 Suibin Lin1†
Suibin Lin1† Zhiming Lin
Zhiming Lin Junmei Feng
Junmei Feng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 29 September 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1206959
This article is part of the Research Topic Cutting-Edge Mechanisms and Technologies in Immunoinflammatory Ocular Diseases View all 5 articles
Behcet’s disease (BD) is a chronic multi-systemic disease characterized by relapsing-remitting oral ulcers, genital ulcers, ocular inflammatory involvements, and numerous other systemic features. Ocular involvements are quite common in BD and may cause severe tissue damage and potentially blindness. Even though the pathogenesis of BD remains ambiguous, growing evidences have shown that genetic factors, environmental triggers and immunological abnormalities play significant roles in its development and progression. Novel biotherapies targeting IFN-γ, TNF-α and interleukins have been used in recent years. In this review, we mainly pay attention to the ocular involvement of BD, and discuss the current understanding of mechanisms and advances in therapeutic approaches, especially novel biologics. Finally, we discuss the management in patients with pregnancy.
Behcet’s disease (BD) is a chronic multi-systemic disease pictured by relapsing-remitting oral aphthous ulcers, genital ulcers, ocular inflammatory involvements, skin impairment, and numerous other symptoms (1). BD is more prevalent in countries along the ancient Silk Road, from East Asian countries to Mediterranean basin (2). Turkey was reported to have the highest prevalence rate around the world with up to 420 cases in every 100,000 residents (3). Ocular involvement is most frequently observed in BD, with a prevalence of 40 to 70% in patients with BD (3, 4). In addition, uveitis is the most common and most classic ocular manifestation, which occurs in 60 to 80% of cases (5). It is usually acute and recurrent, and presents non-granulomatous panuveitis related to retinal vasculitis (5). It may cause severe tissue damage in the eyes and potentially lead to blindness. Other ocular manifestations are relatively rare, such as episcleritis, scleritis, conjunctival ulcers, keratitis, orbital inflammatory disease, isolated optic neuritis and oculomotor palsies (5).
Even though the pathogenesis of BD remains obscure, recent studies have indicated that both genetic and environmental factors play an important part in its development and progression. Due to the advances of recent genome analysis research, a number of susceptibility genes related to the pathophysiology of non-infectious uveitis in BD have been discovered (2). Immunological aberrations in both innate and acquired immune systems are found to be implicated in the mechanisms of BD.
Treatment of ocular involvement in BD includes corticosteroids and immunosuppressant therapy. Conventional immunosuppressors such as azathioprine and cyclosporine A were often used, and they were recommended by EULAR in 2018 (6). However, potential side effects have limited their application and require close monitoring. For example, azathioprine showed hematologic, hepatic and neurotoxicity, whereas cyclosporine A presented nephrotoxicity and hypertension (5). Apart from conventional immunosuppressors, novel biologic agents such as interferon-a (IFN-α), tumor necrosis factor-a (TNF-α) inhibitors, different bio-agents targeting interleukins and related receptors were found to show a significant improvement in the visual prognosis of BD patients.
The main target of this review is to discuss latest advances in areas regarding pathogenesis of BD ocular involvement and related novel treatment approaches.
Various evidences have shown that host genetic factor play a crucial role in the pathogenesis of BD. Familial aggregation and high recurrence risk in siblings suggested the involvement of genetic factor in BD development (7, 8). HLA-B51 has been considered as the strongest predisposing gene in BD. Recent years, with the development of novel research techniques such as genomewide association study (GWAS), more and more genes are identified to be associated with pathogenesis of BD ocular involvement (2).
It has been first reported by Ohno et al. in 1973 that HL-A5 (later known as HLA-B5), which includes HLA-B51, has a strong association with BD among the Japanese population (9). After this initial genetic discovery, HLA-B51 was then found to have a strong association with BD in 1982 (10). Afterwards, this association was further confirmed in multiple studies among different populations of BD patients (11–22). HLAB51 allele accounts for about 19% of the genetic susceptibility and is by far the most powerful genetic factor in BD (23, 24). A meta-analysis of 78 independent researches indicated that individuals with HLA B51/B5 are 5.78 times more likely to develop BD compared with non-carriers (25). The strong relationship between HLA-B51 and BD was also confirmed in two large GWAS studies recently, which was conducted in Turkish and Japanese populations respectively (26, 27). In addition, several studies have reported that HLA-B51 positive BD patients have a higher risk of eye complications and genital ulcers in comparison with HLA-B51 negative BD patients, indicating a potential prognostic valve of HLA-B51 (28, 29).
Apart from HLA-B51, other HLA genes also showed disease susceptibility to BD. HLA-A26 was identified to be correlated with BD in various populations such as Chinese Taiwanese, Greek, Japanese, South Korean, Saudi Arabian and Turks (30–35). Carriers of this allele in Japanese and South Korean BD patients were observed with a higher risk of ocular involvement and a poor visual prognosis (36–38). Besides, the HLA-A02, HLA-A24, HLA-A26, HLA-A31, HLA-B27 and HLA-B57 were recognized as risk alleles, and the HLA-A03, HLA-B15, HLA-B35, HLA-B49 and HLA-B58 were recognized as protective alleles to BD development in different populations (30, 39–46).
The endoplasmic reticulum aminopeptidase-1 (ERAP1) gene, locating at 5q15, encodes an enzyme that trim the proteasome-processed antigenic peptides for attachment to MHC-I molecules and expression on cell surface (47, 48). Genome-wide association tests were performed in the subgroup of GWAS discovery collections with BD uveitis and two SNPs in ERAP1 were identified to confer risk for BD uveitis recessively—rs10050860 and rs17482078, which encode p.Asp575Asn and p.Arg725Gln alterations in ERAP1 respectively (49). And the association was further confirmed by a meta-analysis of the p.Arg725Gln SNP, which combines discovery and replication collections of Turkish population including 790 BD uveitis and 1879 controls (49). In addition, several studies have shown that the ERAP1 variants present higher susceptibility for BD in HLA-B51 positive cases (44). Homozygosity of ERAP1 p.Arg725Gln was more likely to develop BD in HLA-B51 positive individuals than in HLA-B51 negative cases (OR=3.78, 95% CI=1.94-7.35 vs OR=1.48, 95% CI=0.78-2.80) (44). It is assumed that variants of ERAP1 might influence the repertoire of disease-associated peptides that attach to HLA-B51 protein and contributes to disease susceptibility.
MHC class I chain-related gene A (MICA) is positioned in the centromeric region of HLA-B. MICA proteins present homology with classical HLA molecules and act as ligands for NKG2D receptors, which are expressed on natural killer-cell, γδT cells and αβCD8T cells (50). Studies have shown that MICA*009, MICA*019 and MICA*A6 alleles are associated with BD susceptibility (22, 51, 52). A strong linkage disequilibrium between MICA*A6 and HLA-B51 was observed by a Korean study in both BD cases and healthy controls (53). However, independent association between MICA and BD was not observed in recent GWAS studies (26, 27, 41).
IL-10 gene is positioned at 1q21-32. IL-10 is a cytokine with anti-inflammation function that impedes antigen presentation by reducing the MHC expression on cellular surfaces and hinders the co-stimulation activity of macrophages, T lymphocytes and NK-cell activation (54). Existing genotype analyses reported different IL-10 genotypes associated with BD (55, 56). More recently, GWAS have identified numerous variants within the IL-10 gene related to BD in various ethnic populations, including rs1800872, rs1518111, rs1554286, and rs1800871 (26, 27, 55, 57, 58). In addition, the rs1518111 and rs1800871 were also found in non-infectious uveitis patients (26, 27, 59). As shown in expression studies, the genetic IL-10 variants were related to decreased levels of IL-10, which may induce a susceptible inflammatory state and increase BD susceptibility (26). These results indicated that IL-10 gene polymorphisms may contribute to the development of ocular involvement in BD.
Pro-inflammatory cytokines such as IL-12 and IL-23 promote Th1 differentiation and stimulate Th17 proliferation, respectively. GWAS and meta-analysis reported several SNPs in IL23R-IL12RB2 and IL12A related to BD susceptibility in different populations (26, 27). Furthermore, a strong correlation between IL-23R rs17375018 and BD uveitis was found in a Chinese Han population (60). This study also reported that IL-23R SNP rs11209032 was associated with uveitis susceptibility in patients with BD.
Due to the increasing GWAS researches and meta-analyses in recent years, more and more SNPs were identified to be linked to BD uveitis, including SNPs of UBAC2, STAT4, TNFAIP3, CCR1, KLRC4, IL1A-IL1B, IRF8, CEBPB-PTPN1, ADO-EGR2, RIPK2, LACC1, JRKL-CNTN5, FUT2, MEFV, NCOA5 genes and so on (2, 61).
It is not sufficient to elucidate the development of BD by genetic abnormalities alone. In patients with genetic susceptibility to BD, environmental triggers have long been proposed. The environmental triggers contain infections caused by bacteria and viruses, as well as abnormal autoantigens. Bacterial species like Streptococcus sanguis, Helicobacter pylori, and Mycoplasma and many Herpesviridiae such as HSV1, CMV, VZV and EBV have been investigated (62). Furthermore, Streptococcus sanguis and HSV have been proved to induce BD-like symptoms in mice models respectively (63, 64). Autoantigens are suggested to play a crucial role in the mechanisms of BD through molecular mimicry (1). Researchers have identified several autoantigens in BD ocular involvement, such as the heat-shock protein 60 kDa (HSP60), retinal S antigen and interphotoreceptor retinoid-binding protein (IRBP) (62).
Human HSP60 and counterpart HSP65 related to S. sanguinis were revealed to have high homology. Four peptides of bacterial HSP65 (111-125, 154-172, 219-233, and 311-326) were found to stimulate lymphoproliferative immune reactions and these peptides showed 50%-80% homology to the corresponding human HSP60 (65, 66). It is suggested that cross-reaction between human HSP60 and bacterial HSP65 may induce autoimmune disorders and play a significant part in the pathogenesis of BD. Furthermore, several animal studies have shown that immunization of HSP peptide to rats by different routes (subcutaneously, orally or nasally) could induce clinical and/or histological uveitis (67, 68). It is also shown that antigenic homology exists between HSP60 and retinal antigen (69). Thus, HSP is believed to participate in the ocular lesions of BD.
Retinal S-antigen is a well-studied autoantigen for autoimmune uveitis. It can induce experimental autoimmune uveitis (EAU) in animal models, which is similar to human uveitis both clinically and histologically. Besides, it is suggested that administration with human S-Antigen-Ig fusion protein to rats is capable of preventing EAU. On the other hand, autoimmunity to S-antigen has been confirmed in BD patients with retinal vasculitis and uveitis (70, 71). It is also reported that some epitopes of S-antigen are homologous with certain amino acid regions of HLA-B51 and HLA-B27 (72). These findings indicated that retinal S-antigen may be involved in the mechanisms of BD ocular manifestations.
IRBP is considered to facilitate transport of retinoids between the retina and pigment epithelium (73, 74). IRBP has 1264 amino acid residues and consists of four repeating units, with one uveitogenic site in each unit. In particular, strong uveitogenicity is elicited in the fourth repeated unit. IRBP and derived peptides are widely used to induce EAU, especially in mice (75). Injection of bovine IRBP in Lewis rats induced severe autoimmune uveoretinitis (76, 77). And different doses of antigen and the categories of animals applied could lead to different spectrum of uveoretinitis, from hyperacute to chronic. Furthermore, several studies have demonstrated immune responses to IRBP in BD patients with uveitis (70). Cellular autoimmunity and cytokine changes were recognized in BD patients with uveitis, with significantly higher titers of IL-6, IL-17, and IFN-γ compared to healthy controls. And BD patients with active uveitis identified higher IFN-γ compared to remissive uveitis. Therefore, IRBP is potential participated in the development of BD uveitis.
Immune system dysfunction has been observed in BD. T cells are recognized as major lymphocyte subsets implicated in BD development. Growing evidences have shown that NKT cells, γδT cells, Th cells, Treg cells and cytokines with different functions may play significant roles in the pathogenesis of BD ocular involvement and might be potential targets for treatment.
NK cells are main components of the innate immunity. Their functions contain both nonspecific cytotoxic activity and regulatory roles in the innate and acquired immune responses by cytokine production (78). However, inconsistent results have been indicated in BD patients. Some studies have reported that NK cells activity was increased in active BD patients. Inversely, decreased levels of CD56brightCD16- and CD56dimCD16+ NK cells in peripheral blood were reported in patients with BD recently (79). In addition, a study found that the level of CD8+CD56+ NKT cells was higher in aqueous humor as well as peripheral blood in BD patients with uveitis (80). Further study revealed that CD8brightCD56+ T cells in Behcet’s uveitis possess functional NK receptors and display strong cytotoxic effect via Fas-ligand dependent pathway and perforin-dependent pathway (81). Both the clinical severity and histopathological severity of uveoretinitis were significantly milder in experimental autoimmune uveoretinitis-susceptible mice depleted of NK cells (81). Based on the secreted cytokines, NK cells is classified into different subtypes, such as NK1, NK2, NK22, NK17 and NKreg cells. It is indicated that the NK1/NK2 paradigm can regulate pathogenic Th1 or Th2 biased immune reactions in particular. NK2 cells were found to have a significant association with BD in remission stage (62). NK2 cells could inhibit INFγ secretion by Th1 cells in vitro (82). This study suggested that NK cells might control disease remission in patients with BD through modulating Th1 response which is mediated by NK2 cells (82). The characteristic of NK cells and NK1/NK2 paradigm requires further investigation especially in BD patients with ocular manifestations.
It is well known that γδ T cells are involved in regulating autoimmune response. In patients with BD, researchers have found that γδT cells were enriched, activated, and highly proliferative in response to various microbial infections (83–85). It is also found that γδT cells associate with active stage of BD, as well as elevated CD69 expression and increased IFN-γ and TNF-α production (1). The Vγ9/Vδ2T cells are the major subsets of γδT cells which represents up to 90% of the circulating γδT cells in humans. TCR Vγ9Vδ2+ Th1-like cells can be generated from intra-ocular fluid in BD uveitis patients (86, 87). Moreover, activated γδT cells exacerbate EAU by promoting the activation of IL-17+ uveitogenic αβT cells (88). These finding indicated that γδT cells may contribute to the pathogenesis of uveitis in BD.
Elevated levels of Th1 cells and related cytokine production (including IL-2, IL-12, IL-18, and IFN-γ) was found in active BD patients (89, 90) (Figure 1). Different studies also observed higher IFN-γ in aqueous humor of BD patients than that of other diseases (90, 91).
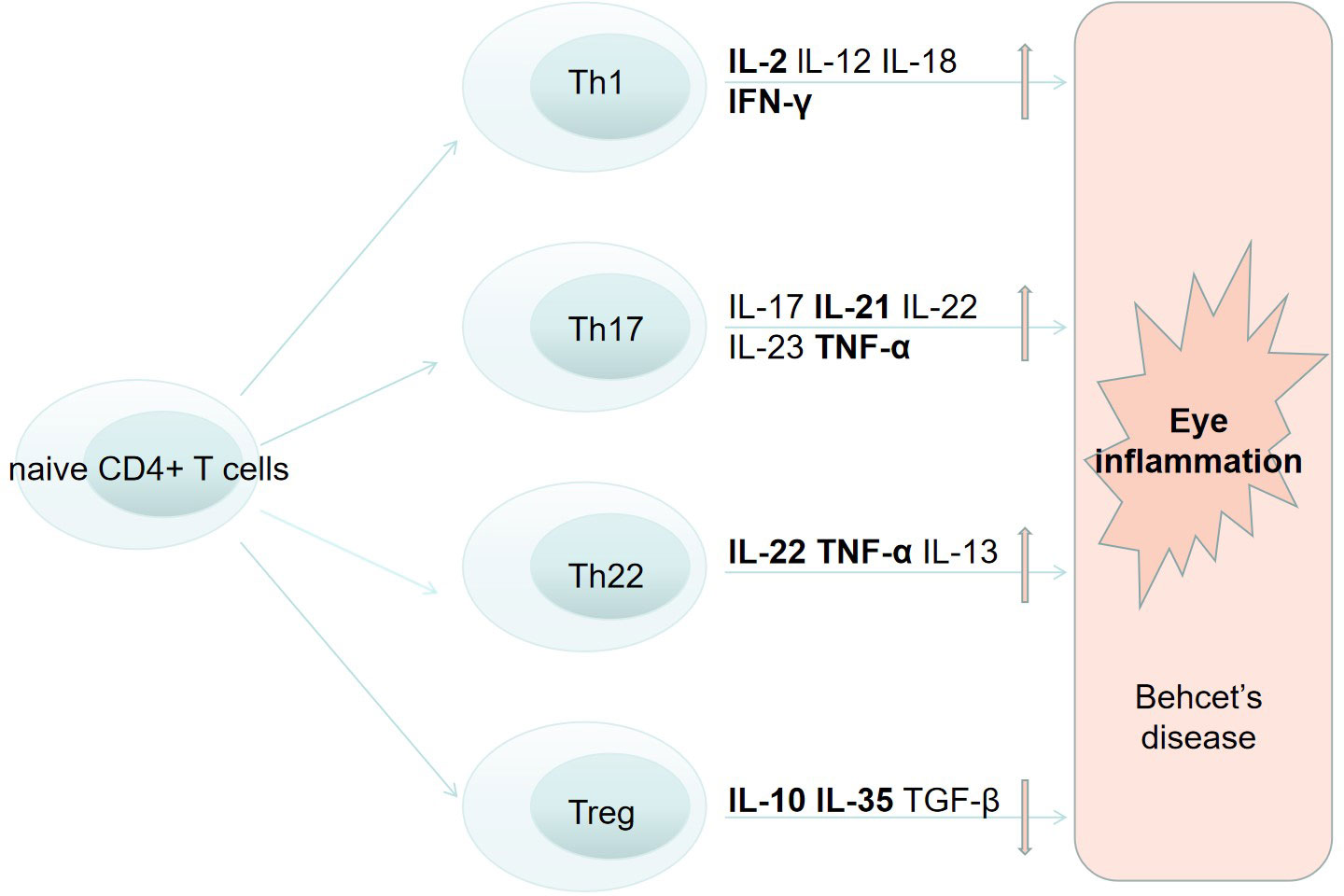
Figure 1 The role of T cells in the pathogenesis of Behcets disease and eye inflammation.
Th17 cells can regulate inflammation and autoimmunity by producing different cytokines, for example IL-17A, IL-17F, IL-21, IL-22, and IL-23 (92). According to previous investigations, higher expression of Th17 cells and relevant cytokines were found in active BD patients rather than inactive patients, as well as in the same patient of remission stage (93–95). IL-23, in cooperation with IL-6, is able to facilitate the differentiation, survival and maintenance of Th17 cells. By inducing pro-inflammatory cytokines production, IL-23 is capable of enhancing Th17 cell immune response (96). The IL-17/23 axis is believed to play a significant part in mediating inflammatory responses in BD (1). In addition, IL21 can stimulate Th17 differentiation and modulate Th1, Tregs and B cells (97). High titers of IL-21 were observed in PBMC from individuals with active BD. IL-21 and IL-2, produced by T lymphocytes in the retina, are also found to be associated with development of EAU (98). These findings suggests that Th17 pathway may be correlated with BD uveitis (Figure 1).
Th22 cells are differentiated from activated naive CD4+ T cells in the presence of IL-6 and TNF-α. Th22 cells not only secrete pro-inflammatory cytokines like IL-22 and TNF-α, but also express chemokine receptors such as CCR4, CCR6, and CCR10 (99). Th22-type T lymphocyte clones were constructed by researchers from ocular samples of active uveitis in BD patients (100). These clones secreted a great number of IL-22 and TNF-α (Figure 1). With the treatment of anti-TNF-α and anti-IL-6 agents, theses clones failed to produce IL-22. Moreover, large quantities of IL-22 were produced by intraocular T cells from EAU animal models of BD with retinal antigens. Higher IL-22 was also found in the supernatant of stimulated PBMCs in active Behcet’s uveitis patients compared to BD patients without eye involvement or in healthy controls (101). And the association between IL-22 level and severity of retinal vasculitis and anterior chamber inflammation was also reported.
Treg cells are able to produce immunosuppressive cytokines including IL-10, IL-35, and TGF-β and are vital in regulating immune responses (Figure 1). However, conflicting results of Treg cells levels were found in different studies with BD. Some studies found increased Tregs in peripheral blood and CSF (102), while others found decreased Tregs (97). Recent studies have reported abnormal expression of IL-35 in EAU, functional analysis suggested that IL-35 play an important part in the onset and development of EAU as well (103).
Proinflammatory cytokines in BD patients mainly include IL-1, IL-6, and TNF-α and are increased in BD patients (104). These inflammatory cytokines have also been observed in ocular tissue of BD patients and inflammation was induced in animal models after intraocular injection (104). Accumulating findings suggested that these cytokines are major inflammatory mediators participated in the development BD and may be promising targets for treatment.
Anti-inflammatory cytokines in BD mainly include IL-37, IL-27 and IL-10. Recent studies found decreased IL-37 levels in BD patients, and functional analysis suggested a negative correlation between IL-37 expression and BD development (105, 106). IL-27 is able to inhibit EAU by inhibiting Th17 cells proliferation and inducing the production of IL-10 (107–109). And the expression level of IL-27 was lower in active BD cases in comparison with controls. Decreased levels of anti-inflammatory cytokines are associated with BD development and their association with BD ocular involvement needs further investigation.
Traditional treatment measures of BD ocular involvement include topical or systemic administration of glucocorticoid and conventional immunosuppressors such as Azathioprine (AZA), Cyclosporine A (CYC) and Tacrolimus. With the occurrence of emerging biological agents, visual outcomes and prognoses of patients have greatly improved during the past few decades.
IFN-α was the first biological agent applied to treat BD due to its anti-viral function against HSV 1 (110). In vitro studies have indicated that IFN-α can lower peripheral γδT cells and impede T cell attachment to endothelial cells (111, 112). IFN-α-2a, as well as azathioprine, cyclosporine-A and monoclonal anti-TNF antibodies,has been considered as choices for BD patients with inflammatory eye disease affecting the posterior segment according to EULAR recommendations in 2018 (6). Moreover, treatment with high-dose glucocorticoids, infliximab or IFN-α were also recommended in patients with an acute sight-threatening uveitis (6). Several retrospective and prospective studies have shown that IFN-α-2a presented effectiveness in severe Behcet’s uveitis or uveitis refractory to conventional immunosuppressive medications (113–125). Treatment of IFN-α-2a can improve or stabilize visual acuity and achieve long-lasting remission of BD, even in some patients discontinued treatment (125–127).
TNF-α antagonists can be classified as monoclonal antibody and soluble receptor. Infliximab, adalimumab, and golimumab belong to the former group whereas etanercept belongs to the latter. Anti-TNF-α therapy possess a fast curative effect on all the clinical symptoms of BD and have also been widely used in severe or refractory Behcet’s uveitis (128–130). Rapid remission of uveitis could be gained after one day while benefit for visual acuity could be achieved within one week. Infliximab and adalimumab are regarded as first-line immunosuppressive agents to treat ocular diseases in BD. In patients who failed treatment using a first TNF-α inhibitor, switching to a different anti-TNF-α biologic should be taken into consideration.
Patients with short disease duration (<18 months) showed better visual effect when treated with infliximab, possibly due to decreased background vascular leakage before permanent eye injury occurs (131). Earlier initiation of infliximab may improve the outcome of Behcet’s uveitis (132). Short-term efficacy of infliximab in Behcet’s uveitis treatment has been well elucidated in many studies (133, 134). However, several factors are limiting the use of infliximab, including its high costs, side effects and lack of efficacy. A discontinuation of infliximab was reported in 15% patients in a recent study (135).
Adalimumab is also recommended in severe, intractable BD uveitis, including patients who are resistant to infliximab treatment, and has shown significant benefit in vision, reduction use of corticosteroid and immunosuppressors, and long-term remission (136). A retrospective study found equivalent efficacy of infliximab versus adalimumab (with response rate of 95-97%) in treatment of BD uveitis, and the rates of complete response or event-free survival showed no significant difference (137). A multicenter retrospective observational study was conducted in Behcet’s uveitis patients to evaluate the efficacy and safety of adalimumab (138). This study found significantly reduction of ocular inflammatory flares at 12-months follow-up, as well as significant improvement of best corrected visual acuity, and reduction of macular thickness and vasculitis occurrence during follow up. Randomized clinical trials towards adalimumab were conducted in non-infectious uveitis including BD patients with inadequate control by steroids (VISUAL I, VISUAL II, and VISUAL III), and the efficacy of adalimumab was observed with a reduced risk of optical activity and visual damage (139–141).
Golimumab appears to have potent efficacy for Behcet’s uveitis patients (142). But related evidence is still inefficient and more studies are needed to better estimate the long-term efficacy and safety of the ocular involvement.
Application of etanercept in Behcet’s uveitis were marginally reported in case reports and small series (143–145). Etanercept may be considered for uveitis in BD patients intolerant to infliximab or adalimumab.
More and more researches have demonstrated the application of bio-agents targeting interleukins and related receptors, including IL-1 blocker, IL-6 blocker, IL-17 blocker, and a monoclonal antibody targeting IL-12/IL-23 (146, 147). A multicenter retrospective observational study, including 19 BD uveitis patients treated with IL-1 blockers anakinra and canakinumab, showed significant effectiveness, remission and decreased steroid dosages in ocular impairment (148). Effectiveness of IL-1 blockers for Behcet’s uveitis was also reported in other small-sample studies (149–151). Tocilizumab is a monoclonal anti-IL-6 antibody. A multicenter study including 11 BD uveitis patients who were refractory to conventional and biologic immunosuppressors showed a rapid and sustained improvement within all optical indicators after the use of tocilizumab (152). Other case reports also illustrated the efficacy of tocilizumab in treating refractory BD uveitis (153, 154). Secukinumab is a human monoclonal anti-IL-17 antibody. It has been reported to inhibit eye inflammation in active non-infectious uveitis patients (155). However, a multicenter RCT including 118 Behcet uveitis patients found no significant effectiveness in the recurrence of uveitis compared with placebo control groups, in which high doses of concomitant immunosuppressive drugs were used in both groups (156). Additional studies are desired to better understand the efficacy and safety of secukinumab in Behcet’s uveitis. Ustekinumab is an inhibitor targeting IL-12/IL-23, and was reported to effectively suppress ocular inflammation in BD patients (157–159).
Experts have recommended the use of infliximab, etanercept, and adalimumab in pregnant women, with a FDA category B where reproduction researches in animal models did not observe risk to the fetus and data in pregnant women are not enough or well-established (160). Infliximab, an IgG1 antibody, will transfer the placenta during the second and third trimesters of pregnancy and can be detected in infant’s blood for months after birth (161–164). Evidence from more than 300 pregnancies suggested that infliximab has low fetal risk and is compatible with use within conception and the first two trimesters (165). Consideration should be taken in discontinuation of infliximab early in the third trimester or at the end of the second trimester in order to reduce late fetal exposure to the full extent (165). In addition, in 2020 ACR recommended continuing TNF-α antagonists therapy with infliximab, etanercept, adalimumab, or golimumab in the first two trimesters, and discontinuation should be considered in the third trimester (166–168). However, evidence mentioned above were mainly from Crohn’s disease, rheumatoid arthritis and systemic lupus erythematosus patients. More data about efficacy and safety are needed focusing on BD patients with ocular involvement.
BD is a chronic multi-systemic disease featured by relapsing-remitting systemic manifestations. Ocular involvements are quite common in BD and may cause severe tissue damage and lead to poor prognosis. Even though the mechanisms of BD remains unclear, advances in genetic and immunological fields have improved our understanding of the immunopathogenesis of BD ocular involvements. Environmental triggers are suggested to be implicated in the pathogenesis of BD in patients with genetic susceptibility. Abnormal autoantigens including HSP60, retinal S-antigen and IRBP might play important parts in ocular BD development via cross reaction. HLAB51 allele accounts for about 19% of the genetic susceptibility and is the most powerful genetic factor in BD. Accumulating evidence have reported various genetic variants including HLA Related Genes (such as SNPs in ERAP1 and MICA gene) and genes outside the MHC region (such as SNPs in IL-10 gene, IL-12/23 gene and others) to be associated with ocular BD. In addition, activation of innate and adaptive immune responses and immunological aberrations were observed. NKT cells, γδT cells, Th cells, Treg cells and cytokines with different functions are assumed to play important roles in the development of BD ocular involvement and might be potential targets for treatment. Novel biotherapies such as IFN-α-2a, TNF-α antagonists and agents targeting interleukins and their receptors have gained increasing attention in recent years. They taget specific molecules in immune response and inflammation process and therefore suppress ocular inflammation in BD. They have shown significant effectiveness, improved remission and prognosis in ocular manifestations of BD. They may make up for the deficiency of conventional immunosuppressors and bring promising prospects for the management of ocular BD. Further studies including RCTs targeting novel bio-agents and mechanisms towards potentially new targets are needed. Finally, the management of BD patients with pregnancy are suggested with infliximab, etanercept, and adalimumab.
SL and ZX collected related research papers. SL, ZX and JF participated in the manuscript writing for this review. JF and ZL developed research plan and modified the draft. SL and ZX contributed equally in this research. BX gave directive opinions during revision and made great contribution, including revising the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor WS declared a shared parent affiliation with the author ZL at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tong B, Liu X, Xiao J, Su G. Immunopathogenesis of behcet's disease. Front Immunol (2019) 10:665. doi: 10.3389/fimmu.2019.00665
2. Takeuchi M, Mizuki N, Ohno S. Pathogenesis of non-infectious uveitis elucidated by recent genetic findings. Front Immunol (2021) 12:640473. doi: 10.3389/fimmu.2021.640473
3. Azizlerli G, Kose AA, Sarica R, Gul A, Tutkun IT, Kulac M, et al. Prevalence of behcet's disease in istanbul, Turkey. Int J Dermatol (2003) 42(10):803–6. doi: 10.1046/j.1365-4362.2003.01893.x
4. Okada AA. Behcet's disease: general concepts and recent advances. Curr Opin Ophthalmol (2006) 17(6):551–6. doi: 10.1097/01.icu.0000247411.59213.bb
5. Ksiaa I, Abroug N, Kechida M, Zina S, Jelliti B, Khochtali S, et al. Eye and behçet's disease. J Fr Ophtalmol (2019) 42(4):e133–e46. doi: 10.1016/j.jfo.2019.02.002
6. Hatemi G, Christensen R, Bang D, Bodaghi B, Celik AF, Fortune F, et al. update of the EULAR recommendations for the management of Behcet's syndrome. Ann Rheum Dis (2018) 77(6):808–18. doi: 10.1136/annrheumdis-2018-213225
7. Dundar SV, Gencalp U, Simsek H. Familial cases of Behcet's disease. Br J Dermatol (1985) 113(3):319–21. doi: 10.1111/j.1365-2133.1985.tb02084.x
8. Gul A, Inanc M, Ocal L, Aral O, Konice M. Familial aggregation of Behcet's disease in Turkey. Ann Rheum Dis (2000) 59(8):622–5. doi: 10.1136/ard.59.8.622
9. Ohno S, Aoki K, Sugiura S, Nakayama E, Itakura K, Aizawa M. Letter: HL-A5 and behcet's disease. Lancet (1973) 2(7842):1383–4. doi: 10.1016/S0140-6736(73)93343-6
10. Ohno S, Ohguchi M, Hirose S, Matsuda H, Wakisaka A, Aizawa M. Close association of HLA-Bw51 with Behcet's disease. Arch Ophthalmol (Chicago Ill 1960) (1982) 100(9):1455–8. doi: 10.1001/archopht.1982.01030040433013
11. Ersoy F, Berkel I, Firat T, Kazokoglu H. HLA antigens associated with Behcet's disease. Arch Dermatol (1977) 113(12):1720–1. doi: 10.1001/archderm.1977.01640120088021
12. Haim S, Gideoni O, Barzilai A. The histocompatibility antigens in patients with Behcet's disease. Acta Derm Venereol (1977) 57(3):243–5. doi: 10.2340/0001555557243245
13. Djawari D, Lang B, Hornstein OP. [HLA typing in patients of German origin with recurrent benign aphthosis and Behcet's disease]. Z Hautkr (1984) 59(15):1005–9.
14. Al-Rawi ZS, Sharquie KE, Khalifa SJ, Al-Hadithi FM, Munir JJ. Behcet's disease in Iraqi patients. Ann Rheum Dis (1986) 45(12):987–90. doi: 10.1136/ard.45.12.987
15. Lee S, Koh YJ, Kim DH, Bang D, Nam IW, Lee KH, et al. A study of HLA antigens in Behcet's syndrome. Yonsei Med J (1988) 29(3):259–62. doi: 10.3349/ymj.1988.29.3.259
16. Balboni A, Pivetti-Pezzi P, Orlando P, Rubini M, Selvatici R, Accorinti M, et al. Serological and molecular HLA typing in Italian Behcet's patients: significant association to B51-DR5-DQw3 haplotype. Tissue Antigens (1992) 39(3):141–3. doi: 10.1111/j.1399-0039.1992.tb01925.x
17. Mineshita S, Tian D, Wang LM, Jian XY, Li SY, Fang GZ, et al. Histocompatibility antigens associated with Behcet's disease in northern Han Chinese. Internal Med (Tokyo Japan) (1992) 31(9):1073–5. doi: 10.2169/internalmedicine.31.1073
18. Yabuki K, Ohno S, Mizuki N, Ando H, Tabbara KF, Goto K, et al. HLA class I and II typing of the patients with Behcet's disease in Saudi Arabia. Tissue Antigens (1999) 54(3):273–7. doi: 10.1034/j.1399-0039.1999.540308.x
19. Verity DH, Wallace GR, Vaughan RW, Kondeatis E, Madanat W, Zureikat H, et al. HLA and tumour necrosis factor (TNF) polymorphisms in ocular Behcet's disease. Tissue Antigens (1999) 54(3):264–72. doi: 10.1034/j.1399-0039.1999.540307.x
20. Yabuki K, Mizuki N, Ota M, Katsuyama Y, Palimeris G, Stavropoulos C, et al. Association of MICA gene and HLA-B*5101 with Behcet's disease in Greece. Invest Ophthalmol Visual Sci (1999) 40(9):1921–6.
21. Mizuki N, Ota M, Katsuyama Y, Yabuki K, Ando H, Yoshida M, et al. HLA class I genotyping including HLA-B*51 allele typing in the Iranian patients with Behcet's disease. Tissue Antigens (2001) 57(5):457–62. doi: 10.1034/j.1399-0039.2001.057005457.x
22. Munoz-Saa I, Cambra A, Pallares L, Espinosa G, Juan A, Pujalte F, et al. Allelic diversity and affinity variants of MICA are imbalanced in Spanish patients with Behcet's disease. Scandinavian J Immunol (2006) 64(1):77–82. doi: 10.1111/j.1365-3083.2006.01780.x
23. Gul A, Hajeer AH, Worthington J, Barrett JH, Ollier WE, Silman AJ. Evidence for linkage of the HLA-B locus in Behcet's disease, obtained using the transmission disequilibrium test. Arthritis Rheum (2001) 44(1):239–40. doi: 10.1002/1529-0131(200101)44:1<239::AID-ANR31>3.0.CO;2-X
24. Deng Y, Zhu W, Zhou X. Immune regulatory genes are major genetic factors to behcet disease: systematic review. Open Rheumatol J (2018) 12:70–85. doi: 10.2174/1874312901812010070
25. de Menthon M, Lavalley MP, Maldini C, Guillevin L, Mahr A. HLA-B51/B5 and the risk of Behcet's disease: a systematic review and meta-analysis of case-control genetic association studies. Arthritis Rheum (2009) 61(10):1287–96. doi: 10.1002/art.24642
26. Remmers EF, Cosan F, Kirino Y, Ombrello MJ, Abaci N, Satorius C, et al. Genome-wide association study identifies variants in the MHC class I, IL10, and IL23R-IL12RB2 regions associated with Behcet's disease. Nat Genet (2010) 42(8):698–702. doi: 10.1038/ng.625
27. Mizuki N, Meguro A, Ota M, Ohno S, Shiota T, Kawagoe T, et al. Genome-wide association studies identify IL23R-IL12RB2 and IL10 as Behcet's disease susceptibility loci. Nat Genet (2010) 42(8):703–6. doi: 10.1038/ng.624
28. Maldini C, Lavalley MP, Cheminant M, de Menthon M, Mahr A. Relationships of HLA-B51 or B5 genotype with Behcet's disease clinical characteristics: systematic review and meta-analyses of observational studies. Rheumatol (Oxford) (2012) 51(5):887–900. doi: 10.1093/rheumatology/ker428
29. Horie Y, Meguro A, Ohta T, Lee EB, Namba K, Mizuuchi K, et al. HLA-B51 Carriers are Susceptible to Ocular Symptoms of Behcet Disease and the Association between the Two Becomes Stronger towards the East along the Silk Road: A Literature Survey. Ocular Immunol Inflammation (2017) 25(1):37–40. doi: 10.3109/09273948.2015.1136422
30. Al-Okaily F, Al-Rashidi S, Al-Balawi M, Mustafa M, Arfin M, Al-Asmari A. Genetic association of HLA-A*26, -A*31, and -B*51 with behcet's disease in saudi patients. Clin Med Insights Arthritis Musculoskelet Disord (2016) 9:167–73. doi: 10.4137/CMAMD.S39879
31. Chung YM, Yeh TS, Sheu MM, Chen MS, Wen MS, Tsai HY, et al. [Behcet's disease with ocular involvement in Taiwan: a joint survey of six major ophthalmological departments]. J Formos Med Assoc (1990) 89(5):413–7.
32. Kamiishi T, Itoh Y, Meguro A, Nishida T, Sasaki S, Nanba K, et al. [Four-digit allele genotyping of HLA-A and HLA-B genes in Japanese patients with Behcet's disease (BD) by a PCR-SSOP-luminex method and stratification analysis according to each major symptom of BD]. Nippon Ganka Gakkai Zasshi (2008) 112(5):451–8.
33. Mizuki N, Inoko H, Ohno S. Molecular genetics (HLA) of Behcet's disease. Yonsei Med J (1997) 38(6):333–49. doi: 10.3349/ymj.1997.38.6.333
34. Nakamura J, Meguro A, Ishii G, Mihara T, Takeuchi M, Mizuki Y, et al. The association analysis between HLA-A*26 and Behcet's disease. Sci Rep (2019) 9(1):4426. doi: 10.1038/s41598-019-40824-y
35. Ombrello MJ, Kirino Y, de Bakker PI, Gul A, Kastner DL, Remmers EF. Behcet disease-associated MHC class I residues implicate antigen binding and regulation of cell-mediated cytotoxicity. Proc Natl Acad Sci USA (2014) 111(24):8867–72. doi: 10.1073/pnas.1406575111
36. Hughes T, Coit P, Adler A, Yilmaz V, Aksu K, Duzgun N, et al. Identification of multiple independent susceptibility loci in the HLA region in Behcet's disease. Nat Genet (2013) 45(3):319–24. doi: 10.1038/ng.2551
37. Kang EH, Kim JY, Takeuchi F, Kim JW, Shin K, Lee EY, et al. Associations between the HLA-A polymorphism and the clinical manifestations of Behcet's disease. Arthritis Res Ther (2011) 13(2):R49. doi: 10.1186/ar3292
38. Kang EH, Park JW, Park C, Yu HG, Lee EB, Park MH, et al. Genetic and non-genetic factors affecting the visual outcome of ocular Behcet's disease. Hum Immunol (2013) 74(10):1363–7. doi: 10.1016/j.humimm.2013.06.036
39. Giza M, Koftori D, Chen L, Bowness P. Is Behcet's disease a 'class 1-opathy'? The role of HLA-B*51 in the pathogenesis of Behcet's disease. Clin Exp Immunol (2018) 191(1):11–8. doi: 10.1111/cei.13049
40. Kaburaki T, Takamoto M, Numaga J, Kawashima H, Araie M, Ohnogi Y, et al. Genetic association of HLA-A*2601 with ocular Behcet's disease in Japanese patients. Clin Exp Rheumatol (2010) 28(4 Suppl 60):S39–44.
41. Meguro A, Inoko H, Ota M, Katsuyama Y, Oka A, Okada E, et al. Genetics of Behcet disease inside and outside the MHC. Ann Rheum Dis (2010) 69(4):747–54. doi: 10.1136/ard.2009.108571
42. Mizuki N, Ohno S, Ando H, Chen L, Palimeris GD, Stavropoulos-Ghiokas E, et al. A strong association between HLA-B*5101 and Behcet's disease in Greek patients. Tissue Antigens (1997) 50(1):57–60. doi: 10.1111/j.1399-0039.1997.tb02835.x
43. Montes-Cano MA, Conde-Jaldon M, Garcia-Lozano JR, Ortiz-Fernandez L, Ortego-Centeno N, Castillo-Palma MJ, et al. HLA and non-HLA genes in Behcet's disease: a multicentric study in the Spanish population. Arthritis Res Ther (2013) 15(5):R145. doi: 10.1186/ar4328
44. Ortiz-Fernandez L, Carmona FD, Montes-Cano MA, Garcia-Lozano JR, Conde-Jaldon M, Ortego-Centeno N, et al. Genetic analysis with the immunochip platform in behcet disease. Identification of residues associated in the HLA class I region and new susceptibility loci. PloS One (2016) 11(8):e0161305. doi: 10.1371/journal.pone.0161305
45. Takeuchi M, Kastner DL, Remmers EF. The immunogenetics of Behcet's disease: A comprehensive review. J Autoimmun (2015) 64:137–48. doi: 10.1016/j.jaut.2015.08.013
46. Yılmaz MA, Türsen Ü. The immunogenetics of behcet's disease. Adv Exp Med Biol (2022) 1367:335–47. doi: 10.1007/978-3-030-92616-8_12
47. Amirzargar A, Shahram F, Nikoopour E, Rezaei N, Saeedfar K, Ziaei N, et al. Proinflammatory cytokine gene polymorphisms in Behcet's disease. Eur Cytokine network (2010) 21(4):292–6. doi: 10.1684/ecn.2009.0209
48. Rock KL, York IA, Goldberg AL. Post-proteasomal antigen processing for major histocompatibility complex class I presentation. Nat Immunol (2004) 5(7):670–7. doi: 10.1038/ni1089
49. Kirino Y, Bertsias G, Ishigatsubo Y, Mizuki N, Tugal-Tutkun I, Seyahi E, et al. Genome-wide association analysis identifies new susceptibility loci for Behcet's disease and epistasis between HLA-B*51 and ERAP1. Nat Genet (2013) 45(2):202–7. doi: 10.1038/ng.2520
50. Groh V, Steinle A, Bauer S, Spies T. Recognition of stress-induced MHC molecules by intestinal epithelial gammadelta T cells. Science (1998) 279(5357):1737–40. doi: 10.1126/science.279.5357.1737
51. Wei F, Zhang YU, Li W. A meta-analysis of the association between Behcet's disease and MICA-A6. BioMed Rep (2016) 4(6):741–5. doi: 10.3892/br.2016.644
52. Mizuki N, Ota M, Kimura M, Ohno S, Ando H, Katsuyama Y, et al. Triplet repeat polymorphism in the transmembrane region of the MICA gene: a strong association of six GCT repetitions with Behcet disease. Proc Natl Acad Sci USA (1997) 94(4):1298–303. doi: 10.1073/pnas.94.4.1298
53. Park SH, Park KS, Seo YI, Min DJ, Kim WU, Kim TG, et al. Association of MICA polymorphism with HLA-B51 and disease severity in Korean patients with Behcet's disease. J Korean Med Sci (2002) 17(3):366–70. doi: 10.3346/jkms.2002.17.3.366
54. Ozbey U, Tug E, Namli M. Interleukin-10 gene promoter polymorphism in patients with schizophrenia in a region of East Turkey. World J Biol Psychiatry (2009) 10(4 Pt 2):461–8. doi: 10.1080/15622970802626580
55. Wallace GR, Kondeatis E, Vaughan RW, Verity DH, Chen Y, Fortune F, et al. IL-10 genotype analysis in patients with Behcet's disease. Hum Immunol (2007) 68(2):122–7. doi: 10.1016/j.humimm.2006.11.010
56. Dilek K, Ozcimen AA, Saricaoglu H, Saba D, Yucel A, Yurtkuran M, et al. Cytokine gene polymorphisms in Behcet's disease and their association with clinical and laboratory findings. Clin Exp Rheumatol (2009) 27(2 Suppl 53):S73–8.
57. Afkari B, Babaloo Z, Dolati S, Khabazi A, Jadidi-Niaragh F, Talei M, et al. Molecular analysis of interleukin-10 gene polymorphisms in patients with Behcet's disease. Immunol Lett (2018) 194:56–61. doi: 10.1016/j.imlet.2017.12.008
58. Hu J, Hou S, Zhu X, Fang J, Zhou Y, Liu Y, et al. Interleukin-10 gene polymorphisms are associated with Behcet's disease but not with Vogt-Koyanagi-Harada syndrome in the Chinese Han population. Mol Vis (2015) 21:589–603.
59. Wu Z, Zheng W, Xu J, Sun F, Chen H, Li P, et al. IL10 polymorphisms associated with Behcet's disease in Chinese Han. Hum Immunol (2014) 75(3):271–6. doi: 10.1016/j.humimm.2013.11.009
60. Jiang Z, Yang P, Hou S, Du L, Xie L, Zhou H, et al. IL-23R gene confers susceptibility to Behcet's disease in a Chinese Han population. Ann Rheum Dis (2010) 69(7):1325–8. doi: 10.1136/ard.2009.119420
61. Takeuchi M, Mizuki N, Meguro A, Ombrello MJ, Kirino Y, Satorius C, et al. Dense genotyping of immune-related loci implicates host responses to microbial exposure in Behcet's disease susceptibility. Nat Genet (2017) 49(3):438–43. doi: 10.1038/ng.3786
62. Pineton de Chambrun M, Wechsler B, Geri G, Cacoub P, Saadoun D. New insights into the pathogenesis of Behcet's disease. Autoimmun Rev (2012) 11(10):687–98. doi: 10.1016/j.autrev.2011.11.026
63. Sohn S, Lee ES, Bang D, Lee S. Behcet's disease-like symptoms induced by the Herpes simplex virus in ICR mice. Eur J Dermatol EJD (1998) 8(1):21–3.
64. Shim J, Byun HO, Lee YD, Lee ES, Sohn S. Interleukin-6 small interfering RNA improved the herpes simplex virus-induced systemic inflammation in vivo Behcet's disease-like mouse model. Gene Ther (2009) 16(3):415–25. doi: 10.1038/gt.2008.180
65. Amoura Z, Guillaume M, Caillat-Zucman S, Wechsler B, Piette JC. [Pathophysiology of behcet's disease]. La Rev medecine interne (2006) 27(11):843–53. doi: 10.1016/j.revmed.2006.02.014
66. Pervin K, Childerstone A, Shinnick T, Mizushima Y, van der Zee R, Hasan A, et al. T cell epitope expression of mycobacterial and homologous human 65-kilodalton heat shock protein peptides in short term cell lines from patients with Behcet's disease. J Immunol (Baltimore Md 1950) (1993) 151(4):2273–82. doi: 10.4049/jimmunol.151.4.2273
67. Hu W, Hasan A, Wilson A, Stanford MR, Li-Yang Y, Todryk S, et al. Experimental mucosal induction of uveitis with the 60-kDa heat shock protein-derived peptide 336-351. Eur J Immunol (1998) 28(8):2444–55. doi: 10.1002/(SICI)1521-4141(199808)28:08<2444::AID-IMMU2444>3.0.CO;2-N
68. Uchio E, Stanford M, Hasan A, Satoh S, Ohno S, Shinnick T, et al. HSP-derived peptides inducing uveitis and IgG and IgA antibodies. Exp Eye Res (1998) 67(6):719–27. doi: 10.1006/exer.1998.0574
69. Kaneko F, Togashi A, Saito S, Sakuma H, Oyama N, Nakamura K, et al. Behcet's disease (Adamantiades-Behcet's disease). Clin Dev Immunol (2011) 2011:681956. doi: 10.1155/2011/681956
70. Takeuchi M, Usui Y, Okunuki Y, Zhang L, Ma J, Yamakawa N, et al. Immune responses to interphotoreceptor retinoid-binding protein and S-antigen in Behcet's patients with uveitis. Invest Ophthalmol Visual Sci (2010) 51(6):3067–75. doi: 10.1167/iovs.09-4313
71. Zhao C, Yang P, He H, Lin X, Li B, Zhou H, et al. S-antigen specific T helper type 1 response is present in Behcet's disease. Mol Vis (2008) 14:1456–64.
72. Pay S, Simsek I, Erdem H, Dinc A. Immunopathogenesis of Behcet's disease with special emphasize on the possible role of antigen presenting cells. Rheumatol Int (2007) 27(5):417–24. doi: 10.1007/s00296-006-0281-6
73. Adamus G, Chan CC. Experimental autoimmune uveitides: multiple antigens, diverse diseases. Int Rev Immunol (2002) 21(2-3):209–29. doi: 10.1080/08830180212068
74. Wiggert B, Kutty G, Long KO, Inouye L, Gery I, Chader GJ, et al. Interphotoreceptor retinoid-binding protein (IRBP) in progressive rod-cone degeneration (prcd)–biochemical, immunocytochemical and immunologic studies. Exp Eye Res (1991) 53(3):389–98. doi: 10.1016/0014-4835(91)90245-A
75. Caspi RR, Roberge FG, Chan CC, Wiggert B, Chader GJ, Rozenszajn LA, et al. A new model of autoimmune disease. Experimental autoimmune uveoretinitis induced in mice with two different retinal antigens. J Immunol (Baltimore Md 1950) (1988) 140(5):1490–5.
76. Dua HS, Abrams M, Barrett JA, Gregerson DS, Forrester JV, Donoso LA. Epitopes and idiotypes in experimental autoimmune uveitis: a review. Curr Eye Res (1992) 11 Suppl:59–65. doi: 10.3109/02713689208999512
77. Donoso LA, Merryman CF, Sery TW, Vrabec T, Arbizo V, Fong SL. Human IRBP: characterization of uveitopathogenic sites. Curr Eye Res (1988) 7(11):1087–95. doi: 10.3109/02713688809001879
78. Kimura MY, Nakayama T. Differentiation of NK1 and NK2 cells. Crit Rev Immunol (2005) 25(5):361–74. doi: 10.1615/CritRevImmunol.v25.i5.20
79. Hasan MS, Ryan PL, Bergmeier LA, Fortune F. Circulating NK cells and their subsets in Behcet's disease. Clin Exp Immunol (2017) 188(2):311–22. doi: 10.1111/cei.12939
80. Ahn JK, Chung H, Lee DS, Yu YS, Yu HG. CD8brightCD56+ T cells are cytotoxic effectors in patients with active Behcet's uveitis. J Immunol (Baltimore Md 1950) (2005) 175(9):6133–42. doi: 10.4049/jimmunol.175.9.6133
81. Kitaichi N, Kotake S, Morohashi T, Onoé K, Ohno S, Taylor AW. Diminution of experimental autoimmune uveoretinitis (EAU) in mice depleted of NK cells. J leukocyte Biol (2002) 72(6):1117–21. doi: 10.1189/jlb.72.6.1117
82. Yamaguchi Y, Takahashi H, Satoh T, Okazaki Y, Mizuki N, Takahashi K, et al. Natural killer cells control a T-helper 1 response in patients with Behcet's disease. Arthritis Res Ther (2010) 12(3):R80. doi: 10.1186/ar3005
83. Freysdottir J, Hussain L, Farmer I, Lau SH, Fortune F. Diversity of gammadelta T cells in patients with Behcet's disease is indicative of polyclonal activation. Oral Dis (2006) 12(3):271–7. doi: 10.1111/j.1601-0825.2005.01185.x
84. Accardo-Palumbo A, Giardina AR, Ciccia F, Ferrante A, Principato A, Impastato R, et al. Phenotype and functional changes of Vgamma9/Vdelta2 T lymphocytes in Behcet's disease and the effect of infliximab on Vgamma9/Vdelta2 T cell expansion, activation and cytotoxicity. Arthritis Res Ther (2010) 12(3):R109. doi: 10.1186/ar3043
85. Bank I, Duvdevani M, Livneh A. Expansion of gammadelta T-cells in Behcet's disease: role of disease activity and microbial flora in oral ulcers. J Lab Clin Med (2003) 141(1):33–40. doi: 10.1067/mlc.2003.1
86. Verjans GM, van Hagen PM, van der Kooi A, Osterhaus AD, Baarsma GS. Vgamma9Vdelta2 T cells recovered from eyes of patients with Behcet's disease recognize non-peptide prenyl pyrophosphate antigens. J neuroimmunology (2002) 130(1-2):46–54. doi: 10.1016/S0165-5728(02)00208-4
87. Lafont V, Liautard J, Sable-Teychene M, Sainte-Marie Y, Favero J. Isopentenyl pyrophosphate, a mycobacterial non-peptidic antigen, triggers delayed and highly sustained signaling in human gamma delta T lymphocytes without inducing eown-modulation of T cell antigen receptor. J Biol Chem (2001) 276(19):15961–7. doi: 10.1074/jbc.M008684200
88. Nian H, Shao H, O'Brien RL, Born WK, Kaplan HJ, Sun D. Activated gammadelta T cells promote the activation of uveitogenic T cells and exacerbate EAU development. Invest Ophthalmol Visual Sci (2011) 52(8):5920–7. doi: 10.1167/iovs.10-6758
89. Aridogan BC, Yildirim M, Baysal V, Inaloz HS, Baz K, Kaya S. Serum levels of IL-4, IL-10, IL-12, IL-13 and IFN-gamma in behcet's disease. J Dermatol (2003) 30(8):602–7. doi: 10.1111/j.1346-8138.2003.tb00442.x
90. Ahn JK, Yu HG, Chung H, Park YG. Intraocular cytokine environment in active Behcet uveitis. Am J Ophthalmol (2006) 142(3):429–34. doi: 10.1016/j.ajo.2006.04.016
91. El-Asrar AM, Struyf S, Kangave D, Al-Obeidan SS, Opdenakker G, Geboes K, et al. Cytokine profiles in aqueous humor of patients with different clinical entities of endogenous uveitis. Clin Immunol (Orlando Fla) (2011) 139(2):177–84. doi: 10.1016/j.clim.2011.01.014
92. Singh RP, Hasan S, Sharma S, Nagra S, Yamaguchi DT, Wong DT, et al. Th17 cells in inflammation and autoimmunity. Autoimmun Rev (2014) 13(12):1174–81. doi: 10.1016/j.autrev.2014.08.019
93. Chi W, Zhu X, Yang P, Liu X, Lin X, Zhou H, et al. Upregulated IL-23 and IL-17 in Behcet patients with active uveitis. Invest Ophthalmol Visual Sci (2008) 49(7):3058–64. doi: 10.1167/iovs.07-1390
94. Nanke Y, Yago T, Kotake S. The role of th17 cells in the pathogenesis of behcet's disease. J Clin Med (2017) 6(7). doi: 10.3390/jcm6070074
95. Hamzaoui K, Bouali E, Ghorbel I, Khanfir M, Houman H, Hamzaoui A. Expression of th-17 and RORgammat mRNA in behcet's disease. Med Sci Monit (2011) 17(4):CR227–34. doi: 10.12659/MSM.881720
96. Zhou L, Ivanov II, Spolski R, Min R, Shenderov K, Egawa T, et al. IL-6 programs T(H)-17 cell differentiation by promoting sequential engagement of the IL-21 and IL-23 pathways. Nat Immunol (2007) 8(9):967–74. doi: 10.1038/ni1488
97. Geri G, Terrier B, Rosenzwajg M, Wechsler B, Touzot M, Seilhean D, et al. Critical role of IL-21 in modulating TH17 and regulatory T cells in Behcet disease. J Allergy Clin Immunol (2011) 128(3):655–64. doi: 10.1016/j.jaci.2011.05.029
98. Wang L, Yu CR, Kim HP, Liao W, Telford WG, Egwuagu CE, et al. Key role for IL-21 in experimental autoimmune uveitis. Proc Natl Acad Sci U.S.A. (2011) 108(23):9542–7. doi: 10.1073/pnas.1018182108
99. Duhen T, Geiger R, Jarrossay D, Lanzavecchia A, Sallusto F. Production of interleukin 22 but not interleukin 17 by a subset of human skin-homing memory T cells. Nat Immunol (2009) 10(8):857–63. doi: 10.1038/ni.1767
100. Sugita S, Kawazoe Y, Imai A, Kawaguchi T, Horie S, Keino H, et al. Role of IL-22- and TNF-alpha-producing Th22 cells in uveitis patients with Behcet's disease. J Immunol (Baltimore Md 1950) (2013) 190(11):5799–808. doi: 10.4049/jimmunol.1202677
101. Cai T, Wang Q, Zhou Q, Wang C, Hou S, Qi J, et al. Increased expression of IL-22 is associated with disease activity in Behcet's disease. PloS One (2013) 8(3):e59009. doi: 10.1371/journal.pone.0059009
102. Hamzaoui K, Borhani Haghighi A, Ghorbel IB, Houman H. RORC and Foxp3 axis in cerebrospinal fluid of patients with neuro-Behcet's disease. J neuroimmunology (2011) 233(1-2):249–53. doi: 10.1016/j.jneuroim.2011.01.012
103. Su LC, Liu XY, Huang AF, Xu WD. Emerging role of IL-35 in inflammatory autoimmune diseases. Autoimmun Rev (2018) 17(7):665–73. doi: 10.1016/j.autrev.2018.01.017
104. Wakefield D, Lloyd A. The role of cytokines in the pathogenesis of inflammatory eye disease. Cytokine (1992) 4(1):1–5. doi: 10.1016/1043-4666(92)90028-P
105. Xu WD, Zhao Y, Liu Y. Insights into IL-37, the role in autoimmune diseases. Autoimmun Rev (2015) 14(12):1170–5. doi: 10.1016/j.autrev.2015.08.006
106. Bouali E, Kaabachi W, Hamzaoui A, Hamzaoui K. Interleukin-37 expression is decreased in Behcet's disease and is associated with inflammation. Immunol Lett (2015) 167(2):87–94. doi: 10.1016/j.imlet.2015.08.001
107. Amadi-Obi A, Yu CR, Liu X, Mahdi RM, Clarke GL, Nussenblatt RB, et al. TH17 cells contribute to uveitis and scleritis and are expanded by IL-2 and inhibited by IL-27/STAT1. Nat Med (2007) 13(6):711–8. doi: 10.1038/nm1585
108. Fitzgerald DC, Zhang GX, El-Behi M, Fonseca-Kelly Z, Li H, Yu S, et al. Suppression of autoimmune inflammation of the central nervous system by interleukin 10 secreted by interleukin 27-stimulated T cells. Nat Immunol (2007) 8(12):1372–9. doi: 10.1038/ni1540
109. Lee YS, Amadi-Obi A, Yu CR, Egwuagu CE. Retinal cells suppress intraocular inflammation (uveitis) through production of interleukin-27 and interleukin-10. Immunology (2011) 132(4):492–502. doi: 10.1111/j.1365-2567.2010.03379.x
110. Pipitone N, Olivieri I, Cantini F, Triolo G, Salvarani C. New approaches in the treatment of Adamantiades-Behcet's disease. Curr Opin Rheumatol (2006) 18(1):3–9. doi: 10.1097/01.bor.0000197995.27579.9b
111. Evereklioglu C. Current concepts in the etiology and treatment of Behcet disease. Survey Ophthalmol (2005) 50(4):297–350. doi: 10.1016/j.survophthal.2005.04.009
112. Treusch M, Vonthein R, Baur M, Gunaydin I, Koch S, Stubiger N, et al. Influence of human recombinant interferon-alpha2a (rhIFN-alpha2a) on altered lymphocyte subpopulations and monocytes in Behcet's disease. Rheumatol (Oxford) (2004) 43(10):1275–82. doi: 10.1093/rheumatology/keh311
113. Yalçindağ FN, Uzun A. Results of interferon alpha-2a therapy in patients with Behcet's disease. J ocular Pharmacol Ther Off J Assoc Ocular Pharmacol Ther (2012) 28(4):439–43. doi: 10.1089/jop.2011.0238
114. Aydinoglu-Candan Ö, Araz-Erşan B, Gul A, Badur S, Tugal-Tutkun I. Anti-interferon alpha antibodies and autoantibodies in patients with Behçet's disease uveitis treated with recombinant human interferon alpha-2a. Graefe's Arch Clin Exp Ophthalmol = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie (2015) 253(3):457–65. doi: 10.1007/s00417-014-2856-3
115. Hatemi G, Seyahi E, Fresko I, Talarico R, Hamuryudan V. One year in review 2017: Behçet's syndrome. Clin Exp Rheumatol (2017) 35 Suppl 108(6):3–15.
116. Wechsler B, Bodaghi B, Huong DL, Fardeau C, Amoura Z, Cassoux N, et al. Efficacy of interferon alfa-2a in severe and refractory uveitis associated with Behcet's disease. Ocular Immunol Inflammation (2000) 8(4):293–301. doi: 10.1076/ocii.8.4.293.6453
117. Calguneri M, Ozturk MA, Ertenli I, Kiraz S, Apras S, Ozbalkan Z. Effects of interferon alpha treatment on the clinical course of refractory Behcet's disease: an open study. Ann Rheum Dis (2003) 62(5):492–3. doi: 10.1136/ard.62.5.492
118. Krause L, Turnbull JR, Torun N, Pleyer U, Zouboulis CC, Foerster MH. Interferon alfa-2a in the treatment of ocular Adamantiades-Behcet's disease. Adv Exp Med Biol (2003) 528:511–9. doi: 10.1007/0-306-48382-3_103
119. Kotter I, Zierhut M, Eckstein A, Vonthein R, Ness T, Gunaydin I, et al. Human recombinant interferon-alpha2a (rhIFN alpha2a) for the treatment of Behcet's disease with sight-threatening retinal vasculitis. Adv Exp Med Biol (2003) 528:521–3. doi: 10.1007/0-306-48382-3_104
120. Tugal-Tutkun I, Guney-Tefekli E, Urgancioglu M. Results of interferon-alfa therapy in patients with Behcet uveitis. Graefe's Arch Clin Exp Ophthalmol = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie (2006) 244(12):1692–5. doi: 10.1007/s00417-006-0346-y
121. Bodaghi B, Gendron G, Wechsler B, Terrada C, Cassoux N, Huong du LT, et al. Efficacy of interferon alpha in the treatment of refractory and sight threatening uveitis: a retrospective monocentric study of 45 patients. Br J Ophthalmol (2007) 91(3):335–9. doi: 10.1136/bjo.2006.101550
122. Gueudry J, Wechsler B, Terrada C, Gendron G, Cassoux N, Fardeau C, et al. Long-term efficacy and safety of low-dose interferon alpha2a therapy in severe uveitis associated with Behcet disease. Am J Ophthalmol (2008) 146(6):837–44 e1. doi: 10.1016/j.ajo.2008.08.038
123. Sobaci G, Erdem U, Durukan AH, Erdurman C, Bayer A, Koksal S, et al. Safety and effectiveness of interferon alpha-2a in treatment of patients with Behcet's uveitis refractory to conventional treatments. Ophthalmology (2010) 117(7):1430–5. doi: 10.1016/j.ophtha.2009.11.022
124. Deuter CM, Zierhut M, Mohle A, Vonthein R, Stobiger N, Kotter I. Long-term remission after cessation of interferon-alpha treatment in patients with severe uveitis due to Behcet's disease. Arthritis Rheum (2010) 62(9):2796–805. doi: 10.1002/art.27581
125. Onal S, Kazokoglu H, Koc A, Akman M, Bavbek T, Direskeneli H, et al. Long-term efficacy and safety of low-dose and dose-escalating interferon alfa-2a therapy in refractory Behçet uveitis. Arch Ophthalmol (Chicago Ill 1960) (2011) 129(3):288–94. doi: 10.1001/archophthalmol.2011.3
126. Hasanreisoglu M, Cubuk MO, Ozdek S, Gurelik G, Aktas Z, Hasanreisoglu B. Interferon alpha-2a therapy in patients with refractory behçet uveitis. Ocular Immunol Inflammation (2017) 25(1):71–5. doi: 10.3109/09273948.2015.1133835
127. Diwo E, Gueudry J, Saadoun D, Weschler B, LeHoang P, Bodaghi B. Long-term efficacy of interferon in severe uveitis associated with behçet disease. Ocular Immunol Inflammation (2017) 25(1):76–84. doi: 10.1080/09273948.2016.1206204
128. Arida A, Fragiadaki K, Giavri E, Sfikakis PP. Anti-TNF agents for Behcet's disease: analysis of published data on 369 patients. Semin Arthritis rheumatism (2011) 41(1):61–70. doi: 10.1016/j.semarthrit.2010.09.002
129. Yamada Y, Sugita S, Tanaka H, Kamoi K, Kawaguchi T, Mochizuki M. Comparison of infliximab versus ciclosporin during the initial 6-month treatment period in Behcet disease. Br J Ophthalmol (2010) 94(3):284–8. doi: 10.1136/bjo.2009.158840
130. Vallet H, Riviere S, Sanna A, Deroux A, Moulis G, Addimanda O, et al. Efficacy of anti-TNF alpha in severe and/or refractory Behcet's disease: Multicenter study of 124 patients. J Autoimmun (2015) 62:67–74. doi: 10.1016/j.jaut.2015.06.005
131. Keino H, Okada AA, Watanabe T, Nakayama M, Nakamura T. Efficacy of infliximab for early remission induction in refractory uveoretinitis associated with behcet disease: A 2-year follow-up study. Ocular Immunol Inflamm (2017) 25(1):46–51. doi: 10.1080/09273948.2016.1239746
132. Guzelant G, Ucar D, Esatoglu SN, Hatemi G, Ozyazgan Y, Yurdakul S, et al. Infliximab for uveitis of Behçet's syndrome: a trend for earlier initiation. Clin Exp Rheumatol (2017) 35 Suppl 108(6):86–9.
133. Giardina A, Ferrante A, Ciccia F, Vadala M, Giardina E, Triolo G. One year study of efficacy and safety of infliximab in the treatment of patients with ocular and neurological Behcet's disease refractory to standard immunosuppressive drugs. Rheumatol Int (2011) 31(1):33–7. doi: 10.1007/s00296-009-1213-z
134. Keino H, Okada AA, Watanabe T, Taki W. Long-term efficacy of infliximab on background vascular leakage in patients with Behcet's disease. Eye (Lond) (2014) 28(9):1100–6. doi: 10.1038/eye.2014.138
135. Takeuchi M, Kezuka T, Sugita S, Keino H, Namba K, Kaburaki T, et al. Evaluation of the long-term efficacy and safety of infliximab treatment for uveitis in Behcet's disease: a multicenter study. Ophthalmology (2014) 121(10):1877–84. doi: 10.1016/j.ophtha.2014.04.042
136. Interlandi E, Leccese P, Olivieri I, Latanza L. Adalimumab for treatment of severe Behçet's uveitis: a retrospective long-term follow-up study. Clin Exp Rheumatol (2014) 32(4 Suppl 84):S58–62.
137. Vallet H, Seve P, Biard L, Baptiste Fraison J, Bielefeld P, Perard L, et al. Infliximab versus adalimumab in the treatment of refractory inflammatory uveitis: A multicenter study from the french uveitis network. Arthritis Rheumatol (2016) 68(6):1522–30. doi: 10.1002/art.39667
138. Fabiani C, Vitale A, Emmi G, Vannozzi L, Lopalco G, Guerriero S, et al. Efficacy and safety of adalimumab in Behçet's disease-related uveitis: a multicenter retrospective observational study. Clin Rheumatol (2017) 36(1):183–9. doi: 10.1007/s10067-016-3480-x
139. Jaffe GJ, Dick AD, Brézin AP, Nguyen QD, Thorne JE, Kestelyn P, et al. Adalimumab in patients with active noninfectious uveitis. N Engl J Med (2016) 375(10):932–43. doi: 10.1056/NEJMoa1509852
140. Nguyen QD, Merrill PT, Jaffe GJ, Dick AD, Kurup SK, Sheppard J, et al. Adalimumab for prevention of uveitic flare in patients with inactive non-infectious uveitis controlled by corticosteroids (VISUAL II): a multicentre, double-masked, randomised, placebo-controlled phase 3 trial. Lancet (2016) 388(10050):1183–92. doi: 10.1016/S0140-6736(16)31339-3
141. Suhler EB, Adán A, Brézin AP, Fortin E, Goto H, Jaffe GJ, et al. Safety and efficacy of adalimumab in patients with noninfectious uveitis in an ongoing open-label study: VISUAL III. Ophthalmology (2018) 125(7):1075–87. doi: 10.1016/j.ophtha.2017.12.039
142. Mesquida M, Victoria Hernández M, Llorenç V, Pelegrín L, Espinosa G, Dick AD, et al. Behçet disease-associated uveitis successfully treated with golimumab. Ocular Immunol Inflammation (2013) 21(2):160–2. doi: 10.3109/09273948.2012.741744
143. Curigliano V, Giovinale M, Fonnesu C, Cerquaglia C, Verrecchia E, Turco S, et al. Efficacy of etanercept in the treatment of a patient with Behcet's disease. Clin Rheumatol (2008) 27(7):933–6. doi: 10.1007/s10067-008-0857-5
144. Atzeni F, Sarzi-Puttini P, Capsoni F, Mecchia M, Marrazza MG, Carrabba M. Successful treatment of resistant Behcet's disease with etanercept. Clin Exp Rheumatol (2005) 23(5):729.
145. Sommer A, Altmeyer P, Kreuter A. A case of mucocutaneous Behcet's disease responding to etanercept. J Am Acad Dermatol (2005) 52(4):717–9. doi: 10.1016/j.jaad.2004.11.031
146. Esatoglu SN, Hatemi G. Update on the treatment of Behcet's syndrome. Intern Emerg Med (2019) 14(5):661–75. doi: 10.1007/s11739-019-02035-1
147. Mirouse A, Barete S, Monfort JB, Resche-Rigon M, Bouyer AS, Comarmond C, et al. Ustekinumab for behcet's disease. J Autoimmun (2017) 82:41–6. doi: 10.1016/j.jaut.2017.05.002
148. Fabiani C, Vitale A, Emmi G, Lopalco G, Vannozzi L, Guerriero S, et al. Interleukin (IL)-1 inhibition with anakinra and canakinumab in Behçet's disease-related uveitis: a multicenter retrospective observational study. Clin Rheumatol (2017) 36(1):191–7. doi: 10.1007/s10067-016-3506-4
149. Cantarini L, Vitale A, Scalini P, Dinarello CA, Rigante D, Franceschini R, et al. Anakinra treatment in drug-resistant Behcet's disease: a case series. Clin Rheumatol (2015) 34(7):1293–301. doi: 10.1007/s10067-013-2443-8
150. Caso F, Costa L, Rigante D, Lucherini OM, Caso P, Bascherini V, et al. Biological treatments in Behcet's disease: beyond anti-TNF therapy. Mediators Inflammation (2014) 2014:107421. doi: 10.1155/2014/107421
151. Vitale A, Rigante D, Caso F, Brizi MG, Galeazzi M, Costa L, et al. Inhibition of interleukin-1 by canakinumab as a successful mono-drug strategy for the treatment of refractory Behcet's disease: a case series. Dermatology (2014) 228(3):211–4. doi: 10.1159/000358125
152. Atienza-Mateo B, Calvo-Río V, Beltrán E, Martínez-Costa L, Valls-Pascual E, Hernández-Garfella M, et al. Anti-interleukin 6 receptor tocilizumab in refractory uveitis associated with Behçet's disease: multicentre retrospective study. Rheumatol (Oxford) (2018) 57(5):856–64. doi: 10.1093/rheumatology/kex480
153. Eser Ozturk H, Oray M, Tugal-Tutkun I. Tocilizumab for the treatment of behcet uveitis that failed interferon alpha and anti-tumor necrosis factor-alpha therapy. Ocular Immunol Inflammation (2018) 26(7):1005–14. doi: 10.1080/09273948.2017.1355471
154. Deroux A, Chiquet C, Bouillet L. Tocilizumab in severe and refractory Behcet's disease: Four cases and literature review. Semin Arthritis rheumatism (2016) 45(6):733–7. doi: 10.1016/j.semarthrit.2015.11.012
155. Hueber W, Patel DD, Dryja T, Wright AM, Koroleva I, Bruin G, et al. Effects of AIN457, a fully human antibody to interleukin-17A, on psoriasis, rheumatoid arthritis, and uveitis. Sci Transl Med (2010) 2(52):52ra72. doi: 10.1126/scitranslmed.3001107
156. Dick AD, Tugal-Tutkun I, Foster S, Zierhut M, Melissa Liew SH, Bezlyak V, et al. Secukinumab in the treatment of noninfectious uveitis: results of three randomized, controlled clinical trials. Ophthalmology (2013) 120(4):777–87. doi: 10.1016/j.ophtha.2012.09.040
157. Baerveldt EM, Kappen JH, Thio HB, van Laar JA, van Hagen PM, Prens EP. Successful long-term triple disease control by ustekinumab in a patient with Behcet's disease, psoriasis and hidradenitis suppurativa. Ann Rheum Dis (2013) 72(4):626–7. doi: 10.1136/annrheumdis-2012-202392
158. Langley RG, Armstrong AW, Lebwohl MG, Blauvelt A, Hsu S, Tyring S, et al. Efficacy and safety of brodalumab in patients with psoriasis who had inadequate responses to ustekinumab: subgroup analysis of two randomized phase III trials. Br J Dermatol (2019) 180(2):306–14. doi: 10.1111/bjd.17318
159. Langley RG, Tsai TF, Flavin S, Song M, Randazzo B, Wasfi Y, et al. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: results of the randomized, double-blind, phase III NAVIGATE trial. Br J Dermatol (2018) 178(1):114–23. doi: 10.1111/bjd.15750
160. Levy-Clarke G, Jabs DA, Read RW, Rosenbaum JT, Vitale A, Van Gelder RN. Expert panel recommendations for the use of anti-tumor necrosis factor biologic agents in patients with ocular inflammatory disorders. Ophthalmology (2014) 121(3):785–96.e3. doi: 10.1016/j.ophtha.2013.09.048
161. Vasiliauskas EA, Church JA, Silverman N, Barry M, Targan SR, Dubinsky MC. Case report: evidence for transplacental transfer of maternally administered infliximab to the newborn. Clin Gastroenterol Hepatol (2006) 4(10):1255–8. doi: 10.1016/j.cgh.2006.07.018
162. Zelinkova Z, de Haar C, de Ridder L, Pierik MJ, Kuipers EJ, Peppelenbosch MP, et al. High intra-uterine exposure to infliximab following maternal anti-TNF treatment during pregnancy. Alimentary Pharmacol Ther (2011) 33(9):1053–8. doi: 10.1111/j.1365-2036.2011.04617.x
163. Kane SV, Acquah LA. Placental transport of immunoglobulins: a clinical review for gastroenterologists who prescribe therapeutic monoclonal antibodies to women during conception and pregnancy. Am J Gastroenterol (2009) 104(1):228–33. doi: 10.1038/ajg.2008.71
164. Simister NE. Placental transport of immunoglobulin G. Vaccine (2003) 21(24):3365–9. doi: 10.1016/S0264-410X(03)00334-7
165. Djokanovic N, Klieger-Grossmann C, Pupco A, Koren G. Safety of infliximab use during pregnancy. Reprod Toxicol (Elmsford NY) (2011) 32(1):93–7. doi: 10.1016/j.reprotox.2011.05.009
166. Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, et al. American college of rheumatology guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Rheumatol (2020) 72(4):529–56. doi: 10.1002/art.41191
167. Broms G, Granath F, Ekbom A, Hellgren K, Pedersen L, Sorensen HT, et al. Low risk of birth defects for infants whose mothers are treated with anti-tumor necrosis factor agents during pregnancy. Clin Gastroenterol Hepatol (2016) 14(2):234–41 e1-5. doi: 10.1016/j.cgh.2015.08.039
Keywords: Behcet’s disease, ocular involvement, Behcet’s uveitis, immunopathogenesis, immunogenetic, biological agent, pregnancy
Citation: Lin S, Xu Z, Lin Z, Xie B and Feng J (2023) Advances in pathogenesis and treatment of ocular involvement in Behcet’s disease. Front. Immunol. 14:1206959. doi: 10.3389/fimmu.2023.1206959
Received: 16 April 2023; Accepted: 08 September 2023;
Published: 29 September 2023.
Edited by:
Wenru Su, Sun Yat-sen University, ChinaReviewed by:
Masaki Takeuchi, Yokohama City University, JapanCopyright © 2023 Lin, Xu, Lin, Xie and Feng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junmei Feng, ZmVuZ2ptMzIxQDE2My5jb20=; Baozhao Xie, eGllYmFvemhhb0AxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.