 Dan D. Wei
Dan D. Wei Jin M. Fang1,3
Jin M. Fang1,3 Yan-Yi Jiang
Yan-Yi Jiang Yuan Jiang
Yuan Jiang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 19 February 2024
Sec. Cancer Immunity and Immunotherapy
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1330785
This article is part of the Research Topic The Current and Future Roles of Immunotherapies in the Multimodal Treatment of Esophageal Cancer View all 9 articles
Esophageal squamous cell carcinoma (ESCC) is the main prevalent histological subtype and accounts for 85% of esophageal cancer cases worldwide. Traditional treatment for ESCC involves chemotherapy, radiotherapy, and surgery. However, the overall prognosis remains unfavorable. Recently, immune checkpoint blockade (ICB) therapy using anti-programmed cell death-1 (PD-1)/PD-1 ligand (PD-L1) antibodies have not only achieved remarkable benefits in the clinical management of ESCC but have also completely changed the treatment approach for this cancer. In just a few years, ICB therapy has rapidly advanced and been added to standard first-line treatment regimen in patients with ESCC. However, preoperative immunotherapy is yet to be approved. In this review, we summarize the ICB antibodies commonly used in clinical immunotherapy of ESCC, and discuss the advances of immunotherapy combined with chemotherapy and radiotherapy in the perioperative treatment of ESCC, aiming to provide reference for clinical management of ESCC patients across the whole course of treatment.
● The combination of immunotherapy and chemotherapy offers a potential perioperative option for patients with resectable ESCC.
● Neoadjuvant immunotherapy combined with chemotherapy results in encouraging major pathologic response rates without introducing new adverse reactions in patients with operable ESCC.
Esophageal cancer ranks among the most common malignant tumors, and causes more than half a million cancer-related mortality world-wide each year (1). Esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma are the two main pathological subtypes of esophageal cancer, and have almost completely distinct biologic, geographic and etiologic characteristics. ESCC accounts for about 85% of the 604,100 incident esophageal cancers each year, predominating in regions of Eastern Asia and Africa (2). Traditional treatment options for ESCC include chemotherapy, radiotherapy, and surgery. However, due to the neglect of early symptoms of ESCC, many patients are diagnosed at an advanced stage, leading to a poor overall prognosis with a five-year survival rate of approximately 10%20% (3). Surgery combined with neoadjuvant chemoradiotherapy is the preferred treatment for locally advanced ESCC patients, but recurrence and metastasis still occur in many patients after treatment (4).
Recent years, cancer immunotherapy has emerged as a promising anti-tumor therapeutic strategy after surgery, radiotherapy and chemotherapy. In particular, immune checkpoint blockade (ICB) antibodies have been developed to enhance immune responses or/and alleviate immunosuppression by acting on immune checkpoints such as cytotoxic T lymphocyte antigen 4 (CTLA-4), programmed cell death-1 (PD-1) or PD-1 ligand (PD-L1) PD-1, and PD-L1. Currently, the most advanced ICB agents are anti-PD-1/PD-L1 antibodies because of the central role of T cells in tumor immunological surveillance, which have demonstrated substantial clinical progress (5). However, the efficacy of immunotherapy alone is only 20%-40% (6). Limited overall responses and the lack of reliable biomarkers predicting patients response are major obstacles to immunotherapy. This reflects the compelling need of unveiling novel targets for immunotherapy that allow to expand the spectrum of ICB-based strategies to achieve optimal therapeutic efficacy and benefit for cancer patients (7). New immune checkpoint inhibitors that mediate T cell inhibitory signaling such as lymphocyte-activation gene 3 (LAG-3), T-cell immunoglobulin and mucin domain-3 (TIM-3), V-domain Ig suppressor of T cell activation (VISTA), T-cell immunoreceptor with Ig and ITIM domains (TIGIT), inducible T-cell co-stimulatory receptor (ICOS), Nuclear receptor subfamily 2, group F, member 6 (NR2F6), sialic acid-binding immunoglobulin-like lectins-8 (SIGLEC8) and B and T lymphocyte attenuator (BTLA) are developed to overcome resistance to cancer immunotherapy and improve the outcome for cancer patients (8–10). Some of these new drugs and therapeutic regimens have been tested in clinical studies and achieved promising results.
In clinical practice, immune combined chemotherapy is mostly recommended to enhance the tumor response rate. Herein, we summarize the progress of immunotherapy combined with chemotherapy in the perioperative treatment of ESCC patients, along with proposing possible challenges and future solutions for the current implementation of perioperative immunotherapy in ESCC.
PD-1/PD-L1 represents a common immune checkpoint in T cell activation, with PD-1 being expressed on the surface of T cells and PD-L1 often expressed in tumor cells except for macrophages (11). The binding of PD-1 to its ligand PD-L1 activates an intercellular inhibitory signaling pathway of T cells, resulting in the inhibition of T cell function. Furthermore, activated T cells can express CD80 as a receptor for transmitting inhibitory signals, leading to the tolerance of peripheral T cell. PD-L1 expression by tumor cells can evade attack by CD8+ T cells (12). When cancer cells release tumour-associated neoantigens, these neoantigens will be recognized by antigen-presenting cells and rendered to immune cells by the interaction with T cell receptor (TCR) (13). CD8+ T cells will be activated and release Granzyme and Perforin to kill cancer cells. Conventionally, PD-L1 or PD-L2 express on the surface of antigen presenting cells to prevent autoimmune disorders. However, tumor cells acquire this skill and escape immune attack successfully, knowing as immune evasion by upregulation of immunoinhibitory molecules (e.g., PD-1, CTLA-4, TIM3, TIGIT, CD96), or their ligands (14). Blocking the interaction between tumor and T cells such as PD-1/PD-L1 or CTLA-4/B7 axis with immune checkpoint inhibitors could avoid immune evasion and eliminate malignant cells. (Figure 1). Anti-PD-1/PD-L1 monoclonal antibody reactivates the immune response of T cells to tumors by blocking the binding of PD-1 to PD-L1 protein, thereby achieving an antitumor effect (15). Immune checkpoints play a complex balance role in the body, maintaining self-tolerance and regulating the immune response. The stimulation pathway promotes T cell activation, while the inhibition pathway inhibits T cell activation. Anti-PD-1/PD-L1 antibodies are currently the most extensively investigated immune checkpoint inhibitors and have been recommended for treating various of malignancies (Table 1).
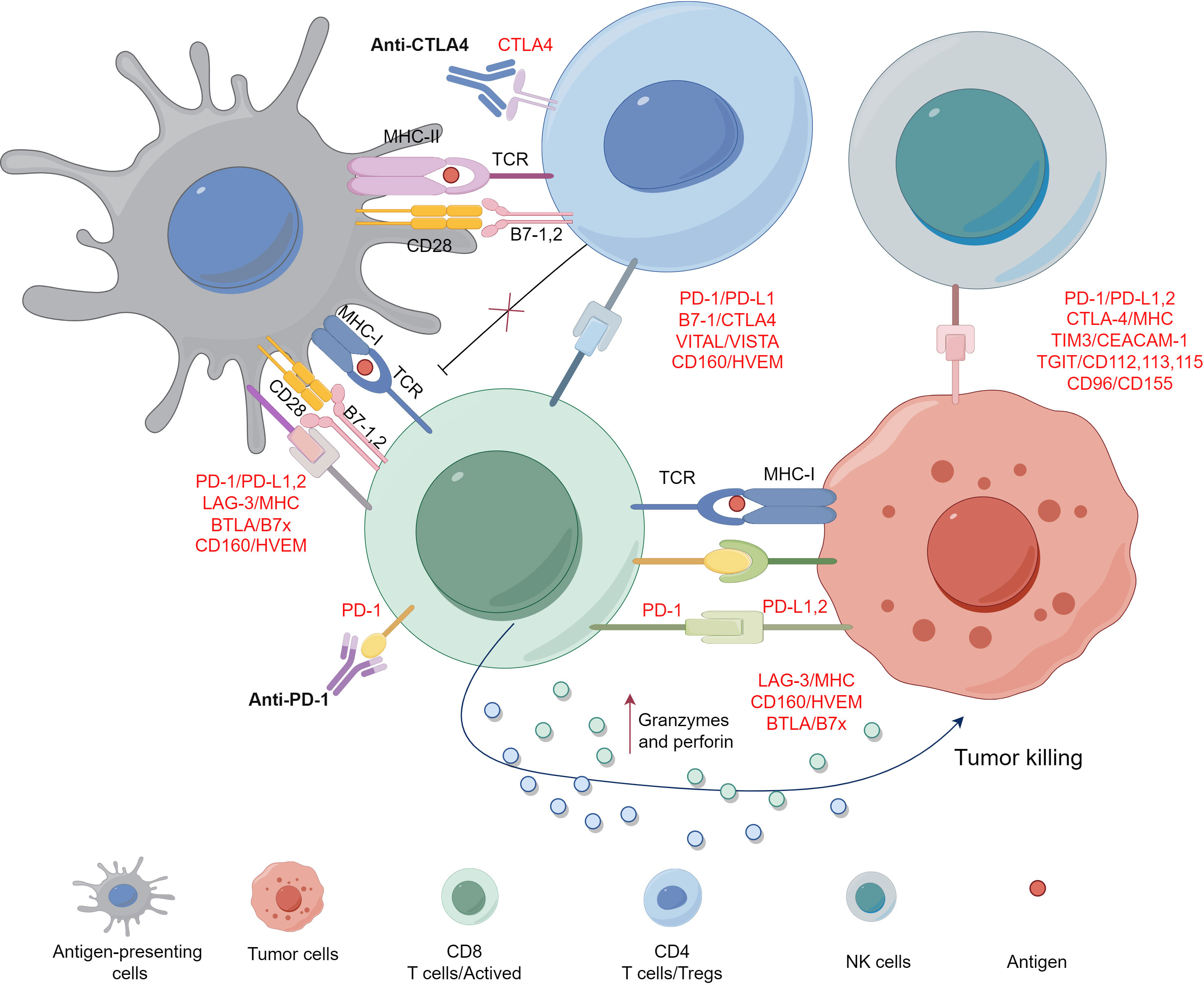
Figure 1 PD-1/PD-L1 interaction between T cell and tumor cell.
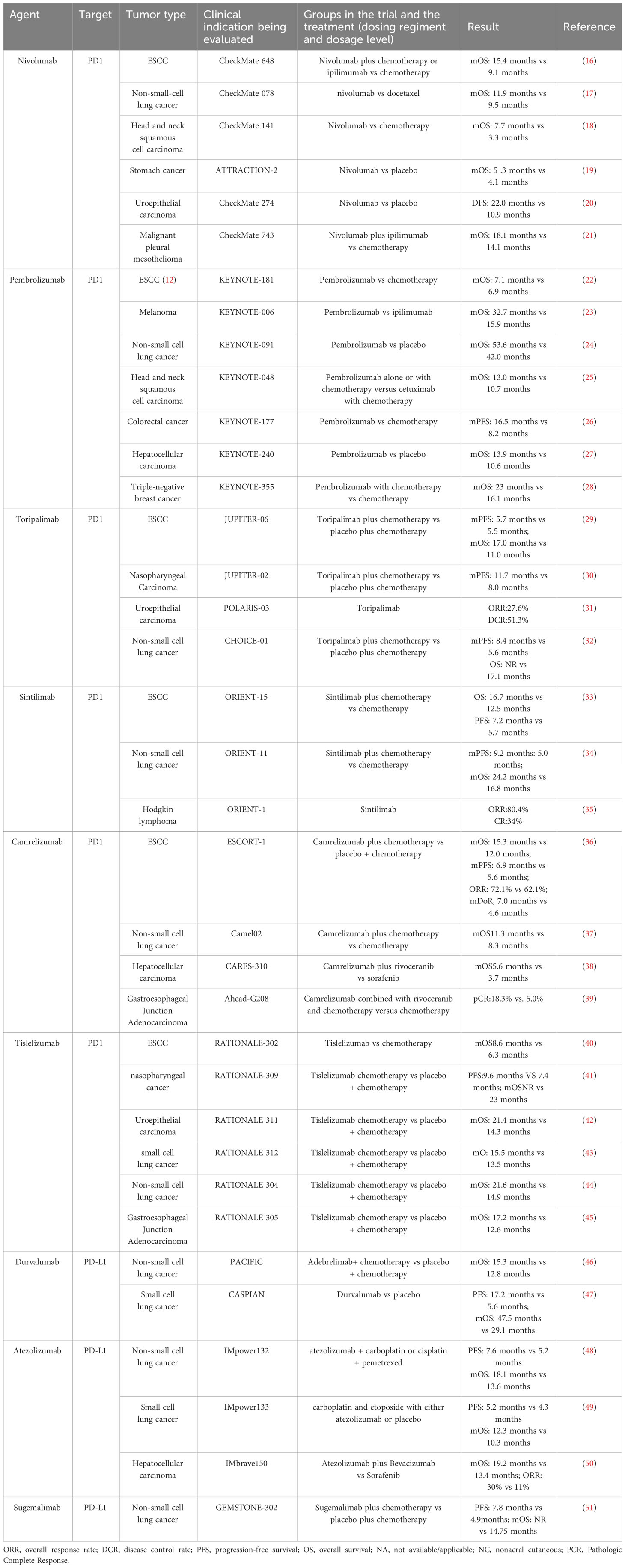
Table 1 Immunotherapies in the clinic.
In recent years, the in-depth study of immunotherapy has ushered ESCC into the era of immunotherapy. Pembrolizumab combined with chemotherapy has gained approval as a first-line treatment for unresectable locally advanced or metastatic esophageal or gastroesophageal junction cancer based on KEYNOTE-590 study (52). This combination is the first approved immunotherapeutic agent for ESCC. Subsequently, several phase III, randomized, multicenter studies in advanced ESCC have demonstrated promising clinical activities. For instance, studies of CheckMate 648 for nivolumab (16), KEYNOTE-181 for pembrolizumab (22), JUPITER-06 for toripalimab (29), ORIENT-15 of sintilimab (33), ESCORT-1st for camrelizumab (36), and RATIONALE-302 for tislelizumab (40) have confirmed the efficacy advantage of immunotherapy in treating advanced ESCC. These drugs have thus been recommended in clinical guideline as first- and second-line treatment options in advanced-stage ESCC. However, the benefit of perioperative immunotherapy especially in the neoadjuvant setting is still being exploring.
As cancer research progresses, cancer diagnosis and treatment have embraced the multi-disciplinary treatment model (MDT). The therapeutic benefits of immunotherapy at various stages of tumor progression have gradually been recognized, although neoadjuvant immunotherapy in ESCC is still rarely investigated. Traditional neoadjuvant chemotherapy aims to minimize tumor lesions and achieve preoperative downstaging for radical surgery, while neoadjuvant immunotherapy can eliminate micro metastatic tumor lesions by enhancing anti-tumor immune response (53). Furthermore, receiving immunotherapy at the initial diagnostic stage occurs when the patient has relatively competent immunity, allowing for activating immune response. Thus, it is theoretically feasible to incorporate immunotherapy in the preoperative neoadjuvant or conversion treatment stage.
The initial exploration of neoadjuvant modality in the perioperative setting of esophageal cancer was CROSS study (54). This study confirmed that neoadjuvant chemoradiotherapy before surgery provided an overall survival (OS) benefit and which persisted for at least 10 years for patients with locally advanced resectable esophageal or gastroesophageal junction cancer. The CROSS study has thus become a landmark trial in the perioperative treatment of esophageal cancer. However, clinical practice has found that patients who underwent surgery after neoadjuvant chemoradiotherapy had a higher risk of postoperative complications such as esophageal fistula and bleeding, which also increased the complexity of the surgery. Previous studies have demonstrated that platinum-based chemotherapeutic agents promoted the expression of PD-L1 on tumor cells, and consequently exhibited a synergistic effect with anti-PD-L1 immunotherapy (55). The application of neoadjuvant immunotherapy in esophageal cancer first emerged from a single-center, prospective, single-arm PALACE-1 study (56), which aimed to assess the effectiveness and safety of preoperative pembrolizumab combined with chemoradiotherapy in the neoadjuvant treatment of locally advanced ESCC. The findings demonstrated that pembrolizumab combined with neoadjuvant concurrent chemoradiotherapy achieved a pathological complete response (pCR) rate of 55.6% (10/18), a major pathological response (MPR) rate of 89% (16/18), and a margin-negative R0 (R0 defined as no vital tumor present within 1 mm of the proximal, distal, or circumferential resection margins) resection rate of 94%. The KEYSTONE-001 study (57), conducted by Tianjin Medical University Cancer Institute & Hospital is the first research in the world to investigate the efficacy and safety of pembrolizumab combined with paclitaxel and cisplatin for neoadjuvant treatment of locally advanced ESCC. The latest findings indicated that among 29 patients who underwent surgery, a pCR rate of 41.4% (12/29), a MPR rate of 72.4% (21/29), and a R0 resection rate of 100% were achieved. These data support a favorable safety and prominent anti-tumor activity for anti-PD-1 immunotherapy combined with chemotherapy in patients with locally advanced resectable ESCC in the neoadjuvant setting. Another study called ESPRIT investigated the effectiveness and safety of neoadjuvant camrelizumab combined with chemotherapy in ESCC (58). Preliminary findings demonstrated that among 11 patients who received surgical treatment, the pCR rate was 45.5% (5/11), which was not associated with the expression of PD-L1, and lymph nodes alone (pT0) rate was 54.5% (6/11), with an R0 resection rate of 100%. The combination of camrelizumab, paclitaxel, and carboplatin as a neoadjuvant therapy regimen demonstrated good tolerability and achieve preoperative downstaging. The KEEP-G 03 study (59) assessed the feasibility and safety of neoadjuvant treatment of resectable ESCC with sintilimab plus triplet chemotherapy (liposomal paclitaxel, cisplatin, and S-1) every 3 weeks for two cycles. Of these 30 patients received surgical treatment, the MPR, pCR rates were 50.0% (15/30; 95% CI 33.2 to 66.9) and 20.0% (6/30; 95% CI 9.5 to 37.3), respectively. R0 resection rates were 100%. In the phase II TD-NICE study (60), 45 resectable ESCC patients were enrolled for 3 cycles of neoadjuvant tislelizumab combined with chemotherapy. Among them, 36 patients underwent surgery, the R0 resection, MPR and pCR rates were respectively 80.5%, 72% (25/36), and 50% (18/36). This study further proposed for the first time that tumor proportion score cut-off>1 was a better indicator to predict pCR than combined proportion score, and it was also confirmed that HLA-A02 gene mutation may be associated with pCR through next-generation sequencing. Additionally, TP53 (86%), NOTCHI (40%), FAT1(26%), CDKN2A (23%), and EP300(17%) were identified as the most mutated genes; however, no clear correlation between these genes and pCR or MPR was revealed. In summary, these studies suggest that immunotherapy combination with chemotherapy is a promising regimen with favorable efficacy and safety for the neoadjuvant treatment of ESCC.
Adjuvant therapy aims to eliminate subclinical metastatic lesions and reduce the recurrence and metastasis rates (61). However, controversies still exist regarding adjuvant treatment for esophageal cancer in clinical practice. The 5-year survival rate with surgery alone for locally advanced esophageal cancer (pT3-4 or pN+) is only 20%40% (62). In the CheckMate577 study (63), the patients were randomly assigned into a 2:1 ratio to receive either nivolumab or placebo from 4 to 16 weeks after neoadjuvant radiotherapy and surgery. It was demonstrated that in patients who did not achieve clinical pCR to neoadjuvant immunotherapy in combination with chemotherapy following surgery, adjuvant nivolumab substantially prolonged median disease-free survival in the intention-to-treat population (20.8 months vs 10.8 months). Moreover, adjuvant nivolumab provided survival benefits regardless of histological type and pathological feature of lymph node, and no major differences were observed on safety in the patients receiving either adjuvant immunotherapy or not. A phase II randomized controlled study from Korea (64) assessed the effectiveness of adjuvant durvalumab after neoadjuvant concurrent chemoradiotherapy and surgery in 86 ESCC patients, with a median 38.7 months follow-up for survival analysis. Median disease-free survival (DFS) was not reached in any group. At 12, 24, and 36 months, the disease-free survival rates were 71%, 58%, and 55% in the durvalumab group and 73%, 61%, and 61% in the placebo group, respectively. No significant differences in disease-free survival and OS were observed between the durvalumab and placebo groups. However, this study initially indicated that PD-L1 expression after concurrent chemoradiotherapy could predict survival benefit in patients receiving adjuvant durvalumab after neoadjuvant concurrent chemoradiotherapy, although this finding needed further validation from larger randomized controlled studies. AIRES is a multicenter phase III trial in ESCC patients in China, aimed to assess the effectiveness and safety of tislelizumab combined with chemotherapy versus adjuvant tislelizumab alone in patients with radical resection for high-risk ESCC. The study is ongoing, and further better clinical data are anticipated.
Currently, the option of adjuvant therapy for esophageal cancer depends more on severity of the disease and local clinical practice models. The traditional belief is that adjuvant therapy may only be beneficial for patients with positive lymph nodes or an increased risk of recurrence, and the National Comprehensive Cancer Network (NCCN) previously recommended its use for patients who underwent incomplete resection (65). In 2021, Food and Drug Administration has approved nivolumab as an adjuvant treatment option for esophageal cancer patients received triple therapy based on the findings of the Checkmate577 study. The nutritional status of patients often deteriorates due to the reconstruction of the digestive system in esophageal cancer patients after surgery, and this issue is particularly prominent in Chinese patients with esophageal cancer. Many patients are often unable to tolerate traditional platinum-containing doublet chemotherapy after surgery, but they have a good tolerance to immune drugs, which makes adjuvant immunotherapy worthy of more in-depth research. From the initial CROSS trial to the Checkmate577 study, numerous curative possibilities have emerged for locally advanced resectable esophageal cancer. These studies also provide valuable references for the clinical managements of esophageal cancer.
In recent years, there has been controversy for the treatment modalities of esophageal cancer in the perioperative setting (66), mainly focusing on neoadjuvant therapy. Current neoadjuvant therapy modalities include chemotherapy, chemoradiotherapy, immunotherapy, and immunotherapy combined with radiotherapy or chemoradiotherapy. In North America, neoadjuvant chemoradiotherapy followed by esophagectomy is the standard treatment option for locally advanced esophageal cancer. In Asia, neoadjuvant chemotherapy or neoadjuvant immunotherapy combined chemotherapy is more commonly conducted. We believe that the findings in clinical studies will provide clear references for the neoadjuvant treatment mode of esophageal cancer. Currently, neoadjuvant treatment for locally advanced esophageal cancer is being recommended as the new standard by the NCCN guidelines and the Chinese Society of Clinical Oncology guidelines (67). Neoadjuvant immunotherapy offers a novel option for neoadjuvant treatment of esophageal cancer, and preliminary clinical results indicate that it can lead to disease remission in some patients with esophageal cancer. Moreover, immunotherapy combined with chemotherapy effectively improves the PCR rate of esophageal cancer patients compared with chemotherapy alone without causing significant treatment-related adverse events. This combination is expected to prolong the survival of patients with locally advanced resectable esophageal cancer and become a crucial model in the neoadjuvant therapy of esophageal cancer in the future. Neoadjuvant immunotherapy for esophageal cancer is still in the exploratory stage, and several ongoing phase III studies in large-scale are expected to further investigate the safety, efficacy and optimal time-window for the administration of immunotherapy drugs.
Although immunotherapy is increasingly recognized as a crucial therapeutic strategy for the management of esophageal cancer treatment, clinical data reveal that only approximately 20%-40% of patients benefit from it. Therefore, understanding how the remaining patients can benefit from immunotherapy is an urgent clinical challenge. Many factors including PD-L1 expression, tumor neoantigen expression and delivery, related cellular signaling pathways, tumor microenvironment, epigenetic modifications have been confirmed to involved in the response to PD-1/PD-L1 blockade therapy (68). Regulatory T cells (Tregs) play a role in suppression of effector T cell response by secretion of IL-10, IL-35, and TGF-β. PD-1 expression upregulates conversion of naive CD4+ T cells to immunosuppressive Treg cells through inhibition of the mTOR-Akt signaling cascade. Aberrant cellular signal transduction including the PI3K/AKT pathway, WNT/β-catenin pathway, JAK/STAT/IFN-γ pathway, and MAPK pathway have also been proved to be major factors to immunotherapy resistance (69–71).
In addition, numerous findings have revealed in ESCC patients the instability of genome and alterations in epigenome (66, 67, 72–74), which led to significant heterogeneity among ESCC patients (75). A study from Cancer Hospital, Chinese Academy of Medical Sciences classified ESCC into four subtypes (cell cycle pathway activation, NRF2 oncogenic activation, immune suppression, and immune modulation) based on multi-omics data analysis. This is the first internationally to establish multi-omics-based classification for ESCC. In addition, they identified potential therapeutic targets/biomarkers that can be employed for diagnosis for each subtype, providing theoretical basis and novel strategies for achieving precision medicine for ESCC patients. Recently, our findings reveal a novel mechanism by which ESCC cells escape immune surveillance through TP63-suppressed interferon-STAT1 axis and cytotoxic CD8 T cells. And importantly, inhibition of TP63 enhance the efficacy of PD-1 mAb therapy in syngeneic mouse models.
Thus, to further improve clinical benefits, future efforts should be made to identify predictive biomarkers and target patients for immunotherapy, to explore factors that affect patient response to immune checkpoint-based therapy. In clinical managements, the cycles of neoadjuvant immunotherapy, the ways to surmount the primary and acquired resistance, as well as the maintenance of a durable efficacy of immunotherapy remain unavoidable challenges in the future.
Improvements have been made to increase R0 resection rates and PCR rate as well as survival outcomes with neoadjuvant chemotherapy combining ICB therapy for locally advanced ESCC. In addition, ICB therapy in an adjuvant setting has revolutionized the treatment landscape of ESCC. In the future, incorporation of immunotherapy in the preoperative neoadjuvant treatment, the optimal time-window for the administration of immunotherapy, multi-disciplinary treatment model and elucidation of pathogenic mechanism of ESCC will provide precise strategies for this type of cancer. In addition, further innovations in endoscopic, surgical resection and radiotherapy approaches as well as cell therapy such as CAR-T, TCR-T would potentially improve the outcomes of ESCC patients.
DW: Conceptualization, Data curation, Funding acquisition, Investigation, Writing – original draft, Writing – review & editing. YJ: Funding acquisition, Writing – review & editing, Data curation. JF: Data curation, Writing – review & editing. HW: Data curation, Writing – review & editing. JC: Data curation, Investigation, Writing – review & editing. SK: Visualization, Writing – review & editing. Y-YJ: Funding acquisition, Investigation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants from the National Natural Science Foundation of China (82103315 and 82273010 to Y-YJ, 32100476 to YJ), Anhui Provincial Natural Science Foundation (2208085J44 to Y-YJ, 2108085MC77 to YJ), and the CASHIPS Directors Fund (BJPY2022B09 to Y-YJ, YZJJ202105 to YJ). The CASHIPS Director’s Fund (YZJJ2023QN49 to DW), and the Excellent Youth Project of Hefei Cancer Hospital (YQJH2021003 to DW).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
2. Chen R, Zheng R, Zhang S, Wang S, Sun K, Zeng H, et al. Patterns and trends in esophageal cancer incidence and mortality in China: An analysis based on cancer registry data. J Natl Cancer Center (2023) 3:21–7. doi: 10.1002/cam4.3647
3. Testa U, Castelli G, Pelosi E. The molecular characterization of genetic abnormalities in esophageal squamous cell carcinoma may foster the development of targeted therapies. Curr Oncol (2023) 30:610–40. doi: 10.3390/curroncol30010048
4. Li X, Chen L, Luan S, Zhou J, Xiao X, Yang Y, et al. The development and progress of nanomedicine for esophageal cancer diagnosis and treatment. Semin Cancer Biol (2022) 86:873–85. doi: 10.1016/j.semcancer.2022.01.007
5. Rieth J, Subramanian S. Mechanisms of intrinsic tumor resistance to immunotherapy. Int J Mol Sci (2018) 19:1340. doi: 10.3390/ijms19051340
6. Zou LQ, Yang X, Li YD, Zhu ZF. Immune checkpoint inhibitors: a new era for esophageal cancer. Expert Rev Anticancer Ther (2019) 19:731–8. doi: 10.1080/14737140.2019.1654379
7. Zhang H, Dai Z, Wu W, Wang Z, Zhang N, Zhang L, et al. Regulatory mechanisms of immune checkpoints PD-L1 and CTLA-4 in cancer. J Exp Clin Cancer Res (2021) 40:184. doi: 10.1186/s13046-021-01987-7
8. Ferragut F, Alcaraz PB, Beati P, Girard MC, Ossowski MS, Chadi R, et al. Expression of inhibitory receptors TIGIT, TIM-3, and LAG-3 on CD4+ T cells from patients with different clinical forms of chronic chagas disease. J Immunol (2023) 210:568–79. doi: 10.4049/jimmunol.2200436
9. Cai L, Li Y, Tan J, Xu L, Li Y. Targeting LAG-3, TIM-3, and TIGIT for cancer immunotherapy. J Hematol Oncol (2023) 16:101. doi: 10.1186/s13045-023-01499-1
10. Yiong CS, Lin TP, Lim VY, Toh TB, Yang VS. Biomarkers for immune checkpoint inhibition in sarcomas - are we close to clinical implementation? biomark Res (2023) 11:75. doi: 10.1186/s40364-023-00513-5
11. Zou W, Wolchok JD, Chen L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci Trans Med (2016) 8:328rv4. doi: 10.1126/scitranslmed.aad7118
12. Yi M, Jiao D, Xu H, Liu Q, Zhao W, Han X, et al. Biomarkers for predicting efficacy of PD-1/PD-L1 inhibitors. Mol Cancer (2018) 17:129. doi: 10.1186/s12943-018-0864-3
13. Waldman AD, Fritz JM, Lenardo MJ. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat Rev Immunol (2020) 20:651–68. doi: 10.1038/s41577-020-0306-5
14. Murciano-Goroff YR, Warner AB, Wolchok JD. The future of cancer immunotherapy: microenvironment-targeting combinations. Cell Res (2020) 30:507–19. doi: 10.1038/s41422-020-0337-2
15. Shen X, Zhao B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: meta-analysis. BMJ (Clinical Res ed.) (2018) 362:k3529. doi: 10.1136/bmj.k3529
16. Kato K, Doki Y, Ogata T, Motoyama S, Kawakami H, Ueno M, et al. First-line nivolumab plus ipilimumab or chemotherapy versus chemotherapy alone in advanced esophageal squamous cell carcinoma: a Japanese subgroup analysis of open-label, phase 3 trial (CheckMate 648/ONO-4538-50). Esophagus (2023) 20:291–301. doi: 10.1177/17588359221122733
17. Wu YL, Lu S, Cheng Y, Zhou C, Wang J, Mok T, et al. Nivolumab versus docetaxel in a predominantly chinese patient population with previously treated advanced NSCLC: checkMate 078 randomized phase III clinical trial. J Thorac Oncol (2019) 14:867–75.
18. Gillison ML, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Long-term outcomes with nivolumab as first-line treatment in recurrent or metastatic head and neck cancer: subgroup analysis of checkMate 141. oncologist (2022) 27:e194–8. doi: 10.1016/j.jtho.2019.01.006
19. Kang YK, Boku N, Satoh T, Ryu MH, Chao Y, Kato K, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet (2017) 390:2461–71. doi: 10.1016/S0140-6736(17)31827-5
20. Witjes JA, Galsky MD, Gschwend JE, Broughton E, Braverman J, Nasroulah F, et al. Health-related quality of life with adjuvant nivolumab after radical resection for high-risk muscle-invasive urothelial carcinoma: results from the phase 3 checkMate 274 trial. Eur Urol Oncol (2022) 5:553–63. doi: 10.1016/j.euo.2022.02.003
21. Baas P, Scherpereel A, Nowak AK, Fujimoto N, Peters S, Tsao AS, et al. First-line nivolumab plus ipilimumab in unresectable Malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet (2021) 397:375–86. doi: 10.1016/S1470-2045(20)30110-8
22. Kojima T, Shah MA, Muro K, Francois E, Adenis A, Hsu CH, et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol (2020) 38:4138–48. doi: 10.1016/S1470-2045(23)00108-0
23. Robert C, Ribas A, Schachter J, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol (2019) 20:1239–51. doi: 10.1016/S1470-2045(19)30388-2
24. O'Brien M, Paz-Ares L, Marreaud S, Dafni U, Oselin K, Havel L, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet (2022) 23:1274–86. doi: 10.1016/S1470-2045(15)00040-6
25. Burtness B, Harrington KJ, Greil R, Soulieres D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet (London England) (2019) 394:1915–28. doi: 10.1016/S0140-6736(19)32591-7
26. Diaz LA Jr., Shiu KK, Kim TW, Jensen BV, Jensen LH, Punt C, et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, phase 3 study. Lancet Oncol (2022) 23:659–70. doi: 10.1016/S1470-2045(22)00197-8
27. Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: A randomized, double-blind, phase III trial. J Clin Oncol (2020) 38:193–202. doi: 10.21037/atm-22-513
28. Cortes J, Cescon DW, Rugo HS, Nowecki Z, Im SA, Yusof MM, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet (London England) (2020) 396:1817–28. doi: 10.1200/JCO.2021.39.15_suppl.e16033
29. Wang ZX, Cui C, Yao J, Zhang Y, Li M, Feng J, et al. Toripalimab plus chemotherapy in treatment-naive, advanced esophageal squamous cell carcinoma (JUPITER-06): A multi-center phase 3 trial. Cancer Cell (2022) 40:277–288.e3. doi: 10.1136/jitc-2022-005830
30. Mai H-Q, Chen Q-Y, Chen D, Hu C, Yang K, Wen J, et al. Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. Nat Med (2021) 27:1536–43. doi: 10.1038/s41591-021-01444-0
31. Zang J, Zhang R, Jin D, Xie F, Shahatiaili A, Wu G, et al. Integrated longitudinal circulating tumor DNA profiling predicts immunotherapy response of metastatic urothelial carcinoma in the POLARIS-03 trial. J Pathol (2023) 261:198–209. doi: 10.1002/path.6166
32. Wang Z, Wu L, Li B, Cheng Y, Li X, Wang X, et al. Toripalimab plus chemotherapy for patients with treatment-naive advanced non-small-cell lung cancer: A multicenter randomized phase III trial (CHOICE-01). J Clin Oncol (2023) 41:651–63. doi: 10.1200/JCO.22.00727
33. Lu Z, Wang J, Shu Y, Liu L, Kong L, Yang L, et al. Sintilimab versus placebo in combination with chemotherapy as first line treatment for locally advanced or metastatic oesophageal squamous cell carcinoma (ORIENT-15): multicentre, randomised, double blind, phase 3 trial. BMJ (2022) 377:e068714. doi: 10.1136/bmj-2021-068714
34. Yang Y, Sun J, Wang Z, Fang J, Yu Q, Han B, et al. Updated overall survival data and predictive biomarkers of sintilimab plus pemetrexed and platinum as first-line treatment for locally advanced or metastatic nonsquamous NSCLC in the phase 3 ORIENT-11 study. J Thorac Oncol (2021) 16:2109–20. doi: 10.1016/j.jtho.2021.07.015
35. Shi Y, Su H, Song Y, Jiang W, Sun X, Qian W, et al. Safety and activity of sintilimab in patients with relapsed or refractory classical Hodgkin lymphoma (ORIENT-1): a multicentre, single-arm, phase 2 trial. Lancet Haematology (2019) 6:e12–9. doi: 10.1016/S2352-3026(18)30192-3
36. Huang J, Xu J, Chen Y, Zhuang W, Zhang Y, Chen Z, et al. Camrelizumab versus investigator's choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): a multicentre, randomised, open-label, phase 3 study. Lancet Oncol (2020) 21:832–42. doi: 10.1016/S1470-2045(20)30110-8
37. Ren S, Chen J, Xu X, Jiang T, Cheng Y, Chen G, et al. Camrelizumab plus carboplatin and paclitaxel as first-line treatment for advanced squamous NSCLC (CameL-sq): A phase 3 trial. J Thorac Oncol (2022) 17:544–57. doi: 10.1016/j.jtho.2021.11.018
38. Qin S, Chan SL, Gu S, Bai Y, Ren Z, Lin X, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet (London England) (2023) 402:1133–46. doi: 10.1016/S0140-6736(23)00961-3
39. Li S, Yu W, Xie F, Luo H, Liu Z, Lv W, et al. Neoadjuvant therapy with immune checkpoint blockade, antiangiogenesis, and chemotherapy for locally advanced gastric cancer. Nat Commun (2023) 14:8. doi: 10.1038/s41467-022-35431-x
40. Xu J, Kato K, Raymond E, Hubner RA, Shu Y, Pan Y, et al. Tislelizumab plus chemotherapy versus placebo plus chemotherapy as first-line treatment for advanced or metastatic oesophageal squamous cell carcinoma (RATIONALE-306): a global, randomised, placebo-controlled, phase 3 study. Lancet Oncol (2023) 24:483–95. doi: 10.1016/S1470-2045(23)00108-0
41. Yang Y, Pan J, Wang H, Zhao Y, Qu S, Chen N, et al. Tislelizumab plus chemotherapy as first-line treatment for recurrent or metastatic nasopharyngeal cancer: A multicenter phase 3 trial (RATIONALE-309). Cancer Cell (2023) 41:1061–72. doi: 10.1016/j.ccell.2023.04.014
42. Yu R, Wang W, Li T, Li J, Zhao K, Wang W, et al. RATIONALE 311: tislelizumab plus concurrent chemoradiotherapy for localized esophageal squamous cell carcinoma. Future Oncol (London England) (2021) 17:4081–9. doi: 10.2217/fon-2021-0632
43. Cheng Y, Fan Y, Zhao Y, Huang D, Li X, Zhang P, et al. First-line chemotherapy with or without tislelizumab for extensive-stage small cell lung cancer: RATIONALE-312 phase 3 study. J Thorac Oncol (2023) 18:S46. doi: 10.1016/j.jtho.2023.09
44. Lu S, Wang J, Yu Y, Yu X, Hu Y, Ai X, et al. Tislelizumab plus chemotherapy as first-line treatment for locally advanced or metastatic nonsquamous NSCLC (RATIONALE 304): A randomized phase 3 trial. J Thorac Oncol (2021) 16:1512–22. doi: 10.1001/jamaoncol.2021.0366
45. Moehler MH, Kato K, Arkenau H-T, Oh D-Y, Tabernero J, Cruz-Correa M, et al. Rationale 305: Phase 3 study of tislelizumab plus chemotherapy vs placebo plus chemotherapy as first-line treatment (1L) of advanced gastric or gastroesophageal junction adenocarcinoma (GC/GEJC). J Clin Oncol (2023) 41:286–6. doi: 10.1200/JCO.2023.41.4_suppl.28
46. Spigel DR, Faivre-Finn C, Gray JE, Vicente D, Planchard D, Paz-Ares L, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol (2022) 40:1301–11. doi: 10.1016/j.jtho.2019.01.006
47. Paz-Ares L, Chen Y, Reinmuth N, Hotta K, Trukhin D, Statsenko G, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open (2022) 7:100408. doi: 10.1093/oncolo/oyab036
48. Lu S, Fang J, Wang Z, Fan Y, Liu Y, He J, et al. Results from the IMpower132 China cohort: Atezolizumab plus platinum-based chemotherapy in advanced non-small cell lung cancer. Cancer Med (2023) 12:2666–76. doi: 10.1016/S0140-6736(17)31827-5
49. Horn L, Mansfield AS, Szczęsna A, Havel L, Krzakowski M, Hochmair MJ, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. New Engl J Med (2018) 379:2220–9. doi: 10.1016/j.euo.2022.02.003
50. Hack SP, Spahn J, Chen M, Cheng AL, Kaseb A, Kudo M, et al. IMbrave 050: a Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol (London England) (2020) 16:975–89. doi: 10.1016/S0140-6736(20)32714-8
51. Zhou C, Wang Z, Sun Y, Cao L, Ma Z, Wu R, et al. Sugemalimab versus placebo, in combination with platinum-based chemotherapy, as first-line treatment of metastatic non-small-cell lung cancer (GEMSTONE-302): interim and final analyses of a double-blind, randomised, phase 3 clinical trial. Lancet Oncol (2022) 23:220–33. doi: 10.1016/S1470-2045(19)30388-2
52. Sun JM, Shen L, Shah MA, Enzinger P, Adenis A, Doi T, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet (London England) (2021) 398:759–71. doi: 10.1016/S1470-2045(22)00518-6
53. Yang H, Wang K, Wang T, Li M, Li B, Li S, et al. The combination options and predictive biomarkers of PD-1/PD-L1 inhibitors in esophageal cancer. Front Oncol (2020) 10:300. doi: 10.1016/S0140-6736(19)32591-7
54. Shapiro J, van Lanschot JJB, Hulshof M, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol (2015) 16:1090–8. doi: 10.1016/S1470-2045(22)00197-8
55. Kelly RJ, Zaidi AH, Smith MA, Omstead AN, Kosovec JE, Matsui D, et al. The dynamic and transient immune microenvironment in locally advanced esophageal adenocarcinoma post chemoradiation. Ann Surg (2018) 268:992–9. doi: 10.1200/JCO.19.01307
56. Li C, Zhao S, Zheng Y, Han Y, Chen X, Cheng Z, et al. Preoperative pembrolizumab combined with chemoradiotherapy for oesophageal squamous cell carcinoma (PALACE-1). Eur J Cancer (Oxford England: 1990) (2021) 144:232–41. doi: 10.1016/S0140-6736(20)32531-9
57. Shang X, Zhao G, Liang F, Zhang C, Zhang W, Liu L, et al. Safety and effectiveness of pembrolizumab combined with paclitaxel and cisplatin as neoadjuvant therapy followed by surgery for locally advanced resectable (stage III) esophageal squamous cell carcinoma: a study protocol for a prospective, single-arm, single-center, open-label, phase-II trial (Keystone-001). Ann Trans Med (2022) 10:229. doi: 10.1038/s41591-021-01444-0
58. Ma J, Zhang J, Yang Y, Zheng D, Wang X, Liang H, et al. Camrelizumab combined with paclitaxel and nedaplatin as neoadjuvant therapy for locally advanced esophageal squamous cell carcinoma (ESPRIT): A phase II, single-arm, exploratory research. J Clin Oncol (2021) 39:e16033–3. doi: 10.1200/JCO.2021.39.15_suppl.e16033
59. Chen X, Xu X, Wang D, Liu J, Sun J, Lu M, et al. Neoadjuvant sintilimab and chemotherapy in patients with potentially resectable esophageal squamous cell carcinoma (KEEP-G 03): an open-label, single-arm, phase 2 trial. J immunotherapy Cancer (2023) 11:e005830. doi: 10.1200/JCO.22.00727
60. Yan X, Duan H, Ni Y, Zhou Y, Wang X, Qi H, et al. Tislelizumab combined with chemotherapy as neoadjuvant therapy for surgically resectable esophageal cancer: A prospective, single-arm, phase II study (TD-NICE). Int J Surg (London England) (2022) 103:106680. doi: 10.1016/j.jtho.2021.07.015
61. Plagne R, Chollet P, Legros M, Cure H, Ferriere JP, Bignon YJ. [Adjuvant medical treatment]. La Rev du praticien (1990) 40:905–8. doi: 10.1016/S2352-3026(18)30192-3
62. Chen R, Zheng R, Zhou J, Li M, Shao D, Li X, et al. Risk prediction model for esophageal cancer among general population: A systematic review. Front Public Health (2021) 9:680967. doi: 10.1016/j.jtho.2021.11.018
63. Kelly RJ, Lockhart AC, Jonker DJ, Melichar B, Andre T, Chau I, et al. CheckMate 577: A randomized, double-blind, phase 3 study of nivolumab (Nivo) or placebo in patients (Pts) with resected lower esophageal (E) or gastroesophageal junction (GEJ) cancer. J Clin Oncol (2017) 35:TPS212–2. doi: 10.1016/S0140-6736(23)00961-3
64. Kelly RJ, Ajani JA, Kuzdzal J, Zander T, Cutsem EV, Piessen G, et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. New Engl J Med (2021) 384:1191–203.
65. Park SY, Kim HK, Jeon YJ, Lee J, Cho JH, Choi YS, et al. The role of adjuvant chemotherapy after neoadjuvant chemoradiotherapy followed by surgery in patients with esophageal squamous cell carcinoma. Cancer Res Treat (2023) 4:1231–9. doi: 10.1016/j.ccell.2023.04.014
66. Lin DC, Hao JJ, Nagata Y, Xu L, Shang L, Meng X, et al. Genomic and molecular characterization of esophageal squamous cell carcinoma. Nat Genet (2014) 46:467–73. doi: 10.1038/ng.3683
67. Hao JJ, Lin DC, Dinh HQ, Mayakonda A, Jiang YY, Chang C, et al. Spatial intratumoral heterogeneity and temporal clonal evolution in esophageal squamous cell carcinoma. Nat Genet (2016) 48:1500–7. doi: 10.1016/j.jtho.2023.09.027
68. Pilard C, Ancion M, Delvenne P, Jerusalem G, Hubert P, Herfs M. Cancer immunotherapy: it's time to better predict patients' response. Br J Cancer (2021) 125:927–38. doi: 10.1016/j.jtho.2021.05.005
69. Zhu S, Zhang T, Zheng L, Liu H, Song W, Liu D, et al. Combination strategies to maximize the benefits of cancer immunotherapy. J Hematol Oncol (2021) 14:156. doi: 10.1200/JCO.2023.41.4_suppl.286
70. Perez-Ruiz E, Melero I, Kopecka J, Sarmento-Ribeiro AB, Garcia-Aranda M, De Las Rivas J. Cancer immunotherapy resistance based on immune checkpoints inhibitors: Targets, biomarkers, and remedies. Drug resistance updates: Rev commentaries antimicrobial Anticancer chemotherapy (2020) 53:100718. doi: 10.1200/JCO.21.01308
71. Bhat AA, Goyal A, Thapa R, Almalki WH, Kazmi I, Alzarea SI, et al. Uncovering the complex role of interferon-gamma in suppressing type 2 immunity to cancer. Cytokine (2023) 171:156376. doi: 10.1016/j.cyto.2023.156376
72. Liu Z, Zhao Y, Kong P, Liu Y, Huang J, Xu E, et al. Integrated multi-omics profiling yields a clinically relevant molecular classification for esophageal squamous cell carcinoma. Cancer Cell (2023) 41:181–95. doi: 10.1016/j.ccell.2022.12.004
73. Jiang YY, Jiang Y, Li CQ, Zhang Y, Dakle P, Kaur H, et al. TP63, SOX2, and KLF5 establish a core regulatory circuitry that controls epigenetic and transcription patterns in esophageal squamous cell carcinoma cell lines. Gastroenterology (2020) 159:1311–27. doi: 10.1053/j.gastro.2020.06.050
74. Jiang YY, Lin DC, Mayakonda A, Hazawa M, Ding LW, Chien WW, et al. Targeting super-enhancer-associated oncogenes in oesophageal squamous cell carcinoma. Gut (2017) 66:1358–68. doi: 10.1136/gutjnl-2016-311818
Keywords: esophageal squamous cell carcinoma, immunotherapy, chemotherapy, immune checkpoint blockade, PD1/PD-L1
Citation: Wei DD, Fang JM, Wang HZ, Chen J, Kong S, Jiang Y-Y and Jiang Y (2024) Perioperative immunotherapy for esophageal squamous cell carcinoma. Front. Immunol. 15:1330785. doi: 10.3389/fimmu.2024.1330785
Received: 31 October 2023; Accepted: 31 January 2024;
Published: 19 February 2024.
Edited by:
Noel Donlon, Trinity College Dublin, IrelandReviewed by:
Jiaxiong Tan, Tianjin Medical University Cancer Institute and Hospital, ChinaCopyright © 2024 Wei, Fang, Wang, Chen, Kong, Jiang and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan-Yi Jiang, eXVueWlqQGNtcHQuYWMuY24=; Yuan Jiang, eXVhbmpAY21wdC5hYy5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.