
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 21 March 2024
Sec. Nutritional Immunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1329092
 Ryan M. Pace1,2*
Ryan M. Pace1,2* Elana A. King-Nakaoka3,4
Elana A. King-Nakaoka3,4 Andrew G. Morse3,4
Andrew G. Morse3,4 Kelsey J. Pascoe5Anna Winquist6Beatrice Caffé7Alexandra D. Navarrete8Kimberly A. Lackey1Christina D.W. Pace1
Kelsey J. Pascoe5Anna Winquist6Beatrice Caffé7Alexandra D. Navarrete8Kimberly A. Lackey1Christina D.W. Pace1 Bethaney D. Fehrenkamp1,3,4Caroline B. Smith7
Bethaney D. Fehrenkamp1,3,4Caroline B. Smith7 Melanie A. Martin9,10
Melanie A. Martin9,10 Celestina Barbosa-Leiker5
Celestina Barbosa-Leiker5 Sylvia H. Ley11
Sylvia H. Ley11 Mark A. McGuire12
Mark A. McGuire12 Courtney L. Meehan7
Courtney L. Meehan7 Janet E. Williams12
Janet E. Williams12 Michelle K. McGuire1*
Michelle K. McGuire1*Background: There is a paucity of data on the presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in feces of lactating women with coronavirus disease 2019 (COVID-19) and their breastfed infants as well as associations between fecal shedding and symptomatology.
Objective: We examined whether and to what extent SARS-CoV-2 is detectable in the feces of lactating women and their breastfed infants following maternal COVID-19 diagnosis.
Methods: This was a longitudinal study carried out from April 2020 to December 2021 involving 57 breastfeeding maternal-infant dyads: 33 dyads were enrolled within 7 d of maternal COVID-19 diagnosis, and 24 healthy dyads served as controls. Maternal/infant fecal samples were collected by participants, and surveys were administered via telephone over an 8-wk period. Feces were analyzed for SARS-CoV-2 RNA.
Results: Signs/symptoms related to ears, eyes, nose, and throat (EENT); general fatigue/malaise; and cardiopulmonary signs/symptoms were commonly reported among mothers with COVID-19. In infants of mothers with COVID-19, EENT, immunologic, and cardiopulmonary signs/symptoms were most common, but prevalence did not differ from that of infants of control mothers. SARS-CoV-2 RNA was detected in feces of 7 (25%) women with COVID-19 and 10 (30%) of their infants. Duration of fecal shedding ranged from 1-4 wk for both mothers and infants. SARS-CoV-2 RNA was sparsely detected in feces of healthy dyads, with only one mother’s and two infants’ fecal samples testing positive. There was no relationship between frequencies of maternal and infant SARS-CoV-2 fecal shedding (P=0.36), although presence of maternal or infant fever was related to increased likelihood (7-9 times greater, P≤0.04) of fecal shedding in infants of mothers with COVID-19.
During the initial phase of the coronavirus disease 2019 (COVID-19) pandemic the risk of maternal-to-child transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was cited as one of a battery of reasons why mother-infant separation was initially recommended following maternal COVID-19 diagnosis (1). In addition to respiratory transmission, several other modes were initially of concern including via breastfeeding and fecal-oral transmission (2–6). A large body of research quickly accumulated that did not support the proposition that human milk is a common vehicle for maternal-to-infant SARS-CoV-2 transmission and is instead a source of passive immunity for infants (7–16). However, less attention has been paid to the fecal-oral route of transmission in breastfeeding dyads.
Nearly 25% of COVID-19 patients manifest gastrointestinal (GI) signs/symptoms (e.g., diarrhea, nausea, vomiting), and the presence of SARS-CoV-2 in feces is a relatively common occurrence in individuals with COVID-19, with some studies observing viral shedding in as many as 40.5% of COVID-19 patients (6, 17–21). In addition, SARS-CoV-2 RNA has been detected in feces of pre-symptomatic and asymptomatic individuals (18). Although SARS-CoV-2 RNA concentrations in feces (an estimated 102-107 genome copies/mL) are several orders of magnitude lower than those of nasopharyngeal (NP) fluids (105-1011 genome copies/mL), there is evidence of viable, replication-competent, SARS-CoV-2 in fecal samples (20–24). Consequently, risk of SARS-CoV-2 transmission via the fecal-oral route is possible. It should be noted that while most of these data were obtained from adult patient populations, several infant case studies have been reported (25–36). The risk for maternal-to-child viral transmission in breastfeeding dyads may be higher than in other settings and situations as repeated close-contact interactions occur frequently between mothers and infants (37, 38). For example, Chen et al. (2020) reported on a family cluster with an asymptomatic female child (11 mo of age) who persistently tested negative via NP swab while also persistently shedding SARS-CoV-2 RNA in her feces for ≥100 d from the date of illness onset (26). In another study of three pediatric cases (1.5 to 6 yr of age), SARS-CoV-2 RNA was detectable in feces for 8 to 20 d after the children’s respiratory swabs first became negative (27). Although infants can be at risk for severe COVID-19, this remains an infrequent outcome (39, 40). Of note, whether any of the infants or older children were breastfed at the time of sampling was not indicated in any of these reports.
We previously reported on the lack of detection of SARS-CoV-2 in milk and the inconsistent detection in swabs of the nipple/areola as well as milk-borne and circulating anti-SARS-CoV-2 receptor binding domain (RBD) antibodies of lactating women with COVID-19 (10, 12, 41). In the study reported herein, we assessed the presence of SARS-CoV-2 RNA in feces collected from these women and their infants following the onset of maternal COVID-19 and in healthy controls for 8 wk. We also characterized associations between SARS-CoV-2 RNA presence in maternal and infant feces and signs and symptoms of COVID-19 in the maternal-infant dyads.
This multicenter prospective study was carried out from April 2020 to March 2021 using a repeated-measures, longitudinal design. Maternal-infant dyads were recruited locally through participating institutions (University of Idaho, Tulane University, University of Washington, and Washington State University) and through national social media and other forms of advertising. To participate, women had to be ≥18 yr of age, lactating, and have an infant younger than 24 mo. Two groups of maternal-infant dyads were recruited (1): those in which the mother was clinically tested/diagnosed with COVID-19 in the last seven days (“COVID-19 group,” n=33), and (2) those with no known prior COVID-19 infections or exposures and who reported no current COVID-19 symptoms (“healthy group,” n=24). One dyad from the COVID-19 group included two lactating parents who both provided milk to the infant. Due to the nature of conducting this research during a pandemic and because test results were often not available soon after testing, some participants were recruited after being tested but prior to receiving results for their COVID-19 tests. Participants receiving a negative COVID-19 result after enrollment were ineligible to participate in the study. Several participating mothers reported receiving a COVID-19 vaccination, including one participant (1 mo after enrollment) from the COVID-19 group and eight participants (n=3, initial vaccine administered on average 9 d prior to enrollment; n=5, initial vaccine administered on average 20 d after enrollment) from the healthy group.
Fecal samples were collected from each mother and child in the COVID-19 group and telephone surveys administered on three separate days during the first week following enrollment (1, 2-6, and 7 d) and again around 2, 3, 4, and 8 wk following enrollment. For the healthy group, fecal samples were collected from each mother and infant and telephone surveys administered on two separate days during the first week after enrollment and again around 3 and 8 wk after enrollment. Women self-collected fecal samples using provided collection kits (Fe-Col Faeces Collection Device, cat. FC2010, Alpha Laboratories; Faeces Collection Tube, cat. 80.734.00, Sarstedt), which were assembled aseptically by study personnel wearing masks, gowns, and gloves. Infant fecal samples were collected by participants using provided fecal collection containers and spatulas (Faeces Collection Tube, cat. 80.734.00, Sarstedt); 2-4 scoops of feces were obtained from either the infant’s diaper or skin. Participants were instructed by study personnel how to use aseptic technique to obtain samples, including the use of gloves and masks. Samples were then immediately frozen in the participant’s freezer. Samples were either shipped overnight from the subject’s home to the University of Idaho (UI) in a cooler containing frozen cold packs or picked up by local study personnel and transported (or overnight shipped on dry ice) back to UI and stored at -80°C. A total of 544 fecal samples (n=255 maternal, n=289 infant) were available for analyses (Supplementary Figure S1, Supplementary Table S1).
Telephone surveys were administered by trained study personnel using a set protocol and included questions about COVID-19 clinical testing results for all household members as well as maternal and infant signs/symptoms of any illnesses or ailments (e.g., congestion, cough, diarrhea, difficulty breathing, fatigue, fever, loss of smell and/or taste, or malaise).
This multi-institutional study was reviewed and approved by the institutional review boards of the University of Idaho (20-056, 20-060) and Tulane University (2020-602). All adult participants gave written informed consent for themselves and written assent for their infants.
Total RNA was extracted from fecal samples using the Quick-DNA/RNA Viral MagBead kit (cat. R2140, Zymo Research). Briefly, ~100 mg of wet feces were mixed with 1000 µL of 1X DNA/RNA Shield (Zymo Research) and incubated for 10 min prior to extraction. Samples were then centrifuged for 2 min at 12,000 x g at 4°C, and RNA extracted from 300 µL of the supernatant following the manufacturer’s instructions, including a DNase I digest to remove double-stranded DNA. For negative and positive controls, fecal samples collected from healthy participants were left unspiked or spiked with heat-inactivated SARS-CoV-2 (isolate USA-WA1/2020, cat. NR-52285, BEI Resources), respectively.
RNA isolated from fecal samples (including negative and positive controls) was used as the input for Quick SARS-CoV-2 multiplex reverse-transcription quantitative polymerase chain reaction (RT-qPCR) assay (cat. R3013, Zymo Research). All RT-qPCR reactions were performed in duplicate. The Quick SARS-CoV-2 multiplex assay detects target sequences of the SARS-CoV-2 nucleocapsid (N) gene and the human RNase P gene. This multiplex assay was based on the US Centers for Disease Control and Prevention (CDC) protocol (42), and samples with Ct values <40 for the SARS-CoV-2 N gene were considered positive. RT-qPCR was performed with the Applied Biosystems 7500 Fast Real-Time PCR system with run mode set to “fast 7500” and cycling parameters set to run for 15 min at 55°C; 10 min at 95°C; followed by 5 sec at 95°C, 30 sec at 72°C, and 30 sec at 57°C for 45 cycles. A 5-point standard curve of SARS-CoV-2 RNA (cat. R3016, Zymo Research) was used to estimate viral load (range 80 to 50,000 genomic copies per reaction).
R (v4.2.2) (43) and GraphPad Prism 9 (v9.3.1; GraphPad Software) were used for data analyses. The R package ggplot2 (v3.4.0) (44) was used for data projection. The exact binomial test was used to calculate confidence intervals. Mann-Whitney tests for continuous data and Fisher’s exact tests for categorical data were used to test for differences in group characteristics. Fisher’s exact test was used to examine differences in the frequency of maternal/infant symptoms between groups, and associations between the presence of SARS-CoV-2 RNA in maternal/infant feces based on the presence of maternal/infant signs/symptoms. For the co-lactating maternal-infant dyad, a composite score of maternal SARS-CoV-2 positivity and symptomatology was created when assessing any relationships with infant outcomes; in all other instances the mothers were analyzed independently. Values are given as median ± interquartile range (IQR), unless otherwise indicated. Statistical significance was declared at P<0.05.
A total of 57 maternal-infant dyads provided maternal and/or infant fecal samples, including 33 dyads in the COVID-19 group and 24 dyads in the healthy group (Table 1). There were no differences between the groups with respect to maternal age, race/ethnicity, parity, time postpartum, infant sex, or breastfeeding exclusivity. Median age of adult participants was 32 yr (interquartile range: 30-35 yr), and they identified predominantly as white and non-Hispanic (88%). Median parity was two children; median infant age was 27 wk at baseline; half the infants were female; and 31% were exclusively breastfeeding. Of note, 11 infants of mothers in the COVID-19 group were also tested for COVID-19 prior to study enrollment, and 45% (n=5) of these infants received a positive COVID-19 diagnosis (Table 1).
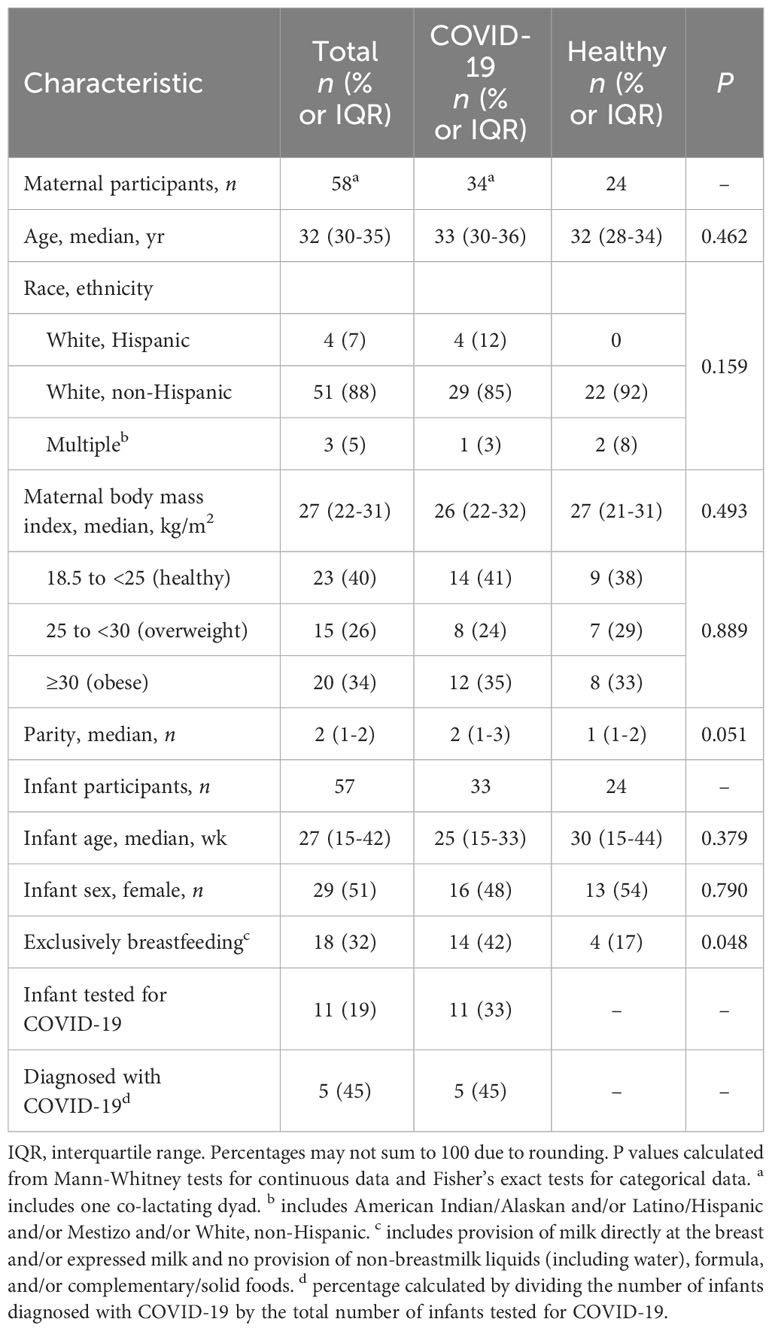
Table 1 Selected baseline characteristics of study participants in the COVID-19 and healthy groups.
The most commonly reported signs/symptoms among the women in the COVID-19 group included those associated with ears, eyes, nose, and throat (EENT; n=28; e.g., headache, loss of taste/smell, nasal congestion, sore throat); general symptoms (n=24; e.g., fatigue/malaise); and cardiopulmonary-related signs/symptoms (n=21; e.g., chest tightness, cough, difficulty breathing) (Figure 1). Compared to women in the healthy group, those in the COVID-19 group had higher frequency of signs/symptoms related to EENT (42 vs. 82%, P=0.002), general (17 vs. 71%, P<0.001), cardiopulmonary (4 vs. 62%, P<0.001), musculoskeletal (e.g., back pain, muscle/joint pain; 0 vs. 41%, P<0.001), and immunologic (e.g., chills, fever, sweating; 0 vs. 29%, P=0.003) variables (Figure 1B). There were no differences in the frequency of GI, breast, neurologic, dermatologic, endocrine, or genitourinary signs/symptoms between participants in the COVID-19 and healthy groups.
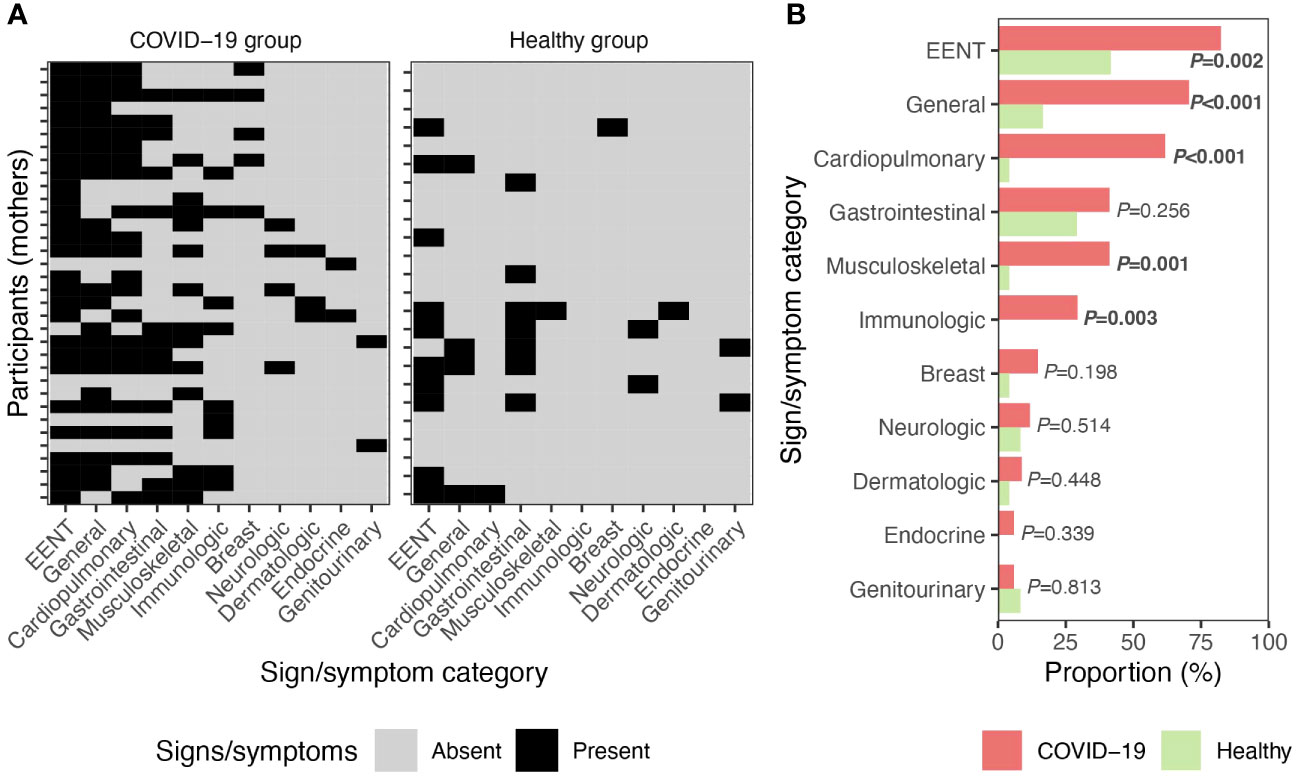
Figure 1 Signs/symptoms of illness in mothers. (A) Signs/symptoms reported by women in the COVID-19 (n=34) and healthy (n=24) groups. (B) Proportion of women diagnosed with COVID-19 (n=34) and self-reported healthy participants (n=24) with signs/symptoms. P values calculated with Fisher’s exact test. EENT, ears, eyes, nose, and throat.
In infants of mothers in the COVID-19 group, EENT, immunologic, and cardiopulmonary signs/symptoms were most common (Figure 2); however, rates of these signs/symptoms were similar to those reported for infants of mothers in the healthy group (Figures 2B). Compared to those in the healthy group, infants of mothers in the COVID-19 group had a higher frequency of immunologic symptoms (13 vs. 45%, P=0.008) (Figure 2B); this was solely attributed to fever.
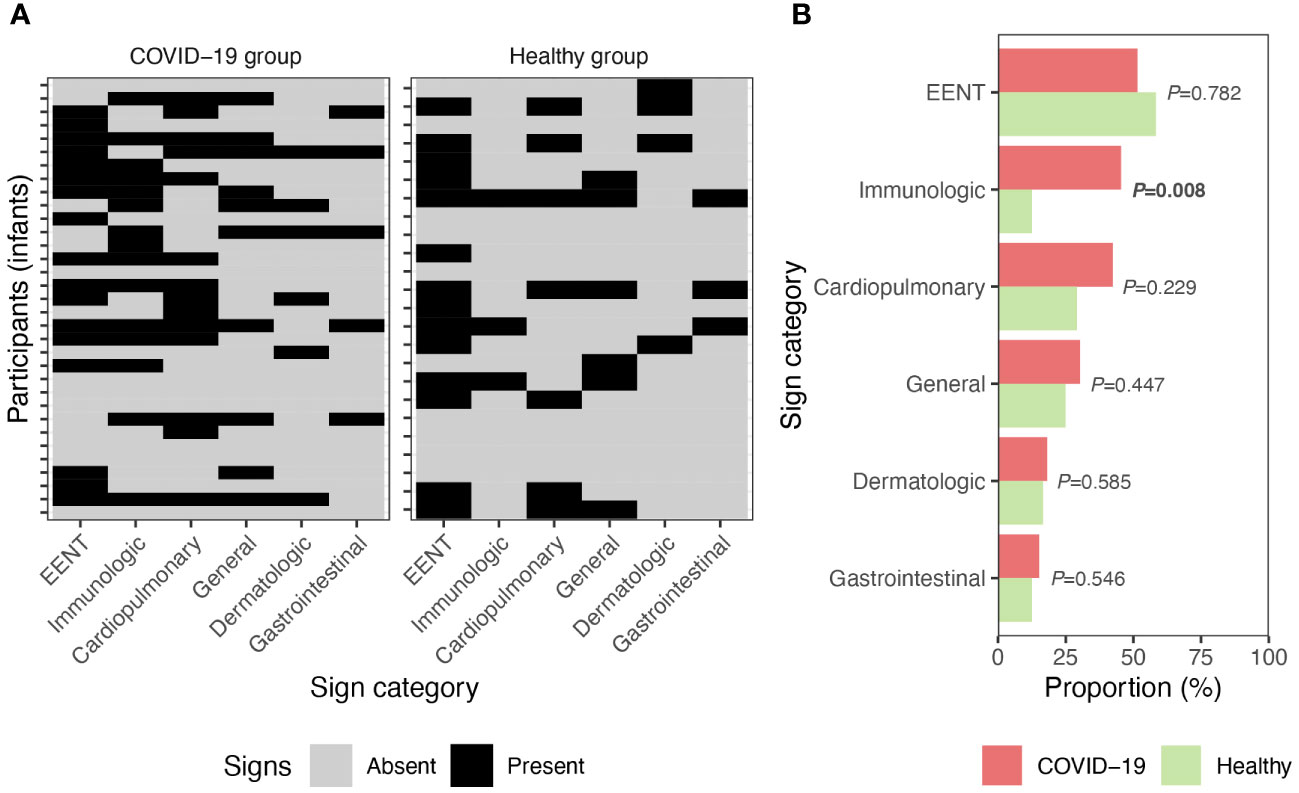
Figure 2 Signs of illness in infants. (A) Signs of illness reported by their parents for infants breastfed by women in the COVID-19 (n=33) and healthy (n=24) groups. (B) Proportion of signs present in infants within the COVID-19 and healthy groups. P values calculated with Fisher’s exact test. EENT, ears, eyes, nose, and throat.
A total of 28 (82.3%) women in the COVID-19 group provided fecal samples, which were collected 1-7 times over the 2-mo study period (Figure 3A; Supplementary Table S1, Supplementary Figure S1). SARS-CoV-2 RNA was detected in feces provided by seven (25%; 95% CI 10-45%) of these women. Five out of 19 (26%) fecal samples collected on the first day were positive for SARS-CoV-2 RNA, 6/21 (29%) at 2-6 d, 4/24 (17%) at 7 d, 3/25 (12%) at 2 wk, and 1/24 (4%) at 4 wk. SARS-CoV-2 RNA was detected in one sample collected from the 24 mothers in the healthy group who provided fecal samples. This sample was collected following enrollment on day 7 (Figure 3B).
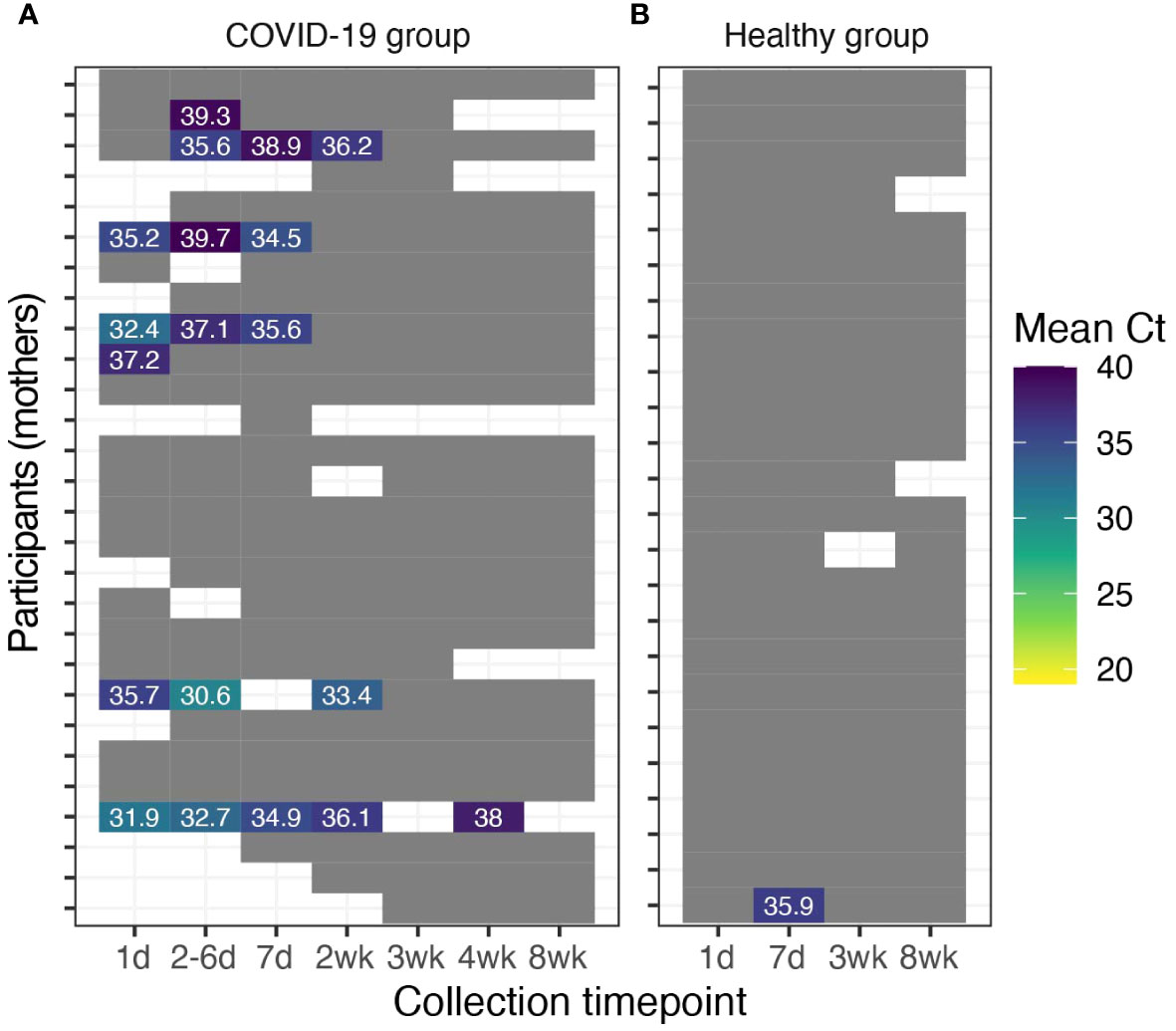
Figure 3 Detection of SARS-CoV-2 RNA in maternal fecal samples. Maternal fecal samples with detectable SARS-CoV-2 from participants (A) diagnosed with COVID-19 (n=28) and (B) healthy participants (n=24). Grey cells indicate fecal samples with no detectable SARS-CoV-2 RNA. White cells indicate uncollected/unavailable fecal samples.
Of the 33 infants of mothers in the COVID-19 group, 10 (30%, 95% CI 16-49%) had at least one sample that was positive for SARS-CoV-2 RNA (Figure 4A; Supplementary Table S1, Supplementary Figure S1). All 10 of these infants provided fecal samples out to 8 wk, at which time all were negative for SARS-CoV-2. In these infants fecal SARS-CoV-2 RNA shedding persisted for a duration ranging between 1 to 4 wks after enrollment. Specifically, 2 infants experienced viral RNA shedding for 1 wk, 1 infant for 2 wk, 5 infants for 3 wk, and 2 infants for 4 wk post-enrollment.
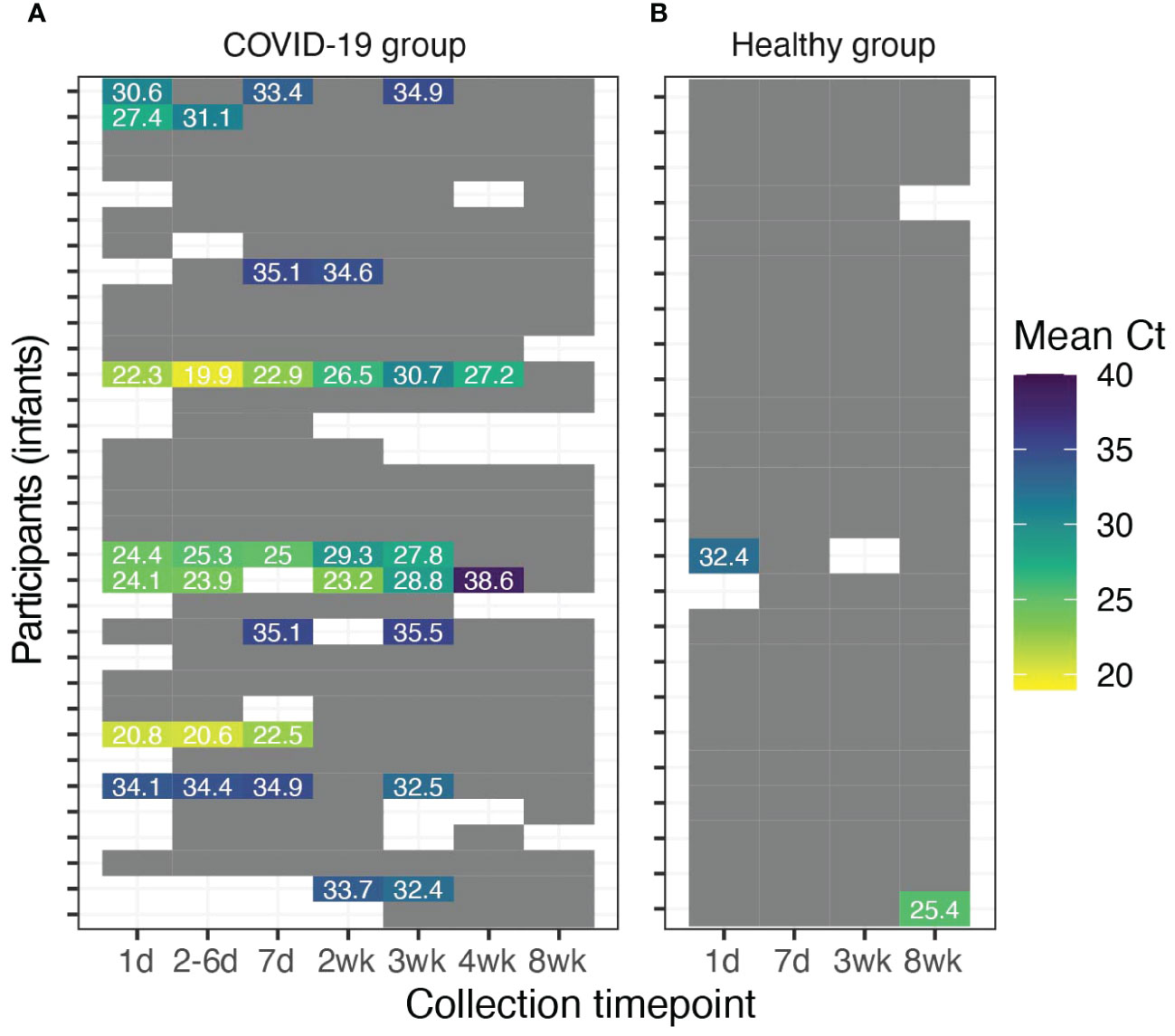
Figure 4 Detection of SARS-CoV-2 RNA in fecal samples of breastfed infants. Infant fecal samples with detectable SARS-CoV-2 RNA in (A) breastfed infants of mothers diagnosed with COVID-19 (n=33) and (B) breastfed infants of healthy mothers (n=24). Grey cells indicate fecal samples with no detectable SARS-CoV-2 RNA. White cells indicate uncollected/unavailable fecal samples.
Among the 24 infants of women in the healthy group, two had single fecal samples positive for SARS-CoV-2 RNA (Figure 4B). Feces collected from one of these infants contained SARS-CoV-2 in the first week following enrollment. In the other case, although the infant’s first three samples (wk 1-3) were negative, the sample collected at the final timepoint (wk 8) was positive.
Examination of SARS-CoV-2 positivity among the 27 maternal-infant dyads in the COVID-19 group that each provided at least one fecal sample revealed that 44% (n=12) of these dyads’ feces were negative for SARS-CoV-2 (Figure 5A). Only one dyads’ feces were simultaneously positive for SARS-CoV-2 (Figure 5C), and this only occurred once within the first week; all remaining samples thereafter testing negative. All other COVID-19 group dyads had discordant presence of SARS-CoV-2 in maternal and infant feces. In 22% (n=6) of dyads, the mother produced feces positive for SARS-CoV-2, whereas the infant did not. In the remaining 30% (n=8) of the dyads, the infants had feces containing SARS-CoV-2, whereas the mothers did not. Overall, there was no association between the presence of SARS-CoV-2 in maternal and infant feces in the COVID-19 group (P=0.36, Fisher’s exact test).
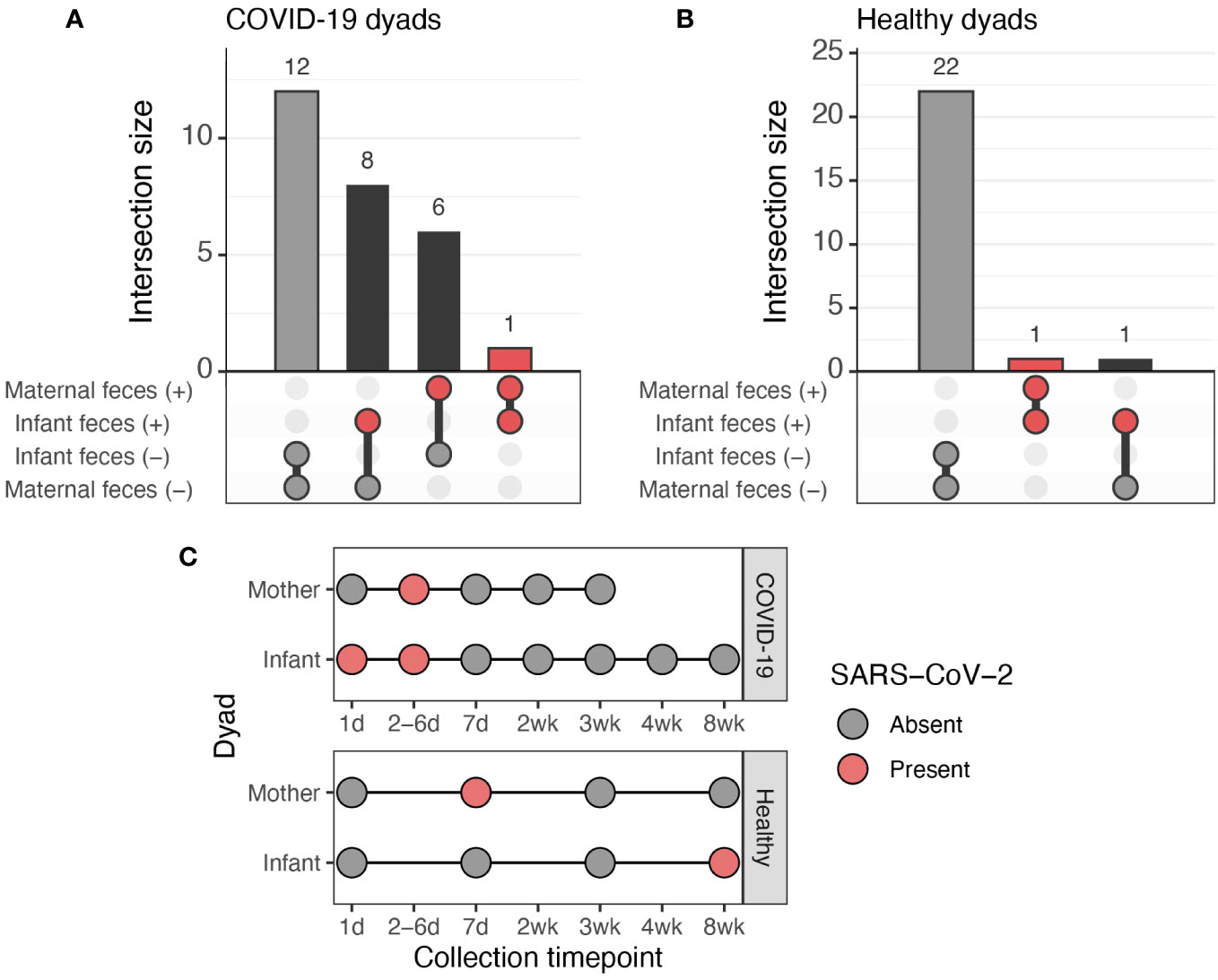
Figure 5 Co-occurrence of SARS-CoV-2 in feces of mothers and infants. (A) Upset plot of the 27 maternal-infant dyads in the COVID-19 group with paired fecal data. (B) Upset plot of the 24 maternal-infant dyads in the healthy group with paired fecal data. (C) Overview of fecal sampling and fecal SARS-CoV-2 results for the two dyads in which both the mother and infant had fecal samples positive for SARS-CoV-2.
Most (92%, n=22) of the 24 maternal-infant dyads in the healthy group provided fecal samples that were consistently negative for SARS-CoV-2 (Figure 5B). One dyad was discordant for the presence of SARS-CoV-2, with one positive sample from the infant (first sample collected, “1 d”) and all negative samples from the mother. The mother and infant in the remaining dyad each had at one fecal sample positive for SARS-CoV-2, with the infant’s being collected in wk 8 and the mother’s during wk 1 (Figure 5C).
We examined whether presence of maternal and/or infant signs/symptoms were related to the likelihood of SARS-CoV-2 positivity in fecal samples provided by mothers and their infants in the COVID-19. For mothers, there were no associations between the presence of EENT, general, cardiopulmonary, gastrointestinal musculoskeletal, or immunologic related signs/symptoms and presence of SARS-CoV-2 in their feces (Table 2). In contrast, the presence of immunologic symptoms in infants was associated with a 9-fold increased likelihood of SARS-CoV-2 in their feces (odds ratio [OR] 9.14 [95% CI 1.71-47.59], P=0.020; Table 2). Similarly, immunologic symptomology in the mother was associated with a 7-fold increased likelihood of SARS-CoV-2 in infant feces (OR 7.00, 95% CI 1.11-32.30; P=0.039; Table 2).
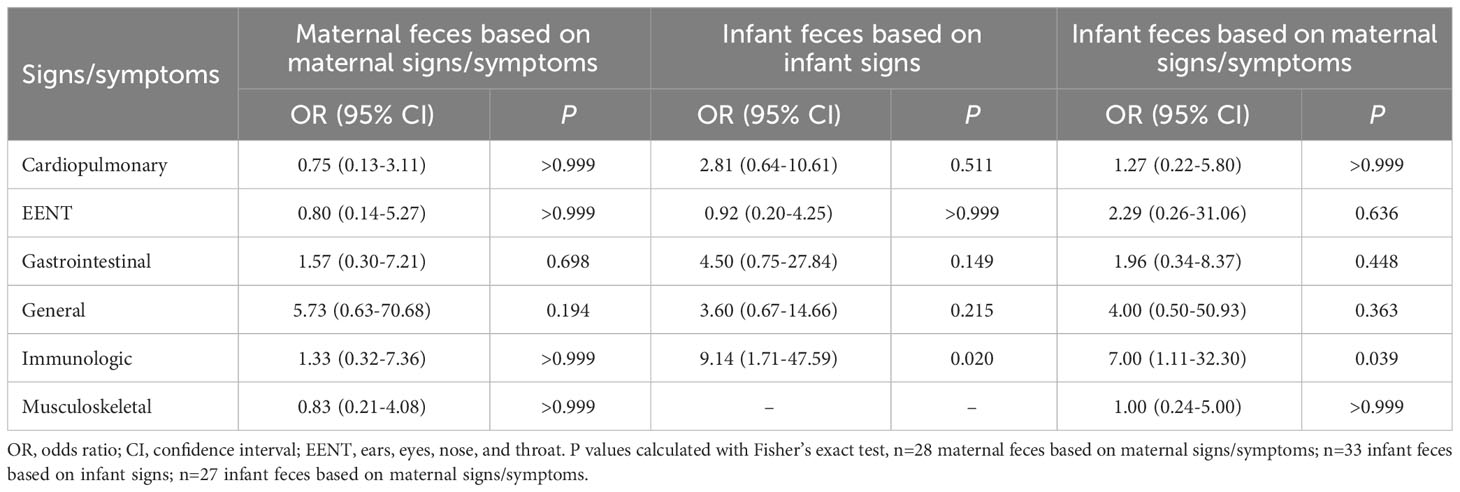
Table 2 Likelihood of SARS-CoV-2 detection in maternal/infant feces based on presence of maternal/infant signs/symptoms.
We assessed and characterized the frequency of SARS-CoV-2 fecal shedding and illness symptomatology across 57 breastfeeding maternal-infant dyads for 8 wk, including 33 dyads with sampling beginning within 7 d of maternal COVID-19 diagnosis (COVID-19 group) and 24 self-reported healthy dyads that served as controls (healthy group). Approximately 25% of women diagnosed with COVID-19 and their infants had detectable SARS-CoV-2 RNA in their feces (Figures 3, 4). Among individuals with SARS-CoV-2 RNA detected in their feces, mean Ct values increased over time (i.e., decreased concentration of SARS-CoV-2), and SARS-CoV-2 RNA was undetectable in all fecal samples tested at 8 wk post-diagnosis except for one infant from the healthy group. Interestingly, in many cases, when SARS-CoV-2 RNA was detected, Ct values in infant feces were lower than the Ct values observed in the maternal fecal samples indicating higher possible higher viral loads. Although we extracted RNA from similar fecal amounts, differences in wet/dry weights and output mass of infant and maternal fecal samples may partially explain some of these differences in Ct values.
Not surprisingly, several groups of symptoms were reported by mothers diagnosed with COVID-19 (Figure 1). Compared to healthy controls, women with COVID-19 reported higher rates of general symptoms (e.g., fatigue/malaise), EENT, and cardiopulmonary, musculoskeletal, and immunologic signs/symptoms. This is consistent with the broad literature that has demonstrated individuals, including lactating women, with COVID-19 display an array of signs/symptoms stereotypical of respiratory virus infections (10, 14, 45–49).
The infants whose mothers were diagnosed with COVID-19 had similar rates of illness signs/symptoms compared to infants of the healthy mothers (Figure 2). The lone exception to this was that, compared to infants with healthy mothers, infants whose mothers were in the COVID-19 group had a higher proportion of immunologic symptoms, which were solely attributed to fever.
Among mothers, despite wide reporting of signs/symptoms, we found no associations between the presence of signs/symptoms of illness, including gastrointestinal, and detection of SARS-CoV-2 RNA in feces (Table 2). In infants, both infant and maternal immunologic-related symptoms (i.e., fever) were related to the detection of SARS-CoV-2 RNA in feces (Table 2).
Finally, we found no relationship between presence of SARS-CoV-2 RNA in maternal and infant feces (Figure 5). Analysis of paired maternal-infant dyad fecal samples indicated that SARS-CoV-2 RNA was absent in 44% of dyads. Only two maternal-infant dyads produced feces that contained SARS-CoV-2 RNA, although only one of these dyads (from the COVID-19 group) produced fecal samples that were concurrently positive (Figure 5C).
Interestingly, although mothers in the healthy group reported having no known contact with COVID-19 cases, the detection of SARS-CoV-2 RNA in the feces of one mother and her infant, as well as that of an unrelated infant, suggests that exposure had likely occurred unknowingly. This is in line with prior data from our group (41) and others on the presence of circulating anti-SARS-CoV-2-spike antibodies in blood samples collected from apparently healthy individuals during the pandemic. We do note that for the dyad with concordant fecal shedding, the mother tested negative for circulating anti-SARS-CoV-2 antibodies at 14-, 30-, and 60-d post-enrollment (circulating anti-SARS-CoV-2 antibody data was not available for the infant; results published previously (41)). Thus, an alternative explanation for this dyad’s results is that they are false positives and/or the fecal samples became inadvertently contaminated at some point in time, although we strictly adhered to containment and decontamination protocols during sample processing and analyses to prevent this scenario.
It is also worth noting that the SARS-CoV-2 RNA that was detected in the infants’ feces is unlikely to have come from their mothers’ milk as we have previously demonstrated that milk samples collected from this group did not contain SARS-CoV-2 RNA. These infants were likely infected via other routes, for example respiratory transmission. Importantly, none of these mothers or infants were hospitalized, and overall infants of mothers with COVID-19 had similar rates of signs of illness compared to infants of healthy mothers, except for an increased proportion of fever.
Findings from prior studies have found evidence of prolonged GI SARS-CoV-2 infections in individuals with symptomatic and asymptomatic COVID-19 (50–52). In many cases, GI symptoms (e.g., abdominal pain, nausea, and vomiting) in individuals with symptomatic COVID-19 are associated with fecal shedding of SARS-CoV-2 RNA (51). Our finding of SARS-CoV-2 RNA in maternal and infant feces during maternal COVID-19 are consistent with these findings. Despite our results, we did not detect a difference in the proportion of GI-related symptomatology in women with COVID-19 or their breasted infants compared to healthy controls.
There are several limitations to the current work. The sample sizes of the COVID-19 and healthy groups were relatively small, and COVID-19 diagnostic testing and results for infants during the study period were limited. Additionally, as most participants were recruited in the week following maternal COVID-19 diagnosis (and thus SARS-CoV-2 infection) we may have missed fecal shedding of SARS-CoV-2 in the immediate period following the onset of infection. Fecal shedding of viral RNA may have also occurred at levels below the limit of detection using RT-qPCR, although data suggest high concordance between RT-qPCR and the much more sensitive method of droplet digital PCR (51). Further, sample preservation and incomplete removal of inhibitors in fecal specimens may have impacted our ability to detect viral RNA (53, 54). Consequently, the results on the prevalence of fecal shedding in breastfeeding dyads should be interpreted to represent a lower bound due to the above. We also lacked serial naso/oropharyngeal sampling and therefore were unable to relate the duration of respiratory SARS-CoV-2 shedding with that in feces. Finally, as with all nucleic acid-based assays (e.g., RT-qPCR, PCR, nucleic acid sequencing), we were unable to determine whether any viral RNA detected came from infectious SARS-CoV-2 virions. Strengths of this study included the longitudinal nature of the experimental design, capture of maternal and infant symptomology, and rigorous and standardized sample collection methodology across study sites.
In this study, we found that fecal shedding of SARS-CoV-2 was relatively common in breastfeeding dyads (≥25% of lactating mothers and breastfeeding infants, respectively) in the 8 wk following maternal COVID-19 diagnosis, although the concordance of fecal shedding within the maternal-infant dyads was less common (~4%). Fecal SARS-CoV-2 shedding in mothers was not associated with any signs/symptoms. In contrast, infant fecal shedding was only associated with fever. Importantly and interestingly, our results do not support a relationship between presence of maternal and infant SARS-CoV-2 fecal shedding and maternal/infant SARS-CoV-2 infection. Together, these data indicate that feces are not a likely vehicle for the transmission of SARS-CoV-2 in breastfeeding dyads.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the institutional review boards of the University of Idaho (20-056, 20-060) and Tulane University (2020-602). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
RP: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. EK: Formal analysis, Investigation, Writing – review & editing. AM: Formal analysis, Investigation, Writing – review & editing. KP: Formal analysis, Investigation, Writing – review & editing. AW: Formal analysis, Investigation, Writing – review & editing. BC: Formal analysis, Investigation, Writing – review & editing. AN: Formal analysis, Investigation, Writing – review & editing. KL: Formal analysis, Investigation, Writing – review & editing. CP: Formal analysis, Investigation, Writing – review & editing. BF: Formal analysis, Investigation, Writing – review & editing. CS: Data curation, Formal analysis, Investigation, Writing – review & editing. MMc: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. CB: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. SL: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. CM: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. JW: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. MAM: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Bill and Melinda Gates Foundation (INV-016943), the National Science Foundation (IOS-BIO 2031753, 2031715, 2031888, 2031761), US National Institutes of Health (NICHD R01HD092297), Washington State University Health Equity Research Center, USDA National Institute of Food and Agriculture (Hatch project IDA01643), and University of Washington Center for Studies in Demography and Ecology (P2C HD042828). In-kind support was provided by Medela and Milk Stork. The funding agencies had no role in the collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
We thank all the families who participated in this study and volunteered their time and effort. We also thank Alexandra Gogel, Jennell Johnson, Romana Hyde, Cassandra Partridge, and Victoria Wilk for help with collection kit assembly and/or shipping; Courtney Buchert, Taylor Dixon, Meghan Lewis, Brett Herrick, and Katlyn Scarrow for help with sample processing; and Josie Ash and Matt Newsom for data entry/management.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1329092/full#supplementary-material
1. Puopolo KM, Hudak ML, Kimberlin D, Cummings J. INITIAL GUIDANCE: Management of infants born to mothers with COVID-19. American Academy of Pediatrics Committee on Fetus and Newborn, Section on Neonatal Perinatal Medicine, and Committee on Infectious Diseases (2020). Available at: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/clinical-guidance/faqs-management-of-infants-born-to-covid-19-mothers/.
2. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. New Engl J Med. (2020) 382:1199–207. doi: 10.1056/nejmoa2001316
3. Groß R, Conzelmann C, Müller JA, Stenger S, Steinhart K, Kirchhoff F, et al. Detection of SARS-CoV-2 in human breastmilk. Lancet. (2020) 395:1757–8. doi: 10.1016/s0140-6736(20)31181-8
4. Lackey KA, Pace RM, Williams JE, Bode L, Donovan SM, Järvinen KM, et al. SARS-CoV-2 and human milk: What is the evidence? Matern Child Nutr. (2020) 16:e13032. doi: 10.1111/mcn.13032
5. Xu Y, Li X, Zhu B, Liang H, Fang C, Gong Y, et al. Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding. Nat Med. (2020) 395:1–4. doi: 10.1038/s41591-020-0817-4
6. Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. (2020) 323:1843–4. doi: 10.1001/jama.2020.3786
7. Chambers C, Krogstad P, Bertrand K, Contreras D, Tobin NH, Bode L, et al. Evaluation for SARS-CoV-2 in breast milk from 18 infected women. JAMA. (2020) 324:1347–8. doi: 10.1001/jama.2020.15580
8. Peng S, Zhu H, Yang L, Cao L, Huang X, Dynes M, et al. A study of breastfeeding practices, SARS-CoV-2 and its antibodies in the breast milk of mothers confirmed with COVID-19. Lancet Reg Health West Pac. (2020) 4:100045. doi: 10.1016/j.lanwpc.2020.100045
9. Martenot A, Labbassi I, Delfils-Stern A, Monroy O, Langlet C, Pichault-Klein V, et al. Favorable outcomes among neonates not separated from their symptomatic SARS-CoV-2-infected mothers. Pediatr Res. (2021) 90:8–11. doi: 10.1038/s41390-020-01226-3
10. Pace RM, Williams JE, Järvinen KM, Belfort MB, Pace CDW, Lackey KA, et al. Characterization of SARS-CoV-2 RNA, antibodies, and neutralizing capacity in milk produced by women with COVID-19. Mbio. (2021) 12:e03192–20. doi: 10.1128/mbio.03192-20
11. Yan J, Guo J, Fan C, Juan J, Yu X, Li J, et al. Coronavirus disease 2019 in pregnant women: a report based on 116 cases. Am J Obstet Gynecol. (2020) 223:111.e1–111.e14. doi: 10.1016/j.ajog.2020.04.014
12. Pace RM, Williams JE, Järvinen KM, Meehan CL, Martin MA, Ley SH, et al. Milk From women diagnosed with COVID-19 does not contain SARS-CoV-2 RNA but has persistent levels of SARS-CoV-2-specific IgA antibodies. Front Immunol. (2021) 12:801797. doi: 10.3389/fimmu.2021.801797
13. Bäuerl C, Randazzo W, Sánchez G, Selma-Royo M, Verdevio EG, Martínez L, et al. SARS-CoV-2 RNA and antibody detection in breast milk from a prospective multicentre study in Spain. Arch Dis Child - Fetal Neonatal Ed. (2022) 107:216–21. doi: 10.1136/archdischild-2021-322463
14. Krogstad P, Contreras D, Ng H, Tobin N, Chambers CD, Bertrand K, et al. No infectious SARS-CoV-2 in breast milk from a cohort of 110 lactating women. Pediatr Res. (2022) 92:1140–5. doi: 10.1038/s41390-021-01902-y
15. Sahin D, Tanacan A, Erol SA, Anuk AT, Eyi EGY, Erdinc ASO, et al. A pandemic center’s experience of managing pregnant women with COVID-19 infection in Turkey: A prospective cohort study. Int J Gynecol Obstet. (2020) 151:74–82. doi: 10.1002/ijgo.13318
16. Young BE, Seppo AE, Diaz N, Rosen-Carole C, Nowak-Wegrzyn A, Vasquez JMC, et al. Association of Human Milk Antibody Induction, Persistence, and Neutralizing Capacity With SARS-CoV-2 Infection vs mRNA Vaccination. JAMA Pediatr. (2022) 176:159–68. doi: 10.1001/jamapediatrics.2021.4897
17. Parasa S, Desai M, Chandrasekar VT, Patel HK, Kennedy KF, Roesch T, et al. Prevalence of gastrointestinal symptoms and fecal viral shedding in patients with coronavirus disease 2019. JAMA Netw Open. (2020) 3:e2011335. doi: 10.1001/jamanetworkopen.2020.11335
18. Jones DL, Baluja MQ, Graham DW, Corbishley A, McDonald JE, Malham SK, et al. Shedding of SARS-CoV-2 in feces and urine and its potential role in person-to-person transmission and the environment-based spread of COVID-19. Sci Total Environ. (2020) 749:141364. doi: 10.1016/j.scitotenv.2020.141364
19. Wu Y, Guo C, Tang L, Hong Z, Zhou J, Dong X, et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol Hepatol. (2020) 5:434–5. doi: 10.1016/s2468-1253(20)30083-2
20. Xiao F, Sun J, Xu Y, Li F, Huang X, Li H, et al. Infectious SARS-CoV-2 in feces of patient with severe COVID-19. Emerg Infect Dis. (2020) 26:1920–2. doi: 10.3201/eid2608.200681
21. Zhang Y, Chen C, Zhu S, Shu C, Wang D, Song J, et al. Isolation of 2019-nCoV from a stool specimen of a laboratory-confirmed case of the coronavirus disease 2019 (COVID-19). China Cdc Wkly. (2020) 2:123–4. doi: 10.46234/ccdcw2020.033
22. vanDoorn AS, Meijer B, Frampton CMA, Barclay ML, Boer NKH. Systematic review with meta-analysis: SARS-CoV-2 stool testing and the potential for faecal-oral transmission. Aliment Pharm Therap. (2020) 52:1276–88. doi: 10.1111/apt.16036
23. Qian Q, Fan L, Liu W, Li J, Yue J, Wang M, et al. Direct evidence of active SARS-CoV-2 replication in the intestine. Clin Infect Dis. (2020) 73:ciaa925–. doi: 10.1093/cid/ciaa925
24. Jeong HW, Kim S-M, Kim H-S, Kim Y-I, Kim JH, Cho JY, et al. Viable SARS-CoV-2 in various specimens from COVID-19 patients. Clin Microbiol Infect. (2020) 26:1520–4. doi: 10.1016/j.cmi.2020.07.020
25. Cho S-M, Ha GY. A case of COVID-19 in a 45-day-old infant with persistent fecal virus shedding for more than 12 weeks. Yonsei Med J. (2020) 61:901–3. doi: 10.3349/ymj.2020.61.10.901
26. Chen S, Si J, Tang W, Zhang A, Pan L, An M, et al. An asymptomatic SARS-CoV-2-infected infant with persistent fecal viral RNA shedding in a family cluster: A rare case report. Front Med. (2020) 7:562875. doi: 10.3389/fmed.2020.562875
27. Xing Y-H, Ni W, Wu Q, Li W-J, Li G-J, Wang W-D, et al. Prolonged viral shedding in feces of pediatric patients with coronavirus disease 2019. J Microbiol Immunol Infect. (2020) 53:473–80. doi: 10.1016/j.jmii.2020.03.021
28. Donà D, Minotti C, Costenaro P, Dalt LD, Giaquinto C. Fecal-oral transmission of SARS-CoV-2 in children. Pediatr Infect Dis J. (2020) 39:e133–4. doi: 10.1097/inf.0000000000002704
29. Slaats MALJ, Versteylen M, Gast KB, Munnink BBO, Pas SD, Bentvelsen RG, et al. Case report of a neonate with high viral SARSCoV-2 loads and long-term virus shedding. J Infect Public Health. (2020) 13(12):1878–84. doi: 10.1016/j.jiph.2020.10.013
30. Han MS, Seong M-W, Heo EY, Park JH, Kim N, Shin S, et al. Sequential analysis of viral load in a neonate and her mother infected with SARS-CoV-2. Clin Infect Dis. (2020) 35:e124. doi: 10.1093/cid/ciaa447
31. Holm-Jacobsen JN, Vonasek JH, Hagstrøm S, Donneborg ML, Sørensen S. Prolonged rectal shedding of SARS-CoV-2 in a 22-day-old-neonate: a case report. BMC Pediatr. (2021) 21:506. doi: 10.1186/s12887-021-02976-7
32. Hariharan SV, Muthusamy S, Asokan SK. Persistent viral shedding after SARS-CoV-2 infection in an infant with severe combined immunodeficiency. Indian J Pediatr. (2022) 89:94–4. doi: 10.1007/s12098-021-03935-x
33. Kam K-Q, Yung CF, Cui L, Pin RLT, Mak TM, Maiwald M, et al. A well infant with coronavirus disease 2019 (COVID-19) with high viral load. Clin Infect Dis. (2020) 361:1701. doi: 10.1093/cid/ciaa201
34. Tang A, Tong Z, Wang H, Dai Y, Li K, Liu J, et al. Detection of novel coronavirus by RT-PCR in stool specimen from asymptomatic child, China. Emerg Infect Dis. (2020) 26:1337–9. doi: 10.3201/eid2606.200301
35. Fan Q, Pan Y, Wu Q, Liu S, Song X, Xie Z, et al. Anal swab findings in an infant with COVID-19. Pediatr Investig. (2020) 4:48–50. doi: 10.1002/ped4.12186
36. Li J, Feng J, Liu T, Xu F, Song G. An infant with a mild SARS-CoV-2 infection detected only by anal swabs: A case report. Braz J Infect Dis. (2020) 24:247–9. doi: 10.1016/j.bjid.2020.04.009
37. Ozella L, Gesualdo F, Tizzoni M, Rizzo C, Pandolfi E, Campagna I, et al. Close encounters between infants and household members measured through wearable proximity sensors. PloS One. (2018) 13:e0198733. doi: 10.1371/journal.pone.0198733
38. Tscherning C, Sizun J, Kuhn P. Promoting attachment between parents and neonates despite the COVID-19 pandemic. Acta Paediatr. (2020) 109:1937–43. doi: 10.1111/apa.15455
39. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiology of COVID-19 among children in China. Pediatrics. (2020) 145:e20200702. doi: 10.1542/peds.2020-0702
40. Liguoro I, Pilotto C, Bonanni M, Ferrari ME, Pusiol A, Nocerino A, et al. SARS-COV-2 infection in children and newborns: a systematic review. Eur J Pediatr. (2020) 179:1029–46. doi: 10.1007/s00431-020-03684-7
41. Martin MA, Keith M, Pace RM, Williams JE, Ley SH, Barbosa-Leiker C, et al. SARS-CoV-2 specific antibody trajectories in mothers and infants over two months following maternal infection. Front Immunol. (2022) 13:1015002. doi: 10.3389/fimmu.2022.1015002
42. Lu X, Wang L, Sakthivel SK, Whitaker B, Murray J, Kamili S, et al. US CDC real-time reverse transcription PCR panel for detection of severe acute respiratory syndrome coronavirus 2. Emerging Infect Dis. (2020) 26:1654–65. doi: 10.3201/eid2608.201246
43. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Available at: https://www.R-project.org/.
44. Wickham H. ggplot2: Elegant graphics for data analysis. Germany: Springer (2009). doi: 10.1007/978-0-387-98141-3
45. Kim G-u, Kim M-J, Ra SH, Lee J, Bae S, Jung J, et al. Clinical characteristics of asymptomatic and symptomatic patients with mild COVID-19. Clin Microbiol Infect. (2020) 26:948.e1–3. doi: 10.1016/j.cmi.2020.04.040
46. Han C, Duan C, Zhang S, Spiegel B, Shi H, Wang W, et al. Digestive symptoms in COVID-19 patients with mild disease severity: Clinical presentation, stool viral RNA testing, and outcomes. Am J Gastroenterol. (2020) 115(6):916–23. doi: 10.14309/ajg.0000000000000664
47. Mizrahi B, Shilo S, Rossman H, Kalkstein N, Marcus K, Barer Y, et al. Longitudinal symptom dynamics of COVID-19 infection. Nat Commun. (2020) 11:6208. doi: 10.1038/s41467-020-20053-y
48. Kashif A, Chaudhry M, Fayyaz T, Abdullah M, Malik A, Anwer JMA, et al. Follow-up of COVID-19 recovered patients with mild disease. Sci Rep. (2021) 11:13414. doi: 10.1038/s41598-021-92717-8
49. Narayanaswamy V, Pentecost B, Alfandari D, Chin E, Minor K, Kastrinakis A, et al. Humoral and cell-mediated immune response in colostrum from women diagnosed positive for SARS-CoV-2. Breastfeed Med. (2021) 16(12):987–84. doi: 10.1089/bfm.2021.0082
50. Park S, Lee C-W, Park D-I, Woo H-Y, Cheong HS, Shin HC, et al. Detection of SARS-coV-2 in fecal samples from patients with asymptomatic and mild COVID-19 in Korea. Clin Gastroenterol Hepatol. (2021) 19:1387–1394.e2. doi: 10.1016/j.cgh.2020.06.005
51. Natarajan A, Zlitni S, Brooks EF, Vance SE, Dahlen A, Hedlin H, et al. Gastrointestinal symptoms and fecal shedding of SARS-CoV-2 RNA suggest prolonged gastrointestinal infection. Med New York N Y. (2022) 3(6):371–387.e9. doi: 10.1016/j.medj.2022.04.001
52. Cerrada-Romero C, Berastegui-Cabrera J, Camacho-Martínez P, Goikoetxea-Aguirre J, Pérez-Palacios P, Santibáñez S, et al. Excretion and viability of SARS-CoV-2 in feces and its association with the clinical outcome of COVID-19. Sci Rep. (2022) 12:7397. doi: 10.1038/s41598-022-11439-7
53. Schrader C, Schielke A, Ellerbroek L, Johne R. PCR inhibitors - occurrence, properties and removal. J Appl Microbiol. (2012) 113:1014–26. doi: 10.1111/jam.2012.113.issue-5
Keywords: breastfeeding, COVID-19, feces, lactation, maternal-infant health, SARS-CoV-2, symptoms, viral shedding
Citation: Pace RM, King-Nakaoka EA, Morse AG, Pascoe KJ, Winquist A, Caffé B, Navarrete AD, Lackey KA, Pace CDW, Fehrenkamp BD, Smith CB, Martin MA, Barbosa-Leiker C, Ley SH, McGuire MA, Meehan CL, Williams JE and McGuire MK (2024) Prevalence and duration of SARS-CoV-2 fecal shedding in breastfeeding dyads following maternal COVID-19 diagnosis. Front. Immunol. 15:1329092. doi: 10.3389/fimmu.2024.1329092
Received: 27 October 2023; Accepted: 08 March 2024;
Published: 21 March 2024.
Edited by:
Weicheng Hu, Yangzhou University, ChinaReviewed by:
Yarden Golan, University of California, San Francisco, United StatesCopyright © 2024 Pace, King-Nakaoka, Morse, Pascoe, Winquist, Caffé, Navarrete, Lackey, Pace, Fehrenkamp, Smith, Martin, Barbosa-Leiker, Ley, McGuire, Meehan, Williams and McGuire. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ryan M. Pace, cm1wYWNlQHVzZi5lZHU=; Michelle K. McGuire, c21jZ3VpcmVAdWlkYWhvLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.