 Simon Fietz1*
Simon Fietz1* Anne Fröhlich1
Anne Fröhlich1 Cornelia Mauch2,3
Cornelia Mauch2,3 Luka de Vos-Hillebrand1
Luka de Vos-Hillebrand1 Tanja Fetter1Jennifer Landsberg1
Tanja Fetter1Jennifer Landsberg1 Friederike Hoffmann1
Friederike Hoffmann1 Judith Sirokay1
Judith Sirokay1- 1Center for Skin Diseases Bonn, University Hospital Bonn, Bonn, Germany
- 2Center for Integrated Oncology, Cologne, Germany
- 3Center for Integrated Oncology, Bonn, Germany
Introduction: The anti-programmed cell death protein 1 (PD-1) antibody cemiplimab has shown promising results in the treatment of unresectable or metastatic squamous cell carcinoma, however, frequently leads to immune-related adverse events limiting therapy efficacy. Although cutaneous side effects are common, only very few cases of cutaneous lupus erythematosus have been reported under anti-PD-1 immunotherapy. So far, no case of cutaneous lupus has been described under treatment with cemiplimab.
Case report: For the first time, we report the case of a patient with advanced squamous cell carcinoma, who developed clinical and histological findings in sun-exposed skin that were consistent with anti-SS-A/Ro antibody-positive subacute cutaneous lupus erythematosus (SCLE) under treatment with cemiplimab. Additionally, laboratory chemical analyses revealed a severe immune-related hepatitis without clinical symptoms. Both, the SCLE and the hepatitis, resolved after the administration of topical and systemic steroids and the discontinuation of anti-PD-1 therapy.
Conclusion: Treatment with cemiplimab can be associated with the appearance of cutaneous lupus erythematosus in sun-exposed areas. Application of topical and systemic glucocorticoids can lead to a rapid resolution of the skin eruptions. Moreover, our case illustrates the possibility of simultaneously occurring severe immune-related adverse events. This highlights the importance of additional diagnostics to avoid overlooking additional immune-related adverse events.
Introduction
The anti-programmed cell death protein 1 (PD-1) antibody cemiplimab has shown remarkable efficacy in the treatment of unresectable or metastatic cutaneous squamous cell carcinoma (CSCC) (1). However, immune-related adverse events frequently occur during anti-PD-1 treatment and can cause discontinuation of therapy (1). Subacute cutaneous lupus erythematosus (SCLE) is a rare but known adverse event during therapy with other anti-PD-1 antibodies, such as pembrolizumab or nivolumab (2). SCLE presents with erythematous, circular, scaly skin lesions on sun-exposed skin and is triggered by various drugs and UV light (3, 4). Diagnosis is based on skin lesion morphology, laboratory findings (e.g., anti-Ro (SS-A) antibodies) and histopathological findings (3, 4). Therapy includes sun protection and anti-inflammatory topical or systemic drugs, such as corticosteroids or hydroxychloroquine. Moreover, it should be considered to discontinue or pause the potentially triggering drug (3, 4). Cutaneous adverse events are very frequently in up to 50% of patients treated with anti-PD-1 therapy (1, 5–8). Among these, the appearance of SCLE was described for pembrolizumab and nivolumab in less than 0.01% of patients (9). In contrast to the vast majority of cutaneous adverse events, the appearance of SCLE frequently leads to discontinuation of therapy and thus constitutes a relevant potential adverse event (10–12). So far, no case of SCLE has been reported for treatment with cemiplimab (5). For the first time, we describe the occurrence of histopathologically and serologically confirmed SCLE in a patient undergoing treatment with cemiplimab (Figure 1).
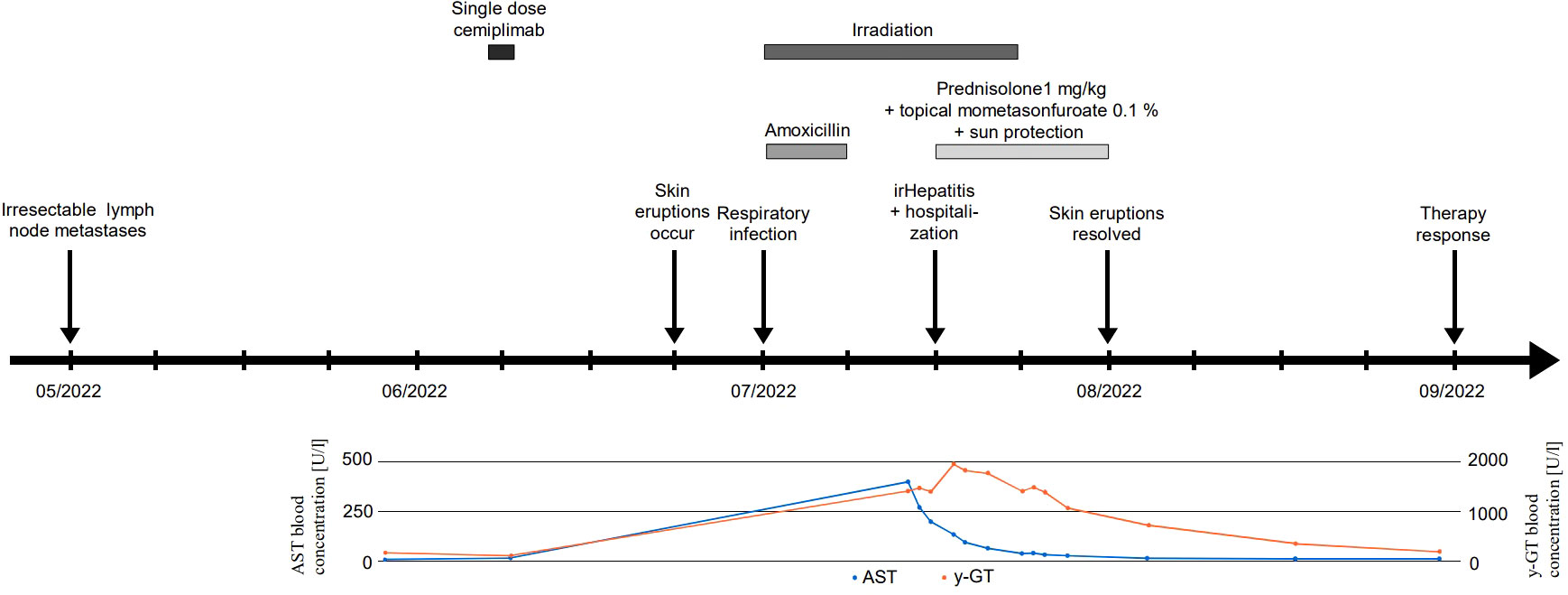
Figure 1 Timeline. Timeline of therapeutic regimens, patient’s symptoms, and laboratory studies.
Case description
A 64-year- old woman with lymphogenic metastasized CSCC of the left limb presented in our dermatological department with a three-week history of severely pruritic, coalescent, erythematous, and scaly macules and papules in sun-exposed areas of the skin (V-area of the upper trunk and neck, forearms, dorsal hands, lower legs, and dorsal feet, Figure 2A) five weeks after the administration of the anti-PD-1 antibody cemiplimab. The patient’s medical history included several benign and malignant light-induced skin eruptions (actinic keratoses, basal cell carcinoma) of the left limb, type 2 diabetes mellitus, and cardiovascular diseases, but no known autoimmune diseases. Despite the successful surgical removal of the primary tumor, the patient developed lymph node metastases of the left axilla (Figure 1). Because of disease progression that could not be managed surgically, we decided to initiate anti-PD-1 antibody therapy as first-line treatment in accordance with the current interdisciplinary guideline on invasive CSCC (13). Five weeks after the occurrence of lymph node metastases the patient received a single dose of cemiplimab 350 mg. Due to an infection of the upper airways three weeks after the first application, which resolved completely after treatment with Amoxicillin for seven days, cemiplimab treatment was halted. Additionally, three weeks after treatment initiation with cemiplimab, the patient underwent fractionated irradiation of symptomatic lymphogenic CSCC metastases of the left axilla for three weeks with a total dose of 40 Gray. The skin eruptions occurred two weeks after administration of cemiplimab and progressed over three weeks.
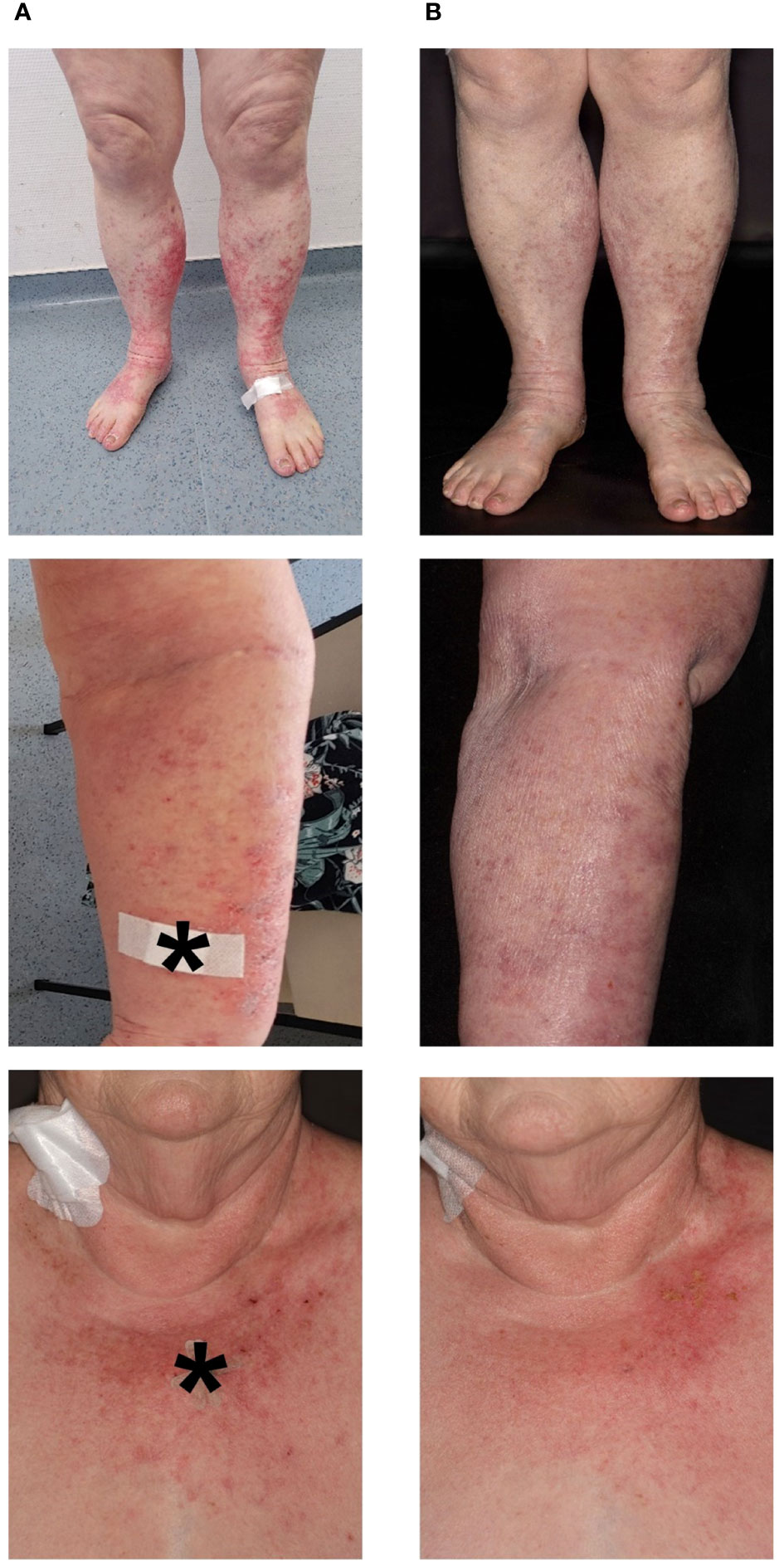
Figure 2 Clinical images (A) on initial contact and (B) 14 days after initiation of steroid treatment. Severely pruritic, scaly, coalescent, and erythematous macules and papules on sun-exposed skin (V-area of the upper trunk and neck, forearms, dorsal hands, lower legs, and dorsal feet). * indicates biopsy site.
A skin biopsy of the chest showed an interface dermatitis with colloid bodies, perifollicular mucin, and mixed immune cells (Figure 3A). A second skin biopsy of the right forearm displayed an acanthosis, parakeratosis, and intraepithelial neutrophil granulocytes, consistent with a psoriasiform inflammation (Figure 3B). Immunoblotting revealed highly positive anti-Ro-52 (SS-A) antibodies (299 U/ml using ELISA), whereas direct immunofluorescence did not show precipitations of IgA, IgG, IgM, C3, or fibrin. Routine blood testing revealed highly elevated liver enzymes and cholestasis parameters (peak values: AST 401 U/l, ALT 267 U/l; γ-GT 1947 U/l, alkaline phosphatase 640 U/l, total bilirubin 2.56 mg/dl; Figure 1) without any pathologies in the clinical examination and computed tomography imaging of the liver. Hepatitis virus serology as well as autoimmune hepatitis panel were negative. The patient was diagnosed with drug-induced, immune-related SCLE, Common Terminology Criteria for Adverse Events version 5.0 (CTCAE v5.0) grade 2 and immune-related hepatitis, CTCAE v5.0 grade 3 (14). Treatment with prednisolone for the severe hepatitis and topical steroids (mometasonfuroate 0.1% ointment) were initiated and tapered over eight weeks. The cutaneous eruptions gradually resolved (Figure 2B) as well as the elevated liver enzymes and cholestasis parameters (Figure 1). Due to the severe CTCAE v5.0 grade 3 hepatitis we decided not to re-initiate treatment with cemiplimab according to the current ASCO guideline (15). Imaging after three months showed therapy response and the patient remained progression-free for eight months.
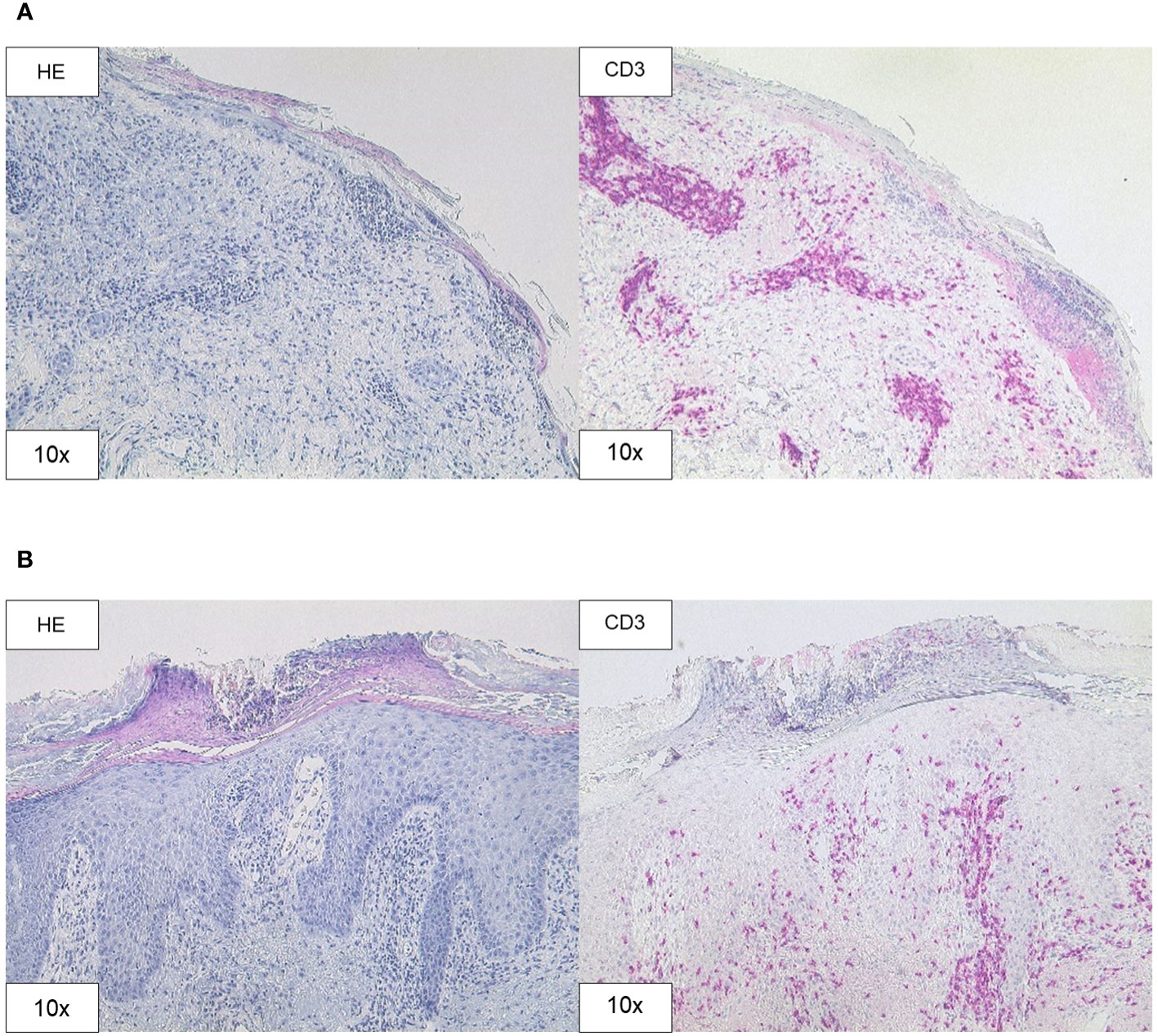
Figure 3 Histopathology. (A) H&E and CD3 staining (original magnification 10x) of the skin biopsy of the chest demonstrating interface dermatitis with colloid bodies, perifollicular mucin, and mixed immune cells, containing lymphocytes, histiocytes, and neutrophil granulocytes. (B) H&E and CD3 staining (original magnification 10x) of the skin biopsy of the right forearm showing acanthosis, parakeratosis, intraepithelial neutrophil granulocytes, and CD3 positive T cell infiltration.
Discussion
For the first time, we present the rare occurrence of SCLE related to cemiplimab therapy complicated by immune-related hepatitis. As described by Marzano et al. drug-induced SCLE usually goes along with elevated anti-Ro (SS-A)-antibodies and is chronologically related to the triggering drug (3). Because of the typical clinical appearance and distribution of the skin eruptions and the high concentration of anti-Ro (SS-A)-antibodies, we diagnosed SCLE despite the lack of lesional immune precipitates. The skin biopsies taken from the chest and the right forearm revealed an interface dermatitis and a psoriasiform inflammation, respectively. Marzano et al. described two different predominant phenotypic variants of drug-induced SCLE: ‘papulosquamous’ and ‘annular polycyclic’ (3). SCLE mostly goes along with histological interface dermatitis (3). However, biopsies taken from ‘papulosquamous’ SCLE can show psoriasiform changes as well (4, 5). In accordance with the clinical phenotype both biopsies contribute to a ‘papulosquamous’ SCLE in the case of our patient.
It remains unclear whether a topical application of glucocorticoids would have been sufficient for the recovery of the skin lesions, as systemic steroid treatment was necessary to treat the concomitant immune-related hepatitis. In patients treated with the anti-PD-1 antibodies pembrolizumab or nivolumab moderate SCLE eruptions could be treated successfully by discontinuation of immunotherapy and were kept under control after re-initiation of systemic treatment by the use of topical steroids (16, 17). In addition to treatment discontinuation and topical steroids the use of systemic hydroxychloroquine and/or glucocorticoids alone or in combination was described to resolve severe SCLE skin eruptions (10–12, 18–23). By this means, immunotherapy could be continued successfully in some cases without or with only a mild relapse of SCLE (20–22). Although the patient only underwent irradiation of the left axilla, radiotherapy is a known trigger of cutaneous lupus erythematosus and was temporally related to the occurrence of the presented skin eruptions in our case (24, 25). Therefore, irradiation could have acted as a trigger for SCLE in the described case. Moreover, the simultaneous irradiation of the metastatic site could have masked response to cemiplimab. In our case, cemiplimab treatment was discontinued because of the severe hepatitis. Monitoring of SCLE and evaluation of possible therapy options under cemiplimab treatment might be of interest for future patients.
In conclusion, our case demonstrates that patients receiving cemiplimab can develop cutaneous lupus erythematosus. The concomitant immune-related hepatitis underlines the need to screen for additional adverse events other than skin conditions. Diagnosis and treatment of patients with adverse events on cemiplimab treatment will be a challenge for dermatologists in the future.
Patient perspective
For the patient, an improvement of the sever pruritus accompanying the cutaneous lesions was of primary importance. As she did not develop any clinical symptoms from the hepatitis, it was challenging for the patient to stay motivated to continue on systemic steroids after resolution of the skin symptoms. Transparent communication of diagnostic results and therapeutic consequences was important for the patient to reach a high level of compliance.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: a publication of datasets containing original patient-related data could affect the patient’s anonymization. Original datasets are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to Simon Fietz, Simon.Fietz@ukbonn.de.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SF: Conceptualization, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing, Data curation, Project administration, Software, Validation. AF: Supervision, Writing – original draft. CM: Conceptualization, Supervision, Writing – original draft. LV: Supervision, Writing – original draft. TF: Data curation, Investigation, Writing – original draft. JL: Supervision, Writing – original draft. FH: Conceptualization, Project administration, Supervision, Writing – original draft. JS: Conceptualization, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. LV received funding from the University Hospital Bonn GEROK program (O-105.0072). FH and AF were partly funded by the Deutsche Krebshilfe through a Mildred Scheel Foundation Grant (grant number 70113307).
Acknowledgments
We thank the Bonn University Medical Faculty and the University Hospital Bonn for the support of this report.
Conflict of interest
JS is a consultant/advisory board member and received speaker’s honoraria from Novartis, BMS, MSD, and Roche.
JL is a consultant/advisory board member and received speaker’s honoraria from Novartis, BMS, MSD, and Roche.
LV received financial support travel expenses from Pierre Fabre.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Migden MR, Rischin D, Schmults CD, Guminski A, Hauschild A, Lewis KD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med (2018) 379(4):341–51. doi: 10.1056/NEJMoa1805131
2. Bolton C, Chen Y, Hawthorne R, Schepel IRM, Harriss E, Hofmann SC, et al. Systematic review: monoclonal antibody-induced subacute cutaneous lupus erythematosus. Drugs R D (2020) 20(4):319–30. doi: 10.1007/s40268-020-00320-5
3. Marzano AV, Vezzoli P, Crosti C. Drug-induced lupus: an update on its dermatologic aspects. Lupus (2009) 18(11):935–40. doi: 10.1177/0961203309106176
4. Eastham AB, Vleugels RA. Cutaneous lupus erythematosus. JAMA Dermatol (2014) 150(3):344. doi: 10.1001/jamadermatol.2013.10393
5. Naik PP. Cemiplimab in advanced cutaneous squamous cell carcinoma. Dermatol Ther (2021) 34(6):e15184. doi: 10.1111/dth.15184
6. Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, Hwu P, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med (2012) 366(26):2455–65. doi: 10.1056/NEJMoa1200694
7. Sibaud V, Meyer N, Lamant L, Vigarios E, Mazieres J, Delord JP. Dermatologic complications of anti-PD-1/PD-L1 immune checkpoint antibodies. Curr Opin Oncol (2016) 28(4):254–63. doi: 10.1097/CCO.0000000000000290
8. Postow MA, Callahan MK, Wolchok JD. Immune checkpoint blockade in cancer therapy. J Clin Oncol (2015) 33(17):1974–82. doi: 10.1200/JCO.2014.59.4358
9. Lowe GC, Henderson CL, Grau RH, Hansen CB, Sontheimer RD. A systematic review of drug-induced subacute cutaneous lupus erythematosus. Br J Dermatol (2011) 164(3):465–72. doi: 10.1111/j.1365-2133.2010.10110.x
10. Andersson NW, Zachariae C, Simonsen AB. Late onset of subacute cutaneous lupus erythematosus following pembrolizumab therapy. Eur J Cancer (2021) 145:168–70. doi: 10.1016/j.ejca.2020.12.017
11. Marano AL, Clarke JM, Morse MA, Shah A, Barrow W, Selim MA, et al. Subacute cutaneous lupus erythematosus and dermatomyositis associated with anti-programmed cell death 1 therapy. Br J Dermatol (2019) 181(3):580–3. doi: 10.1111/bjd.17245
12. Ogawa-Momohara M, Muro Y, Goto K, Obuse C, Satoh M, Kono M, et al. Subacute cutaneous lupus erythematosus with melanocyte elimination induced by pembrolizumab. J Dermatol (2020) 47(6):e217–9. doi: 10.1111/1346-8138.15316
13. Stratigos AJ, Garbe C, Dessinioti C, Lebbe C, Bataille V, Bastholt L, et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 2. Treatment. Eur J Cancer (2020) 128:83–102. doi: 10.1016/j.ejca.2020.01.008
14. . Available at: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
15. Schneider BJ, Naidoo J, Santomasso BD, Lacchetti C, Adkins S, Anadkat M, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol (2021) 39(36):4073–126. doi: 10.1200/JCO.21.01440
16. Blakeway EA, Elshimy N, Muinonen-Martin A, Marples M, Mathew B, Mitra A. Cutaneous lupus associated with pembrolizumab therapy for advanced melanoma: a report of three cases. Melanoma Res (2019) 29(3):338–41. doi: 10.1097/CMR.0000000000000587
17. Shao K, McGettigan S, Elenitsas R, Chu EY. Lupus-like cutaneous reaction following pembrolizumab: An immune-related adverse event associated with anti-PD-1 therapy. J Cutan Pathol (2018) 45(1):74–7. doi: 10.1111/cup.13059
18. Diago A, Hueso L, Ara-Martín M, Abadías-Granado I. Subacute cutaneous lupus erythematosus induced by PD-1 Inhibitor therapy: two case reports and literature review. Australas J Dermatol (2021) 62(2):e347–9. doi: 10.1111/ajd.13538
19. Zitouni NB, Arnault JP, Dadban A, Attencourt C, Lok CC, Chaby G. Subacute cutaneous lupus erythematosus induced by nivolumab: two case reports and a literature review. Melanoma Res (2019) 29(2):212–5. doi: 10.1097/CMR.0000000000000536
20. Manjunath J, Mochel M, Nutan F. Nivolumab-Induced de novo Discoid Lupus Erythematosus. Case Rep Dermatol (2022) 14(1):88–92. doi: 10.1159/000523800
21. Liu RC, Sebaratnam DF, Jackett L, Kao S, Lowe PM. Subacute cutaneous lupus erythematosus induced by nivolumab. Australas J Dermatol (2018) 59(2):e152–4. doi: 10.1111/ajd.12681
22. Kosche C, Owen JL, Choi JN. Widespread subacute cutaneous lupus erythematosus in a patient receiving checkpoint inhibitor immunotherapy with ipilimumab and nivolumab. Dermatol Online J (2019) 25(10):13030/qt4md713j8. doi: 10.5070/D32510045821
23. Wouters A, Durieux V, Kolivras A, Meert AP, Sculier JP. Bullous lupus under nivolumab treatment for lung cancer: A case report with systematic literature review. Anticancer Res (2019) 39(6):3003–8. doi: 10.21873/anticanres.13432
24. Szczęch J, Samotij D, Werth VP, Reich A. Trigger factors of cutaneous lupus erythematosus: a review of current literature. Lupus (2017) 26(8):791–807. doi: 10.1177/0961203317691369
Keywords: case report, cutaneous squamous cell carcinoma, immunotherapy, anti-PD-1 antibody, cutaneous lupus erythematosus
Citation: Fietz S, Fröhlich A, Mauch C, de Vos-Hillebrand L, Fetter T, Landsberg J, Hoffmann F and Sirokay J (2023) Manifestation of subacute cutaneous lupus erythematosus during treatment with anti-PD-1 antibody cemiplimab – a case report. Front. Immunol. 14:1324231. doi: 10.3389/fimmu.2023.1324231
Received: 19 October 2023; Accepted: 22 November 2023;
Published: 08 December 2023.
Edited by:
Prakash Radhakrishnan, University of Nebraska Medical Center, United StatesReviewed by:
Andrea Alberti, University of Brescia, ItalyMingzeng Zhang, Dana–Farber Cancer Institute, United States
Copyright © 2023 Fietz, Fröhlich, Mauch, de Vos-Hillebrand, Fetter, Landsberg, Hoffmann and Sirokay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simon Fietz, c2ltLmZpZXR6QHdlYi5kZQ==