
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 27 September 2023
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1252811
This article is part of the Research TopicCancer Immunotherapy in Solid Organ Transplant RecipientsView all 5 articles
 Olaf Penack1,2*
Olaf Penack1,2* Christophe Peczynski2,3,4
Christophe Peczynski2,3,4 Christian Koenecke2,5
Christian Koenecke2,5 Emmanuelle Polge2,3,4Robin Sanderson6
Emmanuelle Polge2,3,4Robin Sanderson6 Ibrahim Yakoub-Agha7Nathalie Fegueux8
Ibrahim Yakoub-Agha7Nathalie Fegueux8 Michael Daskalakis9,10
Michael Daskalakis9,10 Matthew Collin11Peter Dreger12
Matthew Collin11Peter Dreger12 Nicolaus Kröger13
Nicolaus Kröger13 Urs Schanz14Adrian Bloor15
Urs Schanz14Adrian Bloor15 Arnold Ganser16Caroline Besley17,18
Arnold Ganser16Caroline Besley17,18 Gerald G. Wulf19
Gerald G. Wulf19 Urban Novak20Ivan Moiseev2,21
Urban Novak20Ivan Moiseev2,21 Hélène Schoemans2,22
Hélène Schoemans2,22 Grzegorz W. Basak2,23
Grzegorz W. Basak2,23 Christian Chabannon24,25
Christian Chabannon24,25 Anna Sureda26,27Bertram Glass28,29
Anna Sureda26,27Bertram Glass28,29 Zinaida Peric2,30
Zinaida Peric2,30We investigated ≥ grade 3 (CTC-AE) organ toxicities for commercial CD19 chimeric antigen receptor T cell (CAR-T cell) products in 492 patients (Axi-Cel; n = 315; Tisa-Cel; n = 177) with Large B-cell Lymphoma in the European Society for Blood and Marrow Transplantation (EBMT) CAR-T registry. The incidence of ≥ grade 3 organ toxicities during the first 100 days after CAR-T was low and the most frequent were: renal (3.0%), cardiac (2.3%), gastro-intestinal (2.3%) and hepatic (1.8%). The majority occurred within three weeks after CAR-T cell therapy. Overall survival was 83.1% [79.8-86.5; 95% CI] at 3 months and 53.5% [49-58.4; 95% CI] at one year after CAR-T. The most frequent cause of death was tumour progression (85.1%). Non-relapse mortality was 3.1% [2.3-4.1; 95% CI] at 3 months and 5.2% [4.1-6.5; 95% CI] at one year after CAR-T. The most frequent causes of non-relapse mortality were cell-therapy-related toxicities including organ toxicities (6.4% of total deaths) and infections (4.4% of total deaths). Our data demonstrates good safety in the European real-world setting.
CAR-T cells that target CD19 have become standard treatments of relapsed or refractory large B cell lymphoma (rrLBCL) in 3rd line or beyond, and have moved up to 2nd line following the recent reports of two positive randomized trials (1, 2). The safety of CAR-T cells is of major concern, since this new class of anti-tumour therapy may have unknown side effects. The complete risk profile of CD19+ CAR T-cells has not been fully defined by the relatively small registration trials leading to approval of CAR T-cell products. Therefore, health authorities obliged Marketing Authorization Holders (MAH) to report efficacy and toxicity data on predefined numbers of patients treated with commercial CART products in the real world-setting. The EBMT registry that was established forty years ago in Europe to collect data on patients receiving autologous or allogeneic hematopoietic cell transplants, has recently extended its capacity to the capture of long-term follow-up (up to 15 years) of patients treated with CAR-T Cells through the design and implementation of a Cellular Therapy Form (CTF). Primary use of data allows for the conduct of studies such as the one reported in this manuscript, while secondary use of data allows for the conduct of post-authorization safety studies (PASS) and post-authorization efficacy studies (PAES) in partnership with MAH/Pharmas or other stakeholders. Classical side effects of CD19 CAR-T cell products, which are already well described in clinical cohorts, include cytokine release syndrome (CRS), immune cell associated neurotoxicity syndrome (ICANS) and B-cell aplasia. Currently, there is emerging evidence of additional both short-term and medium-term unwanted effects, which were in part unknown at the time of regulatory approval (3–6). There is evidence on neurological events other than ICANS, including ischemic attacks, peripheral neuropathy and Alzheimer’s dementia (7). The patho-mechanism behind this association is not known. In one study major cardiovascular events occurred in 17% of patients till one month after CAR-T cell infusion (8) and in another study frequent adverse events were observed within one year after CAR-T cell infusion (4). The most frequent pulmonary toxicity symptom observed in previous studies was hypoxia, but also pleural effusion, pulmonary embolism, allergic rhinitis and pneumomediastinum were described (4). In a recent study by Wudikarn and colleagues metabolic toxicities after CART have been detected as a frequent complication (4). Typical electrolyte abnormalities were hypokalemia, hypophosphatemia and hypocalcemia. Hyperglycemia and hypoglycemia were also frequent (4, 9, 10).
In the current study, we have used the EBMT CAR-T cell registry (11) to assess the real-world outcome of CD19 CAR-T cell products. Our study aimed at investigating (non-CRS and non-neurotoxicity) organ complications of CD19 CAR-T cell products in adult patients with LBCL reported to the EBMT.
This is a retrospective multicentre analysis using the dataset of the EBMT registry. The EBMT is a not-for-profit professional association uniting more than 600 transplant centres that are required to register and report regular follow up on all consecutive hematopoietic cell transplantations, and since the recent and first approvals in the summer of 2018 of patients treated with approved CAR-T Cells. In the CAR-T cell registry of the EBMT, a growing fraction of commercial CAR-T cell therapies in Europe are registered, and data on outcome is provided. Audits are routinely performed to determine the accuracy of the data. The study was planned and approved by the Transplant Complications Working Party of the EBMT and by the EBMT board. All patients gave their written informed consent to collect, transfer and use their medical information for research purposes. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
Eligibility criteria for this analysis included patients 18 years of age or older undergoing CD19+ CAR-T cell therapy for LBCL before the end of July 2021. Only patients with an available status on organ toxicities during the first 100 days after CAR-T were included. Data on organ toxicities were collected via a form designed for the post-authorization studies on CAR-T cell therapy. In this form, occurrence, time of onset and grading of renal, cardiac, hepatic, gastro-intestinal, skin, pulmonary toxicities, as well as hypogammaglobulinemia are reported. For the current analysis, we have exclusively included the occurrence of grades 3-4 severe toxicities based on CTCAE criteria (12). The full CTCAE criteria are publicly available for download: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf.
Patients were treated with commercial products and had received axicabtagene ciloleucel (Axicel, 64%) or tisagenlecleucel (Tisacel, 36%). Both are autologous anti-CD19 T cell products containing a second-generation CAR. Axicel is generated by transduction of apheresed and immunoselected blood CD3+ lympohocytes with a retroviral vector and contains a CD28 co-stimulatory domain. Tisacel is manufactured with a lentiviral vector, and contains a CD137 (4-1BB) costimulatory domain.
The frequency of severe grade 3-4 organ complications according CTCAE occurring in the first 100 days was given for the following organs: kidney, heart, liver, gut, skin and lungs. The time from CAR-T cell infusion to the occurrence of each complication, as well as the grade of the complication, were also described.
Additional study endpoints were Overall Survival (OS), Progression-Free Survival (PFS), Relapse Incidence (RI) and Non-Relapse Mortality (NRM). Start time was the date of CAR-T cell infusion for all endpoints. NRM was defined as death without relapse/progression, PFS was defined as survival without relapse or progression. Probability of OS and PFS were calculated using the Kaplan-Meier method. Cumulative incidence functions were used to estimate NRM and Relapse Incidence in a competing risk setting, death and relapse competing with each other (13).
Statistical analyses were performed with R 4.1.2 software (R Development Core Team, Vienna, Austria) packages.
We analysed adult patients with LBCL receiving CD19+ CAR-T cell therapy before the end of July 2021 who were reported to the EBMT and had information on organ toxicities. We identified 492 patients fulfilling the inclusion criteria. Population characteristics are shown in Table 1. Since the first CART cells were approved in the summer of 2018, most patients in this study received CAR-T cell infusion in 2019 (42%) or 2020 (45%). The majority of patients were from the United Kingdom, France, Germany or Switzerland. Median age was 61.6 years (range 18.7-81) and 61% were male. Karnofsky performance score was 90 or higher in 61% of the patients for whom the information was available (363/492).
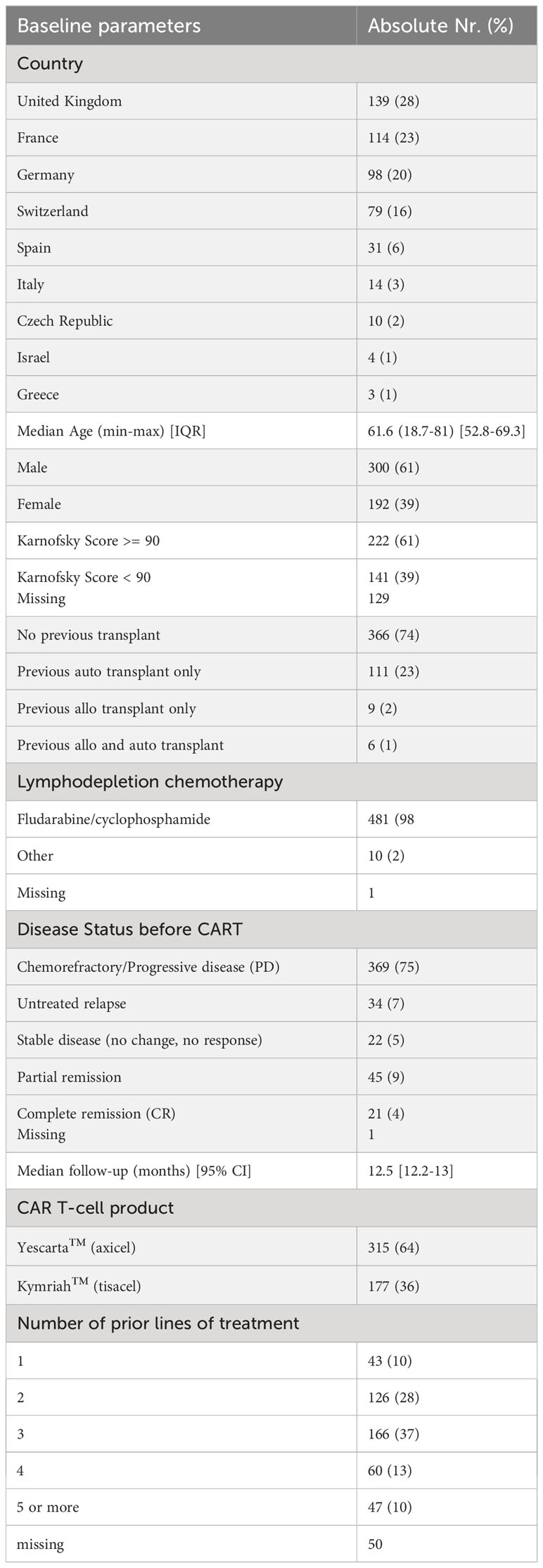
Table 1 Baseline characteristics of the cohort.
Most patients received CAR-T cells without having a previous transplantation (74%). Disease status before CAR-T cell therapy was mainly chemorefractory/progressive disease (75%). Most patients had received either two (28%) or three (37%) previous lines of therapy. However, 23% had four or more lines of previous therapy.
Table 2 describes pre-existing comorbidities in the cohort. 48.7% of patients had at least one pre-existing comorbidity present before CAR-T infusion. The most frequently recorded comorbidity was pulmonary (19.3%), followed by diabetes (7.5%), cardiac (7.3%), obesity (5.9%), solid tumour (5.6%) and psychiatric disturbance (4.7%).
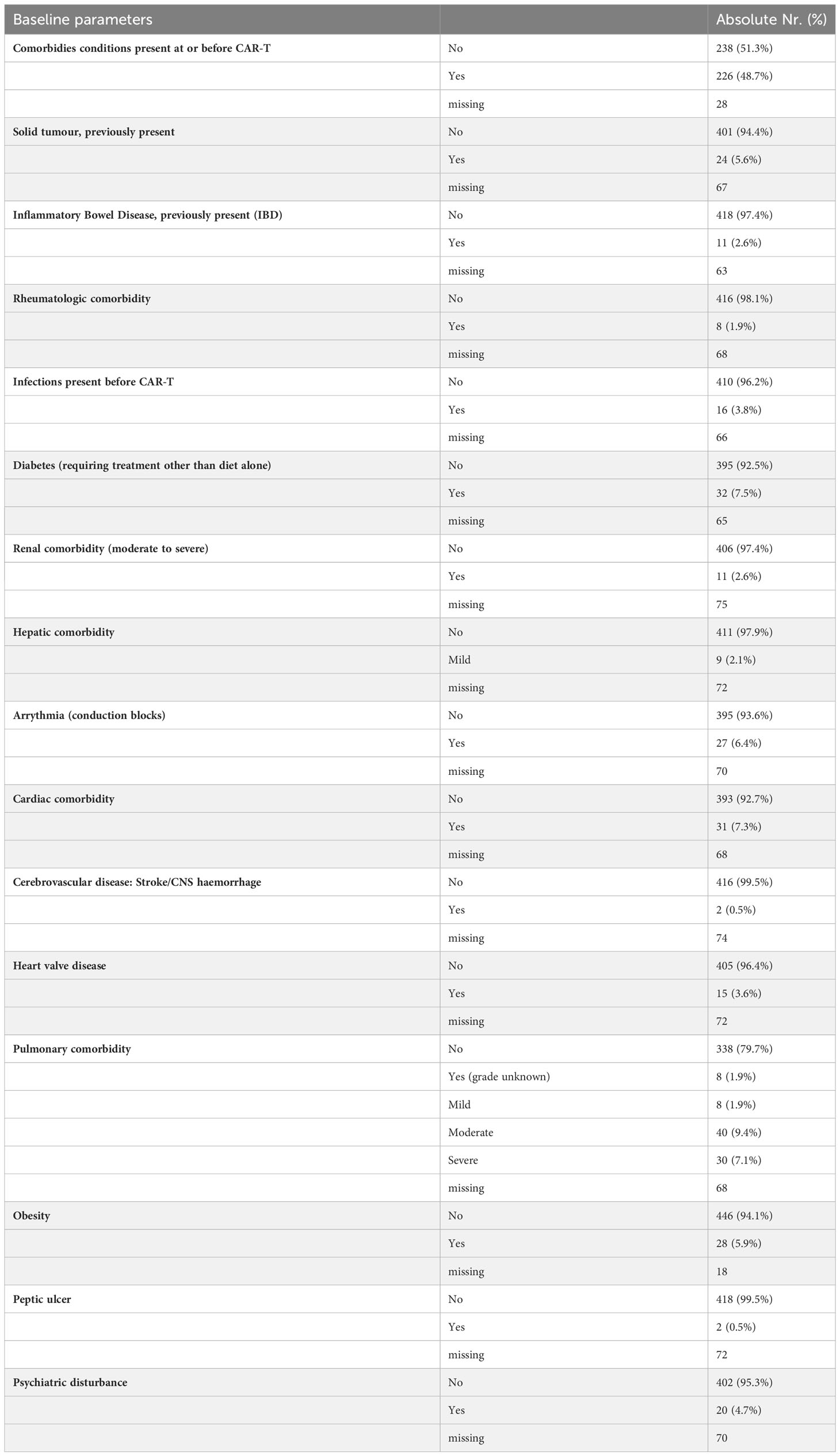
Table 2 Baseline co-morbidities of the cohort.
We were able to collect data on time of onset as well as severity of renal, cardiac, hepatic, gastro-intestinal, skin and pulmonary toxicities. The occurrences of grades 3-4 (CTC-AE) severe toxicities in the different organs are given in Table 3.
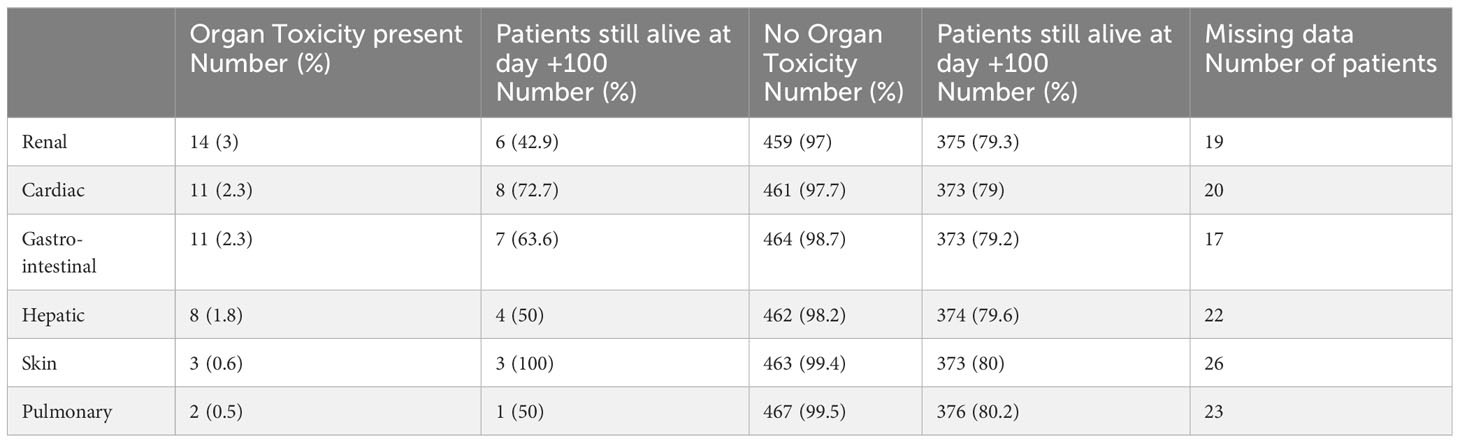
Table 3 Occurrence of severe organ toxicities until day +100 and patients alive at day +100 after CD19+ CART infusion.
Overall, the frequency of severe organ toxicities was relatively low. Severe renal toxicity occurred most frequently (3.0%) followed by severe cardiac, gastro-intestinal and hepatic toxicities (2.3%, 2.3% and 1.8% respectively). Skin toxicity and pulmonary toxicity were only observed in three and two patients, respectively. Data in Table 2 suggest that patients with these severe complications might have a lower chance of survival at day +100 after CAR-T cell therapy as compared to patients without organ complications. We can indeed observe that among the 14 patients developing renal toxicity during the first 100 days, only six were still alive at day 100. Similarly, eight patients were reported as having had liver toxicity during the first 100 days and only four of them were still alive at day 100. However, the numbers of patients with severe organ toxicities were too low to perform advanced statistics. Table 4 shows the proportion of patients with organ toxicities receiving either axi-cel (Yescarta) or tisa-cel (Kymriah) as well as the proportion according to age, using a 60-year cut off.
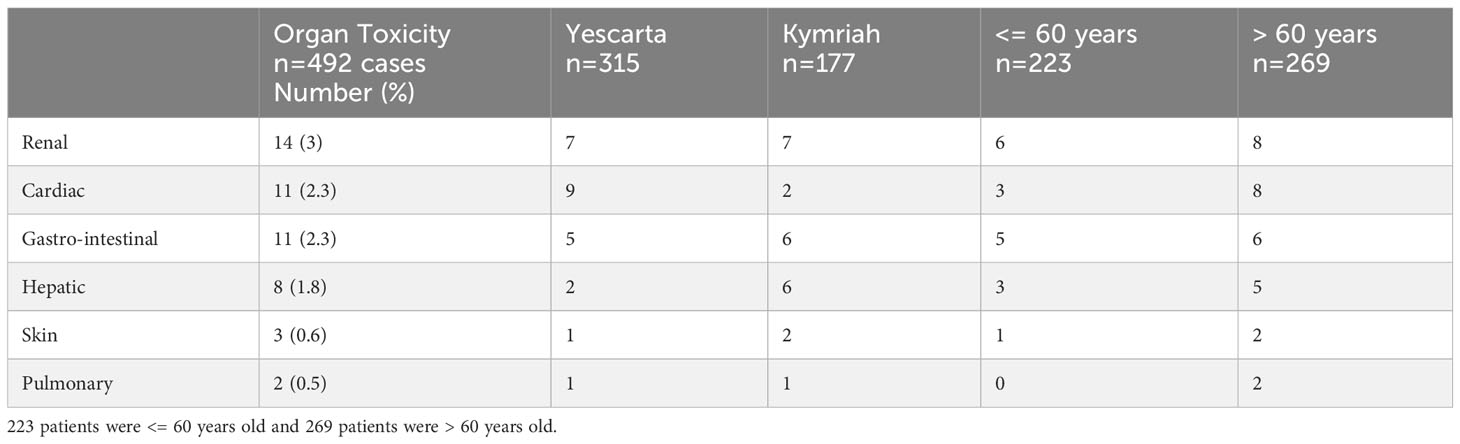
Table 4 Organ toxicities according to administered product and to patient age.
The occurrence of organ complications in relation to time of occurrence and death events in individual patients is visualized in Figure 1. The majority of severe organ complications occurred before day+20, during the early phase after CAR-T cell therapy. However, some renal, hepatic and gastro-intestinal complications occurred at a later time point after CAR-T cell infusion, between day+30 and day+100. The cumulative incidences of cytokine release syndrome (CRS) were the following:
● At 3 days [95% CI] 46.6% [41.8-51.3]
● At 6 days [95% CI] 81.5% [77.5-84.9]
● At 9 days [95% CI] 93% [90.1-95]
● At 12 days [95% CI] 96.5% [94.2-97.9]
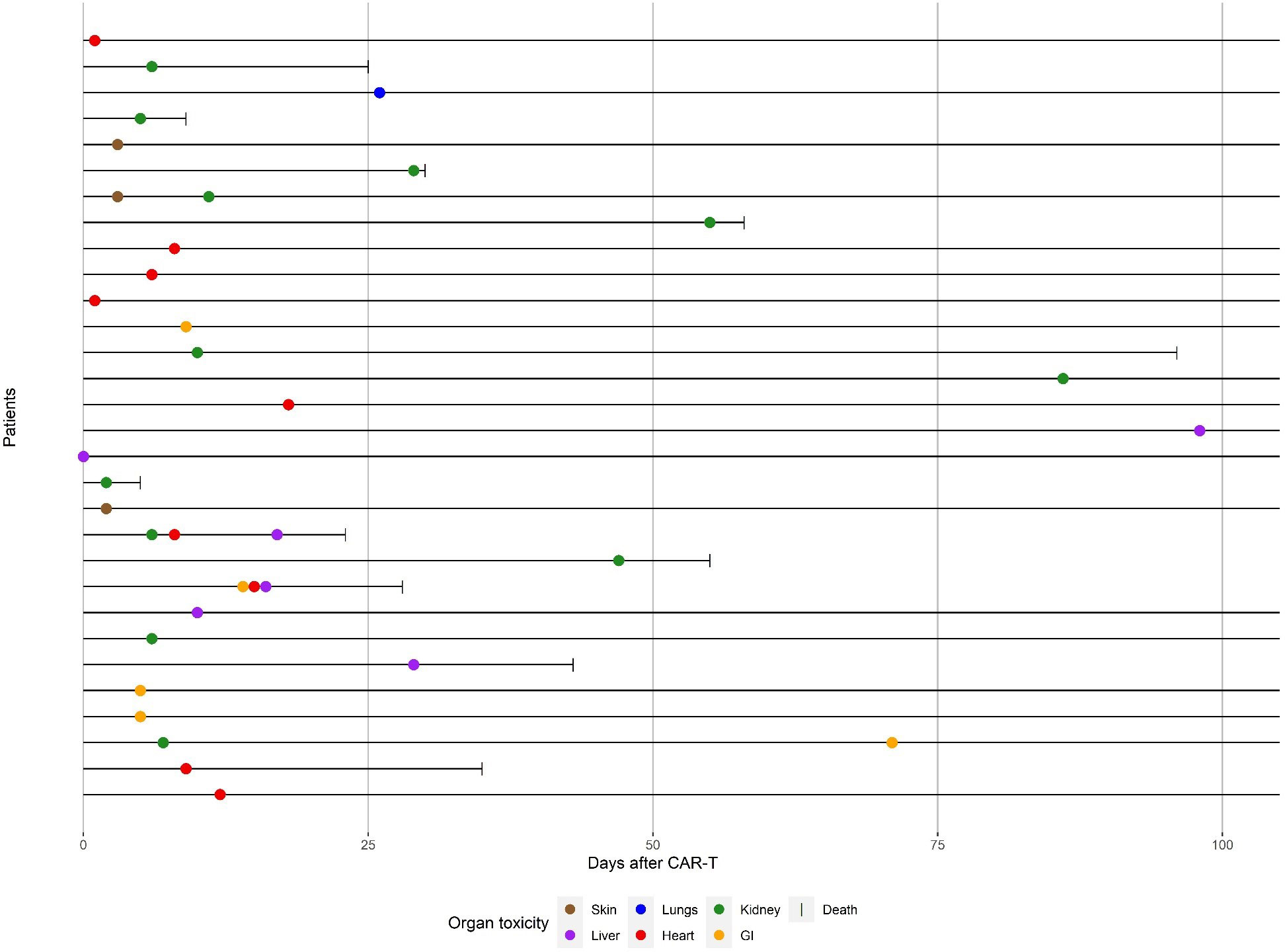
Figure 1 Timing of severe organ toxicities and deaths until day +100 after CD19+ CART infusion.
Hypogammaglubulinemia, (<4g/l) which is paradigmatic of an on target/off tumour effect for CAR-T cells targeting CD19, was observed in 236 patients (57.3%; data missing for 80 cases). Of note, most of those patients (n = 170, 80.2%) had already low IgG levels before CAR-T cell therapy. 87/178 (48.9%, data missing for 58 cases) of the patients have seen their hypogammaglobulinemia worsened following CAR-T cell infusion. Hypogammaglobulinemia resolved in the first 100 days in only 21 (10.7%) patients (data was missing for 39 patients).
In the whole population, we found that NRM was 3.1% [2.3-4.1; 95% CI] at 3 months and 5.2% [4.1-6.5; 95% CI] at one year after CAR-T cell therapy. Overall survival was 83.1% [79.8-86.5; 95% CI] at 3 months and 53.5% [49-58.4; 95% CI] at one year. Progression-free survival was 64.9% [62.5-67.4; 95% CI] at 3 months and 36.5% [33.9-39.2; 95% CI] at one year. Finally, relapse incidence was 32% [29.6-34.4; 95% CI] at 3 months and 58.3% [55.6-61; 95% CI] at one year after CAR-T cell therapy.
A description of the causes of death is given in Table 5. The most frequent cause of death by far was relapse of LBCL (85.1%). The most frequent causes of NRM were toxicities in close connection to the infused CAR-T cell product (cell-therapy-related toxicities including CRS, ICANS, and organ toxicity; 6.4% of total deaths) and infections (4.4% of total deaths). Organ complications, that were likely to be not cell-therapy related (0.4% of total deaths), as well as secondary malignancies (0.4% of total deaths) occurred less frequently. Of note, the decision if NRM was due to organ toxicity related vs. unrelated to the CAR-T cell infusion was done by the centre and no clear definition existed.
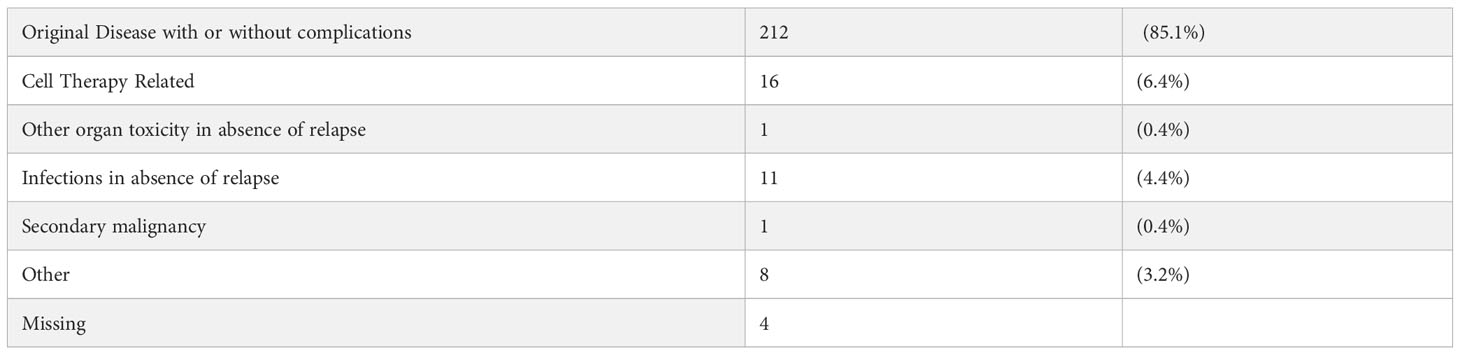
Table 5 Main causes of death.
Our present study is the first analysis of EBMT real-world data on other organ complications than CRS and ICANS after anti-CD19 CAR-T cell therapy for LBCL. Our main finding is that despite high rates of CRS in this dataset a low frequency of severe organ complications occurred, marginally contributing to a relatively low NRM. Of note, disease status before CAR-T cell therapy was mainly chemorefractory/progressive disease (75%) in the patient population reported here, which is considerably higher than in the registration trials. Despite this difference, our present results are mostly in line with follow up data of the initial CAR-T cell trials in patients with LBCL, also showing low NRM and manageable safety (9, 14). However, some of the more frequent organ toxicities found in our present study, such as renal, cardiac and hepatic complications, were not reported in the pivotal Zuma-1 (Axi-Cel) and Juliet (Tisa-Cel) trials. This is most likely due to larger patient numbers and a longer follow up period in our real-world analysis. As expected, our patients in this retrospective analysis had received more prior lines of treatment and had a lower performance status when compared to the patient populations in the two registration trials conducted to support marketing approval of Tisa-Cel and Axi-Cel. These different patient characteristics may also be another relevant aspect explaining the occurrence of organ toxicities in real-world conditions.
Recently, a real world data set of patients with LBCL undergoing CAR-T cell therapy in Germany has been published (n=356) (5). When comparing NRM in this national analysis with our current data, differences in NRM become evident. At a median follow up of 11 months, NRM was 10% in the German analysis vs. 4.2% NRM with 12 months median follow up in our current analysis. Interestingly, the reasons for death were also different with bone marrow aplasia and infections as the driving factor for NRM in the recent German analysis (5) and organ toxicities being the major factor for NRM in our current analysis. We recently found in LBCL patients receiving CD19+ CAR-T cells, that severe cytopenia had no significant impact on overall survival (HR 1.13 [95%CI 0.74-1.73] p=0.57) (15). However, patients with severe cytopenia had a poorer progression-free survival (HR 1.54 [95%CI 1.07-2.22] p=0.02) and a higher relapse incidence (HR 1.52 [95%CI 1.04-2.23] p=0.03). Again, the most likely reason for the pronounced differences in outcome between the two analyses is the difference in patient characteristics. The German analyses reported that only 13% of patients in their dataset fulfilled the inclusion criteria of the Zuma-1 trial, indicating a population at very high risk for toxicities and for NRM. Organ complications were not reported in detail in this publication, making it impossible to compare them to our present study. Also recently, a larger real world data set from France was published mainly comparing results from Axi-Cel vs. Tisa-Cel treated patients, but again organ complications were not reported in detail so far (16). In line, reporting of organ complications was not done in detail so far for the recent trials comparing CAR-T cell therapy to standard of care as second line option for large B-cell lymphoma (17, 18).
There are publications from centres in the USA with detailed information on organ toxicities. The MD Anderson Cancer Center in Houston looked specifically at cardiac complications in a retrospective analysis of 165 patients with LBCL undergoing therapy with axicel or tisacel (19). Sixteen percent developed at least one major adverse cardiac event until day +30. Among them, three myocardial infarctions. However, the occurrence of cardiac events was not associated to NRM. The Memorial Sloan-Kettering Cancer Center published even more comprehensive data on organ complications in a smaller series of patients (n=60) undergoing CD19+ CAR-T cell therapy for LBCL (4). At one year follow up, they found severe cardiovascular, pulmonary, hepatic and gastro-intestinal toxicities in 20%, 13%, 13% and 10% of patients respectively. Again, NRM was low with 1.7% at one year and was not associated to the occurrence of organ complications. Table 6 summarizes the occurrence of organ toxicities in major trials on CD19+ CAR-T cells. Although it is impossible to directly compare the previous trial results to our current data it appears that the previously reported complication rate was relatively high. One reason could be the improved clinical management in the more recent period, but we are unable to rule out underreporting of complications in the EBMT data base (see below).
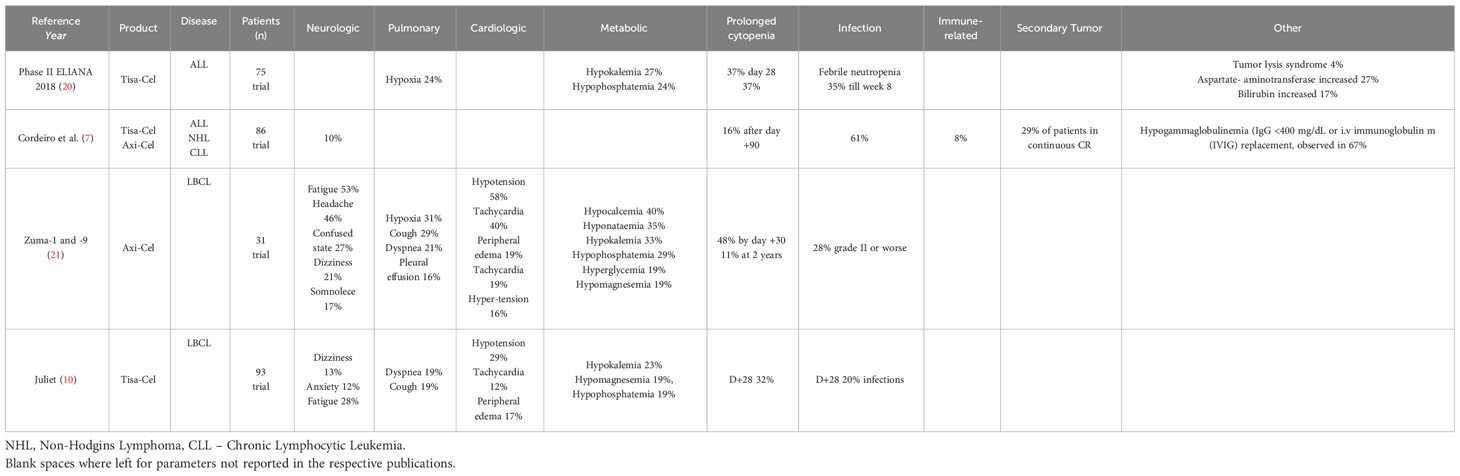
Table 6 Organ complications (other than CRS and ICANS) reported in major trials on CD19+ CAR-T cells.
A limitation of our study is that we were not able to perform advanced statistical analyses on the association of severe organ toxicities and NRM because of the low frequencies of these two events, despite the fact that this is one of the largest patient population ever studied. A possible further limitation of our current results is the retrospective data acquisition. We were therefore unable to monitor primary data to exclude a possible underreporting of organ toxicities in the EBMT data file. Finally, the follow up period was limited and is too short to adequately describe the occurrence of later toxicities – e.g. secondary malignancies.
A different and relevant way of looking at our current results is to compare them to toxicity and NRM data in allogeneic stem cell transplantation, which remains a relevant alternative treatment option in patients with relapsed/refractory LBCL. In a recent analysis, we found 12.2% NRM one year after allogeneic stem cell transplantation (22). Although the patient populations can’t be directly compared, the much lower 5.2% NRM one year after CD19+ CAR-T cell therapy in our current study suggests differences in safety in favour of CAR-T cells.
In conclusion, we found a low frequency of severe organ complications and a relatively low NRM after CAR-T cell therapy for LBCL in this international, multicentre analysis. These data demonstrate good safety in the European real-world setting.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Transplant Complications Working Party of the EBMT, EBMT board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
OP acknowledges the support of José Carreras Leukämie-Stiftung (3R/2019, 23R/2021), Deutsche Krebshilfe (70113519), Deutsche Forschungsgemeinschaft (PE 1450/7-1, PE 1450/9-1) and Stiftung Charité BIH (BIH_PRO_549, Focus Group Vascular Biomedicine).
OP has received honoraria or travel support from Gilead, Jazz, MSD, Novartis, Pfizer and Therakos. He has received research support from Incyte and Priothera. He is member of advisory boards to Equillium Bio, Jazz, Gilead, Novartis, MSD, Omeros, Priothera, Sanofi, Shionogi and SOBI. CC: BELLICUM PHARMACEUTICALS: Membership on an entity’s Board of Directors or advisory committees, BMS/CELGENE: Membership on an entity’s Board of Directors or advisory committees, Speakers Bureau; EBMT: Membership on an entity’s Board of Directors or advisory committees; FRESENIUS KABI: Research Funding; GILEAD: Membership on an entity’s Board of Directors or advisory committees, Speakers Bureau, Honoraria; JANSSEN PHARMACEUTICALS: Membership on an entity’s Board of Directors or advisory committees; MILTENYI BIOTECH: Research Funding; NOVARTIS: Speakers Bureau, SANOFI SA: Honoraria, Research Funding, Speakers Bureau, TERUMO BCT: Speakers Bureau.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1252811/full#supplementary-material
1. Abramson JS, Solomon SR, Arnason J, Johnston PB, Glass B, Bachanova V, et al. Lisocabtagene maraleucel as second-line therapy for large B-cell lymphoma: primary analysis of the phase 3 TRANSFORM study. Blood (2023) 141:1675–84. doi: 10.1182/blood.2022018730
2. Westin JR, Oluwole OO, Kersten MJ, Miklos DB, Perales MA, Ghobadi A, et al. Survival with axicabtagene ciloleucel in large B-cell lymphoma. N Engl J Med (2023) 389:148–57. doi: 10.1056/NEJMoa2301665
3. Penack O, Koenecke C. Complications after CD19+ CAR T-cell therapy. Cancers (Basel) 12 (2020). doi: 10.3390/cancers12113445
4. Wudhikarn K, Pennisi M, Garcia-Recio M, Flynn JR, Afuye A, Silverberg ML, et al. DLBCL patients treated with CD19 CAR T cells experience a high burden of organ toxicities but low nonrelapse mortality. Blood Adv (2020) 4:3024–33. doi: 10.1182/bloodadvances.2020001972
5. Bethge WA, Martus P, Schmitt M, Holtick U, Subklewe M, von Tresckow B, et al. GLA/DRST real-world outcome analysis of CAR-T cell therapies for large B-cell lymphoma in Germany. Blood (2022). doi: 10.1182/blood.2021015209
6. Korell F, Penack O, Mattie M, Schreck N, Benner A, Krzykalla J, et al. EASIX and severe endothelial complications after CD19-directed CAR-T cell therapy-A cohort study. Front Immunol (2022) 13:877477. doi: 10.3389/fimmu.2022.877477
7. Cordeiro A, Bezerra ED, Hirayama AV, Hill JA, Wu QV, Voutsinas J, et al. Late events after treatment with CD19-targeted chimeric antigen receptor modified T cells. Biol Blood Marrow Transplant (2020) 26:26–33. doi: 10.1016/j.bbmt.2019.08.003
8. Lefebvre B, Kang Y, Smith AM, Frey NV, Carver JR, Scherrer-Crosbie M. Cardiovascular effects of CAR T cell therapy: A retrospective study. JACC CardioOncol (2020) 2:193–203. doi: 10.1016/j.jaccao.2020.04.012
9. Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol (2019) 20:31–42. doi: 10.1016/S1470-2045(18)30864-7
10. Schuster SJ, Bishop MR, Tam CS, Waller EK, Borchmann P, McGuirk JP, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med (2019) 380:45–56. doi: 10.1056/NEJMoa1804980
11. McGrath E, Chabannon C, Terwel S, Bonini C, Kuball J. Opportunities and challenges associated with the evaluation of chimeric antigen receptor T cells in real-life. Curr Opin Oncol (2020) 32:427–33. doi: 10.1097/CCO.0000000000000665
12. U.D.o. Health and H. Services, common terminology criteria for adverse events (CTCAE) version 5.0 (2017). Available at: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
13. Fine JP, Gray RJ. A proportianal hazards model for the subdistribution of a competing risk. J Am Stat Assoc (1999) 94:496–509. doi: 10.1080/01621459.1999.10474144
14. Schuster SJ, Tam CS, Borchmann P, Worel N, McGuirk JP, Holte H, et al. Long-term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive B-cell lymphomas (JULIET): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol (2021) 22:1403–15. doi: 10.1016/S1470-2045(21)00375-2
15. Penack O, Peczynski C, Koenecke C, Polge E, Kuhnl A, Fegueux N, et al. Severe cytopenia after CD19 CAR T-cell therapy: a retrospective study from the EBMT Transplant Complications Working Party. J Immunother Cancer (2023) 11. doi: 10.1136/jitc-2022-006406
16. Bachy E, Le Gouill S, Di Blasi R, Sesques P, Manson G, Cartron G, et al. A real-world comparison of tisagenlecleucel and axicabtagene ciloleucel CAR T cells in relapsed or refractory diffuse large B cell lymphoma. Nat Med (2022) 28:2145–54. doi: 10.1038/s41591-022-01969-y
17. Kamdar M, Solomon SR, Arnason J, Johnston PB, Glass B, Bachanova V, et al. Lisocabtagene maraleucel versus standard of care with salvage chemotherapy followed by autologous stem cell transplantation as second-line treatment in patients with relapsed or refractory large B-cell lymphoma (TRANSFORM): results from an interim analysis of an open-label, randomised, phase 3 trial. Lancet (2022) 399:2294–308. doi: 10.1016/S0140-6736(22)00662-6
18. Locke FL, Miklos DB, Jacobson CA, Perales MA, Kersten MJ, Oluwole OO, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med (2022) 386:640–54. doi: 10.1056/NEJMoa2116133
19. Steiner RE, Banchs J, Koutroumpakis E, Becnel M, Gutierrez C, Strati P, et al. Cardiovascular events in patients treated with chimeric antigen receptor t-cell therapy for aggressive B-cell lymphoma. Haematologica (2021). doi: 10.3324/haematol.2021.280009
20. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med (2018) 378:439–48. doi: 10.1056/NEJMoa1709866
21. Strati P, Varma A, Adkins S, Nastoupil LJ, Westin J, Hagemeister FB, et al. Hematopoietic recovery and immune reconstitution after axicabtagene ciloleucel in patients with large B-cell lymphoma. Haematologica (2020). doi: 10.3324/haematol.2020.254045
Keywords: organ complications, CAR T-cell, large B-cell lymphoma, CD19, toxicity
Citation: Penack O, Peczynski C, Koenecke C, Polge E, Sanderson R, Yakoub-Agha I, Fegueux N, Daskalakis M, Collin M, Dreger P, Kröger N, Schanz U, Bloor A, Ganser A, Besley C, Wulf GG, Novak U, Moiseev I, Schoemans H, Basak GW, Chabannon C, Sureda A, Glass B and Peric Z (2023) Organ complications after CD19 CAR T-cell therapy for large B cell lymphoma: a retrospective study from the EBMT transplant complications and lymphoma working party. Front. Immunol. 14:1252811. doi: 10.3389/fimmu.2023.1252811
Received: 04 July 2023; Accepted: 12 September 2023;
Published: 27 September 2023.
Edited by:
Hamid Reza Mirzaei, Tehran University of Medical Sciences, IranReviewed by:
Natalie Grover, University of North Carolina at Chapel Hill, United StatesCopyright © 2023 Penack, Peczynski, Koenecke, Polge, Sanderson, Yakoub-Agha, Fegueux, Daskalakis, Collin, Dreger, Kröger, Schanz, Bloor, Ganser, Besley, Wulf, Novak, Moiseev, Schoemans, Basak, Chabannon, Sureda, Glass and Peric. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Olaf Penack, b2xhZi5wZW5hY2tAY2hhcml0ZS5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.