
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Immunol. , 27 November 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1325299
 Mario Andrea Piga1
Mario Andrea Piga1 Paolo Fraticelli2Leonardo Antonicelli3Maria Stella Garritani3Giulia Ghirelli4
Paolo Fraticelli2Leonardo Antonicelli3Maria Stella Garritani3Giulia Ghirelli4 Matteo Martini3,5Angelica Di Vincenzo3,5
Matteo Martini3,5Angelica Di Vincenzo3,5 Maria Giovanna Danieli2,5,6
Maria Giovanna Danieli2,5,6 Gianluca Moroncini1,2,4,5*
Gianluca Moroncini1,2,4,5* Maria Beatrice Bilò3,5,6
Maria Beatrice Bilò3,5,6The pathogenic role of p-ANCA in eosinophilic granulomatosis with polyangiitis (EGPA) is a long-standing matter of debate. In this work, we report our real-life experience with EGPA patients, treated with biologics targeting type 2 (T2)-eosinophilic inflammation (Mepolizumab, Benralizumab, Dupilumab). Interestingly, we observed EGPA extrarespiratory relapses only in p-ANCA-positive patients (2/5 cutaneous vasculitis, 3/5 constitutional symptoms), with new rise of p-ANCA and normal eosinophil blood count. Notably, revising our cohort with the new ACR 2022 criteria, these five patients were the only ones to satisfy the entry criterion of vasculitis’ defined diagnosis at disease onset. These observations may suggest that biologics, selectively turning off T2 inflammation, may have unmasked p-ANCA exclusive role in the pathogenesis of vasculitis in EGPA. Therefore, we raise the question whether EGPA vasculitis exists only in p-ANCA-positive patients, and whether p-ANCA-negative disease is “only eosinophils without vasculitis”.
Eosinophilic granulomatosis with polyangiitis (EGPA) is an immune-mediated systemic disease, characterized by hypereosinophilia-related damage and necrotizing vasculitis of medium/small vessels (1, 2). Hallmarks are eosinophilic asthma, chronic rhinosinusitis (CRS), especially with nasal polyps (CRSwNP), and peripheral neuropathy. Perinuclear anti-neutrophil cytoplasm antibodies (p-ANCA) are observed only in ~30-35% of cases, and their pathogenetic role is a long-standing matter of debate, while the role of eosinophils is well established. Therapies include corticosteroids, immunosuppressants and Mepolizumab (3, 4), an anti-IL-5 drug directed against type 2 (T2)-eosinophilic inflammation previously approved for the treatment of severe eosinophilic asthma and recently approved also for severe CRSwNP, hypereosinophilic syndrome (HES) and EGPA. Other therapies used in T2 respiratory diseases, such as Benralizumab (anti-IL-5-R, approved for severe eosinophilic asthma) and Dupilumab (anti-IL4/IL-13Rα, approved for severe T2-eosinophilic asthma and CRSwNP), showed efficacy also in the context of EGPA (5, 6). In this work, we discuss about p-ANCA status, reporting our experience with 13 EGPA patients treated with biologics targeting T2-eosinophilic inflammation from 2/2018 to 1/2023 at Internal Medicine Department, Marche University Hospital, Ancona, Italy. Informed consent was obtained for using patients’ data.
All patients were classifiable as EGPA according to the old American College of Rheumatology (ACR) 1990 criteria (7). Diagnosis was based on clinical symptoms and radiological, laboratory and histopathological findings. All patients had asthma, CRS, hypereosinophilia and non-fixed pulmonary infiltrates. 10/13 patients had extra-respiratory manifestations. Organ biopsies were performed in 8/13 patients, all showing extravascular eosinophils, with evidence of necrotizing leukocytoclastic vasculitis in 4/8. 5/13 patients were p-ANCA-positive. Patients’ details are reported in Table 1.
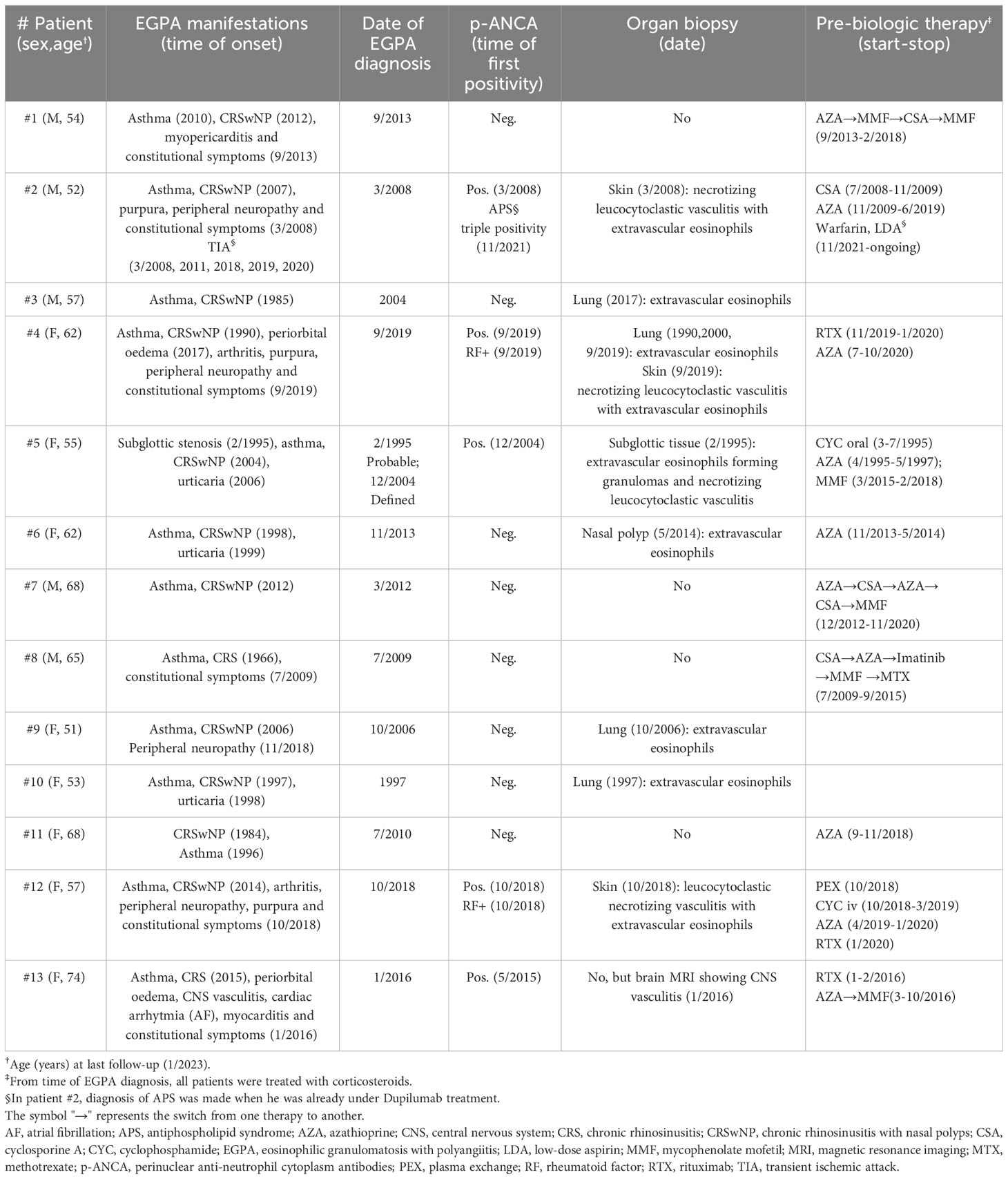
Table 1 Baseline characteristics.
After EGPA diagnosis, all patients were treated with high-dose corticosteroids, and 10/13 with immunosuppressants (Table 1). Complete remission of all clinical manifestations was achieved, with normalization of eosinophils, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and p-ANCA negativization in positive patients.
>However, despite concurrent immunosuppressants’ use, every attempt to reduce/discontinuate steroids resulted in new eosinophils’ increase associated with CRS-asthma relapses (steroid-dependent patients).
In 2018 and 2019, respectively, Mepolizumab and Benralizumab were approved for severe eosinophilic asthma. Since all our patients were affected by this condition, they started Mepolizumab (100 mg/month) or Benralizumab (30 mg/2 months) even if, at that time, these biologics were not approved for EGPA. For this reason, no approval from research ethics board (REB) was needed.
At Mepolizumab/Benralizumab initiation asthma and CRS were the only active clinical manifestations of EGPA, with Birmingham Vasculitis Activity Score (BVAS) = 2. All patients had normal CRP and ESR, and p-ANCA were negative in previously positive patients. Baseline use of oral corticosteroids (OCS) is reported in Table 2. In 12/13 patients, immunosuppressants have been discontinued because of lack of efficacy on respiratory symptoms, remission of extra-respiratory manifestations, side effects.
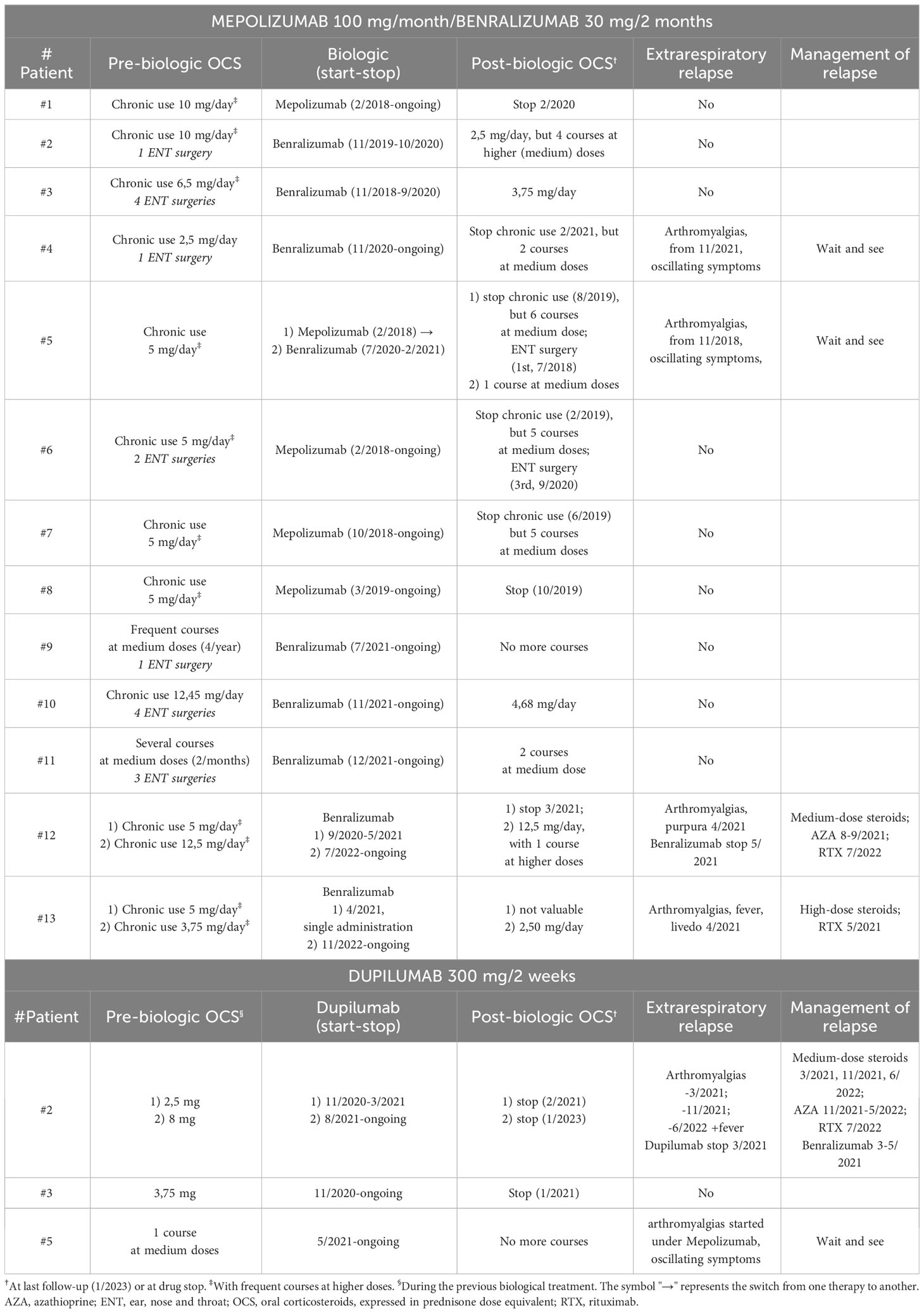
Table 2 Response to biological therapies.
Both Mepolizumab and Benralizumab normalized eosinophils in all patients. A significative improvement in asthma control was observed, as documented by asthma control test and lung function tests (data not reported), and by OCS reduction/discontinuation (reported in Table 2).
For incomplete CRSwNP response, negatively impacting on asthma, three patients were switched to Dupilumab (300 mg/2 weeks) with complete control of both upper and lower respiratory symptoms and OCS withdrawal (Table 2). Even for Dupilumab treatment, no approval from REB was needed, since patients were affected by severe T2 asthma-CRSwNP (approved indications for Dupilumab prescription). Dupilumab-induced hypereosinophilia was observed, but without related clinical symptoms and not exceeding the described alert cut-off of 3000/mmc (8), except for patient #2 (see below).
During treatment with anti-T2 biologics, we observed EGPA extrarespiratory relapses only in the 5 formerly p-ANCA-positive patients, with new rise of p-ANCA, CRP and ESR.
At the time of relapse, patient #2 was under Dupilumab treatment, patients #4, #12 and #13 were under Benralizumab treatment, and patient #5 was under Mepolizumab treatment. Patients #4 and #5 experienced arthromyalgias under Benralizumab and Mepolizumab treatment, respectively, with eosinophils within the normal range. Since the symptoms were mild, episodic, and self-limiting, and values of p-ANCA, ESR and CRP were low, a “wait-and-see” strategy was adopted. Patient 4 maintained Benralizumab therapy, while patient 5, for incomplete CRSwNP response negatively impacting on asthma, was switched from Mepolizumab to Benralizumab and finally to Dupilumab. Over time, in both patients, symptoms remained stable (mild, episodic and self-limiting), while p-ANCA, ESR, CRP mantained at low levels, often with spontaneous normalization at subsequent checks. Patients #12 and #13 relapsed under Benralizumab treatment, with eosinophils within the normal range. Patient #12 experienced arthromyalgias and purpura of the lower limbs, while patient #13 experienced fever, arthromyalgias, and livedo racemose of the arms. Both patients were then treated with steroids and Rituximab (RTX), with clinical remission and p-ANCA persistent negativization, even after steroids withdrawal.
Patient #2 experienced three extrarespiratory relapses under Dupilumab treatment. At first relapse (arthromyalgias), after OCS withdrawal, both p-ANCA and eosinophils were elevated; particularly, Dupilumab-induced hypereosinophilia was severe (5000/mmc). Dupilumab was prudentially stopped and the patient was treated with steroids and resumption of Benralizumab. However, at steroid reduction, Benralizumab again proved not to be effective on CRSwNP, so a new attempt with Dupilumab was made, concurrently using medium-dose OCS (prednisone 10 mg/day) to cover a new possible severe hypereosinophilia. After two months, gradual OCS tapering was started, strictly checking the blood count. In this context, two subsequent relapses (arthromyalgias and fever) occurred. During these relapses, eosinophils were stable at a value of 500-1000 cells/mmc, under low-dose OCS (prednisone 5 mg/day), while p-ANCA increased again. The second relapse was treated with temporary re-increase of OCS (10 mg/day) and azathioprine. For the third relapse, Rituximab was administered, with clinical remission and p-ANCA persistent negativization, allowing steroids discontinuation. After OCS withdrawal, eosinophils rose to 1500-2000/mmc, but the patient maintained asymptomatic. Relapses’ managements are reported in Table 2.
In patients undergoing Mepolizumab/Benralizumab, eosinophils were within the normal range during extrarespiratory relapses. Therefore, we hypothesized that extrarespiratory relapses might be due to the raised p-ANCA. In patient #2, undergoing Dupilumab, both p-ANCA and eosinophils were elevated during the first relapse, making difficult to establish symptoms’ cause (p-ANCA, hypereosinophilia, or both); particularly, Dupilumab-induced hypereosinophilia was severe (5000/mmc). However, during subsequent relapses, eosinophils were stable at a value of 500-1000/mmc, under low-dose OCS, while p-ANCA increased again. Furthermore, p-ANCA negativization following Rituximab coincided with clinical remission, although eosinophils rose to 1500-2000/mmc after OCS discontinuation. Therefore, also in patient #2, we finally hypothesized that extrarespiratory relapses might be due to the raised p-ANCA. Nevertheless, Dupilumab-induced hypereosinophilia could have played a concurrent role in first relapse, so that data relating this patient should be evaluated with great caution.
Based on the above, in our p-ANCA-positive patients, EGPA seemed to have two distinct pathogeneses, sensitive to different therapies: T2-eosinophilic inflammation and p-ANCA-mediated inflammation, responsive to anti-T2 biologics and immunosuppressants, respectively.
This concept has been reported in literature: while T2-eosinophilic inflammation would be responsible for asthma, CRS and eosinophilic organ damage (e.g. myocarditis, gastroenteritis), p-ANCA would underlie vasculitic manifestations (1, 2). However, the verbatim application of this strict dualism cannot always be translated into routine clinical practice (1), and the pathogenic role of p-ANCA is a long-standing matter of debate. An International Consensus reported their poor sensitivity/specificity in differentiating “vasculitic” from “eosinophilic” EGPA (9), stating that p-ANCA cannot guide treatment decision (9).
Nevertheless, in our experience, biologics, selectively turning off T2-eosinophilic inflammation and allowing OCS reduction/withdrawal, may have unmasked p-ANCA exclusive role in the pathogensis of vasculitis in EGPA. Indeed, even if extrarespiratory relapses were mainly represented by aspecific inflammatory constitutional symptoms, 2/5 patients relapsed with frank cutaneous vasculitis (purpura, livedo racemosa). Moreover, the 5 relapsing p-ANCA positive patients were the only ones to have a defined diagnosis of vasculitis at disease onset (4 bioptic, 1 radiologic), so being the only ones to satisfy the entry criterion of the new ACR 2022 criteria (10).
These observations may raise the question whether EGPA vasculitis exists only in p-ANCA-positive patients, and whether p-ANCA-negative disease is only T2-eosinophilic inflammation without vasculitis.
Assuming this, our p-ANCA-negative patients could be considered as having “only” eosinophilic asthma+CRS and/or hypereosinophilic syndrome (HES). The likely bias in their EGPA misdiagnosis would lie in the old ACR 1990 criteria (7), not considering vasculitis’ defined diagnosis.
In literature, however, evidence of organ vasculitis was reported (albeit rarely) also in p-ANCA negative patients. For these cases, some possible explanations could be hypothesized:
1) confounding manifestations, like neuropathy, that are strongly suggestive of vasculitis but can also be exclusively provoked by T2-eosinophilic inflammation (11–13); unfortunately, neuropathy-involved nerves are not always susceptible to diagnostic biopsy in routinary clinical practice;
2) vasculitis not ANCA-associated (drugs, infections, cryoglobulins) that may occur in patients with eosinophilic asthma and/or HES, leading to a clinical picture misdiagnosed as EGPA;
3) vasculitis-like histopathology of involved organs, due to eosinophil-derived vascular damage and thrombosis, but not properly to an autoimmune vasculitis;
4) false negativity of p-ANCA when patients are already undergoing steroid therapy.
A great limit of our hypotheses is that they derive from observations in a small cohort of EGPA patients. However, similar cases have been recently reported, describing the new onset of p-ANCA vasculitis in patients undergoing anti-T2 biologics for severe asthma. In these patients, despite remission of T2-eosinophilic inflammation, development of vasculitis was observed, accompanied by the new finding of p-ANCA positivity (14–18).
Biologics, selectively turning off T2-eosinophilic inflammation and allowing OCS reduction/withdrawal, may have unmasked p-ANCA exclusive role in the pathogenesis of vasculitis in EGPA. If confirmed by larger studies, these observations may have important therapeutic implications, possibly leading to a pathogenesis-based therapy of EGPA.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MP: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. PF: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. LA: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. MG: Data curation, Writing – review & editing. GG: Data curation, Writing – review & editing. MM: Data curation, Writing – review & editing. AV: Data curation, Writing – review & editing. MD: Data curation, Writing – review & editing. GM: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. MB: Conceptualization, Data curation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research leading to these results has received funding from the European Union – NextGenerationEU through the Italian Ministry of University and Research under PNRR – M4C2-I1.3 Project PE_00000019 “HEAL ITALIA” to Prof. Gianluca Moroncini.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fagni F, Bello F, Emmi G. Eosinophilic granulomatosis with polyangiitis: dissecting the pathophysiology. Front Med (2021) 8:627776. doi: 10.3389/fmed.2021.627776
2. Furuta S, Iwamoto T, Nakajima H. Update on eosinophilic granulomatosis with polyangiitis. Allergol Int (2019) 68:430–6. doi: 10.1016/j.alit.2019.06.004
3. Chung SA, Langford CA, Maz M, Abril A, Gorelik M, Guyatt G, et al. 2021 American college of rheumatology/Vasculitis foundation guideline for the management of antineutrophil cytoplasmic antibody-Associated vasculitis. Arthritis Care Res (2021) 73:1088–105. doi: 10.1002/acr.24634
4. Emmi G, Bettiol A, Gelain E, Bajema IM, Berti A, Burns S, et al. Evidence-Based Guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol (2023) 19:378–93. doi: 10.1038/s41584-023-00958-w
5. Cottu A, Groh M, Desaintjean C, Marchand-Adam S, Guillevin L, Puechal X, et al. French Vasculitis Study Group. Benralizumab for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis (2023) 7:ard–2023-224624. doi: 10.1136/ard-2023-224624
6. Molina B, Padoan R, Urban ML, Novikov P, Caminati M, Taillé C, et al. Dupilumab for relapsing or refractory sinonasal and/or asthma manifestations in eosinophilic granulomatosis with polyangiitis: a European retrospective study. Ann Rheum Dis (2023) 21:ard–2023-224756. doi: 10.1136/ard-2023-224756
7. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum (1990) 33:1094–100. doi: 10.1002/art.1780330806
8. Caminati M, Olivieri B, Dama A, Micheletto C, Paggiaro P, Pinter P, et al. Dupilumab-induced hypereosinophilia: review of the literature and algorithm proposal for clinical management. Expert Rev Respir Med (2022) 16:713–21. doi: 10.1080/17476348.2022.2090342
9. Moiseev S, Bossuyt X, Arimura Y, Blockmans D, Csernok E, Damoiseaux J, et al. European EGPA study group. International consensus on ANCA testing in eosinophilic granulomatosis with polyangiitis. Am J Respir Crit Care Med (2020) 202(10), 1360–72. doi: 10.1164/rccm.202005-1628SO
10. Grayson PC, Ponte C, Suppiah R, Robson JC, Craven A, Judge A, et al. DCVAS study group. 2022 american college of rheumatology/european alliance of associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis (2022) 81:309–14. doi: 10.1136/annrheumdis-2021-221794
11. Nishi R, Koike H, Ohyama K, Fukami Y, Ikeda S, Kawagashira Y, et al. Differential clinicopathologic features of EGPA-associated neuropathy with and without ANCA. Neurology (2020) 94:e1726–37. doi: 10.1212/WNL.0000000000009309
12. Oka N, Kawasaki T, Matsui M, Shigematsu K, Unuma T, Sugiyama H. Two subtypes of Churg-Strauss syndrome with neuropathy: the roles of eosinophils and ANCA. Mod Rheumatol (2011) 21:290–5. doi: 10.1007/s10165-010-0400-9
13. Takeuchi H, Kawamura K, Kawasaki T, Oka N. Distinct features of hypereosinophilic syndrome with neuropathy from eosinophilic granulomatosis with polyangiitis. Front Neurol (2022) 13:1057767. doi: 10.3389/fneur.2022.1057767
14. Persaud P, Karmali R, Sankar P, Majid M. Dupilumab-associated eosinophilic granulomatosis with polyangiitis. Cureus (2022) 14:e27670. doi: 10.7759/cureus.27670
15. Lim AKH, Antony A, Gingold M, Simpson I, Looi WF, MacDonald MI. Emergence of extrathoracic manifestations of eosinophilic granulomatosis with polyangiitis during benralizumab treatment. Rheumatol Adv Pract (2021) 5:rkab033. doi: 10.1093/rap/rkab033
16. Hočevar A, Kopač P, Rotar Ž, Novljan MP, Škrgat S. Eosinophilic granulomatosis with polyangiitis evolution during severe eosinophilic asthma treatment with benralizumab. J Allergy Clin Immunol Pract (2020) 8:2448–9. doi: 10.1016/j.jaip.2020.04.006
17. Caminati M, Maule M, Nalin F, Senna G, Lunardi C. Onset of eosinophilic granulomatosis with polyangiitis in a patient treated with an IL-5 pathway inhibitor for severe asthma. Rheumatology (2021) 60:e59–60. doi: 10.1093/rheumatology/keaa572
Keywords: ANCA, biologics, EGPA, eosinophils, vasculitis
Citation: Piga MA, Fraticelli P, Antonicelli L, Garritani MS, Ghirelli G, Martini M, Di Vincenzo A, Danieli MG, Moroncini G and Bilò MB (2023) ANCA-negative EGPA: only eosinophils without vasculitis? Insights from anti-T2 biologics. Front. Immunol. 14:1325299. doi: 10.3389/fimmu.2023.1325299
Received: 21 October 2023; Accepted: 07 November 2023;
Published: 27 November 2023.
Edited by:
Giuseppe Murdaca, University of Genoa, ItalyReviewed by:
Emanuele Bizzi, ASST Fatebenefratelli Sacco, ItalyCopyright © 2023 Piga, Fraticelli, Antonicelli, Garritani, Ghirelli, Martini, Di Vincenzo, Danieli, Moroncini and Bilò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gianluca Moroncini, Zy5tb3JvbmNpbmlAc3RhZmYudW5pdnBtLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.