 Wenqi Geng
Wenqi Geng Shangzhu Zhang
Shangzhu Zhang Jinya Cao
Jinya Cao Xia Hong
Xia Hong Yanping Duan
Yanping Duan Yinan Jiang
Yinan Jiang Jing Wei
Jing Wei
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 21 March 2024
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1323209
This article is part of the Research Topic Immune system disorders: from molecular mechanisms to clinical implications View all 28 articles
Introduction: Early detection of neuropsychiatric systemic lupus erythematosus (NPSLE) remains a challenge in clinical settings. Previous studies have found different autoantibodies as markers for NPSLE. This study aimed to describe the distribution of psychiatric syndromes in a group of patients with systemic lupus erythematosus (SLE) and to investigate the association between psychiatric syndromes and specific autoantibodies.
Methods: This retrospective study was conducted at a single medical center in China. We reviewed medical records of hospitalized patients with SLE who were consulted by psychiatrists due to potential mental disorders. Results of serum autoantibodies and general laboratory tests were collected. The correlation between clinical variables was examined. Binary logistic regression analyses were used to determine factors related to NPSLE and different psychiatric diagnoses.
Results: Among the 171 psychiatric manifestations in 160 patients, 141 (82.4%) were attributed to SLE. Acute confusional state (ACS) had the highest prevalence (57.4%). Anti-cardiolipin (ACL) antibody (X2 = 142.261, p < 0.001) and anti-β2 glycoprotein I (-β2GP1) antibody (X2 = 139.818, p < 0.001) varied significantly between groups, with the highest positive rate found in patients with mood disorders (27.3% and 18.2%). SLE disease activity index – 2000 (SLEDAI-2K) score excluding item ACS and item psychosis was a predictor of NPSLE (OR 1.172 [95% CI 1.105 - 1.243]).
Conclusions: Disease activity reflected by SLEDAI-2K score is a predictor for NPSLE. Antiphospholipid antibodies are associated with mood disorders in SLE. Further separate investigation of neuropsychiatric disorders is needed in order to better comprehend NPSLE’s pathological mechanism.
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease that affects multiple organs or systems, characterized by excessive production of pathogenic autoantibodies (autoabs) against a range of autoantigens (1). Neuropsychiatric lupus (NPSLE) refers to SLE involving the nervous system, including 19 clinical syndromes such as epilepsy, psychosis, and acute confusional state, which are divided into two categories: central nervous system involvement and peripheral nervous system involvement (1). Due to the variety of clinical manifestations from mild to severe, early detection of NPSLE remains a challenge in clinical settings and frequently necessitates multidisciplinary collaboration (2, 3). As a sign of critical illness, NPSLE also predicts an increase in disability and mortality (2, 4). Hence, it is important to identify the risk of neuropsychiatric (NP) involvement in the early stages of the disease in order to achieve an optimal outcome.
The attribution of neuropsychiatric manifestations has been a major challenge in clinical settings, possibly due to the unelucidated etiopathogenesis of NPSLE. This complexity is also mirrored in the study outcomes, as the prevalence of NPSLE drastically span from 14% to 95% (5). Based on the American College of Rheumatology (ACR) Nomenclature of 19 NPSLE syndromes (6), Ainiala et al. distinguished between minor and major manifestations (7). Later attribution models also took into account chronological association of NP symptoms and SLE, in addition to confounding factors, such as the attribution model proposed by the Italian Study Group (8). Until this day, clinical diagnosis remains the gold standard for NPSLE.
Psychiatric syndromes in SLE include acute confusional state (ACS), anxiety disorders, cognitive dysfunction (CD), mood disorders, and psychosis, among which ACS and psychosis are considered of the most diagnostic or “organic” significance of NPSLE (6, 9), or major manifestations by Ainiala et al. (7). Anxiety disorders, mood disorders, and CD are common in patients with SLE, but their contributing factors are more complex. For instance, anxiety disorders and mood disorders may be related to psychosocial factors, while CD may be secondary to cerebrovascular disease (2, 10).
Vasculopathy, autoabs-mediated tissue and neuronal damage, inflammatory mediators, blood-brain barrier (BBB) dysfunction, and others are some of the suggested pathogenetic mechanisms for NPSLE (10, 11). Ho et al. proposed that autoabs such as anti-ribosomal P protein (-ribP) antibodies (abs), and anti-phospholipid (APL) abs may point to more “organic” causes, while patients with negative autoabs, and no positive results from head MRI and EEG results, point to “functional” causes. They also found that among 19 NP syndromes, the positivity of APL abs (serum anti-cardiolipin (ACL) abs, lupus anticoagulants (LA), anti-β2GP1) and anti-ribP abs were specifically significantly associated with the manifestations of mood disorder, psychosis, ACS, and CD (12). NP involvement might be aided by serum anti-Smith (-Sm) abs permeating BBB in patients with NPSLE (13, 14). Similar to the widely varying prevalence of NPSLE, biomarkers including autoabs varied from study to study, possibly as a result of different diagnostic criteria for NPSLE (15, 16).
The purpose of this study was to describe the distribution of psychiatric syndromes in patients with SLE and to investigate the association between psychiatric syndromes and specific autoabs and general laboratory results.
We conducted this single-center retrospective cross-sectional study at Peking Union Medical College Hospital (PUMCH), a tertiary general hospital in Beijing, China. A review of the medical records of patients hospitalized at PUMCH between April 2013 and July 2020 was conducted by combining the efforts of both the Departments of Rheumatology and Clinical Immunology and Psychological Medicine.
The inclusion criteria of this study were: (a) Diagnosed as SLE by treating rheumatologists according to the 2012 Systemic Lupus Collaborating Clinics classification criteria for SLE (17); (b) Received psychiatric consultations due to potential mental disorders. Exclusion criteria were: (a) Comorbidity of other rheumatic diseases; (b) Incomplete information on psychiatric consultations or diagnoses. Psychiatric diagnoses were established through a full consideration of history, findings in mental status examination, and investigations. The diagnostic criteria for psychiatric syndromes in SLE, including ACS, psychosis, anxiety disorder, and mood disorder, were established upon the integration of the International Classification of Diseases Tenth Edition (ICD-10) (18) and the 1999 ACR NPSLE nomenclature (6). CD in NPSLE typically necessitates neuropsychological tests, such as the ACR neuropsychological battery for SLE. The standard procedure of mental status examination executed by consulting psychiatrists at PUMCH include general assessment of cognitive function, normally including tests of attention, memory, executive function and motor performance, verbal function and language skills, and concept formation and reasoning. Should the patient demonstrate dysfunction in a single domain, it is classified as mild CD. Should the patient exhibit cognitive decline in 2-3 domains, it is recognized as moderate CD. If the patient demonstrates impairments in 4-5 domains, it equates to severe CD. In this study, we defined CD related to SLE as the subject exhibiting impairment in at least two of the five cognitive domains.
The attribution of each patient’s psychiatric syndromes was determined by the attending rheumatologist, viewed as the gold standard. The primary basis for diagnosis and differential diagnosis is ACR Nomenclature for NPSLE (6) and EULAR recommendations for the management of SLE with neuropsychiatric manifestations (19). The information typically considered encompasses historical recollection, characteristics of symptoms, laboratory results, autoimmune antibodies, radiological and EEG observations, confounding factors that necessitate exclusion, and opinion from psychiatric consultation.
The study was conducted in accordance with the Helsinki Declaration of the World Medical Association. The design of the study was reviewed and approved by the Ethics Committee of PUMCH, and informed consent was waived due to observational/non-interventional design.
General demographic information, medical features such as SLE disease activity index – 2000 (SLEDAI-2K) scores (20), psychiatric diagnoses, and usage of glucocorticoids (GC) and immunosuppressants (IS) were collected from medical records. Results of the following tests were also collected: complete hemogram, C3 and C4 levels, serum immunoglobulin (Ig), cerebrospinal fluid (CSF) analyses, anti-double stranded DNA (-dsDNA) abs, anti-Sm abs, anti-ribP abs, and the APL abs (LA, anti-β2 glycoprotein I (-β2GP1) abs, ACL abs). All abs were tested by enzyme-linked immunosorbent assay, and range of values to be considered negative were shown in Supplementary Material 1. Results of head MRI were also collected.
All statistical analyses were performed using IBM SPSS Statistics 21.0.0.0. (IBM Corp., Armonk, NY, USA). Categorical variables are described as frequencies (percentages). Quantitative variables are described as mean ± standard deviation or median (interquartile range [IQR]) based on the normality of distribution. Fisher’s 1-way ANOVA and Bonferroni correction or the Kruskal–Wallis test were used for among-group comparisons of continuous normally and non-normally distributed variables, respectively. The Chi-square test or Fisher’s exact test was used for among-group comparisons of categorical variables. The correlation between clinical variables and psychiatric diagnoses was examined using Spearman’s correlation test. Subsequently, binary logistic regression analyses were used to determine factors related to NPSLE and different psychiatric diagnoses, with age and gender incorporated into the model. A two-tailed p value < 0.05 was considered statistically significant.
A total of 160 patients with SLE were included. Demographic information, clinical characteristics, and laboratory data of participants are summarized in Table 1; Supplementary Material 2. There were 145 women (90.6%), with a median age of 28 (IQR 23 - 39), and a median course of disease of 1.5 years (IQR 0.3 - 6). Seventy-five percentage of patients manifested multi-organ or -system involvement. The mean SLEDAI-2K score was 20.2 (SD 8.2). One hundred and forty-eight patients (92.5%) were diagnosed with at least one psychiatric condition. Of the 171 psychiatric manifestations, 141 (82.4%) were attributed to SLE. The highest to lowest prevalence was observed in ACS (81, 57.4%), CD (35, 24.8%), psychosis (14, 9.9%), and mood disorder (11, 7.8%), respectively.
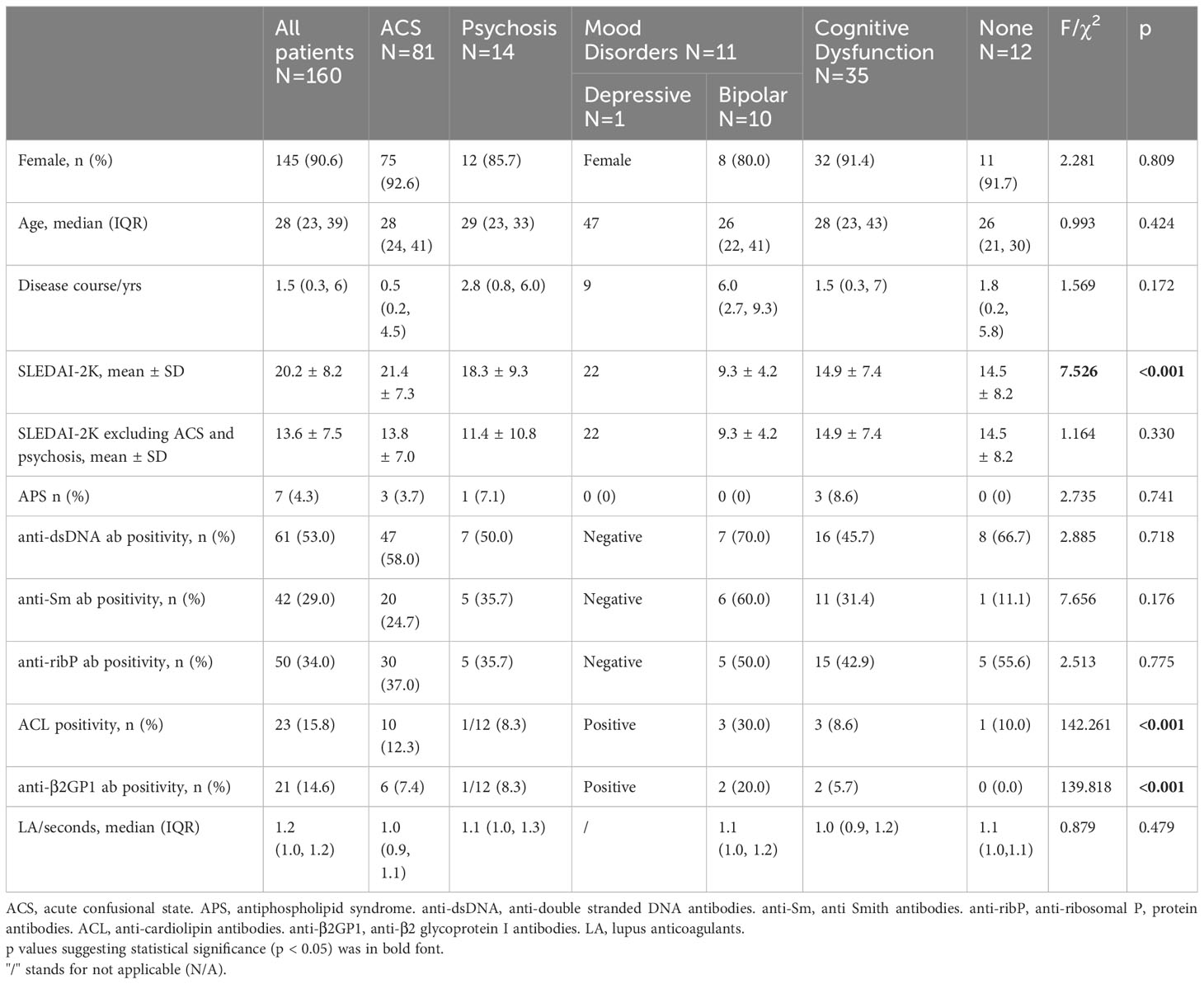
Table 1 Intergroup comparisons of clinical features and autoantibodies.
Compared between groups, there were no significant differences in sex ratio, age, age of onset, or course of disease. Tables 1, 2 depict that the mean SLEDAI-2K score demonstrated a significant variance amongst diagnostic groups (F = 7.526, p < 0.001). Removal of items pertaining to ACS and psychosis, revealed no significant differences in the remainder of the SLEDAI-2K score between groups (F = 1.164, P = 0.330). Patients presenting with bipolar disorder secondary to SLE displayed the lowest mean SLEDAI-2K score of 9.3 ± 4.2. Seven patients (4.3%) were diagnosed concurrently with antiphospholipid syndrome (APS). Three patients experienced ACS, three presented with CD, and one exhibited psychosis.
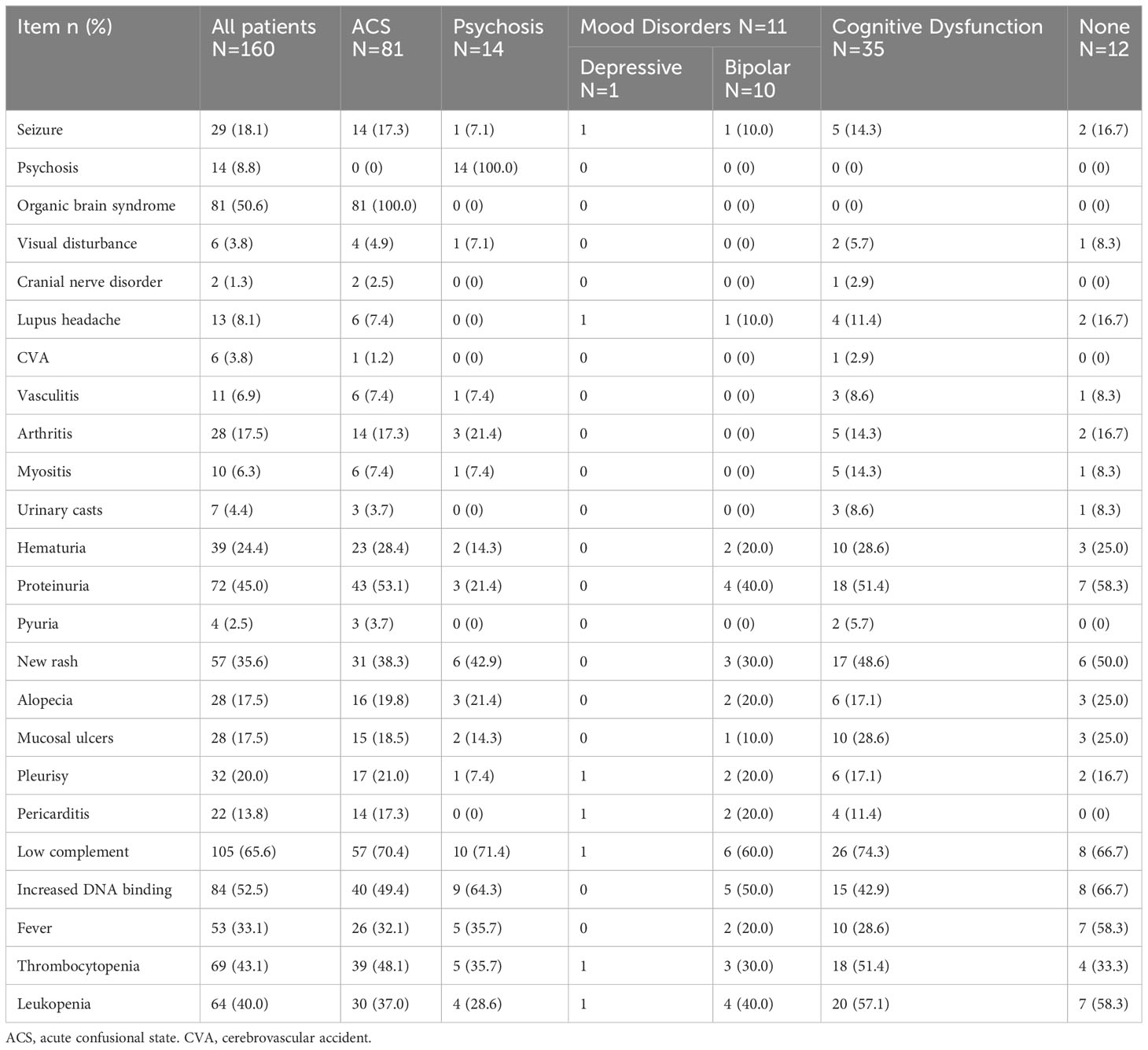
Table 2 SLEDAI-2K results.
All patients were prescribed GC as standardized therapy, and cortisol pulse therapy was implemented in 89 patients (55.6%). The most to least frequently administered IS were cyclophosphamide (66.3%), hydroxychloroquine (61.3%), mycophenolate mofetil (18.1%), tacrolimus (8.8%), cyclosporine A (4.4%), belimumab (1.9%), leflunomide (1.9%), and thalidomide (1.9%).
In relation to specific autoantibodies in various diagnostic cohorts, more patients carried positive ACL and anti-β2GP1 abs in the group of mood disorders (36.4% and 27.3). No notable differences in the positivity rates of anti-dsDNA abs, anti-Sm abs, and anti-ribP abs existed across groups. Additionally, there was no significant difference in hemoglobin, white blood cell count, platelet, plasma Igs, C3, C4, LA, and CSF analyses among diagnostic groups (Supplementary Material 2).
Of the 132 patients who underwent head MRI, abnormal results were noted in 85 patients (64.4%). These included 14 presenting with ischemic lesions, 37 with inflammatory lesions, 5 exhibiting both ischemic and inflammatory lesions, and 29 demonstrating other abnormalities. Notably, the findings of head MRI outcomes did not significantly differ across patients with disparate psychiatric diagnoses, as indicated in Table 3. Of the seven patients with secondary APS, four had ischemic lesions, two demonstrated both ischemic and inflammatory lesions, while the remaining patient did not undergo MRI.
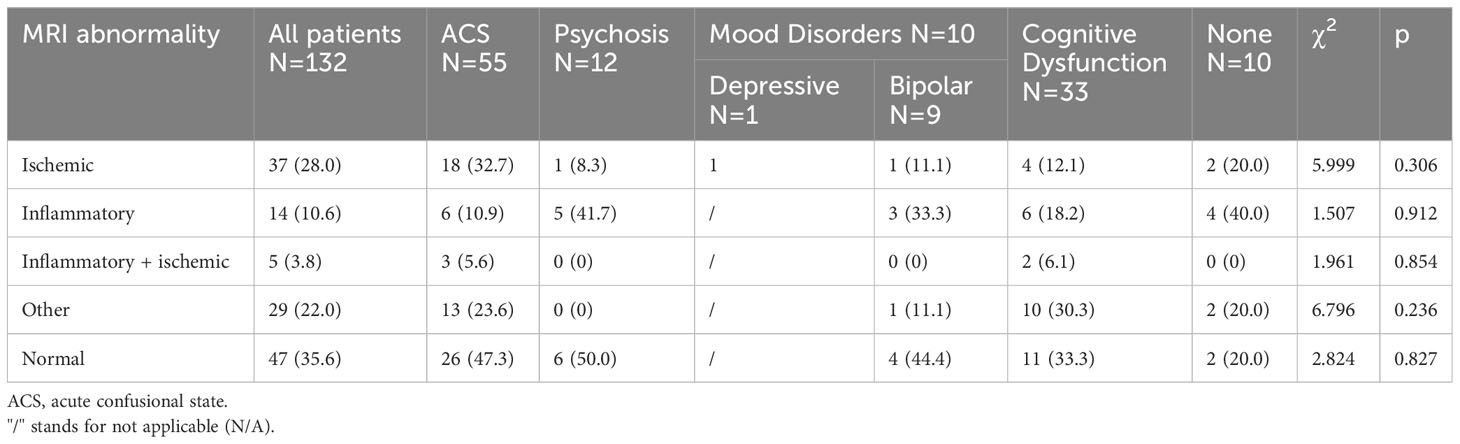
Table 3 Intergroup comparisons of head MRI results.
Correlation analysis revealed that bipolar disorder exhibited a weak correlation with the SLEDAI-2K score excluding the ACS and psychosis item (r=-0.167, p=0.039), course of disease (r=0.170, p=0.035), and anti-Sm ab (r=0.185, p=0.023). Psychosis demonstrated a weak correlation with hemoglobin (r=0.187, p=0.020). ACS and CD were not significantly correlated with any clinical features presented. The SLEDAI-2K score excluding the ACS and psychosis item demonstrated a moderate correlation with NPSLE (r=0.421, p<0.001). Binary logistic regression revealed that the SLEDAI-2K score excluding the ACS and psychosis item was a predictor of NPSLE (OR 1.172 [95% CI 1.105 - 1.243]). With the available data, we did not identify distinct indicators for each specific psychiatric syndrome.
In this research, we analyzed the correlation between clinical variables and NPSLE, concentrating predominantly on psychiatric disorders. Identifying biomarkers associated with the manifestation of diverse syndromes may foster comprehension of the pathogenesis of NPSLE. Psychiatric disorders in SLE, as secondary psychiatric disorders, suggest involvement of the CNS. Comparable to primary mental disorders, whilst there may be common pathological mechanisms among diverse types of syndromes, such as those of NPSLE, it should likewise exist distinct pathological mechanisms, such as those exclusive to psychosis. Presently, a definitive “gold standard” is lacking, and previous endeavors to delineate biomarkers for NPSLE have yielded conflicting results (21). Differences in diagnostic criteria and the absence of standardized reporting may be two possible explanations (15, 22). For instance, from a psychiatric perspective, mood disorders are two types of mental disorders of diverse nature, as both depressive and bipolar disorders consist of several subtypes. Consequently, markedly heterogeneous conclusions are likely to emerge from various studies concerning mood disorders in SLE. Moreover, the exploration of the genesis of primary psychiatric disorders necessitates consideration of the influence of social and psychological factors. Regrettably, in the majority of research pertaining to NPSLE, inclusive of this study, psychometric evaluation data have been omitted or incomplete (5). This deficiency should be rectified in subsequent investigations.
Our study demonstrated that the SLEDAI-2K score exhibits distinctions in disease activity among patients with varied psychiatric syndromes. As ACS and mental disorders are constituents of the SLEDAI-2K score, the SLEDAI-2K global score of patients experiencing ACS or psychosis may surpass other patients who do not fulfill these two classifications. Following the exclusion of these two items, it was determined that there exists no notable disparity in disease activity amongst different diagnostic cohorts. Moreover, there weren’t noteworthy intergroup discrepancies in the majority of investigations, potentially due to the minimal sample size within certain subgroups. The correlation between the SLEDAI-2K score and NPSLE is predictable, as NPSLE is often a sign of critical illness (4). Upon our attempt to remove the ACS and psychosis items, it was evident that the remaining SLEDAI-2K score retained its capability of predicting NPSLE, providing evidence for a strong correlation between disease activity and the manifestation of psychiatric symptoms in SLE patients.
Thus far, research has focused on the association of autoabs with NP conditions in SLE (4). Anti-dsDNA ab, one of the hallmark markers of SLE, is associated with overall disease activity and renal involvement. However, its correlation with neuropsychiatric manifestations was not remarkable (23). Research on anti-Sm ab, another diagnostic marker of SLE, revealed a significant increase in anti-Sm ab in patients with ACS compared to those with focal NPSLE and the fact that it plays a significant role in disrupting BBB in NPSLE (13, 14). Despite the controversy surrounding the conclusion, anti-ribP ab has become known as a highly specific biomarker for the diagnosis of SLE and is frequently associated with NPSLE (24). The presence of positive anti-ribP antibodies at baseline was associated with a greater proportion of neurological involvement (adjusted HR = 3.8, 95% CI 2.7-57) and cumulative neuropsychiatric damage during follow-up in our colleagues’ recent study, which focused on NPSLE (25). In a recent cross-sectional study by Chessa et al., anti-ribP serum level was independently associated with depressive symptoms (26). In our present study, however, the aforementioned abs did not differ significantly between psychiatric diagnostic groups. Hanly et al. discovered that impairment in BBB function is an important contributor to cognitive dysfunction, regardless of circulating SLE-related autoantibodies (27). The correlation between autoantibodies and NPSLE may comprise other mediating factors, necessitating future investigation.
The presence of APL abs is commonly associated with thrombosis (28). In NPSLE, APL ab-mediated thrombosis is considered the etiology of cerebrovascular disease and a possible mechanism for CD (21, 29). Owing primarily to the limited number of patients exhibiting APS in our research, no discernible difference was detected in the prevalence of APS across distinct psychiatric diagnoses. Nonetheless, we did discover that ACL and anti-β2GP1 ab were more frequently observed in patients with mood disorders, a finding consistent with some prior studies. In a previous meta-analysis, anti-β2GP1 ab was found to be significantly associated with mood disorders (OR=6.27 [95% CI, 1.22-32.12]) (12). According to findings from a study focusing on perinatal women with APS, even after pregnancy, women with pure obstetric APS are at increased risk of venous and arterial thrombosis over time, and they also appear to develop more mood disorders (30). Early theoretical models postulated that mood disorders are due to malfunctioning of several neurotransmitters, while recent research has uncovered more neurobiological mechanisms, including vascular dysfunction (31, 32). Phenomena of cerebral hypoperfusion were observed in both depressive and bipolar disorders (33, 34). In order to better elucidate the pathological mechanism of APL abs in mood disorders in SLE, it is important to investigate depressive and bipolar disorders separately in future studies with larger sample sizes.
The main strength of our study lies in that we focused on psychiatric syndrome of patients with SLE, which maximizes the accuracy of diagnoses. Meanwhile, several limitations should not be overlooked. First, as a result of the small sample size of each diagnostic group, certain intergroup differences in autoabs and clinical features may not be fully reflected. Second, the study was conducted at a single medical center in Beijing, China, which may limit the generalizability of the results. Third, due to the retrospective design, data on some clinical confounding factors may have been missed. Validation of these findings requires large-scale prospective multi-center studies, as well as more in-depth research to elucidate the pathological mechanisms underlying NPSLE.
Disease activity reflected by SLEDAI-2K score is a predictor for NPSLE. Antiphospholipid antibodies are associated with mood disorders in SLE. A detailed exploration of neuropsychiatric disorders, ideally inclusive of psychosocial evaluations, is imperative to elaborate on the pathogenic mechanism of NPSLE.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics committee of Peking Union Medical College Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because of observational/non-interventional design.
WG: Writing – review & editing, Writing – original draft, Data curation. SZ: Writing – review & editing, Writing – original draft, Methodology. JC: Writing – review & editing, Writing – original draft, Validation, Supervision, Conceptualization. XH: Writing – review & editing, Supervision. YD: Writing – review & editing. YJ: Writing – review & editing, Project administration, Methodology. JW: Writing – review & editing, Supervision, Funding acquisition.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-B-093), the STI2030-Major Projects (2021ZD0202001), and the Capital Funds for Health Improvement and Research (2022-2-4012).
The authors would like to thank colleagues in the Department of Rheumatology and Clinical Immunology for their diligent work and participation in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1323209/full#supplementary-material
1. Hanly JG, Urowitz MB, Gordon C, Bae SC, Romero-Diaz J, Sanchez-Geurrero J, et al. Neuropsychiatric events in systemic lupus erythematosus: a longitudinal analysis of outcomes in an international inception cohort using a multistate model approach. Ann Rheum Dis. (2020) 79:356–62. doi: 10.1136/annrheumdis-2019-216150. doi:10.1002/1529-0131(199904)42:4<599::AID-ANR2>3.0.CO;2-F.
2. Govoni M, Bortoluzzi A, Padovan M, Silvagni E, Borrelli M, Donelli F, et al. The diagnosis and clinical management of the neuropsychiatric manifestations of lupus. J Autoimmun. (2016) 74:41–72. doi: 10.1016/j.jaut.2016.06.013
3. Hanly JG. Diagnosis and management of neuropsychiatric SLE. Nat Rev Rheumatol. (2014) 10:338–47. doi: 10.1038/nrrheum.2014.15
4. Bertsias GK, Boumpas DT. Pathogenesis, diagnosis and management of neuropsychiatric SLE manifestations. Nat Rev Rheumatol. (2010) 6:358–67. doi: 10.1038/nrrheum.2010.62
5. Carrión-Barberà I, Salman-Monte TC, Vílchez-Oya F, Monfort J. Neuropsychiatric involvement in systemic lupus erythematosus: A review. Autoimmun Rev. (2021) 20:102780. doi: 10.1016/j.autrev.2021.102780
6. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. (1999) 42:599–608. doi: 10.1002/(ISSN)1529-0131
7. Ainiala H, Loukkola J, Peltola J, Korpela M, Hietaharju A. The prevalence of neuropsychiatric syndromes in systemic lupus erythematosus. Neurology. (2001) 57:496–500. doi: 10.1212/wnl.57.3.496
8. Bortoluzzi A, Fanouriakis A, Appenzeller S, Costallat L, Scire CA, Murphy E, et al. Validity of the Italian algorithm for the attribution of neuropsychiatric events in systemic lupus erythematosus: a retrospective multicentre international diagnostic cohort study. BMJ Open. (2017) 7:e15546. doi: 10.1136/bmjopen-2016-015546
9. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 european league against rheumatism/american college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol (Hoboken N.J.). (2019) 71:1400–12. doi: 10.1002/art.40930
10. Schwartz N, Stock AD, Putterman C. Neuropsychiatric lupus: new mechanistic insights and future treatment directions. Nat Rev Rheumatol. (2019) 15:137–52. doi: 10.1038/s41584-018-0156-8
11. Magro-Checa C, Zirkzee EJ, Huizinga TW, Steup-Beekman GM. Management of neuropsychiatric systemic lupus erythematosus: current approaches and future perspectives. Drugs. (2016) 76:459–83. doi: 10.1007/s40265-015-0534-3
12. Ho RC, Thiaghu C, Ong H, Lu Y, Ho CS, Tam WW, et al. A meta-analysis of serum and cerebrospinal fluid autoantibodies in neuropsychiatric systemic lupus erythematosus. Autoimmun Rev. (2016) 15:124–38. doi: 10.1016/j.autrev.2015.10.003
13. Hasegawa Y, Arinuma Y, Muramatsu T, Kondou J, Matsueda Y, Kanayama Y, et al. The pathogenic role of lupus-specific autoantibodies and Interleukin-6 on demyelination of the brainstem and spinal cord in systemic lupus erythematosus. Lupus. (2023) 32:401–10. doi: 10.1177/09612033231151600
14. Hirohata S, Sakuma Y, Matsueda Y, Arinuma Y, Yanagida T. Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus. Clin Exp Rheumatol. (2018) 36:1003–7.
15. Borowoy AM, Pope JE, Silverman E, Fortin PR, Pineau C, Smith CD, et al. Neuropsychiatric lupus: the prevalence and autoantibody associations depend on the definition: results from the 1000 faces of lupus cohort. Semin Arthritis rheumatism. (2012) 42:179–85. doi: 10.1016/j.semarthrit.2012.03.011
16. Cocco C, Manca E, Corda G, Angioni MM, Noli B, Congia M, et al. Brainreactive autoantibodies in neuropsychiatric systemic lupus erythematosus. Front Immunol. (2023) 14:1157149. doi: 10.3389/fimmu.2023.1157149
17. Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2012) 64:2677–86. doi: 10.1002/art.34473
18. World Health Organization(WHO). The ICD-10 classification of mental and behavioural disorders. Genève, Switzerland: World Health Organization (1993).
19. Bertsias GK, Ioannidis JP, Aringer M, Bollen E, Bombardieri S, Bruce IN, et al. EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs. Ann Rheum Dis. (2010) 69:2074–82. doi: 10.1136/ard.2010.130476
20. Gladman DD, Ibañez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29:288–91.
21. Hélène Jeltsch-David SM. Neuropsychiatric systemic lupus erythematosus pathogenesis and biomarkers. Nat Rev Neurol. (2014). 10(10):579–596. doi: 10.1038/nrneurol.2014.148
22. Vivaldo JF, de Amorim JC, Julio PR, de Oliveira RJ, Appenzeller S. Definition of NPSLE: does the ACR nomenclature still hold? Front Med (Lausanne). (2018) 5:138. doi: 10.3389/fmed.2018.00138
23. Yuan F, Wei F, Huang H, Xue Y, Guo P, You Y. The predictive value of autoantibody spectrum on organ damage in patients with systemic lupus erythematosus. Arch Rheumatol. (2018) 34:157–65. doi: 10.5606/ArchRheumatol.2019.6981
24. Mahler M, Kessenbrock K, Szmyrka M, Takasaki Y, Garcia-De La Torre I, Shoenfeld Y, et al. International multicenter evaluation of autoantibodies to ribosomal P proteins. Clin Vaccine Immunol CVI. (2006) . 13:77–83. doi: 10.1128/CVI.13.1.77-83.2006
25. Ding Y, Zhao J, Qian J, Zhang L, Zhang S, Jiang N, et al. The role of anti-ribosomal P autoantibodies in the prediction of neuropsychiatric damage in systemic lupus erythematosus based on CSTAR cohort (XIV). Clin Rheumatol. (2022) 41:1371–9. doi: 10.1007/s10067-021-06034-6
26. Chessa E, Piga M, Perra A, Pintus E, Porcu M, Serafini C, et al. The effect of anti-P ribosomal and anti-NR2 antibodies on depression and cognitive processes in SLE: an integrated clinical and functional MRI study. Lupus Sci Med. (2023). 10(2):e001005 doi: 10.1136/lupus-2023-001005
27. Hanly JG, Legge A, Kamintsky L, Friedman A, Hashmi JA, Beyea SD, et al. Role of autoantibodies and blood-brain barrier leakage in cognitive impairment in systemic lupus erythematosus. Lupus Sci Med. (2022) 9:e000668. doi: 10.1136/lupus-2022-000668
28. Cervera R, Serrano R, Pons-Estel GJ, Ceberio-Hualde L, Shoenfeld Y, de Ramón E, et al. Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. (2015) 74:1011–8. doi: 10.1136/annrheumdis-2013-204838
29. Murray SG, Yazdany J, Kaiser R, Criswell LA, Trupin L, Yelin EH, et al. Cardiovascular disease and cognitive dysfunction in systemic lupus erythematosus. Arthritis Care Res (Hoboken). (2012) 64:1328–33. doi: 10.1002/acr.21691
30. Gris JC, Guillotin F, Chéa M, Bourguignon C, Nouvellon É, Bouvier S. Antiphospholipid antibodies in pregnancy: maternal and neonatal implications. Semin Thromb Hemost. (2023) 49:337–47. doi: 10.1055/s-0042-1756193
31. Schneider MR, DelBello MP, McNamara RK, Strakowski SM, Adler CM. Neuroprogression in bipolar disorder. Bipolar Disord. (2012) 14:356–74. doi: 10.1111/j.1399-5618.2012.01024.x
32. aan het Rot M, Mathew SJ, Charney DS. Neurobiological mechanisms in major depressive disorder. CMAJ. (2009) 180:305–13. doi: 10.1503/cmaj.080697
33. Taylor WD, Aizenstein HJ, Alexopoulos GS. The vascular depression hypothesis: mechanisms linking vascular disease with depression. Mol Psychiatry. (2013) 18:963–74. doi: 10.1038/mp.2013.20
Keywords: systemic lupus erythematosus, neuropsychiatric systemic lupus erythematosus, mental disorders, biomarkers, referral consultation
Citation: Geng W, Zhang S, Cao J, Hong X, Duan Y, Jiang Y and Wei J (2024) Predictive factors of psychiatric syndrome in patients with systemic lupus erythematosus. Front. Immunol. 15:1323209. doi: 10.3389/fimmu.2024.1323209
Received: 17 October 2023; Accepted: 11 March 2024;
Published: 21 March 2024.
Edited by:
Ruben Dario Motrich, National Scientific and Technical Research Council (CONICET), ArgentinaReviewed by:
Natasa Stanisavljevic, University Hospital Medical Center Bezanijska kosa, SerbiaCopyright © 2024 Geng, Zhang, Cao, Hong, Duan, Jiang and Wei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinya Cao, Y2FvamlueWFAcHVtY2guY24=; Jing Wei, d2VpamluZ0BwdW1jaC5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.