 Victoria del Pozo1
Victoria del Pozo1 Irina Bobolea2
Irina Bobolea2 Manuel J. Rial3,4
Manuel J. Rial3,4 Georgina Espigol-Frigolé5Roser Solans Laqué6
Georgina Espigol-Frigolé5Roser Solans Laqué6 Jesús María Hernández-Rivas7Elvira Mora8
Jesús María Hernández-Rivas7Elvira Mora8 Astrid Crespo-Lessmann9*José Luis Izquierdo Alonso10,11
Astrid Crespo-Lessmann9*José Luis Izquierdo Alonso10,11 María Sandra Domínguez Sosa12
María Sandra Domínguez Sosa12 Juan Maza-Solano13Belén Atienza-Mateo14
Juan Maza-Solano13Belén Atienza-Mateo14 David Bañas-Conejero15Abraham L. Moure15Íñigo Rúa-Figueroa16
David Bañas-Conejero15Abraham L. Moure15Íñigo Rúa-Figueroa16- 1Immunology Department, Instituto de Investigación Sanitaria Fundación Jiménez Díaz (IIS-FJD), Madrid, Spain
- 2Allergy Department, Severe Asthma Unit, Hospital Clínic Barcelona, Barcelona, Spain
- 3Allergy Department, Severe Asthma Unit, Complexo Hospitalario Universitario A Coruña, A Coruña, Spain
- 4Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), A Coruña, Spain
- 5Department of Autoimmune Diseases, Hospital Clinic Clínic, University of Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 6Autoimmune Systemic Diseases Unit, Internal Medicine Department, Vall d’Hebron Hospital, Autonomous University of Barcelona, Barcelona, Spain
- 7Department of Medicine, University of Salamanca & Servicio de Hematología, Hospital Universitario de Salamanca, Instituto de Investigación Biomédica de Salamanca (IBSAL), Salamanca, Spain
- 8Hematology Department, La Fe University and Polytechnic Hospital, La Fe Research Institute, Valencia, Spain
- 9Department of Respiratory Medicine, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain
- 10Department of Medicine and Medical Specialties, University of Alcalá, Alcalá de Henares, Madrid, Spain
- 11Pulmonology Service, Guadalajara University Hospital, Guadalajara, Spain
- 12Rhinology Unit, Department of Otolaryngology, Head and Neck Surgery, University Hospital of Gran Canaria Dr. Negrín, Las Palmas de Gran Canaria, Spain
- 13Rhinology Unit, Department of Otolaryngology, Head and Neck Surgery, Virgen Macarena University Hospital, Sevilla, Spain
- 14Division of Rheumatology, University Hospital of Marqués de Valdecilla, Instituto de Investigación Marqués de Valdecilla (IDIVAL), Immunopathology group, Santander, Spain
- 15Specialty Care Medical Department, GSK, Madrid, Spain
- 16Rheumatology Department, University Hospital of Gran Canaria Dr. Negrín, Las Palmas de Gran Canaria, Spain
Eosinophil-related diseases represent a group of pathologic conditions with highly heterogeneous clinical presentation and symptoms ranging from mild to critical. Both systemic and localized forms of disease are typically treated with glucocorticoids. The approval of novel biologic therapies targeting the interleukin-5 pathway can help reduce the use of systemic glucocorticoids (SGC) in eosinophilic diseases and reduce the risk of SGC-related adverse effects (AEs). In this article, a panel of experts from different medical specialties reviewed current evidence on the use of SGC in two systemic eosinophilic diseases: Eosinophilic Granulomatosis with PolyAngiitis (EGPA) and HyperEosinophilic Syndrome (HES); and in two single-organ (respiratory) eosinophilic diseases: Chronic RhinoSinusitis with Nasal Polyps (CRSwNP) and Severe Asthma with Eosinophil Phenotype (SA-EP), and contrasted it with their experience in clinical practice. Using nominal group technique, they reached consensus on key aspects related to the dose and tapering of SGC as well as on the initiation of biologics as SGC-sparing agents. Early treatment with biologics could help prevent AEs associated with medium and long-term use of SGC.
1 Introduction
Eosinophilic diseases are characterized by the presence of high levels of eosinophils in the blood (eosinophilia) and/or in certain tissues, such as respiratory or digestive systems or in the connective tissue, where they can cause inflammation and organ damage (1). The most common causes of eosinophilia or localized eosinophil tissue infiltration are allergic reactions, parasitic infections and certain malignancies, such as Hodgkin lymphoma and leukemia (2, 3).
The clinical presentation of eosinophilic diseases is highly heterogeneous, ranging from localized eosinophilic disease in which a single organ is involved, such as the lung, to systemic disease in which multiple organs are affected, as occurs in Eosinophilic Granulomatosis with PolyAngiitis (EGPA). The magnitude of eosinophilia also varies widely.
Treatment depends on the cause of eosinophilia and the organs and/or systems involved, although it has traditionally relied on eosinophil attenuation by using local and systemic glucocorticoids (SGC) (4). Various international scientific societies have issued guidelines to aid the management of different eosinophilic diseases and the use of SGC (5–11). Prednisone is the most commonly prescribed glucocorticoid as first-line therapy for patients with systemic or localized eosinophilic diseases (12, 13). There is considerable variation in the dose of SGC used and duration of treatment, regardless of whether the disease is localized or systemic (5, 7, 14, 15). In both cases, because SGC are often used in high doses and/or over prolonged periods, patients are at increased risk of well-known SGC-related adverse effects (AEs), such as serious infection (16), and corticoresistance (17–19).
Several novel biologic therapies targeting interleukin-5 (IL-5) and the IL-5 receptor have recently been approved for clinical use, and can help reduce the dose or avoid the use of SGC in eosinophil-related diseases (3, 20–22).
For many eosinophil-related diseases, there is no universally accepted modality of SGC regimen (14, 15, 23, 24). Because of the lack of evidence for some pathologies, healthcare professionals often have to extrapolate the evidence available in managing one pathology, such as Severe Asthma with Eosinophil Phenotype (SA-EP) for which there is more evidence on SGC tapering, to another, such as EGPA and HyperEosinophilic Syndrome (HES), where the scarcity of patients makes this evidence more difficult to generate.
In this article, a panel of experts from different medical specialties reviewed current evidence on the use of SGC in two systemic eosinophilic diseases: EGPA and HES, and in two single-organ (respiratory) eosinophilic diseases: Chronic RhinoSinusitis with Nasal Polyps (CRSwNP) and SA-EP (Box 1); and contrasted it with their experience in clinical practice. They reached consensus on key aspects of the management of these diseases with SGC and on when to initiate biologics with the purpose of reducing the risk of SGC-associated AEs. Further research into the management of eosinophil-related diseases with biologics will help to establish specific evidence-based guidelines to minimize SGC-related AEs and optimize therapy.
Box 1. Eosinophil-related diseases
Systemic eosinophilic diseases:
Eosinophilic Granulomatosis with PolyAngiitis (EGPA)
EGPA, formerly called Churg-Strauss syndrome, is a rare form of vasculitis that primarily affects small blood vessels. Individuals diagnosed with EGPA usually have a history of asthma or allergies.
EGPA is a chronic illness with cycles of relapse and remission that can cause serious health problems.
Treatment typically includes OCS used in combination with non-glucocorticoid immunosuppressive agents. In 2017, mepolizumab (Nucala) was the first biologic drug to be approved by the U.S. Food and Drug Administration (FDA) for the treatment of EGPA in adults (25).
HyperEosinophilic Syndrome (HES)
HES is the term used to refer to a group of rare blood disorders characterised by very high numbers of eosinophils and end-organ damage.
People with HES usually have more than 1,500 eosinophils/microliter in their blood for 6 months or more (vs less than 500), and the cause cannot be identified. These eosinophils make their way into various tissues, causing inflammation and eventually organ dysfunction. The most commonly involved organs in HES include the skin, lungs, heart, gastrointestinal tract, and nervous system.
Patients with HES often keep using SGC to reduce blood eosinophil count despite the fact that new targeted therapies against eosinophils (i.e. anti-IL-5 biologics) have been approved for this indication in Europe and the US (26–28).
Localised (respiratory) eosinophilic diseases:
Severe Asthma with Eosinophil Phenotype (SA-EP)
SA-EPA is a rare type of asthma that is usually only found in adults ages 35-50 with no allergies. Patients can struggle to manage their symptoms even with high doses of inhaled corticosteroids.
Short cycles of high-dose OCS are used to reduce the frequency of eosinophilic asthma attacks. Several biologics, including benralizumab, mepolizumab and reslizumab have been approved for treating SEA (29).
Chronic RhinoSinusitis with Nasal Polyps (CRSwNP)
CRSwNP is a chronic inflammatory disease of the nasal mucosa and paranasal sinuses. Patients suffer from persistent nasal congestion, rhinorrhoea and loss of smell. CRSwNP has a substantial impact on patients’ HRQoL, including sleep quality (30).
Up to 30% of patients with CRS have nasal polyps. The symptoms of CRSwNP are uncontrolled by current standards of care in one-third of patients, especially in cases associated with high levels of eosinophils such as aspirin-exacerbated respiratory disease (31).
Sinonasal surgeries and/or corticosteroids are the most common treatments for CRSwNP. Biologics are an emerging treatment option for patients with severe uncontrolled CRSwNP.
2 Methods
The authors, a multidisciplinary panel of expert clinical immunologists, pulmonologists, ENT (ear, nose and throat) specialists, allergists, rheumatologists, hematologists, and internal medicine specialists involved in the management of eosinophilic diseases across Spain, reviewed 20 articles on severe asthma, 14 articles of nasal polyposis, 10 articles on HES and 12 articles on EGPA. These articles were selected after a PICO-based search (P, patients with eosinophilic disease; I, treatment with systemic corticosteroids; C, without treatment with systemic corticosteroids; O, dose and/or time until the development of AEs) using the PubMed database and predefined keywords (oral glucocorticoids, systemic glucocorticoids, corticosteroids, eosinophils, eosinophilic diseases, chronic rhinosinusitis, nasal polyps, polyposis, severe asthma, hypereosinophilic syndrome, eosinophilic granulomatosis with polyangiitis, Churg-Strauss syndrome). Only articles published in English between 2007-2022 were considered. Search results were filtered to select evidence relating to: current recommendations on the use of SGC for treating eosinophil-related diseases; the impact of SGC at the respiratory tract and systemic level; maximum acceptable SGC dosing; and SGC sparing and AE prevention strategies.
At a meeting held on the 19th of September 2022 in Madrid, Spain, the panelists contrasted the gathered evidence on the use of SGC in eosinophilic diseases (focusing on CRSwNP, SA-EP, EGPA and HES) with their experience in managing these diseases in daily clinical practice. Using nominal group technique, they reached consensus on key aspects related to the dose and tapering of SGC, as well as on the initiation of biologics as SGC-sparing agents, with the aim of reducing the risk of SGC-related AEs in the different eosinophil-related diseases discussed.
3 Results
3.1 SGC dosing and tapering for eosinophilic diseases
In systemic diseases such as EGPA or HES, it is still common practice to start with the maximum dose of SGC to induce remission and then decrease it (EGPA, up to 1mg/kg/day, maximum 80 mg/day prednisone or equivalent; HES, up to 1mg/kg/day prednisone or equivalent, see Table 1). For respiratory eosinophilic diseases like CRSwNP and SA-EP, SGC are used as a last resort for exacerbations in uncontrolled patients and withdrawn without tapering.
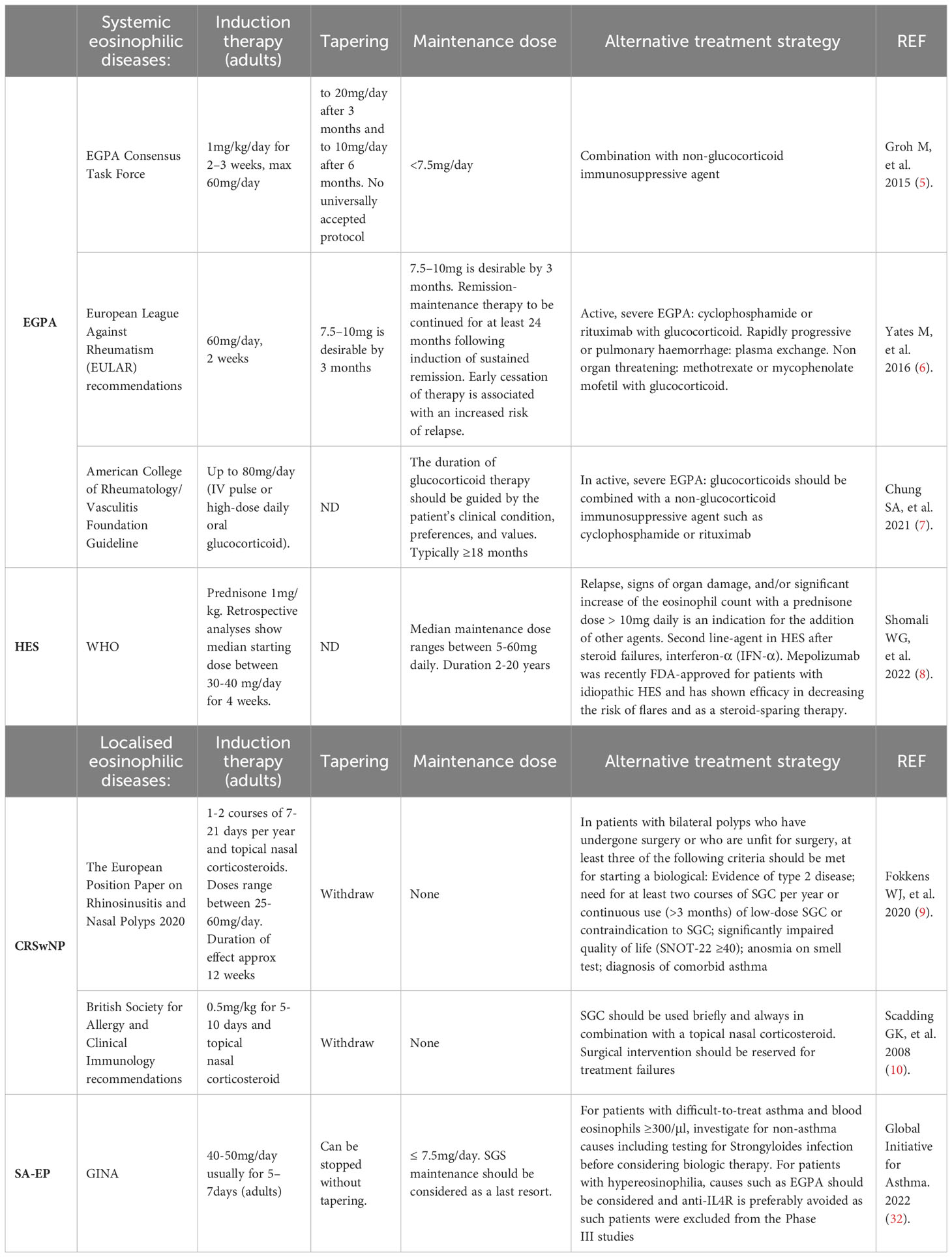
Table 1 Suggested SGC use for eosinophil-related diseases from selected learned societies and groups of experts.
However, the patterns of SGC use differ widely between specialists and the different eosinophilic diseases. This is partly due to different guideline recommendations, limited evidence for some eosinophilic diseases and to the individual patient’s response to SGC and risk of AEs.
The experts agreed with previous literature that in localized diseases, a cumulative dose exceeding 1 g/year prednisone or equivalent is indicative of poor control and is associated with SGC-related AEs (33, 34), but they are aware that in clinical practice this dose is exceeded in many patients. Data from the Optimum Patient Care Research Database (OPCRD) and the British Thoracic Society (BTS) Difficult Asthma Registry show that the median cumulative SGC dose over the 2 study years was 3920 mg in severe asthma patients and that 93% of patients had one or more AE linked to SGC exposure (35). There is growing evidence in the literature that even very brief cycles of SGC have a cumulative effect that significantly increases the risk of developing SGC-related AEs, including osteoporosis, pneumonia, cardiovascular diseases, hypertension, glaucoma, depression/anxiety, type 2 diabetes and growth retardation in children (34, 36–39).
3.1.1 Considerations for systemic eosinophilic diseases: EGPA and HES
To control disease flares in patients with systemic eosinophilic diseases the experts would prescribe between 30-60 mg/day prednisone or equivalent (or 0.5-1 mg/kg/day) for 14–21 days. The prescribed dose can vary widely as it depends on type of disease, symptom severity, the patient’s history and existing medication. After an initial course, the dose should be reduced; rapidly at first (halved after 2–4 weeks) and then more slowly over the course of 3–6 months until withdrawal or a minimum maintenance dose, < 5 mg/day, is achieved, in agreement with the latest recommendations from the European Alliance of Associations for Rheumatology (40). In severe EGPA cases, intravenous pulses of methylprednisolone are frequently used.
The maintenance dose threshold to prevent the development of serious AEs in patients with systemic eosinophilic diseases is difficult to establish given the heterogeneity of patients and the length of exposure, which determines cumulative dose. The risk/benefit balance of low dose SGC in systemic rheumatic diseases is still unclear (41), but the experts agreed that the lowest effective dose of SGC should be used for the shortest time possible.
In EGPA, the duration of corticosteroid therapy should be guided by the patient’s clinical condition, values and preferences. There is insufficient published evidence to support a specific duration of SGC and there are discrepancies between guidelines (12, 42). Many patients with EGPA require low dose glucocorticoids to control their asthma and other symptoms. A reduced-dose regimen has been shown to decrease the risk of serious infections and minimize SGC toxicity (7, 43).
Patients with HES often keep using SGC to reduce blood eosinophil count despite the fact that new targeted therapies against eosinophils (i.e. anti-IL-5 biologics) have been approved for this indication in Europe and the US (26–28).
3.1.2 Considerations for respiratory eosinophilic diseases: CRSwNP and SA-EP
SGC use in CRSwNP and asthma is restricted by guidelines for the management of exacerbations and as a last resort when no other treatment options are available. During worsening of symptoms, the experts would prescribe a 7–21 day cycle of SGC for adults (40–50 mg of prednisone or equivalent per day, depending on patient’s weight) (39, 44–46). If the patient responds, treatment can be discontinued without tapering. As the risk of serious AEs increases with the number of cycles and cumulative dose, it was agreed that these patients should not be prescribed more than 2 cycles/year (38).
Additional research is still needed to determine the minimal effective dose and duration of SGC therapy for the treatment of CRSwNP to prevent the development of AEs (23, 47). Despite evidence that short courses of SGC can ameliorate the symptoms and reduce polyp size in patients with CRSwNP, the beneficial effects are short lived once discontinued (8–12 weeks when used in combination with topical intranasal corticosteroids) (14, 48). Current guidelines restrict the use of SGC to short courses to manage CRSwNP exacerbations. SGC maintenance treatment is rarely prescribed for this pathology (9, 48, 49).
The Global Initiative for Asthma for the management and prevention of asthma recommends using only short-courses of SGC to manage severe asthma exacerbations in adults: 40–50 mg/day usually for 5–7 days (Evidence Level D) (32). An Expert Consensus on the Tapering of Oral Corticosteroids for the Treatment of Asthma involving 131 international experts agreed that 5–7 days should be the maximal duration for a short course of SGC for treatment of an exacerbation and that the optimal dosage of a short course of SGC should be 0.5 mg/kg/day (33). In situations where SGC maintenance treatment is necessary, they considered ≤ 5 mg/day to be an acceptable maximum threshold. The magnitude of dose reduction and speed of SGC tapering needs to be individualized for each patient (33).
3.2 Use of biologics as an alternative to SGC in eosinophil-related diseases
The benefits of SGC need to be balanced against SGC-associated AEs, which place a large burden on patients and healthcare systems (37, 50). Biologics allow discontinuation or significant dose reduction of SGC and improve SGC stewardship (11).
Monoclonal antibodies against IL-5 (mepolizumab, reslizumab) or the IL-5 receptor (benralizumab) have been approved by the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of eosinophilic asthma. Mepolizumab has also been approved in the USA and the EU for EGPA, HES and CRSwNP. These biological agents reduce the risk of severe exacerbations and are effective glucocorticoid-sparing agents in patients with eosinophil-related diseases (51–53).
3.2.1 Biologics for systemic eosinophilic diseases: EGPA and HES
Biologics are generally considered in non-severe patients with a maintenance dose of prednisone or equivalent that cannot be reduced below 7.5 mg/day OR who have two or more relapses/exacerbations per year requiring higher doses of SGC to induce remission.
In EGPA, the severity of the disease (renal involvement, alveolar hemorrhage, infiltrative cardiomyopathy, mesenteric ischemia, multiple mononeuritis or central nervous involvement) and the presence of poor prognostic factors, such as age > 65 years, serum creatinine > 150 μmol/L, and/or no ear, nose and throat involvement, condition the use of SGC and conventional immunosuppressants such as methotrexate, azathioprine, cyclophosphamide or mycophenolate mofetil (6, 7, 12).
For patients in remission maintenance with non severe-EGPA, 300 mg of mepolizumab every 4 weeks can be added to the standard of care to decrease the risk of flare ups and reduce the use of glucocorticoids (25, 54). The results of a multicenter, double-blind, parallel-group, phase 3 trial, showed that mepolizumab resulted in a significantly higher proportion of participants in remission and a longer remission duration than placebo, allowing to reduce glucocorticoid dosage (25). Results from a retrospective study of a large European EGPA cohort suggested that similar complete response rates could be achieved with 100 mg of mepolizumab every 4 weeks (55). The experts agreed that in patients treated with a combination of SGC, immunosuppressants and mepolizumab, SGC should be withdrawn first and then the immunosuppressants so, if possible, patients remain only on mepolizumab.
For inducing remission in patients with EGPA, there is currently a trial underway that is comparing a mepolizumab-based regimen to conventional therapeutic strategy (SGC alone or in combination with conventional immunosuppressive agents) (NCT05030155).
The use of the anti-CD20 monoclonal antibody rituximab is conditionally recommended in current guidelines to induce remission in patients with active, severe EGPA (7, 40). Ongoing trials will test the potential clinical benefits of using rituximab, reslizumab and benralizumab for the treatment of EGPA (56).
Using biologics early in patients with higher risk of developing SGC-related AEs, such as those with hypertension, diabetes, heart failure, glaucoma, low bone density or immunodeficiency could help to accelerate the withdrawal of immunosuppressants and SGC and thus, prevent these SGC-related and disease-related risks.
In HES, signs of organ damage and/or significant increase of the eosinophil count with a prednisone dose > 10 mg daily is an indication for the addition of other agents (8). While 300 mg mepolizumab has been approved for patients with idiopathic HES and has shown efficacy in decreasing the risk of flares as well as a steroid-sparing therapy (57, 58), other anti-IL-5/anti-IL-5 receptor and anti-CD52 antibody approaches for the treatment of HES remain investigational (8, 59, 60). A phase 3 trial of benralizumab (NCT04191304) is ongoing. The factors predicting response to a given therapy are still largely unknown (61).
Several genetic abnormalities define myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase gene fusions (62). Patients with these abnormalities are not considered to have HES and may benefit from targeted therapies. Patients with FIP1L1- PDGFRA or PDGFRB rearrangements, should be prescribed imatinib mesylate (100mg and 400 mg daily, respectively) as first-line therapy (61).
3.2.2 For respiratory eosinophilic diseases: CRSwNP and SEA-EP
In CRSwNP patients, the experts would consider using a biologic in those who continue to experience severe symptoms after their first surgery. They also agreed with the EPOS 2020 guidelines stating that in patients with bilateral polyps who are not candidates for surgery, at least three of the following criteria should be met for starting a biological: 1) Evidence of type 2 disease; 2) need for at least two courses of SGC per year or continuous use (>3 months) of low-dose SGC or contraindication to SGC; 3) significantly impaired quality of life (SNOT-22 ≥40); 4) anosmia on smell test; 5) diagnosis of comorbid asthma (not necessarily severe) (9).
Up to 60% of patients with CRSwNP experience disease recurrence after surgery (63, 64) and previous treatment with SGC together with other comorbidities is a predictive factor for revision surgeries (65). Operated patients are likely to respond faster to biological treatment due to reduced inflammation (66–68). Furthermore, the use of a biologic after first surgery may avert the need for repeated or revision surgeries (69).
Both dupilumab and mepolizumab have been shown to reduce symptoms, improve quality of life, and reduce the need for SGC and surgery over the course of 1 year of treatment versus placebo (70). Further research into the efficacy of biologics in relation to the timing of surgery, combination approaches, their long-term safety and cost-effectiveness, in the context of patient preferences and goals is required (68).
The use of biologics in severe asthma is well defined in clinical guidelines for managing the disease. GINA and Spanish Asthma Management Guidelines (71) now recommend biological agents as a preferred treatment choice over the use of SGC. Thus, biologics are recommended before chronic SGC in uncontrolled patients (72). Despite the proven reduction in exacerbation rates and SGC-sparing effects in real-life studies (73, 74), biologics are still under-prescribed in most regions in Spain (75, 76).
To target patients who are most likely to benefit from biologics, healthcare professionals should assess: adherence to inhaled treatment, comorbidities (such as CRSwNP, atopic dermatitis, food allergy, sleep apnea, gastroesophageal reflux disease and psychiatric conditions including depression and anxiety), presence of other diseases (especially those that mimic asthma-like symptoms, mainly but not exclusively chronic obstructive pulmonary disease (COPD), heart failure and inducible laryngeal obstruction) and other individual risk factors that might be corrected (such as smoking, allergen exposure, infections, obesity, among others). Ideally, all these factors should be rapidly identified and optimally addressed before considering a biologic.
There is an urgent need for standardized guidelines on the implementation of SGC weaning protocols following biologic initiation in patients with severe asthma (77).
3.3 Measures to prevent AEs
The potential benefits of SGC therapy must be weighed against the risk of AEs in every individual patient. Patients on SGC should be followed carefully to prevent AEs. Early detection of AEs is important in the treatment and management of SGC-related complications (78).
All SGC prescriptions should be discussed among specialists treating individual patients to ensure awareness of other concomitant conditions that may also require SGC (in which case the cumulative dose should be calculated) and also of concomitant medications that could reduce the clearance of SGC by interfering with cytochrome P450 3A4 activity.
In asthma, even a short burst of SGC can be associated with AEs and each SGC prescription results in a cumulative burden, regardless of the dose and duration (79, 80). The risk of adverse outcomes is evident and statistically significant with cumulative SGC exposure of 1 to 2.5 g per year (34).
In the case of respiratory eosinophilic disease, the intake of SGC is sometimes subject to patient self-administration and management, based on previous experiences, and sometimes even according to a self-management written action plan agreed with the treating physician that patients may interpret subjectively and/or not further consult with their doctor in case of rapid improvement. Thus, the cumulative dose may easily exceed the recommended maximum. To avoid this, the experts suggest prescribing smaller amounts of medication at a time and educating patients about the risk of SGC-related AEs (47).
The experts recommend asking patients with severe CRSwNP or SA-EP about self-medications with SGC at each follow-up visit, and developing a written action plan for each patient that clearly indicates what to do in the event of an exacerbation and when to consult a doctor.
The thresholds per year in respiratory disease and per day in systemic disease at which the risks of developing SGC-related AEs drastically outweigh the benefits still need to be established and adjusted for age. Prompt administration of SGC-sparing agents could ensure greater therapeutic success and prevent the risk of developing SGC-related AEs.
Different specialties follow different protocols to prevent SGC-related AEs. Although there are no reports indicating that the AEs of SGC are different between systemic and respiratory eosinophilic diseases, the protocols to prevent AEs are better established for systemic eosinophilic diseases. Patients on recurrent or maintenance SGC require more follow-ups to monitor their body mass index, blood pressure, intraocular pressure, cardiovascular risk factors and glycaemia (81). In addition, to prevent osteoporosis and risk of severe infection or reactivation of chronic infections, the authors recommend following guidelines such as The Spanish Society of Rheumatology’s guidelines for managing patients treated with long-term SGC or the Recommendations for Prevention of Infection in Systemic Autoimmune Rheumatic Diseases (16, 82) (Table 2).
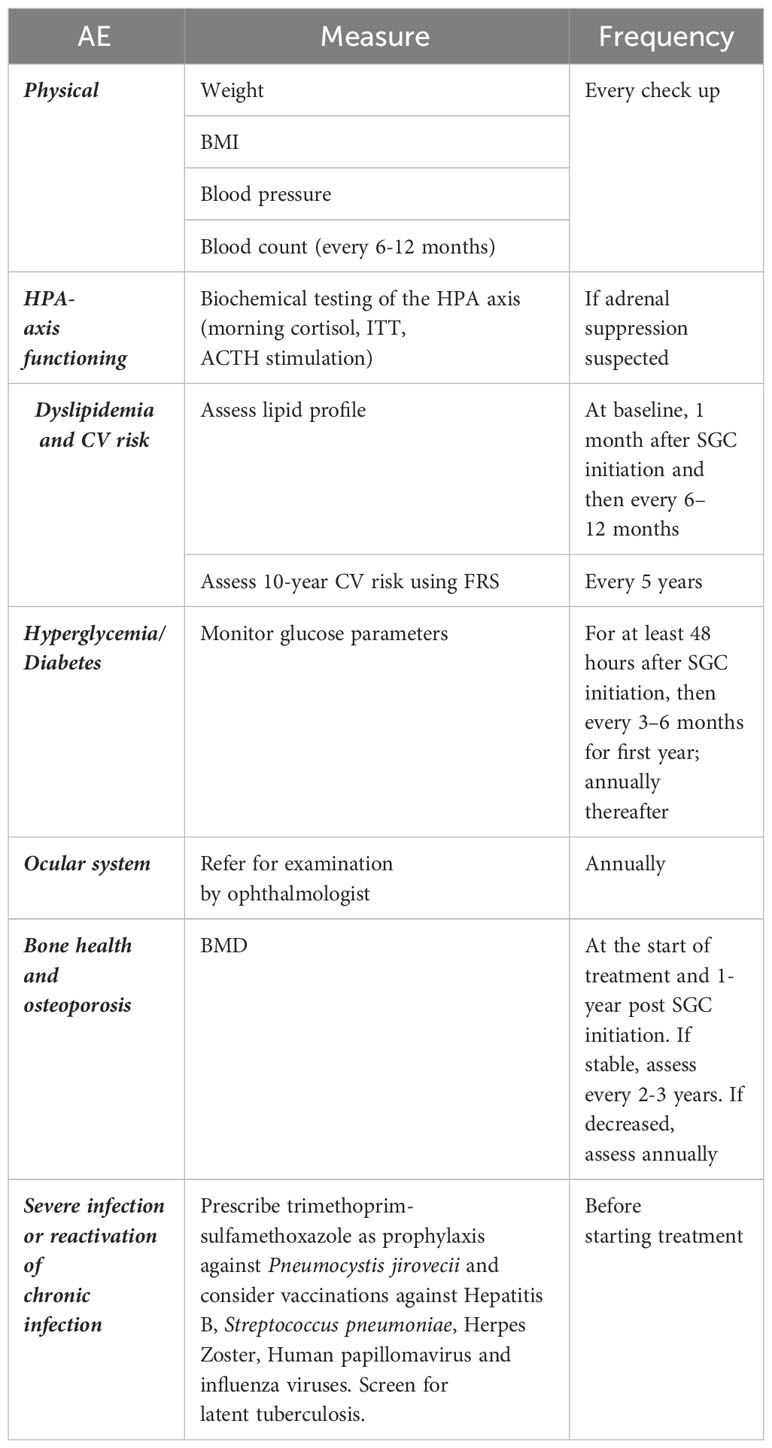
Table 2 Measures to monitor for SGC-related AEs in patients with eosinophil-related diseases.
Up to 40% of individuals taking glucocorticoids develop bone loss over time (83). The Spanish Society of Rheumatology recommends starting pharmacological treatment to prevent osteoporosis in patients receiving ≥ 30 mg/day of prednisone for more than 3 months; in postmenopausal women and men > 50 years of age with low bone mineral density (BMD) receiving doses of prednisone ≥ 5 mg/day for more than 3 months; and in premenopausal women and men < 50 years of age with low BMD receiving doses of prednisone ≥ 7.5 mg/day for more than 3 months (82).
Current guidelines recommend using trimethoprim-sulfamethoxazole as prophylaxis against Pneumocystis jirovecii in patients receiving ≥ 20 mg/day of prednisone; and starting concomitant treatment with antivirals in patients with chronic HBV infection and who are going to receive prednisone or equivalent ≥ 20 mg/day for 4 weeks.
The Glucocorticoid Toxicity Index (GTI) is now in use across a number of diseases, including ANCA-associated vasculitis. The GTI aims to evaluate SGC toxicity and how it changes over time following the introduction of SGC-sparing agents (84, 85). Further knowledge of what constitutes a significant toxicity change could be used as a measure of efficacy of SCS-sparing agents in individual patients, aiding head-to-head comparisons between different drugs.
4 Conclusions
Patients with eosinophil-related diseases require a well-structured and multifaceted treatment approach that considers the presence of co-morbidities, as these can limit the response to treatment or cause similar symptoms or exacerbations.
Treatment recommendations should be interpreted considering the individual patient’s preferences, personal and clinical circumstances, and expectations.
Awareness of the potentially harmful effects of SGC, regardless of the dose, duration or frequency of administration, still needs to be emphasized among healthcare professionals that manage eosinophil-related diseases.
Biologics represent an alternative, well-tolerated option for patients with eosinophilic diseases that allow healthcare professionals to reduce or suspend SGC and avoid the risk of SGC-related AEs. The efficacy and safety of anti-IL-5 therapies, largely derived from their selectivity, have considerably advanced the management of eosinophil-related diseases. An earlier implementation of biological therapies in the course of the disease might help prevent the damage associated with the medium and long-term use of SGC.
Author contributions
VP: Data curation, Investigation, Writing – review & editing. IB: Data curation, Investigation, Writing – review & editing. MJR: Data curation, Investigation, Writing – review & editing. GE-F: Data curation, Investigation, Writing – review & editing. RSL: Data curation, Investigation, Writing – review & editing. JMH-R: Data curation, Investigation, Writing – review & editing. EM: Data curation, Investigation, Writing – review & editing. AC-L: Data curation, Investigation, Writing – review & editing. JLIA: Data curation, Investigation, Writing – review & editing. MSDS: Data curation, Investigation, Writing – review & editing. JM-S: Data curation, Investigation, Writing – review & editing. BA-M: Data curation, Investigation, Writing – review & editing. DB-C: Data curation, Investigation, Writing – review & editing. ALM: Data curation, Investigation, Writing – review & editing. ÍR-F: Data curation, Investigation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The author(s) declare that GSK funded the medical writing support for this manuscript.
Acknowledgments
We would like to thank Mónica Hoyos (medical writer) on behalf of Springer Healthcare Communications. This medical writing assistance was funded by GSK and facilitated by Springer Healthcare.
Conflict of interest
VP has received consulting, speaker fees, grants and support to attend international congresses from AstraZeneca, GSK and Sanofi. IB has received fees from GSK, Novartis, Sanofi, AstraZeneca and Teva for talks at scientific events and as member of advisory boards. MJR has received lecture fees from Novartis, GSK, LETI, Astra-Zéneca, Chiesi and TEVA. GE-F has received consulting fees from GSK and Janssen and support to attend congress from Boehringer Ingelheim. RSL has received consulting fees from GSK and support to attend congresses from Menarini. JMH-R has received honoraria from Amgen, Novartis, Celgene/BMS, Pfizer and GSK and is a member of Novartis, Pfizer, Amgen and Celgene/BMS advisory boards. He has received consulting fees from GSK and research support from Novartis and Celgene/BMS. EM has received consulting fees from GSK. AC-L has received fees in the last 3 years for talks at meetings sponsored by AstraZeneca, Bial, Boehringer Ingelheim, Chiesi, Ferrer, GlaxoSmithKline, MSD, Novartis, Orion Pharma, and Sanofi; travel and attendance expenses for conferences from Bial, Gebro, GlaxoSmithKline, Novartis, and TEVA; and funds/grants for research projects from several state agencies, non-profit foundations, and AstraZeneca and GlaxoSmithKline. JLIA has received fees for consultancy, projects, and talks from AstraZeneca, Bayer, Boehringer Ingelheim, Chiesi, Glaxo, Grifols, Smith Kline, Menarini, Novartis, Orion, Pfizer, Sandoz, and Teva. MSDS has received fees from GSK, Sanofi, MSD and MEDA for talks at scientific events and is a member of advisory boards. JM-S has received fees from GSK, Sanofi, AstraZeneca and Teva for talks at scientific events and as member of advisory boards. BA-M has received grants and research support from Abbvie and Roche, and fees for consulting or participating in company-sponsored speakers bureaus from GSK, Boehringer Ingelheim and Janssen. DB-C and ALM are employees of GSK and hold stocks/shares in GSK. ÍR-F: has received consulting fees from GSK and is on GSK’s advisory board for mepolizumab.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1310211/full#supplementary-material
References
1. Wechsler ME, Munitz A, Ackerman SJ, Drake MG, Jackson DJ, Wardlaw AJ, et al. Eosinophils in health and disease: A state-of-the-art review. Mayo Clin Proc (2021) 96(10):2694–707. doi: 10.1016/j.mayocp.2021.04.025
2. Kovalszki A, Weller PF. Eosinophilia. Prim Care (2016) 43(4):607–17. doi: 10.1016/j.pop.2016.07.010
3. Valent P, Degenfeld-Schonburg L, Sadovnik I, Horny HP, Arock M, Simon HU, et al. Eosinophils and eosinophil-associated disorders: immunological, clinical, and molecular complexity. Semin Immunopathol (2021) 43(3):423–38. doi: 10.1007/s00281-021-00863-y
4. Kuang FL. Approach to patients with eosinophilia. Med Clin North Am (2020) 104(1):1–14. doi: 10.1016/j.mcna.2019.08.005
5. Groh M, Pagnoux C, Baldini C, Bel E, Bottero P, Cottin V, et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss) (EGPA) Consensus Task Force recommendations for evaluation and management. Eur J Intern Med (2015) 26(7):545–53. doi: 10.1016/j.ejim.2015.04.022
6. Yates M, Watts RA, Bajema IM, Cid MC, Crestani B, Hauser T, et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann Rheum Dis (2016) 75(9):1583–94. doi: 10.1136/annrheumdis-2016-209133
7. Chung SA, Langford CA, Maz M, Abril A, Gorelik M, Guyatt G, et al. American college of rheumatology/Vasculitis foundation guideline for the management of antineutrophil cytoplasmic antibody-Associated vasculitis. Arthritis Rheumatol (2021) 73(8):1366–83. doi: 10.1002/art.41773
8. Shomali W, Gotlib J. World Health Organization-defined eosinophilic disorders: 2022 update on diagnosis, risk stratification, and management. Am J Hematol (2022) 97(1):129–48. doi: 10.1002/ajh.26352
9. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology (2020) 58(Suppl S29):1–464. doi: 10.4193/Rhin20.600
10. Scadding GK, Durham SR, Mirakian R, Jones NS, Drake-Lee AB, Ryan D, et al. BSACI guidelines for the management of rhinosinusitis and nasal polyposis. Clin Exp Allergy (2008) 38(2):260–75. doi: 10.1111/j.1365-2222.2007.02889.x
11. Busse WW. Improving systemic corticosteroid stewardship in asthma. Eur Respir J (2022) 60(5). doi: 10.1183/13993003.01440-2022
12. Terrier B, Darbon R, Durel CA, Hachulla E, Karras A, Maillard H, et al. French recommendations for the management of systemic necrotizing vasculitides (polyarteritis nodosa and ANCA-associated vasculitides). Orphanet J Rare Dis (2020) 15(Suppl 2):351. doi: 10.1186/s13023-020-01621-3
13. Scott JR, Ernst HM, Rotenberg BW, Rudmik L, Sowerby LJ. Oral corticosteroid prescribing habits for rhinosinusitis: The American Rhinologic Society membership. Am J Rhinol Allergy (2017) 31(1):22–6. doi: 10.2500/ajra.2017.31.4396
14. De Corso E, Pipolo C, Cantone E, Ottaviano G, Gallo S, Canevari FRM, et al. Survey on use of local and systemic corticosteroids in the management of chronic rhinosinusitis with nasal polyps: identification of unmet clinical needs. J Pers Med (2022) 12(6). doi: 10.3390/jpm12060897
15. Helbig G, Kyrcz-Krzemien S. Diagnostic and therapeutic management in patients with hypereosinophilic syndromes. Pol Arch Med Wewn (2011) 121(1-2):44–52. doi: 10.20452/pamw.1021
16. Rua-Figueroa Fernandez de Larrinoa I, Carreira PE, Brito Garcia N, Diaz Del Campo Fontecha P, Pego Reigosa JM, Gomez Puerta JA, et al. Recommendations for prevention of infection in systemic autoimmune rheumatic diseases. Reumatol Clin (Engl Ed) (2022) 18(6):317–30. doi: 10.1016/j.reumae.2021.04.003
17. Adcock IM, Mumby S. Glucocorticoids. Handb Exp Pharmacol (2017) 237:171–96. doi: 10.1007/164_2016_98
18. Dalal AA, Duh MS, Gozalo L, Robitaille MN, Albers F, Yancey S, et al. Dose-response relationship between long-term systemic corticosteroid use and related complications in patients with severe asthma. J Manag Care Spec Pharm (2016) 22(7):833–47. doi: 10.18553/jmcp.2016.22.7.833
19. Rice JB, White AG, Scarpati LM, Wan G, Nelson WW. Long-term systemic corticosteroid exposure: A systematic literature review. Clin Ther (2017) 39(11):2216–29. doi: 10.1016/j.clinthera.2017.09.011
20. Bourdin A, Adcock I, Berger P, Bonniaud P, Chanson P, Chenivesse C, et al. How can we minimise the use of regular oral corticosteroids in asthma? Eur Respir Rev (2020) 29(155). doi: 10.1183/16000617.0085-2019
21. Katsaounou P, Buhl R, Brusselle G, Pfister P, Martinez R, Wahn U, et al. Omalizumab as alternative to chronic use of oral corticosteroids in severe asthma. Respir Med (2019) 150:51–62. doi: 10.1016/j.rmed.2019.02.003
22. Roufosse F, de Lavareille A, Schandené L, Cogan E, Georgelas A, Wagner L, et al. Mepolizumab as a corticosteroid-sparing agent in lymphocytic variant hypereosinophilic syndrome. J Allergy Clin Immunol (2010) 126(4):828–35.e3. doi: 10.1016/j.jaci.2010.06.049
23. Mansi A, Bui R, Chaaban MR. Oral corticosteroid regimens in the management of chronic rhinosinusitis. Ear Nose Throat J (2022) 101(2):123–30. doi: 10.1177/0145561319876906
24. Mendel A, Ennis D, Carette S, Pagnoux C. Assessment of glucocorticoid tapering in large vessel and anti-neutrophil cytoplasmic antibody-associated vasculitides. Clin Exp Rheumatol (2021) 39 Suppl 129(2):119–24. doi: 10.55563/clinexprheumatol/6spy2c
25. Wechsler ME, Akuthota P, Jayne D, Khoury P, Klion A, Langford CA, et al. Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis. N Engl J Med (2017) 376(20):1921–32. doi: 10.1056/NEJMoa1702079
26. Valent P. Mepolizumab in hypereosinophilic syndromes: proposed therapeutic algorithm. J Allergy Clin Immunol Pract (2022) 10(9):2375–7. doi: 10.1016/j.jaip.2022.06.027
27. FDA approves Nucala as the first and only biologic treatment for Hypereosinophilic Syndrome (HES). GSK (2020). Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-treat-group-rare-blood-disorders-nearly-14-years.
28. European Commission approves Nucala (mepolizumab) in three additional eosinophil-driven diseases. GSK (2021). Available at: https://www.ema.europa.eu/en/documents/product-information/nucala-epar-product-information_en.pdf.
29. McGregor MC, Krings JG, Nair P, Castro M. Role of Biologics in Asthma. Am J Respir Crit Care Med (2019) 199(4):433–45.
30. Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of Disease in Chronic Rhinosinusitis with Nasal Polyps. J Asthma Allergy (2021) 14:127–34.
31. De Corso E, Bilo MB, Matucci A, Seccia V, Braido F, Gelardi M, et al. Personalized Management of Patients with Chronic Rhinosinusitis with Nasal Polyps in Clinical Practice: A Multidisciplinary Consensus Statement. J Pers Med 202212(5).
32. Levy ML, Bacharier LB, Bateman E, Boulet LP, Brightling C, Buhl R, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med (2023) 33(1):7. doi: 10.1038/s41533-023-00330-1
33. Suehs CM, Menzies-Gow A, Price D, Bleecker ER, Canonica GW, Gurnell M, et al. Expert consensus on the tapering of oral corticosteroids for the treatment of asthma. A delphi study. Am J Respir Crit Care Med (2021) 203(7):871–81. doi: 10.1164/rccm.202007-2721OC
34. Price DB, Trudo F, Voorham J, Xu X, Kerkhof M, Ling Zhi Jie J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy (2018) 11:193–204. doi: 10.2147/JAA.S176026
35. Sweeney J, Patterson CC, Menzies-Gow A, Niven RM, Mansur AH, Bucknall C, et al. Comorbidity in severe asthma requiring systemic corticosteroid therapy: cross-sectional data from the Optimum Patient Care Research Database and the British Thoracic Difficult Asthma Registry. Thorax (2016) 71(4):339–46. doi: 10.1136/thoraxjnl-2015-207630
36. Price D, Castro M, Bourdin A, Fucile S, Altman P. Short-course systemic corticosteroids in asthma: striking the balance between efficacy and safety. Eur Respir Rev (2020) 29(155). doi: 10.1183/16000617.0151-2019
37. Pavord ID. Oral corticosteroid-dependent asthma: current knowledge and future needs. Curr Opin Pulm Med (2019) 25(1):51–8. doi: 10.1097/MCP.0000000000000541
38. Zeiger RS, Schatz M, Li Q, Chen W, Khatry DB, Tran TN. Burden of chronic oral corticosteroid use by adults with persistent asthma. J Allergy Clin Immunol Pract (2017) 5(4):1050–60.e9. doi: 10.1016/j.jaip.2016.12.023
39. Bleecker ER, Menzies-Gow AN, Price DB, Bourdin A, Sweet S, Martin AL, et al. Systematic literature review of systemic corticosteroid use for asthma management. Am J Respir Crit Care Med (2020) 201(3):276–93. doi: 10.1164/rccm.201904-0903SO
40. Hellmich B, Sanchez-Alamo B, Schirmer JH, Berti A, Blockmans D, Cid MC, et al. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update. Ann Rheum Dis (2023). doi: 10.1136/ard-2022-223764
41. Luis M, Boers M, Saag K, Buttgereit F, da Silva JAP. The safety of glucocorticoids in the treatment of inflammatory rheumatic disease: new evidence. Curr Opin Rheumatol (2022) 34(3):179–86. doi: 10.1097/BOR.0000000000000870
42. Geetha D, Jin Q, Scott J, Hruskova Z, Hanouneh M, Little MA, et al. Comparisons of guidelines and recommendations on managing antineutrophil cytoplasmic antibody-associated vasculitis. Kidney Int Rep (2018) 3(5):1039–49. doi: 10.1016/j.ekir.2018.05.007
43. Walsh M, Merkel PA, Peh CA, Szpirt WM, Puechal X, Fujimoto S, et al. Plasma exchange and glucocorticoids in severe ANCA-associated vasculitis. N Engl J Med (2020) 382(7):622–31. doi: 10.1056/NEJMoa1803537
44. Edmonds ML, Milan SJ, Brenner BE, Camargo CA Jr., Rowe BH. Inhaled steroids for acute asthma following emergency department discharge. Cochrane Database Syst Rev (2012) 12(12):CD002316. doi: 10.1002/14651858.CD002316.pub2
45. Alobid I, Colas C, Castillo JA, Arismendi E, Del Cuvillo A, Gomez-Outes A, et al. Spanish consensus on the management of chronic rhinosinusitis with nasal polyps (POLIposis NAsal / POLINA 2.0). J Investig Allergol Clin Immunol (2023) 33(5):317–31. doi: 10.18176/jiaci.0910
46. Fokkens WJ, Viskens AS, Backer V, Conti D, De Corso E, Gevaert P, et al. EPOS/EUFOREA update on indication and evaluation of Biologics in Chronic Rhinosinusitis with Nasal Polyps 2023. Rhinology (2023) 61(3):194–202. doi: 10.4193/Rhin22.489
47. Howard BE, Lal D. Oral steroid therapy in chronic rhinosinusitis with and without nasal polyposis. Curr Allergy Asthma Rep (2013) 13(2):236–43. doi: 10.1007/s11882-012-0329-5
48. Orlandi RR, Kingdom TT, Smith TL, Bleier B, DeConde A, Luong AU, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol (2021) 11(3):213–739. doi: 10.1002/alr.22741
49. Hellings PW, Scadding G, Bachert C, Bjermer L, Canonica GW, Cardell LO, et al. EUFOREA treatment algorithm for allergic rhinitis. Rhinology (2020) 58(6):618–22. doi: 10.4193/Rhin20.376
50. Voorham J, Xu X, Price DB, Golam S, Davis J, Zhi Jie Ling J, et al. Healthcare resource utilization and costs associated with incremental systemic corticosteroid exposure in asthma. Allergy (2019) 74(2):273–83. doi: 10.1111/all.13556
51. Bleecker ER, FitzGerald JM, Chanez P, Papi A, Weinstein SF, Barker P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting beta2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet (2016) 388(10056):2115–27. doi: 10.1016/S0140-6736(16)31324-1
52. Castro M, Zangrilli J, Wechsler ME, Bateman ED, Brusselle GG, Bardin P, et al. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir Med (2015) 3(5):355–66. doi: 10.1016/S2213-2600(15)00042-9
53. Nair P, Pizzichini MM, Kjarsgaard M, Inman MD, Efthimiadis A, Pizzichini E, et al. Mepolizumab for prednisone-dependent asthma with sputum eosinophilia. N Engl J Med (2009) 360(10):985–93. doi: 10.1056/NEJMoa0805435
54. Emmi G, Bettiol A, Gelain E, Bajema IM, Berti A, Burns S, et al. Evidence-Based Guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol (2023) 19(6):378–93. doi: 10.1038/s41584-023-00958-w
55. Bettiol A, Urban ML, Dagna L, Cottin V, Franceschini F, Del Giacco S, et al. Mepolizumab for eosinophilic granulomatosis with polyangiitis: A European multicenter observational study. Arthritis Rheumatol (2022) 74(2):295–306. doi: 10.1002/art.41943
56. Uzzo M, Regola F, Trezzi B, Toniati P, Franceschini F, Sinico RA. Novel targets for drug use in eosinophilic granulomatosis with polyangiitis. Front Med (Lausanne) (2021) 8:754434. doi: 10.3389/fmed.2021.754434
57. Chen MM, Roufosse F, Wang SA, Verstovsek S, Durrani SR, Rothenberg ME, et al. An international, retrospective study of off-label biologic use in the treatment of hypereosinophilic syndromes. J Allergy Clin Immunol Pract (2022) 10(5):1217–28 e3. doi: 10.1016/j.jaip.2022.02.006
58. Roufosse F, Kahn JE, Rothenberg ME, Wardlaw AJ, Klion AD, Kirby SY, et al. Efficacy and safety of mepolizumab in hypereosinophilic syndrome: A phase III, randomized, placebo-controlled trial. J Allergy Clin Immunol (2020) 146(6):1397–405. doi: 10.1016/j.jaci.2020.08.037
59. Kim YJ, Prussin C, Martin B, Law MA, Haverty TP, Nutman TB, et al. Rebound eosinophilia after treatment of hypereosinophilic syndrome and eosinophilic gastroenteritis with monoclonal anti-IL-5 antibody SCH55700. J Allergy Clin Immunol (2004) 114(6):1449–55. doi: 10.1016/j.jaci.2004.08.027
61. Klion A. Hypereosinophilic syndrome: approach to treatment in the era of precision medicine. Hematol Am Soc Hematol Educ Program (2018) 2018(1):326–31. doi: 10.1182/asheducation-2018.1.326
62. Khoury JD, Solary E, Abla O, Akkari Y, Alaggio R, Apperley JF, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia (2022) 36(7):1703–19. doi: 10.1038/s41375-022-01613-1
63. Bachert C, Sousa AR, Lund VJ, Scadding GK, Gevaert P, Nasser S, et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J Allergy Clin Immunol (2017) 140(4):1024–31 e14. doi: 10.1016/j.jaci.2017.05.044
64. DeConde AS, Mace JC, Levy JM, Rudmik L, Alt JA, Smith TL. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope (2017) 127(3):550–5. doi: 10.1002/lary.26391
65. Penttila E, Sillanpaa S, Vento SI, Myller J, Koskinen A, Hammaren-Malmi S, et al. Eosinophilia, asthma, NERD and the use of oral corticosteroids predict uncontrolled chronic rhinosinusitis with nasal polyps after surgery. Asian Pac J Allergy Immunol (2021). doi: 10.12932/AP-310321-1102
66. Maza-Solano J, Biadsee A, Sowerby LJ, Calvo-Hernandez C, Tucciarone M, Rocha T, et al. Chronic rhinosinusitis with nasal polyps management in the biologic therapy era: an international YO-IFOS survey. Eur Arch Otorhinolaryngol (2022) 280:2309–16. doi: 10.1007/s00405-022-07762-4
67. Hopkins C, Lund V. Does time from previous surgery predict subsequent treatment failure in Chronic Rhinosinusitis with Nasal Polyps? Rhinology (2021) 59(3):277–83. doi: 10.4193/Rhin21.017
68. Patel GB, Peters AT. The role of biologics in chronic rhinosinusitis with nasal polyps. Ear Nose Throat J (2021) 100(1):44–7. doi: 10.1177/0145561320964653
69. Chandra R. Impact of biologic therapies on surgery for chronic rhinosinusitis with nasal polyposis. Ear Nose Throat J (2021) 100(8):555–6. doi: 10.1177/01455613211034722
70. Bachert C, Han JK, Wagenmann M, Hosemann W, Lee SE, Backer V, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management. J Allergy Clin Immunol (2021) 147(1):29–36. doi: 10.1016/j.jaci.2020.11.013
71. Plaza V, Alobid I, Alvarez C, Blanco M, Ferreira J, Garcia G, et al. Spanish asthma management guidelines (GEMA) VERSION 5.1. Highlights and controversies. Arch Bronconeumol (2022) 58(2):150–8. doi: 10.1016/j.arbres.2021.05.010
72. Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J (2018) 52(4). doi: 10.1183/13993003.00703-2018
73. Pilette C, Canonica GW, Chaudhuri R, Chupp G, Lee FE, Lee JK, et al. REALITI-A study: real-world oral corticosteroid-sparing effect of mepolizumab in severe asthma. J Allergy Clin Immunol Pract (2022) 10(10):2646–56. doi: 10.1016/j.jaip.2022.05.042
74. Casale TB, Burnette A, Bourdin A, Howarth P, Hahn B, Stach-Klysh A, et al. Oral corticosteroid-sparing effects of mepolizumab in severe eosinophilic asthma: evidence from randomized controlled trials and real-world studies. Ther Adv Respir Dis (2022) 16:17534666221107313. doi: 10.1177/17534666221107313
75. Almonacid C, Fitas E, Sanchez-Covisa J, Gutierrez H, Rebollo P. Geographical differences in the use of oral corticosteroids in patients with severe asthma in Spain: heat map based on existing databases analyses. BMC Pulm Med (2023) 23(1):3. doi: 10.1186/s12890-022-02295-2
76. Izquierdo JL, Almonacid C, Campos C, Morena D, Benavent M, Gonzalez-de-Olano D, et al. Systemic corticosteroids in patients with bronchial asthma: A real-life study. J Investig Allergol Clin Immunol (2021) 33(1):30–6. doi: 10.18176/jiaci.0765
77. Lugogo N, Mohan A. Are we poised to change the trajectory of maintenance oral corticosteroid use in severe asthma in the age of biologics? Chest (2022) 162(1):4–5. doi: 10.1016/j.chest.2022.04.004
78. Blakey J, Chung LP, McDonald VM, Ruane L, Gornall J, Barton C, et al. Oral corticosteroids stewardship for asthma in adults and adolescents: A position paper from the Thoracic Society of Australia and New Zealand. Respirology (2021) 26(12):1112–30. doi: 10.1111/resp.14147
79. Chung LP, Upham JW, Bardin PG, Hew M. Rational oral corticosteroid use in adult severe asthma: A narrative review. Respirology (2020) 25(2):161–72. doi: 10.1111/resp.13730
80. Brennan V, Martin-Grace J, Greene G, Heverin K, Mulvey C, McCartan T, et al. The contribution of oral and inhaled glucocorticoids to adrenal insufficiency in asthma. J Allergy Clin Immunol Pract (2022) 10(10):2614–23. doi: 10.1016/j.jaip.2022.05.031
81. Liu D, Ahmet A, Ward L, Krishnamoorthy P, Mandelcorn ED, Leigh R, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol (2013) 9(1):30. doi: 10.1186/1710-1492-9-30
82. Naranjo Hernandez A, Diaz Del Campo Fontecha P, Aguado Acin MP, Arboleya Rodriguez L, Casado Burgos E, Castaneda S, et al. Recommendations by the spanish society of rheumatology on osteoporosis. Reumatol Clin (Engl Ed) (2019) 15(4):188–210. doi: 10.1016/j.reuma.2018.09.004
83. Whittier X, Saag KG. Glucocorticoid-induced osteoporosis. Rheum Dis Clin North Am (2016) 42(1):177–89. doi: 10.1016/j.rdc.2015.08.005
84. McDowell PJ, Stone JH, Heaney LG. The role of quantification of glucocorticoid-associated toxicity in severe asthma. J Cell Immunol (2021) 3(1):31–5. doi: 10.33696/immunology.3.074
Keywords: adverse events, eosinophilic diseases, systemic glucocorticoids, biologics, tapering, treatment optimisation
Citation: del Pozo V, Bobolea I, Rial MJ, Espigol-Frigolé G, Solans Laqué R, Hernández-Rivas JM, Mora E, Crespo-Lessmann A, Izquierdo Alonso JL, Domínguez Sosa MS, Maza-Solano J, Atienza-Mateo B, Bañas-Conejero D, Moure AL and Rúa-Figueroa Í (2024) Expert consensus on the use of systemic glucocorticoids for managing eosinophil-related diseases. Front. Immunol. 14:1310211. doi: 10.3389/fimmu.2023.1310211
Received: 09 October 2023; Accepted: 11 December 2023;
Published: 05 January 2024.
Edited by:
Enrico Heffler, Humanitas University, ItalyReviewed by:
Adriana Sumoza-Toledo, Universidad Veracruzana, MexicoCopyright © 2024 del Pozo, Bobolea, Rial, Espigol-Frigolé, Solans Laqué, Hernández-Rivas, Mora, Crespo-Lessmann, Izquierdo Alonso, Domínguez Sosa, Maza-Solano, Atienza-Mateo, Bañas-Conejero, Moure and Rúa-Figueroa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Astrid Crespo-Lessmann, YWNyZXNwb0BzYW50cGF1LmNhdA==