
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 19 April 2024
Sec. Inflammation
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1361891
This article is part of the Research TopicRoad Trip from Mild to Severe Asthmatic Inflammation: The Traffic Lights of Biomarkers in Asthma Management - Volume IIView all 5 articles
 Celeste M. Porsbjerg1
Celeste M. Porsbjerg1 John Townend2,3Celine Bergeron4,5
John Townend2,3Celine Bergeron4,5 George C. Christoff6Gregory P. Katsoulotos7,8Désirée Larenas-Linnemann9Trung N. Tran10Riyad Al-Lehebi11,12
George C. Christoff6Gregory P. Katsoulotos7,8Désirée Larenas-Linnemann9Trung N. Tran10Riyad Al-Lehebi11,12 Sinthia Z. Bosnic-Anticevich7,13John Busby14Mark Hew15,16
Sinthia Z. Bosnic-Anticevich7,13John Busby14Mark Hew15,16 Konstantinos Kostikas17
Konstantinos Kostikas17 Nikolaos G. Papadopoulos18,19
Nikolaos G. Papadopoulos18,19 Paul E. Pfeffer20,21
Paul E. Pfeffer20,21 Todor A. Popov22
Todor A. Popov22 Chin Kook Rhee23Mohsen Sadatsafavi24
Chin Kook Rhee23Mohsen Sadatsafavi24 Ming-Ju Tsai25,26Charlotte Suppli Ulrik27
Ming-Ju Tsai25,26Charlotte Suppli Ulrik27 Mona Al-Ahmad28,29Alan Altraja30Aaron Beastall2,3Lakmini Bulathsinhala2,3Victoria Carter2,3
Mona Al-Ahmad28,29Alan Altraja30Aaron Beastall2,3Lakmini Bulathsinhala2,3Victoria Carter2,3 Borja G. Cosio31Kirsty Fletton2,3Susanne Hansen32,33
Borja G. Cosio31Kirsty Fletton2,3Susanne Hansen32,33 Liam G. Heaney34Richard B. Hubbard2,3,35Piotr Kuna36
Liam G. Heaney34Richard B. Hubbard2,3,35Piotr Kuna36 Ruth B. Murray3
Ruth B. Murray3 Tatsuya Nagano37
Tatsuya Nagano37 Laura Pini38
Laura Pini38 Diana Jimena Cano Rosales39Florence Schleich40
Diana Jimena Cano Rosales39Florence Schleich40 Michael E. Wechsler41Rita Amaral42,43Arnaud Bourdin44Guy G. Brusselle45,46Wenjia Chen47
Michael E. Wechsler41Rita Amaral42,43Arnaud Bourdin44Guy G. Brusselle45,46Wenjia Chen47 Li Ping Chung48Eve Denton15,49
Li Ping Chung48Eve Denton15,49 Joao A. Fonseca43Flavia Hoyte50
Joao A. Fonseca43Flavia Hoyte50 David J. Jackson51Rohit Katial50Bruce J. Kirenga52Mariko Siyue Koh53
David J. Jackson51Rohit Katial50Bruce J. Kirenga52Mariko Siyue Koh53 Agnieszka Ławkiedraj54Lauri Lehtimäki55,56Mei Fong Liew57,58
Agnieszka Ławkiedraj54Lauri Lehtimäki55,56Mei Fong Liew57,58 Bassam Mahboub59,60Neil Martin10,61Andrew N. Menzies-Gow62,63Pee Hwee Pang64
Bassam Mahboub59,60Neil Martin10,61Andrew N. Menzies-Gow62,63Pee Hwee Pang64 Andriana I. Papaioannou65
Andriana I. Papaioannou65 Pujan H. Patel66Luis Perez-De-Llano67Matthew J. Peters68,69
Pujan H. Patel66Luis Perez-De-Llano67Matthew J. Peters68,69 Luisa Ricciardi70
Luisa Ricciardi70 Bellanid Rodríguez-Cáceres39Ivan Solarte71,72Tunn Ren Tay73
Bellanid Rodríguez-Cáceres39Ivan Solarte71,72Tunn Ren Tay73 Carlos A. Torres-Duque74,75Eileen Wang50,76
Carlos A. Torres-Duque74,75Eileen Wang50,76 Martina Zappa77John Abisheganaden64,78,79Karin Dahl Assing80
Martina Zappa77John Abisheganaden64,78,79Karin Dahl Assing80 Richard W. Costello81Peter G. Gibson82,83
Richard W. Costello81Peter G. Gibson82,83 Enrico Heffler84,85Jorge Máspero86,87Stefania Nicola88
Enrico Heffler84,85Jorge Máspero86,87Stefania Nicola88 Diahn-Warng Perng (Steve)89,90
Diahn-Warng Perng (Steve)89,90 Francesca Puggioni84Sundeep Salvi91
Francesca Puggioni84Sundeep Salvi91 Chau-Chyun Sheu25,26Concetta Sirena92
Chau-Chyun Sheu25,26Concetta Sirena92 Camille Taillé93
Camille Taillé93 Tze Lee Tan94
Tze Lee Tan94 Leif Bjermer95Giorgio Walter Canonica84,85Takashi Iwanaga96
Leif Bjermer95Giorgio Walter Canonica84,85Takashi Iwanaga96 Libardo Jiménez-Maldonado97,75
Libardo Jiménez-Maldonado97,75 Christian Taube98
Christian Taube98 Luisa Brussino99
Luisa Brussino99 David B. Price2,3,100*
David B. Price2,3,100*Background: To date, studies investigating the association between pre-biologic biomarker levels and post-biologic outcomes have been limited to single biomarkers and assessment of biologic efficacy from structured clinical trials.
Aim: To elucidate the associations of pre-biologic individual biomarker levels or their combinations with pre-to-post biologic changes in asthma outcomes in real-life.
Methods: This was a registry-based, cohort study using data from 23 countries, which shared data with the International Severe Asthma Registry (May 2017-February 2023). The investigated biomarkers (highest pre-biologic levels) were immunoglobulin E (IgE), blood eosinophil count (BEC) and fractional exhaled nitric oxide (FeNO). Pre- to approximately 12-month post-biologic change for each of three asthma outcome domains (i.e. exacerbation rate, symptom control and lung function), and the association of this change with pre-biologic biomarkers was investigated for individual and combined biomarkers.
Results: Overall, 3751 patients initiated biologics and were included in the analysis. No association was found between pre-biologic BEC and pre-to-post biologic change in exacerbation rate for any biologic class. However, higher pre-biologic BEC and FeNO were both associated with greater post-biologic improvement in FEV1 for both anti-IgE and anti-IL5/5R, with a trend for anti-IL4Rα. Mean FEV1 improved by 27-178 mL post-anti-IgE as pre-biologic BEC increased (250 to 1000 cells/µL), and by 43-216 mL and 129-250 mL post-anti-IL5/5R and -anti-IL4Rα, respectively along the same BEC gradient. Corresponding improvements along a FeNO gradient (25-100 ppb) were 41-274 mL, 69-207 mL and 148-224 mL for anti-IgE, anti-IL5/5R, and anti-IL4Rα, respectively. Higher baseline BEC was also associated with lower probability of uncontrolled asthma (OR 0.392; p=0.001) post-biologic for anti-IL5/5R. Pre-biologic IgE was a poor predictor of subsequent pre-to-post-biologic change for all outcomes assessed for all biologics. The combination of BEC + FeNO marginally improved the prediction of post-biologic FEV1 increase (adjusted R2: 0.751), compared to BEC (adjusted R2: 0.747) or FeNO alone (adjusted R2: 0.743) (p=0.005 and <0.001, respectively); however, this prediction was not improved by the addition of IgE.
Conclusions: The ability of higher baseline BEC, FeNO and their combination to predict biologic-associated lung function improvement may encourage earlier intervention in patients with impaired lung function or at risk of accelerated lung function decline.
Severe asthma is a heterogenous syndrome encompassing several clinical phenotypes and endotypes, or patterns of airway inflammation (1, 2). The type-2 (T2)-inflammatory endotype, associated with increased blood eosinophil count (BEC) and/or fractional exhaled nitric oxide (FeNO) concentrations or total immunoglobulin E (IgE) and specific IgE, is estimated to account for up to 80% of adults with severe asthma using an algorithm informed by these biomarkers (and clinical characteristics) and developed by expert consensus (2–4). Investigation of how these biomarkers may be associated with better asthma outcomes in patients who initiate biologics or other therapies, and their use in guiding asthma treatment-related decisions is an area of intense research (5–12). However, the effectiveness of T2-directed biologics is variable even in patients with similar biomarker profiles (13). The challenge, therefore, remains to further unravel asthma endotypes within the T2-high severe asthma population and to accurately select patients who will respond best to the selected biologic therapy; matching the right patient to the right biologic in the course of their disease and allowing for a more personalized and targeted approach to asthma treatment. Use of biomarkers to identify non-responders is arguably just as important to avoid unnecessary treatment.
However, there are still many issues with T2 biomarkers in terms of how best to measure and interpret them, as well as with the evidence underpinning their utility to assess and predict response to biologics in patients with severe asthma. For example, biomarker levels show marked temporal variability, are influenced by site of measurement, and must be interpreted in the context of background corticosteroid treatment and treatment adherence (14, 15). Biomarkers also frequently overlap, with their utility considered by some as a means to identify severe asthma rather than select biologic therapy (16). There are also gaps in our knowledge about their relationship with each other (2). Biomarker cut-off values to inform biologic eligibility have also been influenced by randomized clinical trial (RCT) criteria, rather than by studies specifically designed to investigate the utility of biomarker level to predict biologic response in real life, and show marked inter-country variability, indicative of variable interpretation of the same evidence by different regulators and reimbursement bodies (17). There is clearly a need for biomarker validation in terms of predicting response to therapy (18). A clinically applicable biomarker should be ‘Superior’ (outperform current practice), ‘Actionable’ (change patient management), ‘Valuable’ (improve patient outcomes), ‘Economical’ (cost-saving or cost-effective) and ‘clinically Deployable’ (analysis technology available in clinical laboratory) (i.e., the SAVED approach) (18).
To date, previous clinical studies that examined the influence of pre-biologic biomarker levels on post-biologic outcomes have compared biologic effectiveness, stratified by biomarker concentration compared to a placebo group, rather than within a biologic-treated group (i.e. compared to baseline). Whether this relationship is seen when pre-to-post biologic effect is assessed along a pre-biologic biomarker concentration gradient remains to be determined; proof of such a relationship would be more meaningful to clinicians when deciding which biologic to prescribe for which patient. Furthermore, the ability of biomarkers to predict which patients will experience improved lung function is not well-studied (19–21). This is arguably a more valuable endpoint considering that many patients with asthma experience significant irreversible deterioration of their lung function over time, (which is associated with severe disease), that lung function declines more quickly in younger adults compared to older patients who have had the same number of exacerbations (22–24), and that those with better lung function are more likely to achieve asthma remission when treated with biologics (25).
Previous research conducted by the International Severe Asthma Registry (ISAR; https://isaregistries.org/) has shown considerable overlap of inflammatory biomarkers in severe asthma, suggesting that a more comprehensive approach may be needed to identify the best therapy for patients, rather than reliance on a single biomarker threshold positivity (2). ISAR is the largest, real-world data repository of severe asthma cases, including data on >17,000 patients from 25 countries. It offers a unique opportunity to investigate the relationship between biomarker profile and pre-to- post biologic change across a range of biomarkers, asthma outcomes, and biologic classes in a real-world setting that includes patients who would not qualify for entry into RCTs (26–28). Our aim was to investigate T2 inflammatory biomarker distribution and correlations, the association of pre-biologic biomarker levels with pre-to-post biologic change in asthma outcomes, and whether combined biomarker measurements lead to an improved association with pre-to-post biologic change.
This was a registry-based cohort study using data from ISAR (https://isaregistries.org/), the largest adult severe asthma registry in the world (26). Patients with severe asthma included in ISAR have been well characterized (29) and phenotyped (3). The details of this registry have been described elsewhere (27), and details are provided in the Online Supplement. In this study we have included data from 23 countries (Argentina, Australia, Bulgaria, Canada, Colombia, Denmark, Greece, India, Ireland, Italy, Japan, Korea, Kuwait, Mexico, Poland, Portugal, Saudi Arabia, Singapore, Spain, Taiwan, United Arab Emirates, United Kingdom, and United States) that shared data with ISAR between May 1, 2017 and February 24, 2023. The study had two parts. The first part investigated pre-biologic biomarker level distribution and correlations for all patients, regardless of whether a biologic was subsequently initiated. The second part investigated whether an association exists between pre-biologic biomarker levels and change in asthma outcomes pre-to-post biologic in those patients who initiated biologics. For this part, study entry corresponded to date of first biologic initiation, and asthma-related outcomes were assessed both in the 1-year period pre- and post-biologic therapy (Supplementary Figure 1; Table 1).
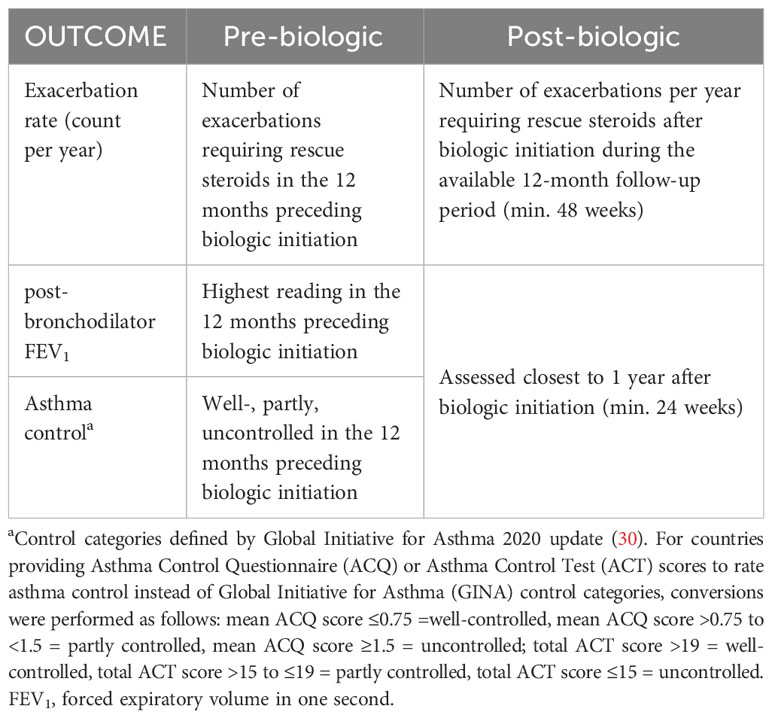
Table 1 Asthma outcome definitions and Asthma outcome definitions and timing of outcome assessments pre- and post-biologic.
All patients were enrolled in ISAR and were required to be aged ≥18 years and have severe asthma (consistently defined as receiving treatment at Global Initiative for Asthma [GINA] 2018 Step 5 or with uncontrolled asthma at GINA Step 4) (31). Subsequent inclusion criteria differed by analysis. For the biomarker distribution and correlation analyses, patients were also required to have a pre-biologic value for any of the biomarkers assessed (i.e., IgE, BEC, or FeNO). For the association of individual biomarkers and pre-to-post biologic change analyses, patients also must have received a biologic and have pertinent information on at least one asthma outcome (i.e., exacerbations, lung function, or asthma control). To be able to attribute any associations with a particular biologic type, patients who switched biologic therapies during follow-up were excluded from these analyses. Finally, for inclusion in the association of multiple biomarkers and pre-to-post biologic change analyses, patients were also required to have pre-biologic values for all three investigated biomarkers. Those who had bronchial thermoplasty were excluded.
Collected variables included pre-biologic demographic and clinical characteristics (Table 2); highest pre-biologic values for FeNO (ppb), IgE (IU/mL), and BEC (cells/µL); and asthma outcomes pre- and post-biologic therapy. For the distribution and correlation analyses, we used the highest pre-biologic biomarker value in the 1-year period prior to biologic initiation (for those who subsequently initiated a biologic) or the highest value at any time for those who did not subsequently initiate a biologic (because all values were pre-biologic). For the association analyses, the highest pre-biologic biomarker value in the 1-year period prior to biologic initiation was used. Median biomarker concentrations in the first 3 months biologic therapy and subsequently at >3-12, >12-24, >24-36 and >36 months post-biologic initiation were also collected to investigate biomarker temporal stability.
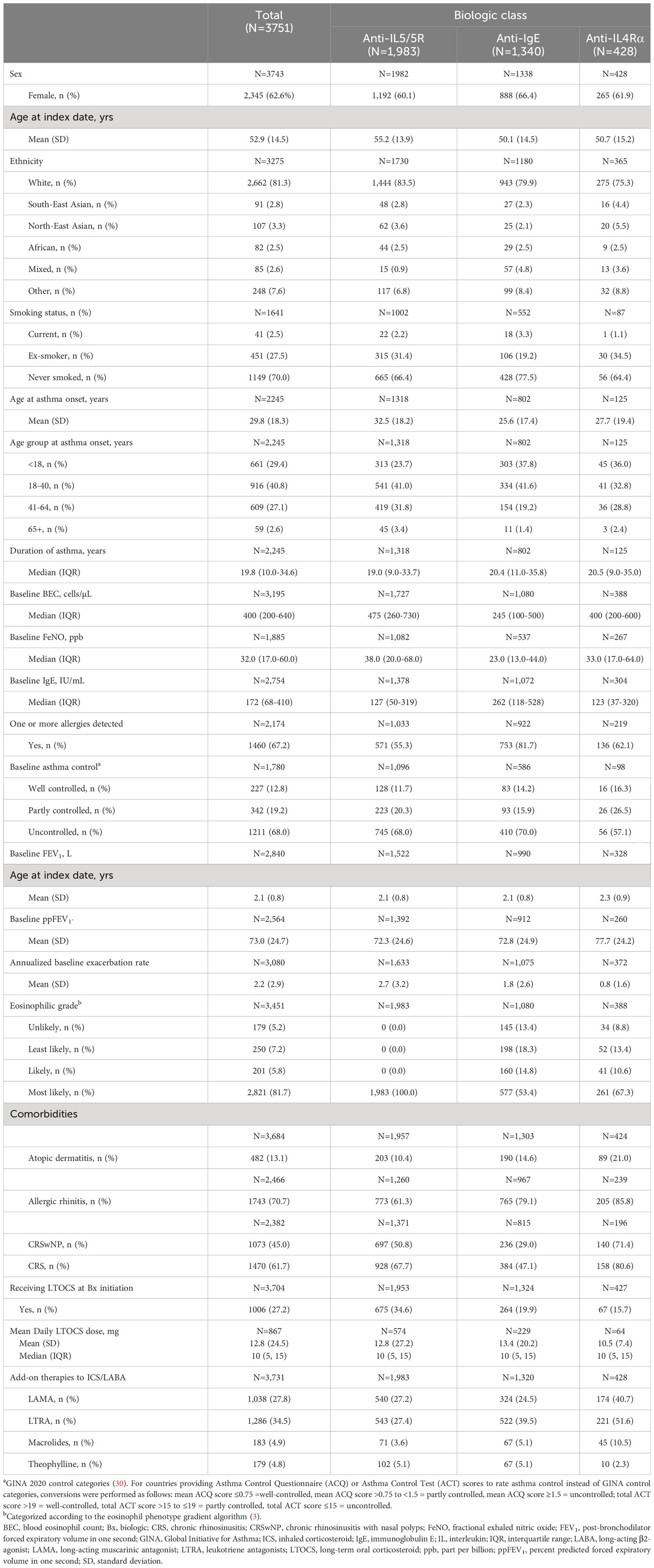
Table 2 Pre-biologic characteristics of patients included in association of T2-biomarkers and pre-to post biologic outcome analyses.
Asthma outcomes investigated included annual exacerbation rate, highest post-bronchodilator forced expiratory volume in one second (FEV1), and asthma control (Table 1). Asthma control was categorized as well-, partly, or uncontrolled according to GINA 2020 criteria (30). If contributing countries used the Asthma Control Test (ACT) (32) or Asthma Control Questionnaire (ACQ) (33) to assess asthma control, conversions were made to fit the GINA control categories as follows: mean ACQ score: well controlled (≤0.75); partly controlled (>0.75 to <1.5), uncontrolled (≥1.5); and total ACT score: well controlled (>19); partly controlled (>15 to ≤19), uncontrolled (≤15). Similar cut-offs and correlations have been described (34, 35) and used by others (36–38).
Correlations of pre-biologic biomarker values collected within 7 days of each other (for patients who had pairs of biomarkers collected at similar times: BEC/FeNO, BEC/IgE and FeNO/IgE) were tested using Pearson’s correlation using log10 values of the biomarkers. Changes in biomarkers in the first 3 months and at >3-12, >12-24, >24-36 and >36 months post-biologic initiation were summarized descriptively.
The association between individual pre-biologic T2 biomarkers and pre-to-post biologic change (by biologic class) was assessed for each of the 3 asthma outcomes using regression models with follow-up outcomes as the response, adjusting for baseline level of the relevant outcome. Linear, negative binomial, and logistic regression models were used for FEV1, exacerbations, and asthma control, respectively, according to the type and distribution of the data. Follow-up rates, means, or probabilities were estimated using adjusted predictions from the models for selected values of the biomarkers. For exacerbations the estimated follow-up rates were calculated for patients with a baseline exacerbation rate of 2.2 per year (mean value in the biologic population), and for FEV1 the estimated follow-up values were calculated for patients with a baseline FEV1 of 2.1 L (mean value in the biologic population). These estimates were plotted in the figures as the change from baseline by subtracting the baseline value at which they were evaluated (2.2 exacerbations per year, or FEV1 = 2.1 L). For asthma control, the adjusted predictions for the probability of uncontrolled asthma at follow-up were estimated for each biologic type assuming the proportion of patients with uncontrolled asthma at baseline was 68% (equal to the proportion amongst all included patients). This was equivalent to estimating the rate of uncontrolled asthma at follow-up in each biologic class as if all included patients had received that biologic. Separate models were fitted for BEC, FeNO and IgE. Analyses for each post-biologic asthma outcome (for all biologic classes combined) were also stratified by various subgroups: long-term oral corticosteroid (LTOCS) at baseline (yes/no), age of asthma onset (<18/≥18 years), presence of allergy (yes/no), and baseline annual exacerbation burden (0/≥1 exacerbation).
The association of multiple biomarkers and pre-to-post biologic change in asthma outcomes was assessed using the same statistical models as described above for each asthma outcome, but also including the additional biomarker(s) as independent variables. The accuracy of the predictions made by the model was assessed using: (i) percentage of variance in follow-up FEV1 explained by the model (adjusted R2); (ii) percentage of uncontrolled asthma outcomes correctly classified by the model (probability > 0.5 = positive outcome predicted, probability < 0.5 = negative outcome predicted); and (iii) mean absolute error in the exacerbation rate predicted by the model compared with the actual follow-up rate. The increase in model fit due to the incorporation of additional biomarkers was tested using likelihood ratio tests. For the regression analyses, positive outlying baseline biomarkers were excluded (defined as > upper quartile + 1.5 x inter-quartile range) (39) to avoid fitting the regressions for a range of biomarker values where there was insufficient coverage in the data. All analyses were undertaken in STATA v15.1, and p-values ≤0.05 were considered statistically significant. We also plotted point estimates from the regression models for the lung function outcome along a BEC plus FeNO gradient and tabulated mean values for pre-to-post biologic change in each asthma outcome assessed according to FeNO/BEC combination categories ranging from low/low (25 ppb/<150 cells/µL) to high/high (>50 ppb/>300 cells/µL).
As of February 24, 2023, ISAR included data on 15,154 adult patients with severe asthma. A total of 11,363 patients from 23 countries were eligible for assessment of biomarker distribution and correlation. Of these, 3,751 were eligible for inclusion in the association of biomarker with biologic effectiveness analyses, of whom 1,983 initiated anti–interleukin-5/5 receptor (anti-IL5/5R) therapy, 1,340 initiated anti-IgE therapy, and 428 initiated anti–interleukin-4 receptor alpha (anti-IL4Rα) therapy (Supplementary Figure 2). A total of 1,323 patients had data available for all three biomarkers (BEC, FeNO and IgE) and were included in the association of multiple biomarkers with biologic effectiveness analyses.
Table 2 summarizes baseline characteristics for those patients included in the analyses investigating the association between pre-biologic biomarker concentration and pre-to-post biologic changes in outcomes (n=3,751). These patients tended to be middle-aged (mean [standard deviation; SD] 52.9 [14.5] years), were predominantly female (62.6%) and White (81.3%), and had adult-onset disease (70.6%). Pre-biologic biomarker concentrations (BEC, FeNO, and IgE) were all elevated, and 81.7% had an eosinophilic asthma phenotype. Morbidity burden was high, evidenced by a mean (SD) exacerbation rate/year of 2.2 (2.9) and percent predicted FEV1 (ppFEV1) of 73.0% pre-biologic initiation, and a high proportion of patients with uncontrolled disease (68.0%) and receiving LTOCS (27.2%). Overall, the mean (SD) daily dose of LTOCS (prednisone equivalent dosing) was 12.8 (24.5) mg pre-biologic and 8.7 (24.3) mg post-biologic (anti-IgE therapy: 8.9 [18.9] mg; anti-IL5/5R therapy: 8.9 [27.2] mg; anti-IL4Rα therapy: 6.2 [7.4] mg), which was a mean (SD) daily decrease of 4.1 (8.2) mg. Potentially T2-related comorbidities were prevalent, notably allergic rhinitis (70.7%), atopic dermatitis (13.1%), and chronic rhinosinusitis with nasal polyps (45.0%). Compared to patients treated with anti-IgE therapy, those who subsequently received anti-IL5/5R therapy tended to have later onset disease and have more severe asthma in terms of exacerbation rate and LTOCS use. Patients treated with anti-IL4Rα therapy tended to have the least severe disease; however, all subsequent analyses were adjusted for baseline for all asthma outcomes assessed. Pre-biologic BEC and FeNO concentrations were elevated in the anti-IL5/5R and anti-IL4Rα biologic groups, whereas patients who subsequently initiated anti-IgE therapy tended to have higher IgE concentrations and one or more allergies. Pre-biologic characteristics (overall and by biologic class) for patients included in the assessment of biologic distribution and correlation analyses are provided in Supplementary Table 1.
Median (interquartile range) values for BEC, FeNO and IgE were 300 (200-600) cells/µL, 29.0 (15.0-60.0) ppb and 158 (52-457) IU/mL, respectively (Supplementary Figure 3) and were generally higher in patients who subsequently initiated a biologic (Supplementary Table 1). BEC and FeNO decreased following treatment with anti-IL5/5R and anti-IL4Rα therapies, respectively. Anti-IgE therapy had little effect on these biomarkers (Supplementary Figure 4; Supplementary Tables 2, 3). Positive correlations between all pairs of biomarkers measured within 7 days of each other were noted, although the strength of the correlations was low (r ≤0.4) in all cases (Supplementary Figures 5A-C), but stronger in those not receiving LTOCS (Supplementary Table 4).
All asthma outcomes assessed improved with biologic treatment; the estimated probability of having uncontrolled asthma was approximately 0.3, and the exacerbation rate decreased by approximately 2 per year post-biologic. Pre-biologic biomarker concentrations were associated with post-biologic outcome, but this association varied by biologic class and asthma outcome assessed (Figures 1-3).
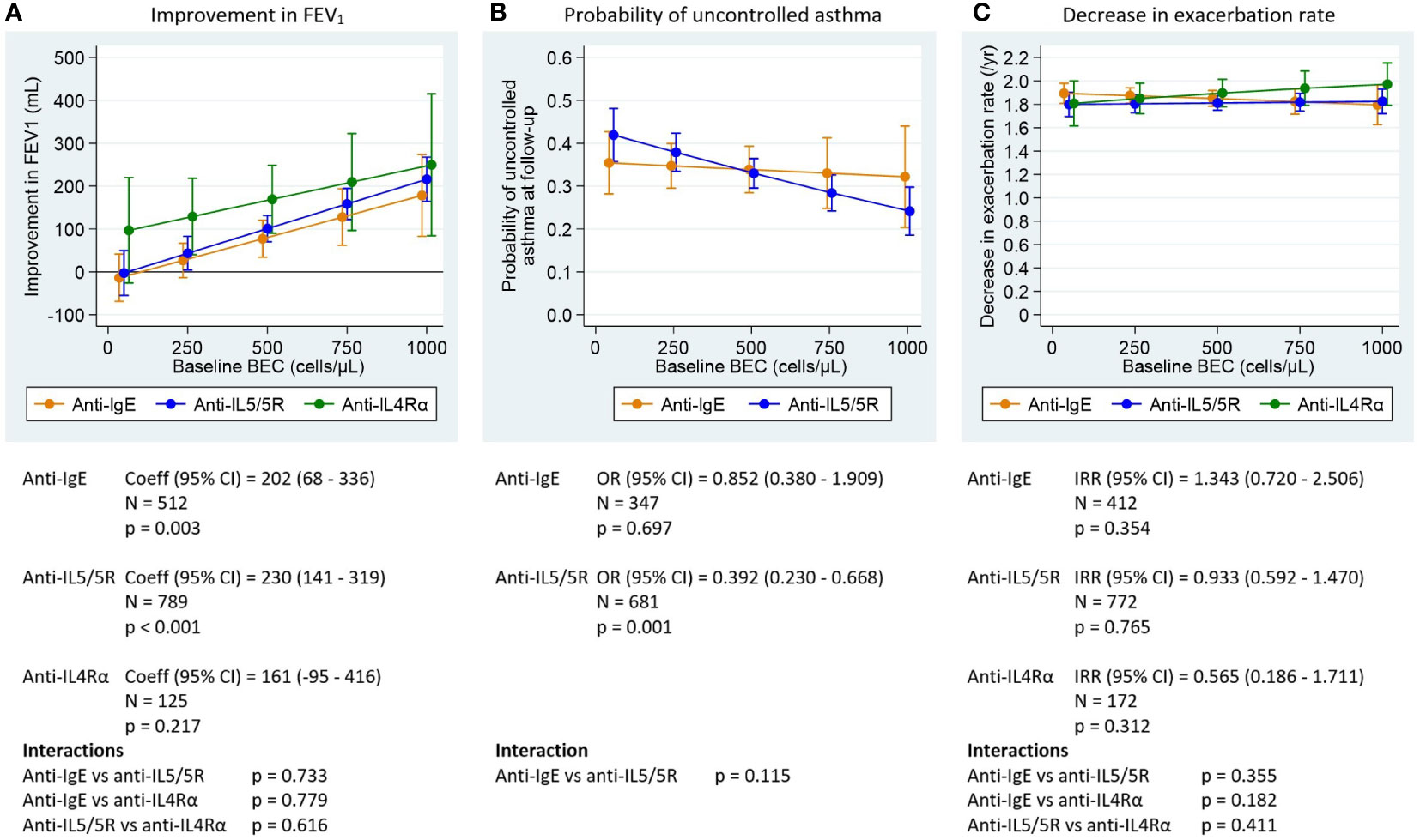
Figure 1 Association between pre-biologic BEC and post-biologic asthma outcomes, by biologic class adjusted for baseline for each outcome. BEC, blood eosinophil; FEV1, post-bronchodilator forced expiratory volume in one second; IgE, immunoglobulin E Graphs show point estimates from the regression models for selected values of the biomarkers. (A) change in FEV1 for a patient with baseline FEV1 = 2.1 L (mean baseline FEV1 for the biologic patients in ISAR), (B) asthma control at follow-up for a population with 68% uncontrolled asthma at baseline (proportion for biologic patients in ISAR), (C) change in exacerbation rate for a patient with 2.2 exacerbations per year at baseline (mean baseline exacerbation rate for the biologic patients in ISAR). Asthma control assessed using Global Initiative for Asthma (GINA) 2020 control categories (30). For countries providing Asthma Control Questionnaire (ACQ) or Asthma Control Test (ACT) scores to rate asthma control instead of GINA control categories, conversions were performed as follows: mean ACQ score ≤0.75 =well-controlled, mean ACQ score >0.75 to <1.5 = partly controlled, mean ACQ score ≥1.5 = uncontrolled; total ACT score >19 = well-controlled, total ACT score >15 to ≤19 = partly controlled, total ACT score ≤15 = uncontrolled. Coefficients, odds ratios, and incidence rate ratios are the estimated change in the outcome per 1000 cells/µL (BEC), per 100 ppb (FeNO) or per 1000 IU/mL (IgE). P-values are for tests of association between the outcomes after treatment and baseline levels of the biomarkers (adjusted for baseline level of the outcome). Interaction tests are for comparisons of the slope coefficients for the different biologic classes, estimated by the model.
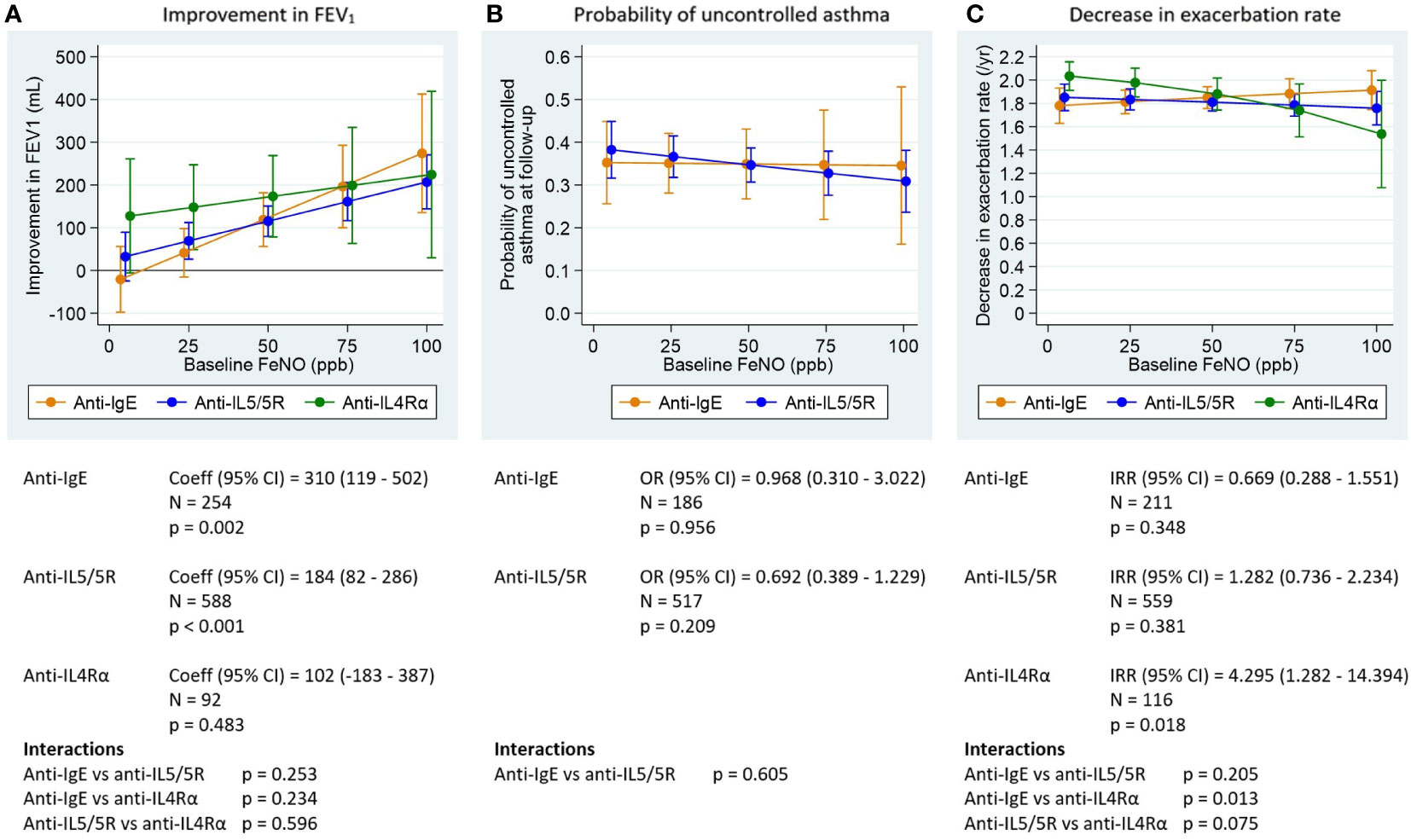
Figure 2 Association between pre-biologic FeNO and post-biologic asthma outcomes by biologic class, adjusted for baseline for each outcome. FeNO, fractional exhaled nitric oxide; FEV1, post-bronchodilator forced expiratory volume in one second; IgE, immunoglobulin E; ppb, parts per billion. Graphs show point estimates from the regression models for selected values of the biomarkers. (A) change in FEV1 for a patient with baseline FEV1 = 2.1 L (mean baseline FEV1 for the biologic patients in ISAR), (B) asthma control at follow-up for a population with 68% uncontrolled asthma at baseline (proportion for biologic patients in ISAR), (C) change in exacerbation rate for a patient with 2.2 exacerbations per year at baseline (mean baseline exacerbation rate for the biologic patients in ISAR). Asthma control assessed using Global Initiative for Asthma (GINA) 2020 control categories (30). For countries providing Asthma Control Questionnaire (ACQ) or Asthma Control Test (ACT) scores to rate asthma control instead of GINA control categories, conversions were performed as follows: mean ACQ score ≤0.75 =well-controlled, mean ACQ score >0.75 to <1.5 = partly controlled, mean ACQ score ≥1.5 = uncontrolled; total ACT score >19 = well-controlled, total ACT score >15 to ≤19 = partly controlled, total ACT score ≤15 = uncontrolled. Coefficients, odds ratios, and incidence rate ratios are the estimated change in the outcome per 1000 cells/µL (BEC), per 100 ppb (FeNO) or per 1000 IU/mL (IgE). P-values are for tests of association between the outcomes after treatment and baseline levels of the biomarkers (adjusted for baseline level of the outcome). Interaction tests are for comparisons of the slope coefficients for the different biologic classes, estimated by the model.
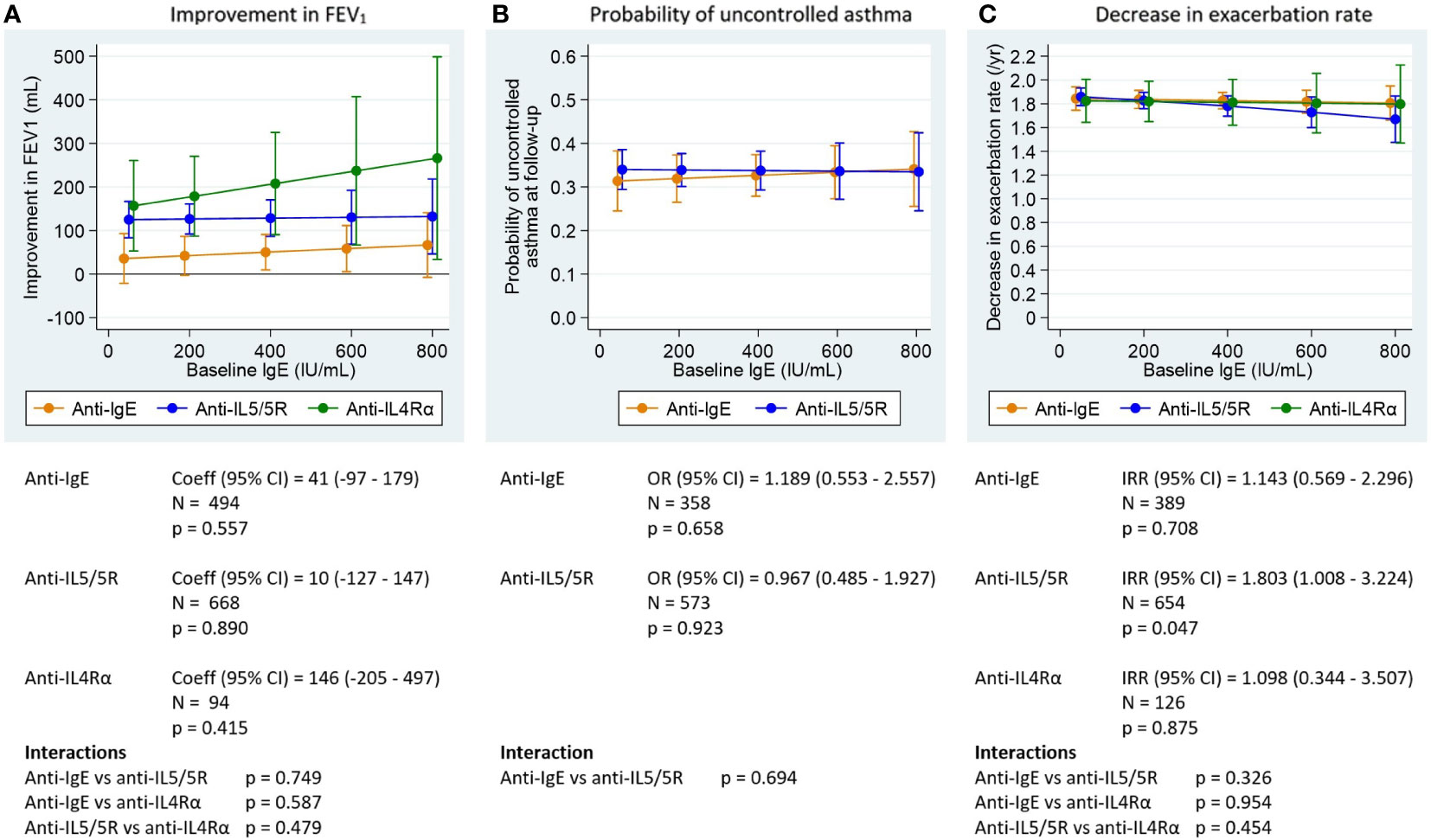
Figure 3 Association between pre-biologic IgE and post-biologic asthma outcomes by biologic class, adjusted for baseline for each outcome. FEV1, post-bronchodilator forced expiratory volume in one second; IgE, immunoglobulin E. Graphs show point estimates from the regression models for selected values of the biomarkers. (A) change in FEV1 for a patient with baseline FEV1 = 2.1 L (mean baseline FEV1 for the biologic patients in ISAR), (B) asthma control at follow-up for a population with 68% uncontrolled asthma at baseline (proportion for biologic patients in ISAR), (C) change in exacerbation rate for a patient with 2.2 exacerbations per year at baseline (mean baseline exacerbation rate for the biologic patients in ISAR). Asthma control assessed using Global Initiative for Asthma (GINA) 2020 control categories (30). For countries providing Asthma Control Questionnaire (ACQ) or Asthma Control Test (ACT) scores to rate asthma control instead of GINA control categories, conversions were performed as follows: mean ACQ score ≤0.75 =well-controlled, mean ACQ score >0.75 to <1.5 = partly controlled, mean ACQ score ≥1.5 = uncontrolled; total ACT score >19 = well-controlled, total ACT score >15 to ≤19 = partly controlled, total ACT score ≤15 = uncontrolled. Coefficients, odds ratios, and incidence rate ratios are the estimated change in the outcome per 1000 cells/µL (BEC), per 100 ppb (FeNO) or per 1000 IU/mL (IgE). P-values are for tests of association between the outcomes after treatment and baseline levels of the biomarkers (adjusted for baseline level of the outcome). Interaction tests are for comparisons of the slope coefficients for the different biologic classes, estimated by the model.
Greater post-biologic improvement in FEV1 was observed in those patients with higher pre-biologic BEC for both anti-IgE and anti-IL5/5R therapies (Figure 1A). FEV1 improved by 27 mL (post- vs pre–anti-IgE therapy) for those with a mean baseline BEC of 250 cells/µL, increasing to 178 mL for those with a baseline BEC of 1000 cells/µL. Patients treated with an anti-IL5/5R therapy experienced a 43-216 mL increase in FEV1 along the same BEC gradient. A trend towards greater post-biologic improvement in FEV1 (129-250 mL) was noted for patients treated with anti-IL4Rα therapy, as pre-biologic BEC increased from 250-1,000 cells/µL (Supplementary Table 5A). Greater baseline BEC was also associated with a lower probability of uncontrolled asthma post-biologic, but only for patients treated with anti-IL5/5R therapy (Figure 1B). The probability of uncontrolled asthma when treated with anti-IL5/5R therapy was reduced from 0.42 (95% CI: 0.36, 0.48) at BEC of 50 cells/µL to 0.24 (95% CI: 0.19, 0.30) at BEC 1000 cells/µL, but remained relatively constant in the anti-IgE group, ranging from 0.35 to 0.32 over the same BEC range (Figure 1B; Supplementary Table 6A). No association was found between pre-biologic BEC and pre-to-post change in exacerbation rate for any biologic class (Figure 1C; Supplementary Table 7A).
Greater pre-biologic FeNO concentrations were also associated with greater FEV1 improvement for both anti-IgE and anti-IL5/5R therapies (Figure 2A). A relationship in the same direction was seen for patients treated with anti-IL4Rα therapy, but was not statistically significant. Mean FEV1 improved by 41 to 274 mL in the anti-IgE group along a 25-100 ppb FeNO gradient and from 69 to 207 mL and 148 to 224 mL in the anti-IL5/5R and anti-IL4Rα groups, respectively, along the same gradient (Supplementary Table 5B). There was no association between pre-biologic FeNO concentration and probability of uncontrolled asthma for any biologic class assessed (Figure 2B; Supplementary Table 6B). There was also no association between pre-biologic FeNO concentrations and exacerbation rate reduction for those treated with anti-IgE or anti-IL5/5R therapies (Figure 2C; Supplementary Table 7B). Although greater pre-biologic FeNO concentrations appeared to be associated with less exacerbation rate reduction for patients treated with anti-IL4Rα therapy (Figure 2C), the results should be interpreted with caution because small patient numbers resulted in a large range of error particularly at the higher FeNO range.
Pre-biologic IgE was a poor predictor of subsequent pre-to-post biologic change for all outcomes assessed, irrespective of biologic class (Figures 3A–C; Supplementary Tables 5C-7C)
Associations between pre-biologic biomarkers and the post-biologic exacerbation and control outcomes were relatively flat irrespective of LTOCS use at biologic initiation. However, post-biologic exacerbation rate reduction tended to be better in those without LTOCS use (Figure 4A), patients without allergies, and for those aged ≥18 years at asthma onset (Supplementary Figure 6) for all biomarkers assessed. The probability of uncontrolled asthma at follow-up was also generally lower for those patients without evidence of LTOCS use at biologic initiation (Figure 4B), as well as those with adult-onset asthma (Supplementary Figure 7) for all biomarkers. By contrast, pre-biologic BEC and FeNO were generally predictive of an improved biologic lung function response in all sub-groups listed above, and irrespective of baseline exacerbation rates, with a greater improvement in FEV1 noted in those patients not taking LTOCS at biologic initiation and for those with adult-onset asthma (Figure 4C; Supplementary Figure 8).
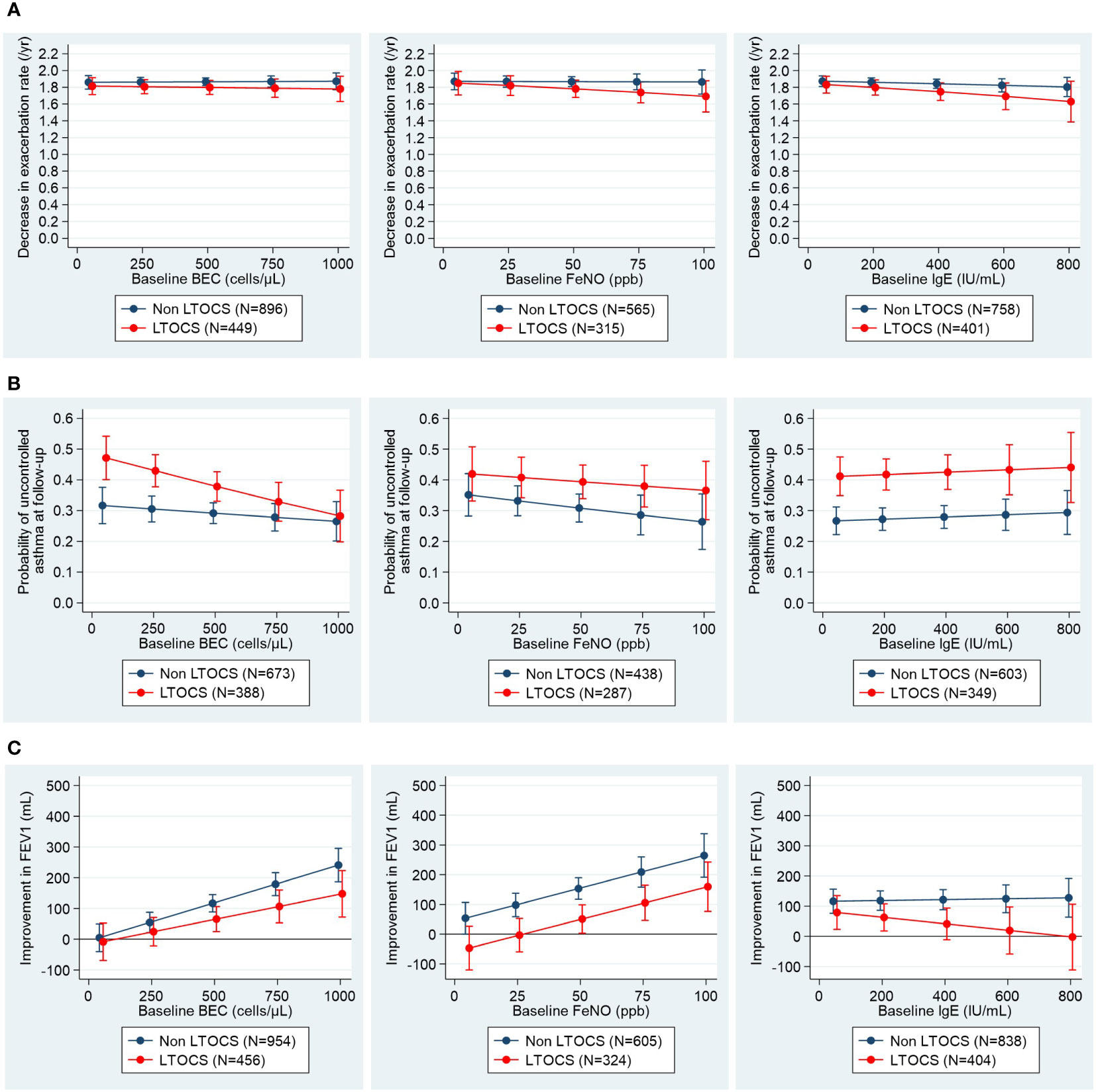
Figure 4 Associations between pre-biologic biomarker levels and post-biologic (A) exacerbation rate, (B) asthma control and (C) FEV1 stratified by LTOCS use. Asthma control assessed using Global Initiative for Asthma (GINA) 2020 control categories (30). For countries providing Asthma Control Questionnaire (ACQ) or Asthma Control Test (ACT) scores to rate asthma control instead of GINA control categories, conversions were performed as follows: mean ACQ score ≤0.75 =well-controlled, mean ACQ score >0.75 to <1.5 = partly controlled, mean ACQ score ≥1.5 = uncontrolled; total ACT score >19 = well-controlled, total ACT score >15 to ≤19 = partly controlled, total ACT score ≤15 = uncontrolled. BEC, blood eosinophil count; FeNO, fractional exhaled nitric oxide; FEV1, post-bronchodilator forced expiratory volume in one second; IgE, immunoglobulin E; LTOCS, long-term oral corticosteroid; ppb, parts per billion.
The addition of BEC + FeNO marginally improved the prediction of post-biologic FEV1 increase (adjusted R2: 0.751), compared to BEC (adjusted R2: 0.747) or FeNO alone (adjusted R2: 0.743) (p=0.005 and <0.001, respectively; Table 3). However, prediction of post-biologic FEV1 improvement was not further improved by the addition of IgE, including all three biomarkers (i.e., BEC + FeNO + IgE; adjusted R2: 0.750; p=0.791 vs BEC + FeNO). The estimated magnitude of BEC and FeNO effects on post-biologic improvement in lung function, when both were included in the same model is presented in Figure 5. We noted a positive linear relationship for BEC and FeNO for each biologic class, with FeNO appearing to have the least effect in the anti-IL4Rα group (i.e. less separation of the lines). Stratifying mean change in lung function by pre-biologic BEC + FeNO categories revealed a post-biologic change (SD) in FEV1, which ranged from -48 (304) mL when both BEC and FeNO were low (i.e. <150 cells/µl and <25 ppb, respectively) to 276 (506) mL when both BEC and FeNO were high (i.e. >300 cells/µL and >50 ppb, respectively) (Supplementary Table 8A; Supplementary Figure 9). A similar pattern was noted by biologic class, with post-biologic lung function improving along a gradient from BEC + FeNO low to BEC + FeNO high, although patient numbers in each category were low (Supplementary Table 8B).
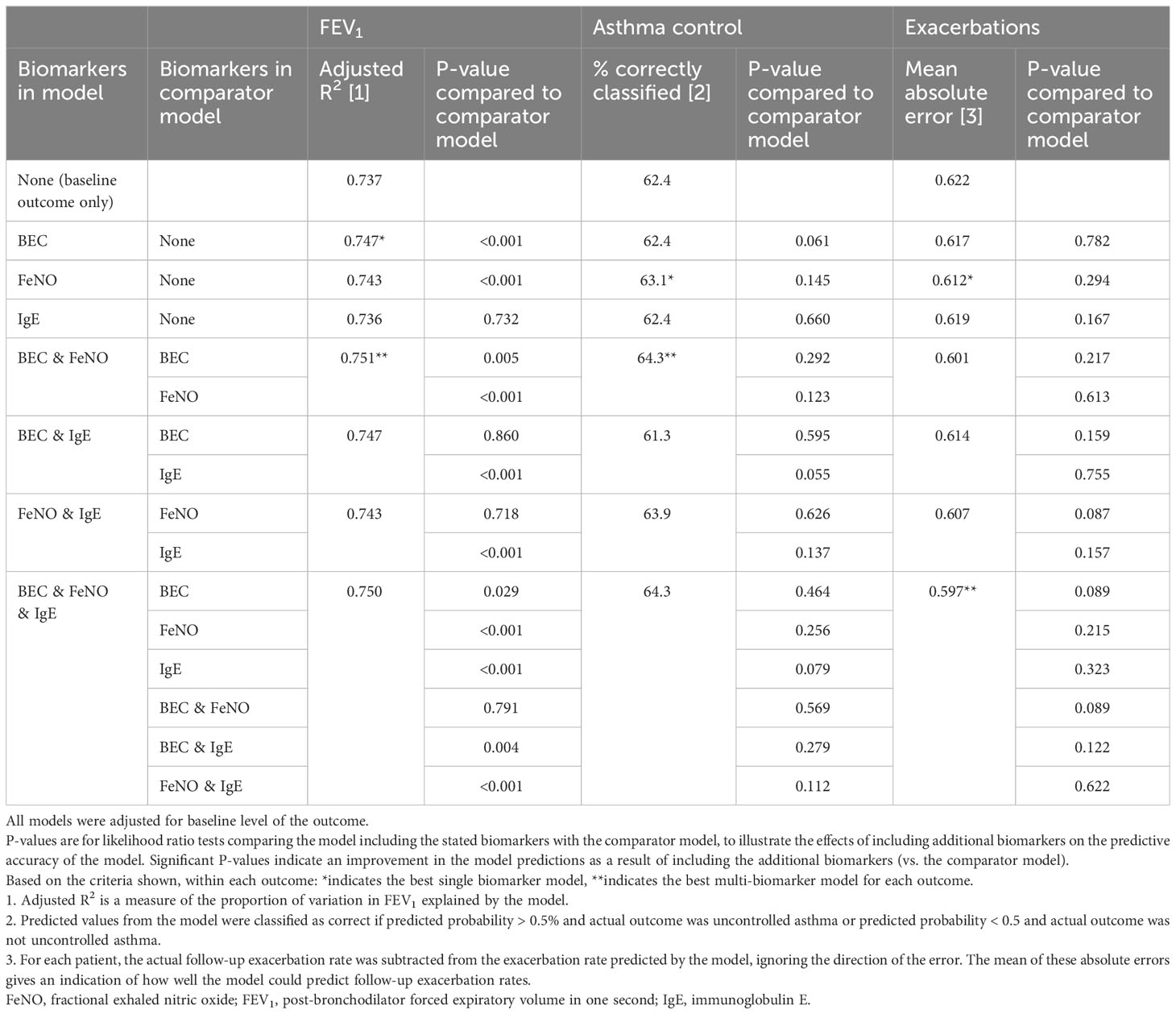
Table 3 Effect of using combined biomarkers to predict outcomes after biologic treatment.
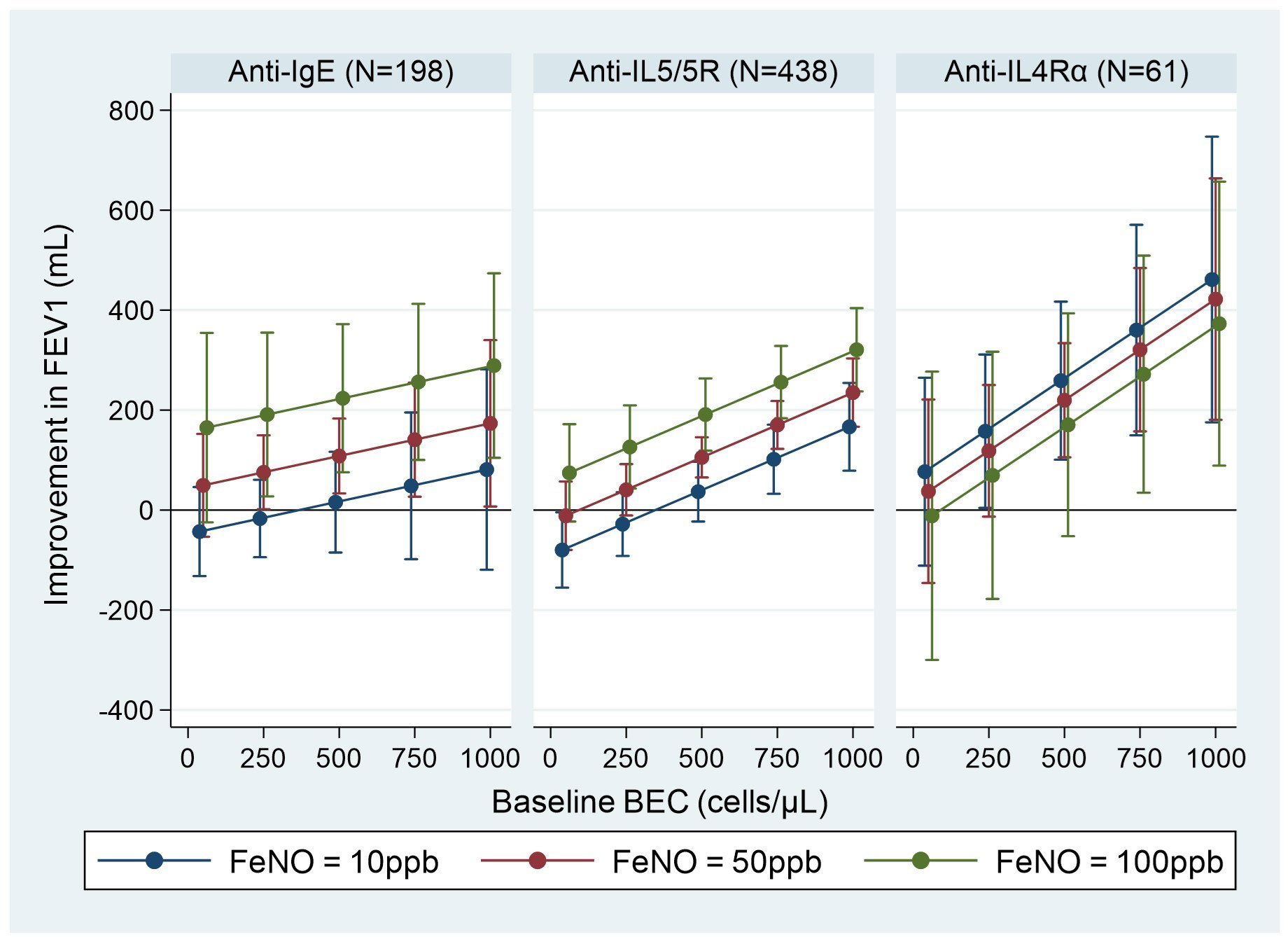
Figure 5 Association between pre-biologic BEC + FeNO and post biologic improvement in FEV1 by biologic class. BEC, blood eosinophil count; FeNO, fractional exhaled nitric oxide; FEV1, post-bronchodilator forced expiratory volume in one second. Graphs show point estimates (95% CI) of improvement in FEV1 for selected values of the biomarkers from the regression model including both baseline BEC and FeNO. Improvement in FEV1 is estimated for a patient with baseline FEV1 = 2.1 L (mean baseline FEV1 for the biologic patients in ISAR).
For efficient and cost-effective adoption of targeted treatment options in daily clinical practice, clinicians need point-of-care, well-defined, and reliable biomarkers or a combination of biomarkers to support them in identifying phenotypes and endotypes of asthma more likely to respond to biologic therapy (40). The real-life nature of our study was designed to directly inform that need, investigating pre-to-post biologic change in asthma outcomes along a gradient for three biomarkers used routinely in clinical practice (i.e., BEC, FeNO, and IgE), for three biologic classes (i.e., anti-IgE, anti-IL5/5R and anti-IL4Rα), and across 3 asthma outcomes (i.e., exacerbation rate, asthma control, and lung function). We found that individual biomarkers at their highest pre-biologic concentrations were associated with greater pre-to-post biologic change in some outcomes assessed; the strength of the association was both asthma outcome- and biologic class-specific. Overall, it appeared that pre-biologic biomarkers were not strongly associated with within-group decreases in exacerbation rate following biologic treatment. However, pre-biologic BEC and FeNO were strongly associated with lung function improvement for both anti-IgE and anti-IL5/5R therapies, with BEC also associated with improved asthma control for patients treated with anti-IL5/5R therapies. Use of biomarker combinations provided a small improvement in prediction of biologic-associated effectiveness, most notably the effectiveness on FEV1, and was unlikely to be of clinical significance for predicting any of the three outcomes studied.
GINA 2023 lists high BEC as a predictor of asthma response to anti-IgE, anti-IL5/5R, anti-IL4Rα, and anti-TSLP therapies for those with severe asthma and exacerbations in the last year (41) based on reported evidence of a strong association between pre-biologic BEC and post-biologic improvement in exacerbations (8, 42). Our results do not contradict that position, but rather represent a consequence of assessing the relationship between pre-biologic biomarker concentration and exacerbations in a different way (i.e., we observed a clinically meaningful reduction in exacerbation rate for anti-IgE, anti-IL5/5R, and anti-IL4Rα therapies, both at the high and low end of the concentration range for each biomarker assessed, but this reduction was relative to pre-biologic status, not compared to control). Indeed, others have shown the same relatively flat association of BEC concentration with pre-to-post biologic-associated exacerbation rate reduction (8, 41, 42). Our findings also may have been influenced by selection bias, i.e. how patients were selected for subsequent biologic treatment. Indeed, an additional post-hoc analysis again found little association between pre-biologic BEC and baseline exacerbation rate for patients who subsequently initiated biologics (most likely due to high BEC, a requirement for treatment with an anti-IL5/5R therapy), but a clear association was observed for those who were not started on any biologic (Supplementary Figure 10). We also included a much wider range of biomarker values (and wider gradient of biologic response) and our results may also have been influenced by noise from non-pathophysiologic factors in real-world patients not observed in tightly controlled RCT populations in which signal outweighs noise.
Higher pre-biologic BEC concentrations were, however, associated with greater improvements in lung function (anti-IgE and anti-IL5/5R therapies) and better asthma control (anti-IL5/5R therapies), a finding supported by others, who showed that sputum T2 markers (e.g. eosinophil count) seemed to be potentially predictive of super-response and remission after anti-IL5/5R therapy in a cohort of patients with severe eosinophilic asthma (43, 44). Improvement in lung function noted in the current study was particularly marked—approximately 100 mL and 200 mL for those with a BEC of 500 cells/µL and 1000 cells/µL, respectively. Even greater lung function improvements have recently been reported with increasing BEC following 52-week treatment with benralizumab: 1,081 mL FEV1 improvement in those with BEC >500 cells/µL compared to a 690 mL improvement in those with BEC ≤500 cells/µL, albeit in a small cohort of 18 patients with marked lung function impairment (mean ppFEV1: 56.7%) (19). Dupilumab, on the other hand, was found to increase lung function in patients with uncontrolled persistent asthma irrespective of BEC, increasing FEV1 by up to 430 mL in those with BEC ≥300 cells/µL (20). The ability to accurately predict which patients will experience a clinically relevant improvement in lung function when treated with biologics has important implications for earlier therapeutic intervention before permanent deterioration in lung function has occurred, when asthma is high-risk rather than severe. Indeed, as lung function in patients with severe asthma is quite heterogenous, it may be a more precise (or useful) tool to gauge biologic response than exacerbation rate (which is consistently high) or control (which is consistently poor) in this asthma population (29). Although Casale and colleagues found in the PROSPERO study that baseline BEC was associated with anti-IgE–induced improvement in asthma control and lung function, the magnitude of this improvement was not considered to be clinically relevant by the investigators and was not explored along a biomarker concentration gradient (45).
The current study also found a relationship between increasing pre-biologic FeNO levels and improved post-biologic outcome, but only for lung function, presumably because increased FeNO levels are associated with poor lung function and accelerated decline in lung function (46). GINA 2023 lists elevated baseline FeNO as predictive of response to anti-IgE, anti-IL4R, and anti-TSLP therapies, but not to anti-IL5/5R therapies (41). Our findings and those of others support this position for anti-IgE therapy (47, 48); however, we also found an association between pre-biologic FeNO and lung function improvement post–anti-IL5/5R treatment. This was not, however, apparent for anti-IL4Rα therapy, likely due to the small numbers of patients in this group and the large confidence intervals, particularly at the higher end of the FeNO concentration range—although interestingly, FeNO levels were markedly reduced with anti-IL4Rα therapy (Supplementary Figure 4). A recent large Phase 3 study by Pavord and colleagues found that baseline FeNO independently predicted dupilumab-associated lung function improvement in patients with moderate-to-severe asthma, with a 350 mL FEV1 improvement relative to placebo seen in those with FeNO >50 ppb compared to 40 mL for those with FeNO <25 ppb (12). Indeed, the European Academy of Allergy Asthma & Clinical Immunology (EAACI) position paper on clinically applicable biomarkers for asthma cites FeNO as the best biomarker to guide anti-IL4Rα-targeted (endotypic) therapy, which was evaluated following the SAVED approach (18). It should be noted that although it is a reproducible, easily measured, non-invasive biomarker, FeNO concentrations can fluctuate within days and may be affected by smoking history, atopy, adherence to inhaled corticosteroids, and high nitrite diet (18, 49–51).
We found no association between serum IgE concentrations and anti-IgE effectiveness. Consistent correlations between anti-IgE treatment response and baseline total serum IgE or antigen-specific IgE concentrations are lacking (52, 53), although recently use of cumulative IgE levels has been suggested (54). When patients were stratified post-hoc by T2 biomarkers, exacerbations were reduced to a greater degree in those with the presence of both modestly elevated IgE and T2 biomarkers, despite similar IgE concentrations (55). The EAACI position paper states that in severe allergic asthma, serum total IgE is useful in identifying patients who could benefit from anti-IgE therapy, but it cannot predict the degree of response after treatment (18). In patients with concomitant high eosinophil levels whose asthma remains uncontrolled, switching to an anti-eosinophilic treatment (i.e., anti-IL5/5R) might be a good option (18).
We found little added value in using composite biomarkers to predict biologic effectiveness. Such an effect may be apparent in a broader population with more heterogeneous asthma control and exacerbation rates, at least within countries. For example, we have previously found a greater pre-to-post biologic effect in patients with severe asthma and comorbid chronic rhinosinusitis with or without nasal polyps, which is associated with high BEC and FeNO levels (56). Lack of an association in our study may be due to poor correlation of biomarkers with each other, particularly for FeNO/IgE and BEC/IgE. One would expect highly correlated biomarkers to tell us the same thing, so a low correlation could be expected to make multiple biomarkers more useful, although this was something we did not find in our analysis. We also examined the effect of pre-biologic biomarker levels within group (i.e., pre-to-post) rather than versus placebo comparisons—hence the need for very large patient numbers to show within-arm difference—and acknowledge that multiple biomarkers will only perform better if they reflect or define a different entity that is capable of responding to treatment.
The RASP (Refractory Asthma Stratification Programme)-UK study group is examining the predictive value of using serum periostin, FeNO, and BEC as a composite biomarker to predict exacerbation risk, with preliminary results indicating that use of the three biomarkers in a ‘composite’ score further differentiated patients on the basis of exacerbation rate (57). U-BIOPRED (Unbiased biomarkers in Prediction of Respiratory Disease Outcomes) and SARP (Severe Asthma Research Program) are also seeking to better understand the prognostic value of individual biomarkers, their relationship to each other, and the prognostic value of using composite biomarkers or biomarker patterns (58).
Strengths of our study include inclusion of a large, heterogenous, adult severe asthma population, encompassing patients from 23 countries and representative of the general severe asthma population. The study was statistically powered to investigate differences across multiple outcome domains (i.e., exacerbation rate, lung function, and asthma control) along a biomarker concentration gradient (not simply dichotomized as high vs low) in a real-life setting. All analyses included at least 90 patients within each of the groups. This would have given us at least 80% power to observe an increase of ≥393 mL in FEV1, an incidence rate ratio of ≥1.85 for exacerbation rates, and an odds ratio ≤0.30 for uncontrolled asthma at follow-up per increment of 1,000 cells/µL BEC.
Limitations of our study included the small sample sizes for those treated with anti-IL4Rα therapy and those with values for all three biomarkers, and small numbers of patients with very high biomarker values, which could affect effect estimates at the highest end of the biomarker concentration spectrum. Timing of biomarker measurements and assessment of outcomes also varied considerably between patients. In common with other real-life studies of similar design without a comparator group, change in asthma outcomes may have been due to regression to the mean, subject to time-varying confounding. Furthermore, although we compared across biologic classes (i.e. anti-IgE, anti-IL5/5R and anti-IL4Rα), the remit of ISAR precludes direct comparison of biologics within class. Finally, 883 of 4,895 (18%) patients eligible for inclusion in the analysis of outcomes were excluded due to biologic switching. This is a potential source of bias; however, inclusion of those who switched biologic therapies may also have introduced bias. Further work on timing of biomarker assessment is warranted (i.e., highest pre-biologic biomarker concentration or value closest to biologic initiation), how biomarkers and combinations of biomarkers are associated with outcomes in those who switch biologics, and the identification of other biomarkers that may predict better response to biologics across a range of outcomes is warranted.
Our results provide a better understanding of pre-biologic biomarkers associated with better specific outcomes when treated with biologic therapy in a real-life setting and may be useful for clinicians when deciding between anti-IgE, anti-IL5/5R, and anti-IL4Rα biologic therapy options. The ability of both BEC and FeNO to predict biologic-associated improvement in FEV1 may encourage earlier intervention in patients at risk of accelerated lung function decline and promotes the use of lung function as a sensitive outcome to both predict and assess biologic effectiveness. The complexity of the asthma endotype requires going beyond the use of a ‘one size fits all’ composite biomarker predictive tool and instead opting for a more personalized approach matching biomarker(s), biologic, and asthma outcome.
The dataset supporting the conclusions of this article was derived from the International Severe Asthma Registry (ISAR). The authors do not have permission to give public access to the study dataset; researchers may request access to ISAR data for their own purposes. ISAR research requests and proposals can be made via the ISAR website (https://isaregistries.org/research-proposal-requests/) or via the enquiries email toaW5mb0Bpc2FyZWdpc3RyaWVzLm9yZw==. In line with ISAR governance restrictions, sharing individual deidentified participant data is subject to the consent of the ISAR steering committee in accordance with patient consent, patient confidentiality and ethical considerations. The study documents (protocol, statistical analysis plan, clinical study report) will be made available in accordance with the criteria of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (EUPAS38128). Proposals should be directed toaW5mb0Bpc2FyZWdpc3RyaWVzLm9yZw==; to gain access, if approved by the regulatory boards, data requestors will need to sign a data access agreement.
This study was designed, implemented, and reported in compliance with the European Network Centres for Pharmacoepidemiology and Pharmacovigilance Code of Conduct (EMA 2014; EUPAS43806) and with all applicable local and international laws and regulation. Registration of the ISAR database with the European Union Electronic Register of Post-Authorization studies was also undertaken (ENCEPP/DSPP/23720). ISAR has ethical approval from the Anonymised Data Ethics Protocols and Transparency (ADEPT) committee (ADEPT0218). Governance was provided by The Anonymous Data Ethics Protocols and Transparency (ADEPT) committee (registration number: ADEPT1621). All data collection sites in the International Severe Asthma Registry (ISAR) have obtained regulatory agreement in compliance with specific data transfer laws, country-specific legislation, and relevant ethical boards and organizations.
CP: Writing – original draft, Writing – review & editing. JT: Writing – original draft, Writing – review & editing. CB: Writing – original draft, Writing – review & editing. GCC: Writing – original draft, Writing – review & editing. GK: Writing – original draft, Writing – review & editing. DL: Writing – original draft, Writing – review & editing. TNT: Writing – original draft, Writing – review & editing. RA-L: Writing – original draft, Writing – review & editing. SB-A: Writing – original draft, Writing – review & editing. JB: Writing – original draft, Writing – review & editing. MH: Writing – original draft, Writing – review & editing. KK: Writing – original draft, Writing – review & editing. NP: Writing – original draft, Writing – review & editing. PEP: Writing – original draft, Writing – review & editing. TP: Writing – original draft, Writing – review & editing. CR: Writing – original draft, Writing – review & editing. MS: Writing – original draft, Writing – review & editing. M-JT: Writing – original draft, Writing – review & editing. CU: Writing – original draft, Writing – review & editing. MA-A: Writing – original draft, Writing – review & editing. AA: Writing – original draft, Writing – review & editing. ABe: Writing – original draft, Writing – review & editing. LBu: Writing – original draft, Writing – review & editing. VC: Writing – original draft, Writing – review & editing. BC: Writing – original draft, Writing – review & editing. KF: Writing – original draft, Writing – review & editing. SH: Writing – original draft, Writing – review & editing. LH: Writing – original draft, Writing – review & editing. RH: Writing – original draft, Writing – review & editing. PK: Writing – original draft, Writing – review & editing. RM: Writing – original draft, Writing – review & editing. TN: Writing – original draft, Writing – review & editing. LP: Writing – original draft, Writing – review & editing. DC: Writing – original draft, Writing – review & editing. FS: Writing – original draft, Writing – review & editing. MW: Writing – original draft, Writing – review & editing. RA: Writing – original draft, Writing – review & editing. ABo: Writing – original draft, Writing – review & editing. GB: Writing – original draft, Writing – review & editing. WC: Writing – original draft, Writing – review & editing. LC: Writing – original draft, Writing – review & editing. ED: Writing – original draft, Writing – review & editing. JF: Writing – original draft, Writing – review & editing. FH: Writing – original draft, Writing – review & editing. DJ: Writing – original draft, Writing – review & editing. RK: Writing – original draft, Writing – review & editing. BK: Writing – original draft, Writing – review & editing. MK: Writing – original draft, Writing – review & editing. AŁ: Writing – original draft, Writing – review & editing. LL: Writing – original draft, Writing – review & editing. ML: Writing – original draft, Writing – review & editing. BM: Writing – original draft, Writing – review & editing. NM: Writing – original draft, Writing – review & editing. AM-G: Writing – original draft, Writing – review & editing. PHwP: Writing – original draft, Writing – review & editing. AP: Writing – original draft, Writing – review & editing. PHP: Writing – original draft, Writing – review & editing. LP-d-L: Writing – original draft, Writing – review & editing. MP: Writing – original draft, Writing – review & editing. LR: Writing – original draft, Writing – review & editing. BR-C: Writing – original draft, Writing – review & editing. IS: Writing – original draft, Writing – review & editing. TRT: Writing – original draft, Writing – review & editing. CT-D: Writing – original draft, Writing – review & editing. EW: Writing – original draft, Writing – review & editing. MZ: Writing – original draft, Writing – review & editing. JA: Writing – original draft, Writing – review & editing. KA: Writing – original draft, Writing – review & editing. RC: Writing – original draft, Writing – review & editing. PG: Writing – original draft, Writing – review & editing. EH: Writing – original draft, Writing – review & editing. JM: Writing – original draft, Writing – review & editing. SN: Writing – original draft, Writing – review & editing. D-WP: Writing – original draft, Writing – review & editing. FP: Writing – original draft, Writing – review & editing. SS: Writing – original draft, Writing – review & editing. C-CS: Writing – original draft, Writing – review & editing. CS: Writing – original draft, Writing – review & editing. CTai: Writing – original draft, Writing – review & editing. TLT: Writing – original draft, Writing – review & editing. LBj: Writing – original draft, Writing – review & editing. GWC: Writing – original draft, Writing – review & editing. TI: Writing – original draft, Writing – review & editing. LJ-M: Writing – original draft, Writing – review & editing. CTau: Writing – original draft, Writing – review & editing. LBr: Writing – original draft, Writing – review & editing. DP: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was conducted by the Observational and Pragmatic Research Institute (OPRI) Pte Ltd and was partially funded by Optimum Patient Care Global (OPCG) and AstraZeneca Ltd. No funding was received by the OPRI for its contribution. The International Severe Asthma Registry (ISAR) is operated by OPCG and co-funded by OPCG and AstraZeneca.
The authors acknowledge Ms. Sarah Burkill (PhD) and Mr Peter Barker (PhD) for their contributions to the protocol development, and thank Ms Pui Yee Lai (MA), of the Observational and Pragmatic Research Institute (OPRI) for the editorial and formatting assistance that supported the development of this publication. Finally, a big thank you to our International Severe Asthma Registry collaborators (see online supplement).
CP has attended advisory boards for AstraZeneca, Novartis, TEVA, and Sanofi-Genzyme; has given lectures at meetings supported by AstraZeneca, Novartis, TEVA, Sanofi-Genzyme, and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, Novartis, MSD, Sanofi-Genzyme, GlaxoSmithKline, and Novartis; and has received educational and research grants from AstraZeneca, Novartis, TEVA, GlaxoSmithKline, ALK, and Sanofi-Genzyme. JT is an employee of the Observational and Pragmatic Research Institute OPRI. OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. CB reports advisory board participation of Sanofi-Regeneron, AstraZeneca, Takeda, ValeoPharma, honorarium for presentations for AstraZeneca/Amgen, GlaxoSmithKline, Grifols, Sanofi-Regeneron, ValeoPharma and grants paid to UBC from BioHaven, Sanofi-Regeneron, AstraZeneca, GlaxoSmithKline. GCC declares relevant research support from AstraZeneca and Sanofi. GK has attended advisory boards for AstraZeneca, GlaxoSmithKline and Chiesi. He has also given lectures at meetings supported by Novartis, Sanofi-Genzyme, AstraZeneca, GlaxoSmithKline, and Boehringer-Ingelheim. DL reports personal fees from ALK-Abelló, AstraZeneca national and global, Bayer, Chiesi, Grunenthal, Grin, GlaxoSmithKline national and global, Viatris, Menarini, MSD, Novartis, Pfizer, Sanofi, Siegfried, UCB, Carnot, grants from Abbvie, Bayer, Lilly, Sanofi, AstraZeneca, Pfizer, Novartis, Circassia, UCB, GlaxoSmithKline, outside the submitted work. TNT is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. RA-L has given lectures at meetings supported by AstraZeneca, Boehringer Ingelheim, Novartis, GlaxoSmithKline, and Sanofi, and participated in advisory board fees from GlaxoSmithKline, AstraZeneca, Novartis, and Abbott. SB-A has received honorarium for participation in expert advisory boards and given lectures for Teva Pharmaceuticals, AstraZeneca, GlaxoSmithKline, Meda, Mundipharma, Sanofi, Mylan and received unrestricted research grants from Mylan, AstraZeneca, Teva, Mundipharma International, GlaxoSmithKline, and Viatris. JB has received research grants from AstraZeneca and personnel fees from NuvoAir, outside the submitted work. MH declares grants and other advisory board fees made to his institutional employer from AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, Teva, and Seqirus, for unrelated projects. KK received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, ELPEN, Gilead, GlaxoSmithKline, Menarini, Novartis, Sanofi, Specialty Therapeutics, WebMD. His department has received funding and grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Innovis, ELPEN, GlaxoSmithKline, Menarini, Novartis and NuvoAir. NP has been a speaker and/or advisory board member for Abbott, Abbvie, ALK, Asit Biotech, AstraZeneca, Biomay, Boehringer Ingelheim, GlaxoSmithKline, HAL, Faes Farma, Medscape, Menarini, MSD, Novartis, Nutricia, OM Pharma, Regeneron, Sanofi, Takeda, and Viatris. PEP has attended advisory boards for AstraZeneca, GlaxoSmithKline, and Sanofi; has given lectures/webinars at meetings supported by AstraZeneca, Chiesi and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, GlaxoSmithKline, Novartis, Regeneron, and Sanofi, for which his institution received remuneration; and has a current research grant funded by GlaxoSmithKline. TP declares relevant research support from Novartis and Chiesi Pharma. CR received consulting/lecture fees from MSD, AstraZeneca, GlaxoSmithKline, Novartis, Takeda, Mundipharma, Boehringer-Ingelheim, Teva, Sanofi, and Bayer. MS has received honoraria from AstraZeneca, Boehringer Ingelheim, Teva, and GlaxoSmithKline for purposes unrelated to the content of this manuscript and has received research funding from AstraZeneca and Boehringer Ingelheim directly into his research account from AstraZeneca for unrelated projects. M-JT has received sponsorship to attend or speak at conferences, honoraria for lecturing or attending advisory boards, and research grants from the following companies: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Pfizer, Shionogi and Orient EuroPharma. CU reports personal fees for talks, participation in advisory boards etc. from AstraZeneca, GlaxoSmithKline, Teva, Boehringer Ingelheim, Orion Pharma, Sanofi Genzyme, TFF Pharmaceuticals, Covis Pharma, Berlin-Chemie, Takeda, Chiesi, and Pfizer, outside the submitted work. MA-A has received advisory board and speaker fees from AstraZeneca, Sanofi, Novartis, and GlaxoSmithKline and received a grant from Kuwait Foundation for the Advancement of Sciences KFAS. AA has received lecture fees from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, MSD, Norameda, Novartis, Orion, Sanofi, and Zentiva; sponsorships from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, GlaxoSmithKline, MSD, Norameda, Novartis, and Sanofi; and has participated in advisory boards for AstraZeneca, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, MSD, Novartis, Sanofi, and Teva. ABe is an employee of Optimum Patient Care Global, a co-funder of the International Severe Asthma Registry. LBu is an employee of the Observational and Pragmatic Research Institute OPRI. OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. VC is an employee of Optimum Patient Care OPC. OPC is a co-funder of the International Severe Asthma Registry. BC declares grants from Chiesi and GlaxoSmithKline; personal fees for advisory board activities from Chiesi, GlaxoSmithKline, Novartis, Sanofi, Teva, and AstraZeneca; and payment for lectures/speaking engagements from Chiesi, Novartis, GlaxoSmithKline, Menarini, and AstraZeneca, outside the submitted work. KF is an employee of Optimum Patient Care Global OPCG, a co-funder of the International Severe Asthma Registry. LH has received grant funding, participated in advisory boards and given lectures at meetings supported by Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Hoffmann la Roche, GlaxoSmithKline, Novartis, Theravance, Evelo Biosciences, Sanofi, and Teva; he has received grants from MedImmune, Novartis UK, Roche/Genentech Inc, and GlaxoSmithKline, Amgen, Genentech/Hoffman la Roche, AstraZeneca, MedImmune, GlaxoSmithKline, Aerocrine, and Vitalograph; he has received sponsorship for attending international scientific meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Napp Pharmaceuticals; he has also taken part in asthma clinical trials sponsored by AstraZeneca, Boehringer Ingelheim, Hoffmann la Roche, and GlaxoSmithKline for which his institution received remuneration; he is the Academic Lead for the Medical Research Council Stratified Medicine UK Consortium in Severe Asthma which involves industrial partnerships with a number of pharmaceutical companies including Amgen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Hoffmann la Roche, and Janssen. RH is an employee for Observational and Pragmatic Research Institute OPRI which conducted this study in collaboration with Optimum Patient Care and AstraZeneca. PK reports personal fees from Adamed, AstraZeneca, Berlin Chemie Menarini, FAES, Glenmark, Novartis, Polpharma, Boehringer Ingelheim, Teva, Zentiva, outside the submitted work. RM is a consultant for Observational and Pragmatic Research Institute OPRI which conducted this study in collaboration with Optimum Patient Care and AstraZeneca. TN received lecture fees from Kyorin, GlaxoSmithKline, Novartis, Sanofi, and AstraZeneca. LP received research grants and lecture fees from GlaxoSmithKline, Menarini, Chiesi, AstraZeneca and Grifols. DC has received speaker fees from AstraZeneca, Boehringer Ingelheim, and has acted as an investigator for trials sponsored by AstraZeneca. FS reports consultancy work for GlaxoSmithKline, AstraZeneca, Sanofi - Advisory board, received speaker fees from GlaxoSmithKline, AstraZeneca, Chiesi, Amgen, Teva and research grants from GlaxoSmithKline, AstraZeneca, and Chiesi. MW reports grants and/or personal fees from Novartis, Sanofi, Regeneron, Genentech, Sentien, Restorbio, Equillium, Genzyme, Cohero Health, Teva, Boehringer Ingelheim, AstraZeneca, Amgen, GlaxoSmithKline, Cytoreason, Cerecor, Sound Biologics, Incyte, and Kinaset. ABo has received industry-sponsored grants from AstraZeneca/MedImmune, Boehringer-Ingelheim, Cephalon/Teva, GlaxoSmithKline, Novartis, Sanofi-Regeneron, and consultancies with AstraZeneca/MedImmune, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, Regeneron-Sanofi, Med-in-Cell, Actelion, Merck, Roche, and Chiesi. GB has received honoraria for lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Novartis. He is a member of advisory boards for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, MSD Merck sharp & Dohme, Novartis, and Sanofi/Regeneron. LC has received speaker and consultancy fees and conference expenses from AstraZeneca, Novartis, GlaxoSmithKline, Boehringer Ingelheim and Menarini. ED declares grants to her institution from AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, Teva, and Seqirus, for unrelated projects and speaker fees from Sanofi. JF reports grants from research agreements with AstraZeneca, Mundipharma, Sanofi Regeneron, and Novartis. Personal fees for lectures and attending advisory boards: AstraZeneca, GlaxoSmithKline, Mundipharma, Novartis, Sanofi Regeneron, and Teva. FH declares honoraria from AstraZeneca, Sanofi, TEVA, GSK, and Genentech. She has been an investigator on clinical trials sponsored by GlaxoSmithKline, Genentech, and Sanofi, for which her institution has received funding. DJ has received speaker fees and consultancy fees from AstraZeneca, GlaxoSmithKline, Sanofi Regeneron, Boehringer Ingelheim and research funding from AstraZeneca. MK reports grant support from AstraZeneca, and honoraria for lectures and advisory board meetings paid to her hospital Singapore General Hospital from GlaxoSmithKline, AstraZeneca, Novartis, Sanofi and Boehringer Ingelheim, outside the submitted work. LL has received personal fees from ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Menarini, Novartis, Orion Pharma and Sanofi. NM is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. AM-G is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. PHwP has received honoraria for talks and advisory board meetings from GlaxoSmithKline, AstraZeneca, and Sanofi. AP has received fees and honoraria from Menarini, GlaxoSmithKline, Novartis, Elpen, Boehringer Ingelheim, AstraZeneca, and Chiesi. PHP has received advisory board and speaker fees from AstraZeneca, GlaxoSmithKline, Novartis, and Sanofi/Regeneron. LP-d-L reports grants, personal fees and non-financial support from AstraZeneca, personal fees and non-financial support from GlaxoSmithKline, grants, personal fees and non-financial support from Teva, personal fees and non-financial support from Chiesi, grants, personal fees and non-financial support from Sanofi, personal fees from MSD, personal fees from Techdow Pharma, grants, personal fees and non-financial support from Faes Farma, personal fees from Leo-Pharma, grants and personal fees from Gebro, personal fees from Gilead, outside the submitted work. MP declares personal fees and non-financial support from AstraZeneca, GlaxoSmithKline, and Sanofi. LR received fees as a speaker from AstraZeneca, GlaxoSmithKline, Novartis, and Sanofi. IS has received fees as advisory board participant and/or speaker from GlaxoSmithKline and Sanofi. CT-D has received fees as advisory board participant and/or speaker from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Sanofi-Aventis; has taken part in clinical trials from AstraZeneca, Novartis, and Sanofi-Aventis; has received unrestricted grants for investigator-initiated studies at Fundacion Neumologica Colombiana from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Grifols and Novartis. EW has received honoraria from AstraZeneca, GlaxoSmithKline, and Genentech. She has been an investigator on studies sponsored by AstraZeneca, GlaxoSmithKline, Genentech, Sanofi, Novartis, and Teva, for which her institution has received funding. RC has received honoraria for lectures from Aerogen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Teva. He is a member of advisory boards for GlaxoSmithKline and Novartis, has received grant support from GlaxoSmithKline and Aerogen and has patents in the use of acoustics in the diagnosis of lung disease, assessment of adherence and prediction of exacerbations. PG has received speaker fees and grants to his institution from AstraZeneca, GlaxoSmithKline, and Novartis. EH declares personal fees for advisory boards participation and/or speaker activities from: Sanofi, Regeneron, GlaxoSmithKline, Novartis, AstraZeneca, Stallergenes-Greer, Circassia, Bosch, Celltrion-Healthcare, Chiesi, and Almirall. JM reports speaker fees, grants or advisory boards for AstraZeneca, Sanofi, GlaxoSmithKline, Novartis, Inmunotek, Menarini and Noucor. D-WP received sponsorship to attend or speak at international meetings, honoraria for lecturing or attending advisory boards, and research grants from the following companies: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Daiichi Sankyo, Shionogi, and Orient Pharma. FP reports having received lectures or advisory board fees from: Menarini, Mundipharma, Chiesi, Alk Abello, AstraZeneca, Boehringer Ingelheim, Guidotti, Malesci, GlaxoSmithKline, Hal Allergy, Novartis, Sanofi, Regeneron, Stallergenes Greer, Valeas, and Almirall. SS declares research support and speaker fees from Cipla, Glenmark, and GlaxoSmithKline. C-CS has received speaker fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Pfizer, and has acted as an investigator for trials sponsored by AstraZeneca, Novartis, Roche, Sanofi-Regeneron, Galapagos, Shionogi, Aridis, Bristol Myers Squibb, Insmed, United Therapeutics, Enanta Pharmaceuticals, Areteia Therapeutics, Meiji, and Horizon Therapeutics. CT has received lecture or advisory board fees and grants to her institution from AstraZeneca, Sanofi, GlaxoSmithKline, Chiesi and Novartis, for unrelated projects. TT is an advisory Board Member for Boehringer Ingelheim, AstraZeneca, Takeda, GlaxoSmithKline, MSD, Mundipharma, and Janssen. Honoraria were received for these advisory boards. Honoraria were received for speaking at CMEs for AstraZeneca in the past. Conference sponsorships from AstraZeneca, Boehringer Ingelheim, Merck Serono, GlaxoSmithKline, Norvatis, Mundipharma and MSD. Research grants from Merck Serono Concor Study, MSD Apbord study. LBj has in the last three years received lecture or advisory board fees from Alk-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Sanofi, Genzyme/Regeneron, and Teva. GWC has received research grants, as well as lecture or advisory board fees from A. Menarini, Alk-Albello, Allergy Therapeutics, Anallergo, AstraZeneca, MedImmune, Boehringer Ingelheim, Chiesi Farmaceutici, Circassia, Danone, Faes, Genentech, Guidotti Malesci, GlaxoSmithKline, Hal Allergy, Merck, MSD, Mundipharma, Novartis, Orion, Sanofi Aventis, Sanofi, Genzyme/Regeneron, Stallergenes, UCB Pharma, Uriach Pharma, Teva, Thermo Fisher, and Valeas. TI received speaker bureau fees from Kyorin, GlaxoSmithKline, Novartis, Boehringer Ingelheim, AstraZeneca and Sanofi. LJ-M has received fees as advisory board participant and/or speaker from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Sanofi-Aventis; has participated in clinical trials for AstraZeneca, Novartis, and GlaxoSmithKline. DP has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; consultancy agreements with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; grants and unrestricted funding for investigator-initiated studies conducted through Observational and Pragmatic Research Institute Pte Ltd from AstraZeneca, Chiesi, Viatris, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Commune Digital, GlaxoSmithKline, Medscape, Viatris, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme, Teva Pharmaceuticals; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Novartis, Medscape, Teva Pharmaceuticals; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd Australia and UK and 92.61% of Observational and Pragmatic Research Institute Pte Ltd Singapore; 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation Programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1361891/full#supplementary-material
Supplementary Table 1 | characteristics of patients included for assessment of biomarker distribution and biomarker correlation analyses.
Supplementary Table 2 | Changes in biomarker concentration compared with baseline at different times post-biologic initiation.
Supplementary Table 3 | Changes in FeNO concentration compared with baseline at different times post-biologic initiation, stratified by baseline (highest pre-biologic) FeNO measurement.
Supplementary Table 4 | correlation of pre-biologic biomarkers taken with 7 days of each other stratified by LTOCS use.
Supplementary Table 5 | Point estimates (with 95% CI) for FEV1 from the regression models are shown for selected levels of (A) BEC, (B) FeNO and (C) IgE.
Supplementary Table 6 | Point estimates (with 95% CI) for probability of uncontrolled asthma from the regression models for selected levels of (A) BEC, (B) FeNO and (C) IgE concentrations.
Supplementary Table 7 | Point estimates (with 95% CI) for exacerbations from the regression models for selected levels of (A) BEC, (B) FeNO and (C) IgE concentration.
Supplementary Table 8 | (A) Pre-to-post biologic change in asthma outcome stratified by BEC and FeNO level: biologics overall (B) Pre-to-post biologic change in asthma outcome stratified by BEC and FeNO level: by biologic class.
Supplementary Figure 1 | Study design.
Supplementary Figure 2 | subject disposition.
Supplementary Figure 3 | Distribution of pre-biologic biomarkers (highest concentration) among patients enrolled in ISAR for all patients and according to LTOCS use at baseline.
Supplementary Figure 4 | Median biomarker changes compared with baseline, at different times after initiation of biologic therapy.
Supplementary Figure 5 | Correlation of pre-biologic biomarkers taken within 7 days of each other among patients enrolled in ISAR.
Supplementary Figure 6 | Associations between post-biologic decrease in exacerbations and pre-biologic biomarker levels by subgroups.
Supplementary Figure 7 | Associations between post-biologic probability of uncontrolled asthma and pre-biologic biomarker levels by subgroups.
Supplementary Figure 8 | Associations between post-biologic improvement in FEV1 and pre-biologic biomarker levels by subgroups.
Supplementary Figure 9 | Pre-to-post biologic change in FEV1 (mL) according to BEC + FeNO categories.
Supplementary Figure 10 | Association between baseline BEC and baseline exacerbation rate for patients, who (A) subsequently initiated and (B) did not initiate a biologic.
1. Wenzel SE. Severe adult asthmas: integrating clinical features, biology, and therapeutics to improve outcomes. Am J Respir Crit Care Med. (2021) 203:809–21. doi: 10.1164/rccm.202009-3631CI
2. Denton E, Price DB, Tran TN, Canonica GW, Menzies-Gow A, FitzGerald JM, et al. Cluster analysis of inflammatory biomarker expression in the international severe asthma registry. J Allergy Clin Immunol Pract. (2021) 9:2680–2688.e7. doi: 10.1016/j.jaip.2021.02.059
3. Heaney LG, Perez de Llano L, Al-Ahmad M, Backer V, Busby J, Canonica GW, et al. Eosinophilic and non-eosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. Chest. (2021) 160:814–30. doi: 10.1016/j.chest.2021.04.013
4. Busse WW, Holgate ST, Wenzel SW, Klekotka P, Chon Y, Feng J, et al. Biomarker profiles in asthma with high vs low airway reversibility and poor disease control. Chest. (2015) 148:1489–96. doi: 10.1378/chest.14-2457
5. Guida G, Carriero V, Bertolini F, Pizzimenti S, Heffler E, Paoletti G, et al. Exhaled nitric oxide in asthma: from diagnosis to management. Curr Opin Allergy Clin Immunol. (2023) 23:29–35. doi: 10.1097/ACI.0000000000000877
6. Lee LA, Bailes Z, Barnes N, Boulet L-P, Edwards D, Fowler A, et al. Efficacy and safety of once-daily single-inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with inadequately controlled asthma (CAPTAIN): a double-blind, randomised, phase 3A trial. Lancet Respir Med. (2021) 9:69–84. doi: 10.1016/S2213-2600(20)30389-1
7. Corren J, Pham T-H, Garcia Gil E, Sałapa K, Ren P, Parnes JR, et al. Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy. (2022) 77:1786–96. doi: 10.1111/all.15197
8. Ortega HG, Yancey SW, Mayer B, Gunsoy NB, Keene ON, Bleecker ER, et al. Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: a secondary analysis of the DREAM and MENSA studies. Lancet Respir Med. (2016) 4:549–56. doi: 10.1016/S2213-2600(16)30031-5
9. Bernstein JA, Virchow JC, Murphy K, Maspero JF, Jacobs J, Adir Y, et al. Effect of fixed-dose subcutaneous reslizumab on asthma exacerbations in patients with severe uncontrolled asthma and corticosteroid sparing in patients with oral corticosteroid-dependent asthma: results from two phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir Med. (2020) 8:461–74. doi: 10.1016/S2213-2600(19)30372-8
10. FitzGerald JM, Bleecker ER, Nair P, Korn S, Ohta K, Lommatzsch M, et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. (2016) 388:2128–41. doi: 10.1016/S0140-6736(16)31322-8
11. Menzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. (2021) 384:1800–9. doi: 10.1056/NEJMoa2034975
12. Pavord ID, Deniz Y, Corren J, Casale TB, FitzGerald JM, Izuhara K, et al. Baseline feNO independently predicts the dupilumab response in patients with moderate-to-severe asthma. J Allergy Clin Immunol Pract. (2023) 11:1213–1220.e2. doi: 10.1016/j.jaip.2022.11.043
13. Ray A, Das J, Wenzel SE. Determining asthma endotypes and outcomes: Complementing existing clinical practice with modern machine learning. Cell Rep Med. (2022) 3:100857. doi: 10.1016/j.xcrm.2022.100857
14. Busby J, Khoo E, Pfeffer PE, Mansur AH, Heaney LG. The effects of oral corticosteroids on lung function, type-2 biomarkers and patient-reported outcomes in stable asthma: A systematic review and meta-analysis. Respir Med. (2020) 173:106156. doi: 10.1016/j.rmed.2020.106156
15. Li H, Zhang Q, Wang J, Gao S, Li C, Wang J, et al. Variability of Type 2 inflammatory markers guiding biologic therapy of severe asthma: A 5-year retrospective study from a single tertiary hospital. World Allergy Organ J. (2021) 14:100547. doi: 10.1016/j.waojou.2021.100547
16. Sánchez J, Morales E, Santamaria L-C, Acevedo A-M, Calle A, Olivares M, et al. IgE, blood eosinophils and FeNO are not enough for choosing a monoclonal therapy among the approved options in patients with type 2 severe asthma. World Allergy Organ J. (2021) 14:100520. doi: 10.1016/j.waojou.2021.100520
17. Porsbjerg CM, Menzies-Gow AN, Tran TN, Murray RB, Unni B, Audrey Ang SL, et al. Global variability in administrative approval prescription criteria for biologic therapy in severe asthma. J Allergy Clin Immunol Pract. (2022) 10:1202–16. doi: 10.1016/j.jaip.2021.12.027
18. Diamant Z, Vijverberg S, Alving K, Bakirtas A, Bjermer L, Custovic A, et al. Toward clinically applicable biomarkers for asthma: An EAACI position paper. Allergy. (2019) 74:1835–51. doi: 10.1111/all.13806
19. Menzella F, Fontana M, Galeone C, Ghidoni G, Capobelli S, Ruggiero P, et al. Real world effectiveness of benralizumab on respiratory function and asthma control. Multidiscip Respir Med. (2021) 16:785. doi: 10.4081/mrm.2021.785
20. Wenzel S, Castro M, Corren J, Maspero J, Wang L, Zhang B, et al. Dupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting β2 agonist: a randomised double-blind placebo-controlled pivotal phase 2b dose-ranging trial. Lancet. (2016) 388:31–44. doi: 10.1016/S0140-6736(16)30307-5
21. Corren J, Weinstein S, Janka L, Zangrilli J, Garin M. Phase 3 study of reslizumab in patients with poorly controlled asthma: effects across a broad range of eosinophil counts. Chest. (2016) 150:799–810. doi: 10.1016/j.chest.2016.03.018
22. Soremekun S, Heaney LG, Skinner D, Bulathsinhala L, Carter V, Chaudhry I, et al. Asthma exacerbations are associated with a decline in lung function: a longitudinal population-based study. Thorax. (2023) 78(7):643–52. doi: 10.1136/thorax-2021-217032
23. Sears MR. Lung function decline in asthma. Eur Respir J. (2007) 30:411–3. doi: 10.1183/09031936.00080007
24. Calhoun WJ, Haselkorn T, Miller DP, Omachi TA. Asthma exacerbations and lung function in patients with severe or difficult-to-treat asthma. J Allergy Clin Immunol. (2015) 136:1125–1127.e4. doi: 10.1016/j.jaci.2015.05.014
25. Perez de Llano L, Scelo G, Tran TN, Le TT, Martin N, Fageras M, et al. Characteristics associated with clinical remission in patients with severe asthma who initiate biologics. Eur Respir J. (2023) 62:PA1892. doi: 10.1183/13993003.congress-2023.PA1892
26. ISAR Study Group. International severe asthma registry (ISAR): mission statement. Chest. (2020) 157:805–14. doi: 10.1016/j.chest.2019.10.051
27. FitzGerald JM, Tran TN, Alacqua M, Altraja A, Backer V, Bjermer L, et al. International severe asthma registry (ISAR): protocol for a global registry. BMC Med Res Methodol. (2020) 20:212. doi: 10.1186/s12874-020-01065-0
28. Cushen B, Koh MS, Tran TN, Martin N, RB M, Uthaman T. Adult severe asthma registries: a global and growing inventory. Prag Observational Res. (2023) 14:127–47. doi: 10.2147/POR.S399879
29. Wang E, Wechsler ME, Tran TN, Heaney LG, Jones RC, Menzies-Gow AN, et al. Characterization of severe asthma worldwide: data from the International Severe Asthma Registry (ISAR). Chest. (2020) 157:790–804. doi: 10.1016/j.chest.2019.10.053
30. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention . Available online at: https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report_-final-_wms.pdf (Accessed 26th March 2024).
31. Global Initiative for Asthma. Global Strategy for Asthma Prevention and Treatment (2018). Available online at: https://ginasthma.org/wp-content/uploads/2019/01/2018-GINA.pdf (Accessed 26th March 2024).
32. Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. (2004) 113:59–65. doi: 10.1016/j.jaci.2003.09.008
33. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. (1999) 14:902–7. doi: 10.1034/j.1399-3003.1999.14d29.x
34. Korn S, Both J, Jung M, Hübner M, Taube C, Buhl R. Prospective evaluation of current asthma control using ACQ and ACT compared with GINA criteria. Ann Allergy Asthma Immunol. (2011) 107:474–9. doi: 10.1016/j.anai.2011.09.001
35. Koolen BB, Pijnenburg MWH, Brackel HJL, Landstra AM, van den Berg NJ, Merkus PJFM, et al. Comparing global initiative for asthma (GINA) criteria with the childhood asthma control test (C-ACT) and asthma control test (ACT). Eur Respir J. (2011) 38:561–6. doi: 10.1183/09031936.00173710
36. Canonica GW, Blasi F, Carpagnano GE, Guida G, Heffler E, Paggiaro P, et al. Severe asthma network Italy definition of clinical remission in severe asthma: A delphi consensus. J Allergy Clin Immunol Pract. (2023) 11(2):3629–37. doi: 10.1016/j.jaip.2023.07.041
37. McDowell PJ, McDowell R, Busby J, Eastwood MC, Patel PH, Jackson DJ, et al. Clinical remission in severe asthma with Biologic Therapy: an analysis from the UK Severe Asthma Registry. Eur Respir J. (2023) 62(6):2300819. doi: 10.1183/13993003.00819-2023
38. Hansen S, Søndergaard M, von Bülow A, Bjerrum A-S, Schmid J, Rasmussen LM, et al. Clinical response and remission in severe asthma patients treated with biologic therapies. Chest. (2024) 105(2):253–66. doi: 10.1016/j.chest.2023.10.046
39. Tukey JW. Some thoughts on clinical trials, especially problems of multiplicity. Science. (1977) 198:679–84. doi: 10.1126/science.333584
40. Muraro A, Lemanske RFJ, Hellings PW, Akdis CA, Bieber T, Casale TB, et al. Precision medicine in patients with allergic diseases: Airway diseases and atopic dermatitis-PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. (2016) 137:1347–58. doi: 10.1016/j.jaci.2016.03.010
41. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention (2023). Available online at: https://ginasthma.org/wp-content/uploads/2023/05/GINA-2023-Full-Report-2023-WMS.pdf (Accessed 26th March 2024).
42. FitzGerald JM, Bleecker ER, Menzies-Gow A, Zangrilli JG, Hirsch I, Metcalfe P, et al. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir Med. (2018) 6:51–64. doi: 10.1016/S2213-2600(17)30344-2
43. Moermans C, Brion C, Bock G, Graff S, Gerday S, Nekoee H, et al. Sputum type 2 markers could predict remission in severe asthma treated with anti-IL-5. Chest. (2023) 163(6):1368–79. doi: 10.1016/j.chest.2023.01.037
44. Gerday S, Graff S, Moermans C, Guissard F, Paulus V, Henket M, et al. Super-responders to anti-IL-5/anti-IL-5R are characterised by high sputum eosinophil counts at baseline. Thorax. (2023) 78:1138–41. doi: 10.1136/thorax-2022-219781
45. Casale TB, Luskin AT, Busse W, Zeiger RS, Trzaskoma B, Yang M, et al. Omalizumab effectiveness by biomarker status in patients with asthma: evidence from PROSPERO, A prospective real-world study. J Allergy Clin Immunol Pract. (2019) 7:156–164.e1. doi: 10.1016/j.jaip.2018.04.043
46. Loewenthal L, Menzies-Gow A. FeNO in asthma. Semin Respir Crit Care Med. (2022) 43:635–45. doi: 10.1055/s-0042-1743290
47. Kavati A, Zhdanava M, Ortiz B, Lecocq J, Schiffman B, Pilon D, et al. Retrospective study on the association of biomarkers with real-world outcomes of omalizumab-treated patients with allergic asthma. Clin Ther. (2019) 41:1956–71. doi: 10.1016/j.clinthera.2019.07.021
48. Solidoro P, Patrucco F, de Blasio F, Brussino L, Bellocchia M, Dassetto D, et al. Predictors of reversible airway obstruction with omalizumab in severe asthma: a real-life study. Ther Adv Respir Dis. (2019) 13:1753466619841274. doi: 10.1177/1753466619841274
49. Schleich FN, Seidel L, Sele J, Manise M, Quaedvlieg V, Michils A, et al. Exhaled nitric oxide thresholds associated with a sputum eosinophil count ≥3% in a cohort of unselected patients with asthma. Thorax. (2010) 65:1039–44. doi: 10.1136/thx.2009.124925
50. Kostikas K, Minas M, Papaioannou AI, Papiris S, Dweik RA. Exhaled nitric oxide in asthma in adults: the end is the beginning? Curr Med Chem. (2011) 18:1423–31. doi: 10.2174/092986711795328436
51. Zuiker RGJA, Boot JD, Calderon C, Piantone A, Petty K, de Kam M, et al. Sputum induction with hypertonic saline reduces fractional exhaled nitric oxide in chronic smokers and non-smokers. Respir Med. (2010) 104:917–20. doi: 10.1016/j.rmed.2010.02.006
52. Wahn U, Martin C, Freeman P, Blogg M, Jimenez P. Relationship between pretreatment specific IgE and the response to omalizumab therapy. Allergy. (2009) 64:1780–7. doi: 10.1111/j.1398-9995.2009.02119.x
53. Korn S, Haasler I, Fliedner F, Becher G, Strohner P, Staatz A, et al. Monitoring free serum IgE in severe asthma patients treated with omalizumab. Respir Med. (2012) 106:1494–500. doi: 10.1016/j.rmed.2012.07.010
54. Naumova V, Beltyukov E, Niespodziana K, Errhalt P, Valenta R, Karaulov A, et al. Cumulative IgE-levels specific for respiratory allergens as biomarker to predict efficacy of anti-IgE-based treatment of severe asthma. Front Immunol. (2022) 13:941492. doi: 10.3389/fimmu.2022.941492
55. Hanania NA, Wenzel S, Rosén K, Hsieh H-J, Mosesova S, Choy DF, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med. (2013) 187:804–11. doi: 10.1164/rccm.201208-1414OC
56. Wechsler ME, Scelo G, Larenas-Linemann DES, Torres-Duque CA, Maspero J, Tran TN, et al. Association between T2-related comorbidities and effectiveness of biologics in severe asthma. Am J Respir Crit Care Med. (2023) 209:262–72. doi: 10.1164/rccm.202305-0808OC
57. Heaney LG, Djukanovic R, Woodcock A, Walker S, Matthews JG, Pavord ID, et al. Research in progress: medical research council United Kingdom refractory asthma stratification programme (RASP-UK). Thorax. (2016) 71:187–9. doi: 10.1136/thoraxjnl-2015-207326
58. Silkoff PE, Moore WC, Sterk PJ. Three major efforts to phenotype asthma: severe asthma research program, asthma disease endotyping for personalized therapeutics, and unbiased biomarkers for the prediction of respiratory disease outcome. Clin Chest Med. (2019) 40:13–28. doi: 10.1016/j.ccm.2018.10.016
Keywords: severe asthma, biomarkers, eosinophil (EOS), FeNO (Fraction of exhaled Nitric Oxide), biologics, FEV1, personalized medicine (PM)
Citation: Porsbjerg CM, Townend J, Bergeron C, Christoff GC, Katsoulotos GP, Larenas-Linnemann D, Tran TN, Al-Lehebi R, Bosnic-Anticevich SZ, Busby J, Hew M, Kostikas K, Papadopoulos NG, Pfeffer PE, Popov TA, Rhee CK, Sadatsafavi M, Tsai M-J, Ulrik CS, Al-Ahmad M, Altraja A, Beastall A, Bulathsinhala L, Carter V, Cosio BG, Fletton K, Hansen S, Heaney LG, Hubbard RB, Kuna P, Murray RB, Nagano T, Pini L, Cano Rosales DJ, Schleich F, Wechsler ME, Amaral R, Bourdin A, Brusselle GG, Chen W, Chung LP, Denton E, Fonseca JA, Hoyte F, Jackson DJ, Katial R, Kirenga BJ, Koh MS, Ławkiedraj A, Lehtimäki L, Liew MF, Mahboub B, Martin N, Menzies-Gow AN, Pang PH, Papaioannou AI, Patel PH, Perez-De-Llano L, Peters MJ, Ricciardi L, Rodríguez-Cáceres B, Solarte I, Tay TR, Torres-Duque CA, Wang E, Zappa M, Abisheganaden J, Assing KD, Costello RW, Gibson PG, Heffler E, Máspero J, Nicola S, Perng D-W, Puggioni F, Salvi S, Sheu C-C, Sirena C, Taillé C, Tan TL, Bjermer L, Canonica GW, Iwanaga T, Jiménez-Maldonado L, Taube C, Brussino L and Price DB (2024) Association between pre-biologic T2-biomarker combinations and response to biologics in patients with severe asthma. Front. Immunol. 15:1361891. doi: 10.3389/fimmu.2024.1361891
Received: 27 December 2023; Accepted: 29 March 2024;
Published: 19 April 2024.
Edited by:
Harissios Vliagoftis, University of Alberta, CanadaCopyright © 2024 Porsbjerg, Townend, Bergeron, Christoff, Katsoulotos, Larenas-Linnemann, Tran, Al-Lehebi, Bosnic-Anticevich, Busby, Hew, Kostikas, Papadopoulos, Pfeffer, Popov, Rhee, Sadatsafavi, Tsai, Ulrik, Al-Ahmad, Altraja, Beastall, Bulathsinhala, Carter, Cosio, Fletton, Hansen, Heaney, Hubbard, Kuna, Murray, Nagano, Pini, Cano Rosales, Schleich, Wechsler, Amaral, Bourdin, Brusselle, Chen, Chung, Denton, Fonseca, Hoyte, Jackson, Katial, Kirenga, Koh, Ławkiedraj, Lehtimäki, Liew, Mahboub, Martin, Menzies-Gow, Pang, Papaioannou, Patel, Perez-De-Llano, Peters, Ricciardi, Rodríguez-Cáceres, Solarte, Tay, Torres-Duque, Wang, Zappa, Abisheganaden, Assing, Costello, Gibson, Heffler, Máspero, Nicola, Perng (Steve), Puggioni, Salvi, Sheu, Sirena, Taillé, Tan, Bjermer, Canonica, Iwanaga, Jiménez-Maldonado, Taube, Brussino and Price. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David B. Price, ZHByaWNlQG9wcmkuc2c=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.