 Janosch Railton1†Martina Volonté1†
Janosch Railton1†Martina Volonté1† Eugenio Isoletta1†
Eugenio Isoletta1† Alice Bonelli1Stefania Barruscotti1†
Alice Bonelli1Stefania Barruscotti1† Valeria Brazzelli1,2*†
Valeria Brazzelli1,2*†- 1Institute of Dermatology, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
- 2Department of Clinical, Surgical, Diagnostic and Pediatric Sciences, Institute of Dermatology, Università degli Studi di Pavia, Pavia, Italy
Objective: The aim of this study is to review the life of patients with psoriasis on biologic therapy during the SARS-CoV-2 pandemic and the relevance of frailty within this context, reviewing studies that describe the course and severity of infection in patients with psoriasis on biologics, the seroprevalence of SARS-CoV-2, and the safety and efficacy of the BNT162b2 vaccine in these patients.
Materials and methods: The keywords “Psoriasis,” “Biologics,” “SARS-CoV-2,” “COVID-19,” and “BNT162b2 Vaccine” were used in various combinations on database engines to find relevant articles on this topic.
Results: A total of 36 articles were found, with 20 concerning the course, severity, and seroprevalence of SARS-CoV-2 in patients with psoriasis on biologic therapy and 16 concerning safety and efficacy of BNT162b2 in these patients.
Discussion: Patients with psoriasis on biologic therapy did not have increased seroprevalence compared with the general population, indicating that they were not at an increased risk of SARS-CoV-2 infection compared with the general population. Furthermore, the immunosuppressive action of biologics may be protective, as patients on biologic therapy had better outcomes and less risk of severe infection. The seroconversion rate against SARS-CoV-2 from the BNT162b2 vaccine was similar in both patients with psoriasis on biologics and the general population, indicating that efficacy is not hindered by the biologic therapy. However, the cellular response in population with psoriasis was significantly less intense, and the humoral immune response was weaker than that in the general population, demonstrating that the possibility of tighter vaccination schedules and additional doses may be advantageous in these patients.
1 Introduction
Frailty is increasingly becoming more and more relevant within the medical and health care world, due to the increasing life expectancy and the increase in personalized medicine. Recognizing frailty is an important step into further personalizing medicine, so that we can fully assess and care for the patients and their needs, especially concerning protection against disease and treating any current diseases at the same time, weighing out the risks and benefits in each individual. -
The invention of biologic therapy has changed how we treat many diseases, including psoriasis. However, these medications come with a risk, due to secondary immunosuppression, leaving patients vulnerable to infection. The Italian Ministry of Health considers patients on biologic therapy frail. This sparked a discussion about whether or not these patients require extra attention and care during the pandemic, considering that booster doses were recommended to frail patients due to a lower seroconversion and efficacy.
The effect of SARS-CoV-2 on this population will be studied, along with the interaction of biologic therapy on the course of the infection and the risk of increased infections or severe infections within this specific cohort. Finally, the interaction of biologic therapy on the BNT162b2 vaccine in this population will be studied.
2 Materials and methods
This review was initiated by searching combinations of the keywords “Psoriasis,” “Biologics,” “Frailty,” “COVID-19,” “SARS-CoV-2,” and “BNT162b2 Vaccine” within various databases such as PubMed and Google Scholar. The abstracts were pre-screened, and the literature was collected.
Following the pre-screening, papers were selected if the met following the criteria:
(1) Literature was written on primary research.
(2) Patients with psoriasis of any form were included.
(3) Patients were on biologic therapy.
(4) The literature was published during the COVID-19 pandemic (from January 2020 to October 2023).
Papers were excluded if they did not follow all of the criteria.
Regarding the literature regarding the BNT162b2 (Pfizer) Vaccine, papers were selected if evidence and results of serologic testing following the efficacy of at least one dose of the vaccine were present.
3 Results
Overall, 1,028 articles were found from the initial keyword search; after a brief pre-screening, five articles were discarded because of being in a different language and one article was not available. After screening the titles and abstracts of the 1,022 remaining articles, 998 articles were excluded because of being unrelated to the study. The full text of the 114 remaining articles was reviewed, with 81 articles being screened out because of not following the criteria after analysis.
The remaining 36 articles all met all the inclusion criteria and were chosen for this study. The studies were divided and reviewed into two tables: first, 30 articles were found regarding the course, severity, and seroprevalence of SARS-CoV-2 inpatients with psoriasis (see Table 1); and, second, 16 articles regarding the efficacy and safety of the BNT162b2 vaccine in the population with psoriasis on biologics were found (see Table 2).
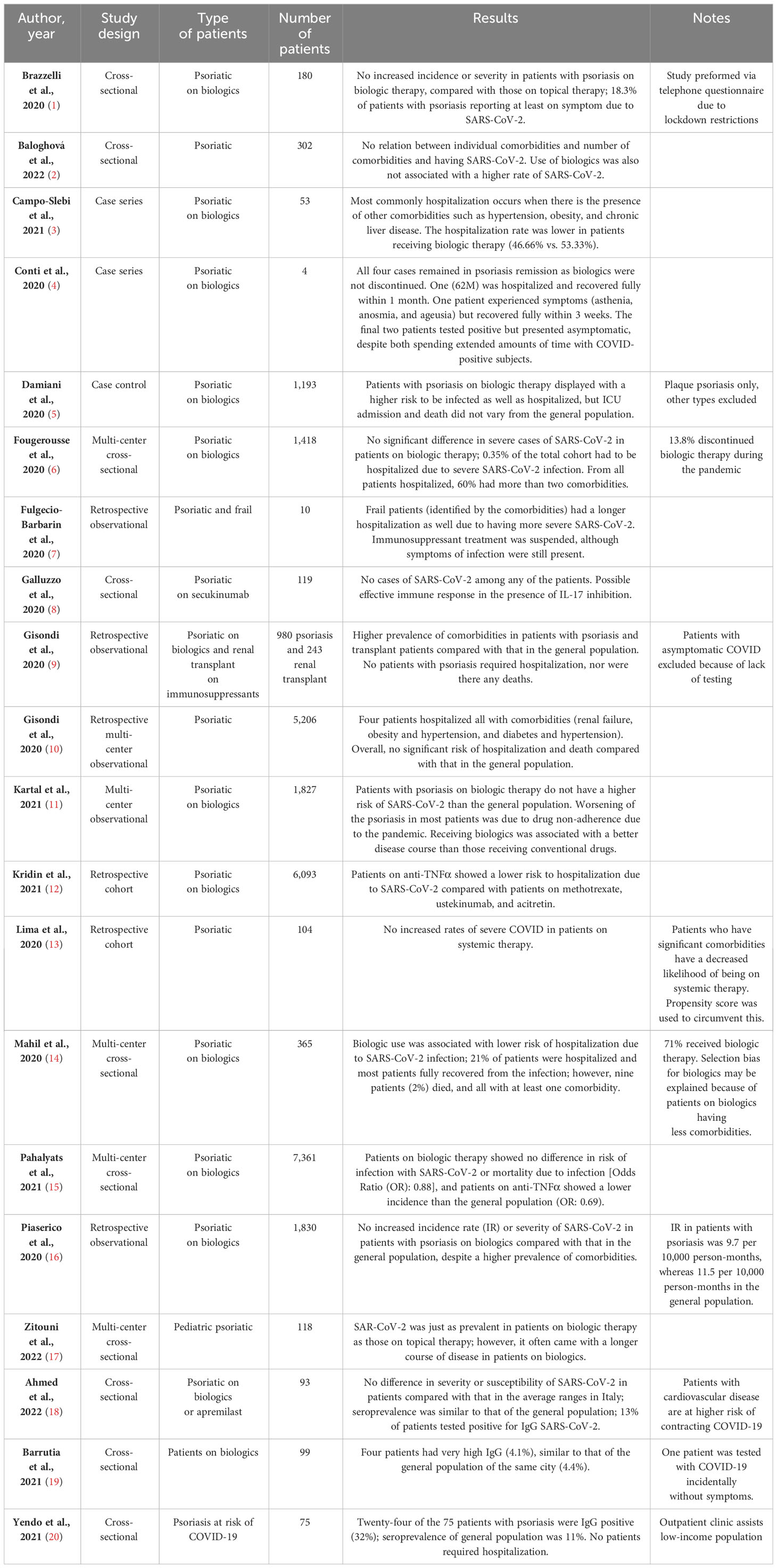
Table 1 Course and severity of SARS-CoV-2 infection in patients with psoriasis on biologic therapy.
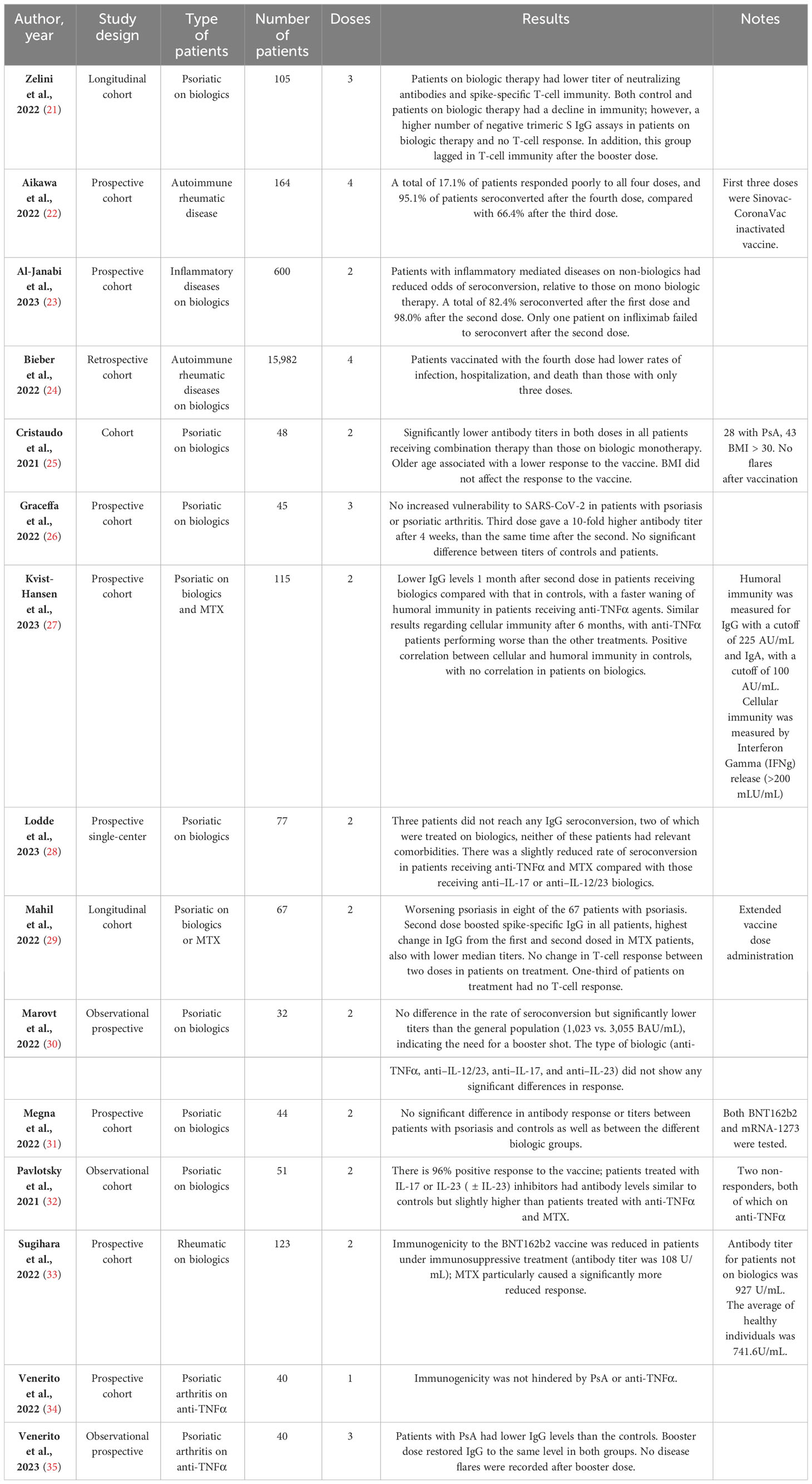
Table 2 Efficacy and safety of the BNT162b2 vaccine in the population with psoriasis on biologic therapy.
3.1 Course and severity of SARS-CoV-2 in patients with psoriasis on biologics
The definition of frailty concerns a wide range of patients and describes a clinical state in which there is an increase in an individual’s vulnerability to developing negative health-related events (including disability, hospitalizations, institutionalizations, and death) when exposed to endogenous or exogenous stressors (36, 37). According to the Italian Ministry of Health, patients on biologic therapy are considered frail, due to immunodeficiency from the inhibition of specific cytokines (38).
At the initial stages of the pandemic, Brazzelli et al. conducted an observational prevalence study over the phone with 180 patients with psoriasis on biologic therapy. Using a questionnaire on self-reported symptoms and SARS-CoV-2 positivity, they found that there was no increased incidence or severity of SARS-CoV-2 in this population. Furthermore, 18.3% of patients with psoriasis reported at least one symptom due to SARS-CoV-2, with no significant difference between patients on biologic therapies and those on other non-biologic therapies (1). With the same cohort of patients, the seroprevalence was assessed by Ahmed et al. It was found that 13% of the patients tested seropositive for SARS-CoV-2. The self-reported data being similar to the seroprevalence indicate a strong awareness of SARS-CoV-2 infection in these patients (1, 18).
Barrutia et al. observed that seroprevalence of SARS-CoV-2 in patients with psoriasis was in line with that of the general population (4.1% vs. 4.4%) (19). Another study by Yendo et al. found that the seroprevalence of SARS-CoV-2 in their cohort of patients with psoriasis of biologic therapy in Sao Paolo was higher than that in the general population (32% vs. 11%) (20). The authors suggest that the numbers are high due to the cohort of patients coming from a lower-income clinic, resulting in socioeconomic disparities, due to limited diagnostic tests, less access to education regarding the pandemic, and lack of contact tracing (20).
Conti et al. described four cases of SARS-CoV-2–positive patients with psoriasis on biologic therapy who fully recovered, only one of which required hospitalization (4). Galluzzo et al. reported that there was not a single SARS-CoV-2–positive case among their cohort of 119 patients with psoriasis on secukinumab, suggesting protective benefits from the biologic therapy (8).
A multitude of studies reported that the prevalence of COVID-19 infection rate and the length of recovery were higher in patients with psoriasis on biologic therapy when comorbidities were present. However, there was no significant difference in the rate of hospitalization or severe disease in psoriatic cohorts on biologic therapy compared with that in the general population (3, 7, 9–11, 17). Fougerousse et al. and Piaserico et al. reported lower rates of severe disease, despite higher rates of comorbidities within their cohorts patients with psoriasis on biologic therapy (6, 39). Mahil et al. found that, along with lower rates of hospitalization, patients on biologic therapy had lower rates of required mechanical ventilation and death (14).
Pahalyats et al. and Kridin et al. identified that there was no association between the use of biologics and SARS-CoV-2 infection and subsequent mortality. They also report that treatment with Tumour Necrosis Factor Alpha (TNFα) inhibitors showed lower infection rates (12, 15). Kridin et al. also noted that the patients on TNFα inhibitors showed a much better disease course compared with those on the other medications used as controls (12).
Lima et al. described that patients who have significant comorbidities have a decreased likelihood of being put on systemic therapy by their dermatologist, mainly due to the complications associated with biologic therapies. However, even when data are readjusted to overcome the variability, they found that patients with psoriasis on biologics were not at increased risk of severe SARS-CoV-2 infection (13).
Contradictorily, Baloghová et al. found that there was no relation between the incidence of SARS-CoV-2 and presence of comorbidities and the use of biologic therapy. The course of infection in most patients in their cohort was mild (2). Damiani et al. described that, within their cohort of patients with plaque psoriasis, the patients on biologic therapy had a higher risk of being infected and hospitalized. The risk of severe infection and death, however, was lower in this cohort (40). Mahil et al. also stated an insight regarding the correlation between biologics and lower rates of hospitalization that it may be due to selection bias; patients with multiple comorbidities are more likely to be put on non-specific therapy and only given biologic therapy in moderate-to-severe cases of psoriasis as well as the fact that patient on biologics being more prone to risk-mitigating behaviors, knowing that they have increased risk of infection due to the therapies (14).
3.2 Efficacy and safety of the BNT162b2 vaccine in the population with psoriasis on biologic therapy
Zelini et al. studied the humoral and cellular response to the BNT162b2 vaccine in patients with psoriasis on biologic therapy and found that a significant proportion of patients on biologics presented with a weakened humoral immune response. On administration of the booster dose, the humoral immunity of both groups was restored to previous levels, but 30.8% of patients on biologic therapy were not able to mount an appropriate cellular response after three doses, against all controls (21).
Regarding solely biologic therapy, several studies were conducted on patients with inflammatory disease on biologic therapy. Al-Janabi et al. reported that, after the second dose, seroconversion rose from 82.4% to 97.0% in patients with inflammatory disease on biologic therapy (23). Sugihara et al. found that the total antibody titer (IgG and IgM) was much lower in the patients on biologic therapy compared with those on non-biologic therapy and healthy controls (108.2 U/mL vs. 927 U/mL and 742.6 U/mL, respectively) (33).
However, several studies were also conducted analyzing the efficacy of the BNT162b2 vaccine in patients with psoriasis on biologic therapy. Most studies found that seroconversion was similar to that of the general population, with lower overall titers. Marovt et al. reported that, within their study, patients with psoriasis on biologics had 100% seroconversion rate. However, the titer levels were significantly lower compared with those in controls (30). Pavlotsky et al. discovered a 96% seroconversion rate [with Immunoglobulin G (IgG) titer levels similar to the controls] in the patients taking Interleukin (IL)-17 or -23 inhibitors and slightly higher than the titers of the patients on the other biologics studied (32). Cristaudo et al. described lower antibody titers in the population with psoriasis and that patients on monotherapy with biologic drugs showed higher IgG response rates than those on combination therapy (25). Lodde et al. found that, in their cohort, 97.0% of patients seroconverted. Two patients did not seroconvert; both patients were on infliximab, one on monotherapy and the other in conjunction with methotrexate (28).
Mahil et al. stated that all patients seroconverted after the second dose, and the IgG titers of patients on biologic therapy (mean titer: 1,816 U/mL) were not significantly different at the end of the second dose, relative to controls (mean titer: 2,749 U/mL). Responses against the alpha and delta variants in the patients on biologics were 97% and 36%, respectively, similar to the controls. Furthermore, after the second dose, only 71% of the patients on biologics showed a detectable T-cell response, which was significantly lower than the controls (100%) (29).
Megna et al. found no significant difference of effective antibody response between the control group and the psoriatic group; they also described the same trend in the antibody titer but a slightly higher average in the control group (41). Graceffa et al. also described that there was no significant difference in the humoral response to the BNT162b2 booster dose in patients with psoriasis compared with their control of healthy subjects, despite a decline in antibody titer 5 months after the second dose. Antibody titers 4 weeks after the booster dose were found to be 10-fold of those after the second dose. Patients on monotherapy had better humoral responses than those on combination therapy with methotrexate, but those patients still gave an effective response regardless. Conversely to other papers, they found no difference in response when comparing patients on TNFα inhibitors and anti–IL-17 monotherapies (26).
Venerito et al. conducted a study specifically to address the relation between immune response of the BNT162b2 vaccine and the use of TNFα inhibitors for psoriatic arthritis. The authors found no significant difference in immune response in these patients, with all patients presenting with a positive immune response (34). In a follow-up study studying the immunogenicity of the booster dose, given 4 months after the second dose, there was a higher decrease of IgG in patients with psoriasis compared with that in the control patients (85.2%, vs. 67.1%). It should be noted that, after the booster dose, the IgG titers returned to levels similar to those after the second dose, with patients with psoriasis having slightly lower levels, just as before (35).
Both cellular and humoral immunity against the vaccine were studied by Kvist-Hansen et al. The authors found that both types of immunity waned slowly within the 6 months in both the control and the patients on biologics, with most patients on biologic therapy having a positive humoral response (95%). The patients on TNFα inhibitors had the lowest humoral response with only 75.8%, whereas the anti–IL-17 group performed the best with a 100% response rate (27). Cellular responses were low in all patients on biologic therapy, especially in the TNFα inhibitor group, where only 44% responded cellularly. Overall, there was no correlation in humoral and cellular immunity in patients on biologics, with a positive correlation seen in the control group. The patients on TNFα inhibitors were found to have a bigger decrease of humoral and cellular immunity compared with the patients on other forms of biologics (with the patients on anti–IL-17 performing the best) (27).
The disproportion of the cellular and humoral response was studied by Hamm et al. and Cassaniti et al., who described the humoral and cellular responses in patients on immunosuppression after organ transplants; in both studies, the humoral and cellular responses are correlated in their decrease (42–44), signifying that the presence of the inflammatory disease may be an explanation for the findings with a lack of correlation between the two responses in their cohort of patients.
To date, no data on the efficacy of the fourth dose in patients with psoriasis on biologics are available in the literature. However, Aikawa et al. outlined the effect of the fourth dose of the BNT162b2 vaccine in patients with autoimmune rheumatic diseases on biologic therapy, 95.1% of patients showed an effective immune response, compared with 66.4% showing an effective immune response after three doses (22). Another study by Bieber et al. reported that the rates of infection, hospitalization, and death were lowest in their cohort of patients with autoimmune rheumatic disease who received the fourth dose, compared with those in the previous results after three doses (24).
4 Discussion
4.1 Course and severity of SARS-CoV-2 in patients with psoriasis on biologics
It can be suggested that the presence of psoriasis itself in patients is not correlated to an increase in the infection rate, hospitalization rate, or severity of disease due to SARS-CoV-2. The presence of heart disease, hypertension, and diabetes was studied extensively as there was a strong positive correlation to a worse prognosis of SARS-CoV-2 infection when comorbidities were present (39). However, with increased incidence of comorbidities within this population, there may be an increased risk of severe SARS-CoV-2 infection possibly requiring hospitalization (39, 45).
Regarding the relationship between biologic therapy and COVID-19 infection, it can be safely assumed that treatment of psoriasis using biologic drugs is not correlated with increased rates of infection. The National Psoriasis Foundation, in their guidelines concerning the COVID-19 pandemic and treatment of psoriasis, which was based on early studies and evidence during the pandemic, advises physicians to continue biologic therapy in patients with psoriasis, regardless of status of SARS-CoV-2 infection (45).
Along with the evidence of lower rates of hospitalizations, death rarely occurred within the population with psoriasis on biologics. The hidden advantages on the inhibition of certain cytokines within these biologic drugs may interfere with the pathogenic mechanism of SARS-CoV-2, allowing for a more favorable course of disease, as the cytokine storms that can be caused by the virion are prevented (46). In addition, IL-17 and TNFα inhibition have been hypothesized to be protective by preventing inappropriate inflammation due to cytokine storms (41, 46, 47). TNFα directly deteriorates the respiratory epithelium by producing inflammatory cytokines such as Granulocyte-Macrophage Colony Stimulating Factor (GM-CSF), IL-8, and intercellular adhesion molecules; worsening the course of the disease; and blocking TNF that has been shown to cause a rapid decline in the level of IL-6 and IL-1 in individuals with active inflammation (46, 48).
However, when prescribing anti-TNFα drugs, we should consider the presence of other immunosuppressive or corticosteroid drugs, the duration of treatments, and disease and comorbidities. All these factors are associated with elevated risk of infections (49, 50). Therefore, we should proceed with caution when evaluating risk and benefit of biologic therapy regarding SARS-CoV-2.
4.2 Efficacy and safety of the BNT162b2 vaccine in patients with psoriasis on biologics
From the data available, evidence shows that the seroconversion rate is not significantly lower in patients with psoriasis on biologic therapy after the BNT162b2 vaccine, compared with that in healthy individuals, suggesting that patients with psoriasis should be vaccinated regardless of treatment regime or status of disease. Among all studies reviewed, the totality of patients with psoriasis on biologic therapy seroconverted within three doses of BNT162b2, even if the response was negative following the first two doses. On the other hand, the cellular response to the vaccine was weaker compared with the humoral response, with a large number of patients not being able to mount an appropriate cellular response within three doses of the BNT162b2 vaccine. The presence of effective, albeit weaker, responses to the vaccine may prove that patients with psoriasis on biologic therapy may benefit from a tighter vaccination schedule and the booster dose.
Regarding the fourth BNT162b2 dose in these patients, evidence still remains inconclusive. The use of a fourth dose in patients who are non-responders may potentially allow for the activation of an immune response, even if activation was not achieved from the three previous doses (24, 51). A fourth dose may allow for a prolonged immune response in those that responded well to previous doses but had decreased time of effectiveness (52).
5 Conclusion
It is clear that patients on biologic therapy have to be treated in a more personalized way, despite having an infection rate comparable with the general population. There are increased rates of comorbidities in these patients due to the multiple inflammatory mechanisms associated with psoriasis (53, 54).
The increased rates of comorbidities put these patients at an elevated risk of severe infection leading to hospitalization (14, 39, 55). It can be argued that this makes the patient frail; despite not being more vulnerable to SARS-CoV-2 infection than the general population, they have a higher risk of severe disease (54).
However, the use of biologic therapy has been suggested to have protective mechanisms, inhibiting pathologic cytokine pathways associated with the cytokine storm that occurs due to SARS-CoV-2. The inhibition of cytokines such as TNFα and IL-17, in particular, has been shown to reduce the levels of other cytokines and to reduce the active SARS-CoV-2 infection (46, 48, 56). This may play a role in the decreased rates of severe disease and hospitalizations due to SARS-CoV-2 infection in patients on biologic therapy. However, we must always approach these cases with caution as the use of biologic therapy may increase the risk of other opportunistic infections (57).
However, because of the smaller sample sizes and variations in treatment regimens within literature, it is difficult to provide a strong conclusion. There is still a need for ongoing studies that encompass the infection rates and immune responses in patients on biologic therapy during SARS-CoV-2 infection as well as follow-up studies on the maintenance of response post-vaccination and whether this has a real impact on the frequency of infections.
Author contributions
JR: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MV: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. EI: Conceptualization, Data curation, Investigation, Writing – review & editing. AB: Conceptualization, Data curation, Investigation, Writing – review & editing. SB: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. VB: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing, Formal Analysis, Supervision, Methodology.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by Fondi Ricerca Corrente, Ministero della Salute, Italy.
Acknowledgments
We thank the patients and the nurses of the Institute of Dermatology, Fondazione Policlinico San Matteo IRCCS Pavia Anna M. and Anna P. for their invaluable contribution to this study.
Conflict of interest
VB has been registered for congresses for Sanofi Genzyme, Novartis, Almirall and has participated in clinical trials for Leo Pharma.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Brazzelli V, Isoletta E, Barak O, Barruscotti S, Vassallo C, Giorgini C, et al. Does therapy with biological drugs influence COVID-19 infection? Observational monocentric prevalence study on the clinical and epidemiological data of psoriatic patients treated with biological drugs or with topical drugs alone. Dermatologic Ther (2020) 33:e14516. doi: 10.1111/dth.14516
2. Baloghová J, Kampe T, Kolarčik P, Hatalová E. Vaccination, risk factors and outcomes of COVID-19 infection in patients with psoriasis—A single centre real-life experience from eastern Slovakia. Viruses (2022) 14:1646. doi: 10.3390/v14081646
3. Campo-Slebi I, Meza-Corso MF, Cárdenas P, Castro-Ayarza JR, González C, Cortés C, et al. COVID-19 in patients with psoriasis: A Latin American case series. JAAD Int (2021) 5:96–7. doi: 10.1016/j.jdin.2021.09.001
4. Conti A, Lasagni C, Bigi L, Pellacani G. Evolution of COVID-19 infection in four psoriatic patients treated with biological drugs. J Eur Acad Dermatol Venereol (2020) 34:e360–1. doi: 10.1111/jdv.16587
5. Damiani G, Pacifico A, Bragazzi NL, Malagoli P. Biologics increase the risk of SARS-CoV-2 infection and hospitalization, but not ICU admission and death: Real-life data from a large cohort during red-zone declaration. Dermatol Ther (2020) 33:e13475. doi: 10.1111/dth.13475
6. Fougerousse A-C, Perrussel M, Bécherel P-A, Begon E, Pallure V, Zaraa I, et al. Systemic or biologic treatment in psoriasis patients does not increase the risk of a severe form of COVID-19. J Eur Acad Dermatol Venereol (2020) 34:e676–9. doi: 10.1111/jdv.16761
7. Fulgencio-Barbarin J, Puerta-Peña M, Ortiz-Romero P, García-Donoso C, Rivera-Diaz R. COVID-19 and systemic therapies in psoriasis: experience of a tertiary hospital in Madrid. Int J Dermatol (2020) 59:1425–6. doi: 10.1111/ijd.15157
8. Galluzzo M, Tofani L, Bianchi L, Talamonti M. Status of a real-life cohort of patients with moderate-to-severe plaque psoriasis treated with secukinumab and considerations on the use of biological agents in the Covid-19 era. Expert Opin Biol Ther (2020) 20:829–30. doi: 10.1080/14712598.2020.1779217
9. Gisondi P, Zaza G, Del Giglio M, Rossi M, Iacono V, Girolomoni G. Risk of hospitalization and death from COVID-19 infection in patients with chronic plaque psoriasis receiving a biologic treatment and renal transplant recipients in maintenance immunosuppressive treatment. J Am Acad Dermatol (2020) 83:285–7. doi: 10.1016/j.jaad.2020.04.085
10. Gisondi P, Facheris P, Dapavo P, Piaserico S, Conti A, Naldi L, et al. The impact of the COVID -19 pandemic on patients with chronic plaque psoriasis being treated with biological therapy: the Northern Italy experience. Br J Dermatol (2020) 183:373–4. doi: 10.1111/bjd.19158
11. Kartal SP, Çelik G, Yılmaz O, Öksüm Solak E, Demirbağ Gül B, Üstünbaş TK, et al. The impact of COVID-19 pandemic on psoriasis patients, and their immunosuppressive treatment: A cross-sectional multicenter study from Turkey. J Dermatol Treat (2022) 33:2137–44. doi: 10.1080/09546634.2021.1927947
12. Kridin K, Schonmann Y, Damiani G, Peretz A, Onn E, Bitan DT, et al. Tumor necrosis factor inhibitors are associated with a decreased risk of COVID-19-associated hospitalization in patients with psoriasis—A population-based cohort study. Dermatol Ther (2021) 34:e15003. doi: 10.1111/dth.15003
13. Lima XT, Cueva MA, Lopes EM, Alora MB. Severe COVID-19 outcomes in patients with psoriasis. J Eur Acad Dermatol Venereol (2020) 34:e776–8. doi: 10.1111/jdv.16867
14. Mahil SK, Dand N, Mason KJ, Yiu ZZN, Tsakok T, Meynell F, et al. Factors associated with adverse COVID-19 outcomes in patients with psoriasis—insights from a global registry–based study. J Allergy Clin Immunol (2021) 147:60–71. doi: 10.1016/j.jaci.2020.10.007
15. Pahalyants V, Murphy WS, Klebanov N, Lu C, Theodosakis N, Klevens RM, et al. Immunosuppressive biologics did not increase the risk of COVID-19 or subsequent mortality: A retrospective matched cohort study from Massachusetts. J Am Acad Dermatol (2022) 86:252–5. doi: 10.1016/j.jaad.2021.08.065
16. Piaserico S, Gisondi P, Cazzaniga S, Naldi L. Lack of evidence for an increased risk of severe COVID-19 in psoriasis patients on biologics: A cohort study from northeast Italy. Am J Clin Dermatol (2020) 21:749–51. doi: 10.1007/s40257-020-00552-w
17. Zitouni J, Bursztejn A -C, Belloni Fortina A, Beauchet A, Di Lernia V, Lesiak A, et al. Children with psoriasis and COVID-19: Factors associated with an unfavourable COVID-19 course, and the impact of infection on disease progression (Chi-PsoCov registry). Acad Dermatol Venereol (2022) 36:2076–86. doi: 10.1111/jdv.18361
18. Ahmed SMA, Volontè M, Isoletta E, Vassallo C, Tomasini CF, Lilleri D, et al. SARS-CoV-2 serology in patients on biological therapy or apremilast for psoriasis: A study of 93 patients in the Italian red zone. J Eur Acad Dermatol Venereol (2022) 36:e86–8. doi: 10.1111/jdv.17721
19. Barrutia L, Volo V, Ruíz-Sánchez D, Valtueña J, Aguado García A, ManChado López P. COVID-19 and biologic therapies in dermatology: Seroprevalence survey and severity analysis in a tertiary hospital in Spain. Int J Dermatol (2021) 60:624–5. doi: 10.1111/ijd.15467
20. Yendo TM, Sato MN, Branco ACCC, Pietrobon AJ, Teixeira FME, Ramos YÁL, et al. Impact of inflammatory immune dysfunction in psoriasis patients at risk for COVID-19. Vaccines (2021) 9:478. doi: 10.3390/vaccines9050478
21. Zelini P, Isoletta E, Volontè M, Lilleri D, Cassaniti I, Musella V, et al. Dynamics of humoral and cellular immunity elicited by the BNT162b2 mRNA vaccine in psoriatic patients under targeted immunosuppression: A longitudinal cohort study. J Eur Acad Dermatol Venereology (2023) 37:e294–6. doi: 10.1111/jdv.18787
22. Aikawa NE, Kupa LVK, Silva CA, Saad CGS, Pasoto SG, Yuki EFN, et al. Strong response after fourth dose of mRNA COVID-19 vaccine in autoimmune rheumatic diseases patients with poor response to inactivated vaccine. Rheumatology (2022) 62:480–5. doi: 10.1093/rheumatology/keac301
23. Al-Janabi A, Ra A, Littlewood Z, Foulkes AC, Hunter HJA, Chinoy H, et al. The effect of immunomodulators on seroconversion after BNT162b2 and AZD1222 vaccines in patients with immune-mediated inflammatory diseases: A prospective cohort study. Br J Dermatol (2023) 188:542–51. doi: 10.1093/bjd/ljac109
24. Bieber A, Brikman S, Novack L, Abuhasira R, Fawaz A, Abu-Shakra M, et al. Fourth dose of BNT162b2 vaccine for patients with autoimmune rheumatic diseases in a nationwide setting. Rheumatology (2023) 62(10):kead064. doi: 10.1093/rheumatology/kead064
25. Cristaudo A, Graceffa D, Pimpinelli F, Sperati F, Spoletini G, Bonifati C, et al. Immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologic drugs. J Eur Acad Dermatol Venereology (2022) 36:e266–8. doi: 10.1111/jdv.17861
26. Graceffa D, Sperati F, Bonifati C, Spoletini G, Lora V, Pimpinelli F, et al. Immunogenicity of three doses of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologics. Front Med (2022) 9:961904. doi: 10.3389/fmed.2022.961904
27. Kvist-Hansen A, Pérez-Alós L, Al-Sofi RF, Heftdal LD, Hamm SR, Møller DL, et al. Waning humoral and cellular immunity after COVID-19 vaccination in patients with psoriasis treated with methotrexate and biologics: A cohort study. Br J Dermatol (2023) 188:661–9. doi: 10.1093/bjd/ljad023
28. Lodde GC, Krefting F, Placke J-M, Schneider L, Fiedler M, Dittmer U, et al. COVID-19 vaccination in psoriasis patients receiving systemic treatment: A prospective single-center study. Front Immunol (2023) 14:1107438. doi: 10.3389/fimmu.2023.1107438
29. Mahil SK, Bechman K, Raharja A, Domingo-Vila C, Baudry D, Brown MA, et al. Humoral and cellular immunogenicity to a second dose of COVID-19 vaccine BNT162b2 in people receiving methotrexate or targeted immunosuppression: a longitudinal cohort study. Lancet Rheumatol (2022) 4:e42–52. doi: 10.1016/S2665-9913(21)00333-7
30. Marovt M, Deželak P, Ekart R, Marko PB. Immune response to SARS-CoV-2 mRNA vaccine in patients with psoriasis treated with biologics. Clin Exp Dermatol (2022) 47:2041–3. doi: 10.1111/ced.15347
31. Megna M, Potestio L, Battista T, Camela E, Genco L, Noto M, et al. Immune response to COVID-19 mRNA vaccination in patients with psoriasis undergoing treatment with biologics. Clin Exp Dermatol (2022) 47:2310–2. doi: 10.1111/ced.15395
32. Pavlotsky F, Segal Z, Barzilai A. Antibody response to BNT162b2 vaccine in immune modifiers–treated psoriatic patients. J Psoriasis Psoriatic Arthritis (2022) 7:24–8. doi: 10.1177/24755303211056059
33. Sugihara K, Wakiya R, Shimada H, Kameda T, Nakashima S, Kato M, et al. Immunogenicity against the BNT162b2 mRNA COVID-19 Vaccine in Rheumatic Disease Patients Receiving Immunosuppressive Therapy. Intern Med (2022) 61:1953–8. doi: 10.2169/internalmedicine.9223-21
34. Venerito V, Stefanizzi P, Fornaro M, Cacciapaglia F, Tafuri S, Perniola S, et al. Immunogenicity of BNT162b2 mRNA SARS-CoV-2 vaccine in patients with psoriatic arthritis on TNF inhibitors. RMD Open (2022) 8:e001847. doi: 10.1136/rmdopen-2021-001847
35. Venerito V, Stefanizzi P, Martinelli A, Fornaro M, Galeone MG, Tafuri S, et al. Anti-SARS-CoV-2 antibody decay after vaccination and immunogenicity of the booster dose of the BNT162b2 mRNA vaccine in patients with psoriatic arthritis on TNF inhibitors. Clin Exp Rheumatol (2023) 41:166–9. doi: 10.55563/clinexprheumatol/hptln9
36. Morley JE, Vellas B, van Kan GA. Frailty consensus: a call to action. J Am Med Dir Assoc (2013) 14:392–7. doi: 10.1016/j.jamda.2013.03.022
37. Kiely DK, Cupples LA, Lipsitz LA. Validation and comparison of two frailty indexes: The MOBILIZE Boston Study. J Am Geriatr Soc (2009) 57(9):1532–9. doi: 10.1111/j.1532-5415.2009.02394.x
38. Franco Salinas G, De Rycke L, Barendregt B, Paramarta JE, Hreggvidstdottir H, Cantaert T, et al. Anti-TNF treatment blocks the induction of T cell-dependent humoral responses. Ann Rheum Dis (2013) 72:1037–43. doi: 10.1136/annrheumdis-2011-201270
39. Chatterjee S, Nalla LV, Sharma M, Sharma N, Singh AA, Malim FM, et al. Association of COVID-19 with comorbidities: An update. ACS Pharmacol Transl Sci (2023) 6:334–54. doi: 10.1021/acsptsci.2c00181
40. Damiani G, Allocco F, Young Dermatologists Italian Network, Malagoli P. COVID-19 vaccination and patients with psoriasis under biologics: Real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol (2021) 46:1106–8. doi: 10.1111/ced.14631
41. Megna M, Napolitano M, Fabbrocini G. May IL-17 have a role in COVID-19 infection? Med Hypotheses (2020) 140:109749. doi: 10.1016/j.mehy.2020.109749
42. Cassaniti I, Gregorini M, Bergami F, Arena F, Sammartino JC, Percivalle E, et al. Effect of a third dose of SARS-CoV-2 mRNA BNT162b2 vaccine on humoral and cellular responses and serum anti-HLA antibodies in kidney transplant recipients. Vaccines (2022) 10:921. doi: 10.3390/vaccines10060921
43. Cassaniti I, Bergami F, Arena F, Sammartino JC, Ferrari A, Zavaglio F, et al. Immune response to BNT162b2 in solid organ transplant recipients: Negative impact of mycophenolate and high responsiveness of SARS-CoV-2 recovered subjects against delta variant. Microorganisms (2021) 9:2622. doi: 10.3390/microorganisms9122622
44. Hamm SR, Møller DL, Pérez-Alós L, Hansen CB, Pries-Heje MM, Heftdal LD, et al. Decline in antibody concentration 6 months after two doses of SARS-CoV-2 BNT162b2 vaccine in solid organ transplant recipients and healthy controls. Front Immunol (2022) 13:832501. doi: 10.3389/fimmu.2022.832501
45. Gelfand JM, Armstrong AW, Bell S, Anesi GL, Blauvelt A, Calabrese C, et al. National Psoriasis Foundation COVID-19 Task Force guidance for management of psoriatic disease during the pandemic: Version 2—Advances in psoriatic disease management, COVID-19 vaccines, and COVID-19 treatments. J Am Acad Dermatol (2021) 84:1254–68. doi: 10.1016/j.jaad.2020.12.058
46. Montazersaheb S, Hosseiniyan Khatibi SM, Hejazi MS, Tarhriz V, Farjami A, Ghasemian Sorbeni F, et al. COVID-19 infection: an overview on cytokine storm and related interventions. Virol J (2022) 19:92. doi: 10.1186/s12985-022-01814-1
47. Leija-Martínez JJ, Huang F, Del-Río-Navarro BE, Sanchéz-Muñoz F, Muñoz-Hernández O, Giacoman-Martínez A, et al. IL-17A and TNF-α as potential biomarkers for acute respiratory distress syndrome and mortality in patients with obesity and COVID-19. Med Hypotheses (2020) 144:109935. doi: 10.1016/j.mehy.2020.109935
48. Costela-Ruiz VJ, Illescas-Montes R, Puerta-Puerta JM, Ruiz C, Melguizo-Rodríguez L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev (2020) 54:62–75. doi: 10.1016/j.cytogfr.2020.06.001
49. Fernández-Ruiz M, Aguado JM. Risk of infection associated with anti-TNF-α therapy. Expert Rev Anti-infective Ther (2018) 16:939–56. doi: 10.1080/14787210.2018.1544490
50. Murdaca G, Spanò F, Contatore M, Guastalla A, Penza E, Magnani O, et al. Infection risk associated with anti-TNF-α agents: a review. Expert Opin Drug Saf (2015) 14:571–82. doi: 10.1517/14740338.2015.1009036
51. Caillard S, Thaunat O, Benotmane I, Masset C, Blancho G. Antibody response to a fourth messenger RNA COVID-19 vaccine dose in kidney transplant recipients: A case series. Ann Intern Med (2022) 175(3): L21–0598. doi: 10.7326/L21-0598
52. Cheung MW, Dayam RM, Shapiro JR, Law JC, Chao GYC, Pereira D, et al. Third and fourth vaccine doses broaden and prolong immunity to SARS-coV-2 in adult patients with immune-mediated inflammatory diseases. J Immunol (2023) 211:351–64. doi: 10.4049/jimmunol.2300190
53. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The “psoriatic march”: a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol (2011) 20(4):303–7. doi: 10.1111/j.1600-0625.2011.01261.x
55. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int J Infect Dis (2020) 94:91–5. doi: 10.1016/j.ijid.2020.03.017
56. Zeng H, Wang S, Chen L, Shen Z. Biologics for psoriasis during the COVID-19 pandemic. Front Med (2021) 8:759568. doi: 10.3389/fmed.2021.759568
Keywords: psoriasis, frailty, biologic therapy, SARS-CoV-2, BNT162b2 vaccine, targeted immunosuppression
Citation: Railton J, Volonté M, Isoletta E, Bonelli A, Barruscotti S and Brazzelli V (2024) Psoriasis and biological drugs at the time of SARS-CoV-2 infection: a mini review outlining risk of infection, seroprevalence, and safety and efficacy of the BNT162b2 vaccine. Front. Immunol. 15:1354729. doi: 10.3389/fimmu.2024.1354729
Received: 14 December 2023; Accepted: 09 January 2024;
Published: 30 January 2024.
Edited by:
Denis Comte, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandReviewed by:
Joan Calvet, Hospital de Sabadell, SpainCopyright © 2024 Railton, Volonté, Isoletta, Bonelli, Barruscotti and Brazzelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valeria Brazzelli, dmJyYXp6ZWxsaUBsaWJlcm8uaXQ=; di5icmF6emVsbGlAc21hdHRlby5wdi5pdA==
†ORCID: Valeria Brazzelli, orcid.org/0000-0001-5898-6448Janosch Railton, orcid.org/0009-0004-0595-3561Martina Volonté, orcid.org/0009-0006-2688-9065Eugenio Isoletta, orcid.org/0000-0003-3398-1354Stefania Barruscotti, orcid.org/0000-0002-9572-4575