 Ariel Israel1,2*
Ariel Israel1,2* Alejandro A. Schäffer3
Alejandro A. Schäffer3 Matitiahu Berkovitch2,4
Matitiahu Berkovitch2,4 David J. Ozeri1,5
David J. Ozeri1,5 Eugene Merzon1,6Ilan Green1,2Avivit Golan-Cohen1,2Eytan Ruppin3Shlomo Vinker1,2
Eugene Merzon1,6Ilan Green1,2Avivit Golan-Cohen1,2Eytan Ruppin3Shlomo Vinker1,2 Eli Magen1,7
Eli Magen1,7- 1Leumit Research Institute, Leumit Health Services, Tel Aviv-Yafo, Israel
- 2School of Public Health and Family Medicine Department, Faculty of Medicine, Tel Aviv University, Tel Aviv-Yafo, Israel
- 3Cancer Data Science Laboratory, National Cancer Institute, Bethesda, MD, United States
- 4Clinical Pharmacology and Toxicology Unit, Shamir Medical Center, Zerifin, Israel
- 5Division of Rheumatology, Sheba Medical Center, Ramat Gan, Israel
- 6Adelson School of Medicine, Ariel University, Ariel, Israel
- 7Medicine A Department, Assuta Ashdod University Hospital Faculty of Health Sciences, Ben-Gurion University, Beer-Sheba, Israel
Introduction: Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an X-linked enzymatic disorder that is particularly prevalent in Africa, Asia, and the Middle East. This study aimed to assess the long-term health risks associated with G6PD deficiency.
Methods: A retrospective cohort study was conducted using data from a national healthcare provider in Israel (Leumit Health Services). A total of 7,473 G6PD-deficient individuals were matched with 29,892 control subjects in a 1:4 ratio, based on age, gender, socioeconomic status, and ethnic groups. The exposure of interest was recorded G6PD diagnosis or positive G6PD diagnostic test. The main outcomes and measures included rates of infectious diseases, allergic conditions, and autoimmune disorders between 2002 and 2022.
Results: Significantly increased rates were observed for autoimmune disorders, infectious diseases, and allergic conditions in G6PD-deficient individuals compared to the control group. Specifically, notable increases were observed for rheumatoid arthritis (odds ratio [OR] 2.41, p<0.001), systemic lupus erythematosus (OR 4.56, p<0.001), scleroderma (OR 6.87, p<0.001), pernicious anemia (OR 18.70, p<0.001), fibromyalgia (OR 1.98, p<0.001), Graves’ disease (OR 1.46, p=0.001), and Hashimoto’s thyroiditis (OR 1.26, p=0.001). These findings were supported by elevated rates of positive autoimmune serology and higher utilization of medications commonly used to treat autoimmune conditions in the G6PD-deficient group.
Discussion: In conclusion, individuals with G6PD deficiency are at a higher risk of developing autoimmune disorders, infectious diseases, and allergic conditions. This large-scale observational study provides valuable insights into the comprehensive association between G6PD deficiency and infectious and immune-related diseases. The findings emphasize the importance of considering G6PD deficiency as a potential risk factor in clinical practice and further research is warranted to better understand the underlying mechanisms of these associations.
Introduction
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is the most common enzymatic X-linked human disorder and it primarily affects red blood cells (1). An estimated 400 million people worldwide carry a mutation in the G6PD gene associated with enzyme deficiency, with marked ethnic and geographic differences (2, 3). G6PD deficiency is prevalent in Africa, Asia and the Middle East. In the United States, about 14% of African-American men are affected (4, 5). There are numerous alleles of different severities and geographic propensities (6). Most individuals with G6PD deficiency remain asymptomatic or experience mild symptoms throughout their lives but may develop hemolysis under certain circumstances such as neonatal jaundice, consumption of specific medications, or following an infection.
Several studies have suggested that G6PD-deficient individuals may be more predisposed to specific autoimmune diseases (7, 8), infections (9–11) and diabetes mellitus (12, 13). Associations were found between G6PD deficiency and cardiovascular risk (14–17) in conflicting directions. Regarding malignancy, key studies have reported lower rates of cancer in G6PD-deficient patients, in particular for cancers of endodermal origin (colorectal, gastric and liver malignancies) (18, 19), but a protective effect of G6PD against cancer was not found for other types of cancer and notably hematologic malignancies (20, 21). We recently reported that individuals with G6PD deficiency had an increased risk of COVID-19 infection and severity, with higher rates of hospitalization and diagnosed long COVID (22).
To date, there is no large-scale study showing the association of G6PD deficiency with infectious and immune-related diseases altogether. This large-scale observational study addresses this knowledge gap.
Methods
Cohort data source
We performed a retrospective cohort study using data from Leumit Health Services (LHS), one of the four nationwide healthcare providers in Israel (23). LHS has been using centrally managed electronic health records (EHR) for the last 20 years. The EHRs includes demographic data, physical measures, laboratory test results, medication prescription and purchases, and diagnosed conditions, documented by physicians according to International Classification of Diseases 9th Revision (ICD-9).
Data were collected from the LHS data warehouse as of December 31, 2022. The study cohort was drawn from a pool of over a million individuals who had been insured at least two years by LHS between 2002 and 2022.
Cohort design
The study involves the comparison of two matched groups of individuals. The G6PD deficiency group consists of patients with a documented diagnosis of G6PD deficiency or a recorded laboratory test of G6PD activity performed in LHS, resulting in a measurement below 4 U/g Hg.
The control group included individuals without G6PD deficiency who exactly matched individuals in the G6PD deficiency group on the following variables: gender, age, geographic area based socio-economic status (SES) category, ethnic group, and year of first documented visit in LHS EHR system, with a ratio of 4 controls for each included G6PD deficient patient. Individuals with G6PD deficiency for which the matching algorithm was not able to find four control individuals with identical matching features were left out from the analysis.
Demographic records were extracted from LHS data warehouse, along with ICD-9 diagnosis records matching a list of pre-defined conditions, the last recorded body mass index (BMI), blood pressure (BP) measures, and smoking habits. The last laboratory test results for a set of predefined laboratory measures performed by LHS laboratory facilities were also extracted.
Statistical methods
Statistical association was assessed using Fisher’s Exact Test for binary variables, with odds-ratio and 95% confidence interval (CI). Numerical variables were tested using the Mann-Whitney U test, which does not assume a normal distribution. Cohort data extraction was performed using programs developed by Leumit Research Institute in Python. Statistics were computed in R statistical software, version 4.0.4.
Results
Demographic and laboratory characteristics
Among the pool of 1,031,354 LHS members with at least two years of medical history in the EHR, we identified 7,827 individuals with either a G6PD deficiency diagnosis or laboratory evidence of G6PD deficiency. The matching procedure selected 7,473 G6PD deficient subjects with 29,892 control subjects (4:1 control ratio) of the same gender, age, socioeconomic category, ethnic group, and year of first recorded visit in LHS (354 G6PD deficient individuals were left out for lack of proper matching controls). The demographic characteristics of the two groups are shown in Table 1. The mean patient age was 29.2 ± 22.3 years, 68.7% were men, and the mean follow-up time was 14.3 ± 6.2 years in both groups. There were no statistically significant differences in gender, age, ethnic and socio-economic groups and follow-up time between the two study groups.

Table 1 Demographic characteristics of G6PD deficient subjects and matched controls.
Comorbidities of G6PD subjects and controls
The proportions of individuals in the two groups who had at least one diagnosis record for the studied conditions are presented in Table 2, together with the odds ratio (OR) and 95% confidence intervals (CI).
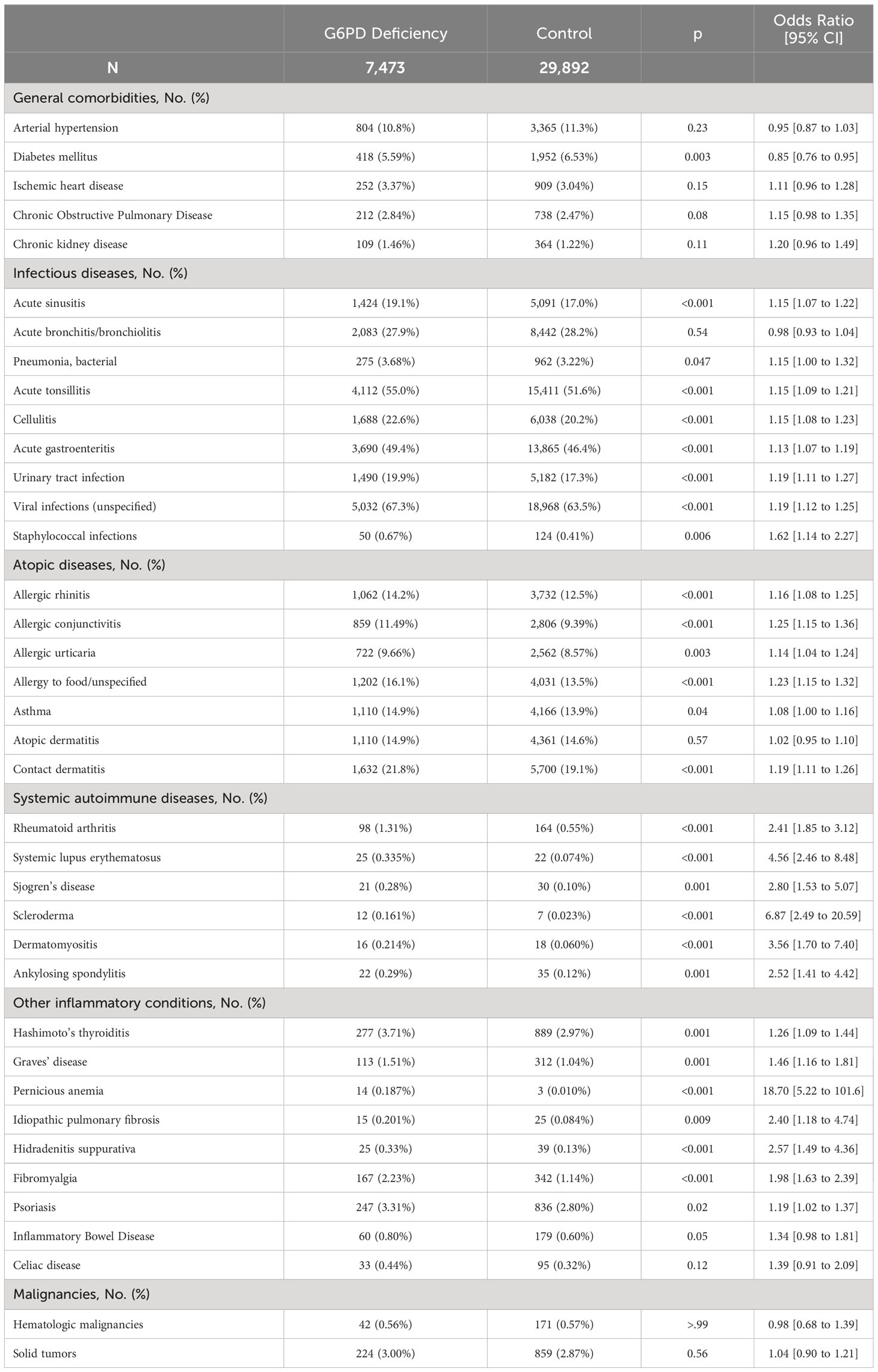
Table 2 Clinical characteristics of G6PD deficient subjects and matched controls.
General comorbidities
The proportions of patients with hypertension, ischemic heart disease, chronic obstructive pulmonary disease (COPD) and chronic kidney disease were not statistically different in the two groups, but there were comparably fewer individuals with diabetes mellitus in the G6PD deficient group (OR 0.85, 95% CI, 0.76 to 0.95, P=.003).
Infectious diseases
Most infectious diseases tested were significantly more frequent among G6PD deficient subjects than in controls (Table 2), with odds ratios typically around 1.15, with the notable exception of acute bronchitis/bronchiolitis which had a similar cumulative occurrence of ~28% in the two groups. Strong associations were observed for urinary tract infections (OR 1.19, 95% CI 1.14 to 1.27, P<0.001) and unspecified viral infections (OR 1.19, 95% CI 1.12 to 1.25, P<0.001). Staphylococcal infections were particularly more frequent among G6PD deficient patients (OR 1.62, 95% CI 1.14 to 2.27, P<.001).
Allergic/atopic conditions
For most of the atopic or allergic conditions assessed, we observed a higher prevalence among G6PD deficient individuals than in the control group (Table 2), notably for allergic conjunctivitis (OR 1.25, 95% CI 1.15 to 1.36, P<.001), allergy to food/unspecified (OR 1.23, 95% CI 1.15 to 1.32, P<.001), contact dermatitis (OR 1.19, 95% CI 1.15 to 1.32, P<.001) and allergic urticaria (OR 1.14, 95% CI 1.04 to 1.24, P<.001). Asthma was slightly more frequent among G6PD deficient individuals (OR 1.08, 95% CI 1.00 to 1.16, P=.043). In contrast, atopic dermatitis rate was similar among G6PD deficient patients and the control group.
Systemic autoimmune diseases
Systemic autoimmune diseases were strikingly more frequent in the G6PD group (Table 2). The association was particularly notable for scleroderma (OR 6.87, 95% CI 2.49 to 20.59, P<.001), systemic lupus erythematosus (SLE) (OR 4.56, 95% CI 2.46 to 8.48, P<.001), dermatomyositis (OR 3.56, 95% CI 1.70 to 7.40, P<.001). Major risk associations were also observed for rheumatoid arthritis (OR 2.41, 95% CI 1.85 to 3.12, P<.001), Sjögren’s syndrome (OR 2.80, 95% CI 1.53 to 5.07, P=.001) and ankylosing spondylitis (OR 2.52, 95% CI 1.41 to 4.42, P=.001).
We confirmed these findings by querying the proportion of individuals in each group who had purchased at least once, medications commonly used for autoimmune diseases, such as methotrexate (OR 2.30, 95% CI 1.74 to 3.02, P<.001), hydroxychloroquine (OR 2.78, 95% CI 2.08 to 3.71, P<.001), etanercept (OR 3.51,95% CI 2.03 to 6.02, P<.001) and leflunomide (OR 3.55, 95% CI 1.93 to 6.47, P<.001). We also queried serological tests commonly used to diagnose autoimmune conditions (Table 3A). The G6PD deficient group had significantly higher rates of positive serological tests for antinuclear (OR 1.81), anti-histones (OR 2.96), RNP-68 (OR 4.00), and anti-Smith (OR 5.00) antibodies.
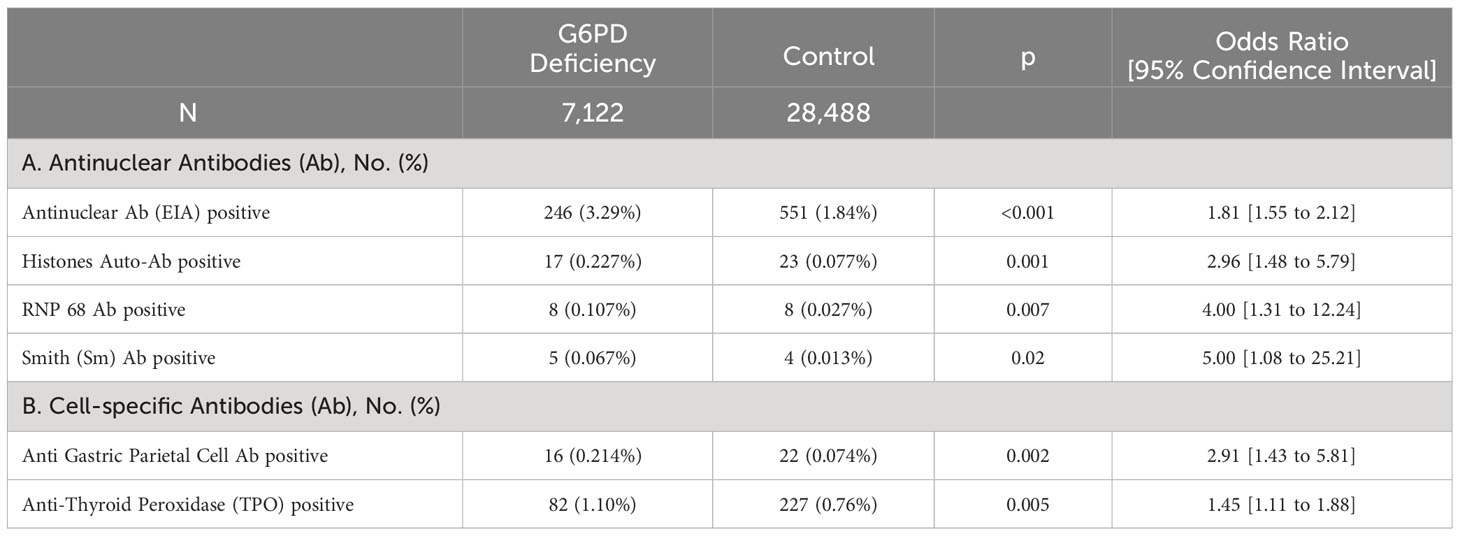
Table 3 Autoimmune serology in G6PD deficient subjects and matched controls.
Other inflammatory conditions
We further compared the two groups for a few organ-specific inflammatory conditions. We observed significantly higher rate of Hashimoto’s thyroiditis (OR 1.26, 95% CI 1.09 to 1.44, P=.001) and Graves’ disease (OR 1.46, 95% CI 1.16 to 1.81, P=.03). Significantly higher rates were also observed for pernicious anemia (OR 18.70, 95% CI 5.22 to 101.6, P<.001), idiopathic pulmonary fibrosis (OR 2.40, 95% CI 1.18 to 4.74, P=.009) and hidradenitis suppurativa (OR 2.57, 95% CI 1.49 to 4.36, P<.001). Psoriasis rate was also elevated to a lesser extent (OR 1.19, 95% CI 1.02 to 1.37, P=.02). Interestingly fibromyalgia rate was significantly higher in the G6PD deficient group (OR 1.98, 95% CI 1.63 to 2.39, P<.001). Inflammatory bowel disease (IBD) was more frequent with borderline statistical significance (OR=1.34, 95% CI 0.98 to 1.81, P=.05). We confirmed the elevated rates of pernicious anemia and thyroiditis by comparing the rate of positive tests for anti-gastric parietal cells and anti-TPO in the two groups. Both were significantly elevated (Table 3B).
Malignancy conditions
There were no statistically significant differences in the rates of hematologic malignancies and solid tumors.
Laboratory tests in G6PD subjects and controls
To better understand the biological basis of these associations, we compared laboratory test results of individuals from the two groups. Table 4 displays the median and interquartile ranges (IQR) of the last test performed per patient together with the p-value for comparison and standardized mean difference (SMD).
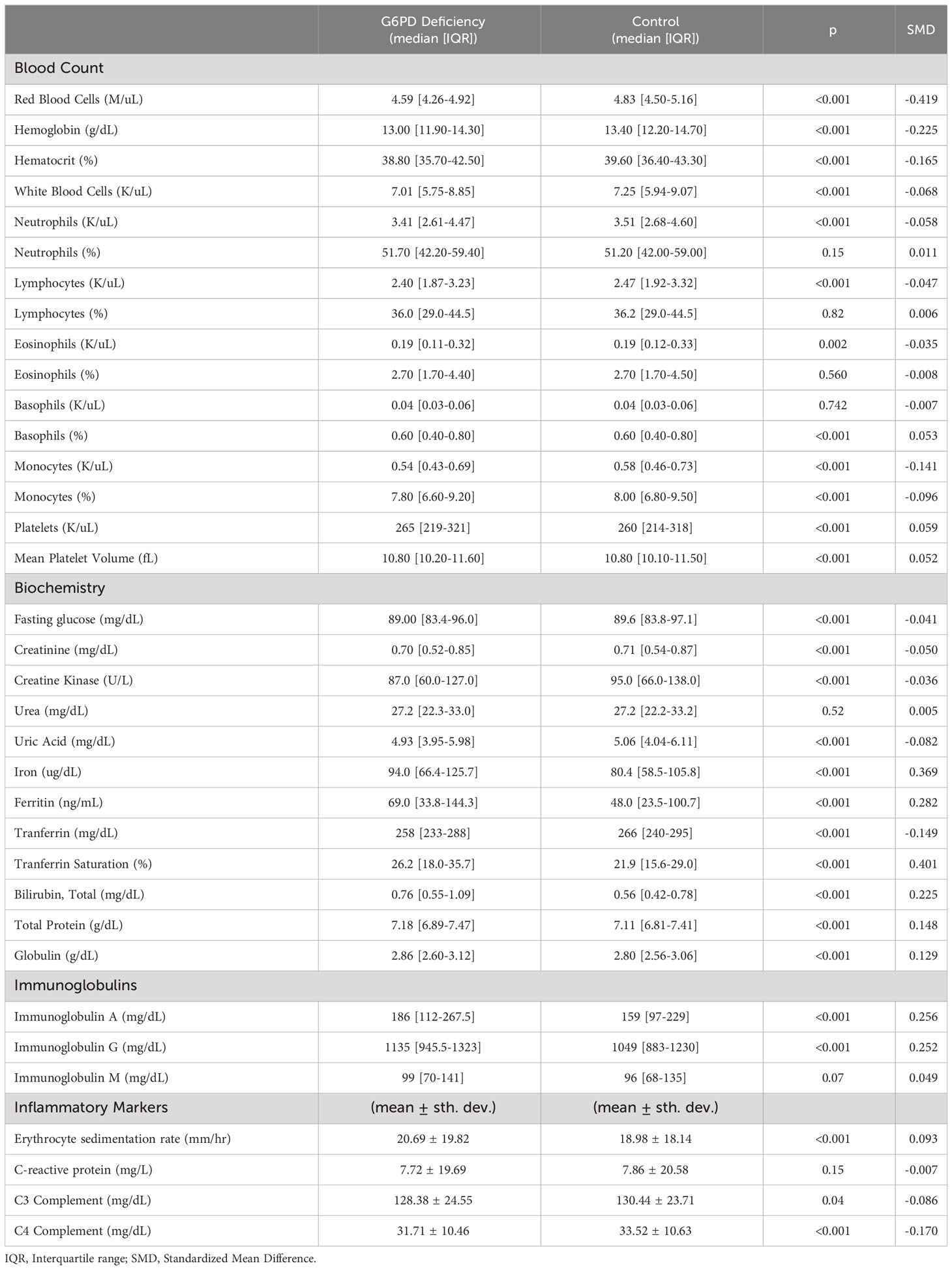
Table 4 Laboratory characteristics of G6PD deficient subjects and matched controls.
As expected for a condition associated with hemolysis, we observed significantly lower levels of red blood cells (P<.001, SMD=-0.419), hemoglobin (P<.001, SMD=-0.225) and hematocrit (P<.001, SMD=-0.165) in the G6PD deficient group. Interestingly, we also observed lower levels of white blood cells (WBC) (P<.001, SMD=-0.068) in general, and more specifically, diminished monocytes (P<.001, SMD=-0.141) and neutrophils (P<.001, SMD=-0.058). The breakdown of cell types among WBC was not significantly different in G6PD deficiency, except for monocytes, which have a decreased percentage among WBC (P<.001, SMD=-0.096), whereas the percentage of basophils was increased in G6PD deficient individuals (P<.001, SMD=0.053). Platelets are also present in higher numbers in G6PD deficient patients (P<.001, SMD=0.059) with increased mean platelet volume (P<.001, SMD=0.052).
In biochemistry tests, we observed lower fasting glucose, creatinine and creatine kinase levels among G6PD deficient patients. Conspicuous differences were observed for iron, ferritin and transferrin saturation, which are elevated with respective SMDs of 0.369, 0.282 and 0.401 (P<.001 for all), while transferrin is markedly decreased (SMD=-0.149). Interestingly both blood total protein and globulin were markedly elevated in G6PD deficiency, with respective SMDs of 0.148 and 0.129 (P<.001 for both). Among immunoglobulins (Ig), we observe markedly elevated levels for IgA and IgG with respective SMDs of 0.256 and 0.252 (P<.001 for both). In contrast, IgM levels were not significantly different in the two groups.
We also evaluated inflammation-associated markers. Erythrocyte sedimentation rate (ESR) is slightly higher in G6PD patients (P<.001, SMD=0.093), but not C-reactive protein. Levels of C4 complement were significantly decreased in G6PD deficient patients (P<.001, SMD=-0.170), but C3 complement were only slightly decreased (P=.038, SMD=-0.086).
Discussion
To our knowledge, this is the first large-scale epidemiologic analysis to assess the association between G6PD deficiency and the long-term risk of immune system associated diseases. We show G6PD deficient patients have globally higher rates of acute infectious diseases, and in particular staphylococcal infections, suggesting a predisposition to infections. The link between G6PD deficiency and infections has been previously recognized in infancy, with lack of G6PD activity identified as a risk factor for neonatal sepsis in males (10). This study is the first to show this association on a large scale and for a wide range of infectious diseases.
Another finding from our study is a higher rate of allergic diseases in G6PD-deficient subjects. No systematic review of allergic comorbidity in G6PD deficiency was found in the literature. However, a retrospective case-control study showed that G6PD deficiency is an independent risk factor for asthma (24) and G6PD was noticeably downregulated in asthmatic children (25). In asthma, the level of reduced glutathione is significantly increased, and G6PD-deficient subjects’ insufficient production of NADPH may contribute to asthma pathogenesis (26). Moreover, the chronic depletion of nitric oxide in G6PD deficient subjects may affect the basal bronchodilator tone (27). In our cohort, we also found an association between asthma and G6PD deficiency (OR=1.08, P=.043), but much more stronger associations were present for other conditions such as allergic conjunctivitis (OR=1.25, P<.001), food allergy (OR=1.23, P<.001), and contact dermatitis (OR=1.19, P<.001).
The most striking finding of our study are the much-elevated rates of autoimmune diseases and chronic inflammatory conditions in G6PD deficient individuals. We notably observed markedly elevated rates of scleroderma (OR=6.87, P<.001), SLE (OR=4.56, P<.001), dermatomyositis (OR=3.56, P<.001), Sjögren’s syndrome (OR=2.80), rheumatoid arthritis (OR=2.41, P<.001) and ankylosing spondylitis (OR=2.52, P=.001) in individuals affected with G6PD deficiency. These findings were corroborated with elevated rates of positive autoimmune serology in G6PD deficiency and higher rates of treatment with medications commonly used to treat autoimmune conditions. This is consistent with a previous study reporting lower levels of G6PD enzymatic activity in patients with rheumatoid arthritis and Sjögren’s syndrome, which in many cases was subclinical and of acquired origin (28).
We also observed significantly higher rates of organ-specific inflammatory diseases such as Hashimoto’s thyroiditis (OR=1.26, P=.001) and Graves’ disease (OR=1.46, P=.001), and particularly elevated rates of pernicious anemia (OR=18.7, P<.001). We corroborated these findings with higher rates of individuals with positive anti-gastric parietal cells and anti-TPO antibodies in the G6PD group. Findings of increased rate of autoimmune thyroid disorders in G6PD patients are consistent with a recently published case-control study from North Sardinia, which identified an odds ratio of 1.36 (95% CI 1.11 to 1.60) for these disorders for G6PD patients (8).
We also observed higher rates of inflammatory bowel disease (OR=1.34, P=.05) and psoriasis (OR=1.19, P=.02) among G6PD deficient patients. Interestingly, we observed markedly higher rates for diseases for which the pathological basis is poorly understood, notably hidradenitis suppurativa (OR=2.57, P<.001) and fibromyalgia (OR=1.98, P<.001). These strong associations with G6PD deficiency suggest that metabolic pathway alterations, as those present in G6PD deficiency, may play a major role in these pathologies.
G6PD deficient individuals differed markedly from the rest of the population for commonly prescribed laboratory tests. They display diminished white blood cells counts, particularly monocytes and neutrophils. Interestingly, activated monocytes and neutrophils produce reactive oxygen species (ROS), which could be particularly harmful to G6PD-deficient cells and could lead to increased cell death. We also observed markedly increased levels of iron, ferritin, and transferrin saturation, with diminished transferrin levels. Immunoglobulins A and G levels were increased in G6PD patients and C4 complement decreased, suggesting a possible activation of the complement system in G6PD deficiency, presumably through the classical pathway and with the production of circulating immune complexes (29). Indeed, immune dysregulation may play a role in the pathogenesis of autoimmune and infectious diseases in G6PD deficiency, presumably through dysregulated NADPH homeostasis and ROS imbalances (30).
G6PD deficiency has been associated with a proinflammatory state with over-expression of IL-8, IL-4, IL-5, and IL-9 cytokines, and increased chemotaxis of eosinophils and Th2 immune polarization (31, 32). Oxidative stress had been suggested in the pathogenesis of human SLE and Sjögren syndrome (33, 34). Oxidative stress in G6PD deficient subjects contributes to developing novel epitopes by oxidizing proteins and lipids and producing anti-DNA antibodies (35, 36). Oxidative stress may also play a role in the sustained activation of lymphocytes and cause autoimmune responses by modulation of T and B cell homeostasis, leading to a loss in immunological tolerance (37, 38). These may be some of the reasons for the observed higher rates of autoimmune diseases. Their roles in food allergy, atopic and allergic contact dermatitis should be elucidated in further research. Autoimmune diseases in G6PD deficient patients may be triggered by activation of TGF-β/NADPH oxidases/ROS signaling, the expression of ICAM-1 and VCAM-1, and the adhesion of leukocytes to the endothelial cells with endothelial to mesenchymal transition (31, 39).
Several mechanisms could explain higher susceptibility to infections in individuals with G6PD deficiency. NADPH is critical for the regeneration of glutathione, reactive oxygen species (ROS) and plays an essential role in the production of reactive nitrogen species and nitric oxide (40). Immune inflammation in airway epithelial cells induces G6PD activity with the concomitant increase of glutathione, ROS, nitrotyrosine, and NADPH oxidase 2 (NOX2) (41). Experimental models have shown that G6PD inhibition suppresses airway inflammation induced by lipopolysaccharides and the ROS derived from NOX2 (42). Dysregulated redox systems and NF-κB signaling in G6PD-deficient cells have been associated with increased susceptibility to coronavirus and enterovirus infection (43, 44). G6PD-deficient individuals also produce lower levels of pro-inflammatory cytokines, IL-6, and IL-1β in peripheral mononuclear cells (45), and their granulocytes display diminished bactericidal activity and increased susceptibility to infection (46). Reduced expression of prostaglandin E2 and cyclooxygenase-2 (47), defective neutrophil extracellular trap (NET) formation (48), and impaired inflammasome activation have also been observed in the neutrophils of G6PD-deficient individuals (49).
In our study, we did not find a significant association between G6PD deficiency and malignancy. Earlier studies have observed decreased cancer risk in G6PD deficient patients, in particular for cancers of endodermal origin (colorectal, gastric and liver), but these findings were not replicated in other studies, notably for hematologic malignancies. In this large cohort of G6PD deficient individuals, carefully matched by multiple factors, we did not find evidence for an association between G6PD deficiency and the overall rate of both solid and hematologic cancers during a mean follow-up of 14.3 years, but the lack of statistical association could be due to the relatively low rate of malignancy (~4%) diagnosed in this relatively young cohort. It is remarkable that even though G6PD deficiency is associated with several chronic inflammatory diseases, this does not translate into cancer risk. This may be explained by the fact that G6PD deficiency is associated with multiple changes in metabolic and cellular states (6) with some changes being pro-tumorigenic and other changes being anti-tumorigenic.
Limitations
This study has the usual limitations of observational studies: potential confounders could be distributed differently between the two groups, clinical records may be inaccurate, and data may be missing. Nonetheless, the large number of participants and the scrupulous matching methodology adopted should minimize the extent of such biases. Another limitation is that the study reflects the link with the G6PD mutations prevalent in the Israeli population, in which the most prevalent mutation is the “Mediterranean” allele, which is associated with severe G6PD enzymatic deficiency (50). Unfortunately, a molecular diagnosis was not available in this large-scale study, and risks may differ with variants present in other populations. Since we lack G6PD enzymatic measures for the whole cohort, we considered G6PD deficiency as a dichotomous trait rather than a continuous spectrum.
Another limitation is that the studied cohort was relatively young, the mean patient age was 29.2, and only 12.5% of the study subjects were above age 60. Cancer and cardiovascular disease, as well as type II diabetes and its complications occur mostly in the elderly, and this study may be insufficiently powered to detect associations for such diseases, which are diagnosed predominantly in patients older than 60.
Conclusions
In conclusion, G6PD deficiency is a condition which appears to be associated with increased susceptibility to autoimmune, infectious and allergic diseases. Additional studies are warranted to confirm these observations and investigate the mechanisms underlying the higher prevalence of these conditions in G6PD deficiency. Some of the novel associations we report with G6PD deficiency are for poorly understood conditions such as fibromyalgia or hidradenitis suppurativa, and this may suggest new directions for investigating the pathological basis of these diseases.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Access to raw patient data is restricted to researchers approved by the institutional ethics committee. Requests to access these datasets should be directed to YWlzcmFlbEBsZXVtaXQuY28uaWw=.
Ethics statement
This study was approved by the ethics committee of Leumit Health Services (LEU 02-23) with a waiver of informed consent. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
AI and EMa: designed research, performed research, collected, analyzed and interpreted the data, performed statistical analysis, and wrote the initial draft of the manuscript; AAS, DO, EMe, IG, AG-C, MB, ER, and SV: analyzed and interpreted data and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was supported in part by the Intramural Research Program, National Institutes of Health, National Cancer Institute, Center for Cancer Research. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, and decision to submit the manuscript for publication. The National Cancer Institute did approve the manuscript via a formal publication clearance process applied to all manuscripts.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Abbreviations
BMI, Body Mass Index; BP, blood pressure; CI, confidence interval; COPD, chronic obstructive pulmonary disease; EHR, electronic health records; ESR, Erythrocyte sedimentation rate; G6PD, Glucose-6-phosphate dehydrogenase; ICD-9, International Classification of Diseases 9th Revision; Ig, Immunoglobulins; IQR, Interquartile range; LHS, Leumit Health Services; NET, neutrophil extracellular trap; NOX2, NADPH oxidase 2; OR, Odds Ratio; ROS, reactive oxygen species; SES, socio-economic status; SLE, systemic lupus erythematosus; SMD, standardized mean difference.
References
1. Cappellini M, Fiorelli G. Glucose-6-phosphate dehydrogenase deficiency. Lancet (London England) (2008) 371:64–74. doi: 10.1016/S0140-6736(08)60073-2
2. Luzzatto L, Nannelli C, Notaro R. Glucose-6-phosphate dehydrogenase deficiency. Hematol Oncol Clin North Am (2016) 30:373–93. doi: 10.1016/j.hoc.2015.11.006
3. Nkhoma ET, Poole C, Vannappagari V, Hall SA, Beutler E. The global prevalence of glucose-6-phosphate dehydrogenase deficiency: A systematic review and meta-analysis. Blood Cells Mol Dis (2009) 42:267–78. doi: 10.1016/j.bcmd.2008.12.005
4. Ruwende C, Khoo SC, Snow RW, Yates SN, Kwiatkowski D, Gupta S, et al. Natural selection of hemi- and heterozygotes for G6PD deficiency in Africa by resistance to severe malaria. Nature (1995) 376:246–9. doi: 10.1038/376246a0
5. Tishkoff SA, Varkonyi R, Cahinhinan N, Abbes S, Argyropoulos G, Destro-Bisol G, et al. Haplotype diversity and linkage disequilibrium at human G6PD: recent origin of alleles that confer malarial resistance. Science (2001) 293:455–62. doi: 10.1126/science.1061573
6. Beutler E. G6PD deficiency. Blood (1994) 84:3613–36. doi: 10.1182/blood.V84.11.3613.bloodjournal84113613
7. Saha N, Ahmed MA, Wasfi AI, El Munshid HA. Distribution of serum proteins, red cell enzymes and haemoglobins in vitiligo. Hum Hered (1982) 32:46–8. doi: 10.1159/000153257
8. Dore MP, Fanciulli G, Pes GM. Is glucose-6-phosphate dehydrogenase deficiency a risk factor for autoimmune thyroid disease? A retrospective case–Control study. Int J Environ Res Public Heal (2023) 20:2709. doi: 10.3390/IJERPH20032709
9. Mondal A, Mukherjee S, Dar W, Upadhyay P, Ranganathan A, Pati S, et al. G6PD deficiency: imbalance of functional dichotomy contributing to the severity of COVID-19. Future Microbiol (2022) 17:1161–70. doi: 10.2217/fmb-2021-0299
10. Rostami-Far Z, Ghadiri K, Rostami-Far M, Shaveisi-Zadeh F, Amiri A, Rahimian Zarif B. Glucose-6-phosphate dehydrogenase deficiency (G6PD) as a risk factor of male neonatal sepsis. J Med Life (2016) 9:34–8.
11. Abu-Osba YK, Mallouh AA, Hann RW. Incidence and causes of sepsis in glucose-6-phosphate dehydrogenase-deficient newborn infants. J Pediatr (1989) 114:748–52. doi: 10.1016/s0022-3476(89)80131-3
12. Saha N. Association of glucose-6-phosphate dehydrogenase deficiency with diabetes mellitus in ethnic groups of Singapore. J Med Genet (1979) 16:431–4. doi: 10.1136/jmg.16.6.431
13. Lai YK, Lai NM, Lee SWH. Glucose-6-phosphate dehydrogenase deficiency and risk of diabetes: a systematic review and meta-analysis. Ann Hematol (2017) 96:839–45. doi: 10.1007/s00277-017-2945-6
14. Cocco P, Todde P, Fornera S, Manca MB, Manca P, Sias AR. Mortality in a cohort of men expressing the glucose-6-phosphate dehydrogenase deficiency. Blood (1998) 91:706–9. doi: 10.1182/blood.V91.2.706
15. Meloni L, Manca MR, Loddo I, Cioglia G, Cocco P, Schwartz A, et al. Glucose-6-phosphate dehydrogenase deficiency protects against coronary heart disease. J Inherit Metab Dis (2008) 31:412–7. doi: 10.1007/s10545-008-0704-5
16. Pes GM, Parodi G, Dore MP. Glucose-6-phosphate dehydrogenase deficiency and risk of cardiovascular disease: A propensity score-matched study. Atherosclerosis (2019) 282:148–53. doi: 10.1016/j.atherosclerosis.2019.01.027
17. Dore MP, Parodi G, Portoghese M, Pes GM. The controversial role of glucose-6-phosphate dehydrogenase deficiency on cardiovascular disease: A narrative review. Oxid Med Cell Longev (2021) 2021:5529256. doi: 10.1155/2021/5529256
18. Dore MP, Davoli A, Longo N, Marras G, Pes GM. Glucose-6-phosphate dehydrogenase deficiency and risk of colorectal cancer in Northern Sardinia: A retrospective observational study. Med (Baltimore) (2016) 95:e5254. doi: 10.1097/MD.0000000000005254
19. Pes GM, Errigo A, Soro S, Longo NP, Dore MP. Glucose-6-phosphate dehydrogenase deficiency reduces susceptibility to cancer of endodermal origin. Acta Oncol (Madr) (2019) 58:1205–11. doi: 10.1080/0284186X.2019.1616815
20. Cocco P. Does G6PD deficiency protect against cancer? A critical review. J Epidemiol Community Health (1987) 41:89–93. doi: 10.1136/jech.41.2.89
21. Ferraris AM, Broccia G, Meloni T, Forteleoni G, Gaetani GF. Glucose 6-phosphate dehydrogenase deficiency and incidence of hematologic Malignancy. Am J Hum Genet (1988) 42:516–20.
22. Israel A, Berkovitch M, Merzon E, Golan-Cohen A, Green I, Ruppin E, et al. Glucose-6-phosphate dehydrogenase deficiency and coronavirus disease 2019. Clin Infect Dis (2023). doi: 10.1093/cid/ciad348
23. Israel A, Merzon E, Schäffer AA, Shenhar Y, Green I, Golan-Cohen A, et al. Elapsed time since BNT162b2 vaccine and risk of SARS-CoV-2 infection: test negative design study. BMJ (2021) 375:e067873. doi: 10.1136/bmj-2021-067873
24. Fois A, Dore MP, Manca A, Scano V, Pirina P, Pes GM. Association between glucose-6-phosphate dehydrogenase deficiency and asthma. J Clin Med (2021) 10:5639. doi: 10.3390/jcm10235639
25. Li M, Wu M, Qin Y, Liu H, Tu C, Shen B, et al. Differentially expressed serum proteins in children with or without asthma as determined using isobaric tags for relative and absolute quantitation proteomics. PeerJ (2020) 8:e9971. doi: 10.7717/peerj.9971
26. Husain Q, Ahmad A, Shameem M. Relation of oxidant-antioxidant imbalance with disease progression in patients with asthma. Ann Thorac Med (2012) 7:226. doi: 10.4103/1817-1737.102182
27. Prado CM, Martins MA, Tibério IFLC. Nitric oxide in asthma physiopathology. ISRN Allergy (2011) 2011:1–13. doi: 10.5402/2011/832560
28. Gheita TA, Kenawy SAB, El Sisi RW, Gheita HA, Khalil H. Subclinical reduced G6PD activity in rheumatoid arthritis and Sjögren’s Syndrome patients: relation to clinical characteristics, disease activity and metabolic syndrome. Mod Rheumatol (2014) 24:612–7. doi: 10.3109/14397595.2013.851639
29. Wang H, Liu M. Complement C4, infections, and autoimmune diseases. Front Immunol (2021) 12:694928. doi: 10.3389/fimmu.2021.694928
30. Brewer AC, Mustafi SB, Murray TVA, Rajasekaran NS, Benjamin IJ. Reductive stress linked to small HSPs, G6PD, and nrf2 pathways in heart disease. Antioxid Redox Signal (2013) 18:1114–27. doi: 10.1089/ars.2012.4914
31. Parsanathan R, Jain SK. G6PD deficiency shifts polarization of monocytes/macrophages towards a proinflammatory and profibrotic phenotype. Cell Mol Immunol (2021) 18:770–2. doi: 10.1038/s41423-020-0428-5
32. Yang H-C, Cheng M-L, Hua Y-S, Wu Y-H, Lin H-R, Liu H-Y, et al. Glucose 6-phosphate dehydrogenase knockdown enhances IL-8 expression in HepG2 cells via oxidative stress and NF-κB signaling pathway. J Inflamm (2015) 12:34. doi: 10.1186/s12950-015-0078-z
33. Kurien BT, Porter A, Dorri Y, Iqbal S, D’Souza A, Singh A, et al. Degree of modification of Ro60 by the lipid peroxidation by-product 4-hydroxy-2-nonenal may differentially induce Sjögren syndrome or systemic lupus erythematosus in BALB/c mice. Free Radic Biol Med (2011) 50:1222–33. doi: 10.1016/j.freeradbiomed.2010.10.687
34. Neumann CA, Krause DS, Carman CV, Das S, Dubey DP, Abraham JL, et al. Essential role for the peroxiredoxin Prdx1 in erythrocyte antioxidant defence and tumour suppression. Nature (2003) 424:561–5. doi: 10.1038/nature01819
35. Lee T-H. Peroxiredoxin II is essential for sustaining life span of erythrocytes in mice. Blood (2003) 101:5033–8. doi: 10.1182/blood-2002-08-2548
36. Zhang J, Zahir N, Jiang Q, Miliotis H, Heyraud S, Meng X, et al. The autoimmune disease–associated PTPN22 variant promotes calpain-mediated Lyp/Pep degradation associated with lymphocyte and dendritic cell hyperresponsiveness. Nat Genet (2011) 43:902–7. doi: 10.1038/ng.904
37. Yeh L-T, Miaw S-C, Lin M-H, Chou F-C, Shieh S-J, Chuang Y-P, et al. Different modulation of ptpn22 in effector and regulatory T cells leads to attenuation of autoimmune diabetes in transgenic nonobese diabetic mice. J Immunol (2013) 191:594–607. doi: 10.4049/jimmunol.1203380
38. Piera-Velazquez S, Jimenez SA. Endothelial to mesenchymal transition: role in physiology and in the pathogenesis of human diseases. Physiol Rev (2019) 99:1281–324. doi: 10.1152/physrev.00021.2018
39. Hal Scofield R, Kurien BT, Ganick S, McClain MT, Pye Q, James JA, et al. Modification of lupus-associated 60-kDa Ro protein with the lipid oxidation product 4-hydroxy-2-nonenal increases antigenicity and facilitates epitope spreading. Free Radic Biol Med (2005) 38:719–28. doi: 10.1016/j.freeradbiomed.2004.11.001
40. Yang H-C, Cheng M-L, Ho H-Y, Tsun-Yee Chiu D. The microbicidal and cytoregulatory roles of NADPH oxidases. Microbes Infect (2011) 13:109–20. doi: 10.1016/j.micinf.2010.10.008
41. Nadeem A, Al-Harbi NO, Ahmad SF, Ibrahim KE, Siddiqui N, Al-Harbi MM. Glucose-6-phosphate dehydrogenase inhibition attenuates acute lung injury through reduction in NADPH oxidase-derived reactive oxygen species. Clin Exp Immunol (2018) 191:279–87. doi: 10.1111/cei.13097
42. Hsieh Y-T, Lin M-H, Ho H-Y, Chen L-C, Chen C-C, Shu J-C. Glucose-6-phosphate dehydrogenase (G6PD)-deficient epithelial cells are less tolerant to infection by staphylococcus aureus. PloS One (2013) 8:e79566. doi: 10.1371/journal.pone.0079566
43. Wu Y-H, Chiu D, Lin H-R, Tang H-Y, Cheng M-L, Ho H-Y. Glucose-6-phosphate dehydrogenase enhances antiviral response through downregulation of NADPH sensor HSCARG and upregulation of NF-κB signaling. Viruses (2015) 7:6689–706. doi: 10.3390/v7122966
44. Ho H-Y, Cheng M-L, Weng S-F, Chang L, Yeh T-T, Shih S-R, et al. Glucose-6-phosphate dehydrogenase deficiency enhances enterovirus 71 infection. J Gen Virol (2008) 89:2080–9. doi: 10.1099/vir.0.2008/001404-0
45. Sanna F, Bonatesta RR, Frongia B, Uda S, Banni S, Melis MP, et al. Production of inflammatory molecules in peripheral blood mononuclear cells from severely glucose-6-phosphate dehydrogenase-deficient subjects. J Vasc Res (2007) 44:253–63. doi: 10.1159/000100903
46. van Bruggen R. Deletion of leucine 61 in glucose-6-phosphate dehydrogenase leads to chronic nonspherocytic anemia, granulocyte dysfunction, and increased susceptibility to infections. Blood (2002) 100:1026–30. doi: 10.1182/blood.V100.3.1026
47. Lin H-R, Wu Y-H, Yen W-C, Yang C-M, Chiu DT-Y. Diminished COX-2/PGE2-mediated antiviral response due to impaired NOX/MAPK signaling in G6PD-knockdown lung epithelial cells. PloS One (2016) 11:e0153462. doi: 10.1371/journal.pone.0153462
48. Cheng ML, Ho HY, Lin HY, Lai YC, Chiu DTY. Effective NET formation in neutrophils from individuals with G6PD Taiwan-Hakka is associated with enhanced NADP + biosynthesis. Free Radic Res (2013) 47:699–709. doi: 10.3109/10715762.2013.816420
49. Yen W-C, Wu Y-H, Wu C-C, Lin H-R, Stern A, Chen S-H, et al. Impaired inflammasome activation and bacterial clearance in G6PD deficiency due to defective NOX/p38 MAPK/AP-1 redox signaling. Redox Biol (2020) 28:101363. doi: 10.1016/j.redox.2019.101363
Keywords: G6PD deficiency, autoimmunity, allergy, infectious diseases, fibromyalgia, hidradenitis suppurativa, rheumatoid arthritis, lupus (SLE)
Citation: Israel A, Schäffer AA, Berkovitch M, Ozeri DJ, Merzon E, Green I, Golan-Cohen A, Ruppin E, Vinker S and Magen E (2023) Glucose-6-phosphate dehydrogenase deficiency and long-term risk of immune-related disorders. Front. Immunol. 14:1232560. doi: 10.3389/fimmu.2023.1232560
Received: 31 May 2023; Accepted: 29 August 2023;
Published: 11 September 2023.
Edited by:
Md Asiful Islam, University of Birmingham, United KingdomReviewed by:
Erkan Yilmaz, Istanbul University-Cerrahpasa, TürkiyeGiovanni Mario Pes, University of Sassari, Italy
Copyright © 2023 Israel, Schäffer, Berkovitch, Ozeri, Merzon, Green, Golan-Cohen, Ruppin, Vinker and Magen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ariel Israel, YWlzcmFlbEBsZXVtaXQuY28uaWw=