 Nansi López-Valverde
Nansi López-Valverde Antonio López-Valverde
Antonio López-Valverde José Antonio Blanco Rueda2
José Antonio Blanco Rueda2- 1Department of Medicine and Medical Specialties, Faculty of Health Sciences, University of Alcalá de Henares, Madrid, Spain
- 2Department of Surgery, Instituto de Investigación Biomédica de Salamanca (IBSAL), University of Salamanca, Salamanca, Spain
Background: Peri-implant diseases (peri-implant mucositis and peri-implantitis) are pathologies of an infectious-inflammatory nature of the mucosa around dental implants. Probiotics are microorganisms that regulate host immunomodulation and have shown positive results in the treatment of peri-implant diseases. The objective of the systematic review and meta-analysis was to evaluate the efficacy of probiotics in the treatment of peri-implant oral diseases.
Methods: According to the PRISMA guidelines, the research question was established: Are probiotics able to favorably modify clinical and immunological biomarkers determinants of peri-implant pathologies? and an electronic search of the databases MEDLINE/PubMed, Embase, Cochrane Central, Web of Science, (until December 2023) was performed. Inclusion criteria were established for intervention studies (RCTs), according to the PICOs strategy in subjects with peri-implant pathology (participants), treated with probiotics (intervention) compared to patients with conventional treatment or placebo (control) and evaluating the response to treatment (outcomes). Results- 1723 studies were obtained and 10 were selected. Risk of bias was assessed using the Cochrane Risk of Bias Tool and methodological quality using the Joanna Briggs Institute for RCTs. Two meta-analyses were performed, one to evaluate probiotics in mucositis and one for peri-implantitis. All subgroups were homogeneous (I2 = 0%), except in the analysis of IL-6 in mucositis (I2 = 65%). The overall effect was favorable to the experimental group in both pathologies. The analysis of the studies grouped in peri-implantitis showed a tendency to significance (p=0.09).
Conclusion: The use of probiotics, as basic or complementary treatment of peri-implant diseases, showed a statistically significant trend, but well-designed studies are warranted to validate the efficacy of these products in peri-implant pathologies.
1 Introduction
Peri-implant oral diseases (peri-implant mucositis and peri-implantitis) are a group of pathologies of an infectious nature, which describe, in the case of peri-implant mucositis, an inflammatory lesion of the mucosa surrounding a dental implant, while in peri-implantitis the supporting bone is affected. The most important parameter for the diagnosis of peri-implant mucositis is bleeding on probing, with a gentle pressure of less than 0.25 N; however, in peri-implantitis alterations appear at the crestal bone level and the presence of purulent fluid in the affected areas is frequent (1). This last aspect is the reason why peri-implantitis, unlike mucositis, is considered an irreversible pathology (2).
The consensus of the Sixth European Workshop on Periodontology (3) reported an incidence of mucositis in dental implants of up to 80% and between 28% and 56% of peri-implantitis, despite the controversy surrounding these high figures (4). This leads to failure of the implanted device, with consequent economic damage (5).
Peri-implantitis is considered a polymicrobial infection associated with Staphylococcus epidermidis and specific gram-negative periodontopathogens, such as Porphyromonas gingivalis, Tannerella forsythia, Fusobacterium nucleatum and Porphyromona intermedia (6) and although the mechanism of the microbial interaction is not precisely known, according to recent sequencing studies, a great diversity of bacterial species are considered responsible (7).
The term probiotic is used to define health-promoting substances released by one organism to enhance the development of another, and probiotics are known to be beneficial microbes that influence health through host immunomodulation and modulation of the bacteriome (8, 9). Several studies have found a positive association between the use of certain probiotic bacterial strains and oral health (10, 11), as well as those certain strains of lactobacilli, have anti-inflammatory capacity and reduce periodontal pathogens in the oral biofilm (12–14) and, precisely in this sense, have begun to be used for the treatment of peri-implantitis (15, 16). It has been shown that biofilms facilitate greater resistance to microorganisms, which translates into greater success in colonization and maintenance of the bacterial population (17), which is why certain biofilm-related infections, such as peri-implantitis, constitute an important clinical problem for the correct functioning and long-term survival of implanted devices (18).
A cause-effect relationship has been demonstrated between the accumulation of bacterial biofilms around titanium dental implants and the development of an inflammatory response (19) and that the clinical parameters evaluated returned to healthy levels after 21 days of biofilm control (20). However, biofilm control escapes both the immune system and the action of numerous antimicrobials, posing a danger to the survival of dental implants (21, 22) and that is, the use of probiotics and their derivatives has gained increasing interest in the fight against oral biofilms, with the aim of inhibiting their maturation and growth (23).
Biofilms together with the breakdown products of peri-implant bone tissue, in the case of peri-implantitis, appear to result in a local immune response in the infected tissue and the production of proinflammatory cytokines such as IL-1β, associated with the stimulation of fibroblasts, endothelial cells and osteoclasts (24). IL-6 also induces bone resorption and, moreover, acts synergistically together with IL-1β, and it has been shown that the levels of both cytokines in peri-implant gingivocrevicular fluid (PGF) are higher in areas with peri-implantitis than in healthy areas (25), although cytokine levels in healthy areas are not perfectly defined (26).
For all these reasons, the aim of the present systematic and meta-analytic approach of randomized clinical studies was to evaluate the efficacy of probiotics in the treatment of peri-implant oral diseases.
2 Methods
2.1 Study presentation and registration
This systematic review has been prepared according to “The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (27) and the guidelines of the Clinical Practice Guidelines (28). The protocol of this systematic review has been registered in INPLASY under the number: INPLASY202410051, doi number: 10.37766/inplasy2024.1.0051.
2.2 Question of interest, PICOs format
The focus of the research question was elaborated according to the PICOs format: “Are probiotics able to favorably modify clinical and immunological biomarkers determinants of peri-implant pathologies?”. Intervention studies in adult patients with mucositis, peri-implantitis or both (P) comparing probiotic treatment alone, or as adjuvant therapy (I) with patients receiving conventional treatment or placebo (C) were included to observe effects on clinical and immunological parameters (O), with only randomized clinical studies considered (Table 1).
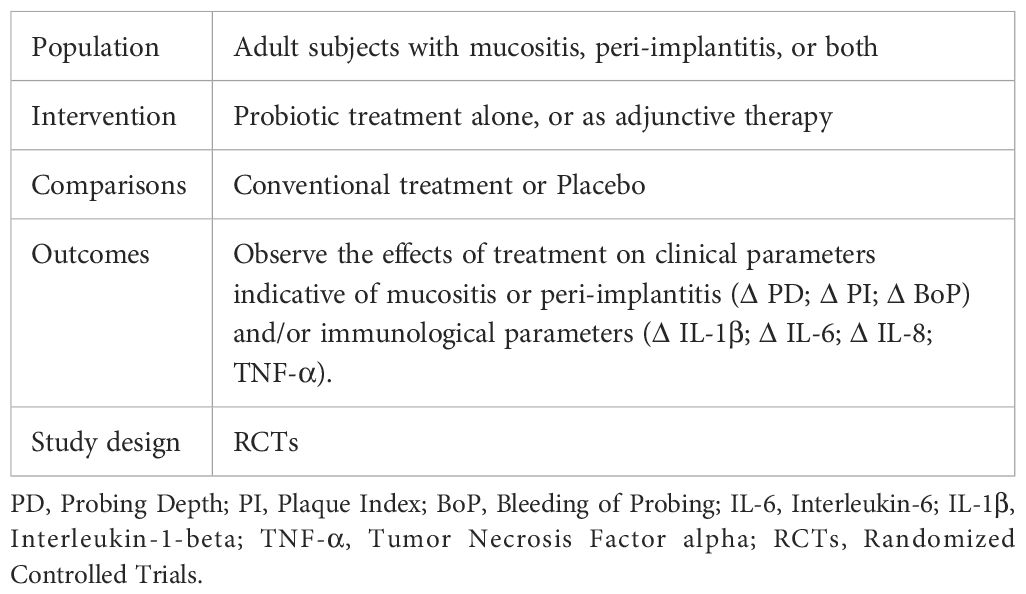
Table 1 PICOs format.
PD, Probing Depth; PI, Plaque Index; BoP, Bleeding of Probing; IL-6, Interleukin-6; IL-1β, Interleukin-1-beta; TNF-α, Tumor Necrosis Factor alpha; RCTs, Randomized Controlled Trials.
2.3 Studies selection, eligibility criteria
The original research studies were selected according to the following inclusion criteria: (i) randomized clinical trials (single or double blind) that included in the study more than 10 subjects ≥ 18 years of age; (ii) with peri-implant pathologies; (iii) that provided data on clinical parameters and/or immunological follow-up indicative of peri-implant disease; (iv) with statistical methods that included mean numerical values and standard deviation, together with units with which to quantify mediator levels; (v) published in English. Studies that did not follow all the criteria defined above, with lack of relevant or demonstrative data on peri-implant disease, preclinical studies or in vitro studies, case series or clinical cases, literature reviews and irrelevant studies (editorial letters, conference abstracts, historical reviews…) were excluded.
2.4 Search approach
Two reviewers (NL-V, AL-V) independently searched four electronic databases (MEDLINE/PubMed, Embase, Cochrane Central, Web of Science) until December 2023, using the terms Medical Subject Headings (MeSH): Peri-Implantitis*/diagnosis OR Peri-Implantitis*/prevention & control OR Mucositis* AND Dental Implants* AND Dental Plaque* AND Probiotics/therapeutic use* AND Lactobacillus* AND Probiotics*/therapeutic use* AND Humans*. In addition, a manual search and consultations in the gray literature were performed; the bibliographic references of the included studies were also consulted to obtain the most information and avoid bibliographic bias.
2.5 Data collection
The data provided by each included study were extracted and tabulated by two reviewers (NL-V, AL-V) using the standardized data extraction tools of JBI-MAStARI. Both reviewers systematically screened the titles and abstracts of the previously selected studies. Those that met the inclusion criteria were extracted for reading and data extraction. Discrepancies between reviewers were resolved by discussion and judgment of a third reviewer (JABR). Cohen’s kappa index (κ) (29) was used to assess inter-reviewer agreement.
Because all included articles were randomized studies, the JBI-MAStARI Data Extraction Form for Randomized Controlled Trials was used. Data extracted from the studies included specific details about the interventions, populations, study methods, specific objectives, and significant outcomes to formulate the question of interest. All results were subjected to double data entry to minimize error bias.
2.6 Methodological rigor of the studies
The studies included in this systematic review and meta-analysis were methodologically evaluated using the tool developed by the Joanna Briggs Institute for RCTs (JBI MAStARI) which takes a particular view of the evidence and the methods used to synthesize the different types of evidence. The checklist consists of thirteen items and the responses to the items are “yes”, “no”, “unclear” or “not applicable”. The answer “yes” scores one point. To include a study, it had to score seven or more (30).
2.7 Risk of bias
Two assessors (NL-V and AL-V) independently assessed the risk of bias of the studies using the Cochrane Risk of Bias Tool (RoB2) (31) which assesses 7 domains of bias: Random sequence generation (Selection bias); Allocation concealment (Selection bias); Blinding of participants and staff (Performance bias); Blinding of outcome assessment (Detection bias); Incomplete outcome data (Attrition bias). Studies were assessed with “high”, “low” and “borderline” risk of bias; “borderline” risk of bias, was applied to those with a lack of information on possible bias. Discrepancies among the assessors were discussed to reach consensus.
2.8 Data synthesis
Data were analyzed using Review Manager software (RevMan Software. Version 5.4.1; The Cochrane Collaboration, Copenhagen, Denmark; 2020). Meta-analyses were performed for studies assessing peri-implantitis, mucositis and for different clinical and immunological variables, as well as a meta-analysis of pooled studies. All were based on mean difference (MD) and standard deviation (SD) to estimate continuous data and to evaluate categorical data, 95% confidence intervals (CI). Heterogeneity was considered unimportant with I2 = 0-30%; moderate, I2 = 40-50%; substantial I2 = 60-75% and considerable I2≥ 75%. The threshold for statistical significance was set as p < 0.05. Due to the homogeneity of results, a fixed-effects meta-analysis was performed.
3 Results
The electronic search found a total of 1723 results, which constituted 316 unique citations. Eighteen full-text publications were evaluated and 8 were excluded based on a priori criteria (Figure 1).
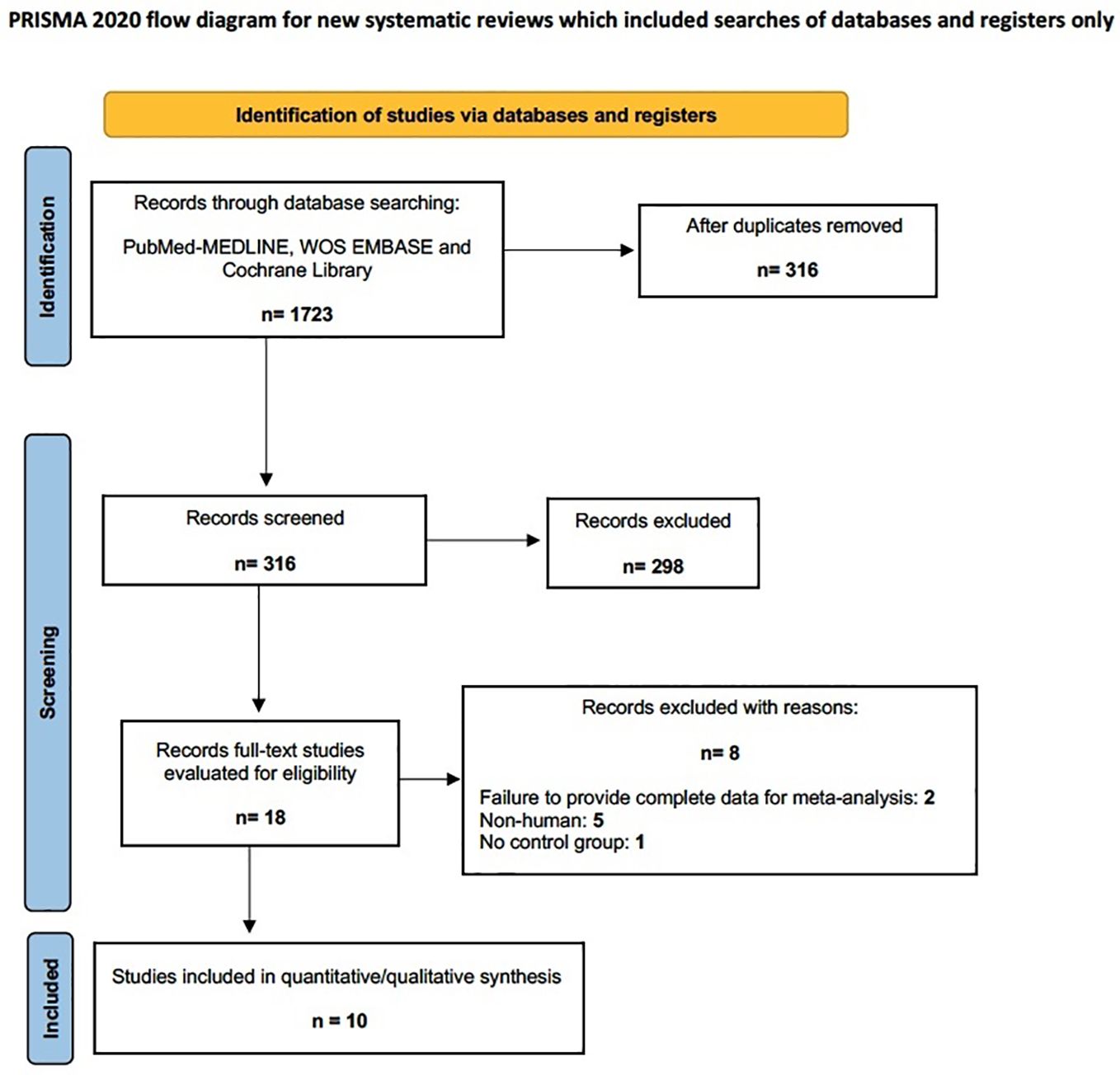
Figure 1 Flow diagram.
3.1 Qualitative analysis, characteristics of the studies
After exclusion, 10 studies were finally included in the meta-analysis (32–41). Inter-reviewer agreement when including studies exceeded 85% (κ > 85%).
A total of 340 patients and 238 implants were studied; however, 4 studies did not report the number of implants studied (33, 35, 37, 39). Follow-up periods ranged from 4 to 24 weeks. Two studies evaluated peri-implant pathology (35, 36) and only one (41) evaluated crestal bone loss (CBL). Regarding clinical evaluation, in the studies that assessed mucositis (32–34, 36–39), the clinical parameters PD and PI were evaluated in 5 studies (32, 33, 36, 38, 41) and BoP in 6 other studies (33, 36, 38–41). The most complete studies were those of Flichy-Fernandez et al. and Santana et al. (32, 39). Regarding immunologic evaluation, 3 studies evaluated cytokines IL-6, IL-8 and IL-1β (32, 33, 39) and only 2 studies evaluated TNF-α (33, 39). The study by Lauritano et al. (37) provided the least amount of analyzable data. The characteristics of the studies are shown in Table 2.
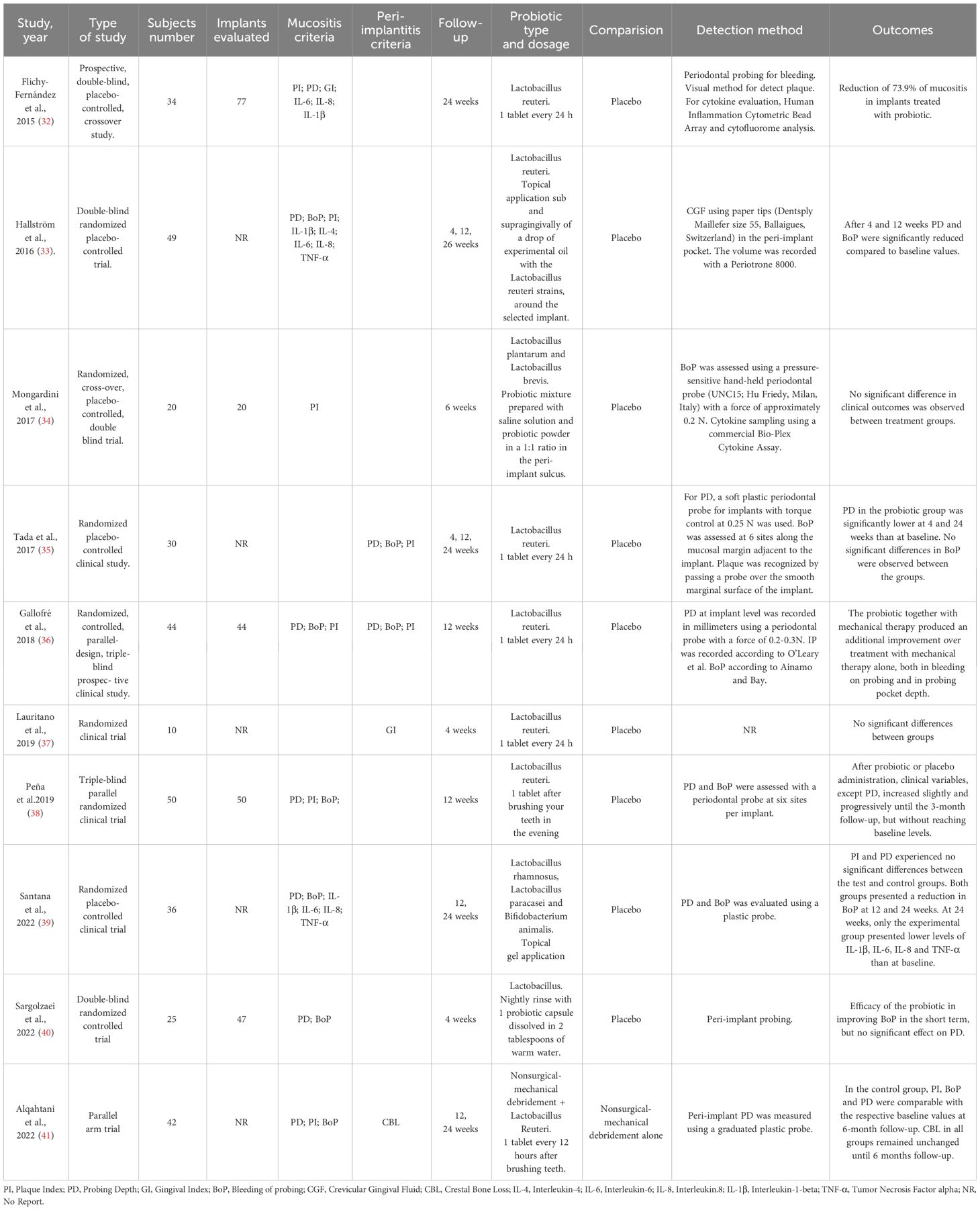
Table 2 Characteristics of studies and participants included in the systematic review.
3.2 Assessment of methodological rigor
The methodological quality of all included studies ranged from high (10 points) to very high (>10 points), as determined by the JBI-MAStARI critical appraisal checklist for RCTs. Only two studies (37, 40) were not evaluated due to missing data. (Table 3).

Table 3 Results of critical appraisal for Randomized Controlled Trials (JBI MAStARI).
3.3 Meta-analysis, risk of bias
For the meta-analysis, only 9 studies were used, as the study by Lauritano et al. (37) was not used because it did not provide analyzable data.
GI variables in mucositis and CBL in peri-implantitis, were not analyzed in the meta-analysis because they were evaluated by only one study each [32 and 41, respectively].
Two meta-analyses were performed, one for studies evaluating probiotics in mucositis and one for studies evaluating probiotics in peri-implantitis. Clinical and immunological parameters and an analysis of grouped variables in both cases (mucositis and peri-implantitis) were analyzed independently. All subgroups were homogeneous (I2 = 0%), except in the analysis of IL-6 in mucositis (32–34, 39), which resulted in substantial heterogeneity (I2 = 65%). In both mucositis and peri-implantitis, the overall effect was in favor of the experimental group. Although not statistically significant, the analysis of studies grouped in peri-implantitis showed a trend towards significance (p=0.09).
No adverse effect analysis was performed due to lack of data.
Risk of bias assessment is one of the pillars of evidence-based medicine; therefore, two reviewers (NL-V and AL-V) independently analyzed the quality of the included studies according to the Cochrane Risk of Bias tool (42). Disagreements between reviewers were resolved by consensus or discussion. The tool evaluates randomized studies in 5 domains: (1) the randomization process; (2) deviations from the intended interventions; (3) missing outcome data; (4) outcome measurement; and (5) selection of the reported outcome and a sixth bias relating to (6) other biases. According to the Cochrane Handbook for Systematic Reviews of Interventions, a “high” rating was given to studies considered at high risk of bias, “low” to those at low risk of bias, and “borderline” to those with uncertain bias or lack of information on potential bias. However, some studies included randomization software, and it was difficult for the reviewers to know which domains they addressed, so most reported uncertainty in the “other biases” domain. Nevertheless, the studies considered met most of the domains and were considered to have a low risk of bias, except for the study by Sargolzaei et al. (40), which did not provide evaluable data. (Figures 2, 3).
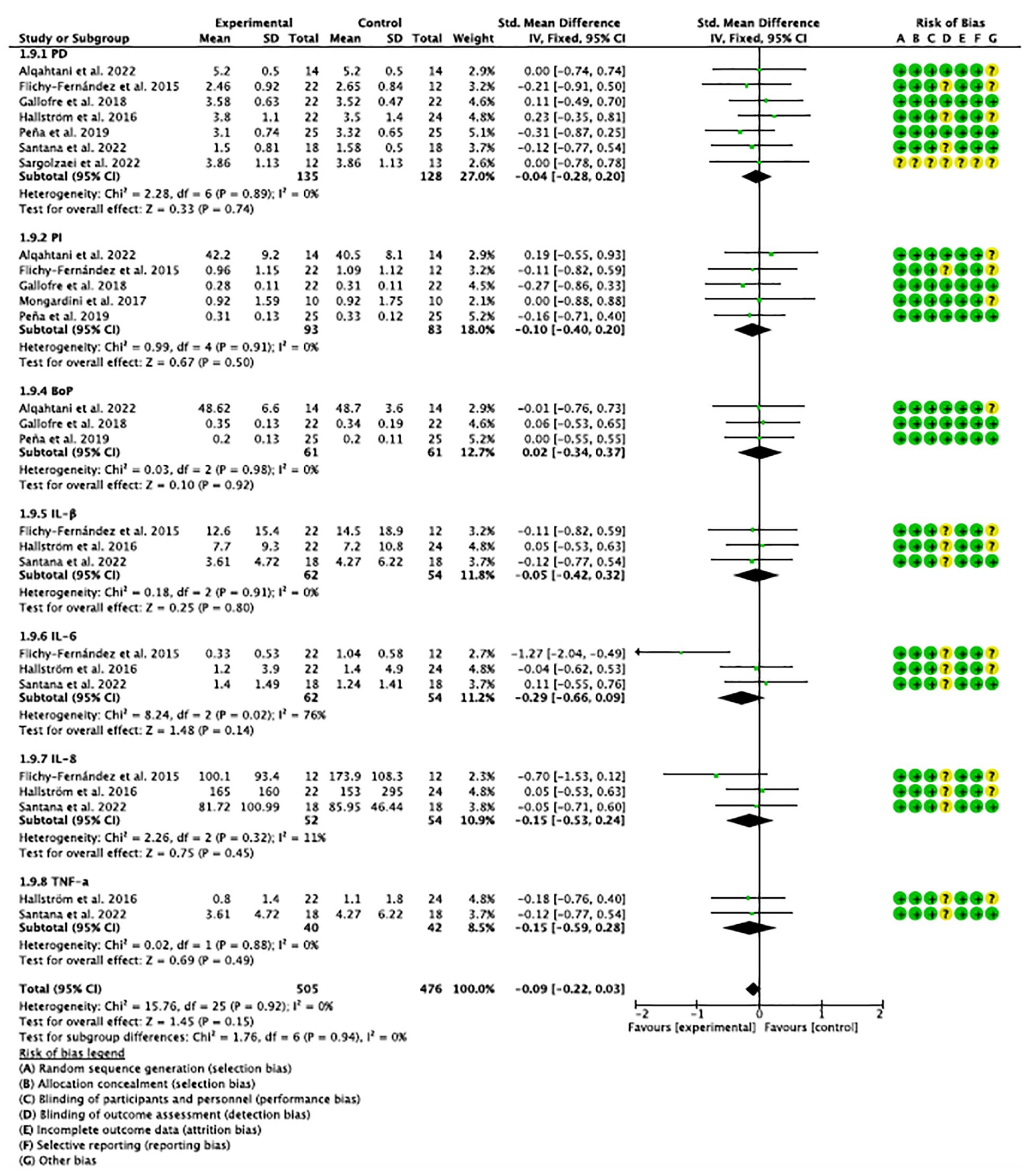
Figure 2 Forest plot and risk of bias (on the side) of studies evaluating clinical and immunological parameters in mucositis.
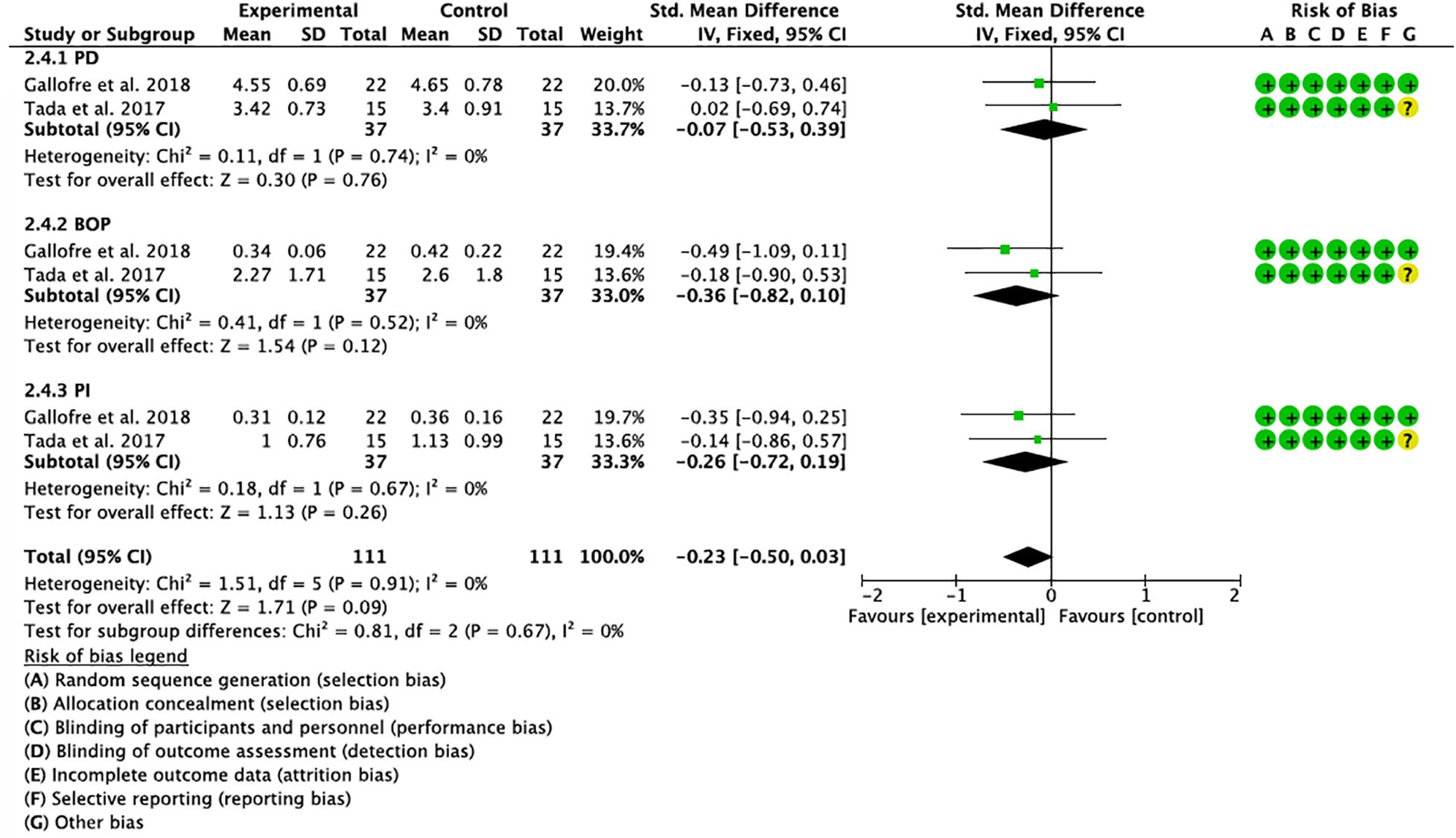
Figure 3 Forest plot and risk of bias (on the side) of studies evaluating clinical parameters in peri-implantitis.
3.4 Publication bias
The graphs in Figures 4, 5, in which the abscissa axis (X) represents the observed results and the ordinate axis (Y) the standard error, show a low asymmetry and, therefore, a low publication bias.
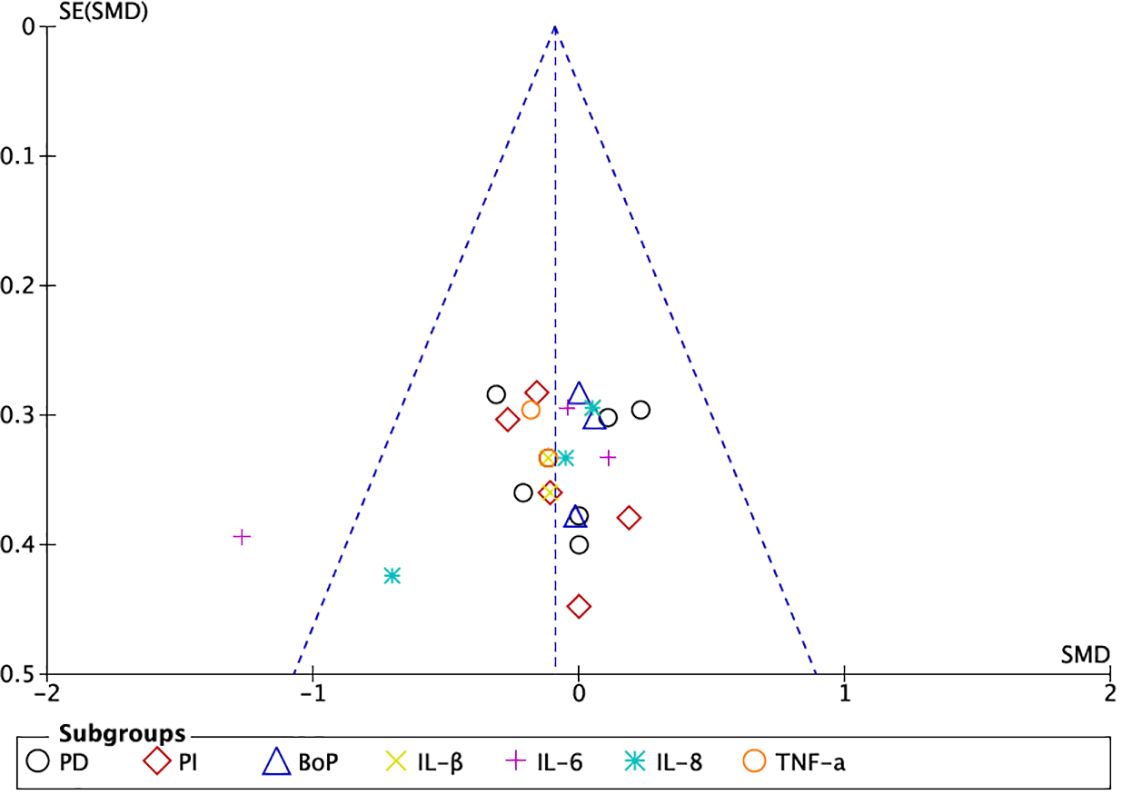
Figure 4 Funnel plot of grouped studies in mucositis.
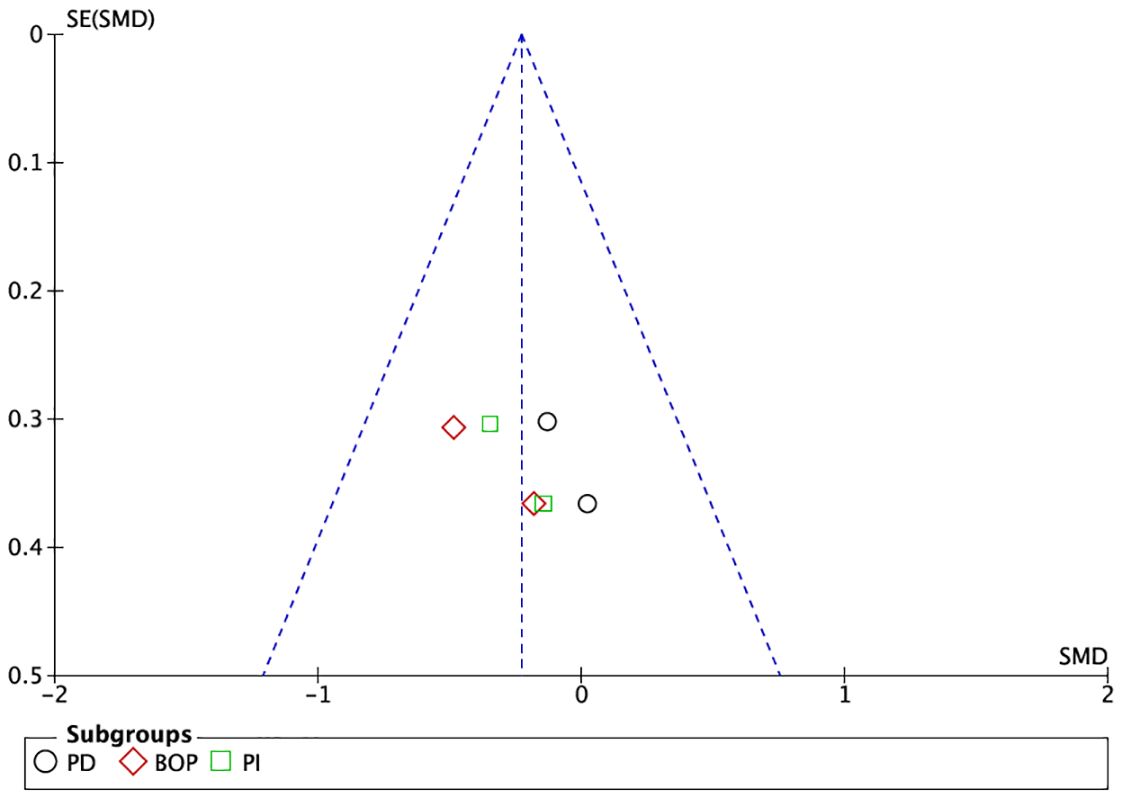
Figure 5 Funnel plot of grouped studies in peri-implantitis.
4 Discussion
4.1 General discussion of results
Nine clinical trials were included in our meta-analysis (32–36, 38–41) and all of them reported beneficial effects of probiotics in the treatment of peri-implant diseases, both for clinical and immunological parameters. Therefore, and taking into consideration the limitations of conventional treatment to solve peri-implant pathologies and especially the inflammatory process, it is interesting to look for therapeutic alternatives, either alone or as adjuvants.
Traditionally, different methods have been applied for the prevention and treatment of peri-implantitis, such as mechanical debridement, surgical therapy with or without regenerative procedures and antibiotics, either local or systemic (43), but it is known that microbial dysbiosis generates inflammatory processes that are difficult to resolve, due to alterations in the immunoinflammatory response of the host; therefore, new treatments that are able to restore the balance of the microbiome and give rise to a healthy oral microbiome are currently being investigated (44). A Cochrane systematic review by Esposito et al. (45) reported that more complex and expensive therapies for the treatment of peri-implantitis were not more beneficial than control therapies, suggesting that, being a chronic pathology, periodic repetition of treatments may be necessary, recommending well-designed RCTs with follow-ups longer than 12 months. Iniesta et al. (46), in a systematic review and meta-analysis demonstrated the beneficial effect of probiotics on clinical inflammatory parameters. In this aspect, our meta-analysis, despite finding an overall favorable effect in the experimental group, did not find statistical significance in any of the groups; only the analysis of studies grouped in peri-implantitis showed a tendency towards significance.
One aspect to take into consideration is the current surfaces of dental implants, which are rougher in order to seek greater bone-implant contact. It has been found that this type of surface, unlike smooth surfaces, in addition to being conducive to the formation of biofilms and bacterial accumulation, makes cleaning difficult when exposed, facilitating peri-implant diseases, although there is no unanimity on these criteria (47, 48). Disruption of host-microbe homeostasis at the implant-mucosa interface caused by biofilm accumulation leads to peri-implant mucositis and optimal removal of biofilm is considered a prerequisite for the prevention and treatment of peri-implant mucositis, a precursor of peri-implantitis (49).
Biomarkers objectively assess biological processes, normal, pathological or in response to a given intervention (50) and are instrumental in the diagnosis and monitoring of peri-implant diseases (51).The cells of the gingival epithelium, fibroblasts, neutrophils and macrophages, release cytokines, such as IL-6, IL-1β and NFα, which cause the degradation of connective tissue and alveolar bone, and about 100 different molecular components have been evaluated in the diagnosis of potential periodontal diseases, although for the diagnosis of peri-implantitis, this number is reduced to half. A recent review by Pliavga et al. (52) involving 1,117 patients with 1,346 implants revealed 49 different biomarkers, with significantly higher values of IL-1β, IL-6 and TNF-α levels in the group of subjects suffering from peri-implantitis. In our meta-analysis, 3 studies (32, 33, 39) evaluated three interleukins (IL-1β, IL-6, IL-8) and only two studies (33, 39) evaluated TNF-α, as indicative of mucositis; however, none of the studies included in our meta-analysis evaluated interleukins as determinants of peri-implantitis, limiting the results, exclusively to clinical parameters. Flichy-Fernandez et al. (32) found statistically significant decreases in IL-1β, IL-6 and IL-8 after probiotic administration; Hallström et al. (33) only found statistical significance in IL-8 and TNF-α values and Santana et al. (39), found lower levels of IL-1β, IL-6, IL-8 and TNF-α, in the group of subjects with mucositis treated with probiotics, only, 24 weeks after the start of the study, finding no differences in shorter time periods.
The effect of probiotics on clinical parameters in peri-implant pathology was evaluated in 8 studies on mucositis (32–34, 36, 38–41) and 2 on peri-implantitis (35, 36), of those included in our meta-analysis.However, the objectives of the studies included after the use of probiotics were discrepant: While most of them studied their effects on mucositis, Tada et al. (35) studied their action on peri-implantitis and Gallofré et al. (36), on both pathologies in patients with associated periodontal pathology. On the other hand, the different studies used different probiotic treatments, dosages and routes of administration. Most of the studies used Lactobacillus reuteri and oral administration; however, Sargolzaei et al. (40) used topical local application and Mongardini et al. (34) combined local and systemic use.
There is controversy about the diagnostic thresholds of peri-implant diseases and about the validity and diagnostic evidence of PD and BoP which, despite having traditionally been clinical markers of periodontal diseases, are not considered as such in peri-implant diseases. The same criterion prevails for CBL and there is no unanimity on whether these parameters could be related to the diagnosis of peri-implant disease (53). One of the studies included in our meta-analysis (41) compared mesial and distal CBL in subjects with adjunctive probiotic treatment, with mechanical debridement alone, finding no differences between groups; however, studies on mucositis (32, 33, 36, 38–41) reported discrepant results for the experimental groups versus placebo: while Flichy-Fernandez et al., Hallström et al., Gallofré et al. (32, 33, 36) reported statistically significant results in decreasing PD, Peña et al., Santana et al., Sargolzaei et al., and Alqahtani et al. (38–41) observed no significant differences between experimental and control groups. Similarly, Tada et al. and Gallofré et al. (35, 36) disagreed on PD measures in peri-implantitis, the former finding no significant differences between the probiotic and placebo groups. We also found discrepant results in studies investigating BoP. Gallofré et al. and Peña et al. (36, 38) reported improvements in bleeding on probing for the probiotic-treated group, both in implants with mucositis and periodontitis, while Santana et al. and Alqahtani et al. (39, 41) found no differences between groups.
In this context of validation of clinical parameters as determinants of peri-implant diseases, these parameters are questioned as indicative of such pathologies. It has been shown that PD and peri-implant soft tissue thickness, is greater in implants than in adjacent teeth (54) and in this regard Doornewaard et al. (53) in a critical review, pointed out a lack of correspondence between PD and BoP values and peri-implant disease.
On the other hand, some studies have shown a genetic disposition on the part of certain subjects to suffer this type of pathology. Cardoso et al. (24) in a pilot study that included a sample of 20 subjects, found a possible relationship between the IL-1 genotype and peri-implantitis, although another larger study on 98 subjects found no differences in the IL-8 polymorphism between groups with peri-implantitis and healthy subjects (55).
Non-surgical treatments of peri-implant diseases include mechanical debridement, adjunctive antiseptic therapy, antibiotic therapy, laser-assisted therapy, adjunctive treatments with natural products and other combined approaches (56), however, in addition to biological parameters, immunoinflammatory mediators have to be considered by clinicians to determine peri-implant health and disease states. In addition, genetic data could contribute to predict the prognosis of treatments.
4.2 Considerations and limitations
The systematic review is essentially an analysis of the evidence in the available scientific literature and a judgment on the efficacy of a treatment, which involves a series of complex steps that can give rise to biases and limitations.
We highlight the latter: the different pathologies analyzed (mucositis and peri-implantitis), with disparate populations and follow-ups and equally different sociodemographic conditions; the different types of probiotic strains used by the studies, their application and comparison; the statistical analyses of the included studies, despite being evaluated as adequate, are unequal. All this biases and may alter the reporting of results. Finally, it should be noted that the Hawthorne effect, which causes behavioral changes in individuals that are observed in epidemiological studies, was only taken into account in the study by Flichy-Fernandez et al. (32) and was not considered in the other included studies.
5 Conclusions
The use of probiotics, either as a basic or complementary treatment of peri-implant diseases, showed a trend towards statistical significance and in view of the increasing demand for alternative natural treatments, they could prove to be a complementary method of treatment of peri-implant diseases.
Well-designed randomized studies are justified and necessary to validate the efficacy of these products in peri-implant pathologies.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
NL-V: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AL-V: Project administration, Writing – original draft, Writing – review & editing. JABR: Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lang NP, Berglundh T. Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now?–Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. (2011) 38, Suppl 11:178–81. doi: 10.1111/j.1600-051X.2010.01674.x
2. Khammissa RA, Feller L, Meyerov R, Lemmer J. Peri-implant mucositis and peri-implantitis: clinical and histopathological characteristics and treatment. SADJ. (2012) 122:124–6.
3. Lindhe J, Meyle J. Group D of european workshop on periodontology. Peri-implant diseases: consensus report of the sixth european workshop on periodontology. J Clin Periodontol. (2008) 35:282–5. doi: 10.1111/j.1600-051X.2008.01283.x
4. Mombelli A, Müller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res. (2012) 23:67–76. doi: 10.1111/j.1600-0501.2012.02541.x
5. Daubert DM, Weinstein BF, Bordin S, Leroux BG, Flemming TF. Prevalence and predictive factors for peri-implant disease and implant failure: a cross-sectional analysis. J Periodontol. (2015) 86:337–47. doi: 10.1902/jop.2014.140438
6. Carvalho ÉBS, Romandini M, Sadilina S, Sant'Ana ACP, Sanz M. Microbiota associated with peri-implantitis-A systematic review with meta-analyses. Clin Oral Implants Res. (2023) 34:1176–87. doi: 10.1111/clr.14153
7. Sun F, Liu J, Li SQ, Wei YP, Hu WJ, Wang C. [Profiles and differences of submucosal microbial in peri-implantitis and health implants: A cross-sectional study]. Beijing Da Xue Xue Bao Yi Xue Ban. (2023) 55:30–7. doi: 10.19723/j.issn.1671-167X.2023.01.005
8. Lilly DM, Stillwell RH. PROBIOTICS: GROWTH-PROMOTING FACTORS PRODUCED BY MICROORGANISMS. Science. (1965) 147:747–8. doi: 10.1126/science.147.3659.747
9. Zidar A, Kristl J, Kocbek P, Zupančič Š. Treatment challenges and delivery systems in immunomodulation and probiotic therapies for periodontitis. Expert Opin Drug Deliv. (2021) 18:1229–44. doi: 10.1080/17425247.2021.1908260
10. Comelli EM, Guggenheim B, Stingele F, Neeser JR. Selection of dairy bacterial strains as probiotics for oral health. Eur J Oral Sci. (2002) 110:218–24. doi: 10.1034/j.1600-0447.2002.21216.x
11. Stamatova I, Meurman JH. Probiotics: health benefits in the mouth. Am J Dent. (2009) 22:329–238.
12. Maekawa T, Hajishengallis G. Topical treatment with probiotic Lactobacillus brevis CD2 inhibits experimental periodontal inflammation and bone loss. J Periodontal Res. (2014) 49:785–91. doi: 10.1111/jre.12164
13. Riccia DN, Bizzini F, Perilli MG, Polimeni A, Trinchieri V, Amicosante G, et al. Anti-inflammatory effects of Lactobacillus brevis (CD2) on periodontal disease. Oral Dis. (2007) 13:376–85. doi: 10.1111/j.1601-0825.2006.01291.x
14. Khalaf H, Nakka SS, Sandén C, Svärd A, Hultenby K, Scherbak N, et al. Antibacterial effects of Lactobacillus and bacteriocin PLNC8 αβ on the periodontal pathogen Porphyromonas gingivalis. BMC Microbiol. (2016) 16:188. doi: 10.1186/s12866-016-0810-8
15. Mulla M, Mulla M, Hegde S, Koshy AV. In vitro assessment of the effect of probiotic lactobacillus reuteri on peri-implantitis microflora. BMC Oral Health. (2021) 21:408. doi: 10.1186/s12903-021-01762-2
16. Mulla M, Hegde S, Koshy A, Mulla M. Effect of probiotic lactobacillus salivarius on peri-implantitis pathogenic bacteria: an in vitro study. Cureus. (2021) 13:e20808. doi: 10.7759/cureus.20808
17. Salas-Jara MJ, Ilabaca A, Vega M, García A. Biofilm forming lactobacillus: new challenges for the development of probiotics. Microorganisms. (2016) 4:35. doi: 10.3390/microorganisms4030035
18. Barzegari A, Kheyrolahzadeh K, Hosseiniyan Khatibi SM, Sharifi S, Memar MY, Zununi Vahed S. The battle of probiotics and their derivatives against biofilms. Infect Drug Resist. (2020) 13:659–72. doi: 10.2147/IDR.S232982
19. Meyer S, Giannopoulou C, Courvoisier D, Schimmel M, Müller F, Mombelli A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin Oral Implants Res. (2017) 28:1005–12. doi: 10.1111/clr.12912
20. Gualini F, Berglundh T. Immunohistochemical characteristics of inflammatory lesions at implants. J Clin Periodontol. (2003) 30:14–8. doi: 10.1034/j.1600-051x.2003.300103.x
21. Sikorska H, Smoragiewicz W. Role of probiotics in the prevention and treatment of meticillin-resistant Staphylococcus aureus infections. Int J Antimicrob. (2013) 42:475–81. doi: 10.1016/j.ijantimicag.2013.08.003
22. Karska-Wysocki B, Bazo M, Smoragiewicz W. Antibacterial activity of Lactobacillus acidophilus and Lactobacillus casei against methicillin-resistant Staphylococcus aureus (MRSA). Microbiol Res. (2010) 165:674–86. doi: 10.1016/j.micres.2009.11.008
23. Cortés-Acha B, Figueiredo R, Blanc V, Soler-Ollé A, León R, Valmaseda-Castellón E. Development and viability of biofilms grown on experimental abutments mimicking dental implants: An in vivo model. Med Oral Patol Oral Cir Bucal. (2019) 24:e511–7. doi: 10.4317/medoral.22868
24. Cardoso JM, Ribeiro AC, Palos C, Proença L, Noronha S, Alves RC. Association between IL-1A and IL-1B gene polymorphisms with peri-implantitis in a Portuguese population-a pilot study. PeerJ. (2022) 10:e13729. doi: 10.7717/peerj.13729
25. Ata-Ali J, Flichy-Fernández AJ, Alegre-Domingo T, Ata-Ali F, Palacio J, Peñarrocha-Diago M. Clinical, microbiological, and immunological aspects of healthy versus peri-implantitis tissue in full arch reconstruction patients: a prospective cross-sectional study. BMC Oral Health. (2015) 15:43. doi: 10.1186/s12903-015-0031-9
26. Javed F, Al-Hezaimi K, Salameh Z, Almas K, Romanos GE. Proinflammatory cytokines in the crevicular fluid of patients with peri-implantitis. Cytokine. (2011) 53:8–12. doi: 10.1016/j.cyto.2010.08.013
27. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
28. Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. Clinical Practice Guidelines We Can Trust. Graham R, Mancher M, Miller Wolman D, Greenfield S, Steinberg E, editors. Washington (DC: National Academies Press (US (2011). doi: 10.17226/13058
29. Casagrande A, Fabris F, Girometti R. Beyond kappa: an informational index for diagnostic agreement in dichotomous and multivalue ordered-categorical ratings. Med Biol Eng Comput. (2020) 58:3089–99. doi: 10.1007/s11517-020-02261-2
30. Barker TH, Stone JC, Sears K, Klugar M, Tufanaru C, Leonardi-Bee J, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid Synth. (2023) 21:494–506. doi: 10.11124/JBIES-22-00430
31. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
32. Flichy-Fernández AJ, Ata-Ali J, Alegre-Domingo T, Candel-Martí E, Ata-Ali F, Palacio JR, et al. The effect of orally administered probiotic Lactobacillus reuteri-containing tablets in peri-implant mucositis: a double-blind randomized controlled trial. J Periodontal Res. (2015) 50:775–85. doi: 10.1111/jre.12264
33. Hallström H, Lindgren S, Widén C, Renvert S, Twetman S. Probiotic supplements and debridement of peri-implant mucositis: a randomized controlled trial. Acta Odontol Scand. (2016) 74:60–6. doi: 10.3109/00016357.2015.1040065
34. Mongardini C, Pilloni A, Farina R, Di Tanna G, Zeza B. Adjunctive efficacy of probiotics in the treatment of experimental peri-implant mucositis with mechanical and photodynamic therapy: a randomized, cross-over clinical trial. J Clin Periodontol. (2017) 44:410–7. doi: 10.1111/jcpe.12689
35. Tada H, Masaki C, Tsuka S, Mukaibo T, Kondo Y, Hosokawa R. The effects of Lactobacillus reuteri probiotics combined with azithromycin on peri-implantitis: A randomized placebo-controlled study. J Prosthodont Res. (2018) 62:89–96. doi: 10.1016/j.jpor.2017.06.006
36. Galofré M, Palao D, Vicario M, Nart J, Violant D. Clinical and microbiological evaluation of the effect of Lactobacillus reuteri in the treatment of mucositis and peri-implantitis: A triple-blind randomized clinical trial. J Periodontal Res. (2018) 53:378–90. doi: 10.1111/jre.12523
37. Lauritano D, Carinci F, Palmieri A, Cura F, Caruso S, Candotto V. Reuterinos® as adjuvant for peri-implant treatment: A pilot study. Int J Immunopathol Pharmacol. (2019) 33:2058738419827745. doi: 10.1177/2058738419827745
38. Peña M, Barallat L, Vilarrasa J, Vicario M, Violant D, Nart J. Evaluation of the effect of probiotics in the treatment of peri-implant mucositis: a triple-blind randomized clinical trial. Clin Oral Investig. (2019) 23:1673–83. doi: 10.1007/s00784-018-2578-8
39. Santana SI, Silva PHF, Salvador SL, Casarin RCV, Furlaneto FAC, Messora MR. Adjuvant use of multispecies probiotic in the treatment of peri-implant mucositis: A randomized controlled trial. J Clin Periodontol. (2022) 49:828–39. doi: 10.1111/jcpe.13663
40. Sargolzaei N, Arab H, Gerayeli M, Ivani F. Evaluation of the topical effect of probiotic mouthwash in the treatment of patients with peri-implant mucositis. J Long Term Eff Med Implants. (2022) 32:85–91. doi: 10.1615/JLongTermEffMedImplants.2021039490
41. Alqahtani F, Alshaikh M, Mehmood A, Alqhtani N, Alkhtani F, Alenazi A. Efficacy of antibiotic versus probiotics as adjuncts to mechanical debridement for the treatment of peri-implant mucositis. J Oral Implantol. (2022) 48:99–104. doi: 10.1563/aaid-joi-D-20-00259
42. Crocker TF, Lam N, Jordão M, Brundle C, Prescott M, Forster A, et al. Risk-of-bias assessment using Cochrane's revised tool for randomized trials (RoB 2) was useful but challenging and resource-intensive: observations from a systematic review. J Clin Epidemiol. (2023) 161:39–45. doi: 10.1016/j.jclinepi.2023.06.015
43. Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. Periodontol 2000. (2014) 66:255–73. doi: 10.1111/prd.12049
44. Willis JR, Gabaldón T. The human oral microbiome in health and disease: from sequences to ecosystems. Microorganisms. (2020) 8:308. doi: 10.3390/microorganisms8020308
45. Esposito M, Grusovin MG, Worthington HV. Treatment of peri-implantitis: what interventions are effective? A Cochrane systematic review. Eur J Oral Implantol. (2012) 5 Suppl:S21–41.
46. Iniesta M, Herrera D, Montero E, Zurbriggen M, Matos AR, Marín MJ, et al. Probiotic effects of orally administered Lactobacillus reuteri-containing tablets on the subgingival and salivary microbiota in patients with gingivitis. A randomized clinical trial. J Clin Periodontol. (2012) 39:736–44. doi: 10.1111/j.1600-051X.2012.01914.x
47. Martines RT, Sendyk WR, Gromatzky A, Cury PR. Sandblasted/acid-etched vs smooth-surface implants: implant clinical reaction to experimentally induced peri-implantitis in Beagle dogs. J Oral Implantol. (2008) 34:185–9. doi: 10.1563/0.880.1
48. Hermann JS, Jones AA, Bakaeen LG, Buser D, Schoolfield JD, Cochran DL. Influence of a machined collar on crestal bone changes around titanium implants: a histometric study in the canine mandible. J Periodontol. (2011) 82:1329–38. doi: 10.1902/jop.2011.090728
49. Heitz-Mayfield LJA, Salvi GE. Peri-implant mucositis. J Clin Periodontol. (2018) Suppl 20:S237–45. doi: 10.1111/jcpe.12953
50. Aronson JK, Ferner RE. Biomarkers-A general review. Curr Protoc Pharmacol. (2017) 76:9.23. doi: 10.1002/cpph.19
51. Kalsi AS, Moreno F, Petridis H. Biomarkers associated with periodontitis and peri-implantitis: a systematic review. J Periodontal Implant Sci. (2021) 51:3–17. doi: 10.5051/jpis.1902840142
52. Pliavga V, Peceliunaite G, Daugela P, Leketas M, Gervickas A, Juodzbalys G. Peri-implantitis diagnosis and prognosis using biomarkers: A systematic literature review. Int J Oral Maxillofac Implants. (2023) 38:1095–105. doi: 10.11607/jomi.10353
53. Doornewaard R, Jacquet W, Cosyn J, De Bruyn H. How do peri-implant biologic parameters correspond with implant survival and peri-implantitis? A Crit review. Clin Oral Implants. (2018) 29 Suppl 18:100–23. doi: 10.1111/clr.13264
54. Parpaiola A, CecChinato D, Toia M, Bressan E, Speroni S, Lindhe J. Dimensions of the healthy gingiva and peri-implant mucosa. Clin Oral Implants Res. (2015) 26:657–62. doi: 10.1111/clr.12359
55. Turkmen M, Firatli E. The study of genetic predisposition on periodontitis and peri-implantitis. Niger J Clin Pract. (2022) 25:1799–804. doi: 10.4103/njcp.njcp_19_22
Keywords: probiotic, prebiotic, peri-implant disease, mucositis, peri-implantitis, inmune-response, randomized clinical trial
Citation: López-Valverde N, López-Valverde A and Blanco Rueda JA (2024) The role of probiotic therapy on clinical parameters and human immune response in peri-implant diseases: a systematic review and meta-analysis of randomized clinical studies. Front. Immunol. 15:1371072. doi: 10.3389/fimmu.2024.1371072
Received: 15 January 2024; Accepted: 02 April 2024;
Published: 15 April 2024.
Edited by:
Jonathan Jantsch, University of Cologne, GermanyReviewed by:
Binnaz Leblebicioglu, The Ohio State University, United StatesOleh Andrukhov, Medical University of Vienna, Austria
Copyright © 2024 López-Valverde, López-Valverde and Blanco Rueda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio López-Valverde, YWxvcGV6dmFsdmVyZGVAdXNhbC5lcw==