
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 11 January 2024
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1298583
 Carlo Garaffoni1
Carlo Garaffoni1 Marianna Tamussin1Ilaria Calciolari1Giovanni Lanza2
Marianna Tamussin1Ilaria Calciolari1Giovanni Lanza2 Alessandra Bortoluzzi1
Alessandra Bortoluzzi1 Carlo Alberto Scirè3,4
Carlo Alberto Scirè3,4 Marcello Govoni1*
Marcello Govoni1* Ettore Silvagni1
Ettore Silvagni1Background: Inflammatory arthritis (IAs), such as rheumatoid arthritis (RA) and psoriatic arthritis (PsA), are characterized by the presence of chronic synovitis. The Krenn’s synovitis score (KSS), a simple tool detectable by haematoxylin/eosin staining of synovial biopsy samples, allows the discrimination between high-grade and low-grade synovitis. The aim of this study was to identify the clinical associations of KSS and to evaluate the relationship between high-grade synovitis and treatment response in IA patients.
Methods: Clinical, laboratory and ultrasound data were retrieved from RA and PsA patients recruited in the prospective MATRIX cohort study. Inclusion criteria were age≥18 years, RA or PsA diagnosis, and presence of active disease with eligibility to start/modify therapy. Patients underwent ultrasound-guided synovial biopsy of one of the most involved joints before starting/modifying treatment according to treat-to-target strategy. The samples were analysed by an expert pathologist for KSS calculation. Univariable and multivariable logistic regression analyses were performed to evaluate the relationship between KSS and baseline variables. The association between KSS and treatment response at 24 weeks of follow-up was investigated in univariable logistic regression analysis.
Results: 53 patients, 34 RA and 19 PsA, completed 24 weeks of follow-up after synovial biopsy. Patients were either treatment naïve (N=6, 11%), csDMARDs-experienced (N=46, 87%) or b/tsDMARDs-experienced (N=20, 38%). Median KSS was 6.00 (Q1-Q3 4.00-7.00) in RA and 4.00 (3.00-6.00) in PsA (p=0.040), and inflammatory infiltrates score was significantly higher in RA than in PsA patients (median 3.00 vs 2.00, p=0.021). In multivariable analysis, synovial effusion in the biopsied joint (OR 9.26, 95%CI 2.12-53.91) and erythrocyte sedimentation rate (ESR) (OR 1.04, 95%CI 1.01-1.08) associated with high KSS. High-grade synovitis significantly associated with a higher probability of achieving DAS28 remission, ACR20/50 response, and Boolean2.0 remission, independently from diagnosis.
Conclusion: Several markers of pro-inflammatory pathways associated with the presence of high-grade synovitis, and patients with higher KSS shared a higher probability of treatment targets achievement in the follow up. The integration of a simple and feasible tool like KSS in the clinical and prognostic stratification of patients with IA might help in intercepting patients with a disease more prone to respond to available treatment paradigms.
Chronic inflammatory arthritis (IAs) encompass a variety of diagnostic entities, including rheumatoid arthritis (RA) and psoriatic arthritis (PsA), all characterised by the presence of chronic synovitis, sharing wide within-disease heterogeneity and between-disease common pathogenic processes (1, 2). When inadequately treated or refractory to standard treatments, IAs may lead to disability, impairment of health-related quality of life, and an increase in mortality. To date, treating rheumatologists have access to several effective disease-modifying anti-rheumatic drugs (DMARDs) approved for RA and PsA (conventional synthetic (cs), biological (b), and targeted synthetic (ts) DMARDs) (3, 4). Most treatments are efficacious in different diseases, but still have a relevant proportion of failures, or suboptimal responses (5, 6). Therefore, matching the right drug to the right patient at the right time, though desirable, is a challenging task in chronic IAs treatment. Actual treatment guidelines recommend a stepwise approach in the management, starting from csDMARDs, and moving to b/tsDMARDs, with not yet available validated predictive biomarkers of response (7–9). To this end, clinical, serological and imaging biomarkers have been extensively investigated to optimise outcomes, without achieving satisfactory results so far (10–12).
Synovial membrane is thought to be the primary target of inflammation in RA, and one of the primary targets in PsA, and studies on synovial biomarkers have been undertaken to evaluate the early effects of different drugs and to predict treatment response (13, 14). At present, reduction in CD68-positive macrophages of the sublining (sl) represents the most accepted and validated response biomarker in longitudinal studies in RA, applicable to several types of drugs, while the reduction in CD3+/CD68+sl cells applies to tumour necrosis factor-alpha inhibitors (TNFis) treatment in PsA (13, 15). Relevant advances in the study of synovial membrane in RA have helped in dissecting the heterogeneity of RA synovium, with different pathotypes stratified across patients and phases of the disease (16–23). However, synovial membrane analysis has not yet entered clinical practice to help clinicians in driving therapeutic decisions, and this aspect remains one of the major unmet needs in the field of chronic inflammatory arthritis, with treatment decisions remaining mainly based on the ‘heuristic’ “trials-and-errors” approach (24–26).
Of particular importance in the reporting of the outcome of synovial biopsy examinations, the Krenn’s Synovitis Score (KSS) is a semi-quantitative histopathological scale which, by means of hematoxylin-eosin staining of the synovial tissue samples obtained through biopsy, allows the quantification of the degree of inflammation (27–29). Synovial lining hyperplasia, stromal cell density and inflammatory infiltrate are the three components that are quantified (0 to 3) and added together to obtain the total KSS score (0 to 9). A total score greater than or equal to 5 indicates the presence of high-grade inflammatory synovitis. Although the use of a semi-quantitative synovitis score is suggested by EULAR (European Alliance of Associations for Rheumatology) and OMERACT (Outcome Measures in Rheumatology) (30), to date few studies evaluated the association between KSS and clinical variables in patients with chronic IAs (31, 32). Event though the KSS is a simple, feasible and informative score for describing the inflammatory burden of synovitis, its association with clinical and instrumental patients’ factors, as well as its role in predicting response to DMARDs and guiding therapeutic decisions, remain uncertain (22). Therefore, we conducted this prospective study to analyze (i) the clinical and instrumental variables associated with high-grade KSS and inflammatory infiltrates; (ii) the relation between high-grade KSS and treatment response; and (iii) the association between synovial infiltrate and treatment response in a cohort of IA patients.
The study protocol was approved by the Ethics Committee of Area Vasta Emilia Centro-Emilia-Romagna (698/2020/Sper/AOUFe, approval 05/08/2020). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation and with the Declaration of Helsinki. All subjects provided signed informed consent and were asked to assess the burden of the intervention.
The MATRIX study is a prospective, experimental, multicentre, diagnostic accuracy study. Here, we provided data from a post hoc analysis assessing the prognostic role of KSS.
Patients with IA attending the Rheumatology Unit, Department of Medical Sciences, University of Ferrara and Azienda Ospedaliero - Universitaria S.Anna, Cona (FE), meeting the following inclusion criteria, were eligible for this study: (i) confirmed diagnosis of RA (33) or PsA (34); (ii) age greater than or equal to 18 years; (iii) active peripheral synovitis; (iv) potential indication to start/modify therapy; (v) ultrasound-guided synovial biopsy of one of the most involved synovial joints; (v) availability of 24-week follow up data; (vi) written informed consent provided. Exclusion criteria were: (i) contraindication to start/modify therapy; (ii) contraindication to synovial biopsy; (iii) treatment with intra-articular steroids within the previous month; (iv) patients with dementia or an altered mental state that would have precluded the understanding and rendering of informed consent.
Ultrasound-guided synovial biopsy was performed at the Rheumatology Unit, Department of Medical Sciences, University of Ferrara and Azienda Ospedaliero - Unversitaria S.Anna, Cona (FE), as part of a comprehensive clinical assessment of active IA patients (‘Refractory Arthritis Clinic’), encompassing clinical evaluation, musculoskeletal ultrasound assessment, joint radiographic assessment, and synovial histopathological evaluation, scored according to KSS for chronic synovitis (27). After 15 days from the ultrasound-guided synovial biopsy procedure, patients started/modified DMARDs therapy following the therapeutic indications of the treating rheumatologist, according to international recommendations (7, 9) and regular clinical practice.
Data captured only at basal visit included:
● Demographic variables (gender, date of birth, ethnicity);
● Lifestyles: smoking habits, alcohol use, physical activity, body mass index (BMI);
● Medical history: comorbidities;
● Disease classification according to EULAR/American College of Rheumatology (ACR) criteria for RA (33), CASPAR criteria for PsA (34) and date of diagnosis; Moll and Wright subgroups (35), serological status (rheumatoid factor, RF, and anti-citrullinated protein antibodies, ACPAs);
● Global OMERACT–EULAR Synovitis Score (GLOESS) for RA patients (36)
● Previous treatment history;
● Patient’s pain, stiffness and swelling of the biopsied joint (0-100).
At baseline and follow up visit (24 weeks), a standard clinical assessment was performed, in order to evaluate clinical response, included ACR response (37), Disease Activity Score CRP (DAS28-CRP) response (38) and ACR/EULAR Remission Criteria 2.0 (39), including:
● Health Assessment Questionnaire–Disability Index (HAQ-DI) (40);
● Patient global activity (PGA);
● Global Health (GH);
● Global pain visual analogic scale (VAS Pain);
● Physician global assessment (PhGA);
● Joint count;
● Disease Activity in PSoriatic Arthritis (DAPSA) Score (41);
● Ultrasound assessment of the biopsied joint (42);
● Erythrocytes sedimentation rate (ESR) and C-reactive protein (CRP);
● Ongoing treatment and treatment modification;
● Adverse events (AEs).
Ultrasound examination was performed by experienced rheumatologists and musculoskeletal ultrasonographers (CG, CS, ES), using a commercially available real-time scanner (3-18 MHz, Samsung RS80A). The ultrasound assessment of the joint suitable for ultrasound-guided synovial biopsy was scored according to Global OMERACT–EULAR Synovitis Score (GLOESS) score for synovitis (36), considering effusion, synovial hypertrophy and Power Doppler signal. For all the ultrasound examinations, the procedures were performed at room temperature. Smoking or use of nicotine substitutions 12 hours before the examination were not permitted.
Ultrasound-guided biopsies were performed with a 14G guillotine-type biopsy-needle (Precisa 1410-HS or Precisa 1415-HS, Hospital Service Spa) for the knee joint, or a 18G guillotine-type biopsy-needle (Precisa 1810-HS, Hospital Service Spa) for the wrist joint, according to recommended procedures (30, 43–45). During each procedure, 6-to-8 fragments were retrieved per joint to guarantee an adequate material for the histological analysis.
Data were recorded using a secure electronic data capture database for IA patients (https://www.redcap.ospfe.it) (46), hosted at the University Hospital of Ferrara.
Histopathological evaluation was scored by a single expert pathologist (GL) according to KSS (27). Tissue samples were fixed in formalin for 24h, embedded in paraffin and stained with haematoxylin/eosin for routine histology. Histopathological evaluation was performed according to the pathologist’s experience and scored accordingly, following KSS, for (i) enlargement of the synovial lining cell layer, (ii) density of the resident cells, (iii) inflammatory infiltrate (Supplementary Table S1). At least two sequential sections for each patient were evaluated, and the highest score obtained was recorded. Globally, the sum of the values for each parameter was summarized as follows: a score of 0–1 (no synovitis), 2–4 (low-grade synovitis), and 5–9 (high-grade synovitis). The pathologist (GL) was unaware of the patients’ clinical and immunologic characteristics.
The results of the descriptive analyses were presented as mean and standard deviation (SD) or median and interquartile range (Q1-Q3) for continuous variables, according to their distribution. Qualitative variables were reported as frequencies and percentages. T test or non-parametric Wilcoxon rank sum test were used for descriptive analysis of continuous variables, assessing the normality of the variable distributions with graphical inspection of histograms and Q-Q plots. The comparison between-group of qualitative variables was performed with Chi-square test or Fisher’s exact test. The association between high-grade synovitis (KSS≥5) and relevant clinical variables was assessed in an exploratory univariable logistic regression analysis. Then, variables with significance level <0.10 were included in multivariable model and the selection of covariates was conducted with the backward stepwise method. The same analysis was repeated considering as dependent variable the presence of Krenn’s inflammatory infiltrates score equal to three. Univariable logistic regression models for prediction of response to therapy were fitted with high-grade synovitis and Krenn’s infiltrates as explanatory variables. Response to therapy was defined as DAS28-CRP<2.6, Boolean2.0 remission criteria, ACR20 or ACR50 response criteria (24 weeks). Finally, multivariable models for prediction of response were fitted by adding diagnosis as a covariate. The statistical analyses and the generation of the graphs were performed using RStudio© software (47).
53 patients (34 RA and 19 PsA) who underwent ultrasound-guided synovial biopsy were enrolled between 14th September 2020 and 1st September 2022. The synovial biopsy was performed in 20 right knees, 31 left knees and 2 left wrists. The procedure was well tolerated and only 2 patients reported minor AEs (one patient had lipothymia during the procedure and one experienced an acute worsening of the arthritis in the biopsied joint during the week after the biopsy). Table 1 shows the baseline characteristics of IAs patients included. RA patients were more frequently female (76% vs 32%, p=0.003), and they had a lower average weight (mean ± SD 71 ±16 Vs 81 ±13, p=0.034) and higher mean ESR value compared to PsA patients (42 ±25 Vs 26 ±25, p=0.020). 13/34 (38.2%) RA patients had seronegative disease and 17/34 (50%) had double positivity for RF and ACPA. Patients with moderate or severe disease activity, calculated as DAS28-CRP, were 48/53 (90.4% of patients); using the other definitions, 98.1% of the patients had moderate-to-severe disease activity according to SDAI and 96.2% to CDAI. Regarding the treatment history, 47/53 (89%) patients had failed at least one DMARDs therapy before the synovial biopsy. Specifically, 6/53 patients were DMARDs-naïve (11%), 46/53 previously failed at least one csDMARDs treatment line (87%), 20 (38%) have previously failed at least one b/tsDMARDs treatment line, of whom 17 failed TNF inhibitors (TNFis) and one failed a tsDMARD.
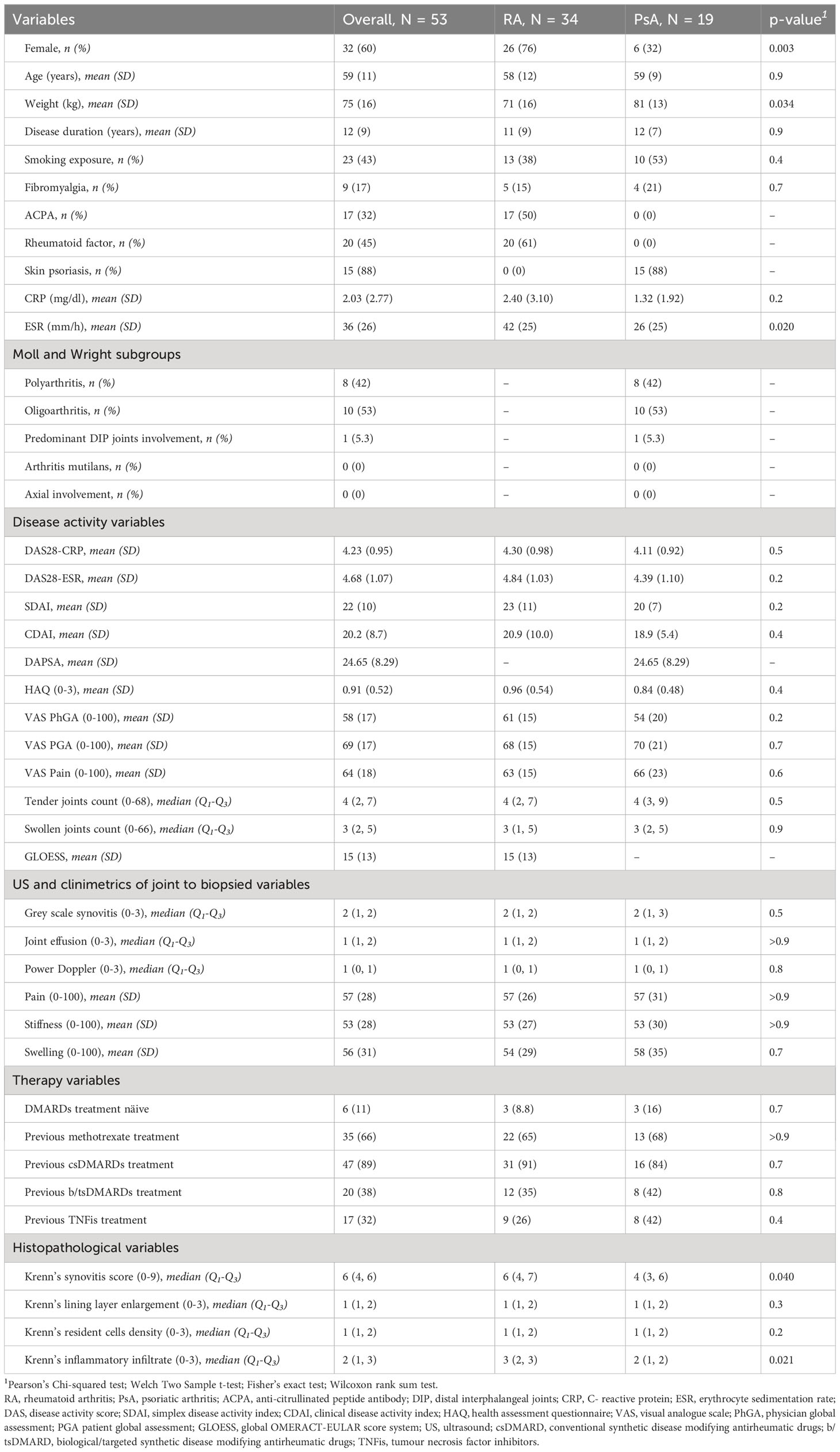
Table 1 Baseline characteristic of the 53 enrolled patients grouped by diagnosis.
KSS was calculated for 50 patients (3 synovial samples were judged inadequate for histological examination). The median KSS was 6 (Q1-Q3 4-6) and high-grade synovitis was found in 30/50 (60%) patients, with higher frequency in RA over PsA patients (RA 67.6% vs PsA 36.8%, p=0.047). Moreover, RA patients showed a higher score in inflammatory infiltrates component (p=0.021) (Figure 1).
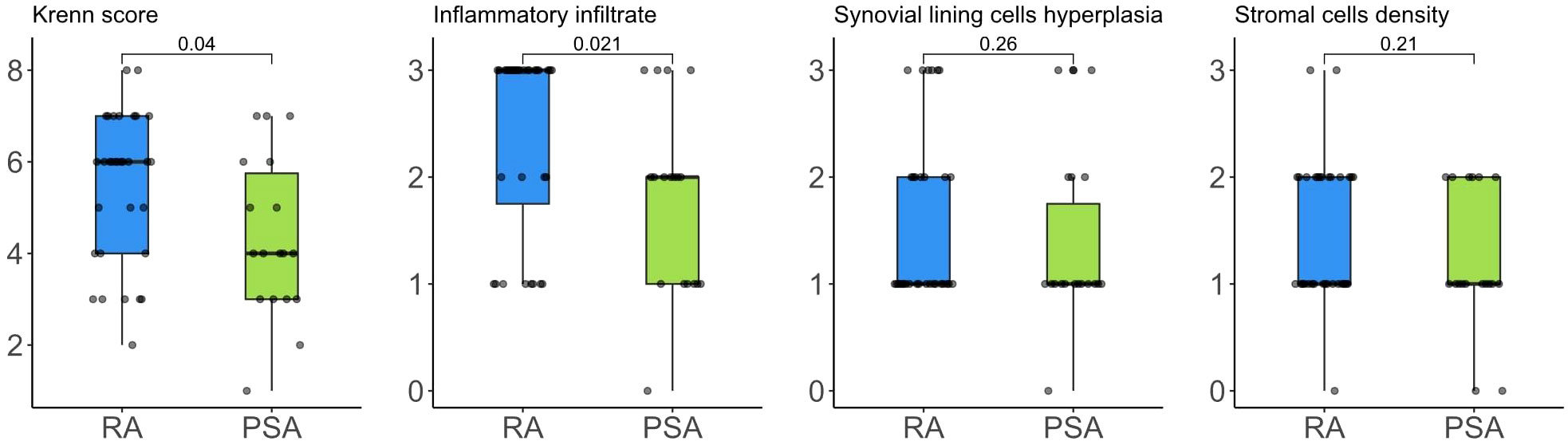
Figure 1 Krenn’s synovitis score and its components distribution in RA e PsA patients.
In univariable logistic regression analysis, ESR (1 mm/h OR 1.04, 95%CI 1.01-1.08), RA diagnosis (OR 4.02, 95%CI 1.22-14.30), DAS28-ESR (OR 2.23, 95%CI 1.16-5.15) associated with higher probability of high-grade KSS at the histological evaluation (Table 2). The detection of positive Power Doppler (PD) signal (OR 3.55, 95%CI 1.08-12.78) and moderate to high synovial effusion (OR 7.56, 95%CI 1.99-37.95) at ultrasound examination of the joint to be biopsied were positively associated to KSS≥5, as well as a greater patient-reported stiffness in the joint to be biopsied (OR 1.03, 95%CI 1.01-1.06). In multivariable analysis, the stepwise backward selection of variables found a stronger association for the ultrasound synovial effusion (OR 9.26, 95%CI 2.12-53.91) and ESR (1 mm/h OR 1.04, 95%CI 1.01-1.08).

Table 2 Univariable logistic regression analysis for association between high grade synovitis (KSS≥5) and baseline clinical variables.
We assessed the association between high Krenn’s inflammatory infiltrates (score =3) and clinical variables in the univariable logistic regression analysis, showing a positive relationship for female gender (OR 4.43, 95%CI 1.33-16.77), ESR (OR 1.03, 95%CI 1.01-1.06), RA diagnosis (OR 5.83, 95%CI 1.66-24.52), DAS28-ESR (OR 2.03, 95%CI 1.09-4.39), joint stiffness (OR 1.03, 95%CI 1.00-1.05) and positive PD signal in the joint to be biopsied (OR 3.33, 95%CI 1.05-11.39) (Table 3). When applying the backward stepwise method, the variables included in the multivariable analysis were RA diagnosis (OR 7.98, 95%CI 2.02-39.53) and joint stiffness (OR 1.03, 95%CI 1.01-1.06).
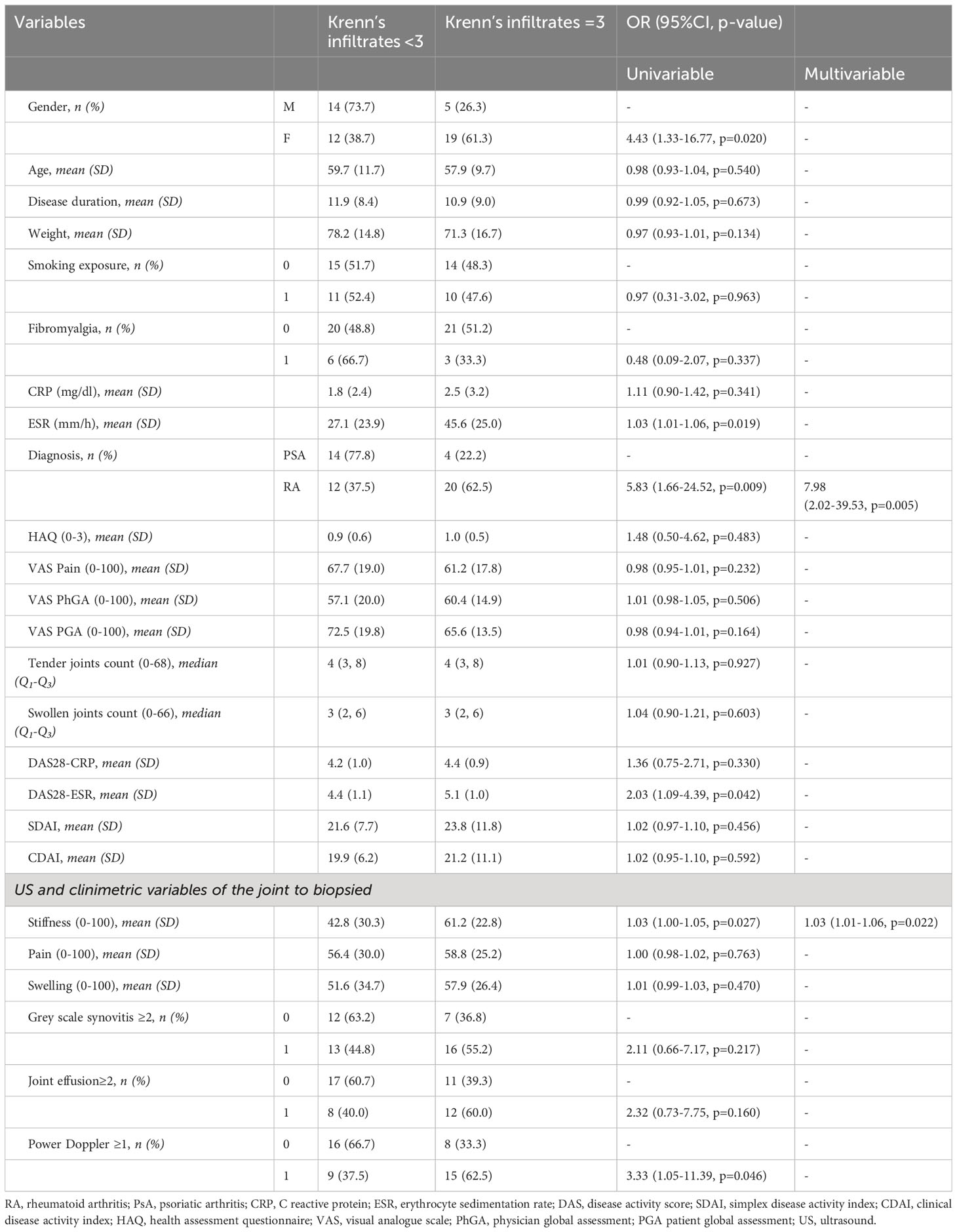
Table 3 Univariable logistic regression analysis for association between high Krenn inflammatory infiltrates score (=3) and baseline clinical variables.
After the synovial biopsy, 38/53 (71.7%) patients started a new b/tsDMARDs therapy and, within these, 6/38 were treated with a Janus Kinases inhibitor (JAKi). The other patients increased the ongoing DMARDs therapy (5/53, 9.4%), started a new csDMARDs (3/53, 5.7%) or were treated with other therapies (i.e., steroid injections, NSAIDs). The patterns of treatment did not significantly differ between patients with high-grade and low-grade synovitis (Table 4).
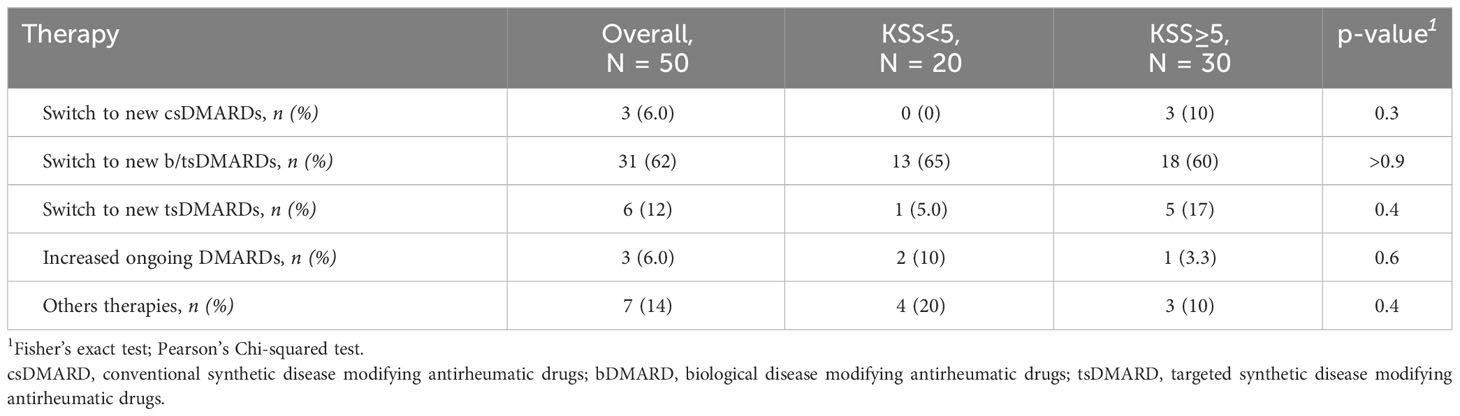
Table 4 Comparison of treatment patterns in patients with high-grade and low-grade synovitis.
At 24 weeks visit, 24/51 (47.1%) patients achieved DAS28-CRP remission, 22/53 (41.5%) ACR20 response, 17/53 (32.1%) ACR50 response and 18/51 (35.3%) Boolean2.0 remission. CRP values at 24 weeks were not available for 2 patients, therefore DAS28 remission and Boolean2.0 criteria were not calculated. Considering PsA patients individually, 5/19 (26,32%) were in remission according to DAPSA (≤4) and 13/19 (68,42%) in DAPSA low disease activity (≤14).
The results of the univariable logistic regression analysis are shown in Figure 2. High-grade KSS significantly associated with higher probability of achieving DAS28-CRP remission (OR 6.14, 95%CI 1.73-26.10), ACR20 response (OR 5.23, 95%CI 1.51-21.79), ACR50 response (OR 4.33, 95%CI 1.15-21.45) and Boolean2.0 remission (OR 7.93, 95%CI 1.83-56.01) criteria (Figure 2). The presence of Krenn’s inflammatory infiltrates score equal to 3 similarly revealed a predictive role in achieving the targets (DAS28-CRP OR 3.31, 95%CI 1.04-11.31, ACR20 3.80, 1.19-13.09, ACR50 5.50, 1.55-23.30, Boolean2.0 remission 5.73, 1.59-24.58). After adjusting the models for diagnosis, the association between high-grade KSS or high Krenn’s inflammatory infiltrates and clinical response to therapy were confirmed independently from diagnosis, apart for the association between high Krenn’s inflammatory infiltrates and DAS28-CRP remission which was not significant (OR 3.36, 95%CI 0.95-13.17, p=0.067) (Supplementary Table S2-S3). Contrariwise, baseline ultrasound features taken individually (positive power Doppler signal, grey scale synovitis score greater than 1 and joint effusions score greater than 1) were not predictive of response and, similarly, baseline clinical variables did not predict the most stringent definitions of response, despite associating with ACR20 (Supplementary Table S4).
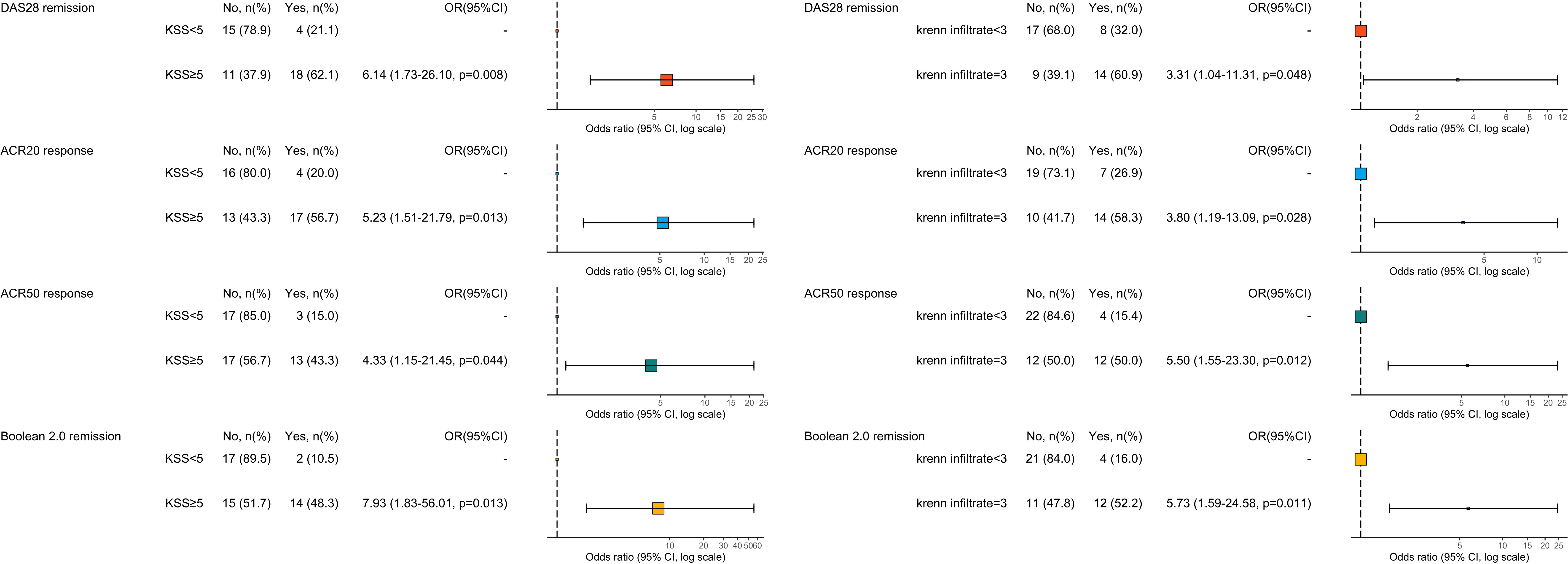
Figure 2 Univariable logistic regression analysis for prediction of response/remission defined by ACR20 response criteria, ACR50 response criteria, Boolean 2.0 remission criteria and DAS28-CRP remission. OR>1 means favour to response, OR<1 means against response. ACR20 and ACR50, American College of Rheumatology response criteria; DAS, disease activity score; KSS, Krenn’s synovitis score; OR, odds ratio.
Among the procedures to be included in the histological reporting of synovial biopsies, semiquantitative scores are suggested, but the clinical role of such scores is still under-recognized and under-reported (30). Here, we investigated the clinical and instrumental determinants of KSS in a prospective cohort of IAs patients, highlighting that several markers of systemic and local inflammation associate with high-grade synovitis, such as ESR, disease activity, PD-positive synovitis, joint effusion and joint stiffness, as well as RA Vs PsA diagnosis. Moreover, we confirmed a predictive role of high-grade KSS and high-grade synovial inflammatory infiltrate score in antedating clinical response to treatment.
Data regarding the clinical determinants of the KSS score are scarce in the literature. In the present study, we demonstrated that pro-inflammatory markers, like ESR, DAS28-ESR, PD-positive synovitis and synovial effusion, associate with high-grade synovitis in IAs. When we focused on the clinical determinants of high Krenn’s inflammatory infiltrates, we demonstrated a significant association with female gender, ESR, DAS28-ESR, joint stiffness and PD-positive synovitis. This partially confirms the available literature data. In patients with long-standing RA (mean disease duration 13.1 years) who underwent isolated synoviectomy or total joint replacement plus synoviectomy or arthrodesis, the KSS reflected disease activity defined by CDAI (31). The same result was obtained in a prospective cohort study with 545 RA and 167 PsA patients, in which DAS28 directly associated with KSS in patients with RA and PsA, both naïve and refractory to treatment with DMARDs (32). Furthermore, DMARDs-naïve RA patients with a disease duration of less than three months had a lower KSS than those with a longer disease duration, but KSS was globally higher in DMARDs-naïve RA than in RA resistant to csDMARDs or in remitting patients. Again, the PD-score in the biopsied joint directly correlated with KSS in both RA and PsA patients (32). In another dataset of patients with early and long-standing RA, the KSS correlated with both the EULAR-OMERACT ultrasound combined score and with the RAMRIS MRI synovitis score (48). However, no compelling association has been already confirmed, suggesting that the informative potential of KSS could not be easily inferred from ultrasound or clinical features. In our cohort of patients with active disease, RA patients had higher median KSS and Krenn’s inflammatory infiltrates than PsA patients; this was not confirmed by other authors (49). With respect to the higher prevalence of female gender among high inflammatory infiltrates scores, the notion of a worse course of the disease in females with RA and PsA is not new (50, 51). Our findings agree with the notion that, whichever inflammatory pathways are involved, high grade synovitis is the result of an active disease, independently from diagnosis. This concept, worthy of further investigation, is partially innovative for rheumatology. Based on this assumption, we could hypothesize that high-grade chronic synovitis, as an expression of the target organ involvement, is transversal to disease classification, and focusing on KSS might serve as a useful information tool for disease stratification especially in the prognostic phase and in prediction of the therapeutic response (52).
Specifically, the role of KSS in predicting response to therapy is debated. The work by Alivernini et al. showed that the presence of a low-grade KSS at baseline predicts a higher response rate to DMARDs (defined as DAS28 remission at 6 months) in treatment-naive RA patients (32). In the R4RA randomized trial, the KSS was not able to discriminate patients who were responders to either tocilizumab or rituximab after the failure of at least one bDMARD (22). In a different and more variegated population, we demonstrated that a high KSS associated with response to therapy according to several definitions, like DAS28-CRP remission, Boolean2.0 remission, ACR20 and ACR50. This was demonstrated also for high Krenn’s inflammatory infiltrates, and independently from diagnosis. We analyzed the single components of the ACR20 response criteria, and none emerged over the others in justifying the absence of response (Supplementary Table S5), so we can summarize that disease activity still persisted in this group of patients. Thus, we hypothesize that, in patients with high-grade KSS, several treatment paradigms (cs/b/tsDMARDs) might permit the achievement of the treatment target, while for patients with low-grade synovitis this remains more difficult. From a speculative point of view, it is possible that high-grade KSS is characterized by a greater involvement of pro-inflammatory pathways, susceptible to modification by the drugs currently approved for the treatment of RA and PsA, resulting in a greater probability of therapeutic response. Conversely, low-grade KSS might involve different pathogenic mechanisms, such as fibrosis, stromal activation and chronic pain phenomena, less susceptible to response via inhibition of the pathways interceptable with the currently available therapies. And this was confirmed, at least partially, with the definition of the ‘synovial pathotypes’ concept. After the initial definition of Dennis et al. derived from patients with long standing RA undergoing arthroplasty or synoviectomy (16), the systematic application of this concept using immunohistochemistry (IHC) to an early RA population (Pathobiology of Early Arthritis Cohort, PEAC) undergoing ultrasound-guided synovial biopsy led to the definition of the ‘diffuse myeloid’, ‘lymphomyeloid’ and ‘pauci-immune’ pathotypes (17–19). This concept was also explored in populations with RA refractory to csDMARDs (21, 53). Studies assessing the prognostic role of synovial pathotypes suggest that TNF-dependent inflammatory pathways are involved in the activation of fibroblast-like synoviocytes (FLS) and enhancement of T cells/FLS interactions, mostly evident in lymphoid pathotypes (23). Myeloid- and lymphoid-associated gene signatures associate with response to rituximab or tocilizumab (20), while, on the other hand, a pauci-immune-fibroid pathotype, which is characterized by low immune cells infiltration, associated with worse response to csDMARDs and TNFis (18, 21). With well-defined treatment schedules for patients with early RA and PsA, and in presence of an acceptable cost-effectiveness profile of first-line methotrexate (MTX) boundary for both the pathologies, a concept like the one explored in our study might apply more appropriately to difficult-to-treat diseases (54, 55). Here, the characterization of the synovial tissue should inform on whether the disease is still supported by a pro-inflammatory movens (e.g. high-grade synovitis) that could be targeted by one of the available therapies, included JAKis, or, conversely, by other non-inflammatory pathways which could belong to low-grade synovitis spectrum (56). Specifically, it remains actually not known the best treatment strategy to adopt for patients with refractory RA deemed to be ‘non-inflammatory’ (NIRRA). Since a treatment-delay for first-line MTX start does not impact on the future development of NIRRA, while its very-early adoption prevents the persistent-inflammatory refractory RA (PIRRA) onset (57), the possibility arising is that a niches of patients with a different low-inflammatory disease exists, and a minimally-invasive procedure like ultrasound-guided synovial biopsy may help to disease stratification (58).
To this end, the role of synovial tissue analysis in translational research is rapidly arising, in particular for new drugs development, drugs repurposing, biomarkers discovery. However, several barriers still limit its complete clinical adoption in patients with IAs (12, 14). With regard to histological scores, EULAR and OMERACT advocate the adoption of a synovitis score, like KSS, as part of the reporting of synovial biopsies in synovial tissue research (30). However, few studies still semi-quantitatively evaluated the features of synovial inflammation in IAs, and this applies particularly to PsA. A recent systematic literature review (SLR) reported that none of the studies assessing the synovial effects of approved b/tsDMARDs in PsA adopted the KSS (13). Among the recently-released EULAR points to consider for minimal reporting requirements in synovial tissue research in rheumatology (59), the adoption of well-categorized scores is advocated, since the available literature rarely describes the scoring systems adopted, with several chains of references to previous publications, but not to the original scoring system. This should help in generalizing and validating the outcomes described. Moreover, the EULAR task force suggested that patient disease activity measures or disease stage should be described, since only 62% of the studies included in the SLR reported clinical data, such as disease activity and current therapy (59). Here, we wanted to focus on a population of patients with active IAs, at the time of treatment modification, with a median KSS score correspondent to high-grade synovitis, in order to analyze in detail the role of the KSS to be practically used in the clinics. Secondly, we decided to focus on both RA and PsA patients with peripheral synovitis, since these diseases share common pathogenic pathways that result in similar treatment algorithms and types of drugs. The available literature regarding the contact points between RA and PsA synovitis focused mostly on the differences, highlighting higher values of neovascularization markers, CD163pos macrophages and CD117pos/c-Kitpos mast cells in PsA, with more enlarged lining layer thickness in RA (60–63). However, the majority of synovial studies frequently reported no significant variations in the number and types of cell infiltrates or in the distribution of inflammatory mediators in RA Vs PsA. As recently suggested, a continuum could exist from seropositive RA to seronegative RA and PsA, with comparable CD68pos macrophages and CD3pos T lymphocytes counts, but with higher CD20pos B-cells scores in seropositive RA Vs seronegative RA and PsA (49), and higher CD138pos plasma cells in seronegative RA Vs PsA (64). This justifies the combined analysis of the synovitis score in patients with different diseases (closer-than-expected), who are experiencing an upgrade in similar treatment schedules.
This study has some limitations that should be mentioned. What emerged from this work represents an analysis of a single-center cohort study, with limited sample size. Furthermore, we did not assess the synovial pathotype or the bulk-tissue mRNA expression, which were out of the scope of this study. Other limitations include the lack of external validation in a different cohort, the absence of joint radiographic assessment data, the estimation of KSS by a single pathologist, and the under-representation of non-Caucasian patients. We focused on PsA patients with peripheral synovitis, thus our results cannot be generalizable to the whole PsA disease spectrum (65), and, similarly, no meaningful information can be provided with respect to specific peripheral PsA subsets, like oligoarticular or polyarticular, which share some histological similarities and differences (49, 62). Finally, no robust information is inferable regarding the single mechanisms of action of DMARDs, since we decided to focus on the treatment modification strategy as a whole. However, our study reasonably reflects a population of chronic IA patients and the clinical heterogeneity of presentation of diseases. Moreover, the applicability of an inexpensive score obtained following a minimally invasive well-tolerated procedure represents an advantageous aspect in terms of reproducibility and potential clinical applicability, as it is expected that ultrasound-guided synovial biopsy procedures may spread to several centers, following training programs and research collaborations (66, 67).
In conclusion, we demonstrated that a simple tool like KSS might help in prognostic characterization of chronic IA patients, and high-grade synovitis represents an expression of pro-inflammatory pathways that appear to be interceptable by currently approved treatment algorithms.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comitato Etico Area Vasta Emilia Centro della Regione Emilia-Romagna (CE-AVEC). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft. MT: Data curation, Investigation, Writing – review & editing. IC: Data curation, Investigation, Writing – review & editing. GL: Conceptualization, Data curation, Methodology, Writing – review & editing. AB: Data curation, Investigation, Supervision, Writing – review & editing. CS: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. MG: Conceptualization, Data curation, Investigation, Project administration, Resources, Supervision, Writing – review & editing. ES: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The author declares the present study was partially supported by local funds from the University of Ferrara (Fondo di Ateneo per la Ricerca Scientifica (FAR) UNIFE 2019, CS).
The authors would like to thank the clinicians and nurses of the Rheumatology Unit, Ferrara University, for their help in the clinical evaluation of patients with chronic inflammatory arthropathies.
ES has received research support from AbbVie and Lilly and consulting/speaker’s fees from AbbVie, Galapagos, Lilly, Novartis, Astra-Zeneca and Amgen. MG has received research support from AbbVie, Pfizer and Lilly and consulting/speaker’s fees from AbbVie, Galapagos, Lilly, Alfa-Sigma, Astra-Zeneca and Amgen. AB has received consulting/speaker’s fees from Astra-Zeneca and GSK.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1298583/full#supplementary-material
1. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet (2016) 388:2023–38. doi: 10.1016/S0140-6736(16)30173-8
2. Veale DJ, Fearon U. The pathogenesis of psoriatic arthritis. Lancet (2018) 391:2273–84. doi: 10.1016/S0140-6736(18)30830-4
3. Garaffoni C, Adinolfi A, Bortoluzzi A, Filippou G, Giollo A, Sakellariou G, et al. Novel insights into the management of rheumatoid arthritis: one year in review 2023. Clin Exp Rheumatol (2023). 41(11):2129–41. doi: 10.55563/clinexprheumatol/nat8nl
4. Silvagni E, Bortoluzzi A, Ciancio G, Govoni M. Biological and synthetic target DMARDs in psoriatic arthritis. Pharmacol Res (2019) 149:104473. doi: 10.1016/j.phrs.2019.104473
5. Janke K, Biester K, Krause D, Richter B, Schürmann C, Hirsch K, et al. Comparative effectiveness of biological medicines in rheumatoid arthritis: systematic review and network meta-analysis including aggregate results from reanalysed individual patient data. BMJ (2020) 370:m2288. doi: 10.1136/bmj.m2288
6. Ruyssen-Witrand A, Perry R, Watkins C, Braileanu G, Kumar G, Kiri S, et al. Efficacy and safety of biologics in psoriatic arthritis: a systematic literature review and network meta-analysis. RMD Open (2020) 6:e001117. doi: 10.1136/rmdopen-2019-001117
7. Smolen JS, Landewé RBM, Bergstra SA, Kerschbaumer A, Sepriano A, Aletaha D, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheumatic Dis (2023) 82:3–18. doi: 10.1136/ard-2022-223356
8. Ogdie A, Coates LC, Gladman DD. Treatment guidelines in psoriatic arthritis. Rheumatol (Oxford) (2020) 59:i37–46. doi: 10.1093/rheumatology/kez383
9. Gossec L, Baraliakos X, Kerschbaumer A, de WM, McInnes I, Dougados M, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheumatic Dis (2020) 79:700–12. doi: 10.1136/annrheumdis-2020-217159
10. Lequerré T, Rottenberg P, Derambure C, Cosette P, Vittecoq O. Predictors of treatment response in rheumatoid arthritis. Joint Bone Spine (2019) 86:151–8. doi: 10.1016/j.jbspin.2018.03.018
11. Generali E, Scirè CA, Favalli EG, Selmi C. Biomarkers in psoriatic arthritis: a systematic literature review. Expert Rev Clin Immunol (2016) 12:651–60. doi: 10.1586/1744666X.2016.1147954
12. Silvagni E, Missiroli S, Perrone M, Patergnani S, Boncompagni C, Bortoluzzi A, et al. From bed to bench and back: TNF-α, IL-23/IL-17A, and JAK-dependent inflammation in the pathogenesis of psoriatic synovitis. Front Pharmacol (2021) 12:672515. doi: 10.3389/fphar.2021.672515
13. Ciliento MS, Venturelli V, Schettini N, Bertola R, Garaffoni C, Lanza G, et al. Evaluation of the synovial effects of biological and targeted synthetic DMARDs in patients with psoriatic arthritis: A systematic literature review and meta-analysis. Int J Mol Sci (2023) 24:5006. doi: 10.3390/ijms24055006
14. Rivellese F, Pitzalis C. Cellular and molecular diversity in Rheumatoid Arthritis. Semin Immunol (2021) 58:101519. doi: 10.1016/j.smim.2021.101519
15. Haringman J, Gerlag D, Zwinderman A, Smeets T, Kraan M, Baeten D, et al. Synovial tissue macrophages: a sensitive biomarker for response to treatment in patients with rheumatoid arthritis. Ann Rheum Dis (2005) 64:834–8. doi: 10.1136/ard.2004.029751
16. Dennis G, Holweg CT, Kummerfeld SK, Choy DF, Setiadi AF, Hackney JA, et al. Synovial phenotypes in rheumatoid arthritis correlate with response to biologic therapeutics. Arthritis Res Ther (2014) 16:R90. doi: 10.1186/ar4555
17. Humby F, Lewis M, Ramamoorthi N, Hackney JA, Barnes MR, Bombardieri M, et al. Synovial cellular and molecular signatures stratify clinical response to csDMARD therapy and predict radiographic progression in early rheumatoid arthritis patients. Ann Rheumatic Dis (2019) 78:761–72. doi: 10.1136/annrheumdis-2018-214539
18. Lliso-Ribera G, Humby F, Lewis M, Nerviani A, Mauro D, Rivellese F, et al. Synovial tissue signatures enhance clinical classification and prognostic/treatment response algorithms in early inflammatory arthritis and predict requirement for subsequent biological therapy: results from the pathobiology of early arthritis cohort (PEAC). Ann Rheumatic Dis (2019). 78(12):1642–52. doi: 10.1136/annrheumdis-2019-215751
19. Lewis MJ, Barnes MR, Blighe K, Goldmann K, Rana S, Hackney JA, et al. Molecular portraits of early rheumatoid arthritis identify clinical and treatment response phenotypes. Cell Rep (2019) 28:2455–2470.e5. doi: 10.1016/j.celrep.2019.07.091
20. Humby F, Durez P, Buch MH, Lewis MJ, Rizvi H, Rivellese F, et al. Rituximab versus tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis (R4RA): 16-week outcomes of a stratified, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial. Lancet (2021) 397:305–17. doi: 10.1016/S0140-6736(20)32341-2
21. Nerviani A, Di Cicco M, Mahto A, Lliso-Ribera G, Rivellese F, Thorborn G, et al. A pauci-immune synovial pathotype predicts inadequate response to TNFα-blockade in rheumatoid arthritis patients. Front Immunol (2020) 11:845. doi: 10.3389/fimmu.2020.00845
22. Rivellese F, Surace AEA, Goldmann K, Sciacca E, Çubuk C, Giorli G, et al. Rituximab versus tocilizumab in rheumatoid arthritis: synovial biopsy-based biomarker analysis of the phase 4 R4RA randomized trial. Nat Med (2022) 28:1256–68. doi: 10.1038/s41591-022-01789-0
23. Kugler M, Dellinger M, Kartnig F, Müller L, Preglej T, Heinz LX, et al. Cytokine-directed cellular cross-talk imprints synovial pathotypes in rheumatoid arthritis. Ann Rheumatic Dis (2023) 82:1142–52. doi: 10.1136/ard-2022-223396
24. Small A, Wechalekar MD. Synovial biopsies in inflammatory arthritis: precision medicine in rheumatoid arthritis. Expert Rev Mol Diagnostics (2019). 20(3):315–25. doi: 10.1080/14737159.2020.1707671
25. Triaille C, Lauwerys BR. Synovial tissue: turning the page to precision medicine in arthritis. Front Med (Lausanne) (2019) 6:46. doi: 10.3389/fmed.2019.00046
26. Pitzalis C, Choy EHS, Buch MH. Transforming clinical trials in rheumatology: towards patient-centric precision medicine. Nat Rev Rheumatol (2020). 16(10):590–9. doi: 10.1038/s41584-020-0491-4
27. Krenn V, Morawietz L, Burmester G-R, Kinne RW, Mueller-Ladner U, Muller B, et al. Synovitis score: discrimination between chronic low-grade and high-grade synovitis. Histopathology (2006) 49:358–64. doi: 10.1111/j.1365-2559.2006.02508.x
28. Krenn V, Perino G, Rüther W, Krenn VT, Huber M, Hügle T, et al. 15 years of the histopathological synovitis score, further development and review: A diagnostic score for rheumatology and orthopaedics. Pathol Res Pract (2017) 213:874–81. doi: 10.1016/j.prp.2017.05.005
29. Krenn V, Morawietz L, Häupl T, Neidel J, Petersen I, König A. Grading of chronic synovitis—A histopathological grading system for molecular and diagnostic pathology1. Pathology-Res Pract (2002) 198:317–25. doi: 10.1078/0344-0338-5710261
30. Najm A, Le Goff B, Orr C, Thurlings R, Cañete JD, Humby F, et al. Standardisation of synovial biopsy analyses in rheumatic diseases: a consensus of the EULAR Synovitis and OMERACT Synovial Tissue Biopsy Groups. Arthritis Res Ther (2018) 20:265. doi: 10.1186/s13075-018-1762-1
31. Schmidt T, Najm A, Mussawy H, Burghardt R, Oehler N, Krenn V, et al. General synovitis score and immunologic synovitis score reflect clinical disease activity in patients with advanced stage rheumatoid arthritis. Sci Rep (2019) 9:8448. doi: 10.1038/s41598-019-44895-9
32. Alivernini S, Tolusso B, Gessi M, Gigante MR, Mannocci A, Petricca L, et al. Inclusion of synovial tissue-derived characteristics in a nomogram for the prediction of treatment response in treatment-naive rheumatoid arthritis patients. Arthritis Rheumatol (2021) 73:1601–13. doi: 10.1002/art.41726
33. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatism (2010) 62:2569–81. doi: 10.1002/art.27584
34. Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H, et al. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheumatism (2006) 54:2665–73. doi: 10.1002/art.21972
35. Moll JMH, Wright V. Psoriatic arthritis. Semin Arthritis Rheumatism (1973) 3:55–78. doi: 10.1016/0049-0172(73)90035-8
36. D’Agostino M-A, Wakefield RJ, Berner-Hammer H, Vittecoq O, Filippou G, Balint P, et al. Value of ultrasonography as a marker of early response to abatacept in patients with rheumatoid arthritis and an inadequate response to methotrexate: results from the APPRAISE study. Ann Rheumatic Dis (2016) 75:1763–9. doi: 10.1136/annrheumdis-2015-207709
37. Felson DT, Anderson JJ, Boers M, Bombardier C, Furst D, Goldsmith C, et al. American college of rheumatology preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheumatism (1995) 38:727–35. doi: 10.1002/art.1780380602
38. Wells G, Becker J-C, Teng J, Dougados M, Schiff M, Smolen J, et al. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann Rheum Dis (2009) 68:954–60. doi: 10.1136/ard.2007.084459
39. Studenic P, Aletaha D, de Wit M, Stamm TA, Alasti F, Lacaille D, et al. American college of rheumatology/EULAR remission criteria for rheumatoid arthritis: 2022 revision. Arthritis Rheumatol (2023) 75:15–22. doi: 10.1002/art.42347
40. Husted JA, Gladman DD, Long JA, Farewell VT. A modified version of the Health Assessment Questionnaire (HAQ) for psoriatic arthritis. Clin Exp Rheumatol (1995) 13:439–43.
41. Schoels MM, Aletaha D, Alasti F, Smolen JS. Disease activity in psoriatic arthritis (PsA): defining remission and treatment success using the DAPSA score. Ann Rheumatic Dis (2016) 75:811–8. doi: 10.1136/annrheumdis-2015-207507
42. Wakefield RJ, Balint PV, Szkudlarek M, Filippucci E, Backhaus M, D’Agostino M-A, et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J Rheumatol (2005) 32:2485–7.
43. van de Sande MGH, Gerlag DM, Lodde BM, van Baarsen LGM, Alivernini S, Codullo V, et al. Evaluating antirheumatic treatments using synovial biopsy: a recommendation for standardisation to be used in clinical trials. Ann Rheumatic Dis (2011) 70:423–7. doi: 10.1136/ard.2010.139550
44. Meric De Bellefon L, Lazarou I. US-guided biopsies: overarching principles. Front Med (2019) 6:1. doi: 10.3389/fmed.2019.00001
45. Humby FC. Synovial tissue sampling in rheumatological practice—Past developments and future perspectives. Front Med (2019) 6:4. doi: 10.3389/fmed.2019.00004
46. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J BioMed Inform (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
47. R: The R Project for Statistical Computing. Available at: https://www.r-project.org/ (Accessed August 5, 2022).
48. Just SA, Nielsen C, Werlinrud JC, Larsen PV, Klinkby CS, Schrøder HD, et al. Six-month prospective trial in early and long-standing rheumatoid arthritis: evaluating disease activity in the wrist through sequential synovial histopathological analysis, RAMRIS magnetic resonance score and EULAR-OMERACT ultrasound score. RMD Open (2019) 5:e000951. doi: 10.1136/rmdopen-2019-000951
49. De Stefano L, Bugatti S, Mazzucchelli I, Rossi S, Xoxi B, Bozzalla Cassione E, et al. Synovial and serum B-cell signature of autoantibody-negative rheumatoid arthritis versus autoantibody-positive rheumatoid arthritis and psoriatic arthritis. Rheumatology (2023):kead378. doi: 10.1093/rheumatology/kead378
50. Sokka T, Toloza S, Cutolo M, Kautiainen H, Makinen H, Gogus F, et al. Women, men, and rheumatoid arthritis: analyses of disease activity, disease characteristics, and treatments in the QUEST-RA Study. Arthritis Res Ther (2009) 11:R7. doi: 10.1186/ar2591
51. Duruöz MT, Gezer HH, Nas K, Kılıç E, Sargın B, Kasman SA, et al. Gender-related differences in disease activity and clinical features in patients with peripheral psoriatic arthritis: A multi-center study. Joint Bone Spine (2021) 88:105177. doi: 10.1016/j.jbspin.2021.105177
52. Hosack T, Thomas T, Ravindran R, Uhlig HH, Travis SPL, Buckley CD. Inflammation across tissues: can shared cell biology help design smarter trials? Nat Rev Rheumatol (2023). 19(10):666–74. doi: 10.1038/s41584-023-01007-2
53. Wang J, Conlon D, Rivellese F, Nerviani A, Lewis MJ, Housley W, et al. Synovial inflammatory pathways characterize anti-TNF –responsive rheumatoid arthritis patients. Arthritis Rheumatol (2022) 74:1916–27. doi: 10.1002/art.42295
54. Nagy G, Roodenrijs NM, Welsing PM, Kedves M, Hamar A, van der Goes MC, et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis (2021) 80:31–5. doi: 10.1136/annrheumdis-2020-217344
55. Kumthekar A, Ashrafi M, Deodhar A. Difficult to treat psoriatic arthritis — how should we manage? Clin Rheumatol (2023). 42(9):2251–65. doi: 10.1007/s10067-023-06605-9
56. Buch MH. Defining refractory rheumatoid arthritis. Ann Rheumatic Dis (2018) 77:966–9. doi: 10.1136/annrheumdis-2017-212862
57. Giollo A, Zen M, Larosa M, Astorri D, Salvato M, Calligaro A, et al. Early characterization of difficult-to-treat rheumatoid arthritis by suboptimal initial management: a multicentre cohort study. Rheumatology (2022) 62(6):2083–9. doi: 10.1093/rheumatology/keac563
58. Nagy G, Roodenrijs NMT, Welsing PMJ, Kedves M, Hamar A, van der GMC, et al. EULAR points to consider for the management of difficult-to-treat rheumatoid arthritis. Ann Rheumatic Dis (2021). 81:20–33. doi: 10.1136/annrheumdis-2021-220973
59. Najm A, Costantino F, Alivernini S, Alunno A, Bianchi E, Bignall J, et al. EULAR points to consider for minimal reporting requirements in synovial tissue research in rheumatology. Ann Rheum Dis (2022). 81:1640–6. doi: 10.1136/annrheumdis-2021-221875
60. Noordenbos T, Yeremenko N, Gofita I, van de Sande M, Tak PP, Caňete JD, et al. Interleukin-17-positive mast cells contribute to synovial inflammation in spondylarthritis. Arthritis Rheumatism (2012) 64:99–109. doi: 10.1002/art.33396
61. van Kuijk AWR, Reinders-Blankert P, Smeets TJM, Dijkmans BAC, Tak PP. Detailed analysis of the cell infiltrate and the expression of mediators of synovial inflammation and joint destruction in the synovium of patients with psoriatic arthritis: implications for treatment. Ann Rheumatic Dis (2006) 65:1551–7. doi: 10.1136/ard.2005.050963
62. Kruithof E, Baeten D, De Rycke L, Vandooren B, Foell D, Roth J, et al. Synovial histopathology of psoriatic arthritis, both oligo-and polyarticular, resembles spondyloarthropathy more than it does rheumatoid arthritis. Arthritis Res Ther (2005) 7:R569. doi: 10.1186/ar1698
63. Ambarus CA, Noordenbos T, de Hair MJ, Tak PP, Baeten DL. Intimal lining layer macrophages but not synovial sublining macrophages display an IL-10 polarized-like phenotype in chronic synovitis. Arthritis Res Ther (2012) 14:R74. doi: 10.1186/ar3796
64. Alivernini S, Bruno D, Tolusso B, Bui L, Petricca L, Gigante MR, et al. Differential synovial tissue biomarkers among psoriatic arthritis and rheumatoid factor/anti-citrulline antibody-negative rheumatoid arthritis. Arthritis Res Ther (2019) 21:116. doi: 10.1186/s13075-019-1898-7
65. Najm A, Goodyear CS, McInnes IB, Siebert S. Phenotypic heterogeneity in psoriatic arthritis: towards tissue pathology-based therapy. Nat Rev Rheumatol (2023). 19(3):153–65. doi: 10.1038/s41584-022-00874-5
66. Coletto LA, Marino V, Rizzo C, Verardi L, Bruno D, Rubortone P, et al. Pos0904 intensive training program for ultrasound-guided minimally invasive synovial tissue biopsy procedure on small and large joints in different phases of joint inflammation. Ann Rheumatic Dis (2023) 82:761–1. doi: 10.1136/annrheumdis-2023-eular.3307
Keywords: rheumatoid arthritis, psoriatic arthritis, chronic synovitis, Krenn’s synovitis score, response to therapy
Citation: Garaffoni C, Tamussin M, Calciolari I, Lanza G, Bortoluzzi A, Scirè CA, Govoni M and Silvagni E (2024) High-grade synovitis associates with clinical markers and response to therapy in chronic inflammatory arthritis: post hoc analysis of a synovial biomarkers prospective cohort study. Front. Immunol. 14:1298583. doi: 10.3389/fimmu.2023.1298583
Received: 25 September 2023; Accepted: 26 December 2023;
Published: 11 January 2024.
Edited by:
Maria I. Bokarewa, University of Gothenburg, SwedenReviewed by:
Serena Bugatti, University of Pavia, ItalyCopyright © 2024 Garaffoni, Tamussin, Calciolari, Lanza, Bortoluzzi, Scirè, Govoni and Silvagni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcello Govoni, Z3ZsQHVuaWZlLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.