 Margaux Lelong1Régis Josien2,3†Marianne Coste-Burel4†
Margaux Lelong1Régis Josien2,3†Marianne Coste-Burel4† Marie Rimbert2Céline Bressollette-Bodin3,4
Marie Rimbert2Céline Bressollette-Bodin3,4 Stéphane Nancey5
Stéphane Nancey5 Guillaume Bouguen6
Guillaume Bouguen6 Matthieu Allez7Mélanie Serrero8Ludovic Caillo9Cléa Rouillon10Pierre Blanc11David Laharie12Raphaël Olivier13
Matthieu Allez7Mélanie Serrero8Ludovic Caillo9Cléa Rouillon10Pierre Blanc11David Laharie12Raphaël Olivier13 Laurent Peyrin-Biroulet14Nina Dib15Astrid De Maissin16Céline Montuclard17Caroline Trang-Poisson1Fabienne Vavasseur1Géraldine Gallot18Mathilde Berthome18
Laurent Peyrin-Biroulet14Nina Dib15Astrid De Maissin16Céline Montuclard17Caroline Trang-Poisson1Fabienne Vavasseur1Géraldine Gallot18Mathilde Berthome18 Cécile Braudeau2,3Justine Chevreuil2Arnaud Bourreille1
Cécile Braudeau2,3Justine Chevreuil2Arnaud Bourreille1 Catherine Le Berre1•
Catherine Le Berre1•- 1Nantes Université, Centre Hospitalier Universitaire (CHU) Nantes, Institut des Maladies de l’Appareil Digestif (IMAD), Hépato-Gastro-Entérologie et Assistance Nutritionnelle, Institut national de la santé et de la recherche médicale (Inserm) CIC 1413, Nantes, France
- 2Nantes Université, Centre Hospitalier Universitaire (CHU) Nantes, Laboratoire d’Immunologie Biologique, Centre d’ImmunoMonitorage Nantes-Atlantique (CIMNA), Nantes, France
- 3Nantes Université, Institut national de la santé et de la recherche médicale (Inserm), Centre Hospitalier Universitaire (CHU) Nantes, CR2TI UMR 1064, Nantes, France
- 4Nantes Université, Centre Hospitalier Universitaire (CHU) Nantes, Laboratoire de Virologie, Nantes, France
- 5Department of Gastroenterology, Lyon-Sud Hospital, Hospices Civils de Lyon, Université Claude Bernard Lyon 1 and INSERM U1111-CIRI, Lyon, France
- 6Centre Hospitalier Universitaire (CHU) and University of Rennes, INSERM, CIC1414, Institut NUMECAN (Nutrition Metabolism and Cancer), Rennes, France
- 7Gastroenterology Department, Hôpital Saint-Louis, Assistance Publique-Hôpitaux de Paris (AP-HP), INSERM U1160, Université de Paris, Paris, France
- 8Department of Gastroenterology, Centre Hospitalier Universitaire (CHU) Marseille, Marseille, France
- 9Department of Gastroenterology, Nimes University Hospital, Nîmes, France
- 10Department of Gastroenterology, Caen University Hospital, Caen, France
- 11Service d’hépatogastroentérologie B, Centre Hospitalier Universitaire (CHU) Montpellier et Université Montpellier, Montpellier, France
- 12Centre Hospitalier Universitaire (CHU) de Bordeaux, Centre Medico-chirurgical Magellan, Hôpital Haut-Lévêque, Gastroenterology department, Université de Bordeaux, INSERM CIC 1401, Bordeaux, France
- 13Gastroenterology Department, University Hospital of Poitiers, Poitiers, France
- 14Department of Gastroenterology and Inserm NGERE U1256, University Hospital of Nancy, University of Lorraine, Vandoeuvre-lès-Nancy, France
- 15Department of HepatoGastroenterology, Angers University Hospital, Angers, France
- 16Centre Hospitalier Départemental (CHD) La Roche Sur Yon, Department of Gastroenterology, La-Roche-sur-Yon, France
- 17Department of Endoscopy and Gastroenterology, Valence Public Hospital, Valence, France
- 18Nantes Université, Centre Hospitalier Universitaire (CHU) Nantes, Centre de ressources biologiques (CRB), Nantes, France
Background: Patients with inflammatory bowel disease (IBD) may have a modified immune response to SARS-CoV-2. The objectives were to evaluate the prevalence of COVID-19 in patients treated with infliximab or vedolizumab, to analyze the factors associated with the infection, the impact of treatments and trough levels.
Methods: Patients with IBD treated with intravenous biologics in 14 French centers were included between March and June 2020 and followed-up for 6 months. Blood samples were collected for serologies and trough levels. The analysis of factors associated with COVID-19 was conducted in a matched 1:1 case-control sub-study with positive patients.
Results: In total, 1026 patients were included (74.9% infliximab). Over the follow-up period, 420 patients reported the occurrence of COVID-19 symptoms; 342 had been tested of whom 18 were positive. At the end of follow-up, 38 patients had a positive serology. Considering both nasal tests and serologies together, 46 patients (4.5%) had been infected. The risk of COVID-19 was related neither to the use of treatments (whatever the trough levels) nor to disease activity. Infections were more frequent when using public transport or living in flats in urban areas.
Conclusions: The prevalence rate of COVID-19 in this IBD population treated with intravenous infliximab or vedolizumab was the same as the one in the French population before the start of the vaccination campaign. The risk was increased by urban living and was not influenced by disease activity or biologics. Sanitary barrier measures remain the best way to protect against SARS-CoV-2 in patients with IBD in biological therapy.
1 Introduction
Inflammatory bowel diseases (IBD), encompassing Crohn’s disease (CD) and ulcerative colitis (UC), are both characterized by chronic inflammation of the digestive tract due to dysregulation of the intestinal immune system. Although IBD do not significantly increase the risk of mortality (1), both CD and UC have been linked to an increased risk of death from infections, for multiple reasons, including chronic inflammation, undernutrition, and the therapies used that all have immunosuppressive properties, with the exception of 5-aminosalicylates (2–4).
Nowadays, more than 50% of patients are treated with immunosuppressants and/or biological therapies (5, 6). The risk of viral infections, in particular herpes viruses (7), is increased with thiopurines, which is less demonstrated with respiratory viruses such as the Influenzae virus (8). When using biologics, the risk of bacterial and opportunistic infections is greater, but this risk mainly concerns anti-tumor necrosis factor (TNF) agents, while ustekinumab and vedolizumab probably have a more favorable safety profile (9–11).
The infection by SARS-CoV-2 has raised questions about the management of patients with IBD. Since the beginning of the COVID-19 pandemic in December 2019, many studies have focused on the clinical factors associated with the risk of complications or death in general, such as older patients, particularly males, or those with co-morbidities including pulmonary, renal, cardiac, cerebrovascular or metabolic diseases (12–14). The link between drug-induced immunosuppression and severe COVID-19 is less clear (15, 16).
Several studies have reported a lower prevalence of SARS-CoV-2 infection in the IBD population, with a trend towards more frequent hospitalizations without increasing the risk of severe COVID-19 infection and admission in intensive care unit (17–21). Data in patients with IBD also tend to show a protective effect of anti-TNF agents (22–24), but there is still some uncertainty on the subject (25). Few studies studied the impact of trough levels on the risk of COVID-19. Data from the British CLARITY IBD study showed that the type of biologic agent did not impact the rates of PCR-confirmed SARS-CoV-2 infection, but seroprevalence rates were lower in infliximab- and adalimumab- than vedolizumab-treated patients. Interestingly, undetectable anti-TNF levels were associated with higher viral seropositivity rates, supporting a causal relationship. However, confounding factors, such as combination therapy with an immunosuppressant, have not been analyzed yet (26, 27).
Moreover, nowadays, vaccine safety and efficacy is a key question in the context of patients who have biological therapy, especially when seeing the rate of COVID-19 vaccine hesitancy in IBD patients (28, 29). Serologic response is good after vaccination in patients with IBD (30, 31), although lower with anti-TNF agents than with other treatments including vedolizumab (32). Real-word data have also proven the safety of COVID-19 vaccines in IBD patients (33, 34). Nevertheless, it is important to be able to provide patients with data regarding the risk of being infected by SARS-CoV-2 and the factors associated with this risk, especially when treated with biologics, outside any vaccination context.
The prospective MICI-SARS-CoV-2 study aimed at bringing more precision to these fundamental questions on a population of French patients with IBD being treated with intravenous infliximab or vedolizumab at day hospital before the start of the vaccination campaign. The objectives of this study were (i) to evaluate the prevalence of COVID-19 in a French cohort of patients with IBD treated with infliximab or vedolizumab during the first pandemic wave; (ii) to identify clinical and socio-demographic factors associated with the risk of COVID-19; (iii) to analyze the impact of biologics (with or without combination therapy with immunosuppressants) and their trough levels on the risk of being infected by SARS-CoV-2.
2 Materials and methods
2.1 Study design and setting
The MICI-SARS-CoV-2 study was a prospective multicenter study with an associated biological collection, starting during the first pandemic wave in France. This study was led in cooperation with the Groupe d’Etude Thérapeutique des Affections Inflammatoires du Tube Digestif (GETAID), of which all the 15 participating centers are members and are used to conduct collaborative research projects, allowing the rapid constitution of this large cohort.
The inclusion period started in March 2020 and lasted until June 2020 – the first two months of the study corresponding to the first lockdown period in France. Patients were recruited consecutively in the day hospital of each center. The follow-up period ended in January 2021 before the start of the vaccination campaign in France.
2.2 Study population
All patients with an established diagnosis of IBD (CD, UC or IBD-unclassified), aged over 18, treated with either intravenous (IV) infliximab or vedolizumab, could be included. No patient under subcutaneous biologic therapy was included in this study in order to have a homogeneous population of patients during this lockdown period – all included patients had to leave home and come to day hospital to receive their treatment. Non-inclusion criteria included patients under legal protection (guardianship, curatorship) or under safeguard of justice, insufficient command of French language, and contra-indications to infliximab or vedolizumab at baseline.
At baseline, patient information was given orally and in writing, then the physician collected patient’s oral non-opposition. Patients were followed-up for a period of 6 months at a rhythm depending on the interval between infliximab or vedolizumab infusions.
2.3 Questionnaire administration and data collection procedures
Clinical data were collected by the physician at baseline, including gender, type of IBD (CD, UC or IBD-unclassified), age at baseline, disease duration, body mass index (BMI) at baseline, smoking status, disease location and behavior according to the Montreal classification, history of perianal disease, presence of extra-intestinal manifestations, presence of comorbidities, history of intestinal resection, ongoing disease-related treatments, previous treatments used, disease activity index (Harvey Bradshaw Index [HBI] for CD, Mayo clinical sub-score for UC), and level of C-reactive protein (CRP) if available.
At baseline, patients filled-in a questionnaire regarding their lifestyle during the lockdown period, including type of professional activity (continuation of their usual activity, teleworking or stopping work), their family environment (number of people living at home, including those who continued their professional activities, as well as the number of children under 15 years of age), their type of accommodation (house or flat), their area of residence (city center, suburban area, rural area), and their means of transport to come to the day hospital (private car, public transport, other including taxi).
At each visit, patients filled-in another questionnaire on the occurrence of an intercurrent event due to their IBD, especially the need of corticosteroids between two infusions (self-medication was not excluded). An active disease during the follow-up period was defined by treatment intensification (addition of at least one medication, shortening of the interval between infusions, increase in the dose of infliximab infusion), change of biological therapy, steroids intake, hospitalization(s) or emergency consultation(s) with their general practitioner or gastroenterologist.
At each of their visit at day hospital, patients were also questioned about the occurrence of symptoms that could suggest COVID-19 during the interval since the last infusion (fever, cough, anosmia, myalgias, dyspnea, aches and pains, or other), and if so the performance of diagnostic tests (rapid antigen test, Polymerase Chain Reaction [PCR] test via nasal swab, or computed-tomography [CT] scan). It should be noted that the occurrence of symptoms suggestive of COVID-19 did not systematically result in testing in all patients. SARS-CoV-2 infection was considered as confirmed by a positive rapid antigen test and/or positive PCR test and/or a CT scan with characteristic lung involvement.
2.4 Blood sample collection procedures
After having obtained the subject’s written consent, blood samples were collected at each visit immediately before drug administration.
A dry blood tube of 10 mL was collected at each visit for all patients included, then prepared at 4°C and divided into 3 aliquots of serum of 1 mL frozen at – 80°C. These aliquots were used for SARS-CoV-2 antibody assays and dosage of infliximab or vedolizumab trough levels. Residual blood samples collected during the study were kept for new scientific interest. In 9 centers, 3 additional blood ethylenediaminetetraacetic acid (EDTA) tubes of 10 mL were collected at each visit, then prepared at room temperature for isolating peripheral blood mononuclear cells (PBMC) and frozen either at – 80°C or at – 130°C depending on the future immunological analyzes.
All samples from all centers were transferred to Nantes University Hospital using a specific frozen carrier, then integrated into the collection of human biological samples MICI-SARS-CoV-2 located in the Centre de Ressources Biologiques (CRB, BRIF: BB-0033-00040) of Nantes University Hospital.
2.5 Biological analysis
At the end of the follow-up, SARS-CoV-2 antibody assays were performed for all patients. For patients who were seropositive at the time of their last infusion, SARS-CoV-2 antibodies were assessed at each of their visit in order to determine the timing of seroconversion. SARS-CoV-2 antibodies were detected using the Elecsys® Anti-SARS-CoV-2 S kit (Roche Diagnostics), an immunoassay for the qualitative detection of total antibodies (including IgG) directed against the spike protein receptor binding domain. In comparison with other similar tests, such as Abbott® or Siemens®, the Elecsys® kit has a good sensitivity and can detect more than 90% of positive samples 14 days after the onset of symptoms. It has also been showed to be well correlated to neutralizing antibodies results, with an area under the curve (AUC) between 0.959 and 0.987 in Receiver Operating Characteristic (ROC) curve analysis (35).
Residual drug levels were determined using the commercial Promonitor® kits (Progenika Biopharma, Spain) supplied by GRIFOLS France SARL (Paris, France). They were performed at the time of seroconversion for seropositive patients, and at the end of follow-up for matched controls, in order to have comparable tubes already thawed once, then refrozen. The Promonitor® ELISA tests are of the type “capture” for the measurement of infliximab, “sandwich” for the measurement of vedolizumab, “bridging” for the measurement of anti-drug antibodies. An enzymatic reaction using a chromogen (Tetramethylbenzidine [TMB]) then allows the quantification of the number of complexes (anti-infliximab/infliximab, anti-vedolizumab/vedolizumab) by evaluating the intensity of the colorimetric reaction spectrophotometrically and using a calibration curve. The signal obtained is proportional to the amount of infliximab, vedolizumab or anti-drug antibodies in the patient sample. The concentration measurement ranges are as follows: 0.3 to 14.4 µg/mL for infliximab trough levels, 3.5 to 54.8 μg/mL for vedolizumab trough levels, 5 to 1440 Arbitrary Unit (AU)/mL for anti-infliximab antibodies, and 27 to 300 AU/mL for anti-vedolizumab antibodies.
2.6 Statistical analysis
Statistics were performed using SAS 9.4 software.
2.6.1 Descriptive statistics
Continuous variables are described using means and standard deviations and were tested using Student t-test for continuous variables. Categorical variables are described as raw counts and percentages and were tested using Chi-squared test (or Fisher’s exact test if statistically inappropriate). Missing values are systematically presented.
2.6.2 Analysis of factors associated with SARS-CoV-2 infection
Due to the small number of patients tested positive for COVID-19 in the study population (confirmed either by positive rapid antigen test/PCR test/CT-scan during follow-up or by positive serology at the end of follow-up), a 1:1 case-control matching was performed according to several variables representing potential confounding factors in the risk of being infected by SARS-CoV-2 (age, gender, BMI, type of IBD, disease activity, use of an associated immunosuppressant). Matching by center could not be performed because there were too few patients per center for matching in addition to the other variables.
In this case-control sub-study, variables are described according to the COVID+/COVID– groups and in aggregate. Quantitative variables at baseline were compared between groups using a Student’s t test for paired data or a Mann-Whitney-Wilcoxon rank test for paired data. Binary categorical variables at baseline were compared between groups using a MacNemar test (for matched data). If more than two modalities, an exact symmetry test was performed to account for data matching. Variables measured at several visits (longitudinal follow-up) were analyzed using a mixed logistic model that took into account intra-patient correlation and matching by putting matching in random effect. In the model, the group, time (visit) effect and group*time interaction were analyzed.
2.7 Ethical considerations
This study was a non-interventional trial approved by the Comité de Protection des Personnes (CPP) Ile-de-France VI (institutional review board) on 30 March 2020 under the number 20.03.27.48341.
The blood samples were integrated into the collection of human biological samples attached to the « Hépato-Gastro-Entérologie » research program declared on 5 September 2011 under the number DC-2011-1399 and in the following amending declarations (DC-2012-1555; DC-2013-1832; DC2014-2206 and DC-2017-2987 currently pending) at the Ministry of Research and having obtained a favorable decision from the CPP Ouest IV on 7 April 2015. The consent form for this biological collection was validated by the CPP Ouest IV on 8 October 2020.
3 Results
In total, 1184 patients were included in 17 centers. Patients from 2 centers had to be excluded due to lack of follow-up or mislabeling, and 6 patients were excluded due to missing data at baseline. Thus, serologies were performed on 1026 patients (Figure 1).
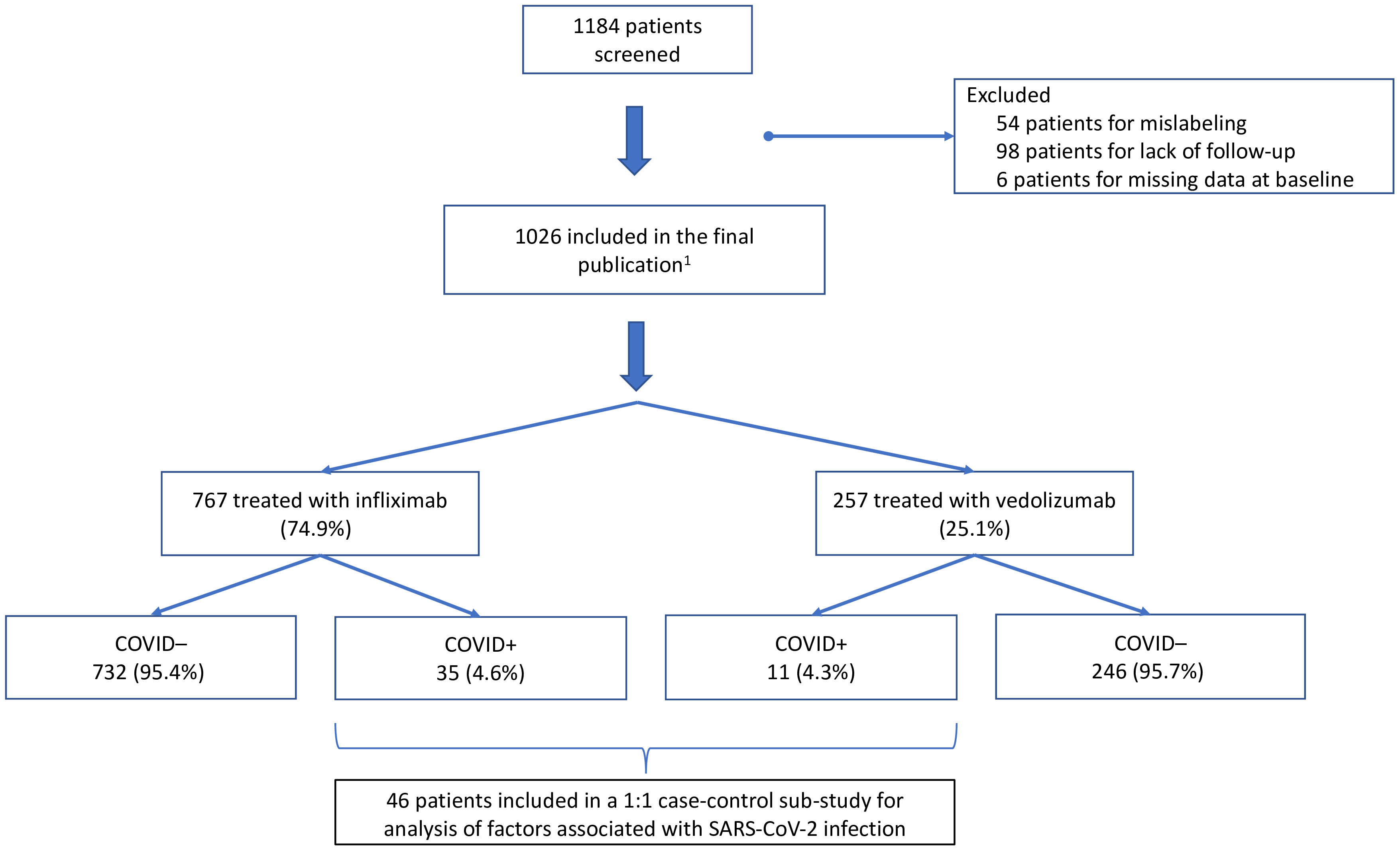
Figure 1 Flow chart of the study. 1: 2 missing data.
3.1 Baseline characteristics
Clinical characteristics of the study population at baseline are described in Table 1. More than 60.0% of patients had at least one extra-intestinal manifestation; the most frequent were rheumatologic manifestations, present in more than 11.2% of patients, particularly ankylosing spondylitis for 6.1% of them, and skin manifestations for 6.9%, especially psoriasis in 3.1% of cases. Digestive comorbidities including associated liver disease, primary sclerosing cholangitis or pancreatic disorders were present in 5.0% of cases. Regarding comorbidities that have been described to increase the risk of severe SARS-CoV-2 infection in the general population, 14.8% of patients were considered as obese, 5.4% had a pulmonary disease including chronic obstructive pulmonary disease (COPD) or asthma, 5.2% suffered from a vascular disease including hypertension, 2.3% had diabetes, 1.7% had a cardiac disease, 1.5% had cancer, 1.3% suffered from another autoimmune disease, and 0.9% had kidney failure.
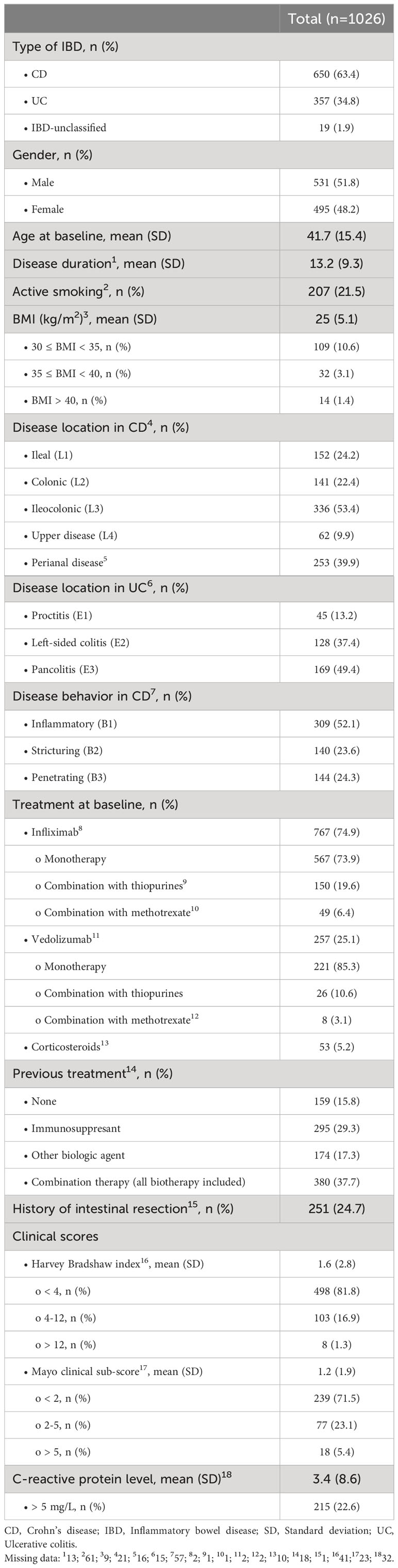
Table 1 Clinical characteristics of the study population at baseline (n=1026).
Socio-demographic data of the study population at baseline are described in Table 2.
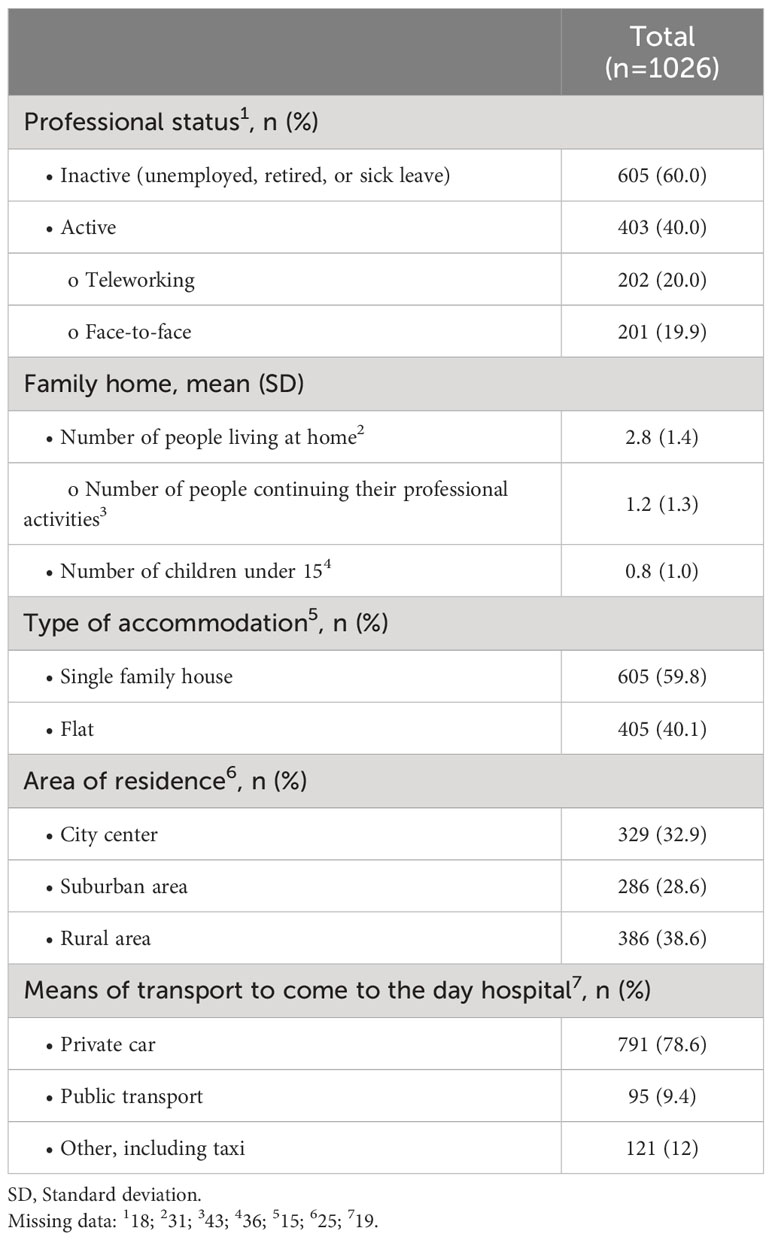
Table 2 Socio-demographic characteristics of the study population at baseline (n=1026).
3.2 Evolution of disease activity during follow-up
Over the 6 months of follow-up, 556 patients (54.2%) had an active disease defined by an HBI score >4 (n=159, 15.5%) or Mayo clinical sub-score >2 (n=105, 10.2%), and/or treatment intensification (addition of at least one medication or increase in the dose [n=341 (33.2%)], shortening of the interval between infusions [n=161, 15.7%], increase in the dose of infliximab infusion [n=75, 7.3%]), and/or change of biological therapy (n=19, 1.85%). Among them, 103 patients (10%) had received corticosteroids at least occasionally (self-medication was not excluded), 314 (30.6%) had visited their general practitioner, 37 patients (3.6%) had been hospitalized, and 33 patients (3.2%) had visited the emergency room for any reason during follow-up. The pandemic did not influence the adherence to intravenous biologics in this cohort because all patients kept their appointments in day hospital without any postponement.
3.3 SARS-CoV-2 outcomes during follow-up
All visits considered together, 420 patients (40.9%) reported the occurrence of symptoms suggestive of COVID-19 during the interval between two infusions. Although not specific, aches and pain were the most reported symptoms for 388 patients (37.8%). Cough was reported during follow-up by 225 patients (21.9%), dyspnea in 194 patients (18.9%). Anosmia was described in 120 patients (11.7%), and fever in 109 patients (10.6%). Of note, 150 patients (14.6%) reported other symptoms, notably digestive symptoms (diarrhea, abdominal pain).Over the 6 months of follow-up, 342 patients (33.3%) had been tested for SARS-CoV-2 infection, of whom 85 (24.9%) had been tested several times (twice or more). Most patients tested reported cough and dyspnea. The majority of patients (n=322, 94.2%) was tested by PCR test; rapid antigen test was performed in 19 patients (5.6%), of whom 2 also had a PCR test (10.5%); CT-scan was performed in 13 patients (3.8%), of whom 10 also had a PCR test (76.2%). Of the 342 tests, only 18 were positive (1 positive rapid antigen test, 17 positive PCR tests, no positive CT-scan). In those cases, the infusion of biologic was postponed by 14 days from the date of the positive test. There was no severe case of COVID-19. Only one patient had been hospitalized without requiring an admission in intensive care unit.
3.4 SARS-CoV-2 seroprevalence
Table 3 summarizes the outcomes linked to SARS-CoV-2 infection in the study population. At the end of follow-up, 38 patients (3.7%) had anti-SARS-CoV-2 antibodies, of whom 28 (73.7%) never had a positive PCR test (25 had not been tested, 3 had been tested negative). Among the 3 patients who were tested negative by PCR with a positive serology at the end of follow-up, 2 of them were tested by PCR approximately at the same time as the serology was performed, but they had low levels of antibodies; the third patient had a negative PCR test 3 months before the detection of anti-SARS-CoV-2 antibodies which was strongly positive, probably reflecting a later contamination. Among the 18 patients who had been tested positive by nasal swab for SARS-CoV-2 during the follow-up, only 10 (55.6%) were seropositive at the end of follow-up.

Table 3 SARS-CoV-2 outcomes in the study population (n=1026).
Considering both positive nasal tests and serologies together, 46 patients had been infected by SARS-CoV-2 during their follow-up in the first wave of the pandemic, i.e. 4.5% of the study cohort. None of these patients had any long-term sequelae of COVID-19.
3.5 Influence of clinical and socio-demographic factors on the risk of being infected by SARS-CoV-2
For the analysis of factors associated with SARS-CoV-2 infection in the study population, COVID+ patients were included in a matched 1:1 case-control sub-study (Table 4). All 46 patients who had had a SARS-CoV-2 infection in our cohort (confirmed either by positive rapid antigen test, PCR test, and/or anti-SARS-CoV-2 antibodies at the end of follow-up), were included in this case-control sub-study for analyzing clinical, socio-demographic and biological factors associated with COVID-19 in this population (Figure 1). Figure 2 illustrates the number of inclusions per group per center in this sub-study.
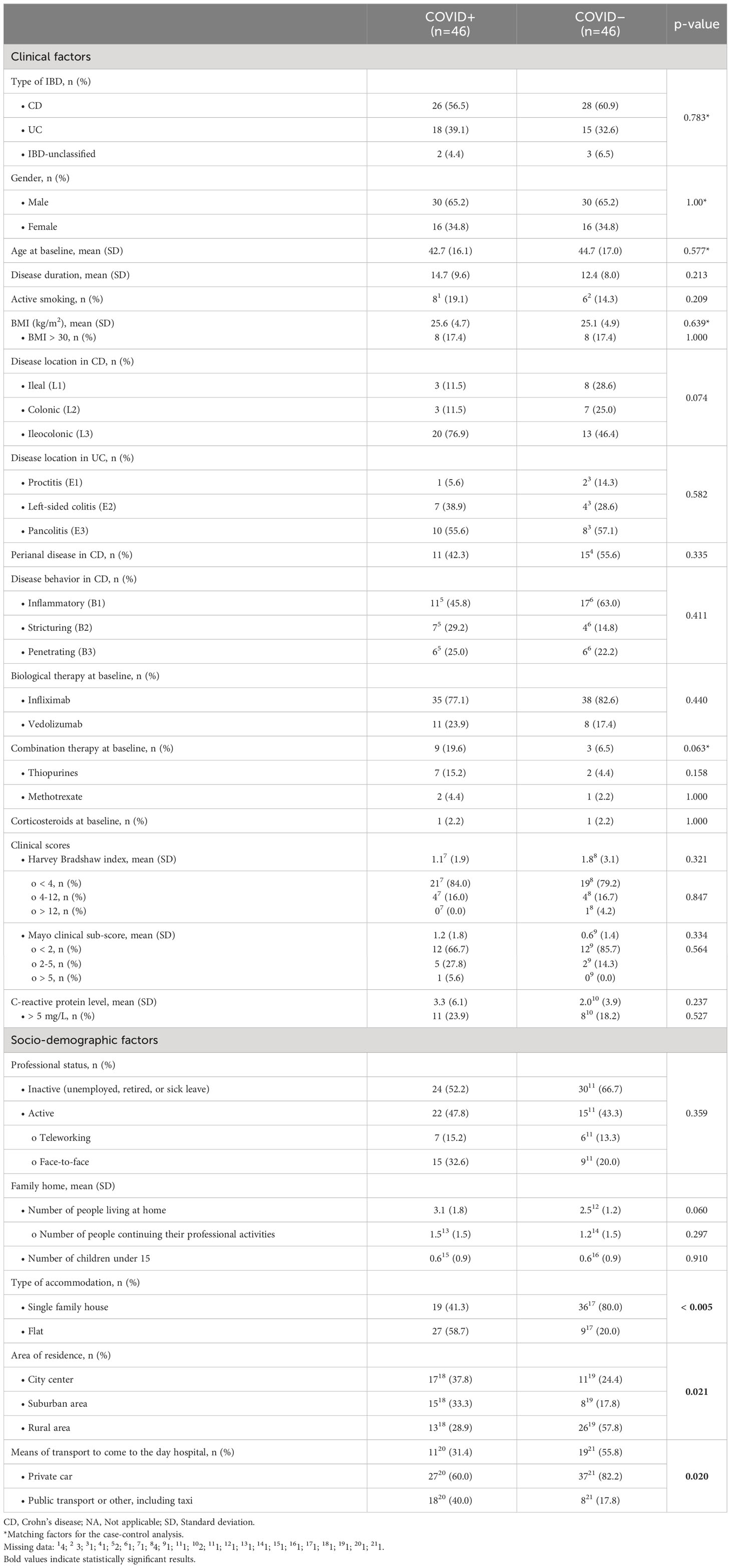
Table 4 Analysis of clinical and socio-demographic factors at baseline associated with SARS-CoV-2 infection in a matched 1:1 case-control sub-study (n=92).
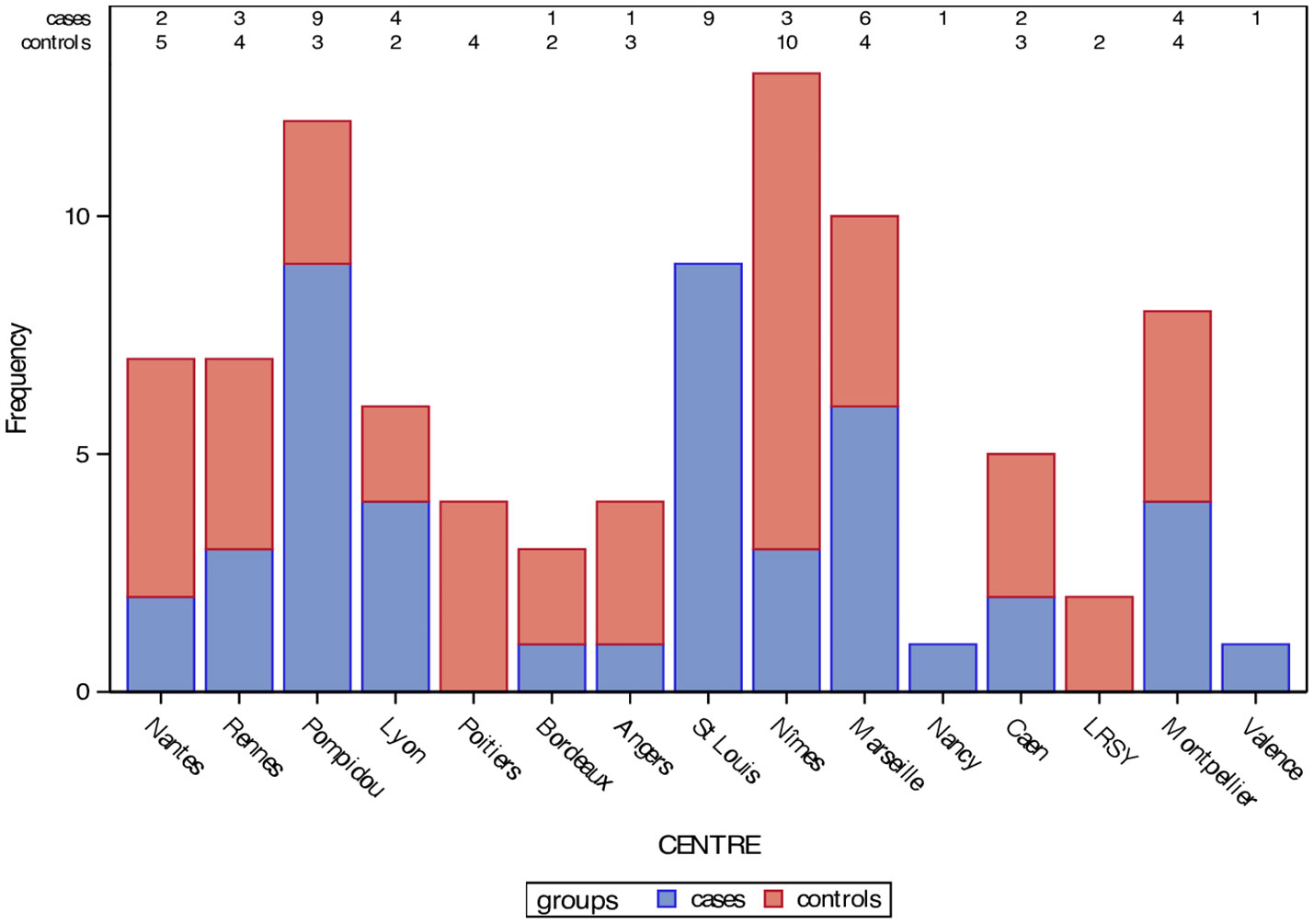
Figure 2 Number of inclusions per group per center in the matched 1:1 case-control sub-study.
3.5.1 Clinical factors
At baseline, none of the clinical factors that were analyzed was associated with an increased risk of being infected by SARS-CoV-2. There was no difference regarding the type of biological therapy received at baseline. Patients tested positive for COVID-19 tended to be more treated in combination therapy with an immunosuppressant, but this was not statistically significant (p=0.063). Only one (2.2%) of the positive patients was taking corticosteroids at baseline. Regarding comorbidities, diabetes tended to be more frequent in patients with IBD tested positive for COVID-19 (8.7% vs 2.2%) but the difference was not significant (p=0.361), as was the case for vascular diseases including hypertension (6.5% vs 2.2%, p=0.617). There was no significant difference between both groups in the proportion of patients suffering from a pulmonary disease including COPD or asthma (10.9% in COVID+ patients vs 8.7% in COVID– patients, p=1.000). None of the patients tested positive for COVID-19 suffered from a cardiac disease, kidney failure or cancer.
During follow-up, there was no statistically significant difference between both groups over time in terms of steroids intake (p=0.850), thiopurine intake (p=0.686), or all immunosuppressants combined (p=0.482). The number of patients under infliximab or vedolizumab did not differ between positive and negative patients over the 6 months of follow-up (p=0.719). The mean dose of infliximab (p=0.666) and the interval between two infusions of infliximab (p=0.853) or vedolizumab (p=0.716) did not significantly differ over time between both groups. Regarding disease activity during the follow-up period, there was no significant difference between both groups over time in terms of Mayo clinical sub-score (p=0.499), HBI (p=0.471), CRP (p=0.358), or the occurrence of a disease relapse defined by the physician (p=0.804).
3.5.2 Socio-demographic factors
There were numerically more COVID-19 positive patients who still worked at their place of work (32.6% vs 20.0%), but the difference was not statistically significant (p=0.359), knowing that the outset of the study took place during the first lockdown period in France. The number of people living at home, including those who continued their professional activities, as well as the number of children under 15 years of age did not differ between both groups. Interestingly, COVID+ patients lived significantly more frequently in a flat compared to COVID– patients who lived more frequently in a house (p<0.005), and lived more frequently in urban areas (p=0.021). Patients tested positive for COVID-19 used significantly more public transport or taxi to come to the day hospital compared to negative patients who preferably used their own car (p=0.021).
3.6 Influence of trough levels on the risk of being infected by SARS-CoV-2
Neither infliximab nor vedolizumab trough levels significantly differed between COVID+ and COVID– patients (Table 5).
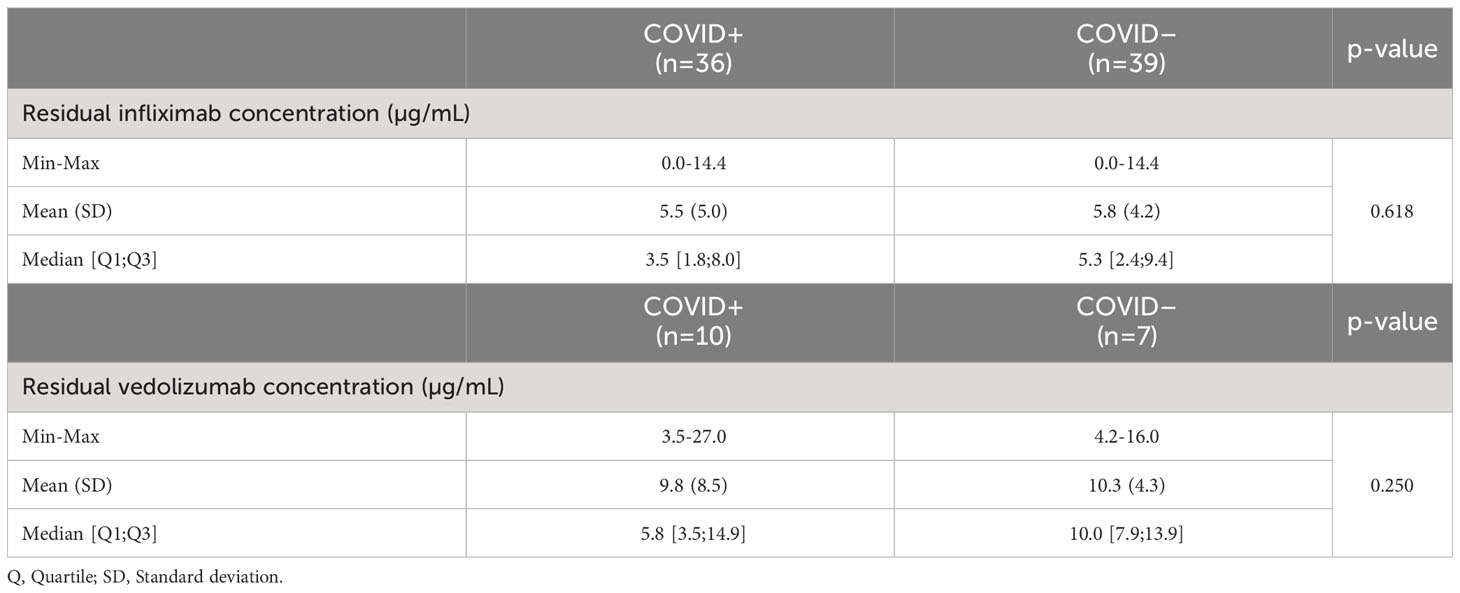
Table 5 Analysis of residual trough levels associated with SARS-CoV-2 infection in a matched 1:1 case-control sub-study (n=92).
Among the patients tested positive for COVID-19, 22 patients (61.1%) receiving infliximab had a residual drug level above the minimal trough concentration of 3 µg/mL defined by the BRIDGe consensus (36), versus 29 patients (74.4%) in the control group (p=0.900). Regarding vedolizumab, although the minimal trough concentration is less consensual, 3 patients (30.0%) had a residual drug level above 15 µg/mL, versus 3 (42.9%) in the control group (p=0.698).
4 Discussion
Based on a large cohort of French patients with IBD treated with either infliximab or vedolizumab during the first pandemic wave of COVID-19, we showed that the prevalence of SARS-CoV-2 infection in patients with IBD treated with intravenous biologics at day hospital was the same (4.5%) as the one in the general population at the same period (4.5%) (37), before the start of the vaccination campaign in France (January 2021).
In our cohort, there was no difference between patients treated with infliximab and those treated with vedolizumab in the risk of being infected by SARS-CoV-2. Neither infliximab nor vedolizumab trough levels significantly differed between COVID+ and COVID–patients with IBD. Patients tested positive for COVID-19 tended to be more treated in combination therapy with an immunosuppressant. Diabetes tended to be more frequent in patients with IBD tested positive, as was the case for hypertension, but none of these clinical factors was significantly associated with an increased risk of COVID-19. Interestingly, demographic factors seemed to be more influent in the risk of getting infected by SARS-CoV-2, notably the use of public transport and the way of living (flat in urban areas).
Recent data suggest that pre-existing auto-immune disease is associated with increased severity of COVID-19, but IBD was not the most frequent auto-immune disease in the dataset and the same study showed a protective effect of anti-TNF therapy, which is the most frequently used in patients with IBD (38). Conversely, the BELCOMID study described a benign course of COVID-19 infection in a cohort of more than 2000 patients with immune mediated inflammatory diseases (IMID) of whom more than 60% had IBD (39). The MICI-SARS-CoV-2 study provides physicians with data on this specific population of patients with IBD theoretically immunocompromised by their biological therapy before the start of the vaccination campaign.
The main strength of the MICI-SARS-CoV-2 study lies in its prospective and multicenter design with a large number of patients included over a short period of time, making it highly representative of the population of interest and very homogenous – all patients having been included during the first pandemic wave in France.
Our results are broadly similar with data published in the literature. European data from the first wave of the pandemic were also in favor of a low incidence of SARS-CoV-2 infection in patients with IBD, with slightly more hospitalizations but no severe infection (17, 18). In a study led in 24 Italian IBD centers in a region particularly affected during the first wave of the pandemic in Europe with more than 140,000 cases in March 2020 and more than 18,000 deaths, only 79 positive patients were reported, with 6 deaths (7%), in which anti-TNF was not a risk factor (odds ratio [OR] 0.4; 95% CI 0.04-3.78; p=0.42) (40). The trend is the same for non-digestive conditions in which anti-TNF drugs are frequently used, especially rheumatologic diseases. In an observational multicenter cohort retrospective study including patients suffering from rheumatologic diseases, only 600 cases of COVID-19 were reported in more than 40 countries. Nearly half of them were hospitalized due to the more frequent use of corticosteroids (32% in this population), with twice the risk of hospitalization under treatment (OR 2.05; 95% CI 1.06-3.96); conversely, biologics such as anti-TNF were at lower risk of hospitalization in this study (OR 0.40; 95% CI 0.19-0.81) (41).
Regarding the association of the occurrence of COVID-19 with socio-demographic factors, a single-center prospective Italian study including 386 patients with IBD also demonstrated that the prevalence of anti-SARS-CoV-2 antibodies was determined neither by the ongoing IBD-specific treatment nor disease-related characteristics. Only a close contact with SARS-CoV-2 positive individuals and the use of non-FFP2 masks were independently associated with a higher likelihood of seropositivity amongst patients with IBD, supporting the data of our study in which sanitary barrier measures look more important than clinical IBD characteristics (42).
The main limitation of the MICI-SARS-CoV-2 study is the low percentage of positive patients, probably limiting the statistical power of the results. This may be partly explained by the fact that the study was led during the first lockdown period in France, as we demonstrated a statistically significant difference between positive and negative patients on means of transport or accommodation, resulting in a decrease in the number of positive cases in the cohort.
The low seroprevalence at the end of the follow-up may also be due to a decrease in antibody levels in patients treated with infliximab, which may also explain the discordance in patients who had a positive PCR test during the follow-up but no anti-SARS-CoV-2 antibodies at the end of follow-up. Indeed, in this study, anti-SARS-CoV-2 antibodies were only assessed at the end of the follow-up for all patients, and in patients who were seropositive at the time of their last infusion, anti-SARS-CoV-2 antibody assays were retrospectively performed at each of their visit in order to determine the time of seroconversion. Thus, we may have underestimated the number of pauci-symptomatic infections if they were contracted early during the follow-up, particularly for patients treated with anti-TNF, that can attenuate seroprevalence as suggested in some studies (43, 44), even though another study recently showed that patients with IBD previously infected with COVID-19 have similar quantitative antibody response as healthy controls previously infected with COVID-19 (45). The parallel can be drawn with the response to the vaccination because the antibody levels after vaccination have been shown to be lower with anti-TNF agents than with other treatments, studied in this prospective case-control study (483 cases for 121 controls) between May and November 2021, in which the antibody level measured between 53 and 92 days after the second vaccination dose was lower under infliximab (geometric mean ratio 0.12, 95% CI 0.08-0.17; p<0.0001), compared to thiopurines (0.89, 0.64-1.24; p=0.50), ustekinumab (0.69, 0.41-1.19; p=0.18), or vedolizumab (1.16, 0.74-1.83; p=0.51) (32). These attenuated serological responses still exist after a third dose of an mRNA-based vaccine in infliximab- but not in vedolizumab-treated patients, as demonstrated recently in an analysis of the CLARITY IBD study (46).
It is important to note that the center effect could not be taken into account in our study because of the small number of COVID+ patients, thus we were not able to demonstrate higher seropositivity rates in regions in the east of France where the prevalence of SARS-CoV-2 infection was higher in the general population during the first wave of the pandemic in France.
The biological collection that was created during this study, with multiples serum samples per patient stored in optimal conditions, will be used for further immunological analyses to try to address some of these pending issues.
In conclusion, the prevalence rate of SARS-CoV-2 infection in this French IBD population treated with intravenous infliximab or vedolizumab was the same as the one in the general population before the start of the vaccination campaign, with no severe case of COVID-19 and no long-term sequelae. We demonstrated that the risk of COVID-19 is related neither to the use of treatment, including in combination therapy, nor to the activity of the disease. Importantly, residual drug levels do not seem to influence the risk of infection. Conversely, infections were more frequent when using public transport or living in flats in urban areas. Sanitary barrier measures are therefore fundamental for these patients, as much or more important than vaccination coverage. Thus, simple measures such as regular hand washing and wearing a face mask in enclosed spaces remain the best way to protect against the virus.
These real-world data on the risk of COVID-19 in IBD patients treated with intravenous biologics outside any vaccination context are important for physicians who are confronted daily with patients reluctant to be vaccinated. Indeed, although the safety and efficacy of COVID-19 vaccination in IBD patients is now well established (34), a significant proportion of patients, especially the youngest (28), still wonder on the risk-benefit ratio of being vaccinated, perhaps with good reason given the low prevalence of COVID-19 in this cohort of IBD patients established before any vaccination, and the lower risk of severe form of COVID-19 in young patients than in the elderly (12). Thus, these data from the MICI-SARS-COV-2 study will enable physicians to emphasize the importance of maintaining sanitary barrier measures to these vaccine-refractory patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was a non-interventional trial approved by the Comité de Protection des Personnes (CPP) Ile-de-France VI (institutional review board) on 30 March 2020 under the number 20.03.27.48341. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ML, FV, AB and CLB: study concept and design. ML, RJ, MB, MR, CB-B, FV, GG, MB, CB, JC, AB, CLB: acquisition of data, analysis and interpretation of data. ML, AB, CLB: drafting of the manuscript. ML, RJ, MB, MR, CB-B, LP-B, FV, GG, MB, CB, JC, AB, CLB: critical revision of the manuscript for important intellectual content. All the authors read and approved the final version of the manuscript.
Funding
Fonds de dotation CHU Nantes (AB). AOI analyse secondaire 2020 (CHU Nantes) (AB). Fondation SantéDige 2020 (AB). Fonds métropolitain d’appui aux innovations en santé liées au COVID-19 (Nantes Métropole) (AB). GETAID.
Acknowledgments
We thank the GETAID for the financial and practical support provided for this study. We thank GRIFOLS INTERNATIONAL SA for having provided the kits for the dosage of infliximab and vedolizumab trough levels.
Conflict of interest
SN declares counseling, boards, transports or fees from Abbvie, Biogen, HAC-pharma, Janssen, MSD, Novartis, Pfizer, Takeda, Tillots, BMS, Amgen, Galapagos and Fresenius. Prof. Bouguen received lecture fees from Abbvie, Ferring, MSD, Takeda and Pfizer and consultant fees from Takeda, Janssen. MA reports consulting or lecture fees from AbbVie, Amgen, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Ferring, Genentech, Gilead, IQVIA, Janssen, Novartis, Pfizer, Roche, Takeda, and Tillots; and grant support from Innate Pharma, Janssen, Takeda, and Genentech/Roche. MS has received lecture or consulting fees from Abbvie, Ferring, Amgen, Celltrion, Janssen, Ferring, Takeda and Tillotts. LC received board and lecture fees from Abbvie, Janssen, Pfizer, Takeda, Amgen. CR has received payment for lectures from Abbvie, Biogen and Galapagos. PB has received payment for lectures from Abbvie, Pfizer, Tillotts, Fresenius Kabi and Gilead. DL declares counseling, boards, transports or fees from Abbvie, Biogaran, Biogen, Ferring, Galapagos, Janssen, Lilly, MSD, Novartis, Pfizer, Prometheus, Roche, Takeda. LP-B has served as a consultant for Abbvie, Alimentiv, Alma Bio Therapeutics, Amgen, Applied Molecular Transport, Arena, Biogen, BMS, Celltrion, CONNECT Biopharm, Cytoki Pharma, Enthera, Ferring, Fresenius Kabi, Galapagos, Genentech, Gilead, Gossamer Bio, GSK, HAC-Pharma, IAG Image Analysis, Index Pharmaceuticals, Inotrem, Janssen, Lilly, Medac, Mopac, Morphic, MSD, Norgine, Novartis, OM Pharma, ONO Pharma, OSE Immunotherapeutics, Pandion Therapeutics, Par’Immune, Pfizer, Prometheus, Protagonist, Roche, Sandoz, Takeda, Theravance, Thermo Fisher, Tigenix, Tillots, Viatris, Vifor, Ysopia, Abivax; has received payment for lectures from Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Sandoz, Biogen, MSD, Amgen, Vifor, Arena, Lilly, Gilead, Viatris, Medac, Sanofi; reports grant support from Takeda, Fresenius Kabi, Celltrion; has received meeting support fees from Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Gossamer Bio, Sandoz, MSD, Amgen, Lilly, Gilead, Thermo Fisher, Medac, CONNECT Biopharm. AM has received payment for lectures from Galapagos. CT-P has reveived lecture fees from Ferring, Janssen, Mayoly spindler, Norgine, Abbvie, MSD, and Takeda. AB declares lecture or consulting fees from Abbvie, Amgen, Celltrion, Ferring, Fresenius Kabi, Galapagos, Gilead, Janssen, MSD, OSE Immunotherapeutics, Pfizer, Roche, Takeda, and Tillotts. CLB has served as a consultant for Abbvie, Janssen and Gilead; has received payment for lectures from Abbvie, Amgen, Celltrion, Ferring, Fresenius Kabi, Galapagos, Janssen, Lilly, MSD, Pfizer, and Takeda; reports grant support from Abbvie and Takeda; has received meeting support fees from Abbvie, Ferring, Fresenius Kabi, Galapagos, Janssen, Lilly, Pfizer, Sandoz, and Takeda.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol (2020) 5:17–30. doi: 10.1016/S2468-1253(19)30333-4
2. Bitton A, Vutcovici M, Sewitch M, Suissa S, Brassard P. Mortality trends in Crohn’s disease and ulcerative colitis: A population-based study in Québec, Canada. Inflammation Bowel Dis (2016) 22:416–23. doi: 10.1097/MIB.0000000000000608
3. Jussila A, Virta LJ, Pukkala E, Färkkilä MA. Mortality and causes of death in patients with inflammatory bowel disease: a nationwide register study in Finland. J Crohns Colitis (2014) 8:1088–96. doi: 10.1016/j.crohns.2014.02.015
4. Bernstein CN, Nugent Z, Targownik LE, Singh H, Lix LM. Predictors and risks for death in a population-based study of persons with IBD in Manitoba. Gut (2015) 64:1403–11. doi: 10.1136/gutjnl-2014-307983
5. Lelli F, Nuhoho S, Lee XY, Xu W. Systematic review: treatment pattern and clinical effectiveness and safety of pharmaceutical therapies for Crohn’s disease in Europe. Clin Exp Gastroenterol (2016) 9:311–23. doi: 10.2147/CEG.S109696
6. Armuzzi A, DiBonaventura Md, Tarallo M, Lucas J, Bluff D, Hoskin B, et al. Treatment patterns among patients with moderate-to-severe ulcerative colitis in the United States and Europe. PloS One (2020) 15:e0227914. doi: 10.1371/journal.pone.0227914
7. Wisniewski A, Kirchgesner J, Seksik P, Landman C, Bourrier A, Nion-Larmurier I, et al. Increased incidence of systemic serious viral infections in patients with inflammatory bowel disease associates with active disease and use of thiopurines. United Eur Gastroenterol J (2020) 8:303–13. doi: 10.1177/2050640619889763
8. Tinsley A, Navabi S, Williams ED, Liu G, Kong L, Coates MD, et al. Increased risk of influenza and influenza-related complications among 140,480 patients with inflammatory bowel disease. Inflammation Bowel Dis (2019) 25:369–76. doi: 10.1093/ibd/izy243
9. Kirchgesner J, Lemaitre M, Carrat F, Zureik M, Carbonnel F, Dray-Spira R. Risk of serious and opportunistic infections associated with treatment of inflammatory bowel diseases. Gastroenterology (2018) 155:337–346.e10. doi: 10.1053/j.gastro.2018.04.012
10. Abraham E, Wunderink R, Silverman H, Perl TM, Nasraway S, Levy H, et al. Efficacy and safety of monoclonal antibody to human tumor necrosis factor alpha in patients with sepsis syndrome. A randomized, controlled, double-blind, multicenter clinical trial. TNF-alpha MAb Sepsis Study Group. JAMA (1995) 273:934–41. doi: 10.1001/jama.1995.03520360048038
11. Singh S, Facciorusso A, Dulai PS, Jairath V, Sandborn WJ. Comparative risk of serious infections with biologic and/or immunosuppressive therapy in patients with inflammatory bowel diseases: A systematic review and meta-analysis. Clin Gastroenterol Hepatol (2020) 18:69–81.e3. doi: 10.1016/j.cgh.2019.02.044
12. Fang X, Li S, Yu H, Wang P, Zhang Y, Chen Z, et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: a systematic review and meta-analysis. Aging (2020) 12:12493–503. doi: 10.18632/aging.103579
13. Li J, He X, Yuan Y, Zhang W, Li X, Zhang Y, et al. Meta-analysis investigating the relationship between clinical features, outcomes, and severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia. Am J Infect Control (2021) 49:82–9. doi: 10.1016/j.ajic.2020.06.008
14. Zhou Y, Chi J, Lv W, Wang Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid-19). Diabetes Metab Res Rev (2021) 37:e3377. doi: 10.1002/dmrr.3377
15. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
16. Caillard S, Thaunat O, Hazzan M. Covid-19 en transplantation rénale, leçons du registre français. Nephrol Ther (2021) 17:233–44. doi: 10.1016/j.nephro.2021.01.002
17. Zabana Y, Marín-Jiménez I, Rodríguez-Lago I, Vera I, Martín-Arranz MD, Guerra I, et al. Nationwide COVID-19-EII study: incidence, environmental risk factors and long-term follow-up of patients with inflammatory bowel disease and COVID-19 of the ENEIDA registry. J Clin Med (2022) 11:421. doi: 10.3390/jcm11020421
18. Attauabi M, Poulsen A, Theede K, Pedersen N, Larsen L, Jess T, et al. Prevalence and outcomes of COVID-19 among patients with inflammatory bowel disease-A danish prospective population-based cohort study. J Crohns Colitis (2021) 15:540–50. doi: 10.1093/ecco-jcc/jjaa205
19. Meyer A, Semenzato L, Zureik M, Weill A, Carbonnel F, Dray-Spira R. Risk of severe COVID-19 in patients treated with IBD medications: a French nationwide study. Aliment Pharmacol Ther (2021) 54:160–6. doi: 10.1111/apt.16410
20. Ludvigsson JF, Axelrad J, Halfvarson J, Khalili H, Larsson E, Lochhead P, et al. Inflammatory bowel disease and risk of severe COVID-19: A nationwide population-based cohort study in Sweden. United Eur Gastroenterol J (2021) 9:177–92. doi: 10.1002/ueg2.12049
21. Tripathi K, Godoy Brewer G, Thu Nguyen M, Singh Y, Saleh Ismail M, Sauk JS, et al. COVID-19 and outcomes in patients with inflammatory bowel disease: systematic review and meta-analysis. Inflammation Bowel Dis (2021) 28(8):1265–79. doi: 10.1093/ibd/izab236
22. Alrashed F, Battat R, Abdullah I, Charabaty A, Shehab M. Impact of medical therapies for inflammatory bowel disease on the severity of COVID-19: a systematic review and meta-analysis. BMJ Open Gastroenterol (2021) 8:e000774. doi: 10.1136/bmjgast-2021-000774
23. Ungaro RC, Brenner EJ, Agrawal M, Zhang X, Kappelman MD, Colombel J-F, et al. Impact of medications on COVID-19 outcomes in inflammatory bowel disease: analysis of more than 6000 patients from an international registry. Gastroenterology (2022) 162:316–319.e5. doi: 10.1053/j.gastro.2021.09.011
24. Bezzio C, Armuzzi A, Furfaro F, Ardizzone S, Milla M, Carparelli S, et al. Therapies for inflammatory bowel disease do not pose additional risks for adverse outcomes of SARS-CoV-2 infection: an IG-IBD study. Aliment Pharmacol Ther (2021) 54:1432–41. doi: 10.1111/apt.16663
25. Agrawal M, Zhang X, Brenner EJ, Ungaro RC, Kappelman MD, Colombel J-F. The impact of vedolizumab on COVID-19 outcomes among adult IBD patients in the SECURE-IBD registry. J Crohns Colitis (2021) 15:1877–84. doi: 10.1093/ecco-jcc/jjab071
26. Chanchlani N, Lin S, Chee D, Hamilton B, Nice R, Arkir Z, et al. Adalimumab and infliximab impair SARS-CoV-2 antibody responses: results from a therapeutic drug monitoring study in 11 422 biologic-treated patients. J Crohns Colitis (2022) 16:389–97. doi: 10.1093/ecco-jcc/jjab153
27. Kennedy NA, Goodhand JR, Bewshea C, Nice R, Chee D, Lin S, et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut (2021) 70:865–75. doi: 10.1136/gutjnl-2021-324388
28. Clarke K, Pelton M, Stuart A, Tinsley A, Dalessio S, Bernasko N, et al. COVID-19 vaccine hesitancy in patients with inflammatory bowel disease. Dig Dis Sci (2022) 67:4671–7. doi: 10.1007/s10620-021-07377-5
29. Shehab M, Zurba Y, Al Abdulsalam A, Alfadhli A, Elouali S. COVID-19 vaccine hesitancy among patients with inflammatory bowel disease receiving biologic therapies in Kuwait: A cross-sectional study. Vaccines (2021) 10:55. doi: 10.3390/vaccines10010055
30. Martín Arranz MD, García-Ramírez L, Martín Arranz E, Montero Vega D, Rueda García JL, Sánchez-Azofra M, et al. Serologic response to COVID-19 vaccines in patients with inflammatory bowel disease: a prospective study. Rev Esp Enferm Dig (2023) 115(8):444–9. doi: 10.17235/reed.2022.9101/2022
31. Shehab M, Alrashed F, Alfadhli A, Alotaibi K, Alsahli A, Mohammad H, et al. Serological response to BNT162b2 and chAdOx1 nCoV-19 vaccines in patients with inflammatory bowel disease on biologic therapies. Vaccines (Basel) (2021) 9:1471. doi: 10.3390/vaccines9121471
32. Alexander JL, Kennedy NA, Ibraheim H, Anandabaskaran S, Saifuddin A, Castro Seoane R, et al. COVID-19 vaccine-induced antibody responses in immunosuppressed patients with inflammatory bowel disease (VIP): a multicentre, prospective, case-control study. Lancet Gastroenterol Hepatol (2022) 7:342–52. doi: 10.1016/S2468-1253(22)00005-X
33. Pellegrino R, Pellino G, Selvaggi L, Selvaggi F, Federico A, ROmano M, et al. BNT162b2 mRNA COVID-19 vaccine is safe in a setting of patients on biologic therapy with inflammatory bowel diseases: a monocentric real-life study. Expert Rev Clin Pharmacol (2022) 15:1243–52. doi: 10.1080/17512433.2022.2120466
34. Markovinović A, Quan J, Herauf M, Hracs L, Windsor JW, Sharifi N, et al. Adverse events and serological responses after SARS-coV-2 vaccination in individuals with inflammatory bowel disease. Am J Gastroenterol (2023). doi: 10.14309/ajg.0000000000002337
35. Kim Y, Lee JH, Ko GY, Ryu JH, Jang JH, Bae H, et al. Quantitative SARS-CoV-2 spike antibody response in COVID-19 patients using three fully automated immunoassays and a surrogate virus neutralization test. Diagnostics (2021) 11:1496. doi: 10.3390/diagnostics11081496
36. Papamichael K, Cheifetz AS, Melmed GY, Irving PM, Vande Casteele N, Kozuch PL, et al. Appropriate therapeutic drug monitoring of biologic agents for patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol (2019) 17:1655–1668.e3. doi: 10.1016/j.cgh.2019.03.037
37. Santé Publique France. J du COVID19_PE_20201231. Available at: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-31-decembre-2020.
38. Yadaw AS, Sahner DK, Sidky H, Afzali B, Hotaling N, Pfaff ER, et al. N3C consortium. Pre-existing autoimmunity is associated with increased severity of COVID-19: A retrospective cohort study using data from the National COVID Cohort Collaborative (N3C). Clin Infect Dis (2023) 19:ciad294. doi: 10.1093/cid/ciad294
39. Geldof J, Truyens M, Sabino J, Ferrante M, Lambert J, Lapeere H, et al. SARS-CoV-2 infection and COVID19 vaccination across eight immune-mediated inflammatory disorders: A prospective, real-life Belgian cohort study – the BELCOMID study. Front Immunol (2023) 14:1126351. doi: 10.3389/fimmu.2023.1126351
40. Bezzio C, Saibeni S, Variola A, Allocca M, Massari A, Gerardi V, et al. Outcomes of COVID-19 in 79 patients with IBD in Italy: an IG-IBD study. Gut (2020) 69:1213–7. doi: 10.1136/gutjnl-2020-321411
41. GianFrancesco M, Hyrich KL, Al-Adely S, Carmona L, Danila MI, Gossec L, et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis (2020) 79:859–66. doi: 10.1136/annrheumdis-2020-217871
42. Di Ruscio M, Lunardi G, Buonfrate D, Gobbi F, Bertoli G, Piccoli D, et al. A seroprevalence study of anti-SARS-CoV-2 antibodies in patients with inflammatory bowel disease during the second wave of the COVID-19 pandemic in Italy. Medicina (Kaunas) (2021) 57:1048. doi: 10.3390/medicina57101048
43. Kaplan GG, Ma C, Charlton C, Kanji JN, Tipples G, Sharifi N, et al. Antibody response to SARS-CoV-2 among individuals with IBD diminishes over time: a serosurveillance cohort study. Gut (2022) 71:1229–31. doi: 10.1136/gutjnl-2021-325238
44. van Dam KPJ, Volkers AG, Wieske L, Stalman EW, Kummer LYL, van Kempen ZLE, et al. Primary SARS-CoV-2 infection in patients with immune-mediated inflammatory diseases: long-term humoral immune responses and effects on disease activity. BMC Infect Dis (2023) 23:332. doi: 10.1186/s12879-023-08298-6
45. Doherty J, Morain N O, Stack R, Tosetto M, Inzitiari R, Reilly SO, et al. Reduced serological response to COVID-19 booster vaccine is associated with reduced B cell memory in patients with Inflammatory Bowel Disease; VARIATION (VAriability in Response in IBD AgainsT SARS-CoV-2 ImmunisatiON). J Crohns Colitis (2023) 5:jjad065. doi: 10.1093/ecco-jcc/jjad065
Keywords: Crohn’s disease, ulcerative colitis, infliximab, vedolizumab, SARS-CoV-2, trough levels
Citation: Lelong M, Josien R, Coste-Burel M, Rimbert M, Bressollette-Bodin C, Nancey S, Bouguen G, Allez M, Serrero M, Caillo L, Rouillon C, Blanc P, Laharie D, Olivier R, Peyrin-Biroulet L, Dib N, De Maissin A, Montuclard C, Trang-Poisson C, Vavasseur F, Gallot G, Berthome M, Braudeau C, Chevreuil J, Bourreille A and Le Berre C (2023) The risk of COVID-19 in IBD patients is increased by urban living and is not influenced by disease activity or intravenous biologics. Front. Immunol. 14:1243898. doi: 10.3389/fimmu.2023.1243898
Received: 21 June 2023; Accepted: 14 August 2023;
Published: 28 August 2023.
Edited by:
Pier Paolo Sainaghi, University of Eastern Piedmont, ItalyReviewed by:
Alenka Gagro, Children’s Hospital Zagreb, CroatiaAntonietta G. Gravina, University of Campania Luigi Vanvitelli, Italy
Copyright © 2023 Lelong, Josien, Coste-Burel, Rimbert, Bressollette-Bodin, Nancey, Bouguen, Allez, Serrero, Caillo, Rouillon, Blanc, Laharie, Olivier, Peyrin-Biroulet, Dib, De Maissin, Montuclard, Trang-Poisson, Vavasseur, Gallot, Berthome, Braudeau, Chevreuil, Bourreille and Le Berre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Le Berre, Y2F0aGVyaW5lQGxlYmVycmUub3Jn
†These authors have contributed equally to this work