 Eva Frison1,2
Eva Frison1,2 Maxime Breban
Maxime Breban Félicie Costantino
Félicie Costantino- 1UMR1173, INSERM, UFR Simone Veil, Versailles-Saint-Quentin-Paris-Saclay University, Saint-Quentin-en-Yvelines, France
- 2Labex Inflamex, Paris Diderot Sorbonne Paris-Cité University, Paris, France
- 3Rheumatology Division, Ambroise Paré Hospital, Assistance Publique des Hôpitaux de Paris (AP-HP), Boulogne-Billancourt, France
Spondyloarthritis (SpA) is characterized by a strong genetic predisposition evidenced by the identification of up to 50 susceptibility loci, in addition to HLA-B27, the major genetic factor associated with the disease. These loci have not only deepened our understanding of disease pathogenesis but also offer the potential to improve disease management. Diagnostic delay is a major issue in SpA. HLA-B27 testing is widely used as diagnostic biomarker in SpA but its predictive value is limited. Several attempts have been made to develop more sophisticated polygenic risk score (PRS). However, these scores currently offer very little improvement as compared to HLA-B27 and are still difficult to implement in clinical routine. Genetics might also help to predict disease outcome including treatment response. Several genetic variants have been reported to be associated with radiographic damage or with poor response to TNF blockers, unfortunately with lack of coherence across studies. Large-scale studies should be conducted to obtain more robust findings. Genetic and genomic evidence in complex diseases can be further used to support the identification of new drug targets and to repurpose existing drugs. Although not fully driven by genetics, development of IL-17 blockers has been facilitated by the discovery of the association between IL23R variants and SpA. Development of recent approaches combining GWAS findings with functional genomics will help to prioritize new drug targets in the future. Although very promising, translational genetics in SpA remains challenging and will require a multidisciplinary approach that integrates genetics, genomics, immunology, and clinical research.
1 Introduction
Spondyloarthritis (SpA) is a chronic immune mediated inflammatory disease characterized by a combination of articular and extraarticular inflammatory manifestations. One of the hallmarks of this disease is its strong genetic predisposition. Following the discovery of the strong association of HLA-B27 allele with the disease, up to 50 other susceptibility loci have been reported through genome-wide association studies (GWAS). All these loci have provided new insights into disease pathogenesis but might also help to improve disease diagnosis, to detect patient at risk of poor outcome and to identify genetic predictors of treatment response and new drug targets. However, translating genetic findings into clinically meaningful applications remains challenging in complex diseases such as SpA. The purpose of this review is to describe the current status and outline the potential usefulness of clinical applications of genetic knowledge in SpA (Figure 1).
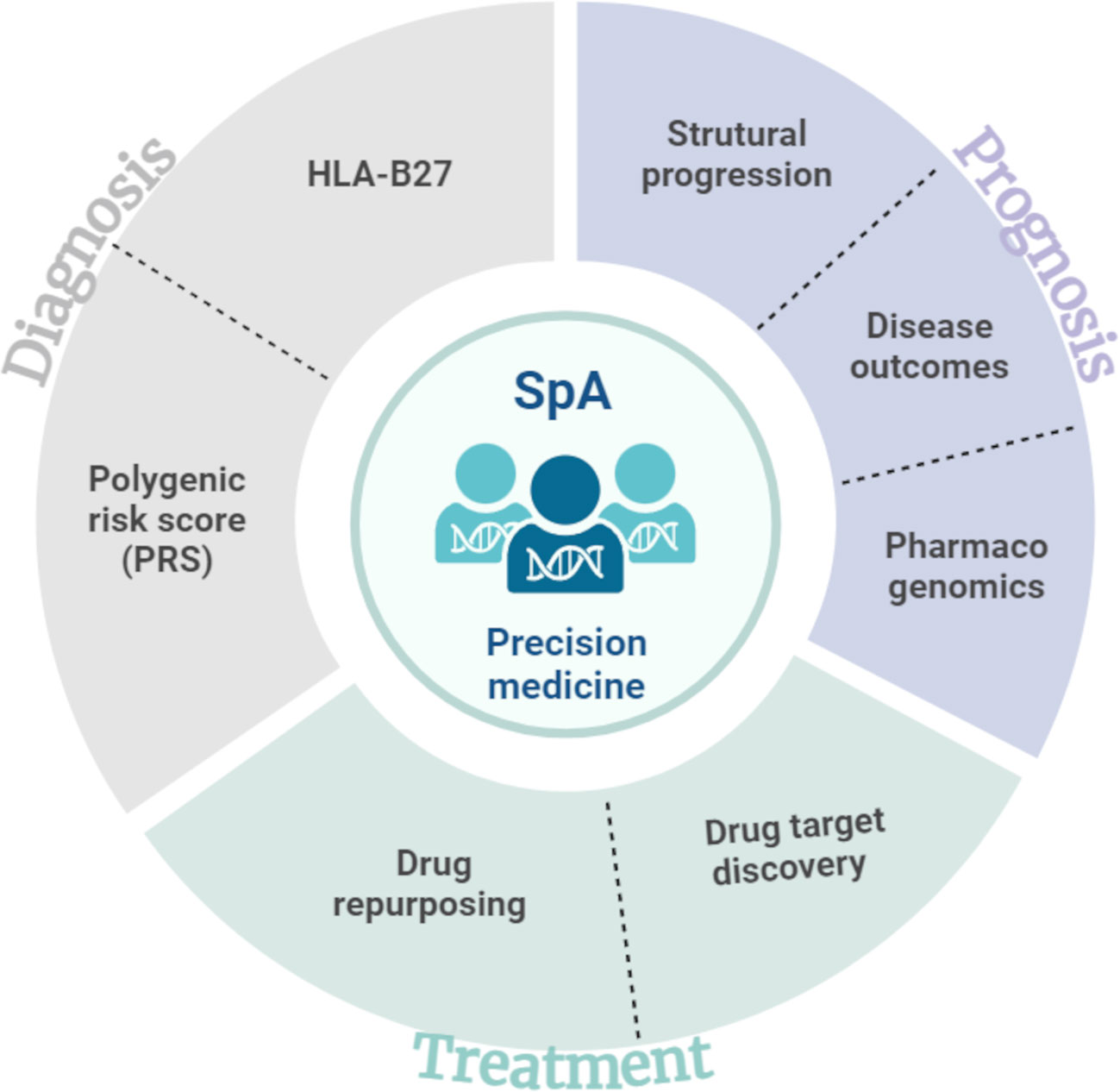
Figure 1 Overview of translational applications of genetic findings in spondyloarthritis.
2 Diagnosis
Diagnosis delay is still a major issue in axial spondyloarthritis (axSpA) with an average time between symptom onset and definite diagnosis of around 5 years (1). Low specificity of most of the frequent clinical manifestations and lack of accurate diagnostic biomarkers contribute to this delay. Given the significant genetic predisposition to axSpA, use of genetic biomarkers to reduce diagnosis delay appears attractive. However, apart for HLA-B27, no single genetic marker has demonstrated noteworthy diagnostic efficacy, prompting the development of more sophisticated polygenic risk score.
2.1 HLA-B27
HLA-B27 testing has been widely used as diagnostic biomarker in axSpA since the discovery of its strong association with the disease (2). However, several factors limit its diagnostic performance (3). First, a substantial proportion (up to 30%) of patients with axSpA do not carry the HLA-B27 allele, affecting the sensitivity. Second, HLA-B27 allele frequency in the general population (e.g. 5 to 10% in Caucasians) is generally higher than required to offer valuable specificity (4). Diagnostic utility of HLA-B27 is also highly dependent on the pre-test probability based on clinical judgement of the physician. Indeed, to provide an acceptable post-test probability of 95%, the physician confidence on diagnosis before HLA-B27 testing should be higher than 50% (5).
Thus, HLA-B27 cannot be used alone for diagnostic purpose and needs to be combined with clinical and imaging features. Rudwaleit et al. estimated in 2004 the utility of several SpA features in axSpA diagnosis. They showed that the presence of two to three SpA features was necessary to increase the diagnostic probability of axSpA to 90% in patients with chronic back pain. With a positive likelihood ratio (LR+) of 9.0, HLA-B27 was the most useful feature together with positive sacroiliac joint MRI (LR+ = 9.0) (6).
2.2 Other single genetic markers
Thanks to genomewide association studies (GWAS), more than 50 independent loci have been associated with ankylosing spondylitis (AS) (7). Although these loci have been significantly associated with AS, the individual risk conferred by each of them is low with odds ratios ranging from 1.1 to 1.7, as compared to an odds ratio of 46 for HLA-B27 (8). Therefore, diagnostic value of single variant is negligible and has no interest in daily practice.
2.3 Polygenic risk scores
Instead of focusing on a single genetic marker to assess genetic risk, an increasingly popular approach is to use aggregate measures of several genetic risk factors into polygenic risk scores (PRS). The initial strategy was to use only loci significantly associated with the disease to elaborate PRS (9). More recently, is has been demonstrated that models incorporating a large number of SNPs without individually significant effect outperformed those employing only GWAS-associated SNPs (10). This aligns with the evidence that a significant fraction of the heritability of complex traits relies on a large number of low-level effect polymorphisms (11).
In SpA, several attempts have been made to elaborate an accurate PRS for diagnostic purpose. In 2017, Thomas et al. demonstrated good diagnostic performance for both AS and non-radiographic axial SpA of a PRS based on the combination of 31 GWAS-associated SNPs and HLA-B27 allele (area under the curve (AUC) of 0.9 and 0.84 respectively) (12). However, the authors did not provide the AUC of using HLA-B27 alone to estimate the additional value of their PRS. A similar approach was used with more recent GWAS results by Rostami et al. (13) who developed a PRS based on 110 GWAS-associated SNPs. They showed low discrimination capacity of PRS alone (AUC = 0.62) lower than that of HLA-B27 alone (AUC = 0.88). Combination of PRS and HLA-B27 improved diagnostic prediction (AUC = 0.9) but the improvement was small and of uncertain clinical value. More recently, Li and al. developed two PRSs based on a larger number of SNPs in two distinct ethnic populations (European descent and East-Asian). These PRSs have good predictive performance in AS, slightly outperforming HLA-B27 alone or MRI (14). Moreover, they showed that PRSs performances were better if developed in the ethnic group to which they are to be applied.
Recent work suggests that rare variants that are poorly tagged by common variants can explain part of missing heritability (15). Incorporating those rare variants into PRS (either as rare-variant polygenic risk score (RVPRS) or in combination with common variant risk score) might increase diagnostic performance (16).
While PRS shows promise in improving SpA diagnosis, widespread use of such score will require further research and validation. Cost-effectiveness of this kind of approach also needs to be demonstrated.
3 Prognosis
Identification of genetic predictors of poor prognosis could significantly improve treatment strategies in SpA. However, defining severity in SpA is challenging because it encompasses multiple domains, including pain, disease activity, physical function, radiographic structural damage, and treatment response. Disease severity is at least partially genetically determined as demonstrated by high heritability of disease activity functional impairment and radiographic damage (17, 18). Until now, a majority of research efforts have been focused on the identification of genetic predictors of radiographic progression.
3.1 Radiographic severity
Studying genetic factors associated with radiographic damage in SpA raises significant challenges. First, it requires available spinal X-rays of good quality to allow the calculation of a reliable scoring system such as mSASSS (modified Stoke Ankylosing Spondylitis Spine Score) (19). Studied population also needs to be well characterized, including information on factors known to be associated with radiographic progression such as male sex, older age, longer disease duration, elevated CRP, smoking status, CRP level or TNF blockers use (20).
Genetic studies targeting radiographic damage in axSpA are still sparse. Most of the studies focused on SNPs in well-established AS susceptibility loci, such as ERAP1 (Endoplasmic Reticulum AminoPeptidase 1), IL23R (Interleukin 23 Receptor) or HLA region or on candidate genes involved in ossification or bone remodelling. Those studies reported associations with several genes, including HLA-B27 (21), RANK (Receptor Activator of Nuclear factor Kappa B) and PTGS1 (Prostaglandin-Endoperoxide Synthase 1) (22), FGB (FibrinoGen Beta chain) (23), LMP2 (Latent Membrane Protein 2) (24), ADRB1 (ADRenoceptor Beta 1), NELL1 (Neural EGFL Like 1) (25), IL23R (26) and TAP2 (Transporter 2, ATP binding cassette subfamily B member) (25). However, most of them did not reach statistical significance and none of them was independently replicated. More recently, Nam et al. performed in a Korean population the first GWAS focused on radiographic severity (27). The best associated SNP in this GWAS was an exonic variant in RYR3 (RYanodine Receptor) but it did not reach genomewide significance threshold. However, given the sample size of the study (444 AS patients), the classical GWAS significance threshold of 5x10-8 might be too conservative and authors provided functional data linking RYR3 with matrix mineralisation which is consistent with a possible role in structural damage in AS.
3.2 Other disease outcomes
Genetic studies have also been conducted on other disease outcomes such as BASDAI or BASFI. However, all those studies suffered from a limited statistical power and a lack of consistent replication, thereby preventing definite conclusions from being drawn, except for the HLA-B27 allele. Indeed, current evidence suggests that B27-positive patients with axSpA might suffer from a worse disease prognosis than B27-negative patients, with higher disease activity (as measured by CRP and ASDAS) and more frequent MRI inflammation of the SI joints and the spine (28, 29).
4 Treatment
4.1 Treatment response prediction
With the growing number of therapeutic options in axSpA, it is increasingly important to be able to predict the likelihood of treatment response and to identify the best therapeutic target for a given patient. Pharmacogenomics is an emerging field aiming at identifying genetic markers that can predict at individual level the response to a particular medication. Objectives are not only to increase treatment efficacy but also to reduce the risk of adverse drug reaction.
The genetic contribution to drug response in SpA has been recently the subject of a systematic literature review by Ortolan et al. (30). Only 26 studies of 393 screened studies were analysed after selection process, 21 of them investigating TNF blockers efficacy. The most frequent reported associations were with polymorphisms in TNFRSF1A/1B (TNF receptor superfamily member 1A/1B) and TNF but results were often conflicting. HLA-B27, not included in this systematic literature review, has also been identified as a predictor of good response to TNF blockers (31).
Implementing pharmacogenomics results into clinical practice faces many challenges, including the determination of which gene-drug pairs are actionable. The Clinical Pharmacogenetics Implementation Consortium (CPIC) has established a gene/drug database to help the identification of situations in which a given genotype results in dose modification or in drug substitution (https://cpicpgx.org/genes-drugs/). Interrogation of this database shows limited evidence for actionable gene/drug pairs in the field of SpA (Table 1). In fact, high level of evidence of actionable gene/drug pairs was only found for non steroidal anti inflammatory drugs and CYP2C9 (cytochrome P450 family 2 subfamily C member 9) (32).
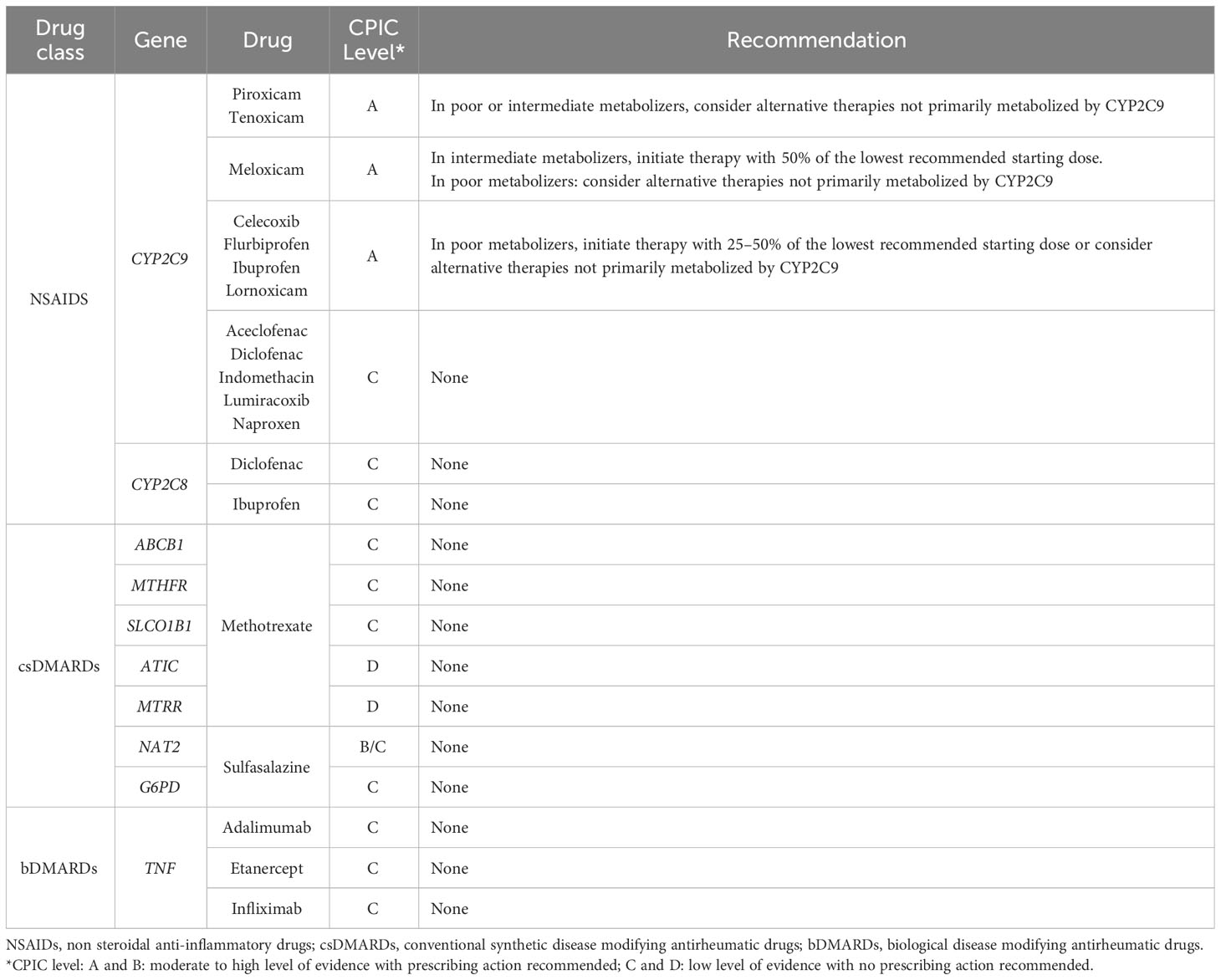
Table 1 Summary of CPIC levels for genes/drugs pairs and recommendations for drugs used in SpA.
4.2 Drug repurposing or drug target discovery
New drug development is a highly expensive process with a high rate of failure. Genomics might help to decrease this failure rate as drug targets with genetic support are more than twice as likely to be successful in clinical development (33, 34). Recent development of evolocumab and alirocumab based on the discovery of PCSK9 (Proprotein Convertase Subtilisin/Kexin type 9) mutations causing hypercholesterolemia corroborates the utility of genomics-driven drug development (35). Genomics might also be very useful for drug repurposing, a strategy in which new indications are identified for existing therapies (36). This approach has a greater likelihood of success and requires significantly less time and monetary investment. In recent years, an increasing number of methods using genetic data for systematically prioritizing drug targets have been proposed (37).
Although no genetic findings have completely driven drug development in SpA, association between AS and several variants in genes involved in IL-17/IL-23 axis have facilitated the development of secukinumab, an IL-17 blocker (38). Several studies have tried to identify candidate drugs in AS by using GWAS findings. In 2016, Ellinghaus et al. performed a cross-phenotype GWAS of 5 immune-mediated diseases including AS (7). Through integration of their GWAS findings with protein-protein interaction networks they found interesting therapeutic targets, some of them currently being tested in AS. More recently, Brown et al. used a genetics-led approach that annotates GWASs with functional genomic data to prioritize new therapeutic targets in AS (39). They found that their algorithm had good performance to prioritize currently approved drug targets for AS with some known AS drug targets such as IL23R, JAK2 (JAnus Kinase 2) among the top 1% of prioritized genes. They also identified new pathways and potential drug targets, including PTGER4 (ProsTaGlandin E Receptor 4), ERBB (ErbB), PI3K (PhosphatidylInositol 3-Kinase), NOTCH1 (NOTCH receptor 1) and GPCR (G Protein Coupled Receptor).
5 Discussion
5.1 Challenges in genomics-driven precision medicine in SpA
As outlined in this review, advances in technology and decreasing costs of genetic sequencing are enhancing the feasibility of integrating genetic information into daily practice. This might help to address unmet needs in SpA, by enabling earlier diagnosis, personalized treatment plan and new drugs development. However, there are several hurdles that need to be surmounted to unlock this potential.
First, the genetic architecture of SpA needs to be better understood, with only a small fraction of disease heritability currently explained. Sample sizes of GWAS performed to date are relatively modest in comparison with other immune mediated diseases such as inflammatory bowel diseases or rheumatoid arthritis. Thus, there is a need for new GWAS with larger sample size and better coverage of the whole genome. Another critical point, especially in the perspective of drug target discovery, is the identification of causal variants and consequently of the functional mechanisms behind the genetic associations.
Moreover, diagnostic, prognostic or theragnostic biomarkers require robust validation to be usable in daily routine. This will require large scale collaborative efforts to constitute large DNA cohort of well phenotyped patients, in diverse populations, ensuring that the identified biomarkers are relevant for different ethnic groups and disease subtypes.
Integration of other “omics” technologies with genetics is also a critical step to improve precision medicine. In particular, epigenetics plays a crucial role in incorporating environmental factors into precision medicine. Analysing epigenetic modifications alongside genetic and transcriptomic data might help to understand how environmental factors contribute to disease susceptibility and progression. As epigenetic modifications are reversible, they might also be accessible to therapeutic interventions. This opens us new opportunities for tailored treatment considering both individual’s genetic background and environment.
5.2 Ethical and social concerns
Beyond technical and methodological challenges already described, personalized medicine also raises ethical and social issues. In a recent position paper, the American College of Physicians recommended that, before conducting any testing, patients should be adequately informed about several important aspects (40). First, they should understand the potential advantages, drawbacks, and constraints of the testing process. They should also be aware of the possibility of incidental findings (i.e. unexpected genetic variants or mutations unrelated to the primary reason for the genetic analysis) and of the fact that such testing may also have consequences for their family relatives. Concerns have also been raised regarding the privacy and security of genetic data, in particular in the context of commercial direct-to-consumer genomic service (41).
Precision medicine might also raise socioeconomical issues. A first concern is the risk of discrimination in employment or health insurance addressed by the emerging concept of “genetic discrimination” (42). Another point to consider is the cost which might lead to an unequal access to precision medicine (43).
6 Conclusion
In conclusion, the integration of genomics is very promising to improve not only SpA daily management, but also to develop new innovative therapies. However, to obtain the full benefits of genomic medicine in SpA, genetic architecture of the disease has to be better understood. There is also a need for strong collaboration between researchers and clinicians. Finally, ethical and social issues related to precision medicine should not be neglected.
Author contributions
EF: Writing – original draft. MB: Writing – review & editing. FC: Writing – original draft, Writing – review & editing.
Acknowledgments
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article. Eva Frison is supported by grant from FOREUM. Félicie Costantino was supported by grants from Société française de rhumatologie (SFR), Fondation pour la recherche médicale (FRM SPE201803005058) and Fondation Bettencourt Schueller.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hay CA, Packham J, Ryan S, Mallen CD, Chatzixenitidis A, Prior JA. Diagnostic delay in axial spondyloarthritis: a systematic review. Clin Rheumatol (2022) 41(7):1939–50. doi: 10.1007/s10067-022-06100-7
2. Brewerton DA, Hart FD, Nicholls A, Caffrey M, James DC, Sturrock RD. Ankylosing spondylitis and HL-A 27. Lancet (1973) 1(7809):904–7. doi: 10.1016/S0140-6736(73)91360-3
3. Lim CSE, Sengupta R, Gaffney K. The clinical utility of human leucocyte antigen B27 in axial spondyloarthritis. Rheumatology (2018) 57(6):959–68. doi: 10.1093/rheumatology/kex345
4. Deodhar A, Gill T, Magrey M. Human leukocyte antigen B27-negative axial spondyloarthritis: what do we know? ACR Open Rheumatol (2023) 5(7):333–44. doi: 10.1002/acr2.11555
5. Hawkins BR, Dawkins RL, Christiansen FT, Zilko PJ. Use of the B27 test in the diagnosis of ankylosing spondylitis: a statistical evaluation. Arthritis Rheumatol (1981) 24(5):743–6. doi: 10.1002/art.1780240524
6. Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J. How to diagnose axial spondyloarthritis early. Ann Rheum Dis (2004) 63(5):535–43. doi: 10.1136/ard.2003.011247
7. Ellinghaus D, Jostins L, Spain SL, Cortes A, Bethune J, Han B, et al. Analysis of five chronic inflammatory diseases identifies 27 new associations and highlights disease-specific patterns at shared loci. Nat Genet (2016) 48(5):510–8. doi: 10.1038/ng.3528
8. International Genetics of Ankylosing Spondylitis Consortium (IGAS), Cortes A, Hadler J, Pointon JP, Robinson PC, Karaderi T, et al. Identification of multiple risk variants for ankylosing spondylitis through high-density genotyping of immune-related loci. Nat Genet (2013) 45(7):730–8. doi: 10.1038/ng.2667
9. Evans DM, Visscher PM, Wray NR. Harnessing the information contained within genome-wide association studies to improve individual prediction of complex disease risk. Hum Mol Genet (2009) 18(18):3525–31. doi: 10.1093/hmg/ddp295
10. Crouch DJM, Bodmer WF. Polygenic inheritance, GWAS, polygenic risk scores, and the search for functional variants. Proc Natl Acad Sci (2020) 117(32):18924–33. doi: 10.1073/pnas.2005634117
11. Speed D, Cai NUCLEB Consortium, Johnson MR, Nejentsev S, Balding DJ. Reevaluation of SNP heritability in complex human traits. Nat Genet (2017) 49(7):986–92. doi: 10.1038/ng.3865
12. Thomas GP, Willner D, Robinson PC, Cortes A, Duan R, Rudwaleit M, et al. Genetic diagnostic profiling in axial spondyloarthritis: a real world study. Clin Exp Rheumatol (2017) 35(2):229–33.
13. Rostami S, Hoff M, Brown MA, Hveem K, Holmen OL, Fritsche LG, et al. Prediction of ankylosing spondylitis in the HUNT study by a genetic risk score combining 110 single-nucleotide polymorphisms of genome-wide significance. J Rheumatol (2020) 47(2):204–10. doi: 10.3899/jrheum.181209
14. Li Z, Wu X, Leo PJ, De Guzman E, Akkoc N, Breban M, et al. Polygenic Risk Scores have high diagnostic capacity in ankylosing spondylitis. Ann Rheum Dis (2021) 80(9):1168–74. doi: 10.1136/annrheumdis-2020-219446
15. Wainschtein P, Jain D, Zheng Z, TOPMed Anthropometry Working Group, NHLBI Trans-Omics for Precision Medicine (TOPMed) Consortium, Cupples LA, et al. Assessing the contribution of rare variants to complex trait heritability from whole-genome sequence data. Nat Genet (2022) 54(3):263–73. doi: 10.1038/s41588-021-00997-7
16. Lali R, Chong M, Omidi A, Mohammadi-Shemirani P, Le A, Cui E, et al. Calibrated rare variant genetic risk scores for complex disease prediction using large exome sequence repositories. Nat Commun (2021) 12(1):5852. doi: 10.1038/s41467-021-26114-0
17. Hamersma J, Cardon LR, Bradbury L, Brophy S, van der Horst-Bruinsma I, Calin A, et al. Is disease severity in ankylosing spondylitis genetically determined? Arthritis Rheumatol (2001) 44(6):1396–400. doi: 10.1002/1529-0131(200106)44:6<1396::AID-ART233>3.0.CO;2-A
18. Brophy S, Hickey S, Menon A, Taylor G, Bradbury L, Hamersma J, et al. Concordance of disease severity among family members with ankylosing spondylitis? J Rheumatol (2004) 31(9):1775–8.
19. Creemers MCW, Franssen MJAM, van ’t Hof MA, Gribnau FWJ, van de Putte LBA, van Riel PLCM. Assessment of outcome in ankylosing spondylitis: an extended radiographic scoring system. Ann Rheumatic Diseases. (2005) 64(1):127–9. doi: 10.1136/ard.2004.020503
20. Pimentel-Santos FM, Atas N. Editorial: Radiographic progression in axial spondyloarthritis. Front Med (Lausanne). (2023) 10:1216466. doi: 10.3389/fmed.2023.1216466
21. Dougados M, Sepriano A, Molto A, van Lunteren M, Ramiro S, de Hooge M, et al. Sacroiliac radiographic progression in recent onset axial spondyloarthritis: the 5-year data of the DESIR cohort. Ann Rheum Dis (2017) 76(11):1823–8. doi: 10.1136/annrheumdis-2017-211596
22. Cortes A, Maksymowych WP, Wordsworth BP, Inman RD, Danoy P, Rahman P, et al. Association study of genes related to bone formation and resorption and the extent of radiographic change in ankylosing spondylitis. Ann Rheumatic Diseases. (2015) 74(7):1387–93. doi: 10.1136/annrheumdis-2013-204835
23. Hoppe B, Schwedler C, Haibel H, Verba M, Proft F, Protopopov M, et al. Predictive value of C-reactive protein for radiographic spinal progression in axial spondyloarthritis in dependence on genetic determinants of fibrin clot formation and fibrinolysis. RMD Open (2021) 7(2):e001751. doi: 10.1136/rmdopen-2021-001751
24. Haroon N, Maksymowych WP, Rahman P, Tsui FWL, O’Shea FD, Inman RD. Radiographic severity of ankylosing spondylitis is associated with polymorphism of the large multifunctional peptidase 2 gene in the Spondyloarthritis Research Consortium of Canada cohort. Arthritis Rheumatol (2012) 64(4):1119–26. doi: 10.1002/art.33430
25. Bartolomé N, Szczypiorska M, Sánchez A, Sanz J, Juanola-Roura X, Gratacós J, et al. Genetic polymorphisms inside and outside the MHC improve prediction of AS radiographic severity in addition to clinical variables. Rheumatology. (2012) 51(8):1471–8. doi: 10.1093/rheumatology/kes056
26. Kadi A, Costantino F, Izac B, Leboime A, Said-Nahal R, Garchon HJ, et al. Brief report: the IL23R nonsynonymous polymorphism rs11209026 is associated with radiographic sacroiliitis in spondyloarthritis. Arthritis Rheumatol (2013) 65(10):2655–60. doi: 10.1002/art.38060
27. Nam B, Jo S, Bang SY, Park Y, Shin JH, Park YS, et al. Clinical and genetic factors associated with radiographic damage in patients with ankylosing spondylitis. Ann Rheum Dis (2023) 82(4):527–32. doi: 10.1136/ard-2022-222796
28. Chung HY, MaChado P, van der Heijde D, D’Agostino MA, Dougados M. HLA-B27 positive patients differ from HLA-B27 negative patients in clinical presentation and imaging: results from the DESIR cohort of patients with recent onset axial spondyloarthritis. Ann Rheum Dis (2011) 70(11):1930–6. doi: 10.1136/ard.2011.152975
29. Zhang S, Wang Y, Peng L, Su J, Zeng X, Li M, et al. Comparison of clinical features in HLA-B27 positive and negative patients with axial spondyloarthritis: results from a cohort of 4,131 patients. Front Med (Lausanne). (2020) 7:609562. doi: 10.3389/fmed.2020.609562
30. Ortolan A, Cozzi G, Lorenzin M, Galozzi P, Doria A, Ramonda R. The genetic contribution to drug response in spondyloarthritis: a systematic literature review. Front Genet (2021) 12:703911. doi: 10.3389/fgene.2021.703911
31. Fröhlich F, Micheroli R, Hebeisen M, Kissling S, Bürki K, Exer P, et al. HLA-B27 as a predictor of effectiveness of treatment with TNF inhibitors in axial spondyloarthritis: data from the Swiss Clinical Quality Management Registry. Clin Rheumatol (2023) 42(5):1267–74. doi: 10.1007/s10067-022-06490-8
32. Theken KN, Lee CR, Gong L, Caudle KE, Formea CM, Gaedigk A, et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2C9 and nonsteroidal anti-inflammatory drugs. Clin Pharmacol Ther (2020) 108(2):191–200. doi: 10.1002/cpt.1830
33. Nelson MR, Tipney H, Painter JL, Shen J, Nicoletti P, Shen Y, et al. The support of human genetic evidence for approved drug indications. Nat Genet (2015) 47(8):856–60. doi: 10.1038/ng.3314
34. King EA, Davis JW, Degner JF. Are drug targets with genetic support twice as likely to be approved? Revised estimates of the impact of genetic support for drug mechanisms on the probability of drug approval. PloS Genet (2019) 15(12):e1008489. doi: 10.1371/journal.pgen.1008489
35. Mullard A. Nine paths to PCSK9 inhibition. Nat Rev Drug Discov (2017) 16(5):299–301. doi: 10.1038/nrd.2017.83
36. Ashburn TT, Thor KB. Drug repositioning: identifying and developing new uses for existing drugs. Nat Rev Drug Discovery (2004) 3(8):673–83. doi: 10.1038/nrd1468
37. Reay WR, Cairns MJ. Advancing the use of genome-wide association studies for drug repurposing. Nat Rev Genet (2021) 22(10):658–71. doi: 10.1038/s41576-021-00387-z
38. Baeten D, Sieper J, Braun J, Baraliakos X, Dougados M, Emery P, et al. Secukinumab, an interleukin-17A inhibitor, in ankylosing spondylitis. New Engl J Med (2015) 373(26):2534–48. doi: 10.1056/NEJMoa1505066
39. Brown AC, Cohen CJ, Mielczarek O, Migliorini G, Costantino F, Allcock A, et al. Comprehensive epigenomic profiling reveals the extent of disease-specific chromatin states and informs target discovery in ankylosing spondylitis. Cell Genomics (2023) 3(6):100306. doi: 10.1016/j.xgen.2023.100306
40. Lehmann LS, Snyder Sulmasy L, Burke W. Ethical considerations in precision medicine and genetic testing in internal medicine practice: a position paper from the American College of physicians. Ann Intern Med (2022) 175(9):1322–3. doi: 10.7326/M22-0743
41. Bonomi L, Huang Y, Ohno-MaChado L. Privacy challenges and research opportunities for genomic data sharing. Nat Genet (2020) 52(7):646–54. doi: 10.1038/s41588-020-0651-0
42. McClellan KA, Avard D, Simard J, Knoppers BM. Personalized medicine and access to health care: potential for inequitable access? Eur J Hum Genet (2013) 21(2):143–7. doi: 10.1038/ejhg.2012.149
Keywords: genetics, genomics, translational genetics, spondyloarthritis, ankylosing spondylitis, diagnosis, prognosis, therapeutic target
Citation: Frison E, Breban M and Costantino F (2024) How to translate genetic findings into clinical applications in spondyloarthritis? Front. Immunol. 15:1301735. doi: 10.3389/fimmu.2024.1301735
Received: 25 September 2023; Accepted: 08 January 2024;
Published: 24 January 2024.
Edited by:
Maria Sole Chimenti, University of Rome Tor Vergata, ItalyReviewed by:
Augusta Ortolan, Agostino Gemelli University Polyclinic (IRCCS), ItalyCopyright © 2024 Frison, Breban and Costantino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Félicie Costantino, ZmVsaWNpZS5jb3N0YW50aW5vQGluc2VybS5mcg==