 Simona Arientová
Simona Arientová Kateřina Matúšková
Kateřina Matúšková Oldřich Bartoš
Oldřich Bartoš Michal Holub
Michal Holub Ondřej Beran
Ondřej Beran- 1Department of Infectious Diseases, First Faculty of Medicine, Charles University and Military University Hospital Prague, Prague, Czechia
- 2Military Health Institute, Military Medical Agency, Prague, Czechia
Although vaccines against COVID-19 are effective tools in preventing severe disease, recent studies have shown enhanced protection after vaccine boosters. The aim of our study was to examine the dynamics and duration of both humoral and cellular immune responses following a three-dose regimen of the BNT162b2 mRNA vaccine. In a longitudinal prospective study we enrolled 86 adults who received the BNT162b2 vaccine, 35 unvaccinated individuals with a history of mild COVID-19 and a control group of 30 healthy SARS-CoV-2 seronegative persons. We assessed the SARS-CoV-2-specific T cell responses and IgG production up to 12 months post the third BNT162b2 dose in 24 subjects. The vaccinated group had significantly higher IgG antibody levels after two doses compared to the convalescent group (p<0.001). After the third dose, IgG levels surged beyond those detected after the second dose (p<0.001). Notably, these elevated IgG levels were maintained 12 months post the third dose. After two doses, specific T cell responses were detected in 87.5% of the vaccinated group. Additionally, there was a significant decrease before the third dose. However, post the third dose, specific T cell responses surged and remained stable up to the 12-month period. Our findings indicate that the BNT162b2 vaccine induces potent and enduring humoral and cellular responses, which are notably enhanced by the third dose and remain persistant without a significant decline a year after the booster. Further research is essential to understand the potential need for subsequent boosters.
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), remains a significant public health threat worldwide (1). Vaccines against COVID-19 are highly efficient tools for the prevention of severe disease and death (2). The mRNA vaccine BNT162b2 (Pfizer-BioNTech) contains the spike protein and has demonstrated high safety and efficacy in studies and clinical practice (3, 4). Similar to other viral infections, SARS-CoV-2-specific humoral and cellular immune responses are important for prevention of the infection, viral dissemination and subsequent clearance of the virus (5). Memory immune responses are also critical in protection against reinfections (6).
Current mRNA vaccines induce a robust antibody immune response, which soon begins to decline (7, 8). Several studies have reported an association between the decrease in circulating antibodies and a higher risk of COVID-19 (9). The contribution of specific T-cellular immunity to protection against SARS-CoV-2 infection has also been documented (10, 11). Vaccination with mRNA vaccines induces the development of specific T cells, but their role in long-term protection against the disease is poorly understood (12).
The viral evolution and development of new variants caused decreasing effectiveness of the immunization and led to booster dose strategies. Recent studies have documented better protection against COVID-19 infection after vaccine boosters, but data about the dynamics and duration of immune responses are scarce (13).
Therefore, the aim of our study was to evaluate the dynamics and duration of humoral and cellular responses after 2-dose BNT162b2 mRNA vaccination and after the third (first booster) dose.
Patients and methods
Study design and participants
A longitudinal prospective study was conducted in the Vaccination Centre of the Department of Infectious Diseases, Military University Hospital Prague. A group of 86 adults, aged over 18 years, vaccinated with 2 doses of the BNT162b2 vaccine was enrolled between January and March 2021. A group of 35 patients with a history of mild COVID-19 (post-COVID-19) and a control group of 30 healthy SARS-CoV-2 seronegative persons were enrolled between May and June 2021. Demographic parameters of all participants are presented in Table 1. A SARS-Co-V-2 infection in the post-COVID group was confirmed by RT-PCR positivity from nasopharyngeal swabs. The individuals had not been vaccinated before the study and their blood samples were taken 1-3 months after their SARS-CoV-2 infection. We analyzed SARS-CoV-2-specific T and B cell immunity in the entire vaccinated group after their second dose and compared it with the post-COVID-19 and control groups. Blood samples for follow-up were taken at these intervals: 8-9 months after the second dose before the third dose (T2), 1 month after the third dose (T3) and 10-12 months after the third dose (T4). The blood draw schedule is depicted in Figure 1. Out of the entire vaccinated cohort, 24 participants fully adhered to the study protocol, allowing us to assess the kinetics of both cellular and humoral immune responses at every scheduled time-point. Sampling continued until December 2022. Notably, the main reasons for participant exclusion were SARS-CoV-2 infections after the second vaccine dose and non-adherence to the study protocol. The study was approved by the Ethics Committee of the Military University Hospital Prague. All participants provided informed consent upon enrollment. The study was conducted in accordance with the last version of the Declaration of Helsinki.
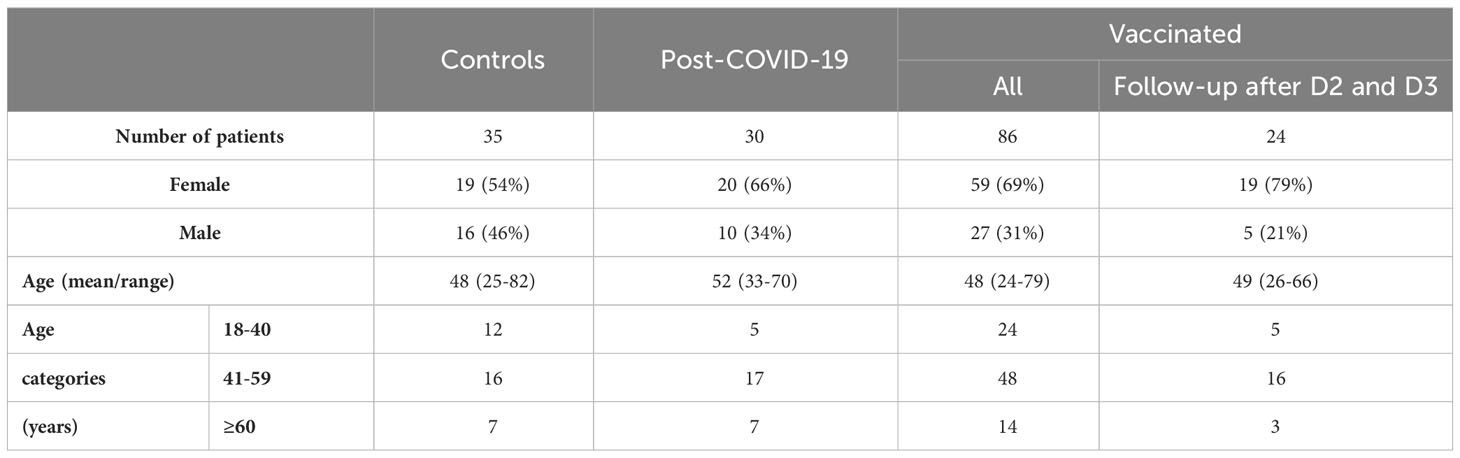
Table 1 Demographic characteristics of the control group (n=30), the post-COVID-19 group (n=35), the group of all vaccinated persons (n=86) and the group of vaccinated subjects who underwent the complete follow-up after receiving the second dose (D2) and the third dose (D3) of the BNT162b2 vaccine (n=24).
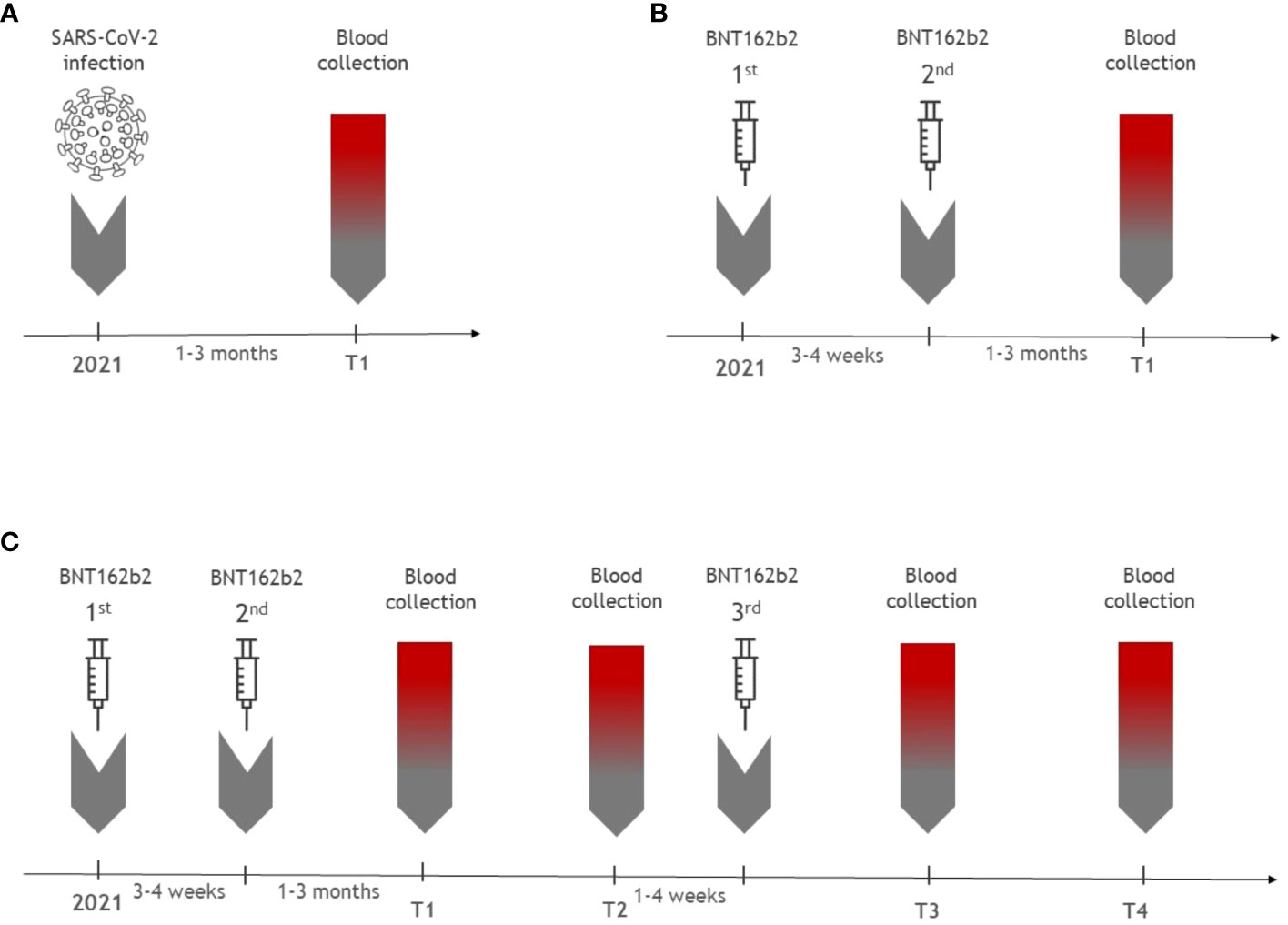
Figure 1 The overview of blood sampling time points (T) in the cohorts. (A) illustrates the timing of the blood draw for 35 patients with a history of mild COVID-19. Samples were collected 1-3 months after SARS-CoV-2 infection (T1). (B) shows blood sampling of the group of 86 vaccinated individuals post their second vaccine dose. (C) provides blood draw schedule for the group of 24 patients who underwent the complete follow-up after receiving all three doses of the mRNA vaccine. Samples were collected 1-3 months after the second dose of the BNT162b2 vaccine (T1), 8-9 months after the second dose (T2), 1 month after the third dose (T3) and 10-12 months after the third dose (T4).
Methods
All peripheral blood samples were collected in VACUETTE® EDTA tubes (Greiner Bio-One, Austria). The fresh samples were processed on the day of collection. Plasma aliquots were immediately frozen at -20 °C and thereafter at -80 °C for subsequent ELISA analyses.
Analysis of SARS-CoV-2-specific T cell immunity
Spike protein-specific T cell responses were evaluated by the Quan-T-Cell SARS-CoV-2 test and Quan-T-Cell ELISA (EuroimmunTM, Luebeck, Germany). The principle of the test is based on the determination of IFN-gamma produced by CD4 and CD8 T cells as well as natural killer cells. The Quan-T-Cell SARS-CoV-2 stimulation tube set consists of three stimulation tubes (BLANK, TUBE, STIM). Fresh human whole blood is incubated in tubes for 24 hours: BLANK: no T cell stimulation, used to determine individual IFN-gamma background, which is subtracted from the following two tubes; TUBE: specific T cell stimulation for SARS-CoV-2 spike protein components of the S1 domain; STIM: nonspecific T cell stimulation to anchored mitogen, used as a positive control. After incubation, all three tubes were centrifuged at 12,000g/10 min at room temperature, and stimulated heparin plasmas were collected in microcentrifuge tubes. Samples were stored in a freezer at -20 °C for a maximum of two months and then measured using a Quan-T-Cell ELISA kit. In accordance with the recommendations from EuroimmunTM, values less than 200 mIU/ml were considered negative, while values greater than 200 mIU/ml were considered positive.
Analysis of SARS-CoV-2-specific humoral immunity
For all participants, plasma samples were stored after blood draw at -80 °C. SARS-CoV-2-specific antibodies were analyzed using Anti-SARS-CoV-2 IgG ELISA test (EuroimmunTM, Luebeck, Germany) according to the manufacturer´s instructions. The results were expressed as binding antibody units (BAU/ml). Samples were considered positive when values were ≥ 33.8 BAU/ml.
Statistical analysis
All statistical analyses were conducted by a certified biostatistician (O.B.) using the R software for statistical computing (R Core Team 2019, Vienna, Austria). We evaluated differences between the study's participant groups based on two primary parameters: sex and age classes. To assess the distribution equality of these parameters across the cohorts, we employed the Fisher's exact test. Data normality was assessed using the Shapiro-Wilk test. To determine any statistically significant differences between defined groups, we used a non-parametric Kruskal-Wallis test followed by pairwise Wilcoxon rank sum tests with corrections for multiple testing (pairwise.wilcox.test). Correlations among individual parameters were evaluated using Pearson's product moment correlation coefficient. In all cases, only p values <0.05 were assumed to be significant.
Results
The cohort of 86 healthy persons with a mean age of 48 years was vaccinated with two doses of the BNT162b2 vaccine. At T1 after the second dose of the vaccine, anti-SARS-CoV-2 IgG antibody levels and specific T cell responses were compared with the group of 35 patients (mean age of 48 years) with a recent history of SARS-CoV-2 infection (mean interval of 2 months). The results of the comparison of the immunological parameters between the groups are shown in Supplementary Figure 1. After the second dose, IgG antibody levels were significantly higher than in the post-COVID-19 group (p<0.001). Specific T cell responses evaluated using the IFN-gamma release assay were not significantly different between the groups. Moreover, a weak correlation was found between humoral and cellular responses (r=0.40, p=0.0003).
A total of 24 vaccinees provided samples at all time points after the second dose (T1 and T2) and after the third dose (T3 and T4). The IgG levels were positive in all vaccinated participants at all time points (Supplementary Table 1). The IgG levels progressively decreased between T1 and T2, but after the first booster dose at T3, IgG titres increased to higher levels than those at T2 (p<0.001, Figure 2). Interestingly, only a nonsignificant decrease in IgG levels was observed between T3 and T4.
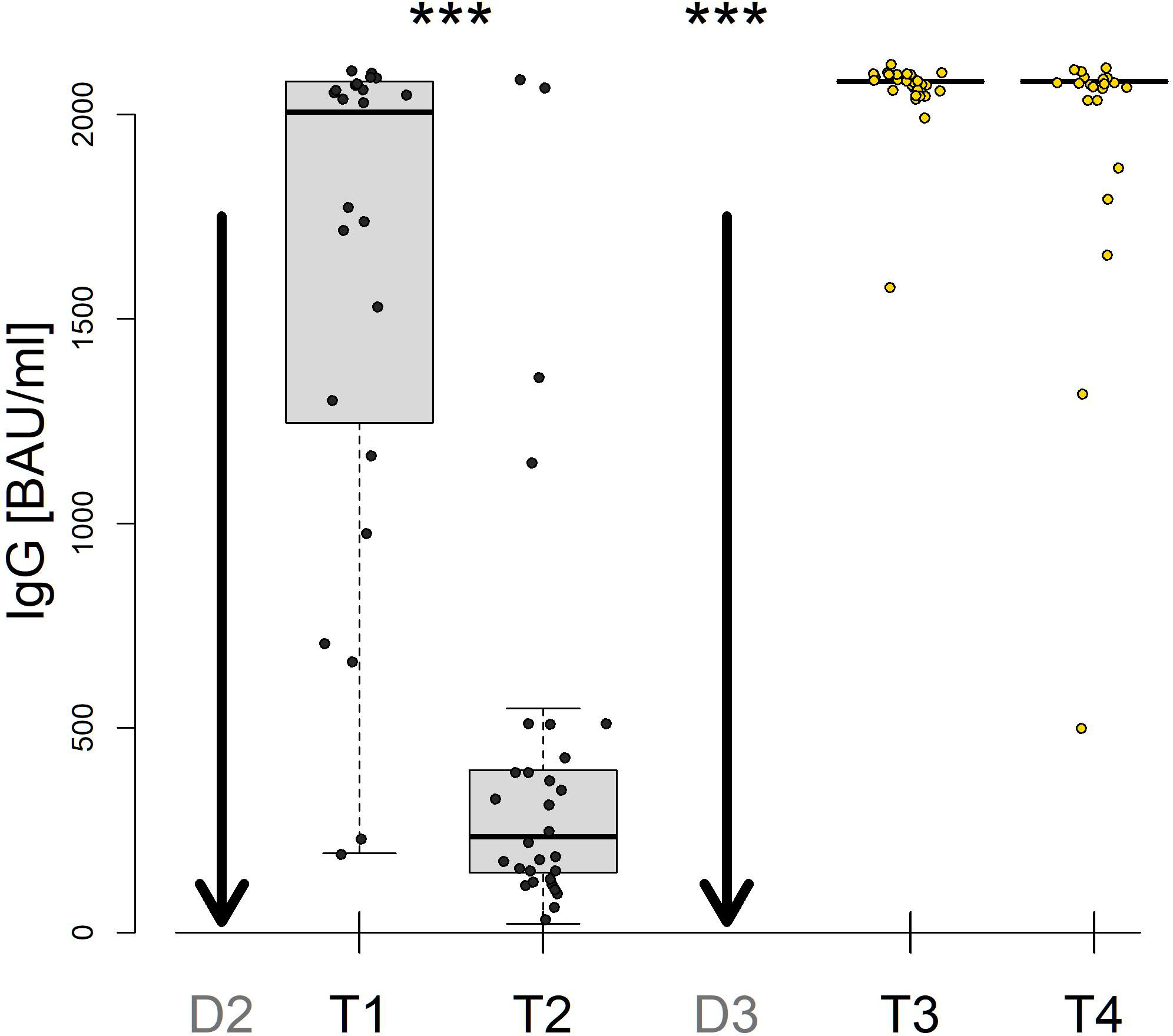
Figure 2 SARS-CoV-2 spike-specific IgG levels after vaccination with the second dose (D2) and the third dose (D3) of the BNT162b2 vaccine. Samples were collected from 24 patients 1-3 months after D2 (T1), 8-9 months after D2 (T2), 1 month after D3 (T3) and 10-12 months after D3 (T4). *** denote P values less than 0.001.
After two doses, specific T cell responses were detected in 21 vaccinated subjects (87.5%) at T1 and T2 (Supplementary Table 1). Additionally, there was a significant decrease before the third dose. However, post the third dose, specific T cell responses surged increased (p<0.001) and remained stable up to the 12 month period (Figure 3). Moreover, in 2 out of the 3 subjects with negative results after the second dose, specific T cell responses developed after the third dose (T3 and T4). One patient was persistantly negative for T cell responses throughout the follow-up.
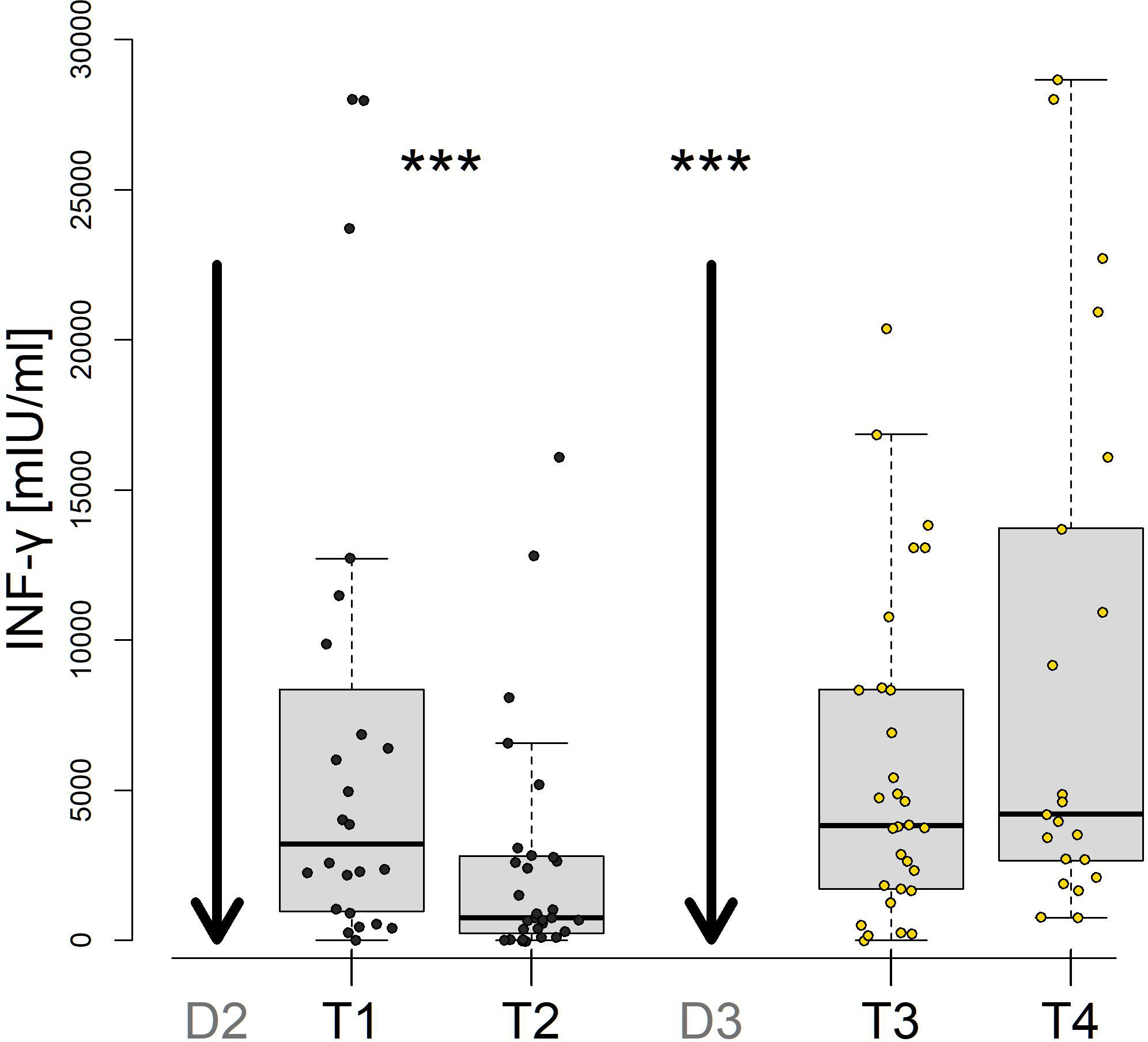
Figure 3 SARS-CoV-2-specific INF-gamma T-cell responses after vaccination with the second dose (D2) and the third dose (D3) of the BNT162b2 vaccine. Samples were collected from 24 patients 1-3 months after D2 (T1), 8-9 months after D2 (T2), 1 month after D3 (T3) and 10-12 months after D3 (T4). *** denote P values less than 0.001.
Discussion
In this study, we evaluated the humoral and cellular immune responses in vaccinated subjects after three doses of the BNT162b2 mRNA vaccine at four time points with a last time point 12 months after the booster dose. The results in this cohort documented a very robust increase in specific IgG levels and a moderate increase in specific T cell responses after the vaccine booster. Both humoral and cellular responses remained stable after the booster up to 12 months of follow-up. Interestingly, postvaccination titres of specific IgG antibodies after the second dose were higher than those in convalescent sera of patients with a mild course of COVID-19. This finding align with a previous study by Hurme et al., which reported elevated IgG levels in healthcare workers who had received two doses of the BNT162b2 vaccine, in comparison to individuals who had recovered from a natural COVID-19 infection (14). Conversely, a study research by Keshavarz et al. indicated that while the BNT162b2 vaccine elicited IgG levels that were lower than those observed in patients hospitalized due to COVID-19, the mRNA-1273 vaccine (Moderna) did not show this trend (15). Such variations can be attributed to multiple factors: timing of measurements, vaccine type, population differences, severity of COVID-19 etc. While B cell responses varied in our study, T cell response levels remained consistent across all groups. Specific IgG levels after immunizations against COVID-19 waned within 5-8 months after the second dose but remained stable after the booster dose. The decrease in humoral immunity after vaccination was shown in previous studies to correlate with age (16). The long-term persistence of high IgG titres after the first booster in our study probably reflects the low mean age of our vaccinated cohort. Moreover, high IgG levels in some persons could be caused by unrecognized exposure to the Omicron variant during 2022. Grikscheit et al. documented that sera from subjects who contracted SARS-CoV-2 Omicron BA.1 after the first or second booster exhibited significantly elevated IgG levels against SARS-CoV-2 Spike-RBD compared to persons vaccinated with a second booster (17). Elevated levels of IgG antibodies after breakthrough infections in previously vaccinated persons were described in other studies (18).
The cellular immune responses, including T cell memory subsets, provide protection against SARS-CoV-2 together with humoral responses (19). Presence of SARS-CoV-2-specific CD4 and CD8 T cells were found to be associated with a decreased severity of COVID-19. Functional memory T cell responses were also detected in vaccinees, and the magnitudes were shown to be comparable to those in convalescent patients. Accordingly, we found similar levels of T cell production of IFN-gamma upon stimulation in vaccinated persons 1-3 months after the second dose and in patients after COVID-19. Similar to the humoral responses, T cell responses waned within the interval after vaccination with the second dose but increased and remained stable after the first booster dose during the follow-up period. Interestingly, three vaccinated persons showed a lack of IFN-gamma production after the second dose with positive IgG levels. Moreover, only one person remained negative for IFN-gamma after the first booster, and the other two subjects converted to moderate positivity of the T cell response.
In conclusion, our findings indicate that the BNT162b2 vaccine induces potent and enduring humoral and cellular responses, which are notably enhanced by the third dose and remain persistant without a significant decline a year after the booster. Further research is essential to understand the potential need for subsequent boosters.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Military University Hospital Prague. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SA: Data curation, Writing – original draft. KM: Methodology, Data curation, Investigation, Writing – original draft. OBa: Data curation, Methodology, Writing – review & editing. MH: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. OBe: Data curation, Conceptualization, Formal Analysis, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the project of the Ministry of Defense of the Czech Republic MO1012 and the project of the Ministry of Interior of the Czech Republic VI04000078.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1271353/full#supplementary-material
Supplementary Figure 1 | Comparison of SARS-CoV-2 INF-gamma T cell responses (A) and SARS-CoV-2-specific spike-specific B-cell responses (B) in patients after a recent SARS-CoV-2 infection (n=35) vs vaccinated persons after two doses of the BNT162b2 vaccine (n=86) and the control group (n=30).
References
1. Tao K, Tzou PL, Nouhin J, Gupta RK, de Oliveira T, Kosakovsky Pond SL, et al. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat Rev Genet (2021) 22(12):757–73. doi: 10.1038/s41576-021-00408-x
2. Thompson MG, Burgess JL, Naleway AL, Tyner H, Yoon SK, Meece J, et al. Prevention and attenuation of Covid-19 with the BNT162b2 and mRNA-1273 vaccines. N Engl J Med (2021) 385(4):320–9. doi: 10.1056/NEJMoa2107058
3. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med (2020) 383(27):2603–15. doi: 10.1056/NEJMoa2034577
4. Graña C, Ghosn L, Evrenoglou T, Jarde A, Minozzi S, Bergman H, et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst Rev (2022) 12(12):CD015477. doi: 10.1002/14651858.CD015477
5. Moss P. The T cell immune response against SARS-CoV-2. Nat Immunol (2022) 23(2):186–93. doi: 10.1038/s41590-021-01122-w
6. Soleimanian S, Alyasin S, Sepahi N, Ghahramani Z, Kanannejad Z, Yaghobi R, et al. An update on protective effectiveness of immune responses after recovery from COVID-19. Front Immunol (2022) 13:884879. doi: 10.3389/fimmu.2022.884879
7. Levin EG, Lustig Y, Cohen C, Fluss R, Indenbaum V, Amit S, et al. Waning immune humoral response to BNT162b2 Covid-19 vaccine over 6 months. N Engl J Med (2021) 385(24):e84. doi: 10.1056/NEJMoa2114583
8. Fedele G, Palmieri A, Malara A, Damiano C, Di Lonardo A, Schiavoni I, et al. A third dose of mRNA COVID-19 vaccine significantly enhances anti-SARS-CoV-2 spike igG response in nursing home residents in Italy. J Am Med Dir Assoc (2022) 23(7):1114–5. doi: 10.1016/j.jamda.2022.05.006
9. Feikin DR, Higdon MM, Abu-Raddad LJ, Andrews N, Araos R, Goldberg Y, et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet (2022) 399(10328):924–44. doi: 10.1016/S0140-6736(22)00152-0
10. Almendro-Vázquez P, Laguna-Goya R, Ruiz-Ruigomez M, Utrero-Rico A, Lalueza A, Maestro de la Calle G, et al. Longitudinal dynamics of SARS-CoV-2-specific cellular and humoral immunity after natural infection or BNT162b2 vaccination. PloS Pathog (2021) 17(12):e1010211. doi: 10.1371/journal.ppat.1010211
11. Schiavoni I, Palmieri A, Olivetta E, Leone P, Di Lonardo A, Mazzoli A, et al. T-cell mediated response after primary and booster SARS-CoV-2 messenger RNA vaccination in nursing home residents. J Am Med Dir Assoc (2023) 24(2):140–147.e2. doi: 10.1016/j.jamda.2022.11.024
12. Bonnet B, Chabrolles H, Archimbaud C, Brebion A, Cosme J, Dutheil F, et al. Decline of humoral and cellular immune responses against SARS-CoV-2 6 months after full BNT162b2 vaccination in hospital healthcare workers. Front Immunol (2022) 13:842912. doi: 10.3389/fimmu.2022.842912
13. Busà R, Sorrentino MC, Russelli G, Amico G, Miceli V, Miele M, et al. Specific anti-SARS-CoV-2 humoral and cellular immune responses after booster dose of BNT162b2 Pfizer-bioNTech mRNA-based vaccine: integrated study of adaptive immune system components. Front Immunol (2022) 13:856657. doi: 10.3389/fimmu.2022.856657
14. Hurme A, Jalkanen P, Heroum J, Liedes O, Vara S, Melin M, et al. Long-lasting T cell responses in BNT162b2 COVID-19 mRNA vaccinees and COVID-19 convalescent patients. Front Immunol (2022) 13:869990. doi: 10.3389/fimmu.2022.869990
15. Keshavarz B, Richards NE, Workman LJ, Patel J, Muehling LM, Canderan G, et al. Trajectory of igG to SARS-CoV-2 after vaccination with BNT162b2 or mRNA-1273 in an employee cohort and comparison with natural infection. Front Immunol (2022) 13:850987. doi: 10.3389/fimmu.2022.850987
16. Ciabattini A, Nardini C, Santoro F, Garagnani P, Franceschi C, Medaglini D. Vaccination in the elderly: The challenge of immune changes with aging. Semin Immunol (2018) 40:83–94. doi: 10.1016/j.smim.2018.10.010
17. Grikscheit K, Rabenau HF, Ghodratian Z, Widera M, Wilhelm A, Toptan Grabmair T, et al. Characterization of the antibody and interferon-gamma release response after a second COVID-19 booster vaccination. Vaccines (Basel) (2022) 10(7):1163. doi: 10.3390/vaccines10071163
18. Ibarrondo FJ, Hofmann C, Ali A, Ayoub P, Kohn DB, Yang OO. Previous infection combined with vaccination produces neutralizing antibodies with potency against SARS-CoV-2 variants. mBio (2021) 12(6):e0265621. doi: 10.1128/mBio.02656-21
Keywords: COVID-19; SARS-CoV-2, vaccination, BNT162b2, humoral immunity, T cell immunity
Citation: Arientová S, Matúšková K, Bartoš O, Holub M and Beran O (2023) Specific immune responses after BNT162b2 mRNA vaccination and COVID-19 infection. Front. Immunol. 14:1271353. doi: 10.3389/fimmu.2023.1271353
Received: 02 August 2023; Accepted: 28 September 2023;
Published: 17 October 2023.
Edited by:
T. Mark Doherty, GlaxoSmithKline, BelgiumReviewed by:
Igor Stoma, Gomel State Medical University, BelarusAnnapina Palmieri, National Institute of Health (ISS), Italy
Copyright © 2023 Arientová, Matúšková, Bartoš, Holub and Beran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ondřej Beran, b25kcmVqLmJlcmFuQGxmMS5jdW5pLmN6
†These authors have contributed equally to this work