
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 01 February 2024
Sec. Viral Immunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1343124
This article is part of the Research Topic Challenges of Non-AIDS-Defining Diseases in People Living with HIV View all 7 articles
 Raquel Ron1,2,3*
Raquel Ron1,2,3* Javier Martínez-Sanz1,3
Javier Martínez-Sanz1,3 Sabina Herrera4
Sabina Herrera4 Luis Ramos-Ruperto5
Luis Ramos-Ruperto5 Alejandro Díez-Vidal5
Alejandro Díez-Vidal5 Talía Sainz6Noelia Álvarez-Díaz7Andrea Correa-Pérez8,9,10
Talía Sainz6Noelia Álvarez-Díaz7Andrea Correa-Pérez8,9,10 Alfonso Muriel2,10Jesús López-Alcalde8,10,11José A. Pérez-Molina1,2,3
Alfonso Muriel2,10Jesús López-Alcalde8,10,11José A. Pérez-Molina1,2,3 Santiago Moreno1,2,3
Santiago Moreno1,2,3 Sergio Serrano-Villar1,2,3
Sergio Serrano-Villar1,2,3Background: In people living with HIV (PLHIV), the CD4/CD8 ratio has been proposed as a useful marker for non-AIDS events. However, its predictive ability on mortality over CD4 counts, and the role of CD8+ T-cell counts remain controversial.
Methods: We conducted a systematic review and meta-analysis of published studies from 1996 to 2023, including PLHIV on antiretroviral treatment, and reporting CD4/CD8 ratio or CD8+ counts. The primary outcome was non-AIDS mortality or all-cause mortality. We performed a standard random-effects pairwise meta-analysis comparing low versus high CD4/CD8 ratio with a predefined cut-off point of 0.5. (CRD42020170931).
Findings: We identified 2,479 studies for screening. 20 studies were included in the systematic review. Seven studies found an association between low CD4/CD8 ratio categories and increased mortality risk, with variable cut-off points between 0.4-1. Four studies were selected for meta-analysis, including 12,893 participants and 618 reported deaths. Patients with values of CD4/CD8 ratio below 0.5 showed a higher mortality risk (OR 3.65; 95% CI 3.04 - 4.35; I2 = 0.00%) compared to those with higher values. While the meta-analysis of CD8+ T-cell counts was not feasible due to methodological differences between studies, the systematic review suggests a negative prognostic impact of higher values (>1,138 to 1,500 cells/uL) in the long term.
Conclusions: Our results support the use of the CD4/CD8 ratio as a prognostic marker in clinical practice, especially in patients with values below 0.5, but consensus criteria on ratio timing measurement, cut-off values, and time to event are needed in future studies to get more robust conclusions.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020170931, identifier CRD42020170931.
The optimization of antiretroviral treatment (ART) has facilitated a marked increase in life expectancy for individuals living with HIV (PLHIV) (1, 2). However, this enhancement in survival has also led to an upsurge in the prevalence of comorbidities and non-AIDS-related diseases (3–5). Despite the high rates of virological suppression obtained with current drugs, a percentage of patients do not achieve complete immune restoration. This is represented by the persistence of a decreased CD4/CD8 ratio, partially attributable to a high CD8+ T-cell count (6–8). PLHIV with a low CD4/CD8 ratio demonstrates heightened inflammation and immunosenescence, even under successful ART and adequate CD4+ count recovery (>500 cells/μL) (7, 9), and chronic HIV infection is characterized by an increase in CD8+ T-cell count along with functionality changes (10).
Therefore, the CD4/CD8 ratio has evolved as a valuable proxy for immune dysfunction among PLHIV. Its ease of monitoring in standard clinical settings, along with its correlation to markers of immunosenescence and inflammation enhances its utility at an individual level (5, 6, 11). In PLHIV on ART, the ratio correlates with a spectrum of comorbidities, such as cerebrovascular disease (12), chronic obstructive pulmonary disease (13), chronic kidney disease (14), and non-AIDS related cancers (15–17), thereby highlighting its role as a predictive marker for severe non-AIDS events (SNAEs) such as non-AIDS related mortality. However, the relevance of the CD4/CD8 ratio over isolated CD4+ or CD8+ count and its potential use as a predictor of mortality remains unclear. While some studies have reported a higher risk of non-AIDS events and mortality in patients with a CD4/CD8 ratio <0.4 (18, 19), others did not confirm this association (20, 21). In older subjects, the persistence of high levels of CD8+ lymphocyte activation after one year of virological suppression is associated with an increased risk of AIDS and non-AIDS events, and chronic CD8+ proliferation has been signified as a risk factor for non-Hodgkin’s lymphoma, acute myocardial infarction, and functional impairment (22, 23).
Determining the role of CD4/CD8 ratio or CD8+ count as new prognostic markers would help identify those patients at high risk for morbidity and mortality. This information could be used to classify patients at risk for persistent inflammation and age-related conditions, helping us to intensify health interventions and prevention. This systematic review and meta-analysis aimed to evaluate the independent role of the CD4/CD8 ratio and CD8+ T-cell count as predictors of non-AIDS-related mortality in PLHIV on ART.
We performed a systematic literature review and meta-analysis and followed the PRISMA statement to report our findings (24). The study protocol was prospectively registered in PROSPERO (CRD42020170931).
Studies were eligible if they included PLHIV ≥18 years starting or on current ART with undetectable viral load, as defined by the viral load threshold determined by the primary studies. The studies should evaluate the role of CD4/CD8 ratio or CD8+ T cell count as independent prognostic factors after adjustment for key covariates. We considered age, sex, risk factors for HIV transmission, CD4 nadir, Hepatitis C virus (HCV) or Cytomegalovirus (CMV) coinfection, and type of ART as principal covariates. The adjustment for these covariates was not an inclusion criterion but was considered in the risk of bias assessment. The primary outcome was non-AIDS mortality or all-cause mortality at the longest follow-up as provided by primary studies. We set viral suppression as an inclusion criterion to reduce AIDS-related mortality. The secondary composite outcome was non-AIDS events or death, including any definition of non-AIDS events considered by authors if mortality was reported. We included experimental or observational studies, always that had provided adjusted estimates for at least one review outcome. Studies with elite controllers were excluded. A detailed description of the inclusion criteria is included in the supplemental material (Supplementary 1).
We conducted a systematic search of the literature from January 1996 to January 2023, without language restriction, in Medline (Ovid), Embase (Elsevier), Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science databases. This period was established to avoid publications before the implementation of highly active antiretroviral therapy. We used controlled vocabulary (such as MeSH terms) and keywords related to the topics “HIV”, “ CD4/CD8 ratio or CD8” and “mortality/death”. The search strategy is described in Supplementary 1.
We used Covidence tool (25), for implementing the study selection process. Every study was independently screened by two reviewers at title/abstract and full-text stages. In case of discrepancy, the final decision was solved by a third one. We extracted the data from each included study with a predesigned Microsoft Excel form based on the CHARMS-PF checklist (26), and we piloted the form in three studies for usability. We classified the studies by CD4/CD8 ratio measurement as a categorical or continuous variable. We reached out to several corresponding authors to acquire additional data needed to reconcile differences and establish reference values. We assessed the risk of bias in the included studies with the QUIPS tool, which is designed for prognostic factor studies (26). The tool domains are described in Supplementary 2. Two authors assessed the risk of bias in each included study independently. Discrepancies were resolved by discussion and mutual agreement. The quality of evidence was evaluated with GRADE framework, adapted to prognostic studies as previously reported in the literature (27). The items to consider were related to the phase of investigation: with a high level of evidence assigned to cohort studies; study limitations and bias; inconsistency of results: related to the heterogeneity of findings; indirectness: assessing optimal population, prognostic factors and outcomes, and imprecision: to determine the certainty and interpretation of the results.
We conducted a meta-analysis to assess the risk of “non-AIDS mortality” and “all-cause mortality” in patients with low versus high CD4/CD8 ratios, using the high ratio as the reference category. A secondary analysis extended this to composite outcomes, including “AIDS, non-AIDS events, and all-cause mortality.” Due to the lack of studies reporting the CD4/CD8 ratio as a continuous variable, and the high heterogeneity in ratio measurement, we limited the statistical analysis to studies reporting the ratio as a categorical variable. Due to varying CD4/CD8 ratio cut-offs across studies (ranging from 0.3 to 1), we standardized our approach for better comparability. We focused on studies using clinically relevant cut-offs below 0.5, as supported by prior research linking low ratios to immunosenescence and increased morbidity and mortality (9, 12, 15, 16, 18). For instance, in studies with a 0.3 cut-off, subjects with ratios below 0.3 were categorized as “low ratio,” and those with ratios of 0.3 or higher as “high ratio”. For CD8+ T-cell counts, the cut-offs used across the selected studies were too variable to meta-analyse these results. A detailed description of the data adjustment to these cut-offs is included in Supplementary 3. Six studies (28–33) were excluded from the meta-analysis due to deviations from our study protocol but were accounted for in the systematic review based on follow-up after ART initiation and reported outcomes. Reasons for exclusion are reported in Supplementary 4.
We computed the effect measures, including Odds Ratio and Hazard Ratios, and their standard errors using each subgroup’s data, and performed a standard random-effects pairwise meta-analysis model to provide a pooled prognostic effect estimate for the primary and secondary outcomes. The conversion of the association measures into OR was discarded given the variability obtained in the results and the risk of bias. Heterogeneity was assessed with the I2 statistic and prediction intervals (34). The protocol also included publication bias assessment for each meta-analysis with 10 or more studies by funnel plot representation and Peter’s test (10% level), but due to the scarce number of studies included in the meta-analysis, this evaluation was not possible. All statistical analyses were performed using Stata (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC).
Table 1 summarizes the risk of bias in each study according to the QUIPS tool domains. A detailed description is presented in Supplementary 5. Items assessing study attrition showed the highest risk of bias. The overall risk of bias in the included studies was high (n=7; 35%) (28, 30, 31, 36, 37, 40, 43), moderate (n=11: 55%) (9, 18, 19, 21, 29, 32, 33, 35, 38, 39, 41), or low (n=2; 10%) (20, 42). Nearly all included studies (n=18; 90%) (9, 18, 19, 21, 28–33, 35–41, 43) lacked a description of the lost and censored participants, their characteristics, and the methodology for statistical imputation of the missing values. Time definition, including the timing of CD4/CD8 ratio measurement (n=7; 35%) (19, 28, 33, 36, 38, 39, 41), as well as the definition of the time to the event, were penalized in most of the studies (n=16; 80%) (9, 18, 19, 21, 28–33, 36, 37, 39, 41–43). Eight studies (40%) (19, 21, 28, 33, 36, 38, 39, 41) reported CD4/CD8 ratio measurement at the baseline evaluation of the cohorts, with subsequent updating of the data during follow-up, but without specifying the frequency of determination. Age and sex were considered in the adjusted analysis in more than half of the included studies (n=17; 85%) (9, 18, 20, 21, 29–33, 35–39, 41–43). The CD4 T-cell nadir or the baseline values reported in the cohorts were included as adjustment covariates in 8 studies (40%) (9, 18, 20, 21, 29, 39, 41, 42), and current or updated CD4 counts during follow-up were also considered as adjustment covariates by some authors (n=8; 40%) (20, 21, 29, 30, 32, 33, 39, 42). Nine studies (45%) (20, 21, 31–33, 35, 39, 41, 42) considered risk factors for HIV infection. Type of ART (n=5) (20, 29, 31, 35, 41), and HCV coinfection (n=5) (19, 28, 31, 33, 42) were each reported in 25% of the studies. For the studies included in the meta-analysis, again age, sex, and risk group were the most frequent adjustment variables, followed by nadir or baseline CD4 T-cell counts.
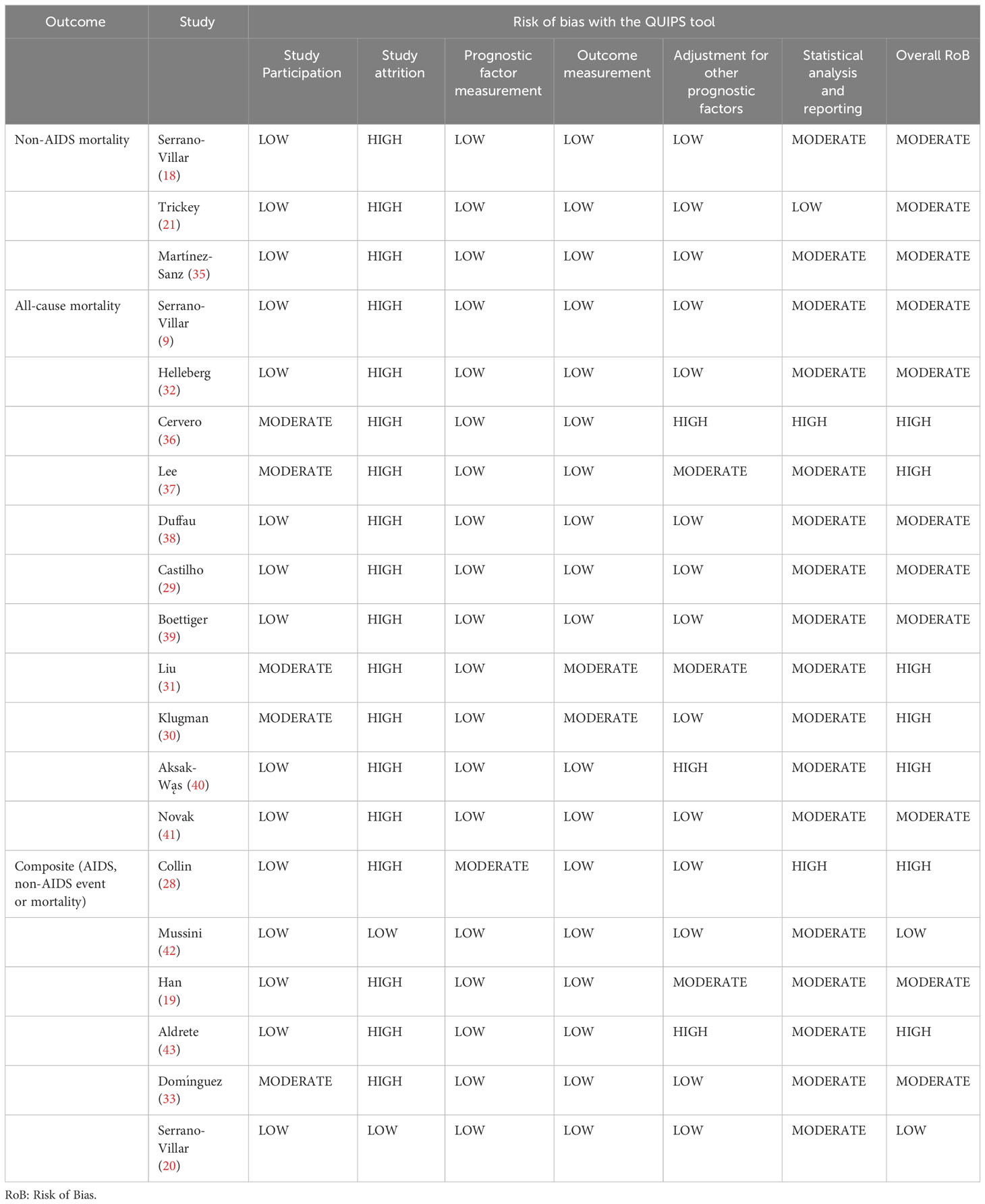
Table 1 Risk of bias assessment for primary studies.
Other relevant adjustment variables reported in the primary studies were the CDC/WHO classification or history of AIDS and the time since ART initiation. CMV infection was marginally recorded, being the least analyzed covariate. As six of the seven studies included in the meta-analysis were graded with a moderate overall risk of bias, we did not perform sensitivity analyses. The overall quality of evidence was moderate for the studies evaluating the CD4/CD8 ratio as a prognostic factor for non-AIDS mortality and all-cause mortality included in the meta-analysis. For the studies included in the systematic review assessing the role of the CD4/CD8 ratio or CD8+ T-cell counts as prognostic markers, the overall quality was low, mainly related to the risk of bias and the variability in results across studies. A detailed report of the adapted GRADE framework used is presented in Supplementary 6.
We screened 2,478 studies and identified 169 for eligibility. Studies selection flowchart is represented in Figure 1. After a full-text review, we included 20 studies in the systematic review. Most of the included studies (n=18) were hospital-based multicentric prospective cohorts, with two case-control studies (9, 18). The observed follow-up period ranged between 3 and 16 years, with a total number of 184,402 participants and 6,940 reported deaths (number of deaths not reported in all studies). The general characteristics of the primary studies are described in Table 2. The threshold defined for virological suppression went from 20 copies/mL to 1,000 copies/mL. Except for the study by Helleberg et al. (32), which reported only the CD8+ counts, all the selected studies measured CD4/CD8 ratio, with six studies reporting CD8+ T-cells as independent values. The main results are detailed in Table 3.
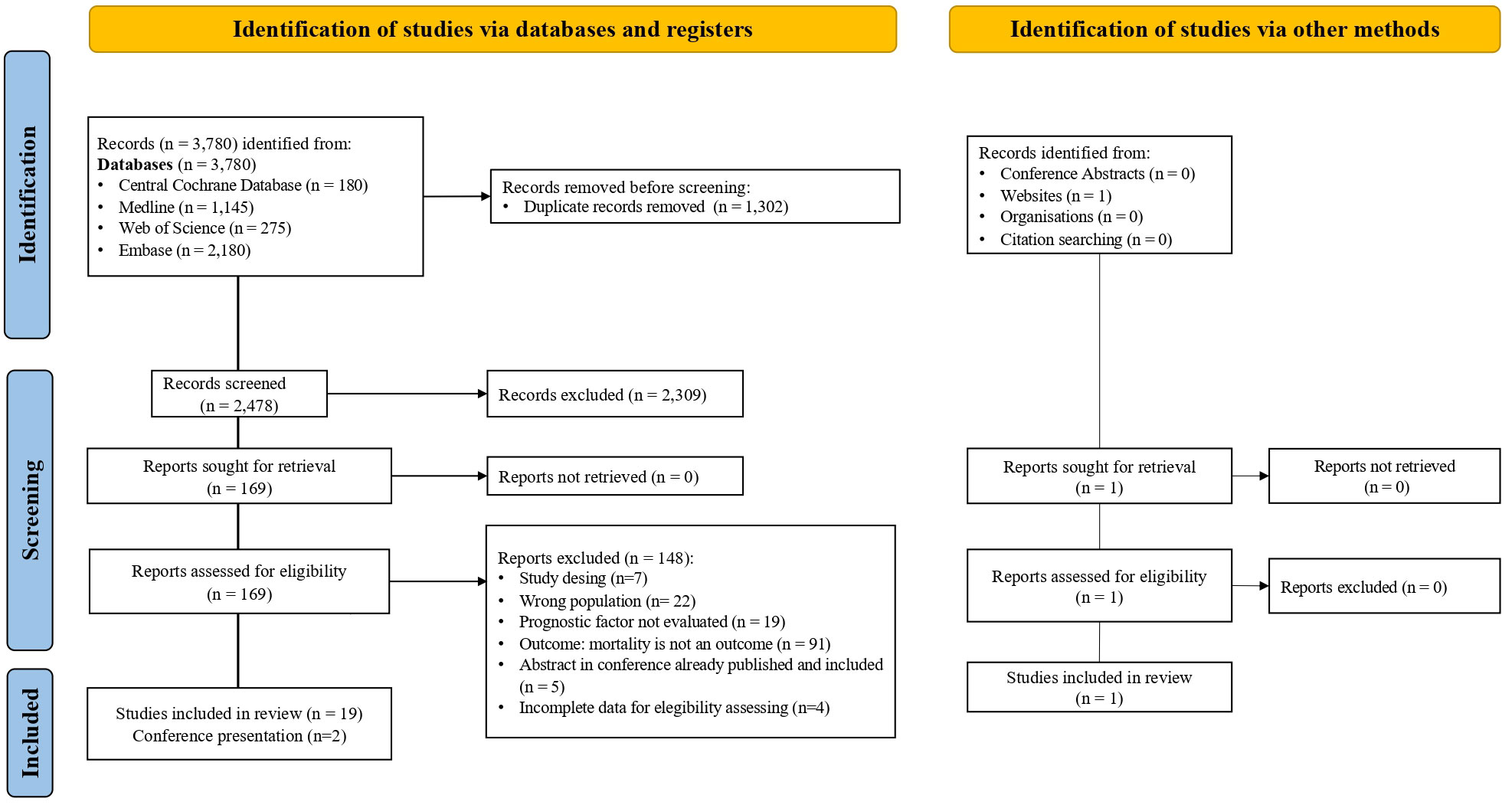
Figure 1 Studies selection flowcharts showing identification, screening, inclusion and exclusion process.
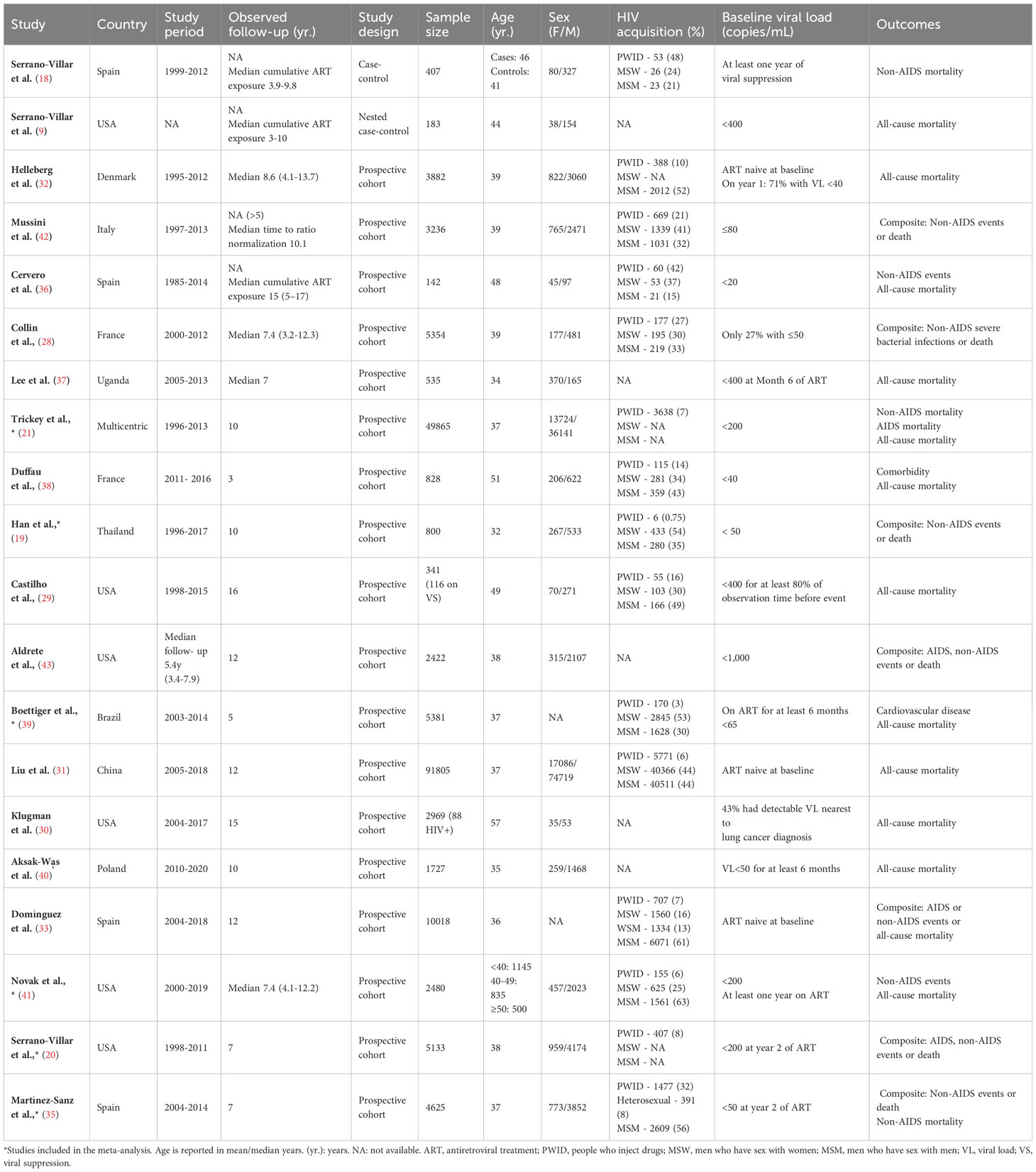
Table 2 Characteristics of the selected studies.
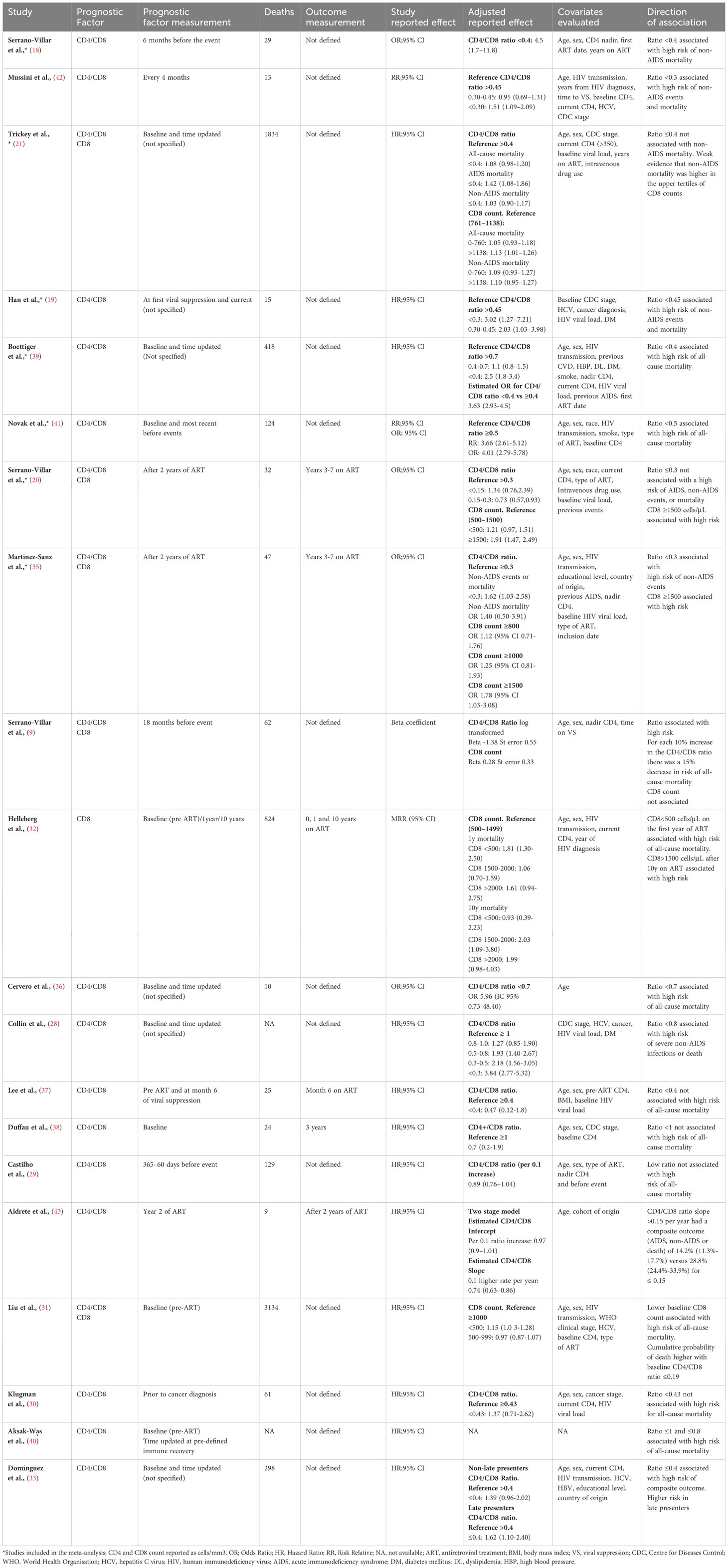
Table 3 Main results of selected studies.
Among twenty studies included in the systematic review, three (18, 21, 35) evaluated “non-AIDS mortality”, and twelve (9, 19, 21, 30–32, 36–41) reported “all-cause mortality” as independent outcomes, for a total follow-up between 3 and 16 years (Table 2). Seven of these studies (9, 18, 31, 36, 39–41) found an association between the lower CD4/CD8 ratio categories and increased mortality risk, with variable cut-off points reported, including 0.4, 0.5, 0.7, 0.8, and 1. Most of these studies reported the last ratio measurement before the development of the event or updated during follow-up. After considering the studies with our pre-specified cut-off values, the meta-analysis of non-AIDS or all-cause mortality (18, 35, 39, 41) showed an increased risk of mortality in subjects with a CD4/CD8 ratio below 0.5 (OR 3.64; 95% CI 3.04-4.35; 4 studies; n= 12,893; Follow-up: range 4.1 to 12.2 years; I2 = 0.00%; 95% Prediction interval: 2.46 to 5.38) compared to those above 0.5, with a reference threshold between 0.3 and 0.5 (Figure 2).
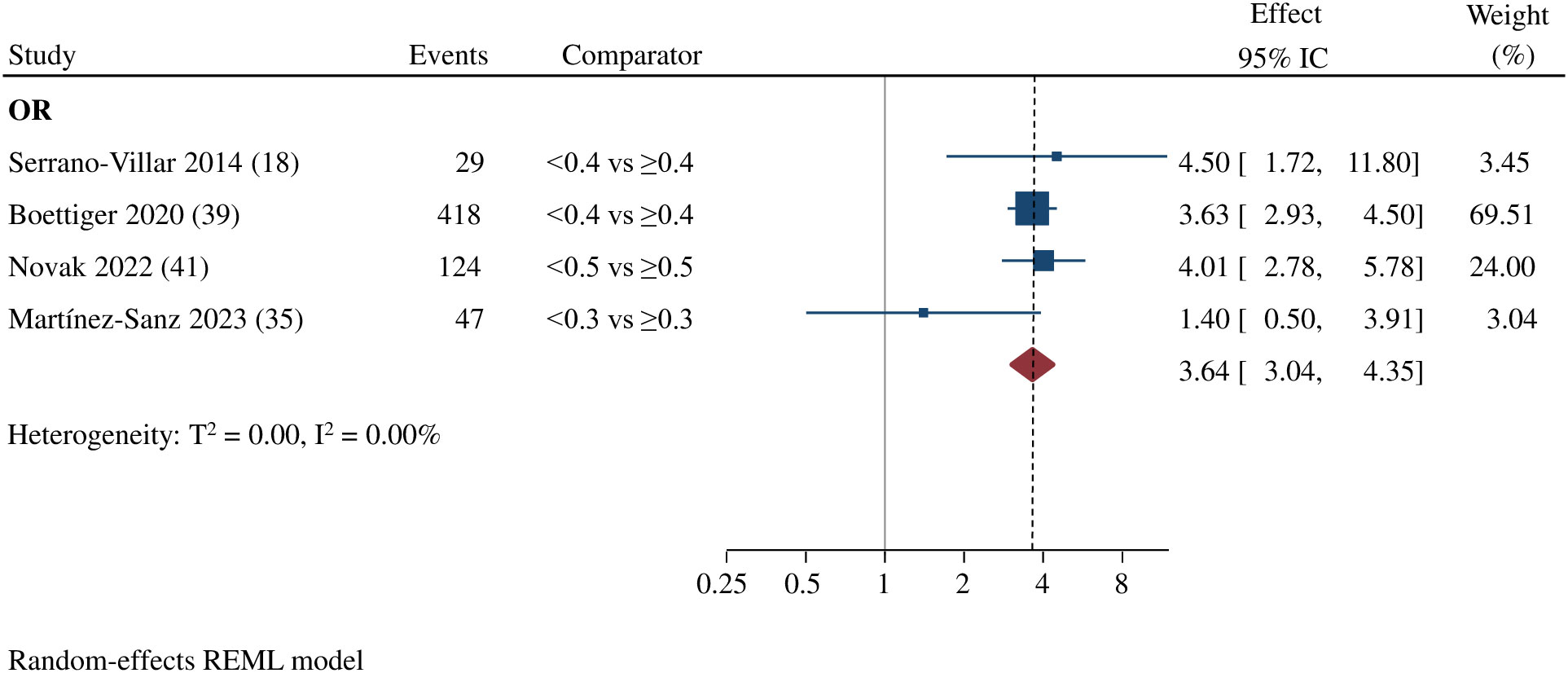
Figure 2 Estimated effect of CD4 /CD8 ratio on the risk on non-AIDS mortality or all-cause mortality. Random effect of meta-analysis comparing low vs. high CD4/CD8 ratios. (OR, Odds Ratio). Events include the total number of deaths reported.
Analysis of CD8+ T-cell count as an independent mortality predictor was not feasible, due to high variability in cut-off points, reference values, and timing of CD8+ measurement concerning ART initiation and the clinical event (Table 3). The systematic review suggests a double trend. First, lower baseline CD8+ levels appear to be associated with a higher risk of overall mortality. Two studies found an association with higher mortality risk in subjects with CD8+ count <500 cells/uL before ART initiation and in the first year of treatment (31, 32). Furthermore, four studies reported an increased risk of mortality or clinical events in virally suppressed patients with CD8+ counts in the higher categories (with cut-offs ranging from 1138 to 1,500 cells/uL) (20, 21, 32, 35), suggesting that the persistence of high CD8+ T-cell counts represent a negative prognostic factor in PLHIV on ART.
Seven studies looked at the risk for composite outcomes including AIDS, non-AIDS events, and mortality (19, 20, 28, 33, 35, 42, 43), with five authors finding an association with an increased risk of events for CD4/CD8 ratio values below 0.3 and 0.8 (19, 28, 33, 35, 42). Due to differences in effect measurement, statistical methodology, and baseline characteristics of the cohorts, it was not possible to conduct a meta-analysis to assess the risk of composite events independently. Therefore, primary studies with composite events were evaluated together with mortality outcomes in a second analysis. The meta-analysis including five studies reporting OR as the effect measure (18, 20, 35, 39, 41) showed an increased risk of AIDS, non-AIDS clinical events, or mortality in subjects with lower CD4/CD8 ratio categories (OR:2.49; 95% CI 1.39-4.45; 5 studies; n= 18,026 patients; Follow-up: 4.1-12.2 years; I2 = 89.06%; 95% Prediction interval: 0.30 to 20.94), compared to those with higher values, with cut-offs and reference thresholds ranging between 0.3 and 0.5. For two studies reporting HR (19, 21), we did not detect a significant effect of a CD4/CD8 ratio below 0.4 (HR 1.50, 95% CI 0.67-3.36; 2 studies; n= 50,665 patients; Follow-up: 10 years; I2 = 88.74%; 95% Prediction interval not calculable) compared to those with values above 0.45, with cut-offs and reference thresholds ranging between 0.4 and 0.45. (Figure 3). Statistical heterogeneity was high for both analyses.

Figure 3 Estimated effect of CD4/CD8 ratio on the risk of clinical events or mortality. Random effects meta-analysis by association measurement (HR, Hazard Ratio/OR, Odss Ratio) comparing low vs. high CD4/CD8 ratios. 1 composite including AIDS, non-AIDS events, and all-cause mortality. 2 composite outcomes including non-AIDS events and non-AIDS mortality.
Sixteen studies evaluated a spectrum of non-AIDS events (Supplementary 7). The most prevalent reported were cardiovascular and cerebrovascular disease (acute myocardial infarction, coronary heart disease, and stroke); chronic renal and liver disease; and non-AIDS-defining cancers. Four studies also considered AIDS events (20, 21, 33, 43), two of them as part of the composite outcome definition. All these analyses were performed or stratified by patients under ART-mediated viral suppression. In the study by Aldrete et al. (43), AIDS events accounted for 27.3%, determined by a poor CD4 or CD4/CD8 ratio recovery in the first years of ART. The study by Serrano-Villar et al. (20) reported a 7% of AIDS events.
This is, to our knowledge, the first systematic review evaluating the CD4/CD8 ratio as a predictor of mortality in PLHIV. Considering assessing the predictive value of the CD4/CD8 ratio, our primary focus was on mortality, a robust event for which most previous studies lacked sufficient statistical power to produce precise estimates. The findings from our study provide evidence to suggest that a low CD4/CD8 ratio, as defined by values below 0.3, 0.4, or 0.5 across different studies, serves as an adverse prognostic indicator for non-AIDS and all-cause mortality. Based on the evaluated evidence, PLHIV on ART who exhibit low CD4/CD8 ratios may face more than a threefold increase in mortality risk compared to those with higher ratios. When considering composite outcomes including comorbidities and mortality, we also found an association between lower CD4/CD8 ratios and high risk of AIDS, non-AIDS events, and all-cause mortality.
Persistent immune imbalance in PLHIV and its possible related outcomes have been evaluated by different authors. Recently data have confirmed an increased risk of different types of cancer, including AIDS and non-AIDS cancers in patients with lower ratios (0.30 vs. 0.80). These observations were made up to two years before diagnosis, suggesting the potential utility of the CD4/CD8 ratio as a clinical biomarker (44). Concerning cardiovascular disease, a low CD4/CD8 ratio has been associated with a higher prevalence of coronary atherosclerosis in young men living with HIV and virological suppression, in association with other classical cardiovascular risk factors (45). Previous studies have also unveiled a correlation between heightened CD8+ lymphocyte activation, persistently high CD8+ count, and an increased risk of both AIDS and non-AIDS events (22, 23, 46, 47). The study by Badejo et al. (48) explored the relationship between CD8+ counts and myocardial infarction risk. A higher risk of acute myocardial infarction (AMI) was observed in patients with CD4+ counts less than 200 and low CD8+ counts, while those with CD4+ counts over 200 cells/uL had a higher risk when CD8+ values were elevated. These findings align with results from several studies in our review. It suggests that imbalances in CD8+ levels may exert varying impacts, largely depending on the timing of the assessment. This differential effect is discernible both at baseline, characterized by lymphocyte loss and immunosuppression, and during chronic ART where excessive immune activation and persistently high counts are observed.
In this context, the definition of a cut-off point with the greatest predictive capacity is essential, to confirm a prognostic impact of the CD4/CD8 ratio or CD8+ count, homogenize conclusions of future studies, and facilitate the implementation of the ratio as a risk marker in clinical practice. Although a CD4/CD8 ratio <1 is considered indicative of immune dysfunction in the general population (49), initial studies in PLHIV on ART demonstrated the predictive capacity of lower cut-off points (0.3-0.4) (18, 42). Values close to this cut-off have proven useful in identifying patients with increased immune dysfunction despite a high CD4 count. In the most recent study included in our review (35), several cut-off points were specifically evaluated, and the value of 0.3 was found to discriminate the risk of non-AIDS events.
Given the methodological heterogeneity in the studies related to the impact of CD8+ count, they were unsuitable for inclusion in a meta-analysis. Regarding the most discriminative threshold for CD8+ count, three of the reviewed studies, reporting similar cut-off points and reference values showed that in people on ART, CD8+ counts >1,500 cells/uL, were associated with a significant increase in the risk of clinical events and mortality (32) (20) (35). Also, the study by Trickey et al. (21), including patients with ≥350 CD4, found a moderate risk of all-cause mortality among subjects with high CD8+ levels (>1,138 cell/uL). CD8+ count seems to be determinant both in the initial immune response to HIV infection as well as in the maintained immune activation during ART, but future studies are needed to explore the applicability of these cut-off values on specific clinical events.
Our study has several limitations. The main issue was the heterogeneity in CD4/CD8 ratio and CD8+ measurement between studies. The differences in the established cut-off points, its report as a continuous or categorical variable with varying intervals, and the variability of the reference values (ranging from ≥0.3 to ≥1 for the CD4/CD8 ratio) have been the main drawbacks, restricting the number of studies included in the meta-analysis. Another key factor is the timing of ratio measurement concerning ART initiation and the subsequent outcomes, with some studies clearly defining these times, while others employ a follow-up strategy with flexible time intervals. This is particularly important given the stability of the CD4/CD8 ratio as a parameter, especially for assessing non-AIDS events in patients already receiving treatment (50). Additionally, there was variation in the laboratory threshold for viral suppression, which we set as an inclusion criterion to minimize AIDS mortality. The evolution of ART regimens over time contributes to the heterogeneity, with potential implications for morbidity and mortality. Covariates, such as CMV seropositivity, HCV co-infection, and risk factors for comorbidities, were inconsistently recorded across the studies. The geographical location of the studies may affect the generalizability of our results, as most were conducted in Western European or North American countries, where treatment coverage and clinical care standards for HIV patients might differ significantly from other regions. Finally, the risk of bias assessment underscores the ongoing need for further research of higher methodological quality. This is particularly relevant concerning study attrition, an area that requires more comprehensive exploration to provide more accurate answers to our critical questions.
In conclusion, our systematic review and meta-analysis highlight the significant role of the CD4/CD8 ratio as a prognostic indicator for mortality and non-AIDS events in PLHIV on ART. However, to enhance the validity and applicability of these findings, future studies should pursue a more uniform design, with predefined, standardized measures and intervals for both the ratio and events, a clear definition of censoring timings, and a particular focus on non-AIDS events and mortality. Leveraging the CD4/CD8 ratio as a mortality biomarker presents an opportunity to define an “immunological threshold”, potentially enabling better patient stratification, surveillance, and more targeted preventive measures for those with lower values. This development could bring about direct improvements in routine clinical practice and serve as a starting line in the search for ratio recovery strategies and future research.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
RR: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JM-S: Data curation, Investigation, Writing – review & editing. SH: Data curation, Investigation, Writing – review & editing. LR-R: Data curation, Investigation, Writing – review & editing. AD: Data curation, Investigation, Writing – review & editing. TS: Data curation, Investigation, Writing – review & editing. NÁ-D: Data curation, Methodology, Writing – review & editing. AC-P: Data curation, Methodology, Writing – review & editing. AM: Data curation, Formal analysis, Methodology, Writing – review & editing. JL-A: Conceptualization, Methodology, Supervision, Writing – review & editing. JP-M: Methodology, Supervision, Writing – review & editing. SM: Supervision, Writing – review & editing. SS-V: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Carl Armon, Cerner Corporation, Kansas City, MO, USA; Sulggi Lee, University of California–San Francisco; Patrick W. G. Mallon and Padraig McGettrick, HIV Molecular Research Group, School of Medicine and Medical Science, University College Dublin, Ireland; Bogusz Jan Aksak-Wąs, Department of Infectious, Tropical Diseases and Immune Deficiency, Pomeranian Medical University in Szczecin, Szczecin, Poland; Adam Trickey, School of Social and Community Medicine, University of Bristol, United Kingdom. We want to thank all these authors for data sharing and collaboration. This work was supported by a European Society of PediatricInfectious Diseases (ESPID) Springboard Award.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1343124/full#supplementary-material
1. Antiretroviral Therapy Cohort Collaboration. Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet (2008) 372(9635):293–9. doi: 10.1016/S0140-6736(08)61113-7
2. May MT, Gompels M, Delpech V, Porter K, Orkin C, Kegg S, et al. Impact on life expectancy of HIV-1 positive individuals of CD4+ cell count and viral load response to antiretroviral therapy. AIDS (2014) 28(8):1193–202. doi: 10.1097QAD.0000000000000243
3. Serrão R, Piñero C, Velez J, Coutinho D, Maltez F, Lino S, et al. Non-AIDS-related comorbidities in people living with HIV-1 aged 50 years and older: The AGING POSITIVE study. Int J Infect Dis (2019) 79:94–100. doi: 10.1016/j.ijid.2018.10.011
4. Collins LF, Sheth AN, Mehta CC, Naggie S, Golub ET, Anastos K, et al. The prevalence and burden of non-AIDS comorbidities among women living with or at risk for human immunodeficiency virus infection in the United States. Clin Infect Dis (2021) 72(8):1301–11. doi: 10.1093/cid/ciaa204
5. Pelchen-Matthews A, Ryom L, Borges ÁH, Edwards S, Duvivier C, Stephan C, et al. Aging and the evolution of comorbidities among HIV-positive individuals in a European cohort. AIDS (2018) 32(16):2405–16. doi: 10.1097/QAD.0000000000001967
6. Caby F. CD4+/CD8 + ratio restoration in long-term treated HIV-1-infected individuals. AIDS (2017) 31(12):1685–95. doi: 10.1097/QAD.0000000000001533
7. Mutoh Y, Nishijima T, Inaba Y, Tanaka N, Kikuchi Y, Gatanaga H, et al. Incomplete recovery of CD4 cell count, CD4 percentage, and CD4/CD8 ratio in patients with human immunodeficiency virus infection and suppressed viremia during long-term antiretroviral therapy. Clin Infect Dis (2018) 67(6):927–33. doi: 10.1093/cid/ciy176
8. Gras L, May M, Ryder LP, Trickey A, Helleberg M, Obel N, et al. Determinants of restoration of CD4 and CD8 cell counts and their ratio in HIV-1–positive individuals with sustained virological suppression on antiretroviral therapy. JAIDS J Acquir Immune Defic Syndr (2019) 80(3):292–300. doi: 10.1097/QAI.0000000000001913
9. Serrano-Villar S, Sainz T, Lee SA, Hunt PW, Sinclair E, Shacklett BL, et al. HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality. Silvestri G editor. PloS Pathog (2014) 10(5):e1004078. doi: 10.1371/journal.ppat.1004078
10. Perdomo-Celis F, Taborda NA, Rugeles MT. CD8+ T-cell response to HIV infection in the era of antiretroviral therapy. Front Immunol (2019) 10:1896. doi: 10.3389/fimmu.2019.01896
11. Ron R, Moreno E, Martínez-Sanz J, Brañas F, Sainz T, Moreno S, et al. CD4/CD8 ratio during human immunodeficiency virus (HIV) treatment: time for routine monitoring? Clin Infect Dis (2023) 76(9):88-1696. doi: 10.1093/cid/ciad136
12. Chow FC, Wilson MR, Wu K, Ellis RJ, Bosch RJ, Linas BP. Stroke incidence is highest in women and non-Hispanic blacks living with HIV in the AIDS Clinical Trials Group Longitudinal Linked Randomized Trials cohort. AIDS (2018) 32(9):1125–35. doi: 10.1097/QAD.0000000000001799
13. Triplette M, Attia EF, Akgün KM, Soo Hoo GW, Freiberg MS, Butt AA, et al. A low peripheral blood CD4/CD8 ratio is associated with pulmonary emphysema in HIV. PloS One (2017) 12(1):e0170857. doi: 10.1371/journal.pone.0170857
14. Qin F, Lv Q, Hong W, Wei D, Huang K, Lan K, et al. Association between CD4/CD8 ratio recovery and chronic kidney disease among human immunodeficiency virus-infected patients receiving antiretroviral therapy: A 17-year observational cohort study. Front Microbiol (2022) 13:827689. doi: 10.3389/fmicb.2022.827689
15. Hema MN, Ferry T, Dupon M, Cuzin L, Verdon R, Thiébaut R, et al. Low CD4/CD8 ratio is associated with non AIDS-defining cancers in patients on antiretroviral therapy: ANRS CO8 (Aproco/copilote) prospective cohort study. PloS One (2016) 11(8):e0161594. doi: 10.1371/journal.pone.0161594
16. Sigel K, Wisnivesky J, Crothers K, Gordon K, Brown ST, Rimland D, et al. Immunological and infectious risk factors for lung cancer in US veterans with HIV: a longitudinal cohort study. Lancet HIV. (2017) 4(2):e67–73. doi: 10.1016/S2352-3018(16)30215-6
17. Geltzeiler CB, Xu Y, Carchman E, Ghouse Y, Beczkiewicz J, Son J, et al. CD4/CD8 ratio as a novel marker for increased risk of high-grade anal dysplasia and anal cancer in HIV+ Patients: A retrospective cohort study. Dis Colon Rectum. (2020) 63(12):1585–92. doi: 10.1097/DCR.0000000000001763
18. Serrano-Villar S, Pérez-Elías MJ, Dronda F, Casado JL, Moreno A, Royuela A, et al. Increased risk of serious non-AIDS-related events in HIV-infected subjects on antiretroviral therapy associated with a low CD4/CD8 ratio. PloS One (2014) 9(1):e85798. doi: 10.1371/journal.pone.0085798
19. Han WM, Apornpong T, Kerr SJ, Hiransuthikul A, Gatechompol S, Do T, et al. CD4/CD8 ratio normalization rates and low ratio as prognostic marker for non-AIDS defining events among long-term virologically suppressed people living with HIV. AIDS Res Ther (2018) 15(1):13. doi: 10.1186/s12981-018-0200-4
20. Serrano-Villar S, Wu K, Hunt PW, Lok JJ, Ron R, Sainz T, et al. Predictive value of CD8+ T cell and CD4/CD8 ratio at two years of successful ART in the risk of AIDS and non-AIDS events. eBioMedicine (2022) 80:104072. doi: 10.1016/j.ebiom.2022.104072
21. Trickey A, May MT, Schommers P, Tate J, Ingle SM, Guest JL, et al. CD4:CD8 ratio and CD8 count as prognostic markers for mortality in human immunodeficiency virus–infected patients on antiretroviral therapy: the antiretroviral therapy cohort collaboration (ART-CC). Clin Infect Dis (2017) 65(6):959–66. doi: 10.1093/cid/cix466
22. Caby F, Guiguet M, Weiss L, Winston A, Miro JM, Konopnicki D, et al. CD4/CD8 ratio and the risk of kaposi sarcoma or non-hodgkin lymphoma in the context of efficiently treated human immunodeficiency virus (HIV) infection: A collaborative analysis of 20 european cohort studies. Clin Infect Dis (2021) 73(1):50–9. doi: 10.1093/cid/ciaa1137
23. Lang S, Mary-Krause M, Simon A, Partisani M, Gilquin J, Cotte L, et al. HIV replication and immune status are independent predictors of the risk of myocardial infarction in HIV-infected individuals. Clin Infect Dis (2012) 55(4):600–7. doi: 10.1093/cid/cis489
24. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
25. Covidence. Veritas health innovation. Melbourne, Australia. Available at: www.covidence.org.
26. Riley RD, Moons KGM, Snell KIE, Ensor J, Hooft L, Altman DG, et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ (2019) 364:k4597. doi: 10.1136/bmj.k4597
27. Huguet A, Hayden JA, Stinson J, McGrath PJ, Chambers CT, Tougas ME, et al. Judging the quality of evidence in reviews of prognostic factor research: adapting the GRADE framework. Syst Rev (2013) 2(1):71. doi: 10.1186/2046-4053-2-71
28. Collin A, Le Marec F, Vandenhende MA, Lazaro E, Duffau P, Cazanave C, et al. Incidence and risk factors for severe bacterial infections in people living with HIV. ANRS CO3 aquitaine cohort, 2000–2012. PloS One (2016) 11(4):e0152970. doi: 10.1371/journal.pone.0152970
29. Castilho JL, Turner M, Shepherd BE, Koethe JR, Furukawa SS, Bofill CE, et al. CD4/CD8 ratio and CD4 nadir predict mortality following noncommunicable disease diagnosis in adults living with HIV. AIDS Res Hum Retroviruses (2019) 35(10):960–7. doi: 10.1089/aid.2019.0064
30. Klugman M, Fazzari M, Xue X, Ginsberg M, Rohan TE, Halmos B, et al. The associations of CD4 count, CD4/CD8 ratio, and HIV viral load with survival from non-small cell lung cancer in persons living with HIV. AIDS Care (2022) 34(8):1014–21. doi: 10.1080/09540121.2021.1934380
31. Liu J, Wang L, Hou Y, Zhao Y, Dou Z, Ma Y, et al. Immune restoration in HIV-1-infected patients after 12 years of antiretroviral therapy: a real-world observational study. Emerg Microbes Infect (2020) 9(1):2550–61. doi: 10.1080/22221751.2020.1840928
32. Helleberg M, Kronborg G, Ullum H, Ryder LP, Obel N, Gerstoft J. Course and clinical significance of CD8 + T-cell counts in a large cohort of HIV-infected individuals. J Infect Dis (2015) 211(11):1726–34. doi: 10.1093/infdis/jiu669
33. Domínguez-Domínguez L, Rava M, Bisbal O, Lopez-Cortés L, Portilla J, Podzamczer D, et al. Low CD4/CD8 ratio is associated with increased morbidity and mortality in late and non-late presenters: results from a multicentre cohort study, 2004–2018. BMC Infect Dis (2022) 22(1):379. doi: 10.1186/s12879-022-07352-z
34. Borenstein M, Higgins JPT, Hedges LV, Rothstein HR. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res Synth Methods (2017) 8(1):5–18. doi: 10.1002/jrsm.1230
35. Martínez-Sanz J, Álvarez JD, Rosas M, Ron R, Iribarren JA, Bernal E, et al. Expanding HIV clinical monitoring: the role of CD4, CD8, and CD4/CD8 ratio in predicting non-AIDS events. EBioMedicine (2023) 95:104773. doi: 10.1101/2023.03.31.23288001
36. Cervero M, Torres R, Agud JL, Pastor S, Jusdado JJ. Envejecimiento e influencia de la inversión del cociente CD4/CD8 en la incidencia de las comorbilidades y mortalidad de una cohorte de pacientes infectados por el virus de inmunodeficiencia humana. Med Clínica. (2016) 146(5):189–93. doi: 10.1016/j.medcli.2015.10.014
37. Lee S, Byakwaga H, Boum Y, Burdo TH, Williams KC, Lederman MM, et al. Immunologic pathways that predict mortality in HIV-infected Ugandans initiating antiretroviral therapy. J Infect Dis (2017) 215(8):1270–4. doi: 10.1093/infdis/jix113
38. Duffau P, Ozanne A, Bonnet F, Lazaro E, Cazanave C, Blanco P, et al. Multimorbidity, age-related comorbidities and mortality: association of activation, senescence and inflammation markers in HIV adults. AIDS (2018) 32(12):1651–60. doi: 10.1097/QAD.0000000000001875
39. Boettiger DC, Escuder MM, Law MG, Veloso V, Souza RA, Ikeda MLR, et al. Cardiovascular disease among people living with HIV in Brazil. Trop Med Int Health (2020) 25(7):886–96. doi: 10.1111/tmi.13405
40. Aksak-Wąs BJ, Kowalska JD, Ząbek P, Serwin K, Rafalska-Kosior M, Gołąb J, et al. Immune restoration affects 10-year survival in people living with HIV / AIDS. HIV Med (2023) 24(3):325–34. doi: 10.1111/hiv.13391
41. Novak RM, Armon C, Battalora L, Buchacz K, Li J, Ward D, et al. Aging, trends in CD4+/CD8+ cell ratio, and clinical outcomes with persistent HIV suppression in a dynamic cohort of ambulatory HIV patients. AIDS (2022) 36(6):815–27. doi: 10.1097/QAD.0000000000003171
42. Mussini C, Lorenzini P, Cozzi-Lepri A, Lapadula G, Marchetti G, Nicastri E, et al. CD4/CD8 ratio normalisation and non-AIDS-related events in individuals with HIV who achieve viral load suppression with antiretroviral therapy: an observational cohort study. Lancet HIV. (2015) 2(3):e98–106. doi: 10.1016/S2352-3018(15)00006-5
43. Aldrete S, Jang JH, Easley KA, Okulicz J, Dai T, Chen YN, et al. CD4 rate of increase is preferred to CD4 threshold for predicting outcomes among virologically suppressed HIV-infected adults on antiretroviral therapy. PloS One (2020) 15(1):e0227124. doi: 10.1371/journal.pone.0227124
44. Castilho JL, Bian A, Jenkins CA, Shepherd BE, Sigel K, Gill MJ, et al. CD4/CD8 ratio and cancer risk among adults with HIV. JNCI J Natl Cancer Inst (2022) 114(6):854–62. doi: 10.1093/jnci/djac053
45. Lo J, Abbara S, Shturman L, Soni A, Wei J, Rocha-Filho JA, et al. Increased prevalence of subclinical coronary atherosclerosis detected by coronary computed tomography angiography in HIV-infected men. AIDS (2010) 24(2):243–53. doi: 10.1097/QAD.0b013e328333ea9e
46. Lok JJ, Hunt PW, Collier AC, Benson CA, Witt MD, Luque AE, et al. The impact of age on the prognostic capacity of CD8+ T-cell activation during suppressive antiretroviral therapy. AIDS (2013) 27(13):2101–10. doi: 10.1097/QAD.0b013e32836191b1
47. Erlandson KM, Allshouse AA, Jankowski CM, Lee EJ, Rufner KM, Palmer BE, et al. Association of functional impairment with inflammation and immune activation in HIV type 1–infected adults receiving effective antiretroviral therapy. J Infect Dis (2013) 208(2):249–59. doi: 10.1093/infdis/jit147
48. Badejo OA, Chang CC, So-Armah KA, Tracy RP, Baker JV, Rimland D, et al. CD8 + T-cells count in acute myocardial infarction in HIV disease in a predominantly male cohort. BioMed Res Int (2015) 2015:1–5. doi: 10.1155/2015/246870
49. Strindhall J, Skog M, Ernerudh J, Bengner M, Löfgren S, Matussek A, et al. The inverted CD4/CD8 ratio and associated parameters in 66-year-old individuals: the Swedish HEXA immune study. AGE (2013) 35(3):985–91. doi: 10.1007/s11357-012-9400-3
Keywords: HIV, CD4/CD8 ratio, mortality, comorbidities, non-AIDS events
Citation: Ron R, Martínez-Sanz J, Herrera S, Ramos-Ruperto L, Díez-Vidal A, Sainz T, Álvarez-Díaz N, Correa-Pérez A, Muriel A, López-Alcalde J, Pérez-Molina JA, Moreno S and Serrano-Villar S (2024) CD4/CD8 ratio and CD8+ T-cell count as prognostic markers for non-AIDS mortality in people living with HIV. A systematic review and meta-analysis. Front. Immunol. 15:1343124. doi: 10.3389/fimmu.2024.1343124
Received: 01 December 2023; Accepted: 15 January 2024;
Published: 01 February 2024.
Edited by:
Jürgen Rockstroh, University Hospital Bonn, GermanyReviewed by:
Christina K. Psomas, Hôpital Européen Marseille, FranceCopyright © 2024 Ron, Martínez-Sanz, Herrera, Ramos-Ruperto, Díez-Vidal, Sainz, Álvarez-Díaz, Correa-Pérez, Muriel, López-Alcalde, Pérez-Molina, Moreno and Serrano-Villar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Ron, cmFxdWVsLnJvbmdvbnphbGV6QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.