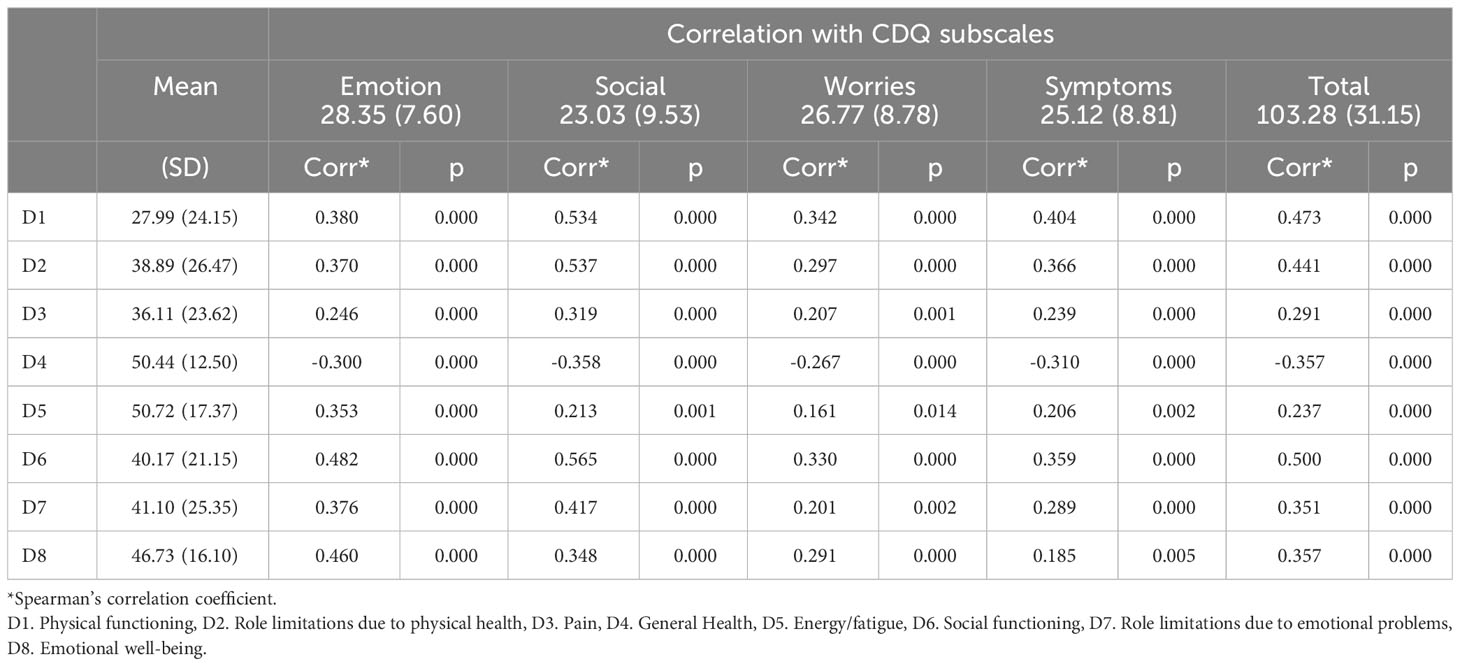
Table 2 Mean and SD of SF-36 V2 scores and correlation between CDQ scale subscores.
4 Discussion
This study recently evaluated the QoL perception of Portuguese celiac patients using a general questionnaire (SF-36) and compared its association with the specific questionnaire CDQ since CD symptoms and a lifelong GFD may significantly impact celiacs’ QoL. In our sample, about 45% of participants (n = 105) did not comply with the GFD, similar to data found in a previous study performed in Portugal in 2014 with 195 celiac patients, in which 47.7% did not comply with the GFD (44). The authors did not find an association between the QoL perception using the SF-36 and GFD compliance (44) and mentioned that it would be expected that GFD compliance would be positively associated with QoL. They list some potential explanations for their results: i) celiac patients who do not comply with the GFD were those who present milder symptoms, which do not significantly compromise their QoL; ii) those who did not comply with the GFD consider it less disruptive to their daily lives than that compliance with the GFD and iii) the possibility that the SF-36 was not sensitive enough to differentiate compliance with the GFD. In our study, celiacs not complying with the GFD showed the best scores for D1, D2, D6 and D7.
The D1(Physical functioning) scores were higher for males, > 40 y/o, those with the lowest educational levels, with partners and those not following the GFD. This SF-36 domain is important for identifying physical compromise in chronic diseases that impair common routine and exercise activities. A study (55) estimating the impact of chronic pain on patients’ QoL and found that the participants presented significantly lower mean QoL scores across all domains of the SF-36. The score for the D1 domain among the 78 chronic pain subjects was 31.8 ± 27.2 in comparison to scores of 94.0 ± 12.4 and 90.2 ± 18.9 from the general population in studies from England and Wales, respectively (p=0.001). Regarding CD, however, the impact of the condition on patients’ physical functioning has been poorly studied. Tiredness/fatigue are common manifestations described in CD (56), but they do not severely compromise physical abilities. Nonetheless, some celiac patients may experience neurological manifestations (neuropathy and ataxia), which might affect the physical domain to a certain extent. Peripheral neuropathy usually manifests as tingling, pain, and numbness, primarily in the hands and feet (57).
Two dimensions measure the impact of health limitations due to role limitations arising from physical health (D2) or emotional problems (D7), considering the type and amount of work performed, the necessity to reduce work, or the challenges faced in carrying it out. D2 scores were higher for males, those with the lowest educational levels, and those not following the GFD. The role limitations due to emotional problems (D7) presented the lowest scores for females, those complying with the GFD and not using antidepressants.
The Pain dimension (D3) measures the intensity and discomfort caused by pain and how this interferes with normal work. D3 dimension was only affected by educational level, in which those with the highest educational level showed the worst score. Abdominal pain is a frequent symptom in celiac individuals, although more frequently found in childhood (58). Although a strict GFD improves CD clinical manifestations such as abdominal pain (59), participants from our study presented low scores in D3, possibly related to the poor diet compliance found in our sample.
Energy/fatigue dimension (D5) showed higher scores for females, those complying with the GFD, and those with the age of diagnosis > 20 y/o. Although fatigue is often reported among celiac individuals, it usually improves once the GFD is implemented by the patient (56), which is in accordance with our finding that those compliant with the diet had better scores for this domain.
Social functioning (D6) was higher in those with age at diagnosis up to 20 years old, with the lowest educational levels, and who did not comply with the GFD. The finding that participants who did not comply with the GFD had higher scores for the social functioning domain is not surprising. As mentioned above, although the restriction of gluten from the diet is essential to good health in celiac patients, it interferes with social situations in the patients’ family, friends, and school/work environments (59). Wolf et al. (60) evaluated the association of QOL and GFD knowledge and adherence among 80 teenagers and adults. When asked about barriers to the GFD, 56% of adults and 70% of teens mentioned its adverse social impact. Feelings such as misunderstanding, embarrassment, stigma, exclusion, awkwardness, and guilt were expressed by participants (60).
The Emotional well-being dimension (D8) did not vary with sociodemographic data, or GFD compliance. Mental health problems have been documented in CD. Depression and/or depressive symptoms seem more frequent and/or severe in celiac patients than in healthy samples (61). Even though adherence to the GFD did not influence the D8 dimension in our sample, Sainsbury and Marques (61) suggest that poor diet adherence and self-reported depressive symptoms are associated, with the direction of causation being unclear. The authors mention that maintaining gluten on the diet may contribute to the appearance of a depressive state due to physiological mechanisms such as malabsorption of nutrients. On the other hand, being depressed compromises the individual’s ability to provide self-care and implement a safe GFD.
Males presented better scores than females on D1, D2 and D7, and worse on D4 and D5. These data differ from the previous study performed in Portugal (44) in which gender differed in D3, D5 and D8 with best results from males. Interestingly, the “general health” domain of SF-36 showed a negative association with all CDQ domains, contrary to what the authors of this study would have anticipated. A Turkish study (23) performed in 2015 with 81 celiac participants who answered the CDQ and SF-36 questionnaires showed a correlation between both questionnaires for all domains, similar to what Hauser (13) found in a study performed with 463 German celiac patients and Marchese (31) in a study performed in Italy with 171 celiac patients. An important factor to consider analyzing our results is that nearly half of the subjects in the sample (45%, n = 105) did not adhere to the GFD. It might be possible that the SF-36 does not accurately capture the influence of the GFD on the QoL of celiac patients, as previously demonstrated in a study conducted in Portugal (40). Consequently, this limitation could potentially impact the interpretation of results for questions related to the GFD. It is expected that the complete elimination of gluten from the diet leads to the remission of symptoms, normalization of intestinal histology and reduced risk for other health complications associated with CD (53), which are necessary for good health status.
Another interesting point to consider in this regard is question 2 from the SF-36 v2. “Compared to one year ago, how would you rate your health in general now?”. It might be reasonable to assume that this question, when applied to celiac individuals, would be influenced by diet compliance and time since the diagnosis. Patients who have received their diagnosis longer will probably have more tools to deal with difficulties related to the diet and the disease itself. There is evidence that more knowledge about CD and the diet, and support by health professionals and family improves the GFD compliance (53), all of which require time being diagnosed to be accomplished. Moreover, GFD effects on time until clinical improvement occurs and health depends on the length of time the patient remained undiagnosed due to the magnitude of intestinal mucosa damage (59).
This study presents some limitations. The sample comprised adult celiacs recruited using the snowball method by social media, leading to a possible selection bias due to a non-probabilistic sample. In this sense, our results may not represent the general Portuguese celiac people. In addition, despite the broad use of self-reported compliance to a GDF (34, 39, 48–52), we could not confirm the information (62), since data collection occurred online due to the COVID-19 pandemic restrictions, limiting the access to confirmation by laboratory tests. Despite the Portuguese Celiac Association has distributed the questionnaire to participants from all regions of Portugal to encompass the range of experiences and viewpoints of people living with CD in the country, the questionnaire did not ask for their exact location limiting the discussion about cultural and sociodemographic aspects.
5 Conclusions
In our study, seven out of the eight SF-36 v2 Portuguese Health Survey domains showed a positive correlation to the specific questionnaire CDQ. However, the “General Health” domain (domain 4) exhibited a negative correlation with the CDQ. Differences in content between the two instruments might be able to explain this finding, since the CDQ explores issues regarding specificities of CD and the lifelong GFD burden. Given that about half of the sample from this study displayed poor diet adherence, it is possible that the SF-36 could not reflect the impact of CD treatment - the complete elimination of gluten from the diet - on patients’ health. This is a possible explanation for this result. Nonetheless, this issue should be carefully evaluated in future research.
Specific validated questionnaires for CD individuals, such as the CDQ, contemplate social, economic, and clinical variables that permeate the patient’s life context. Therefore, these instruments may be more suitable for evaluating QOL in this public. However, using a general questionnaire such as the SF-36 would be indicated for comparing QOL between celiac patients and the general population or even between CD and other disease individuals. In this case, we recommend to parallelly assess GFD compliance for control.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The study was conducted in accordance with the American Psychological Association (APA) for research involving human subjects, and approved by the Ethics Committee of Polythecnic University of Viseu (59/SUB/2021). The studies were conducted in accordance with local and international laws and institutional guidelines. The participants provided their written informed consent to participate in this study.
Author contributions
CC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. RZ: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. AR: Conceptualization, Formal analysis, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. EN: Formal analysis, Writing – review & editing. FR: Formal analysis, Funding acquisition, Investigation, Writing – review & editing. PF: Writing – original draft, Writing – review & editing. ET-L: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work is funded by National Funds through the FCT-Foundation for Science and Technology, I.P., within the scope of the projects Refa UIDB/05507/2020 and UIDB/00681/202. The study was also supported by FAPDF N° 539/2022 and the Brazilian National Council for Scientific and Technological Development (CNPq -N° 302602/2021-6).
Acknowledgments
Authors would like to extend special acknowledgment to Associação Portuguesa de Celı́acos (APC) and the students of the Health School of the Polytechnic University of Viseu, Ana Rita Santos, Carlota Oliveira, Carolina Nogueira, Christophe Oliveira, Dylan Oliveira. This work was supported by the FCT—Foundation for Science and Technology, Portugal. Furthermore, we would like to thank the Centre for Studies in Education and Innovation (CI&DEI), and the Institute Polytechnic of Viseu for their support. Renata Puppin Zandonadi acknowledges The University of Brası́lia, Fundação de Apoio à Pesquisa do Distrito Federal (FAPDF) and the Brazilian National Council for Scientific and Technological Development (CNPq) for their scientific support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. McDermid JM, Almond MA, Roberts KM, Germer EM, Geller MG, Taylor TA, et al. Celiac disease: an academy of nutrition and dietetics evidence-based practice guideline. J Acad Nutr Diet. (2023) 123(12):1793–1807.e4. doi: 10.1016/j.jand.2023.07.018
2. Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2018) 16:823–836.e2. doi: 10.1016/J.CGH.2017.06.037
3. Husby S, Koletzko S, Korponay-Szabó I, Kurppa K, Mearin ML, Ribes-Koninckx C, et al. European society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2019. J Pediatr Gastroenterol Nutr. (2019) 70(1):141–56. doi: 10.1097/MPG.0000000000002497
4. Lohiniemi S, Mäki M, Kaukinen K, Laippala P, Collin P. Gastrointestinal symptoms rating scale in coeliac disease patients on wheat starch-based gluten-free diets. Scand J Gastroenterol. (2009) 35(9):947–9. doi: 10.1080/003655200750023002
5. Häuser W, Gold J, Stein J, Caspary WF, Stallmach A. CDQ Germany. Eur J Gastroenterol Hepatol. (2006) 18(7):747–53. doi: 10.1097/01.meg.0000221855.19201.e8
6. Pratesi CB, Häuser W, Uenishi RH, Selleski N, Nakano EY, Gandolfi L, et al. Quality of life of celiac patients in Brazil: questionnaire translation, cultural adaptation and validation. Nutrients. (2018) 10(9):1167. doi: 10.3390/nu10091167
7. Falcomer AL, Araújo LS, Farage P, Monteiro JS, Nakano EY, Zandonadi RP. Gluten contamination in food services and industry: A systematic review. Crit Rev Food Sci Nutr. (2018) 0:1–15. doi: 10.1080/10408398.2018.1541864
8. Itzlinger A, Branchi F, Elli L, Schumann M, Itzlinger A, Branchi F, et al. Gluten-free diet in celiac disease—Forever and for all? Nutrients. (2018) 10:1796. doi: 10.3390/nu10111796
9. Lobão ARF, Gonçalves RFLL, Monteiro RB, Castro FV. Qualidade de vida da pessoa celíaca adulta. Int J Dev Educ Psychol. (2010) 1:479–85. Available at: https://www.redalyc.org/pdf/3498/349832324051.pdf.
10. Fagerdahl A-M, Boström L, Ulfvarson J, Bergström G, Ottosson C. Translation and validation of the wound-specific quality of life instrument cardiff wound impact schedule in a swedish population. Scand J Caring Sci. (2014) 28:398–404. doi: 10.1111/scs.12050
11. Hauser W, Gold J, Stein J, Caspary WF, Stallmach A. Health-related quality of life in adult coeliac disease in Germany: results of a national survey. Eur J Gastroenterol Hepatol. (2006) 18:747–54. doi: 10.1097/01.meg.0000221855.19201.e8
12. Zingone F, Iavarone A, Tortora R, Imperatore N, Pellegrini L, Russo T, et al. The italian translation of the celiac disease-specific quality of life scale in celiac patients on gluten free diet. Digestive Liver Dis. (2013) 45:115–8. doi: 10.1016/j.dld.2012.10.018
13. Häuser W, Gold J, Stallmach A, Caspary WF, Stein J. Development and validation of the Celiac Disease Questionnaire (CDQ), a disease-specific health-related quality of life measure for adult patients with celiac disease. J Clin Gastroenterol. (2007) 41(2):157–66. doi: 10.1097/01.mcg.0000225516.05666.4e
14. Hughey JJ, Ray BK, Lee AR, Voorhees KN, Kelly CP, Schuppan D. Self-reported dietary adherence, disease-specific symptoms, and quality of life are associated with healthcare provider follow-up in celiac disease. BMC Gastroenterol. (2017) 17:1–8. doi: 10.1186/s12876-017-0713-7
15. Guennouni M, Admou B, Elkhoudri N, Bouchrit S, Ait Rami A, Bourrahouat A, et al. Quality of life of moroccan patients with celiac disease: arabic translation, cross-cultural adaptation, and validation of the celiac disease questionnaire. Arab J Gastroenterol. (2022) 23:246–52. doi: 10.1016/J.AJG.2022.06.009
16. Kurppa K, Collin P, Mäki M, Kaukinen K. Celiac disease and health-related quality of life. (2014) 5:83–90. doi: 10.1586/EGH.10.81
17. Real-Delor RE, Centurión-Medina IC. Quality of life in Paraguayan adults with celiac disease. Duazary. (2018) 15(1):61–70. doi: 10.21676/2389783X.2026
18. Leffler DA, Acaster S, Gallop K, Dennis M, Kelly CP, Adelman DCA. Novel patient-derived conceptual model of the impact of celiac disease in adults: implications for patient-reported outcome and health-related quality-of-life instrument development. Value Health. (2017) 20:637–43. doi: 10.1016/j.jval.2016.12.016
19. Casellas F, Rodrigo L, Molina-Infante J, Vivas S, Lucendo AJ, Rosinach M, et al. Transcultural adaptation and validation of the celiac disease quality of life transcultural adaptation and validation of the celiac disease quality of life ( CD-QOL ) survey , a specific questionnaire to measure quality of life in patients with celiac dis. Rev Espanõla Enfermedades Digestivas. (2013) 105:585–93. doi: 10.4321/S1130-01082013001000003
20. Casellas F, Rodrigo L, López Vivancos J, Riestra S, Pantiga C, Baudet JS, et al. Factors that impact health-related quality of life in adults with celiac disease: A multicenter study. World J Gastroenterol. (2008) 14:46–52. doi: 10.3748/wjg.14.46
21. Meyer S, Rosenblum S. Activities, participation and quality of life concepts in children and adolescents with celiac disease: A scoping review. Nutrients. (2017) 9:1–15. doi: 10.3390/NU9090929
22. Rodríguez-Almagro J, Hernández-Martínez A, Lucendo AJ, Casellas F, Solano-Ruiz MC, Siles-González J, et al. Health-related quality of life and determinant factors in celiac disease. A population-based analysis of adult patients in Spain. Rev Esp Enferm Dig. (2016) 108(4):181–9. doi: 10.17235/reed.2016.4094/2015
23. Aksan AAA, Mercanligil SM, Häuser W, Karaismailo E, Mercanlıgil SM, Häuser W, et al. Validation of the turkish version of the celiac disease questionnaire (CDQ). Health Qual Life Outcomes. (2015) 13:1–7. doi: 10.1186/s12955-015-0272-y
24. Al Nofaie N, Al Ahmadi J, Saadah O. Health related quality of life among saudi children and adolescents with celiac disease. Saudi J Gastroenterol. (2020) 26:26. doi: 10.4103/sjg.SJG_74_19
25. Ware JE, Kosinski M, Keller SD. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston: The Health Institute. (1994).
26. Brazier JE, Harper R, Jones N, O’Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. Gen Pract. (1992) 305:160–4. doi: 10.1016/S0140-6736(61)91704-4
27. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Med. (2016) 4:1–12. doi: 10.1177/2050312116671725
28. Burger JPW, Van Middendorp H, Drenth JPH, Wahab PJ, Evers AWM. How to best measure quality of life in coeliac disease? A validation and comparison of disease-specific and generic quality of life measures. Eur J Gastroenterol Hepatol. (2019) 31:941–7. doi: 10.1097/MEG.0000000000001432
29. Taft TH. When not to use a generic: measuring HRQoL in chronic digestive disease necessitates the use of disease-specific questionnaires. Dig Dis Sci. (2021) 66:3219–21. doi: 10.1007/S10620-020-06780-8/METRICS
30. Glise H, Wiklund I. Health-related quality of life and gastrointestinal disease. J Gastroenterol Hepatol. (2002) 17:S72–84. doi: 10.1046/J.1440-1746.17.S1.6.X
31. Marchese A, Klersy C, Biagi F, Balduzzi D, Bianchi PI, Trotta L, et al. Quality of life in coeliac patients: italian validation of a coeliac questionnaire. Eur J Intern Med. (2013) 24:87–91. doi: 10.1016/j.ejim.2012.09.015
32. Pouchot J, Despujol C, Malamut G, Ecosse E, Coste J, Cellier C. Validation of a french version of the quality of life "Celiac disease questionnaire". PloS One. (2014) 9:e96346. doi: 10.1371/journal.pone.0096346
33. Mahadev S, Gardner R, Lewis SK, Lebwohl B, Green PH. Quality of Life in Screen-detected Celiac Disease Patients in the United States. J Clin Gastroenterol. (2016) 50(5):393–7. doi: 10.1097/MCG.0000000000000433
34. Falcomer AL, Farage P, Pratesi CB, Pratesi R, Gandolfi L, Nakano EY, et al. Health-related quality of life and experiences of Brazilian celiac individuals over the course of the sars-cov-2 pandemic. Nutrients. (2021) 13:1582. doi: 10.3390/NU13051582
35. C D, Berry N, Vaiphei K, Dhaka N, Sinha SK, Kochhar R. Quality of life in celiac disease and the effect of gluten-free diet. J Gastroenterol Hepatol. (2018) 6(4):124–8. doi: 10.1002/jgh3.12056
36. Zysk W, Głąbska D, Guzek D. Social and emotional fears and worries influencing the quality of life of female celiac disease patients following a gluten-free diet. Nutrients. (2018) 10:1414. doi: 10.3390/NU10101414
37. Barzegar F, Pourhoseingholi MA, Rostami-Nejad M, Gholizadeh S, Malekpour MR, Sadeghi A, et al. Transcultural adaptation and validation of persian version of celiac disease questionnaire (CDQ); A specific questionnaire to measure quality of life of Iranian patients. Galen Med J. (2018) 7:e1106–6. doi: 10.31661/GMJ.V7I0.1106
38. Harnett JE, Myers SP. Quality of life in people with ongoing symptoms of coeliac disease despite adherence to a strict gluten-free diet. Sci Rep. (2020) 10:1–5. doi: 10.1038/s41598-020-58236-8
39. Selleski N, Zandonadi RP, Milde LB, Gandolfi L, Pratesi R, Häuser W, et al. Evaluation of quality of life of adult patients with celiac disease in Argentina: from questionnaire validation to assessment. Int J Environ Res Public Health. (2020) 17:7051. doi: 10.3390/IJERPH17197051
40. Henrietta S, Zsolt H, Gabriella dr V, Loránd Tudományegyetem E, és Pszichológiai Kar P, Doktori Iskola P. A szégyen mediációs szerepe a stigma és az életminőség kapcsolatában coeliakiában szenvedő Betegek körében.: A 8 tételes stigmatizáció Krónikus betegségekben kérdőív magyar adaptálása. Orv Hetil. (2021) 162:1968–76. doi: 10.1556/650.2021.32258
41. Lobão C, Gonçalves R, Monteiro BR. Development of the portuguese version of the celiac disease questionnaire. Soc REVIEW. Int Soc Sci Rev / Rev Internacional Cienc Sociales. (2013) 2:1–8. doi: 10.37467/GKA-REVSOCIAL.V2.1229
42. Chaves C, Raposo A, Zandonadi RP, Nakano EY, Ramos F, Teixeira-Lemos E. Quality of life perception among portuguese celiac patients: A cross-sectional study using the celiac disease questionnaire (CDQ). Nutrients. (2023) 15:2051. doi: 10.3390/nu15092051
43. Moreno M, de L, Sánchez-Muñoz D, Sousa C. Quality of life in teenagers and adults with coeliac disease: from newly spanish coeliac disease questionnaire validation to assessment in a population-based study. Front Nutr. (2022) 9:887573/BIBTEX. doi: 10.3389/FNUT.2022.887573/BIBTEX
44. Pimenta-Martins A, Pinto E, Gomes AMP. Perceção Do Estado de Saúde e Da Qualidade de Vida Numa Amostra de Celíacos Portugueses. GE Jornal Português Gastrenterologia. (2014) 21:109–16. doi: 10.1016/j.jpg.2013.09.006
45. Leighton K, Kardong-Edgren S, Schneidereith T, Foisy-Doll C. Using social media and snowball sampling as an alternative recruitment strategy for research. Clin Simul Nurs. (2021) 55:37–42. doi: 10.1016/j.ecns.2021.03.006
46. Webber-Ritchey KJ, Aquino E, Ponder TN, Lattner C, Soco C, Spurlark R, et al. Recruitment strategies to optimize participation by diverse populations. Nurs Sci Q. (2021) 34:235–43. doi: 10.1177/08943184211010471
47. Ferreira PL, Noronha Ferreira L, Nobre Pereira L. Medidas Sumário Física e Mental de Estado de Saúde Para a População Portuguesa. Rev Portuguesa Saúde Pública. (2012) 30:163–71. doi: 10.1016/j.rpsp.2012.12.007
48. Bulka CM, Davis MA, Karagas MR, Ahsan H, Argos M. The unintended consequences of a gluten-free diet. Epidemiology. (2017) 28:e24. doi: 10.1097/EDE.0000000000000640
49. Arámburo-Gálvez J, Carvalho Gomes I, André T, Beltrán-Cárdenas C, Macêdo-Callou M, Braga Rocha É, et al. Translation, cultural adaptation, and evaluation of a Brazilian portuguese questionnaire to estimate the self-reported prevalence of gluten-related disorders and adherence to gluten-free diet. Medicina (B Aires). (2019) 55:593. doi: 10.3390/medicina55090593
50. Ontiveros N, Rodríguez-Bellegarrigue CI, Galicia-Rodríguez G, Vergara-Jiménez M, de J, Zepeda-Gómez EM, et al. Prevalence of self-reported gluten-related disorders and adherence to a gluten-free diet in salvadoran adult population. Int J Environ Res Public Health. (2018) 15:786. doi: 10.3390/IJERPH15040786
51. Silvester JA, Weiten D, Graff LA, Walker JR, Duerksen DR. Is it gluten-free? Relationship between self-reported gluten-free diet adherence and knowledge of gluten content of foods. Nutrition. (2016) 32:777–83. doi: 10.1016/J.NUT.2016.01.021
52. de Oliveira PM, Zandonadi RP, Cutrim AMV, Nakano EY, de Queiroz FLN, Botelho RBA, et al. Eating competence and aspects related to a gluten-free diet in Brazilian adults with gluten-related disorders. Nutrients. (2022) 14:2815. doi: 10.3390/nu14142815
53. Al-Toma A, Volta U, Auricchio R, Castillejo G, Sanders DS, Cellier C, et al. European society for the study of coeliac disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur Gastroenterol J. (2019) 7:583–613. doi: 10.1177/2050640619844125
54. Husby S, Koletzko S, Korponay-Szabó I, Kurppa K, Mearin ML, Ribes-Koninckx C, et al. European society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2020. J Pediatr Gastroenterol Nutr. (2020) 70:141–56. doi: 10.1097/MPG.0000000000002497
55. Hadi MA, McHugh GA, Closs SJ. Impact of chronic pain on patients’ Quality of life: A comparative mixed-methods study. J Patient Exp. (2019) 6:133–41. doi: 10.1177/2374373518786013
56. Jelsness-Jørgensen L-P, Bernklev T, Lundin K. Fatigue as an extra-intestinal manifestation of celiac disease: A systematic review. Nutrients. (2018) 10:1652. doi: 10.3390/nu10111652
57. Mearns E, Taylor A, Thomas Craig K, Puglielli S, Leffler D, Sanders D, et al. Neurological manifestations of neuropathy and ataxia in celiac disease: A systematic review. Nutrients. (2019) 11:380. doi: 10.3390/nu11020380
58. Leonard MM, Sapone A, Catassi C, Fasano A. Celiac disease and nonceliac gluten sensitivity. JAMA. (2017) 318:647. doi: 10.1001/jama.2017.9730
59. Bascuñán KA, Vespa MC, Araya M. Celiac disease: understanding the gluten-free diet. Eur J Nutr. (2017) 56:449–59. doi: 10.1007/s00394-016-1238-5
60. Wolf RL, Lebwohl B, Lee AR, Zybert P, Reilly NR, Cadenhead J, et al. Hypervigilance to a gluten-free diet and decreased quality of life in teenagers and adults with celiac disease. Dig Dis Sci. (2018) 63:1438–48. doi: 10.1007/s10620-018-4936-4
61. Sainsbury K, Marques MM. The relationship between gluten free diet adherence and depressive symptoms in adults with coeliac disease: A systematic review with meta-analysis. Appetite. (2018) 120:578–88. doi: 10.1016/j.appet.2017.10.017
Keywords: celiac disease, gluten-free diet, Portugal, quality of life, questionnaire
Citation: Chaves C, Zandonadi RP, Raposo A, Nakano EY, Ramos F, Farage P and Teixeira-Lemos E (2024) Health-related quality of life among celiacs in Portugal: a comparison between general and specific questionnaires. Front. Immunol. 15:1372369. doi: 10.3389/fimmu.2024.1372369
Received: 17 January 2024; Accepted: 20 February 2024;
Published: 04 March 2024.
Edited by:
Ángela Ruiz-Carnicer, Sevilla University, SpainReviewed by:
Verónica Segura Montero, University of Sevilla, SpainIvan Milos Stankovic, University of Belgrade, Serbia
Diego Sánchez Muñoz, Instituto Digestivo, Spain
Copyright © 2024 Chaves, Zandonadi, Raposo, Nakano, Ramos, Farage and Teixeira-Lemos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: António Raposo, YW50b25pby5yYXBvc29AdWx1c29mb25hLnB0; Edite Teixeira-Lemos, ZXRsZW1vczNAZ21haWwuY29t