 Yi Liu
Yi Liu Yin Zhou3
Yin Zhou3
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 24 August 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1211953
Introduction: Rosacea, a widespread chronic skin condition, may be influenced by macrophages, key immune cells in the skin, although their exact role is not yet fully understood. This review delves into the function of macrophages, their potential contribution to rosacea pathogenesis, current treatments, and promising macrophage-targeted therapies. It concludes by identifying knowledge gaps and potential areas for future rosacea research.
Method: Leveraging systematic and narrative literature review techniques, we conducted a comprehensive search of databases such as PubMed, Embase, and Web of Science. Utilizing keywords like “rosacea” and “macrophages”, we targeted English articles from the last 5 years (2018-2023). We manually checked reference lists of relevant articles for additional studies. We included only articles emphasizing macrophages’ role in rosacea and/or the development of related therapies and published within the specified timeframe.
Results: The systematic search of electronic databases yielded a total of 4,263 articles. After applying the inclusion and exclusion criteria, 156 articles were selected for inclusion in this review. These articles included original research studies, review articles, and clinical trials that focused on the role of macrophages in rosacea and/or the development of macrophage-targeted therapies for the disease. The selected articles provided a comprehensive and up-to-date overview of the current state of research on macrophages in rosacea, including their function in the skin, the potential mechanisms through which they may contribute to rosacea pathogenesis, and the current treatments and therapies available for the disease. Additionally, the articles identified gaps in knowledge regarding the role of macrophages in rosacea and suggested potential areas for future research.
Conclusion: This literature review emphasizes the important role that macrophages, vital immune cells in the skin, may play in the pathogenesis of rosacea, a common chronic inflammatory skin disorder. The selected studies suggest potential mechanisms by which these cells might contribute to rosacea progression, although these mechanisms are not yet fully understood. The studies also spotlight current rosacea treatments and illuminate the promising potential of new macrophage-focused therapies. Despite these insights, significant gaps persist in our understanding of the precise role of macrophages in rosacea. Future research in this area could provide further insights into the pathogenesis of rosacea and contribute to the development of more effective, targeted therapeutic strategies.
Rosacea is a common chronic skin condition with redness, flushing, inflammation, and sometimes visible blood vessels or red, pus-filled bumps. Recent studies reveal variations within the disease spectrum (1–4). These phenotypes include erythematotelangiectatic rosacea (ETR) (3), characterized by persistent facial redness and visible blood vessels; papulopustular rosacea (PPR) (5), characterized by papules, pustules, and occasional nodules; and phymatous rosacea characterized by skin thickening and enlargement, predominantly affecting the nose (rhinophyma) (6). Identifying rosacea phenotypes is crucial for precise diagnosis and personalized management (7). Rosacea, usually appearing in adults over 30, has an unclear pathophysiology (8). Rosacea is influenced by genetics, environment, vascular factors, inflammation, and microbes (9). Rosacea’s prevalence in northern European populations and among those with a family history suggests a genetic predisposition (10). Rosacea can worsen due to environmental triggers like sunlight, heat, spicy foods, alcohol, stress, and certain cosmetics (11). Vascular issues in rosacea lead to facial blood vessel dysfunction, causing persistent redness, flushing, and visible vessels (12). Elevated Demodex folliculorum levels in rosacea sufferers suggest its involvement in the disease’s development (13). Rosacea’s pathophysiology involves skin barrier dysfunction and overproduction of proteins such as cathelicidin and kallikrein (14). These proteins cause inflammation, redness, and swelling and can trigger reactions to harmless bacteria (15). Rosacea treatment includes lifestyle changes, topical medication, oral antibiotics, and laser therapy (16). Topical treatments include metronidazole, azelaic acid, ivermectin, and brimonidine. Oral antibiotics like doxycycline are commonly used for their anti-inflammatory effects (17). Macrophages are essential immune cells that protect against pathogens in the skin and throughout the body (18). They ingest and digest pathogens through phagocytosis (19). Macrophages control inflammation, aid in healing and tissue repair, and remove damaged cells. Their role in rosacea is being studied, but their contribution to the disease is likely (20–22). Macrophages release mediators that cause redness, swelling, and pus-filled bumps in rosacea (23). Macrophages promote blood vessel growth, leading to persistent redness and visible vessels in rosacea (24). Macrophages respond to microbial stimuli, including the presence of D. folliculorum mites in rosacea patients, exacerbating inflammation (4). Abnormal immune response to environmental triggers may activate macrophages and contribute to rosacea (25). Research on macrophages in rosacea aims to uncover their role and develop new treatments. Understanding their function could reduce inflammation, improve patients’ quality of life, and shed light on related conditions. Further research is required to validate these findings and apply them in clinical practice.
The main databases used for the search included PubMed, Embase, and Web of Science. Our search strategy employed specific keywords related to “rosacea” and “macrophages”, with a particular emphasis on English language articles published within the timeframe of 2018 and 2023. Our research methodology extended to manual searches of reference lists from related articles to identify additional studies that could contribute valuable insights to our investigation. To ensure the integrity and relevance of our review, we followed strict inclusion and exclusion criteria, which were determined based on the focus of the article, its relevance to our study, the timeframe of publication, and the language in which the article was written. Our literature review process was the involvement of a multidisciplinary team composed of clinical physicians, dermatology researchers, and immunologists. This diverse team conducted the screening and evaluation process, ensuring a comprehensive and unbiased assessment of the articles based on our predefined criteria. The detailed process of our screening and evaluation, including the specific criteria used, is outlined in the Method section of our study. Flowchart could be referred (Figure 1). We believe that this rigorous and comprehensive methodology allowed us to capture a broad and current understanding of the relationship between macrophages and rosacea, contributing valuable insights to the existing body of knowledge.

Figure 1 Flowchart according to guideline of PRISMA 2020. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
A systematic search yielded 4,263 articles, with 156 qualifying for inclusion post-criteria application. These articles, encompassing original studies, reviews, and clinical trials, highlighted macrophages’ role in rosacea and potential macrophage-targeted therapies. They provided an updated understanding of macrophages in rosacea, including their functions, contributions to pathogenesis, and current treatments. The articles also identified knowledge gaps and suggested future research areas.
Macrophages are immune cells that play a crucial role in maintaining tissue homeostasis and regulating the immune response in the skin (26). Macrophages have several crucial functions, including phagocytosis, debris clearance, antigen presentation, and cytokine secretion to recruit other immune cells to inflammation sites (27). In the skin, macrophages inhabit the dermis and epidermis, interacting with other cells like fibroblasts, keratinocytes, and dendritic cells to sustain skin health (28). In addition to aiding wound healing and tissue repair, macrophages resolve skin inflammation. In rosacea, they are thought to contribute to chronic inflammation and vascular dysfunction (29). Recent advancements underscore the pivotal role of macrophages in rosacea’s pathophysiology (30). Macrophages, acting as scavengers, clear body debris and microbes and are essential for wound healing, tissue repair, and resolving skin inflammation (31). In rosacea, macrophages seemingly contribute to the condition’s hallmark chronic inflammation and vascular dysfunction (32). In rosacea patients, researchers have discovered an overproduction of pro-inflammatory cytokines and angiogenic factors by macrophages (33), which promote inflammation and blood vessel formation. Also, these macrophages exhibit a hindered ability to transition from an inflammatory to a reparative state, extending the inflammatory response and intensifying tissue damage (34). This updated understanding of macrophages’ role in rosacea has unveiled potential therapies, like targeting macrophage function or specific cytokines (35), to alleviate the chronic inflammation and vascular dysfunction associated with the disease. Macrophages have multifaceted roles in rosacea, participating in maintaining skin health and wound healing and contributing to rosacea’s chronic inflammation and vascular dysfunction. A comprehensive overview of these functions and potential therapeutic implications is provided in Table 1.

Table 1 Role and therapeutic implications of macrophages in rosacea.
Studies have shown elevated macrophage levels in the skin of individuals with rosacea, indicating their involvement in the condition (36). Carvedilol effectively treated rosacea by reducing inflammation, improving facial manifestations, and decreasing redness in patients after 4 and 6 months of treatment. It achieved this by inhibiting macrophage TLR2 expression, which may contribute to the vascular dysfunction associated with the disease (37). Studies have shown that macrophages in rosacea-affected skin express elevated levels of pro-inflammatory cytokines like IL-1β and TNF-α, surpassing those found in healthy skin (33). This heightened inflammatory response is thought to contribute to the persistent redness and inflammation seen in rosacea (38). The study examined facial biopsies from rosacea patients, revealing immune system activation and pro-inflammatory cell infiltration across all phenotypes. This prevalent chronic skin disorder presents with diverse signs on the central face, and a standardized system aims to aid diagnosis, research, and health-care communication, underscoring the significance of early identification and treatment to manage symptom progression (2). The updated classification system by the National Rosacea Society improves investigations, diagnosis, and treatment, particularly in specific demographics with a prevalence of 10% or higher, and more frequent diagnoses in women after the age of 30 (39). The efficacy and adverse event rates of various rosacea treatments are summarized in Supplementary Table 1 (40). Immunohistochemistry and flow cytometry techniques have shed light on the role of macrophages in rosacea by identifying and quantifying these cells in affected skin samples. This is crucial for understanding the immune response in the disease (41). Macrophages may contribute to rosacea pathogenesis through several potential mechanisms (42). One possibility is that they release pro-inflammatory cytokines that contribute to the persistent inflammation seen in the disease (43). These cytokines can trigger immune cell activation and attract more inflammatory cells to the skin, perpetuating an ongoing cycle of inflammation (44). Additionally, macrophages may play a role in the vascular dysfunction seen in rosacea (45). Macrophages are believed to play a role in both angiogenesis (formation of new blood vessels) and vasodilation (widening of existing vessels) in the skin (46), leading to the characteristic redness and flushing of rosacea (47). In rosacea, mast cell activation and the release of matrix metalloproteinases (MMPs) are additional potential mechanisms involved in the disease (48), which can break down the extracellular matrix and contribute to tissue damage (49). Gene expression analysis and functional assays unveil macrophages’ role in rosacea, with observed variations in gene expression profiles between healthy and affected skin samples (5, 50–53). Table 2 provides an example of such a comparison, highlighting differences in the expression of key genes involved in inflammation and macrophage function.
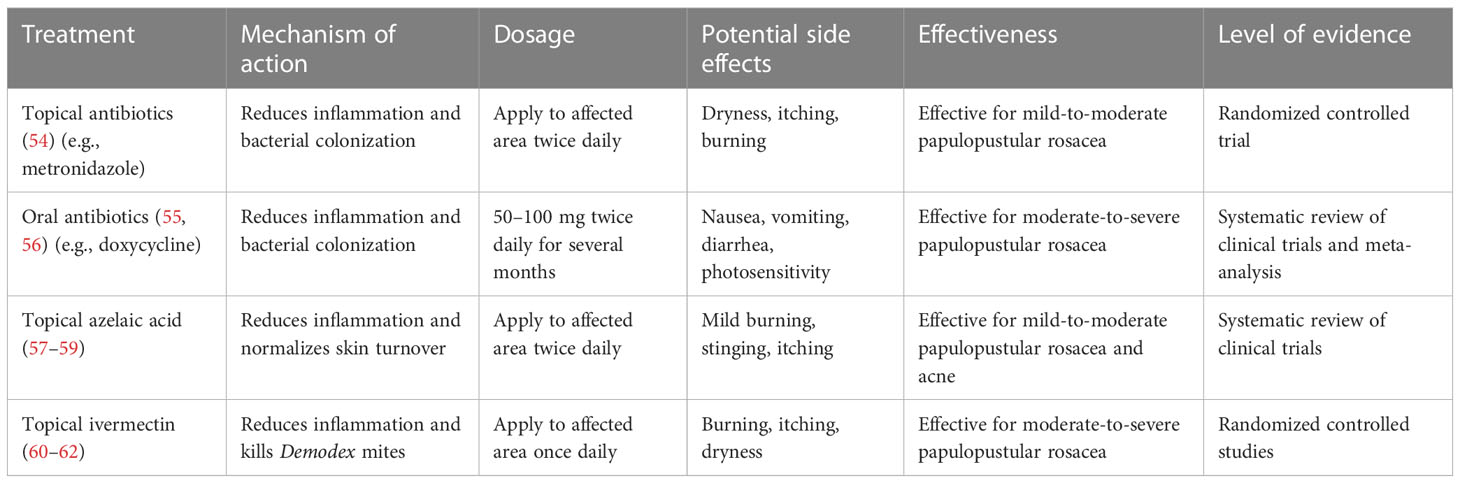
Table 2 Comparison of current treatments for rosacea.
Current treatments for rosacea typically focus on managing the symptoms of the disease rather than addressing its underlying cause (30). Metronidazole and doxycycline, in topical and oral forms, are commonly used to reduce skin inflammation and bacterial colonization (63). Topical azelaic acid and ivermectin have also been shown to be effective in reducing inflammation and improving the symptoms of rosacea (64). These treatments manage rosacea symptoms but do not address the underlying immune dysregulation and vascular dysfunction associated with the disease (30). Therefore, there is a need for novel, macrophage-targeted therapies that can address the root cause of rosacea (65). A potential macrophage-targeted therapy for rosacea involves using inhibitors that target pro-inflammatory cytokine production (66), such as IL-1β, by macrophages. Anakinra and canakinumab, IL-1β pathway inhibitors with a track record of reducing inflammation in other conditions, hold promise as potential treatments for rosacea (67). Another potential approach is targeting macrophage activation by environmental triggers like UV radiation (68). AhR-modulating drugs can reduce macrophage activation and inflammation in rosacea by targeting the skin’s response to environmental toxins (69). Tapinarof, an innovative topical treatment acting as an AhR agonist, holds promise in treating rosacea (70). This molecular mechanism focuses on the AhR, a ligand-activated transcription factor located in the cytoplasm (71). When tapinarof binds to AhR, it activates the receptor, leading to its translocation into the nucleus of skin cells (70, 72). This triggers the transcription of target genes that regulate inflammatory responses and strengthen the skin barrier function (73). Tapinarof has the potential to alleviate inflammatory responses and vascular dysregulation in rosacea (74, 75). Tapinarof’s potential effectiveness in improving skin barrier integrity may help alleviate rosacea symptoms (70, 76, 77). Referring to current sources is recommended for the latest information, as it may have evolved. In vitro assays and preclinical animal models can assess macrophage-targeted therapies’ efficacy and safety for rosacea (78), paving the way for the development of new treatments for this chronic skin disorder (79). Several clinical trials have investigated the efficacy of macrophage-targeted therapies for the treatment of rosacea (65). Table 3 summarizes trials with anakinra, canakinumab, and an AhR agonist, comparing current rosacea treatments. Topical and oral antibiotics reduce inflammation and bacterial colonization. Topical azelaic acid and ivermectin target skin turnover and Demodex mites, respectively. Topical steroids and oral non-steroidal anti-inflammatory drugs (NSAIDs) alleviate redness and inflammation but have potential side effects. Macrophage-targeted therapies show promise in addressing immune dysregulation and vascular dysfunction in rosacea. By targeting the pro-inflammatory cytokines and other molecules produced by macrophages (88), these therapies may be effective in reducing inflammation and improving the symptoms of rosacea (89). Targeted drug delivery systems or immunomodulatory nanoparticles can enhance the efficient and selective delivery of these therapies to the skin, minimizing potential side effects (90). However, there are also several limitations and challenges associated with macrophage-targeted therapies (91). Targeting macrophages specifically while avoiding impact on other skin cell types is challenging due to the complex interactions among immune cells in the skin’s immune response (92). Additionally, the potential for the development of drug resistance and the risk of side effects, such as immunosuppression, must be carefully considered (93). Table 4 outlines environmental triggers of macrophage activation in rosacea, including UV radiation, temperature changes, stress, alcohol, and spicy foods. These triggers induce inflammation, angiogenesis, nerve sensitivity, and macrophage activation, contributing to the disease’s progression. Furthermore, the cost and availability of these therapies may be a barrier to their widespread use (99). In vitro assays, animal models, and clinical trials are valuable for evaluating macrophage-targeted therapies in rosacea and addressing associated challenges (78). Recent progress in understanding the role of macrophages in rosacea has identified macrophage-targeted therapies as a promising treatment approach for the disease (78). However, developing effective macrophage-targeted therapies for rosacea is not without challenges (78). To address these challenges, various techniques have been used to assess the potential advantages and drawbacks of macrophage-targeted therapies for rosacea (78). In vitro assays evaluate treatment effects on macrophage function in a controlled environment, while preclinical animal models provide a whole organism setting for testing purposes (100). Clinical trials offer a valuable opportunity to assess the safety and efficacy of macrophage-targeted therapies in human patients (101).

Table 3 Comparison of the gene expression profiles of macrophages in healthy vs. rosacea skin.
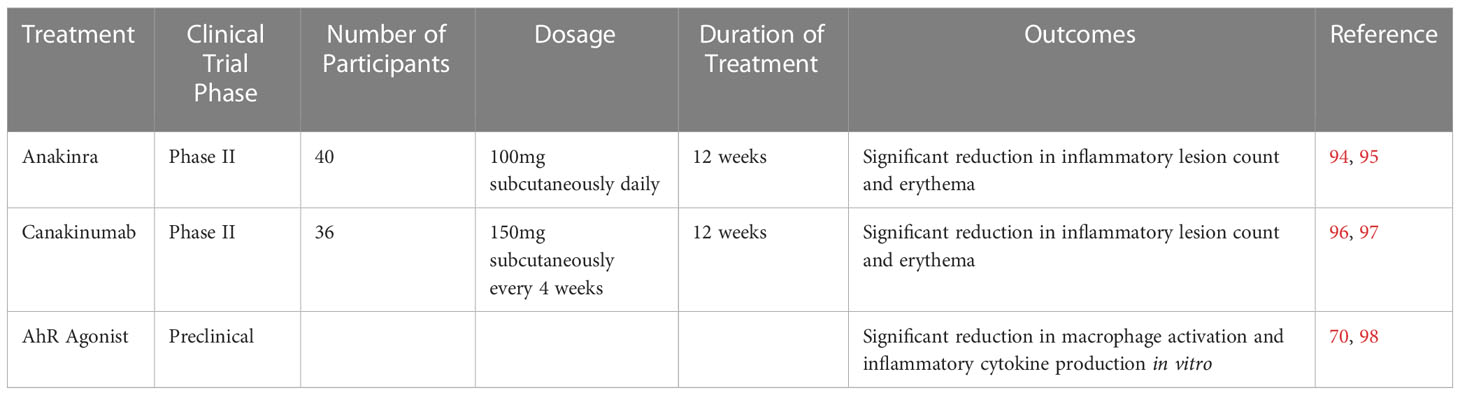
Table 4 Summarizing the results of clinical trials of macrophage-targeted therapies in rosacea.
An international group of dermatologists and ophthalmologists has unanimously endorsed a phenotype-based diagnostic and classification system for rosacea, a shift from the traditional approach of consensus-defined primary and secondary features. This new approach primarily identifies two phenotypes, persistent centrofacial erythema and phymatous changes, as independent diagnostic markers, whereas other features such as flushing, telangiectasia, and inflammatory lesions were not considered individually diagnostic. Moreover, the patient-focused transition from subtyping to phenotyping, backed by the ROSacea COnsensus (ROSCO) 2017 recommendations, aims to enhance personalized treatment strategies, taking into account the diverse range of rosacea manifestations and their impact on the patient’s quality of life. The panel also reevaluated treatment modalities based on recent advances in our understanding of rosacea’s pathophysiology, endorsing combination therapies, continued monitoring, and the use of a novel clinical tool, the Rosacea Tracker. These strategic changes aim to promote the utilization of the phenotypes approach in clinical practice and enhance rosacea patient management (47, 102, 103). These techniques reveal the mechanisms and benefits of macrophage-targeted therapies for rosacea. Anakinra and canakinumab showed reductions in inflammatory lesions and erythema in phase II trials, while preclinical studies on AhR agonists demonstrated decreased macrophage activation and cytokine production in vitro. Consult Table 5 for further details on these treatments and clinical trial results.
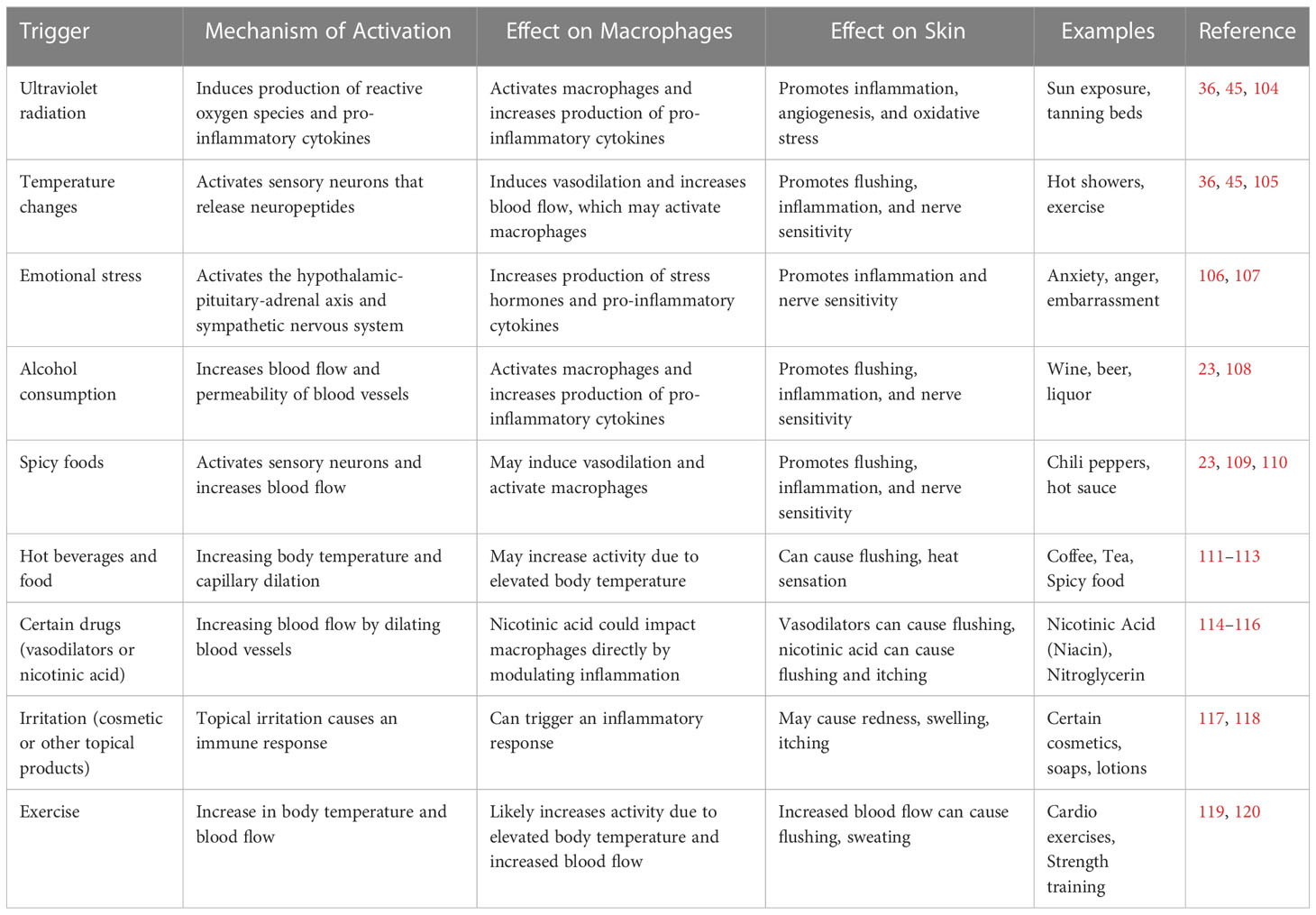
Table 5 Summarizing the known environmental triggers of macrophage activation in rosacea.
Recent progress has improved our understanding of macrophages’ role in rosacea, a chronic skin condition marked by persistent redness and visible blood vessels (111). Various investigative techniques have been utilized to understand the intricate role of macrophages in the disease (121). One significant method used in this pursuit is immunohistochemistry (122). Immunohistochemistry allows scientists to visualize and assess the distribution and activation state of macrophages in rosacea-affected skin tissue samples using fluorescent or enzyme tags (123). By employing antibodies that target macrophage surface markers like CD68 or CD163, researchers can quantify and identify macrophages at different stages of rosacea progression (33). Flow cytometry, which uses laser light to assess cellular characteristics, is invaluable in determining the phenotype and functional attributes of macrophages (124). Flow cytometry assesses surface markers and cytokine expression to identify macrophage subsets, revealing their roles in triggering inflammation in rosacea (124, 125). Advanced molecular profiling techniques like single-cell RNA sequencing have improved our understanding of the diverse macrophage population (126). Single-cell RNA sequencing is a powerful tool that uncovers gene expression patterns associated with macrophage phenotypes, providing insights into their roles and interactions in rosacea (29, 127). These techniques aid in understanding how macrophages affect rosacea’s development and progression. They pave the way for targeted therapeutic interventions, revolutionizing management by addressing immune responses for more effective treatments in the future.
Despite recent advances, significant knowledge gaps remain regarding the mechanisms by which macrophages contribute to rosacea (128). The environmental triggers that activate macrophages in rosacea, as well as the signaling pathways governing macrophage-mediated inflammation and angiogenesis, remain incompletely understood (129). The heterogeneity of skin macrophages and their interactions with other immune cells and structural cells like fibroblasts are still being investigated (130). Future research should address these knowledge gaps and develop new tools and techniques for studying skin macrophages (131). Advancements in single-cell sequencing, proteomics, and imaging technologies allow for detailed analysis of macrophage phenotypic and functional heterogeneity in the skin (132), as well as their interactions with other cell types. Identifying new macrophage-targeted therapies and improving rosacea treatments rely on these efforts. Recent progress in studying macrophages has paved the way for future research in rosacea (133). One key area of focus will be the development of new macrophage-targeted therapies that can address the underlying immune dysregulation and vascular dysfunction in the disease (134). This may involve identifying new molecular targets for therapy, as well as developing innovative drug delivery systems to improve the efficacy and safety of these therapies (135). Another important area of research will be the use of novel techniques to study macrophage function in the skin (136). Advances in imaging technologies, single-cell sequencing, and other high-throughput techniques may enable a more detailed analysis of macrophage heterogeneity and their interactions with other cells in the skin (137). Various techniques like flow cytometry, single-cell RNA sequencing, and in vitro assays, each with unique features and trade-offs, are employed to study macrophage function in rosacea. An overview of these techniques, including their advantages and limitations, is provided in Table 6. In addition, the use of preclinical animal models and clinical trials will be critical for evaluating the safety and efficacy of macrophage-targeted therapies and for identifying new molecular targets for therapy (150). Ultimately, the development of new macrophage-targeted therapies and a deeper understanding of macrophage function in rosacea may lead to improved treatments and outcomes for patients with this chronic skin disorder (65).
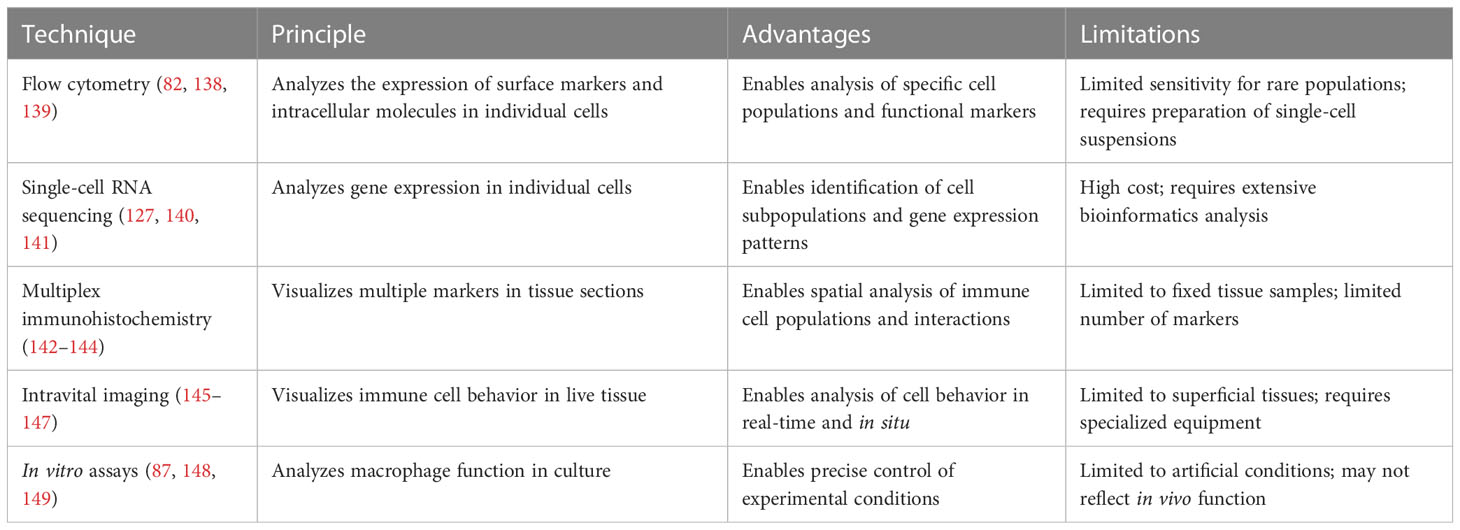
Table 6 An overview of techniques for studying macrophage function in rosacea.
In conclusion, recent research has highlighted the potential role of macrophages in the pathogenesis of rosacea. Macrophages are important immune cells that play a critical role in regulating inflammation in the skin, and recent studies have suggested that their dysregulation may contribute to the chronic inflammation and vascular dysfunction seen in rosacea. While current treatments for rosacea focus on managing symptoms, the development of macrophage-targeted therapies represents a promising new approach to treating the underlying cause of the disease. Future research efforts will need to focus on addressing the gaps in our knowledge of macrophage function in rosacea, as well as developing new techniques and therapies to improve patient outcomes. The potential clinical implications of this research are significant, as the development of new macrophage-targeted therapies may lead to more effective treatments for rosacea, a common and chronic skin disorder that can significantly impact patients’ quality of life.
YL: Writing, concept; CC, YZ: Revise; YL, XJ: Revise, manage the project. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1211953/full#supplementary-material
Supplementary Table 1 | Overview of Rosacea Treatments: Efficacy and Adverse Event Rates.
1. Rivero AL, Whitfeld M. An update on the treatment of rosacea. Aust Prescr. (2018) 41:20. doi: 10.18773/austprescr.2018.004
2. Gallo RL, Granstein RD, Kang S, Mannis M, Steinhoff M, Tan J, et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol (2018) 78:148–55. doi: 10.1016/j.jaad.2017.08.037
3. Searle T, Al-Niaimi F, Ali FR. Rosacea and the cardiovascular system. (2020) 19:2182–7. doi: 10.1111/jocd.13587
4. Forton FM. Rosacea, an infectious disease: why rosacea with papulopustules should be considered a demodicosis. A narrative review. J Eur Acad Dermatol Venereol (2022) 36:987–1002. doi: 10.1111/jdv.18049
5. Liu F, Chen M, Huang C, Xiao W, Gao S, Jian D, et al. Keratinocyte-immune cell crosstalk in a STAT1-mediated pathway: novel insights into rosacea pathogenesis. Front Immunol (2021) 12:674871. doi: 10.3389/fimmu.2021.674871
7. Maruthappu T, Taylor MJC, Dermatology E. Acne and rosacea in skin of colour. Clin Exp Dermatol (2022) 47:259–63. doi: 10.1111/ced.14994
8. Agarwal P. Acne, rosacea, and similar disorders. In: Concise Dermatology. CRC Press (2021). p. 134–49.
9. Holmes AD, Spoendlin J, Chien AL, Baldwin H, Chang ALS. Evidence-based update on rosacea comorbidities and their common physiologic pathways. J Am Acad Dermatol (2018) 78:156–66. doi: 10.1016/j.jaad.2017.07.055
10. Awosika O, Oussedik EJDC. Genetic predisposition to rosacea. Dermatol Clin (2018) 36(2):87–92. doi: 10.1016/j.det.2017.11.002
11. Morgado-Carrasco D, Granger C, Trullas C, Piquero-Casals J. Impact of ultraviolet radiation and exposome on rosacea: Key role of photoprotection in optimizing treatment. J Cosmet Dermatol (2021) 20(11):3415–21. doi: 10.1111/jocd.14020
12. Rastogi V, Singh D, Mazza JJ, Parajuli D, Yale SH. Flushing disorders associated with gastrointestinal symptoms: part 1, neuroendocrine tumors, mast cell disorders and hyperbasophila. Clin Med Res (2018) 16(1-2):16–28. doi: 10.3121/cmr.2017.1379a
13. Lugović-Mihić L, Špiljak B, Blagec T, Delaš Aždajić M, Franceschi N, Gašić A, et al. Factors participating in the occurrence of inflammation of the lips (Cheilitis) and perioral skin. Cosmetics (2023) 10:9. doi: 10.3390/cosmetics10010009
14. Deng Z, Chen M, Liu Y, Xu S, Ouyang Y, Shi W, et al. A positive feedback loop between mTORC1 and cathelicidin promotes skin inflammation in rosacea. EMBO Mol Med (2021) 13(5): e13560. doi: 10.15252/emmm.202013560
15. Efferth T, Oesch F. The immunosuppressive activity of artemisinin-type drugs towards inflammatory and autoimmune diseases. Med Res Rev (2021) 41(6):3023–61. doi: 10.1002/med.21842
16. Wladis EJ, Adam AP. Treatment of ocular rosacea. Surv Ophthalmol (2018) 63(3):340–6. doi: 10.1016/j.survophthal.2017.07.005
17. Bonamigo RR, Bertolini W, de Oliveira FB, Dornelles SIT. Rosacea. In: Dermatology in Public Health Environments: A Comprehensive Textbook. Springer (2023). p. 603–20.
18. Peng G, Fadeel B. Understanding the bidirectional interactions between two-dimensional materials, microorganisms, and the immune system. Adv Drug Deliv Rev (2022) 188:114422. doi: 10.1016/j.addr.2022.114422
19. Minasyan H. Phagocytosis and oxycytosis: two arms of human innate immunity. Immunol Res (2018) 66(2):271–80. doi: 10.1007/s12026-018-8988-5
21. Guerriero J. Macrophages: their untold story in T cell activation and function. Int Rev Cell Mol Biol (2019) 342:73–93doi: 10.1016/bs.ircmb.2018.07.001.
22. Wang F-Y, Chi C-C. Rosacea, germs, and bowels: a review on gastrointestinal comorbidities and gut–skin axis of rosacea. Adv Ther (2021) 38(3):1415–24. doi: 10.1007/s12325-021-01624-x
23. Ande SN, Bodakhe AA, Bakal RL, Chandewar AV. How do acute and chronic inflammatory skin diseases arise? A Brief Rev (2022).
24. Rodrigues-Braz D, Zhao M, Yesilirmak N, Aractingi S, Behar-Cohen F, Bourges JL. Cutaneous and ocular rosacea: Common and specific physiopathogenic mechanisms and study models. Mol Vis (2021) 27:323.
25. Wang L, Wang YJ, Hao D, Wen X, Du D, He G, et al. The theranostics role of mast cells in the pathophysiology of rosacea. Front Med (Lausanne) (2020) 6:324. doi: 10.3389/fmed.2019.00324
26. Diaz-Jimenez D, Kolb JP, Cidlowski JA. Glucocorticoids as regulators of macrophage-mediated tissue homeostasis. Front Immunol (2021) 12:669891. doi: 10.3389/fimmu.2021.669891
27. Zhu W, Su J. Immune functions of phagocytic blood cells in teleost. Rev Aquac (2022) 14:630–46. doi: 10.1111/raq.12616
28. Sumpter TL, Balmert SC, Kaplan DH. Cutaneous immune responses mediated by dendritic cells and mast cells. JCI Insight (2019) 4(1):e123947. doi: 10.1172/jci.insight.123947
29. Guimarães GR, Almeida PP, de Oliveira Santos L, Rodrigues LP, de Carvalho JL, Boroni M. Hallmarks of aging in macrophages: consequences to skin inflammaging. Cells (2021) 10(6):1323.doi: 10.3390/cells10061323
30. Delans K, Kelly K, Feldman SR. Treatment strategies, including antibiotics, to target the immune component of rosacea. Expert Rev Clin Immunol (2022) 18(12):1239–51. doi: 10.1080/1744666X.2022.2128334
31. Huang C, Dong L, Zhao B, Lu Y, Huang S, Yuan Z, et al. Anti-inflammatory hydrogel dressings and skin wound healing. Clin Transl Med (2022) 12(11): e1094. doi: 10.1002/ctm2.1094
32. Meli VS, Veerasubramanian PK, Atcha H, Reitz Z, Downing TL, Liu WF. Biophysical regulation of macrophages in health and disease. J Leukoc Biol (2019) 106:283–99. doi: 10.1002/JLB.MR0318-126R
33. Sun Q, Hu S, Lou Z, Gao J. The macrophage polarization in inflammatory dermatosis and its potential drug candidates. Biomed Pharmacother (2023) 161:114469. doi: 10.1016/j.biopha.2023.114469
34. Irizarry-Caro RA, McDaniel MM, Overcast GR, Jain VG, Troutman TD, Pasare C. TLR signaling adapter BCAP regulates inflammatory to reparatory macrophage transition by promoting histone lactylation. Proc Natl Acad Sci U S A (2020) 117(48):30628–38. doi: 10.1073/pnas.2009778117
35. Mookherjee N, Anderson MA, Haagsman HP, Davidson D. Antimicrobial host defence peptides: functions and clinical potential. Nat Rev Drug Discov (2020) 19(5):311–32. doi: 10.1038/s41573-019-0058-8
36. Zhang J, Jiang P, Sheng L, Liu Y, Liu Y, Li M, et al. A novel mechanism of carvedilol efficacy for rosacea treatment: toll-like receptor 2 inhibition in macrophages. Front Immunol (2021) 12:609615. doi: 10.3389/fimmu.2021.609615
37. Silveira Rossi JL, Barbalho SM, Reverete de Araujo R, Bechara MD, Sloan KP, Sloan LA. Metabolic syndrome and cardiovascular diseases: Going beyond traditional risk factors. Diabetes Metab Res Rev (2022) 38(3): e3502doi: 10.1002/dmrr.3502.
38. Marson JW, Baldwin HE. Rosacea: a wholistic review and update from pathogenesis to diagnosis and therapy. Int J Dermatol (2020) 59(6):e175–82. doi: 10.1111/ijd.14757
39. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, et al. Standard classification of rosacea: Report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol (2002) 46:584–7. doi: 10.1067/mjd.2002.120625
40. Kang CN, Shah M, Tan J. Rosacea: an update in diagnosis, classification and management. Skin Ther Lett (2021) 26(4):1–8.
41. Luque-Martin R, Angell DC, Kalxdorf M, Bernard S, Thompson W, Eberl HC, et al. IFN-γ drives human monocyte differentiation into highly proinflammatory macrophages that resemble a phenotype relevant to psoriasis. J Immunol (2021) 207(2):555–68. doi: 10.4049/jimmunol.2001310
42. Zhang H, Zhang Y, Li Y, Wang Y, Yan S, Xu S, et al. Bioinformatics and network pharmacology identify the therapeutic role and potential mechanism of melatonin in AD and Rosacea. Front Immunol (2021) 12:756550. doi: 10.3389/fimmu.2021.756550
43. Ross R, Conti P. COVID-19 induced by SARS-CoV-2 causes Kawasaki-like disease in children: Role of pro-inflammatory and anti-inflammatory cytokines. Front Immunol (2020) 34:767–73doi: 10.23812/EDITORIAL-RONCONI-E-59.
44. Ni X, Lai Y. Keratinocyte: A trigger or an executor of psoriasis? J Leukoc Biol (2020) 108(2):485–91. doi: 10.1002/JLB.5MR0120-439R
45. Liu Z, Zhang J, Jiang P, Yin Z, Liu Y, Liu Y, et al. Paeoniflorin inhibits the macrophage-related rosacea-like inflammatory reaction through the suppressor of cytokine signaling 3-apoptosis signal-regulating kinase 1-p38 pathway. Medicine (Baltimore) (2021) 100(3):e23986. doi: 10.1097/MD.0000000000023986
46. Lee HJ, Hong YJ, Kim M. Angiogenesis in chronic inflammatory skin disorders. (2021) 22:12035. doi: 10.3390/ijms222112035
47. van Zuuren EJ, Arents BWM, van der Linden MMD, Vermeulen S, Fedorowicz Z, Tan J. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol (2021) 22:457–65. doi: 10.1007/s40257-021-00595-7
48. Jiang P, Liu Y, Zhang J, Liu Y, Li M, Tao M, et al. Mast cell stabilization: new mechanism underlying the therapeutic effect of intense pulsed light on rosacea. Inflamm Res (2023) 72(1):75–88. doi: 10.1007/s00011-022-01635-6
49. Theocharis AD, Manou D, Karamanos NK. The extracellular matrix as a multitasking player in disease. FEBS J (2019) 286(15):2830–69. doi: 10.1111/febs.14818
50. Yang L, Shou Y-H, Yang Y-S, Xu J-H. Elucidating the immune infiltration in acne and its comparison with rosacea by integrated bioinformatics analysis. PLoS One (2021) 16(3): e0248650. doi: 10.1371/journal.pone.0248650
51. Dull K, Lénárt K, Dajnoki Z, Póliska S, Uchiyama E, Hendrik Z, et al. Barrier function-related genes and proteins have an altered expression in acne-involved skin. J Eur Acad Dermatol Venereol (2023) 37(7):1415–25. doi: 10.1111/jdv.19062
52. Liu T, Deng Z, Xie H, Chen M, Xu S, Peng Q, et al. ADAMDEC1 promotes skin inflammation in rosacea via modulating the polarization of M1 macrophages. Biochem Biophys Res Commun (2020) 521:64–71. doi: 10.1016/j.bbrc.2019.10.073
53. Xiao W, Chen M, Peng Q, Sha K, Liu T, Xia J, et al. Lithocholic acid promotes rosacea-like skin inflammation via G protein-coupled bile acid receptor. Biochim Biophys Acta Mol Basis Dis (2022) 1868(12):166563. doi: 10.1016/j.bbadis.2022
54. Gold LS, Del Rosso JQ, Kircik L, Bhatia ND, Hooper D, Nahm WK, et al. Minocycline 1.5% foam for the topical treatment of moderate to severe papulopustular rosacea: results of 2 phase 3, randomized, clinical trials. J Am Acad Dermatol (2020) 82(5):1166–73.
56. Husein-ElAhmed H, Steinhoff M. Evaluation of the efficacy of subantimicrobial dose doxycycline in rosacea: a systematic review of clinical trials and meta-analysis. J Dtsch Dermatol Ges (2021) 19(1):7–17. doi: 10.1111/ddg.14247
57. Del Rosso JQ, Tanghetti E, Webster G, Stein Gold L, Thiboutot D, Gallo RL. Update on the management of rosacea from the American acne & Rosacea Society (AARS). J Clin Aesthetic Dermatol (2020) 13(6 Suppl):S17–s24.
58. van Zuuren EJ, Fedorowicz Z, Tan J, van der Linden MMD, Arents BWM, Carter B, et al. Interventions for rosacea based on the phenotype approach: an updated systematic review including GRADE assessments. Br J Dermatol (2019) 181:65–79. doi: 10.1111/bjd.17590
59. Searle T, Ali FR, Carolides S, Al-Niaimi F. Rosacea and Diet: What is New in 2021? J Clin Aesthet Dermatol (2021) 14(12):49–54.
60. Ebbelaar CCF, Venema AW, Van Dijk MR. Topical Ivermectin in the treatment of Papulopustular Rosacea: A systematic review of evidence and clinical guideline recommendations. Dermatol Ther (2018) 8:379–87. doi: 10.1007/s13555-018-0249-y
61. Ávila MY, Martínez-Pulgarín DF, Madrid C.R.J.C.L., Eye A. Topical ivermectin-metronidazole gel therapy in the treatment of blepharitis caused by Demodex spp.: a randomized clinical trial. Cont Lens Anterior Eye (2021) 44(3):101326. doi: 10.1016/j.clae.2020.04.011
62. Schaller M, Kemény L, Havlickova B, Jackson JM, Ambroziak M, Lynde C, et al. A randomized phase 3b/4 study to evaluate concomitant use of topical ivermectin 1% cream and doxycycline 40-mg modified-release capsules, versus topical ivermectin 1% cream and placebo in the treatment of severe rosacea. J Am Acad Dermatol (2020) 82:336–43. doi: 10.1016/j.jaad.2019.05.063
63. Fukuta Y, Chua H, Phe K, Lee Poythress E, Brown CA. Infectious diseases management in wound care settings: common causative organisms and frequently prescribed antibiotics. Adv Skin Wound Care (2022) 35(10):535–43. doi: 10.1097/01.ASW.0000855744.86686.ea
64. Sharma A, Kroumpouzos G, Kassir M, Galadari H, Goren A, Grabbe S, et al. Rosacea management: a comprehensive review. J Cosmet Dermatol (2022) 21(5):1895–904 10.1111/jocd.14816.
65. Jain AK, Jain S, Abourehab MA, Mehta P, Kesharwani P. An insight on topically applied formulations for management of various skin disorders. J Biomater Sci Polym Ed (2022) 33(18):2406–32. doi: 10.1080/09205063.2022.2103625
66. Quaresma JAS. Organization of the skin immune system and compartmentalized immune responses in infectious diseases. Clin Microbiol Rev (2019) 32(4):e00034–00018. doi: 10.1128/CMR.00034-18
67. Ferguson PJ, de Jesus AA, Goldbach-Mansky R. Autoinflammatory diseases affecting bone and joints, and autoinflammatory interferonopathies. In: Stiehm’s Immune Deficiencies. Elsevier (2020). p. 685–720.
68. Wang M, Charareh P, Lei X, Zhong JL. Autophagy: multiple mechanisms to protect skin from ultraviolet radiation-driven photoaging. Oxid Med Cell Longev (2019) 2019:8135985. doi: 10.1155/2019/8135985
69. Passeron T, Zouboulis CC, Tan J, Andersen ML, Katta R, Lyu X, et al. Adult skin acute stress responses to short-term environmental and internal aggression from exposome factors. J Eur Acad Dermatol Venereol (2021) 35(10):1963–75. doi: 10.1111/jdv.17432
70. Paik SJ, Kim DJ, Jung SK. Preventive effect of pharmaceutical phytochemicals targeting the Src family of protein tyrosine kinases and aryl hydrocarbon receptor on environmental stress-induced skin disease. Int J Mol Sci (2023) 24:5953. doi: 10.3390/ijms24065953
71. Xia T, Fu S, Yang R, Yang K. Advances in the study of macrophage polarization in inflammatory immune skin diseases. Authorea (2023). doi: 10.22541/au.168369484.44857588/v1
72. Napolitano M, Fabbrocini G, Martora F, Picone V, Morelli P, Patruno C. Role of aryl hydrocarbon receptor activation in inflammatory chronic skin diseases. Cells (2021) 10(11):3559. doi: 10.3390/cells10123559
73. Fernández-Gallego N, Sánchez-Madrid F, Cibrian DJC. Role of AHR ligands in skin homeostasis and cutaneous inflammation. Cells (2021) 10(11):3176. doi: 10.3390/cells10113176.
75. Bissonnette R, Gold LS, Rubenstein DS, Tallman AM, Armstrong A. Tapinarof in the treatment of psoriasis: A review of the unique mechanism of action of a novel therapeutic aryl hydrocarbon receptor–modulating agent. J Am Acad Dermatol (2021) 84(4):1059–67. doi: 10.1016/j.jaad.2020.10.085
76. Fabbrocini G, Monteil CB, Carballido F. A cream containing the sap of oat plantlets and mandarin extract soothes the symptoms of rosacea and improves the quality of life of patients. J Eur Acad Dermatol Venereol (2022) 36:3–11. doi: 10.1111/jdv.18201
77. Yosipovitch G, Misery L, Proksch E, Metz M, Ständer S, Schmelz M. Skin barrier damage and itch: review of mechanisms, topical management and future directions. Acta Derm Venereol (2019) 99(13):1201–9. doi: 10.2340/00015555-3296
78. Jain K, Ahmad J. Nanotheranostics for Treatment and Diagnosis of Infectious Diseases. Academic Press (2022).
79. Di Cola I, Ruscitti P, Giacomelli R, Cipriani P. The pathogenic role of interferons in the hyperinflammatory response on adult-onset Still’s disease and macrophage activation syndrome: paving the way towards new therapeutic targets. J. Clin. Med (2021) 10:1164. doi: 10.3390/jcm10061164
80. Casas C, Paul C, Lahfa M, Livideanu B, Lejeune O, Alvarez-Georges S, et al. Quantification of Demodex folliculorum by PCR in rosacea and its relationship to skin innate immune activation. Exp Dermatol (2012) 21(12):906–10. doi: 10.1111/exd.12030
81. Searle T, Ali FR, Carolides S, Al-Niaimi F. Rosacea and the gastrointestinal system. Australas J Dermatol (2020) 61(4):307–11. doi: 10.1111/ajd.13401
82. Gao C, Ge L, Chen D, Zhang M, Zhao L, Liu W, et al. Increased frequency of circulating classical monocytes in patients with Rosacea. Clin Cosmetic Investigational Dermatol (2021) 14:1629–36. doi: 10.2147/CCID.S336194
83. Li M, Tao M, Zhang Y, Pan R, Gu D, Xu Y. Neurogenic rosacea could be a small fiber neuropathy. Front Pain Res (Lausanne) (2023) 4:1122134. doi: 10.3389/fpain.2023.1122134
84. Kim J, Kim KJM. Elucidating the potential pharmaceutical mechanism of Gyejibokryeong-hwan on rosacea using network analysis. Medicine (Baltimore) (2023) 102(9):e33023. doi: 10.1097/MD.0000000000033023
85. Muto Y, Wang Z, Vanderberghe M, Two A, Gallo RL, Di Nardo A. Mast cells are key mediators of cathelicidin-initiated skin inflammation in rosacea. J Invest Dermatol (2014) 134(11):2728–36. doi: 10.1038/jid.2014.222
86. Zhou L, Zhao H, Zhao H, Meng X, Zhao Z, Xie H, et al. GBP5 exacerbates rosacea-like skin inflammation by skewing macrophage polarization towards M1 phenotype through the NF-κB signalling pathway. J Eur Acad Dermatol Venereol: JEADV (2023) 37:796–809. doi: 10.1111/jdv.18725
87. Peng Q, Sha K, Liu Y, Chen M, Xu S, Hongfu Xie H, et al. mTORC1-mediated angiogenesis is required for the development of Rosacea. Front Cell Dev Biol (2021) 9:751785. doi: 10.3389/fcell.2021.751785
88. Siouti E, Andreakos E. The many facets of macrophages in rheumatoid arthritis. Biochem Pharmacol (2019) 165:152–69. doi: 10.1016/j.bcp.2019.03.029
89. Barbarino SC, Bucay VW, Cohen JL, Gold MH. Integrative skincare trial of intense pulsed light followed by the phyto-corrective mask, phyto-corrective gel, and resveratrol BE for decreasing post-procedure downtime and improving procedure outcomes in patients with rosacea. J Cosmet Dermatol (2022) 21(9):3759–67. doi: 10.1111/jocd.15189
90. Sahu T, Ratre YK, Chauhan S, Bhaskar LVKS, Nair MP, Verma HK. Nanotechnology based drug delivery system: Current strategies and emerging therapeutic potential for medical science. Journal of Drug Delivery Science and Technology (2021) 63:102487. doi: 10.1016/j.jddst.2021.102487
91. Zhao Y-D, Muhetaerjiang M, An HW, Fang X, Zhao Y, Wang H. Nanomedicine enables spatiotemporally regulating macrophage-based cancer immunotherapy. Biomaterials (2021) 268:120552. doi: 10.1016/j.biomaterials.2020.120552
92. Wahab S, Ghazwani M, Hani U, Hakami AR, Almehizia AA, Ahmad W, et al. Nanomaterials-based novel immune strategies in clinical translation for cancer therapy. Molecules (2023) 28(3):1216. doi: 10.3390/molecules28031216
93. Kothari D, Patel S, Kim S-K. Probiotic supplements might not be universally-effective and safe: A review. Biomed Pharmacother (2019) 111:537–47. doi: 10.1016/j.biopha.2018.12.104
94. Goldbach-Mansky R, Shroff SD, Wilson M, Snyder C, Plehn S, Barham B, et al. A pilot study to evaluate the safety and efficacy of the long-acting interleukin-1 inhibitor rilonacept (interleukin-1 Trap) in patients with familial cold autoinflammatory syndrome. Arthritis Rheumatism (2008) 58(8):2432–42. doi: 10.1002/art.23620
96. Arnold DD, Yalamanoglu A, Boyman O. Systematic review of safety and efficacy of IL-1-targeted biologics in treating immune-mediated disorders. Front Immunol (2022) 13:888392. doi: 10.3389/fimmu.2022.888392
98. Sun Y, Chen LH, Wang HX, Zhu PY, Jiang SB, Qi RQ, et al. Activation of aryl hydrocarbon receptor ameliorates rosacea-like eruptions in mice and suppresses the TLR signaling pathway in LL-37-induced HaCaT cells. Toxicol Appl Pharmacol (2022) 451:116189. doi: 10.1016/j.taap.2022.116189
99. Rafiq S, Hackett CS, Brentjens R. Engineering strategies to overcome the current roadblocks in CAR T cell therapy. Nat Rev Clin Oncol (2020) 17(3):147–67. doi: 10.1038/s41571-019-0297-y
100. Movia D, Prina-Mello A. Preclinical development of orally inhaled drugs (OIDs)—are animal models predictive or shall we move towards in vitro non-animal models? Animals (Basel) (2020) 10(8):1259. doi: 10.3390/ani10081259
101. Wang S, Yang Y, Ma P, Huang H, Tang Q, Miao H, et al. Landscape and perspectives of macrophage targeted cancer therapy in clinical trials. Mol Ther Oncolytic (2022) 24:799–813. doi: 10.1016/j.omto.2022.02.019
102. Tan J, Almeida LM, Bewley A, Cribier B, Dlova NC, Gallo R, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol (2017) 176(2):431–8. doi: 10.1111/bjd.15122
103. Schaller M, Almeida LMC, Bewley A, Cribier B, Del Rosso J, Dlova NC, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol (2020) 182:1269–76. doi: 10.1111/bjd.18420
104. Melnik B. C. Endoplasmic reticulum stress: key promoter of rosacea pathogenesis. Exp Dermatol (2014) 23(12):868–73. doi: 10.1111/exd.12517
105. Oh S, Son M, Park J, Kang D, Byun KJM. Radiofrequency irradiation modulates TRPV1-related burning sensation in rosacea. Molecules (2021) 26(5):1424. doi: 10.3390/molecules26051424
106. Chen M, Deng Z, Huang Y, Li J. Prevalence and risk factors of anxiety and depression in rosacea patients: a cross-sectional study in China. Front Psychiatry (2021) 12:659171. doi: 10.3389/fpsyt.2021.659171
107. Kreidel MK, Jhaveri M. Introduction to essential oils and essential oil processing. (2021), 99–122. doi: 10.1007/978-3-030-58954-7_5
108. Kim J, Ahamed A, Chen K, Lebig EG, Petros B, Saeed S, et al. Skin microbiota and its role in health and disease with an emphasis on wound healing and chronic wound development. In: Microbiome, Immunity, Digestive Health and Nutrition. Elsevier (2022). p. 297–311. doi: 10.1016/B978-0-12-822238-6.00027-3
109. Forton FM. The pathogenic role of Demodex mites in Rosacea: a potential therapeutic target already in erythematotelangiectatic Rosacea? Dermatol Ther (Heidelb) (2020) 10(6):1229–53. doi: 10.1007/s13555-020-00458-9
110. Shaxnoza M, Yelena Y, Sevara M. Determination of the level of some indicators of inflammation in patients with Rosacea. European Journal of Modern Medicine and Practice (2022) 2:38–42.
112. Jabbehdari S, Memar OM, Caughlin B, Djalilian AR. Update on the pathogenesis and management of ocular rosacea: an interdisciplinary review. Eur J Ophthalmol (2021) 31(1):22–33. doi: 10.1177/1120672120937252
113. Patel NV, Gupta N, Shetty R. Preferred practice patterns and review on rosacea. Indian J Ophthalmol (2023) 71:1382–90.
114. Wienholtz NKF, Egeberg A, Thyssen JPJR. Rosacea and cardiovascular comorbidities. Rosacea (2020), 105–12. doi: 10.1007/978-3-030-52097-7_10
115. Alia E, Feng H. Rosacea pathogenesis, common triggers, and dietary role: the cause, the trigger, and the positive effects of different foods. Clinics Dermatol (2022) 40:122–7. doi: 10.1016/j.clindermatol.2021.10.004
117. Nowicka D, Chilicka K, Dzieńdziora-Urbińska I, Szyguła R. Skincare in Rosacea from the cosmetologist’s perspective: A narrative review. J Clin Med (2022) 12(1):115. doi: 10.3390/jcm12010115
118. Santoro F, Lachmann N. An open-label, intra-individual study to evaluate a regimen of three cosmetic products combined with medical treatment of Rosacea: cutaneous tolerability and effect on hydration. Dermatol Ther (Heidelb) (2019) 9:775–84. doi: 10.1007/s13555-019-00331-4
119. Yamasaki K, Miyachi Y. Perspectives on rosacea patient characteristics and quality of life using baseline data from a phase 3 clinical study conducted in Japan. J Dermatol (2022) 49(12):1221–7. doi: 10.1111/1346-8138.16596
120. Caf N, Özkök Akbulut T, Can MM, Sarı M, Atsü AN, Türkoğlu Z. Evaluation of subclinical atherosclerosis in rosacea patients by flow-mediated dilatation method. J Cosmet Dermatol (2023) 22:1001–10. doi: 10.1111/jocd.15492
121. Alford MA, Baquir B, Santana FL, Haney EF, Hancock RE. Cathelicidin host defense peptides and inflammatory signaling: Striking a balance. Front Microbiol (2020) 11:1902. doi: 10.3389/fmicb.2020.01902
122. Cribier B. Rosacea: Treatment targets based on new physiopathology data. In: Annales de Dermatologie et de Vénéréologie, vol. 149. Elsevier (2022). p. 99–107.
123. Hauck S, et al. Collagen/hyaluronan based hydrogels releasing sulfated hyaluronan improve dermal wound healing in diabetic mice via reducing inflammatory macrophage activity. Bioact Mater (2021) 6(12):4342–59. doi: 10.1016/j.bioactmat.2021.04.026
124. Ross R, Maxwell J, Chandra S, Liu X, Lapine M, Shaw T, et al. British Society for Investigative Dermatology Annual. (2019).
125. Syed MH. MRGPRX2 Mediated Mast Cell Responses Are Suppressed by Lactic Acid. Michigan State University (2021).
126. Kim D, Kobayashi T, Voisin B, Jo J. Single-cell RNA sequencing-guided patient care in refractory drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms. J Invest Dermatol (2019) 139:S170–0. doi: 10.1016/j.jid.2019.03.1056
127. Jin S, Ramos R. Computational exploration of cellular communication in skin from emerging single-cell and spatial transcriptomic data. Biochem Soc Trans (2022) 50:297–308. doi: 10.1042/BST20210863
128. Wolff D, et al. National Institutes of Health Consensus Development project on criteria for clinical trials in chronic graft-versus-host disease: IV. The 2020 highly morbid forms report. Transplant Cell Ther (2021) 27(10):817–35. doi: 10.1016/j.jtct.2021.06.001
129. Roh K-B, Jang Y, Cho E, Park D, Kweon DH, Jung E. Chlorogenic acid isomers isolated from artemisia lavandulaefolia exhibit anti-rosacea effects in vitro. Biomedicines (2022) 10(2):463. doi: 10.3390/biomedicines10020463
130. Franklin RA. Fibroblasts and macrophages: Collaborators in tissue homeostasis. Immunol Rev (2021) 302:86–103. doi: 10.1111/imr.12989
131. Falanga V, Isseroff RR, Soulika AM, Romanelli M, Margolis D, Kapp S, et al. Chronic wounds. Nat Rev Dis Primers (2022) 8(1):50. doi: 10.1038/s41572-022-00377-3
132. Lei Y, Tang R, Xu J, Wang W, Zhang B, Liu J, et al. Applications of single-cell sequencing in cancer research: progress and perspectives. J Hematol Oncol (2021) 14(1):91. doi: 10.1186/s13045-021-01105-2
133. Sallam MA, Prakash S, Kumbhojkar N, Shields CW 4th, Mitragotri S. Formulation-based approaches for dermal delivery of vaccines and therapeutic nucleic acids: Recent advances and future perspectives. (2021) 6(3): e10215. doi: 10.1002/btm2.10215
134. Apaydin DC, Zakarauskas-Seth BI, Carnevale L, Apaydin O, Perrotta M, Carnevale R, et al. Interferon-γ drives macrophage reprogramming, cerebrovascular remodelling, and cognitive dysfunction in a zebrafish and a mouse model of ion imbalance and pressure overload. Cardiovasc Res (2022) 119(5):1234–49. doi: 10.1093/cvr/cvac188
135. Jain KK. An overview of drug delivery systems. Methods Mol Biol (2020) 2059:1–54. doi: 10.1007/978-1-4939-9798-5_1
136. Nour S, Imani R, Chaudhry GR, Sharifi AM. Skin wound healing assisted by angiogenic targeted tissue engineering: A comprehensive review of bioengineered approaches. J Biomed Mater Res A (2021) 109(4):453–78. doi: 10.1002/jbm.a.37105
137. Zhao M, Jiang J, Zhao M, Chang C, Wu H, Lu Q. The application of single-cell RNA sequencing in studies of autoimmune diseases: a comprehensive review. Clin Rev Allergy Immunol (2021) 60(1):68–86. doi: 10.1007/s12016-020-08813-6
138. Gazi U, Gureser AS, Oztekin A, Karasartova D, Kosar-Acar N, Derici MK, et al. Skin-homing T-cell responses associated with Demodex infestation and rosacea. Parasite Immunol (2019) 41(8): e12658. doi: 10.1111/pim.12658
139. Zhao Z, Liu T, Liang Y, Cui W, Li D, Zhang G, et al. N2-polarized neutrophils reduce inflammation in rosacea by regulating vascular factors and proliferation of CD4+ T cells. J Invest Dermatol (2022) 142(7):1835–1844. e1832. doi: 10.1016/j.jid.2021.12.009
140. Do T, Perrie J, Pellegrini M, Gudjonsson J, Ma F, Modlin RL, et al. 373 Identification of immune cell pathways in acne vs. rosacea by single-cell RNA sequencing and single-cell spatial imaging. J Invest Dermatol (2023) 143:S64. doi: 10.1016/j.jid.2023.03.378
141. Clark R. Harnessing Single-Cell Technologies to Understand and Diagnose Rejection in Clinical Face and Upper Extremity Transplantations. Brigham and Women’s Hospital (2020).
142. Harden JL, Shih Y, Rajendran D, Hofland H, Chang A. LB1144 Quantitative analysis of differentially expressed proteins in papulopustular rosacea. Journal of Investigative Dermatology (2019) 139:B25. doi: 10.1016/j.jid.2019.06.117
143. Vicino A, Cochet S, Pistocchi S, Conrad C, Ribi C, Du Pasquier R, et al. A severe case of neuroleukemiosis caused by B cell chronic lymphocytic leukemia, presenting as mononeuritis multiplex. J Peripher Nerv Syst (2023) 28(2):266–8. doi: 10.1111/jns.12552
144. Zhao Z, Zhu H, Li Q, Liao W, Chen K, Yang M, et al. Skin CD4+ Trm cells distinguish acute cutaneous lupus erythematosus from localized discoid lupus erythematosus/subacute cutaneous lupus erythematosus and other skin diseases. J Autoimmun (2022) 128:102811. doi: 10.1016/j.jaut.2022.102811
145. Furlong-Silva J, Cross SD, Marriott AE, Pionnier N, Archer J, Steven A, et al. Tetracyclines improve experimental lymphatic filariasis pathology by disrupting interleukin-4 receptor–mediated lymphangiogenesis. J Clin Invest (2021) 131(5):e140853. doi: 10.1172/JCI140853
146. Sudarshan K, Boda AK, Dogra S, Bose I, Yadav PN, Aidhen IS, et al. Discovery of an isocoumarin analogue that modulates neuronal functions via neurotrophin receptor TrkB. Bioorg Med Chem Lett (2019) 29(4):585–90. doi: 10.1016/j.bmcl.2018.12.057
147. Keum H, Yoo D, Jon S. Photomedicine based on heme-derived compounds. Adv Drug Deliv Rev (2022) 182:114134. doi: 10.1016/j.addr.2022.114134
148. Son M, Park J, Oh S, Choi J, Shim M, Kang D, et al. Radiofrequency irradiation attenuates angiogenesis and inflammation in UVB-induced rosacea in mouse skin. Exp Dermatol (2020) 29(7):659–66. doi: 10.1111/exd.14115
149. Nisbet SJ, Targett D, Rawlings AV, Qian K, Wang X, Lin CB, et al. Clinical and in vitro evaluation of new anti-redness cosmetic products in subjects with winter xerosis and sensitive skin. Int J Cosmetic Sci (2019) 41:534–47. doi: 10.1111/ics.12559
Keywords: rosacea, macrophage, inflammation, targeted therapies, skin, immune system
Citation: Liu Y, Zhou Y, Chu C and Jiang X (2023) The role of macrophages in rosacea: implications for targeted therapies. Front. Immunol. 14:1211953. doi: 10.3389/fimmu.2023.1211953
Received: 25 April 2023; Accepted: 14 July 2023;
Published: 24 August 2023.
Edited by:
Steven O’Reilly, STipe Therapeutics, DenmarkReviewed by:
Nita Katarina Frifelt Wienholtz, Bispebjerg Hospital, DenmarkCopyright © 2023 Liu, Zhou, Chu and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xian Jiang, amlhbmd4aWFuQHNjdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.