
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 22 May 2024
Sec. Cytokines and Soluble Mediators in Immunity
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1372300
 Arnold Matovu Dungu1*
Arnold Matovu Dungu1* Agnete Troen Lundgaard2
Agnete Troen Lundgaard2 Camilla Koch Ryrsø1,3
Camilla Koch Ryrsø1,3 Maria Hein Hegelund1Andreas Vestergaard Jensen1
Maria Hein Hegelund1Andreas Vestergaard Jensen1 Peter Lommer Kristensen4,5
Peter Lommer Kristensen4,5 Rikke Krogh-Madsen3,5,6
Rikke Krogh-Madsen3,5,6 Daniel Faurholt-Jepsen5,7
Daniel Faurholt-Jepsen5,7 Sisse Rye Ostrowski5,8Karina Banasik2
Sisse Rye Ostrowski5,8Karina Banasik2 Birgitte Lindegaard1,3,5
Birgitte Lindegaard1,3,5Introduction: Diabetes is associated with dysregulated immune function and impaired cytokine release, while transient acute hyperglycaemia has been shown to enhance inflammatory cytokine release in preclinical studies. Although diabetes and acute hyperglycaemia are common among patients with community-acquired pneumonia (CAP), the impact of chronic, acute, and acute-on-chronic hyperglycaemia on the host response within this population remains poorly understood. This study investigated whether chronic, acute, and acute-on- chronic hyperglycaemia are associated with distinct mediators of inflammatory, endothelial, and angiogenic host response pathways in patients with CAP.
Methods: In a cross-sectional study of 555 patients with CAP, HbA1c, admission plasma (p)-glucose, and the glycaemic gap (admission p-glucose minus HbA1c- derived average p-glucose) were employed as measures of chronic, acute, and acute-on-chronic hyperglycaemia, respectively. Linear regression was used to model the associations between the hyperglycaemia measures and 47 proteins involved in inflammation, endothelial activation, and angiogenesis measured at admission. The models were adjusted for age, sex, CAP severity, pathogen, immunosuppression, comorbidity, and body mass index. Adjustments for multiple testing were performed with a false discovery rate threshold of less than 0.05.
Results: The analyses showed that HbA1c levels were positively associated with IL-8, IL-15, IL-17A/F, IL-1RA, sFlt-1, and VEGF-C. Admission plasma glucose was also positively associated with these proteins and GM-CSF. The glycaemic gap was positively associated with IL-8, IL-15, IL-17A/F, IL-2, and VEGF-C.
Conclusion: In conclusion, chronic, acute, and acute-on-chronic hyperglycaemia were positively associated with similar host response mediators. Furthermore, acute and acute-on-chronic hyperglycaemia had unique associations with the inflammatory pathways involving GM-CSF and IL-2, respectively.
Community-acquired pneumonia (CAP) is a global public health concern associated with high morbidity and mortality (1, 2). Cytokines and chemokines mediate the inflammatory response in CAP, with excessive responses increasing mortality risk (2–5). Inflammation also involves endothelial activation, which promotes leukocyte migration (6). However, excessive endothelial activation with aberrant angiogenic responses increases the risk of sepsis, septic shock, and mortality in CAP (7–9). Therefore, an improved understanding of factors associated with inflammatory, endothelial, and angiogenic host responses in CAP is crucial to improving care.
Type 2 diabetes, common in CAP (10), is associated with immune cell defects, inflammatory endothelial activation, and hypercoagulability (11). Transient acute hyperglycaemia, assessed by admission p-glucose or the glycaemic gap, is also common in CAP and is associated with mortality (12–14). The glycaemic gap represents the absolute difference between the admission p-glucose and the HbA1c-derived average glucose within the past 3 months (13). This metric quantifies the extent of acute-on-chronic hyperglycaemia by capturing deviations from the baseline, particularly in acute illnesses such as CAP (13). Moreover, transient hyperglycaemia has been shown to induce inflammatory endothelial activation (15) and enhance leukocyte cytokine release in preclinical studies (16), contrasting with the impaired cytokine responses seen in chronic hyperglycaemia as in type 2 diabetes (11). While chronic hyperglycaemia (as seen in type 2 diabetes), acute hyperglycaemia, and acute-on-chronic hyperglycaemia have been linked to dysregulation of the immune host response in COVID-19 pneumonia (17, 18), these associations have been sparingly explored in non-COVID-19 CAP.
Given this, we hypothesised that chronic, acute, and acute-on-chronic hyperglycaemia are associated with distinct inflammatory, endothelial, and angiogenic host response pathways.
The aim of this study was to investigate the associations between chronic, acute, and acute-on-chronic hyperglycaemia and 47 circulating proteins involved in inflammatory, endothelial, and angiogenic host response pathways in patients admitted with CAP.
This study was a cross-sectional study of patients enrolled in the Surviving Pneumonia cohort, a prospective observational cohort study of patients hospitalised with CAP at Copenhagen University Hospital, North Zealand, Denmark (19). The patients enrolled in this study were recruited between January 2019 and November 2021.
Inclusion criteria were adults ≥ 18 years old and hospitalised < 24 h with a new infiltrate on chest x-ray or computed tomography scan, and symptoms (e.g., cough, shortness of breath, and chest pain) or clinical signs (e.g., body temperature ≥38.0°C and abnormal chest examination) consistent with pneumonia.
Exclusion criteria were a positive polymerase chain reaction test for coronavirus disease 2019 (COVID-19) or no admission p-glucose and HbA1c measurement. The study protocol was designed before the COVID-19 pandemic; thus, COVID-19 cases were excluded from the present study. In addition, the roles of chronic, acute, and acute-on-chronic hyperglycaemia as risk factors for dysregulated inflammatory responses in COVID-19 have been described elsewhere (17, 18).
The study was approved by the Scientific Ethics Committee at the Capital Region of Denmark (H-18024256), registered on ClinicalTrials.gov (NCT03795662), and conducted in accordance with the Declaration of Helsinki (20). Eligible patients were enrolled after oral and written informed consent was obtained. If a patient could not provide consent, the written consent was obtained from a legal guardian or next of kin and an independent physician not part of the study following the guidelines set by the Ethics Committee at the Capital Region of Denmark.
Data were prospectively collected during admission through pre-planned patient interviews and medical record reviews. The collected data included demographic information, anthropometry, comorbidities, clinical data, microbiological findings, and laboratory results.
Body mass index (BMI) was calculated using self-reported height and measured weight at admission (Seca, Hamburg, Germany). CAP severity was defined using CURB-65 criteria (21). Data on selected comorbidities (known type 1 and type 2 diabetes, cardiovascular disease, chronic obstructive pulmonary disease, asthma, rheumatological disease, cancer, and immunosuppression) and treatment with glucocorticoids at admission were obtained from the electronic patient file. Immunosuppression was defined as treatment with cancer chemotherapy within the last 28 days, immunosuppressive drugs (e.g., glucocorticoids for more than 14 days corresponding to a prednisolone-equivalent of ≥20 mg/day, monoclonal antibodies used to treat autoimmune and inflammatory diseases), HIV infection, a history of solid organ or bone marrow transplant, or an inborn error of immunity (22).
Microbiological sampling and testing were at the discretion of the attending physicians. Clinically significant microbiological findings in respiratory samples, blood cultures, or pneumococcal/legionella urinary antigen tests were categorised into bacterial, viral, or mixed bacterial–viral aetiology. The cause of CAP was listed as unknown aetiology if the microbiological results were negative or if there was no microbiological sampling.
Based on HbA1c measurements obtained at admission and medical history, the study patients were classified according to their chronic hyperglycaemia status, encompassing euglycaemia, prediabetes, undiagnosed diabetes, and known diabetes. Among patients with no prior diabetes diagnosis, HbA1c < 39 mmol/mol (5.7%) was classified as euglycaemia, HbA1c ≥ 39 mmol/mol (5.7%) and < 48 mmol/mol (6.5%) as prediabetes, and HbA1c ≥ 48 mmol/mol (6.5%) as undiagnosed diabetes (10). Known diabetes was based on a prior diabetes diagnosis or treatment with glucose-lowering medication (i.e., metformin, sodium-glucose co-transporter-2 inhibitors, glucagon-like peptide-1 receptor agonists, insulin, and sulfonylureas), regardless of HbA1c level (23). At the time of inclusion, no sodium-glucose co-transporter-2 inhibitors were approved for treating heart failure and kidney disease in people without diabetes.
The definition of acute hyperglycaemia was based on the admission p-glucose level. Euglycaemia: p-glucose < 6.0 mmol/L; mild hyperglycaemia: p-glucose ≥ 6.0 and <11 mmol/L; severe hyperglycaemia: p-glucose ≥ 11.0 mmol/L (10).
Acute-on-chronic hyperglycaemia was determined using the glycaemic gap, calculated by subtracting the admission p-glucose from the HbA1c-derived estimate of the average p-glucose over the previous 2–3 months (13) and categorised in two ways in our analyses. Firstly, the glycaemic gap was categorised such that values above 0 signified the presence of acute-on-chronic hyperglycaemia, while values below 0 indicated the absence of this condition. Secondly, the glycaemic gap was divided into quartiles to provide a granular view of its distribution across our patient cohort (13).
Venous blood samples were drawn at admission, collected in EDTA tubes, and centrifuged at 3,000 g for 15 min at 4°C. Plasma was stored at −80°C until analysis. Technical covariates relating to the biobank samples included elapsed time between hospital admission and sample collection and total storage time since sample collection. Sine and cosine transformation of the biobank sampling date was used to calculate seasonality, as the cause of CAP varies throughout the year (24).
The Meso Scale Discovery (MSD) V-PLEX Human Biomarker 54-Plex is based on electrochemiluminescence technology and was used to measure 54 host response mediators (Meso Scale Diagnostics, Maryland, USA). This kit consists of 7 individual multiplex panels. However, we excluded the Th17 panel, which consists of 7 host response mediators, due to quality control issues. The 47 host response mediators in each of the remaining six panels are detailed in Supplementary Table 1, while their primary functions and cellular sources are provided in Supplementary Tables 2–5. Measurements were conducted on the Meso QuickPlex SQ 120 platform (Meso Scale Diagnostics, Maryland, USA) following the manufacturer’s instructions across three different sites in Denmark (Supplementary Table 1).
Biomarker concentrations were quantified with the light signal intensity instead of calculated concentrations to avoid noise introduced by standard curves. The sample pre-processing involved removing outliers, correcting batch effects with median normalisation, and transforming the data logarithmically to achieve a normal distribution. Further details about sample pre-processing are provided in the Supplementary Methods section.
The dependent variables consisted of log-transformed and median-normalised light signal values from 47 proteins, encompassing a wide range of functions, including pro-inflammatory, T cell associated, chemokines, endothelial activation, angiogenesis, and growth factors (Supplementary Tables 1–5).
In the primary analysis, the predictor variables were HbA1c, admission p-glucose, and the glycaemic gap as measures of chronic, acute, and acute-on-chronic hyperglycaemia, respectively. For the secondary analyses, we used categorised versions of these predictors—diabetes status for chronic hyperglycaemia, acute hyperglycaemia groups, and glycaemic gap quartiles for acute-on-chronic hyperglycaemia. In addition, factors that might affect the quality of the biobank samples (i.e., technical covariates) or might be associated with altered or distinct inflammatory, endothelial, and angiogenic activation (e.g., chronic diseases, pathogen) were included as covariates (7, 25).
The continuous variables were summarised as the median with the interquartile range (IQR), while the categorical variables were summarised as counts with percentages.
Principal component analysis (PCA) was conducted on all host response mediators to visualise whether the patients clustered according to the chronic, acute, and acute-on-chronic hyperglycaemia groups.
Linear regression was used to estimate the association between the predictors and the dependent variables. The predictors were evaluated separately to avoid multicollinearity. The associations were first estimated with a base model consisting of each predictor separately, the technical covariates, age, and sex, followed by the adjusted models consisting of base model covariates, microbiology, clinical covariates, and BMI. Model estimates were exponentiated and presented as fold changes with the corresponding 95% confidence intervals.
As detailed in Supplementary Material, BMI was missing in 17% of the patients and imputed with the missingness pattern assumed to be missing at random. The adjusted model estimates from each imputed dataset were combined with Rubin’s rules and compared to model estimates from complete case analyses. Each model was checked for linearity, homogeneity of variance, normality of residuals, and absence of multicollinearity.
Correction for multiple testing was performed using the Benjamini–Hochberg method with a false discovery rate threshold of 0.05. All statistical comparisons were two-sided, with p < 0.05 considered significant. The statistical analyses were performed with R software (R version 4.0.3), and multiple imputations were performed using the R package MICE.
Among 756 patients enrolled in the Surviving Pneumonia cohort during the study period, 653 had an available biobank sample. Ninety-eight patients were excluded due to a positive COVID-19 test (N = 95) or the absence of HbA1c or admission p-glucose samples (N = 3), leaving 555 patients for inclusion in this study (Figure 1). Patient characteristics are presented in Table 1. The median age was 74 years (IQR: 64, 81), 268 (48%) were women, 196 (35%) had prediabetes, 22 (4.0%) had undiagnosed diabetes, and 101 (18%) had known diabetes. Admission p-glucose concentrations were classified as normal (<6 mmol/L) in 100 (18%) patients, mild (6-11 mmol/L) in 390 (70%) patients, and severe (≥11 mmol/L) in 65 (12%) patients. The glycaemic gap was > 0 mmol/mol in 360 (65%) patients.

Figure 1 Flowchart of study enrolment. COVID-19, coronavirus disease 2019.
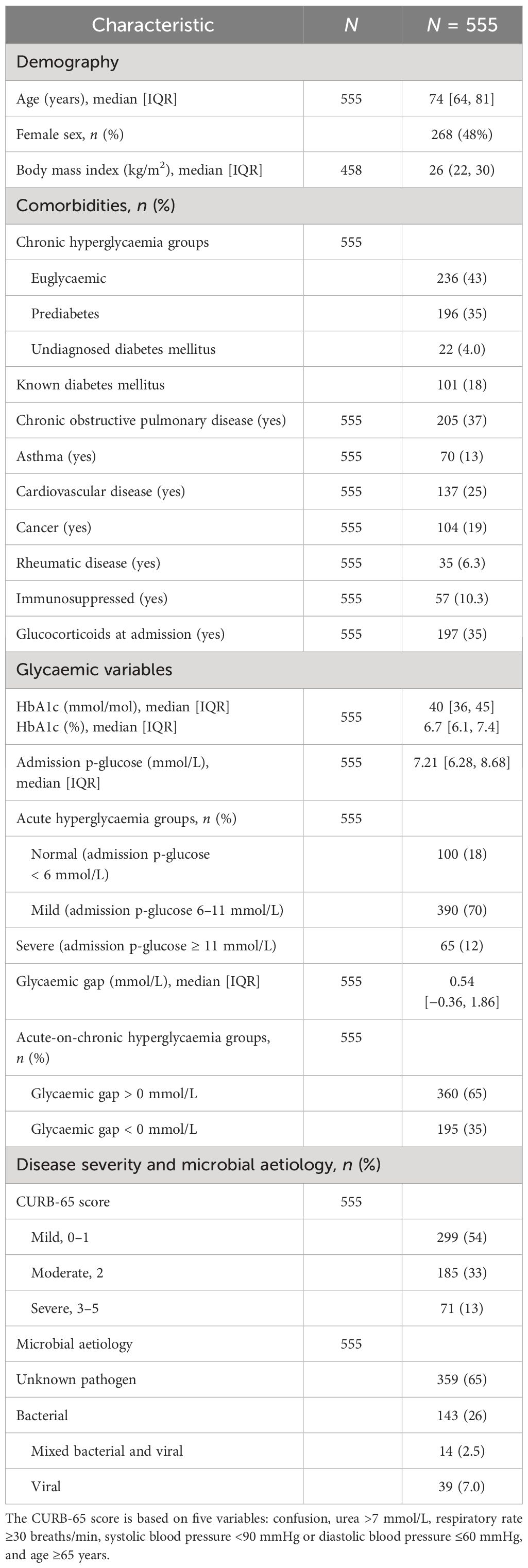
Table 1 Patient characteristics.
A pathogen was identified in 196 (35%) patients. The most frequently isolated pathogens were Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus, Legionella pneumophila, and influenza A virus (Supplementary Figure 1).
The PCA plots of the first and second principal components revealed no distinct clustering of host response pathways in the 47 host response mediators according to chronic (Supplementary Figure 2A), acute (Supplementary Figure 2B), or acute-on-chronic (Supplementary Figure 2C) hyperglycaemia groups.
In the base models, HbA1c was positively associated with concentrations of the chemokine IL-8, proinflammatory cytokines IL-15 and IL-16, T helper (Th)17 cytokine IL-17A/F, anti-inflammatory cytokine IL-1RA, endothelial activation marker soluble vascular cell adhesion molecule-1 (sVCAM1), and proteins involved in angiogenesis: vascular endothelial growth factor-C (VEGF-C), soluble fms-like tyrosine kinase-1 (sFlt-1), and soluble tyrosine kinase with immunoglobulin-like and EGF-like domains 2 (sTie-2) (Figure 2A).
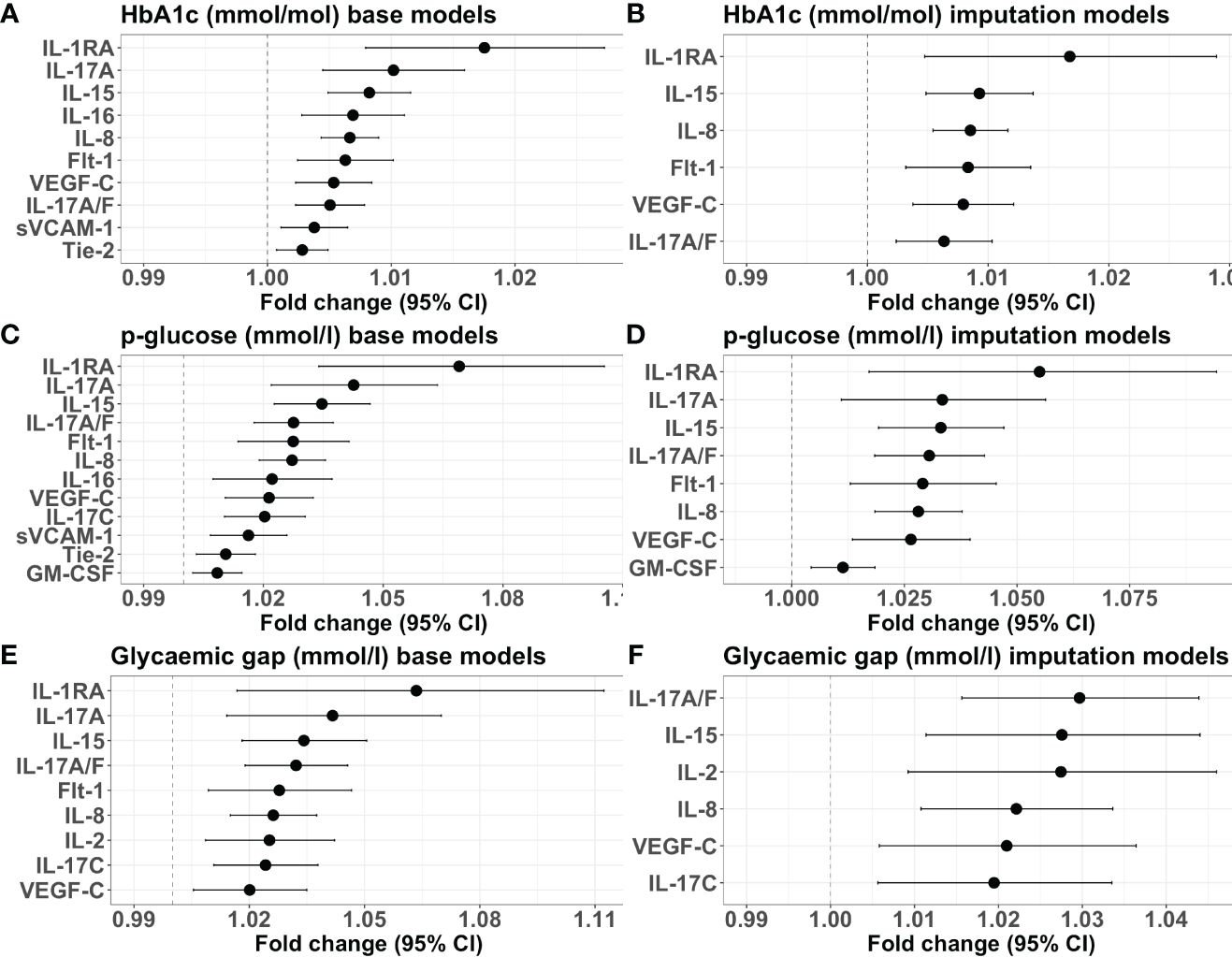
Figure 2 Forest plots illustrating the associations in base and adjusted models. (A) Base models with HbA1c as the predictor. (B) Adjusted models with HbA1c as the predictor. (C) Base models with admission p-glucose as the predictor. (D) Adjusted models with admission p-glucose as the predictor. (E) Base models with the glycaemic gap as the predictor. (F) Adjusted models with the glycaemic gap as the predictor. The x-axis shows the fold change in protein concentration for each 1 unit increase in HbA1c (mmol/mol), admission p-glucose (mmol/L), or glycaemic gap (mmol/L), with the corresponding 95% confidence intervals. Only proteins with statistically significant false discovery rate-adjusted p-values are included.
In the adjusted models, the positive associations between HbA1c and IL-8, IL-15, IL-17A/F, IL-1RA, VEGF-C, and sFlt-1 remained significant (Figure 2B).
HbA1c was not associated with other proteins, including the pro-inflammatory cytokines IL-6 and tumour necrosis factor-alpha (TNF-α) (Supplementary Figure 3). The model estimates remained consistent when results using imputed data and complete case analyses were compared (Supplementary Figures 4, 5A).
In the secondary analyses, there were no associations between diabetes status and the host response mediators in base (Supplementary Table 6) and adjusted models (Supplementary Table 7).
In the base models, admission p-glucose was positively associated with the haemopoietic growth factor granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-8, IL-15, IL-16, IL-1RA, IL-17A/F, IL-17A, IL-17C, sVCAM-1, VEGF-C, sFlt-1, and sTie-2 (Figure 2C).
The positive associations between admission p-glucose and IL-8, IL-15, IL-17A/F, IL-17A, IL-1RA, GM-CSF, VEGF-C, and sFlt-1 remained significant in the adjusted analyses (Figure 2D).
No associations between admission p-glucose and other proteins were found (Supplementary Figure 6). When comparing estimates from fully adjusted models using imputed data and complete case analysis, IL-17A, sFlt-1, and IL-1RA were significant only in analyses using imputed data (Supplementary Figures 7, 5B).
The secondary analyses found no associations between the acute hyperglycaemia groups and the host response mediators in the base (Supplementary Table 8) and adjusted models (Supplementary Table 9).
In the base models, the glycaemic gap was positively associated with concentrations of the proinflammatory cytokine IL-2, IL-8, IL-15, IL-1RA, IL-17A/F, IL-17A, IL-17C, sFlt-1, and VEGF-C (Figure 2E).
In the adjusted models, the positive associations between the glycaemic gap and IL-2, IL-8, IL-15, IL-17A/F, IL-17C, and VEGF-C remained significant (Figure 2F).
No associations between the glycaemic gap and other proteins were observed (Supplementary Figure 8). When comparing estimates from fully adjusted models using imputed data and complete case analysis, IL-17C and VEGF-C were found significant only in analyses using imputed data (Supplementary Figures 9, 5C).
In models with the glycaemic quartiles as the predictors, no associations were found between acute-on-chronic hyperglycaemia and the host response mediators in base (Supplementary Table 10) and adjusted models (Supplementary Table 11).
HbA1c, admission p-glucose, and the glycaemic gap were positively associated with overlapping inflammatory, endothelial, and angiogenic host response pathways. The main findings of the present study are as follows: (1) chronic hyperglycaemia (HbA1c), acute hyperglycaemia (admission p-glucose), and acute-on-chronic hyperglycaemia (glycaemic gap) were positively associated with the chemokine IL-8, pro-inflammatory cytokine IL-15, Th17 cytokine IL-17A/F, and lymphangiogenic growth factor VEGF-C; (2) chronic and acute hyperglycaemia were positively associated with the anti-inflammatory cytokine IL-1RA and the anti-angiogenic decoy receptor sFlt1; (3) acute hyperglycaemia was positively associated with the haematopoietic growth factor and proinflammatory cytokine GM-CSF; and (4) acute-on-chronic hyperglycaemia was positively associated with the pro-inflammatory cytokine IL-2.
The secondary analyses found no associations between the three hyperglycaemia measures entered as categorical variables and the host response mediators after adjustment for multiple testing.
The immune response to CAP is a complex process of innate and adaptive immunity mediated by pro-inflammatory responses, endothelial activation, and pneumonia resolution mediated by anti-inflammatory responses (2, 26, 27). Preclinical in vitro and in vivo studies have shown that acute hyperglycaemia induces proinflammatory cytokine and chemokine responses and endothelial activation (28–30), while type 2 diabetes is associated with dysregulated immune responses and endothelial dysfunction (11). Currently, data on the impact of acute, chronic, and acute-on-chronic on the host response in CAP remain limited, highlighting a gap in our understanding of how chronic and acute glucometabolic dysregulation influences CAP immunopathogenesis.
We used various glycaemic measures to investigate the associations of chronic, acute, and acute-on-chronic hyperglycaemia with host response pathways. HbA1c concentrations provide insight into glycaemic control over the preceding 2–3 months and are unaffected by the acute stress response induced by acute illness (31), while the admission p-glucose level encompasses chronic hyperglycaemia and stress-induced hyperglycaemia during infection (32). In addition, by utilising HbA1c-adjusted glycaemic variables, such as the glycaemic gap, we were able to explore the impact of acute-on-chronic hyperglycaemia itself, minimising potential interference from long-term hyperglycaemia (13).
The observation that all three measures of hyperglycaemia in our study were associated with IL-8, IL-15, IL-17, and VEGF-C suggests that these chemokine, cytokine, and lymphangiogenic pathways are influenced by chronic hyperglycaemia rather than solely acute and acute-on-chronic hyperglycaemia.
To our knowledge, our study is the first to show that chronic, acute, and acute-on-chronic hyperglycaemia are positively associated with the mediators of innate immunity IL-8 and IL-15 in patients with CAP. IL-8 is a central mediator of innate immunity as a chemotactic factor and activator of neutrophils (33). In patients with CAP, IL-8 has been positively associated with increased risk of mortality (34). During acute inflammation, IL-15 plays a crucial role in bridging innate and adaptive immunity by regulating the activation, proliferation, and survival of T cells and natural killer (NK) cells and enhancing neutrophil IL-8 secretion (35). Conceptually, our findings are consistent with prior research that showed that chronic hyperglycaemic conditions, such as type 2 diabetes mellitus, elevated HbA1c levels, and insulin resistance, are associated with higher concentrations of IL-8 (36) and IL-15 (37). However, the role of IL-15 in chronic hyperglycaemia is multifaceted, with animal studies associating it with positive glucometabolic effects, including reduced fat mass, decreased insulin resistance, and reduced adipose tissue inflammation (38).
Furthermore, our findings are in line with a study in individuals without diabetes mellitus that reported an increase in systemic IL-8 levels during an oral glucose tolerance test, with a positive correlation between IL-8 and post-load glucose levels and a more pronounced IL-8 increase in individuals with impaired glucose tolerance (30). Similar data regarding increased concentration of IL-15 during transient hyperglycaemia are lacking.
Cellular adaptive immunity is mediated by cytokines secreted by T cells (39). To our knowledge, our study is the first to describe that chronic, acute, and acute-on-chronic hyperglycaemia are positively associated with cytokines in the IL-17 family in patients with CAP. The cytokines in the IL-17 family are secreted by the adaptive T helper 17 cells and mediate the immune response to extracellular pathogens and essential for mucosal immunity (39). Although crucial for adaptive immunity, increased IL-17 concentrations have been associated with greater disease severity, higher mortality rates, and an increased risk of ICU admission in patients with CAP (5).
The cytokines in the IL-17 family are secreted by the adaptive T helper (Th) 17 cells and mediate the immune response to extracellular pathogens and essential for mucosal immunity (39).
Our results regarding chronic hyperglycaemia are consistent with previous research showing that individuals with type 2 diabetes mellitus exhibit elevated levels of Th17 cell subsets and IL-17 concentrations (40, 41). IL-17 is thought to be involved in the pathogenesis of type 2 diabetes by inducing adipose tissue inflammation and upregulation of pro-inflammatory cytokines that induce insulin resistance and β-cell failure (42). However, evidence is scarce on whether short-term acute hyperglycaemia can stimulate IL-17 production in humans. In contrast, research using mouse models of autoimmune diseases indicates that high glucose consumption stimulates Th17 cell generation and exacerbates Th17-driven autoimmune responses (43).
Endothelial and angiogenic responses are essential for the migration of leukocytes from blood vessels to inflammation sites (6). Our study is the first, to our knowledge, to show that chronic, acute, and acute-on-chronic hyperglycaemia are positively associated with VEGF-C.
The main function of VEGF-C is to promote the proliferation, migration, and survival of lymphatic endothelial cells (44). Currently, the prognostic significance of VEGF-C in patients with CAP remains unexplored. Furthermore, the positive association between chronic hyperglycaemia and VEGF-C are similar to previous findings from a study that found the HbA1c and fasting p-glucose were positively correlated with VEGF-C levels (30). Furthermore, hyperglycaemic conditions have been shown to increase VEFG-C expression in vitro (45).
Thus, our findings suggest that chronic, acute, and acute-on-chronic hyperglycaemia might be associated with enhanced host response mediators of innate and adaptive immunity and lymphatic function.
Anti-inflammatory responses during CAP are essential for CAP resolution and prevention of immune-mediated tissue damage (2). To our knowledge, our study is the first to show that chronic and acute hyperglycaemia were positively associated with the anti-inflammatory cytokine IL-1RA (39). IL-1RA mediates the anti-inflammatory response by binding to the receptors of the pro-inflammatory cytokines of IL-1α and IL-1β (39), which induce fever, the acute phase response, proinflammatory cytokine production, upregulation of endothelial adhesion molecules, and T- and B-cell proliferation, to name the most essential (46). However, high IL-1RA concentrations are associated with an increased risk of mortality in CAP (47). Regarding chronic hyperglycaemia, our findings are consistent with previous research showing that IL-1RA concentrations are elevated in conditions with impaired glucose tolerance and type 2 diabetes, presumably as an anti-inflammatory response to adipose tissue inflammation induced by IL-1α and IL-1β secreted by macrophages (48).
Furthermore, our findings are consistent with a previous study that showed that acute hyperglycaemia was associated with higher IL-1RA concentrations in mechanically ventilated patients with CAP and sepsis (49).
Furthermore, our study is the first to suggest that chronic and acute hyperglycaemia might also impact antiangiogenic processes in CAP, considering the association with sFlt-1, a decoy receptor for angiogenic growth factors like VEGF-A, VEGF-B, and placental growth factor (50). Our findings thus align with previous research that has shown that sFlt-1 and VEGFs are elevated in chronic hyperglycaemic states, such as impaired glucose tolerance and type 2 diabetes (51, 52). In chronic hyperglycaemia, elevated sFlt-1 is thought to counteract the abnormal angiogenesis mediated by VEGFs (51, 52). On the other hand, the relationship between transient acute hyperglycaemia and sFlt-1 levels remains unclear, as does the impact of sFlt-1 on the prognosis of patients with CAP.
Notably, in the adjusted analyses, chronic and acute hyperglycaemia were not associated with sVCAM-1, an endothelial activation marker, or Tie-2, which regulates angiogenesis. These findings might be explained by adjusting for chronic diseases associated with higher levels of sVCAM-1 and sTie-2 and endothelial injury, such as diabetes and cardiovascular disease (53, 54).
Our findings suggest that chronic and acute hyperglycaemia might play a role in the anti-inflammatory responses and modulation of angiogenic processes in patients with CAP.
Acute hyperglycaemia was uniquely associated with the haematopoietic growth factor GM-CSF. A similar association has, to our knowledge, not been previously described in patients with CAP. GM-CSF plays a crucial role in innate immunity by promoting the production, maturation, and inflammatory activation of myeloid cells, such as monocytes and neutrophils (55). Another essential function of GM-CSF during the inflammatory response is to repair damaged alveolar epithelium by expanding the alveolar epithelial cells (55). In preclinical studies, GM-CSF has been shown to be protective in animal models of viral and bacterial pneumonia, and GM-CSF has been tested as a therapeutic in patients with alveolar damage due to acute respiratory distress syndrome (56).
The distinct association between acute hyperglycaemia and GM-CSF within the context of CAP is intriguing yet unclear. Nonetheless, our findings align with a study that showed a significant increase in GM-CSF production during acute hyperglycaemia during a hyperglycaemic clamp, with p-glucose levels clamped at 9–11 mmol/L, compared to a euglycaemic clamp with p-glucose clamped at 4–6 mmol/L (57). Thus, our findings suggest an association between acute hyperglycaemia and myeloid cell production in CAP.
To the best of our knowledge, our study is the first to identify an association between acute-on-chronic hyperglycaemia and IL-2 in CAP. IL-2 is primarily produced by activated T cells, and it plays a crucial role in the differentiation and function of Th cell effector subsets, cytotoxic T cells, anti-inflammatory T regulatory (Treg) cells, and NK cells (58). Furthermore, our results align with in vitro findings where incubation of CD4+ cells in escalating glucose concentrations led to progressively higher activation of the IL-2 pathway (59).
It was surprising that we did not observe an association between chronic hyperglycaemia and many inflammatory mediators previously associated with chronic hyperglycaemia or type 2 diabetes in non-acutely ill individuals, such as CRP; the pro-inflammatory cytokines IL-1α, IL-6, and TNF-α (47, 48); or the chemokines eotaxin, macrophage inflammatory protein-1α, interferon-gamma inducible protein-10, and monocyte chemoattractant protein-1 (36).
Similar to the largest study (n = 1,895) examining the association between chronic hyperglycaemia stratified by diabetes diagnosis and the inflammatory host response in CAP, we did not find an association between chronic hyperglycaemia and IL-6, TNF-α, or the anti-inflammatory cytokine IL-10 (49). Our study adds to these findings by evaluating the association between chronic hyperglycaemia estimated using HbA1c and inflammatory host response.
One possible explanation is that the intense acute inflammatory response during CAP might mask or outweigh the low-grade inflammatory effects of chronic hyperglycaemia. However, considering the specific associations we found between chronic and other inflammatory mediators, such as the IL-17 cytokine family, chronic hyperglycaemia might be associated with activating specific inflammatory pathways in CAP.
The associations between the three hyperglycaemic measures and the host response mediators observed in this study are not yet understood, highlighting the need for additional research. While acute and acute-on-chronic hyperglycaemia are recognised as risk factors for short-term mortality, diabetes is associated with increased long-term mortality in CAP (12). However, whether the host response mediators identified in this study as associated with chronic, acute, and acute-on-chronic hyperglycaemia mediate the increased CAP mortality risk associated with hyperglycaemia remains an open question.
Our study is the first to investigate the association of chronic, acute, and acute-on-chronic with inflammatory, endothelial, and angiogenic host responses in CAP. We sought to minimise information loss and avoid arbitrary cutoff values, enhance statistical power, and increase the precision of effect estimation by estimating the predictors as continuous variables in our primary analysis.
However, our study has some limitations. We acknowledge that the design of our observational study precludes the ability to establish causality. Additionally, the current body of research limits our capacity to provide a detailed mechanistic explanation for the association of the three hyperglycaemia measures with different sets of host response mediators. These limitations highlight the preliminary nature of our findings and the need for further research. Using raw signal values to estimate the protein concentrations in patients with CAP is novel, and its validity in this population requires further investigation. Although we performed extensive adjustments, residual confounding cannot be ruled out. Moreover, 17% of patients had missing BMI data, which were imputed. However, the directions of the associations were similar when analyses performed with imputed data and complete case analyses were compared. Nevertheless, some associations with admission p-glucose and the glycaemic gap as predictors that were significant in analyses with imputed data were not significant in complete case analyses, probably due to lack of power. Even though we performed extensive adjustment for potential confounders, we cannot rule out residual confounding.
Our findings indicate that chronic, acute, and acute-on-chronic hyperglycaemia were associated with the activation of similar inflammatory, endothelial, and angiogenic host response pathways in patients with CAP. The exceptions were the associations between acute hyperglycaemia and GM-CSF and between acute-on-chronic hyperglycaemia and IL-2, suggesting that acute and acute-on-chronic hyperglycaemia might activate specific inflammatory pathways.
The datasets used for the current study are not publicly available. However, pseudonymised data can be provided by the corresponding author upon a reasonable request.
The studies involving humans were approved by Scientific Ethics Committee at the Capital Region of Denmark. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AD: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. AL: Formal analysis, Methodology, Supervision, Writing – review & editing. CR: Data curation, Writing – review & editing. MH: Data curation, Writing – review & editing. AJ: Conceptualization, Supervision, Writing – review & editing. PK: Conceptualization, Supervision, Writing – review & editing. RK-M: Conceptualization, Supervision, Writing – review & editing. DF: Conceptualization, Data curation, Supervision, Writing – review & editing. SO: Data curation, Writing – review & editing. KB: Data curation, Formal Analysis, Writing – review & editing. BL: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Financial support for this study was provided by the Research Council at Copenhagen University Hospital, North Zealand, Grosserer L. F. Foghts Fond, Olga Bryde Nielsens Fond, Helen Rudes Fond, Kaptajnløjtnant Harald Jensens og Hustrus Fond, and Fonden til Lægevidenskabens Fremme. The study’s funders did not impact the study design, data collection, data analysis, interpretation, manuscript writing, or publication decision.
The research nurses Hanne Hallager, Malene Pilegaard Schønnemann, and Christina Brix (Department of Pulmonary and Infectious Diseases, Copenhagen University Hospital, North Zealand, Denmark) assisted with enrolling study participants and data collection, which we gratefully acknowledge.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1372300/full#supplementary-material
1. Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL. Measuring population ageing: an analysis of the Global Burden of Disease Study 2017. Lancet Public Health. (2019) 4:e159–67. doi: 10.1016/S2468-2667(19)30019-2
2. Torres A, Cilloniz C, Niederman MS, Menéndez R, Chalmers JD, Wunderink RG, et al. Pneumonia. Nat Rev Dis Primers. (2021) 7:1–28. doi: 10.1038/s41572-021-00259-0
3. Yende S, van der Poll T, Lee M, Huang DT, Newman AB, Kong L, et al. The influence of pre-existing diabetes mellitus on the host immune response and outcome of pneumonia: analysis of two multicentre cohort studies. Thorax. (2010) 65:870–7. doi: 10.1136/thx.2010.136317
4. Bendib I, Beldi-Ferchiou A, Schlemmer F, Surenaud M, Maitre B, Plonquet A, et al. Alveolar compartmentalization of inflammatory and immune cell biomarkers in pneumonia-related ARDS. Crit Care. (2021) 25:23. doi: 10.1186/s13054-020-03427-y
5. Feng CM, Wang XM, Li MD, Xu Z, Hua DX, Cheng JY, et al. Serum interleukin-17 predicts severity and prognosis in patients with community acquired pneumonia: a prospective cohort study. BMC Pulm Med. (2021) 21:393. doi: 10.1186/s12890-021-01770-6
6. Dolmatova EV, Wang K, Mandavilli R, Griendling KK. The effects of sepsis on endothelium and clinical implications. Cardiovasc Res. (2021) 117:60–73. doi: 10.1093/cvr/cvaa070
7. Schuurman AR, Reijnders TDY, van Engelen TSR, Léopold V, de Brabander J, van Linge C, et al. The host response in different aetiologies of community-acquired pneumonia. EBioMedicine. (2022) 81:104082. doi: 10.1016/j.ebiom.2022.104082
8. Chang PY, Tsao SM, Chang JH, Chien MH, Hung WY, Huang YW, et al. Plasma levels of soluble intercellular adhesion molecule-1 as a biomarker for disease severity of patients with community-acquired pneumonia. Clin Chim Acta. (2016) 463:174–80. doi: 10.1016/j.cca.2016.10.030
9. Yang KY, Liu KT, Chen YC, Chen CS, Lee YC, Perng RP, et al. Plasma soluble vascular endothelial growth factor receptor-1 levels predict outcomes of pneumonia-related septic shock patients: a prospective observational study. Crit Care. (2011) 15:R11. doi: 10.1186/cc9412
10. Jensen AV, Faurholt-Jepsen D, Egelund GB, Andersen SB, Petersen PT, Benfield T, et al. Undiagnosed diabetes mellitus in community-acquired pneumonia: A prospective cohort study. Clin Infect Dis. (2017) 65:2091–8. doi: 10.1183/1393003.congress-2017.PA4104
11. Daryabor G, Atashzar MR, Kabelitz D, Meri S, Kalantar K. The effects of type 2 diabetes mellitus on organ metabolism and the immune system. Front Immunol. (2020) 11:1582. doi: 10.3389/fimmu.2020.01582
12. Barmanray RD, Cheuk N, Fourlanos S, Greenberg PB, Colman PG, Worth LJ. In-hospital hyperglycemia but not diabetes mellitus alone is associated with increased in-hospital mortality in community-acquired pneumonia (CAP): a systematic review and meta-analysis of observational studies prior to COVID-19. BMJ Open Diabetes Res Care. (2022) 10:e002880. doi: 10.1136/bmjdrc-2022-002880
13. Jensen AV, Baunbæk Egelund G, Bang Andersen S, Petersen PT, Benfield T, Witzenrath M, et al. The glycemic gap and 90-day mortality in community-acquired pneumonia. A prospective cohort study. Ann Am Thorac Soc. (2019) 16:1518–26. doi: 10.1513/AnnalsATS.201901-007OC
14. Jensen AV, Egelund GB, Andersen SB, Trier Petersen P, Benfield T, Faurholt-Jepsen D, et al. The impact of blood glucose on community-acquired pneumonia: a retrospective cohort study. ERJ Open Res. (2017) 3(2):00114–2016. doi: 10.1183/1393003.congress-2017.PA4104
15. Popov D. Endothelial cell dysfunction in hyperglycemia: Phenotypic change, intracellular signaling modification, ultrastructural alteration, and potential clinical outcomes. Int J Diabetes Mellitus. (2010) 2:189–95. doi: 10.1016/j.ijdm.2010.09.002
16. Jafar N, Edriss H, Nugent K. The effect of short-term hyperglycemia on the innate immune system. Am J Med Sci. (2016) 351:201–11. doi: 10.1016/j.amjms.2015.11.011
17. Da Porto A, Tascini C, Colussi G, Peghin M, Graziano E, De Carlo C, et al. Relationship between cytokine release and stress hyperglycemia in patients hospitalized with COVID-19 infection. Front Med (Lausanne). (2022) 9:988686. doi: 10.3389/fmed.2022.988686
18. Lim S, Bae JH, Kwon HS, Nauck MA. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol. (2021) 17:11–30. doi: 10.1038/s41574-020-00435-4
19. Ryrsø CK, Hegelund MH, Dungu AM, Faurholt-Jepsen D, Pedersen BK, Ritz C, et al. Association between barthel index, grip strength, and physical activity level at admission and prognosis in community-acquired pneumonia: A prospective cohort study. J Clin Med. (2022) 11:6326. doi: 10.3390/jcm11216326
20. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
21. Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. (2003) 58:377–82. doi: 10.1136/thorax.58.5.377
22. Cheng GS, Crothers K, Aliberti S, Bergeron A, Boeckh M, Chien JW, et al. Immunocompromised host pneumonia: definitions and diagnostic criteria: an official american thoracic society workshop report. Ann ATS. (2023) 20:341–53. doi: 10.1513/AnnalsATS.202212-1019ST
23. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. (2019) 42:S13–28. doi: 10.2337/dc19-S002
24. Holter JC, Müller F, Bjørang O, Samdal HH, Marthinsen JB, Jenum PA, et al. Etiology of community-acquired pneumonia and diagnostic yields of microbiological methods: a 3-year prospective study in Norway. BMC Infect Dis. (2015) 15:64. doi: 10.1186/s12879-015-0803-5
25. Furman D, Campisi J, Verdin E, Carrera-Bastos P, Targ S, Franceschi C, et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. (2019) 25:1822–32. doi: 10.1038/s41591-019-0675-0
26. Stotts C, Corrales-Medina VF, Rayner KJ. Pneumonia-induced inflammation, resolution and cardiovascular disease: causes, consequences and clinical opportunities. Circ Res. (2023) 132:751–74. doi: 10.1161/CIRCRESAHA.122.321636
27. Quinton LJ, Walkey AJ, Mizgerd JP. Integrative physiology of pneumonia. Physiol Rev. (2018) 98:1417–64. doi: 10.1152/physrev.00032.2017
28. Langouche L, Vanhorebeek I, Vlasselaers D, Vander Perre S, Wouters PJ, Skogstrand K, et al. Intensive insulin therapy protects the endothelium of critically ill patients. J Clin Invest. (2005) 115:2277–86. doi: 10.1172/JCI25385
29. Esposito K, Nappo F, Marfella R, Giugliano G, Giugliano F, Ciotola M, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. (2002) 106:2067–72. doi: 10.1161/01.CIR.0000034509.14906.AE
30. Straczkowski M, Kowalska I, Nikolajuk A, Dzienis-Straczkowska S, Szelachowska M, Kinalska I. Plasma interleukin 8 concentrations in obese subjects with impaired glucose tolerance. Cardiovasc Diabetol. (2003) 2:5. doi: 10.1186/1475-2840-2-5
31. The International Expert Committee. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care. (2009) 32:1327–34. doi: 10.2337/dc09-9033
32. Dungan KM, Braithwaite SS, Preiser JC. Stress hyperglycaemia. Lancet. (2009) 373:1798–807. doi: 10.1016/S0140-6736(09)60553-5
33. Matsushima K, Yang D, Oppenheim JJ. Interleukin-8: An evolving chemokine. Cytokine. (2022) 153:155828. doi: 10.1016/j.cyto.2022.155828
34. Pinargote-Celorio H, Miralles G, Cano M, Caparros E, Portilla J, González-Alcaide G, et al. Cytokine levels predict 30-day mortality in octogenarians and nonagenarians with community-acquired pneumonia: a retrospective observational study. Eur J Clin Microbiol Infect Dis. (2020) 39:299–307. doi: 10.1007/s10096-019-03725-6
35. Perera PY, Lichy JH, Waldmann TA, Perera LP. The role of Interleukin-15 in inflammation and immune responses to infection: implications for its therapeutic use. Microbes Infect. (2012) 14:247–61. doi: 10.1016/j.micinf.2011.10.006
36. Pan X, Kaminga AC, Wen SW, Liu A. Chemokines in prediabetes and type 2 diabetes: A meta-analysis. Front Immunol. (2021) 12:622438. doi: 10.3389/fimmu.2021.622438
37. Kuczyński S, Winiarska H, Abramczyk M, Szczawińska K, Wierusz-Wysocka B, Dworacka M. IL-15 is elevated in serum patients with type 1 diabetes mellitus. Diabetes Res Clin Practice. (2005) 69:231–6. doi: 10.1016/j.diabres.2005.02.007
38. Duan Y, Li F, Wang W, Guo Q, Wen C, Li Y, et al. Interleukin-15 in obesity and metabolic dysfunction: current understanding and future perspectives. Obes Rev. (2017) 18:1147–58. doi: 10.1111/obr.12567
39. McGeachy MJ, Cua DJ, Gaffen SL. The IL-17 family of cytokines in health and disease. Immunity. (2019) 50:892–906. doi: 10.1016/j.immuni.2019.03.021
40. Zi C, He L, Yao H, Ren Y, He T, Gao Y. Changes of Th17 cells, regulatory T cells, Treg/Th17, IL-17 and IL-10 in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Endocrine. (2022) 76:263–72. doi: 10.1007/s12020-022-03043-6
41. Zhou T, Hu Z, Yang S, Sun L, Yu Z, Wang G. Role of adaptive and innate immunity in type 2 diabetes mellitus. J Diabetes Res. (2018) 2018:7457269. doi: 10.1155/2018/7457269
42. Abdel-Moneim A, Bakery HH, Allam G. The potential pathogenic role of IL-17/Th17 cells in both type 1 and type 2 diabetes mellitus. Biomed Pharmacother. (2018) 101:287–92. doi: 10.1016/j.biopha.2018.02.103
43. Zhang D, Jin W, Wu R, Li J, Park SA, Tu E, et al. High glucose intake exacerbates autoimmunity through reactive-oxygen-species-mediated TGF-β Cytokine activation. Immunity. (2019) 51:671–681.e5. doi: 10.1016/j.immuni.2019.08.001
44. Rauniyar K, Jha SK, Jeltsch M. Biology of vascular endothelial growth factor C in the morphogenesis of lymphatic vessels. Front Bioeng Biotechnol. (2018) 6:7. doi: 10.3389/fbioe.2018.00007
45. Huang YL, Lin YC, Lin CC, Chen WM, Chen BPC, Lee H. High glucose induces VEGF-C expression via the LPA1/3-akt-ROS-LEDGF signaling axis in human prostate cancer PC-3 cells. Cell Physiol Biochem. (2018) 50:597–611. doi: 10.1159/000494177
46. Turner MD, Nedjai B, Hurst T, Pennington DJ. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim Biophys Acta (BBA) Mol Cell Res. (2014) 1843:2563–82. doi: 10.1016/j.bbamcr.2014.05.014
47. Tejera A, Santolaria F, Diez ML, Alemán-Valls MR, González-Reimers E, Martínez-Riera A, et al. Prognosis of community acquired pneumonia (CAP): value of triggering receptor expressed on myeloid cells-1 (TREM-1) and other mediators of the inflammatory response. Cytokine. (2007) 38:117–23. doi: 10.1016/j.cyto.2007.05.002
48. Frühbeck G, Catalán V, Ramírez B, Valentí V, Becerril S, Rodríguez A, et al. Serum levels of IL-1 RA increase with obesity and type 2 diabetes in relation to adipose tissue dysfunction and are reduced after bariatric surgery in parallel to adiposity. J Inflamm Res. (2022) 15:1331–45. doi: 10.2147/JIR.S354095
49. Farooq N, Chuan B, Mahmud H, El Khoudary SR, Nouraie SM, Evankovich J, et al. Association of the systemic host immune response with acute hyperglycemia in mechanically ventilated septic patients. PloS One. (2021) 16:e0248853. doi: 10.1371/journal.pone.0248853
50. Wu FTH, Stefanini MO, Gabhann FM, Kontos CD, Annex BH, Popel AS. A systems biology perspective on sVEGFR1: its biological function, pathogenic role and therapeutic use. J Cell Mol Med. (2010) 14:528–52. doi: 10.1111/j.1582-4934.2009.00941.x
51. Nandy D, Mukhopadhyay D, Basu A. Both vascular endothelial growth factor and soluble Flt-1 are increased in type 2 diabetes but not in impaired fasting glucose. J Investig Med. (2010) 58:804–6. doi: 10.2310/JIM.0b013e3181e96203
52. Fadini GP, Albiero M, Bonora BM, Avogaro A. Angiogenic abnormalities in diabetes mellitus: mechanistic and clinical aspects. J Clin Endocrinol Metab. (2019) 104:5431–44. doi: 10.1210/jc.2019-00980
53. Troncoso MF, Ortiz-Quintero J, Garrido-Moreno V, Sanhueza-Olivares F, Guerrero-Moncayo A, Chiong M, et al. VCAM-1 as a predictor biomarker in cardiovascular disease. Biochim Biophys Acta Mol Basis Dis. (2021) 1867:166170. doi: 10.1016/j.bbadis.2021.166170
54. Rasul S, Reiter MH, Ilhan A, Lampichler K, Wagner L, Kautzky-Willer A. Circulating angiopoietin-2 and soluble Tie-2 in type 2 diabetes mellitus: a cross-sectional study. Cardiovasc Diabetol. (2011) 10:55. doi: 10.1186/1475-2840-10-55
55. McCormick TS, Hejal RB, Leal LO, Ghannoum MA. GM-CSF: orchestrating the pulmonary response to infection. Front Pharmacol. (2022) 12:735443. doi: 10.3389/fphar.2021.735443
56. Herold S, Hoegner K, Vadász I, Gessler T, Wilhelm J, Mayer K, et al. Inhaled granulocyte/macrophage colony–stimulating factor as treatment of pneumonia-associated acute respiratory distress syndrome. Am J Respir Crit Care Med. (2014) 189:609–11. doi: 10.1164/rccm.201311-2041LE
57. Cherney DZI, Scholey JW, Sochett E, Bradley TJ, Reich HN. The acute effect of clamped hyperglycemia on the urinary excretion of inflammatory cytokines/chemokines in uncomplicated type 1 diabetes. Diabetes Care. (2011) 34:177–80. doi: 10.2337/dc10-1219
58. Boyman O, Sprent J. The role of interleukin-2 during homeostasis and activation of the immune system. Nat Rev Immunol. (2012) 12:180–90. doi: 10.1038/nri3156
Keywords: admission p-glucose, community-acquired pneumonia, glycaemic gap, glycated haemoglobin (HbA1c), host response mediators, hyperglycaemia
Citation: Dungu AM, Lundgaard AT, Ryrsø CK, Hegelund MH, Jensen AV, Kristensen PL, Krogh-Madsen R, Faurholt-Jepsen D, Ostrowski SR, Banasik K and Lindegaard B (2024) Inflammatory and endothelial host responses in community-acquired pneumonia: exploring the relationships with HbA1c, admission plasma glucose, and glycaemic gap—a cross-sectional study. Front. Immunol. 15:1372300. doi: 10.3389/fimmu.2024.1372300
Received: 17 January 2024; Accepted: 22 April 2024;
Published: 22 May 2024.
Edited by:
Elzbieta Kolaczkowska, Jagiellonian University, PolandReviewed by:
Estibalitz Laresgoiti-Servitje, Tecnológico de Monterrey, MexicoCopyright © 2024 Dungu, Lundgaard, Ryrsø, Hegelund, Jensen, Kristensen, Krogh-Madsen, Faurholt-Jepsen, Ostrowski, Banasik and Lindegaard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arnold Matovu Dungu, YXJub2xkLm1hdG92dS5kdW5ndUByZWdpb25oLmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.