 Robin Arcani1,2*†
Robin Arcani1,2*† Florian Correard3†Pierre Suchon4
Florian Correard3†Pierre Suchon4 Gilles Kaplanski2,5Rodolphe Jean5
Gilles Kaplanski2,5Rodolphe Jean5 Raphael Cauchois2,5Marine Leprince5Vincent Arcani3Julie Seguier6Benjamin De Sainte Marie6Baptiste Andre6Marie Koubi7Pascal Rossi7Stéphane Gayet1Nirvina Gobin1Victoria Garrido1Joris Weiland1
Raphael Cauchois2,5Marine Leprince5Vincent Arcani3Julie Seguier6Benjamin De Sainte Marie6Baptiste Andre6Marie Koubi7Pascal Rossi7Stéphane Gayet1Nirvina Gobin1Victoria Garrido1Joris Weiland1 Elisabeth Jouve8Anne-Laure Couderc9,10Patrick Villani1,10‡
Elisabeth Jouve8Anne-Laure Couderc9,10Patrick Villani1,10‡ Aurélie Daumas1,2‡
Aurélie Daumas1,2‡- 1Internal Medicine and Therapeutics Department, CHU La Timone, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 2Center for Cardiovascular and Nutrition Research (C2VN), INRA 1260, INSERM UMR_S 1263, Aix-Marseille University, Marseille, France
- 3Pharmacy Department, CHU La Timone, AP-HM, Marseille, France
- 4Hematology Laboratory, CHU La Timone, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 5Internal Medicine and Clinical Immunology Department, CHU La Conception, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 6Internal Medicine Department, CHU La Timone, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 7Department of Internal Medicine, CHU Nord, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 8Service Evaluation Médicale, CHU la Conception, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 9Internal Medicine, Geriatrics and Therapeutic Department, CHU Sainte-Marguerite, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 10Aix-Marseille University, CNRS, EFS, ADES, Marseille, France
Background: Tocilizumab and anakinra are anti-interleukin drugs to treat severe coronavirus disease 2019 (COVID-19) refractory to corticosteroids. However, no studies compared the efficacy of tocilizumab versus anakinra to guide the choice of the therapy in clinical practice. We aimed to compare the outcomes of COVID-19 patients treated with tocilizumab or anakinra.
Methods: Our retrospective study was conducted in three French university hospitals between February 2021 and February 2022 and included all the consecutive hospitalized patients with a laboratory-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection assessed by RT-PCR who were treated with tocilizumab or anakinra. A propensity score matching was performed to minimize confounding effects due to the non-random allocation.
Results: Among 235 patients (mean age, 72 years; 60.9% of male patients), the 28-day mortality (29.4% vs. 31.2%, p = 0.76), the in-hospital mortality (31.7% vs. 33.0%, p = 0.83), the high-flow oxygen requirement (17.5% vs. 18.3%, p = 0.86), the intensive care unit admission rate (30.8% vs. 22.2%, p = 0.30), and the mechanical ventilation rate (15.4% vs. 11.1%, p = 0.50) were similar in patients receiving tocilizumab and those receiving anakinra. After propensity score matching, the 28-day mortality (29.1% vs. 30.4%, p = 1) and the rate of high-flow oxygen requirement (10.1% vs. 21.5%, p = 0.081) did not differ between patients receiving tocilizumab or anakinra. Secondary infection rates were similar between the tocilizumab and anakinra groups (6.3% vs. 9.2%, p = 0.44).
Conclusion: Our study showed comparable efficacy and safety profiles of tocilizumab and anakinra to treat severe COVID-19.
1 Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1) and has led to more than 6 million deaths around the world (2). COVID-19 can range from a simple asymptomatic viral infection to acute respiratory distress syndrome (ARDS) requiring intensive care; 15%–20% of hospitalized patients develop severe pneumonia (3, 4). Currently, the standard of care for in-hospitalized patients requiring oxygen is based on corticosteroids (5, 6), which have broad-spectrum anti-inflammatory actions. Despite the extensive use of dexamethasone, 15%–30% of patients remain refractory to corticosteroids and require intubation or progress to death (5–7).
Tocilizumab (an interleukin (IL)-6 receptor antagonist) and anakinra (an IL-1 receptor antagonist) have been proven effective in reducing mortality in patients with severe inflammatory COVID-19 (8–12). In France, since 2021, the French High Council for Public Health (HCSP) recommends adding anti-IL-6 or anti-IL-1 drugs in patients requiring high-flow oxygen therapy and having a marked inflammatory state in the absence of improvement (C-reactive protein (CRP) >75 mg/L) after 48 h of the standard of care, including dexamethasone (13). However, to date, there is no evidence showing which anti-IL drug is the most effective. Scarce data have compared the efficacy of tocilizumab versus anakinra in dexamethasone-refractory COVID-19 patients (14, 15). We aimed to retrospectively compare the outcomes of dexamethasone-refractory COVID-19 patients treated with tocilizumab or anakinra using propensity score matching.
2 Materials and methods
2.1 Patients
We retrospectively included all consecutive adult patients (aged ≥18 years) admitted with a laboratory-confirmed SARS-CoV-2 infection assessed by RT-PCR on nasopharyngeal swabs requiring oxygen, who were dexamethasone-refractory (defined by an absence of clinical improvement and/or an absence of a decrease in CRP after 72 h of dexamethasone) and treated with tocilizumab or anakinra between February 2021 and February 2022 in six internal medicine departments in three hospitals (La Timone, La Conception and Hôpital Nord, and University Hospitals of Marseille, France). Patients were not included if they had received both anti-IL drugs or one anti-IL and one JAK inhibitor to treat COVID-19 or if there were insufficient patient follow-up data to perform analysis (e.g., patient transferred to another hospital).
Clinical, biological, radiological, and follow-up data were collected from electronic medical records. Patients were divided into three groups based on low-dose chest computed tomography (CT) extent of lung parenchymal lesions (minimal, <10%; moderate, 10%–25%; and severe, >25%). The vaccine status of the patients was unvaccinated, partially vaccinated, or fully vaccinated (0, 1, or 2 doses received, respectively).
Patients received tocilizumab (8 mg/kg, 800 mg maximum) intravenously over a 1-h infusion once or repeated after 24 h, according to the opinion of the attending clinician. Patients were treated with subcutaneous anakinra 100 mg/day until clinical improvement (maximum 10 days) or with 300 mg/day for 5 days and then tapering 200 mg/day for 2 days and 100 mg/day for 1 day. All patients were treated with dexamethasone (6 mg/day, administered intravenously, until oxygen discontinuation). Patients could also have received anti-spike monoclonal antibodies [casirivimab/imdevimab (Ronapreve®), or sotrovimab (Xevudy®) according to the SARS-CoV-2 variants], antibiotics, and prophylactic (enoxaparin 40 mg/day), intermediate (enoxaparin 40 mg twice a day), or therapeutic (tinzaparin 175 anti-Xa IU/kg/day) thromboprophylaxis according to the current recommendations from the French Society of Critical Care (16) until discharge.
Patients were considered under immunosuppressive therapy when they took anti-rejection therapy, immunosuppressive therapy, corticosteroids > 10 mg/day, biotherapy, or chemotherapy before COVID-19. Patients were considered with a secondary infection when they needed a new antibiotic 48 h after the introduction of the anti-IL drug or when a new bacterial infection was identified (by culture or molecular testing).
2.2 Ethics
This study was approved by the Institutional Review Board of Assistance Publique - Hôpitaux de Marseille (GDPR number PADS22-339). The study was conducted in compliance with good clinical practices and the Declaration of Helsinki principles. Formal approval from an ethics committee was not required for this observational study.
2.3 Statistical analysis
Quantitative variables were described using means and standard deviations (SD); categorical variables were described using numbers and percentages. Quantitative data were compared using Student’s t-test or the Mann–Whitney U test, while qualitative data were compared with the chi-square or Fisher’s exact test when appropriate. A propensity score matching was performed to minimize confounding effects due to the non-random allocation. The propensity score matching function matched the two groups of patients with an anti-IL drug (tocilizumab or anakinra) as the dependent variable. Based on risk factors described in the literature (17–21), propensity score matching of 1:1 was performed with age, sex, vaccine status (partial/full versus none), the extent of lung involvement, comorbidities (hypertension, cancer, chronic kidney disease, diabetes, and obesity), a high-flow requirement before anti-IL introduction, CRP level at the anti-IL drug introduction, use of anti-spike monoclonal antibodies, and thromboprophylaxis as covariates using the optimal method. To confirm the results found with the optimal method, we performed the nearest neighbor propensity score matching method (caliper = 0.25). After matching, McNemar’s test was used to test the association of the mortality rate/rate of high-flow oxygen requirement with the anti-IL drug between matched pairs. The tests were two-sided. p-Values <0.05 were considered significant. All analyses were performed with R software (R Foundation for Statistical Computing, Vienna, Austria), and the propensity score was performed with the MatchIt package.
3 Results
3.1 Characteristics of the population
During the study period, 259 patients were treated with anti-IL drugs; 19 patients were excluded because they received tocilizumab and anakinra (n = 16) or JAK inhibitor and anakinra (n = 3), and five patients were excluded because of a lack of follow-up data. A total of 235 patients were included in the analysis. The main characteristics of the population are presented in Table 1. The mean age was 72 ± 15 years (range, 28–99), with 143 male patients (60.9%). The main comorbidities were hypertension (51.5%), type 2 diabetes (34.0%), obesity (23.4%), overweight (19.4%), chronic kidney disease (18.7%), coronary artery disease (14.0%), pulmonary diseases (chronic obstructive pulmonary disease, asthma, or obstructive sleep apnea, 13.6%), and active cancer (13.2%). Of the total patients, 21 (8.9%) received previous immunosuppressive therapy, and 116 (49.4%) had a “not to be resuscitated” status.
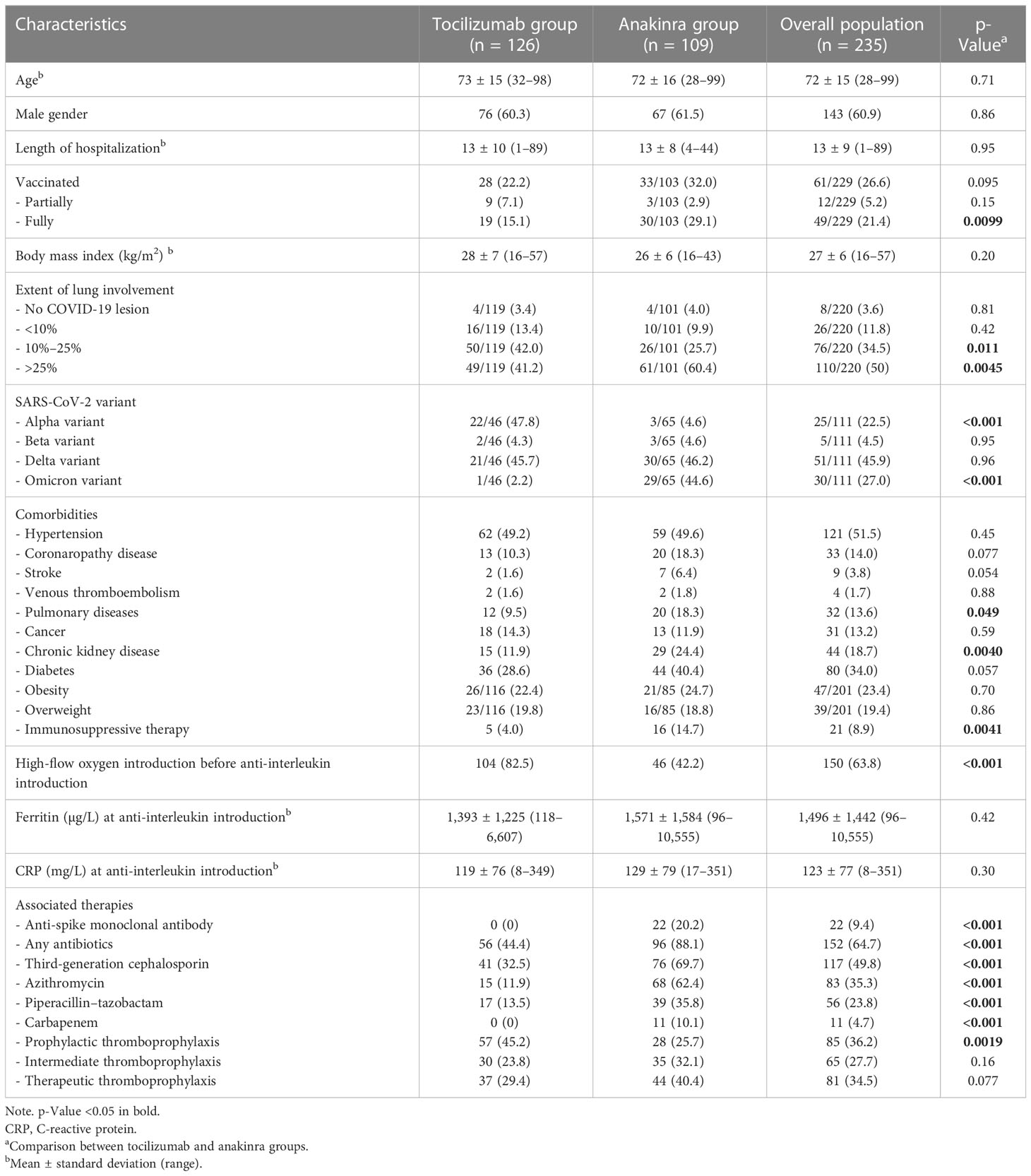
Table 1 Description of the cohort.
Vaccine status was available for 229 patients: 61 patients (26.6%) received at least one dose of vaccine, 12 patients (5.2%) were partially vaccinated (only one dose of vaccine), and 49 (21.4%) were fully vaccinated (two doses of vaccine). Assessment of SARS-CoV-2 variants was available in 111 patients: 25 (22.5%) carried the alpha variant, 5 (4.5%) carried the beta variant, 51 (45.9%) carried the delta variant, and 30 (27.0%) carried the omicron variant. Lung CT showed typical lesions of COVID-19 in 212 out of 220 patients (96.4%), consisting of minimal, moderate, and severe lesions in 11.8%, 34.5%, and 50.0%, respectively. Of 152 patients (64.7%) who received antibiotics, 117 of them (49.8%) received third-generation cephalosporin, 83 patients (35.3%) received azithromycin, 56 patients (23.8%) received piperacillin–tazobactam, and 11 patients (4.7%) received carbapenem. Sixty-six patients (28.1%) received only one antibiotic, 61 patients (26.0%) received two antibiotics, 21 patients (8.9%) received three antibiotics, and four patients (1.7%) received four antibiotics. Of 235 patients, 231 (98.3%) were treated with low-molecular-weight heparin at prophylactic, intermediate, or therapeutic doses of 36.2%, 27.7%, and 34.5%, respectively; 22 patients (9.4%) were treated with monoclonal anti-spike antibodies; 150 patients (63.8%) were treated with an anti-IL drug once under high-flow oxygen. At the time of anti-IL introduction, ferritin was 1,496 ± 1,442 µg/L (range, 96–10,555), and C-reactive protein was 123 ± 77 mg/L (range, 8–351).
3.2 Comparisons of the baseline characteristics between patients receiving tocilizumab and anakinra
A total of 126 (53.6%) patients received tocilizumab, and 109 (46.4%) patients received anakinra (Table 1). The two cohorts were similar in age, gender, and main comorbidities (hypertension, coronaropathy disease, obesity, overweight, and cancer). There were some differences between the two cohorts in terms of vaccine status (fully vaccinated patients: 15.1% of the tocilizumab group vs. 29.1% of the anakinra group, p = 0.01), extent of lung involvement (42.0% of intermediate lesions in the tocilizumab group vs. 25.7% in the anakinra group, p = 0.011; 41.2% of severe lesions in the tocilizumab group vs. 60.4% in the anakinra group, p = 0.0045), SARS-CoV-2 variants (47.8% of alpha variant in the tocilizumab group vs. 4.6% in the anakinra group, p < 0.001; 2.2% of omicron variant in the tocilizumab group vs. 44.6% in the anakinra group, p < 0.001), comorbidities (9.5% of the tocilizumab group had pulmonary diseases vs. 18.3% of the anakinra group, p = 0.049; 11.9% of the tocilizumab group had chronic kidney disease vs. 24.4% of the anakinra group, p = 0.0040; 4.0% of the tocilizumab group were under immunosuppressive therapy vs. 14.7% of the anakinra group, p = 0.0041), severity of clinical state (82.5% of the tocilizumab group were under high-flow oxygen before anti-IL introduction vs. 42.2% of the anakinra group, p < 0.001), thromboprophylaxis management (45.2% of the tocilizumab group received prophylactic dose of low-molecular-weight heparin vs. 25.7% of the anakinra group, p = 0.0019), or associated therapies (0% of the tocilizumab group received anti-spike monoclonal antibody vs. 20.2% of the anakinra group, p < 0.001; 44.4% of the tocilizumab group received antibiotics vs. 88.1% of the anakinra group, p < 0.001).
After propensity score matching using the optimal method (Table 2), 79 patients treated with tocilizumab and 79 patients treated with anakinra had similar characteristics (except for anti-spike monoclonal antibodies; no patients in the tocilizumab group received anti-spike monoclonal antibodies vs. 26.6% of the anakinra group, p < 0.001; for high-flow oxygen introduction before anti-IL introduction, 73.4% were under high-flow oxygen at tocilizumab introduction vs. 43.0% at anakinra introduction). Because of the imbalance of covariates between the two groups, we performed a propensity score matching using the nearest neighbor method (Table 3). Similar characteristics were found in 36 patients treated with tocilizumab and 36 patients treated with anakinra.
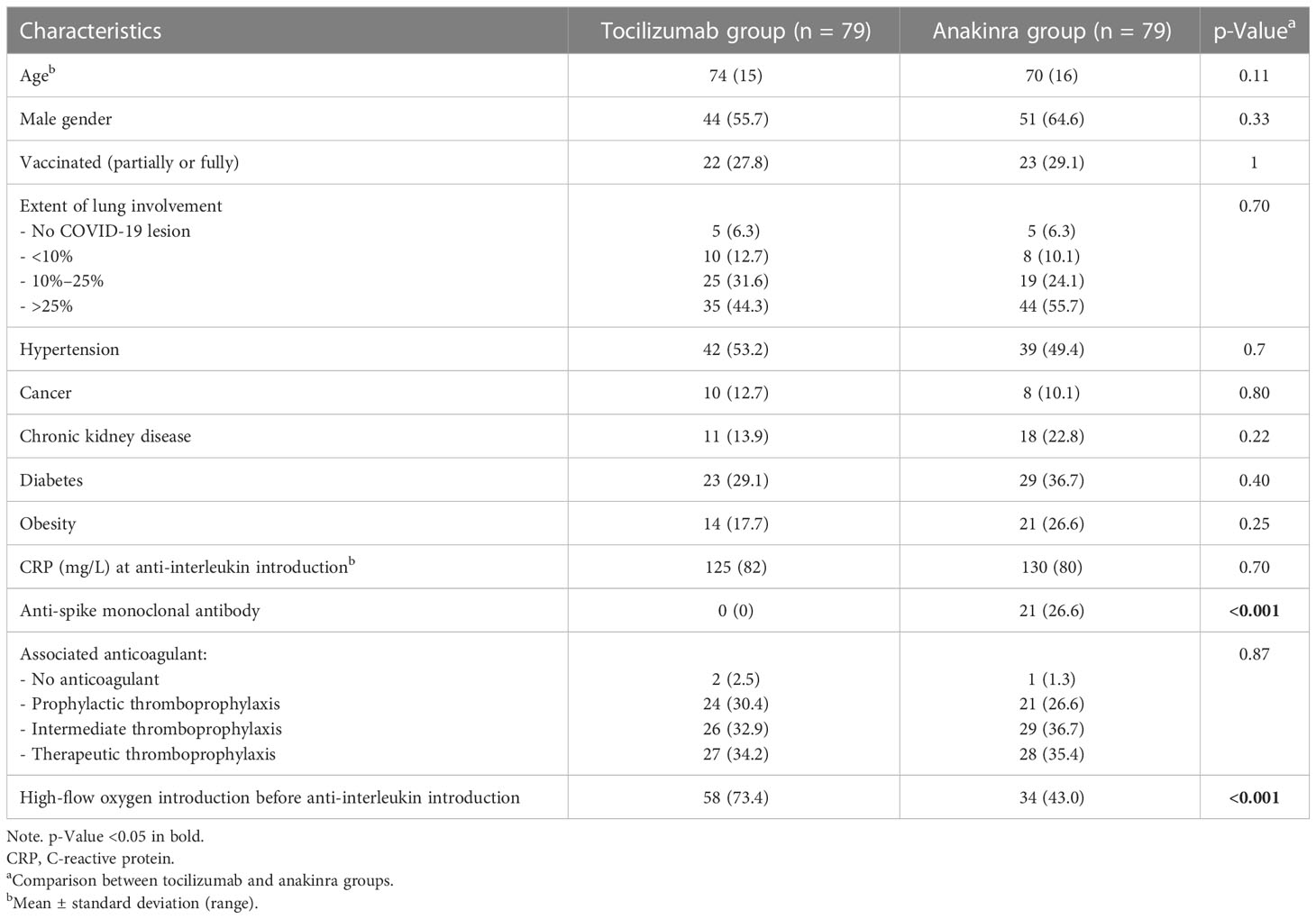
Table 2 Patient characteristics after matching (optimal method).
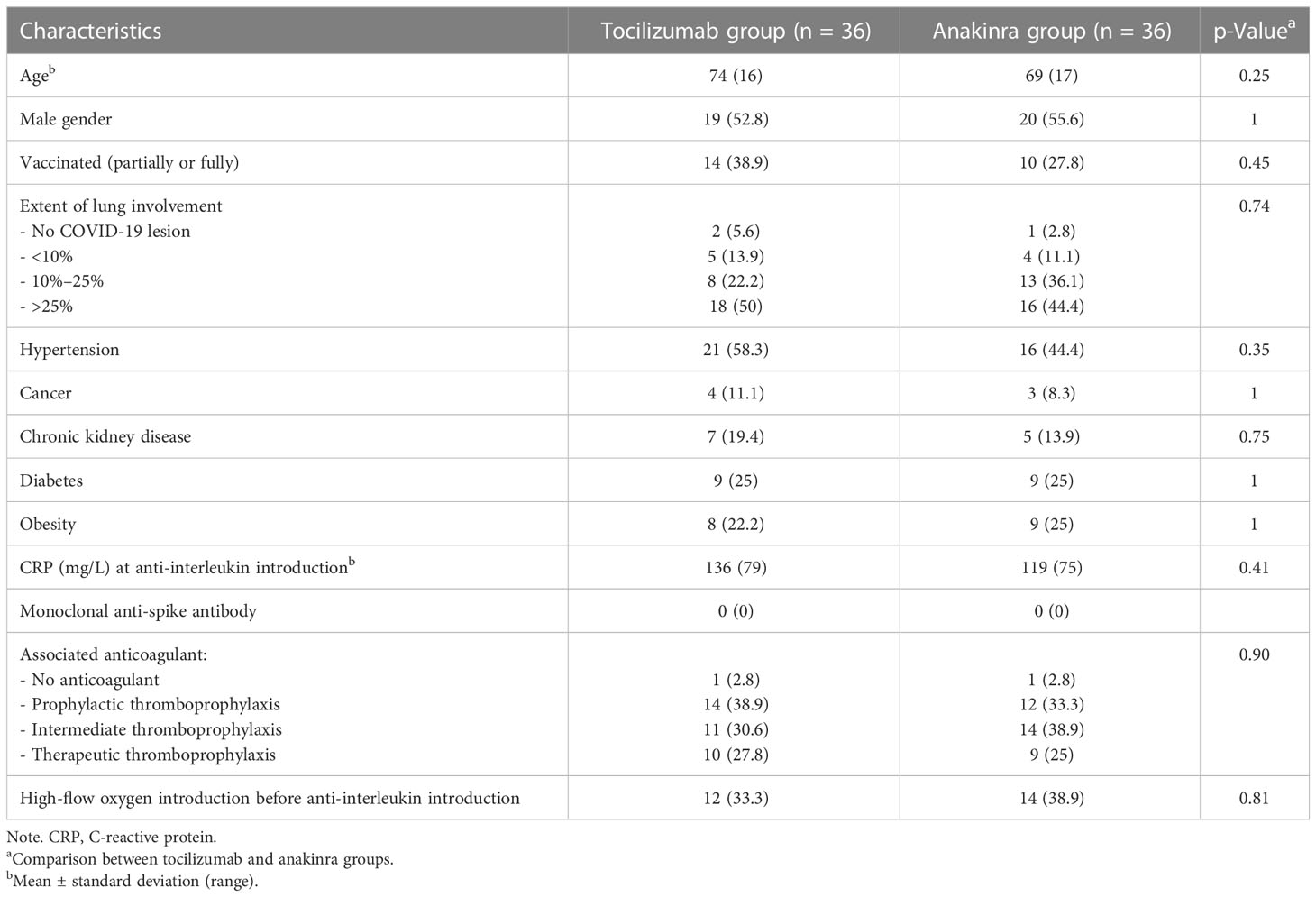
Table 3 Patient characteristics after matching (nearest neighbor method).
3.3 Outcomes of patients under anti-IL drugs
The 28-day mortality was similar between the two groups (29.4% in the tocilizumab group vs. 31.2% in the anakinra group, p = 0.76), as was in-hospital mortality (31.7% in the tocilizumab group vs. 33.0% in the anakinra group, p = 0.83). High-flow oxygen was required in similar proportions (17.5% in the tocilizumab group vs. 18.3% in the anakinra group, p = 0.86). Among patients without a “not to be resuscitated” status (n = 119), the transfer rate into intensive care units (ICUs) was similar between the two groups (30.8% in the tocilizumab group vs. 22.2% in the anakinra group, p = 0.30). The secondary infections following anti-IL drugs were quite scarce (6.3% in the tocilizumab group vs. 9.2% in the anakinra group, p = 0.44) (Table 4).
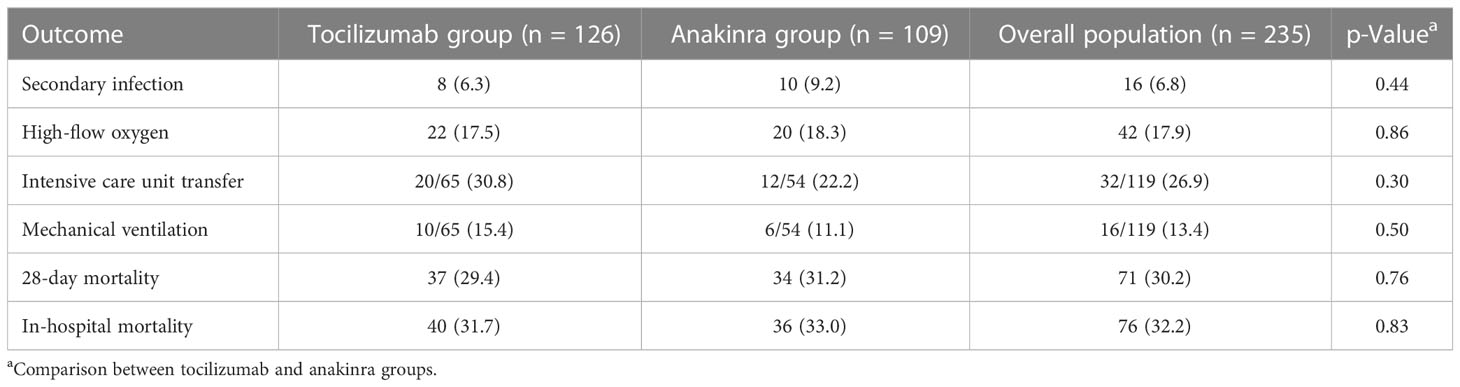
Table 4 Outcomes of the cohort.
After propensity score matching using the optimal method, the 28-day mortality (29.1% in the tocilizumab group vs. 30.4% in the anakinra group, p = 1) and the rate of high-flow oxygen requirement (10.1% in the tocilizumab group vs. 21.5% in the anakinra group, p = 0.081) did not differ between the two groups. Using the nearest neighbor method, we found a similar 28-day mortality (33.3% in the tocilizumab group vs. 30.6% in the anakinra group, p = 1) and a similar rate of high-flow oxygen requirement (5.6% in the tocilizumab group vs. 13.9% in the anakinra group, p = 0.43) between the pseudo-populations.
4 Discussion
We reported a cohort of hospitalized COVID-19 before ICU admission and intubation who were treated with an anti-IL drug. We showed that the 28-day mortality and the high-flow oxygen requirement did not differ according to the treatment received, tocilizumab or anakinra. The two treatments had the same risk of infections.
These results follow the few data available about this subject. IL-1 and IL-6 are two cytokines mainly involved in cytokine storm initiation and amplification, particularly in COVID-19 ARDS (22). Anakinra is an IL-1-receptor antagonist blocking the effect of both IL-1α and IL-1β. IL-1β leads to the production of IL-6 (23). However, tocilizumab blocks IL-6-mediated signal transduction by targeting both the membrane and soluble forms of the IL-6 receptor (24). Thus, it seems logical that the use of tocilizumab or anakinra could be effective in COVID-19. A large amount of data in the literature confirm the efficacy of the two anti-IL drugs (10, 25–27).
However, to date, randomized trials comparing the efficacy of different agents are lacking. The effect of tocilizumab and anakinra seems similar among all the meta-analyses (28–31). One Turkish study compared many patients receiving tocilizumab or anakinra using propensity score matching (15). The authors concluded a lower mortality and ICU transfer rate in the anakinra group. However, in this cohort, patients received very high doses of anakinra (600 mg daily mean versus 100 mg daily in most studies) and were also treated with hydroxychloroquine and favipiravir. Finally, the patients in the tocilizumab group received less corticosteroid than in the anakinra group, which is a major bias. Langer-Gould et al. (32) compared 52 patients treated with tocilizumab to 41 patients treated with anakinra using a propensity score matching and found no statistical difference in mortality. Some other studies, with a few participants, have directly compared tocilizumab to anakinra. Iglesias-Julian et al. (33) showed the same mortality under tocilizumab or anakinra. Patoulias et al. (14) performed a meta-analysis on three non-randomized studies comparing 125 patients under tocilizumab to 112 patients under anakinra and found lower mortality in the anakinra group. Unfortunately, they did not adjust their results with confounding factors. To the best of our knowledge, here, we report one of the largest cohorts of patients treated with tocilizumab compared to anakinra using an adjustment on confounding factors.
We acknowledge some limitations of this study. First, it was retrospective, but we could compare the patients using propensity score matching despite the absence of randomization. We used a combination of clinical, biological, and radiological prognosis factors to build our propensity score matching. Second, the patients were recruited over a large period, including patients infected by different variants of SARS-CoV-2. We could not add variants in the propensity score matching because there were too much missing data, which would have led to the inability to build the propensity score matching. Furthermore, we included a few patients with the omicron variant, which is now dominating. However, there is no evidence that the SARS-CoV-2 omicron variant changes the response to the anti-inflammatory therapy (34, 35). In effect, even if the omicron variant is less severe than the others, thanks to the propensity score matching, we could compare patients with COVID-19 with the same severity (according to the extent of lung involvement, the CRP level, or the rate of high-flow requirement before anti-IL introduction, which are well-known factors of severity). We also acknowledge the lack of assessment of inflammatory biomarkers such as interleukin-6 and soluble urokinase plasminogen activator receptor (suPAR) at baseline. Nevertheless, their utility was not clear, hyperinflammation was defined by CRP and ferritin levels, and IL-6 and suPAR are not routinely available biomarkers in all the centers. Furthermore, the two groups could not be matched on anti-spike monoclonal antibodies (using the optimal method) because no patients in the tocilizumab group have received these treatments (they were not available during the second and third waves when most patients receiving tocilizumab were included). Therefore, we performed a second propensity score matching, in which the use of anti-spike monoclonal antibodies was balanced between the two groups. Despite the small sample size, similar results were found with this method. Moreover, the rate of antibiotic prescriptions was different between the two groups. However, there is no evidence in the literature showing that antibiotics influence the response to anti-IL drugs or the evolution of COVID-19 (36–38).
Since the efficacy of tocilizumab seems to be similar to the efficacy of anakinra, clinicians should consider the cost of the treatment to choose it. In France, the cost of a 10-day anakinra course is lower than that of an 8 mg/kg dose of tocilizumab. In our study, the average cost of tocilizumab per patient was 1,052€/1,124 USD compared to 189€/202 USD per patient treated with anakinra. Moreover, the half-life of anakinra [a few hours (39)] is lower than that of tocilizumab [14–21 days (40)]. In patients with secondary infection due to the anti-IL drug, the infection would be easier to manage with a short half-life therapy such as anakinra than with tocilizumab.
Despite the small sample sizes of groups after propensity score matching, our study showed the same efficacy and secondary infection risk of tocilizumab and anakinra to treat severe COVID-19. Thus, anakinra and tocilizumab represented equivalent therapies in conjunction with corticosteroids. Our results need to be confirmed in larger randomized studies in order to choose the most effective and personalized treatment plans for each patient.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the corresponding authors, upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Portail d’Accès aux Données de Santé - Assistance Publique Hôpitaux de Marseille. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
RA, FC, PS, PV and AD contributed to the design of the study. All the authors participated in the enrolment of study participants and data collection. RA and PS analyzed the data. RA, FC, PV and AD drafted the manuscript. All authors contributed to the data interpretation and in revising the final manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
GK has received from ROCHE-CHUGAI Research Grants <€20,000 and fees from Sobi France for scientific presentations <€4,000 and participated in a SOBI Advisory Board on COVID unpaid and an OLATEC Monitoring Board unpaid.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus; ARDS, acute respiratory distress syndrome; IL, interleukin; HCSP, High Council for Public Health; CT, computed tomography; SD, standard deviations; ICU, intensive care unit.
References
1. WHO director-general’s remarks at the media briefing on 2019-nCoV on 11 February 2020. Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (Accessed February 3, 2021).
2. WHO coronavirus (COVID-19) dashboard. Available at: https://covid19.who.int (Accessed April 25, 2021).
3. Chen G, Wu D, Guo W, Cao Y, Huang D, Wang H, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest (2022) 130:2620–9. doi: 10.1172/JCI137244
4. Ramasamy S, Subbian S. Critical determinants of cytokine storm and type I interferon response in COVID-19 pathogenesis. Clin Microbiol Rev (2021) 34:e00299-20. doi: 10.1128/CMR.00299-20
5. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in hospitalized patients with covid-19. N Engl J Med (2021) 384:693–704. doi: 10.1056/NEJMoa2021436
6. Arcani R, Cauchois R, Suchon P, Jean R, Jarrot P-A, Gomes De Pinho Q, et al. Factors associated with dexamethasone efficacy in COVID-19. a retrospective investigative cohort study. J Med Virol (2022) 94:3169–75. doi: 10.1002/jmv.27712
7. Munch MW, Myatra SN, Vijayaraghavan BKT, Saseedharan S, Benfield T, Wahlin RR, et al. Effect of 12 mg vs 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia. JAMA (2021) 326:1–11. doi: 10.1001/jama.2021.18295
8. Salama C, Han J, Yau L, Reiss WG, Kramer B, Neidhart JD, et al. Tocilizumab in patients hospitalized with covid-19 pneumonia. N Engl J Med (2021) 384:20–30. doi: 10.1056/NEJMoa2030340
9. RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet (2021) 397:1637–45. doi: 10.1016/S0140-6736(21)00676-0
10. Kyriazopoulou E, Huet T, Cavalli G, Gori A, Kyprianou M, Pickkers P, et al. Effect of anakinra on mortality in patients with COVID-19: a systematic review and patient-level meta-analysis. Lancet Rheumatol (2021) 3:e690–7. doi: 10.1016/S2665-9913(21)00216-2
11. Kyriazopoulou E, Poulakou G, Milionis H, Metallidis S, Adamis G, Tsiakos K, et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: a double-blind, randomized controlled phase 3 trial. Nat Med (2021) 27:1752–60. doi: 10.1038/s41591-021-01499-z
12. Cavalli G, De Luca G, Campochiaro C, Della-Torre E, Ripa M, Canetti D, et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: a retrospective cohort study. Lancet Rheumatol (2020) 2:e325–31. doi: 10.1016/S2665-9913(20)30127-2
13. Covid-19: IL1 and IL6 antagonist treatment recommendations. Available at: https://www.hcsp.fr/Explore.cgi/AvisRapportsDomaine?clefr=1110 (Accessed August 26, 2022).
14. Patoulias D, Dimosiari A, Michailidis T. Anakinra or tocilizumab for prevention of COVID-19 death? a big dilemma. Eur J Intern Med (2021) 90:107–8. doi: 10.1016/j.ejim.2021.05.039
15. Küçükşahin O, Erden A, Karakaş Ö, Güven SC, Armağan B, Şahiner EŞ, et al. Comparison of anakinra and tocilizumab in management of severe COVID-19: a retrospective cohort study. Turk J Med Sci (2022) 52:1486–94. doi: 10.55730/1300-0144.5487
16. Propositions du GFHT/GIHP pour le traitement anticoagulant pour la prévention du risque thrombotique chez un patient hospitalisé avec COVID-19. groupe d’etude sur l’hemostase et la thrombose. Available at: https://site.geht.org/actu/propositions-du-gfht-gihp-pour-le-traitement-anticoagulant-pour-la-prevention-du-risque-thrombotique-chez-un-patient-hospitalise-avec-covid-19/ (Accessed December 19, 2022).
17. Gupta A, Gonzalez-Rojas Y, Juarez E, Crespo Casal M, Moya J, Falci DR, et al. Early treatment for covid-19 with SARS-CoV-2 neutralizing antibody sotrovimab. N Engl J Med (2021) 385:1941–50. doi: 10.1056/NEJMoa2107934
18. RECOVERY Collaborative Group. Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet (2022) 399:665–76. doi: 10.1016/S0140-6736(22)00163-5
19. Gao Y-D, Ding M, Dong X, Zhang J-J, Kursat Azkur A, Azkur D, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy (2021) 76:428–55. doi: 10.1111/all.14657
20. Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis (2021) 21:855. doi: 10.1186/s12879-021-06536-3
21. Zhang J-J, Dong X, Liu G-H, Gao Y-D. Risk and protective factors for COVID-19 morbidity, severity, and mortality. Clin Rev Allergy Immunol (2023) 64:90–107. doi: 10.1007/s12016-022-08921-5
22. Fajgenbaum DC, June CH. Cytokine storm. N Engl J Med (2020) 383:2255–73. doi: 10.1056/NEJMra2026131
23. Kozak W, Kluger MJ, Soszynski D, Conn CA, Rudolph K, Leon LR, et al. IL-6 and IL-1β in fever: studies using cytokine-deficient (Knockout) micea. Ann New York Acad Sci (1998) 856:33–47. doi: 10.1111/j.1749-6632.1998.tb08310.x
24. Aliyu M, Zohora FT, Anka AU, Ali K, Maleknia S, Saffarioun M, et al. Interleukin-6 cytokine: an overview of the immune regulation, immune dysregulation, and therapeutic approach. Int Immunopharmacol (2022) 111:109130. doi: 10.1016/j.intimp.2022.109130
25. Hermine O, Mariette X, Tharaux P-L, Resche-Rigon M, Porcher R, Ravaud P, et al. Effect of tocilizumab vs usual care in adults hospitalized with COVID-19 and moderate or severe pneumonia: a randomized clinical trial. JAMA Intern Med (2021) 181:32–40. doi: 10.1001/jamainternmed.2020.6820
26. Tleyjeh IM, Kashour Z, Damlaj M, Riaz M, Tlayjeh H, Altannir M, et al. Efficacy and safety of tocilizumab in COVID-19 patients: a living systematic review and meta-analysis. Clin Microbiol Infect (2021) 27:215–27. doi: 10.1016/j.cmi.2020.10.036
27. Pasin L, Cavalli G, Navalesi P, Sella N, Landoni G, Yavorovskiy AG, et al. Anakinra for patients with COVID-19: a meta-analysis of non-randomized cohort studies. Eur J Intern Med (2021) 86:34–40. doi: 10.1016/j.ejim.2021.01.016
28. Khan FA, Stewart I, Fabbri L, Moss S, Robinson K, Smyth AR, et al. Systematic review and meta-analysis of anakinra, sarilumab, siltuximab and tocilizumab for COVID-19. Thorax (2021) 76:907–19. doi: 10.1136/thoraxjnl-2020-215266
29. Peng J, Fu M, Mei H, Zheng H, Liang G, She X, et al. Efficacy and secondary infection risk of tocilizumab, sarilumab and anakinra in COVID-19 patients: a systematic review and meta-analysis. Rev Med Virol (2022) 32:e2295. doi: 10.1002/rmv.2295
30. Davidson M, Menon S, Chaimani A, Evrenoglou T, Ghosn L, Graña C, et al. Interleukin-1 blocking agents for treating COVID-19. Cochrane Database Systematic Rev (2022). doi: 10.1002/14651858.CD015308
31. Albuquerque AM, Eckert I, Tramujas L, Butler-Laporte G, McDonald EG, Brophy JM, et al. Effect of tocilizumab, sarilumab, and baricitinib on mortality among patients hospitalized for COVID-19 treated with corticosteroids: a systematic review and meta-analysis. Clin Microbiol Infect (2022) 29(1):13–21. doi: 10.1016/j.cmi.2022.07.008
32. Langer-Gould A, Smith JB, Gonzales EG, Castillo RD, Figueroa JG, Ramanathan A, et al. Early identification of COVID-19 cytokine storm and treatment with anakinra or tocilizumab. Int J Infect Dis (2020) 99:291–7. doi: 10.1016/j.ijid.2020.07.081
33. Iglesias-Julián E, López-Veloso M, de-la-Torre-Ferrera N, Barraza-Vengoechea JC, Delgado-López PD, Colazo-Burlato M, et al. High dose subcutaneous anakinra to treat acute respiratory distress syndrome secondary to cytokine storm syndrome among severely ill COVID-19 patients. J Autoimmun (2020) 115:102537. doi: 10.1016/j.jaut.2020.102537
34. Atluri K, Aimlin I, Arora S. Current effective therapeutics in management of COVID-19. J Clin Med (2022) 11:3838. doi: 10.3390/jcm11133838
35. Oliynyk O, Barg W, Oliynyk Y, Dubrov S, Gurianov V, Rorat M. Lack of difference in tocilizumab efficacy in the treatment of severe COVID-19 caused by different SARS-CoV-2 variants. J Pers Med (2022) 12:1103. doi: 10.3390/jpm12071103
36. Chedid M, Waked R, Haddad E, Chetata N, Saliba G, Choucair J. Antibiotics in treatment of COVID-19 complications: a review of frequency, indications, and efficacy. J Infect Public Health (2021) 14:570–6. doi: 10.1016/j.jiph.2021.02.001
37. Popp M, Stegemann M, Riemer M, Metzendorf M-I, Romero CS, Mikolajewska A, et al. Antibiotics for the treatment of COVID-19. Cochrane Database Syst Rev (2021) 10:CD015025. doi: 10.1002/14651858.CD015025
38. Akbari A, Razmi M, Sedaghat A, Alavi Dana SMM, Amiri M, Halvani AM, et al. Comparative effectiveness of pharmacological interventions on mortality and the average length of hospital stay of patients with COVID-19: a systematic review and meta-analysis of randomized controlled trials. Expert Rev Anti Infect Ther (2022) 20:585–609. doi: 10.1080/14787210.2022.1997587
39. Yang B-B, Gozzi P, Sullivan JT. Pharmacokinetics of anakinra in subjects of heavier vs. lighter body weights. Clin Transl Sci (2019) 12:371–8. doi: 10.1111/cts.12622
40. EMA. RoActemra (2018). European Medicines Agency. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/roactemra (Accessed December 19, 2022).
Keywords: anakinra, tocilizumab, anti-interleukin drugs, COVID-19, mortality, SARS-CoV-2, anti-interleukin 6, interleukin 1 receptor antagonist
Citation: Arcani R, Correard F, Suchon P, Kaplanski G, Jean R, Cauchois R, Leprince M, Arcani V, Seguier J, De Sainte Marie B, Andre B, Koubi M, Rossi P, Gayet S, Gobin N, Garrido V, Weiland J, Jouve E, Couderc A-L, Villani P and Daumas A (2023) Tocilizumab versus anakinra in COVID-19: results from propensity score matching. Front. Immunol. 14:1185716. doi: 10.3389/fimmu.2023.1185716
Received: 13 March 2023; Accepted: 15 May 2023;
Published: 26 May 2023.
Edited by:
Antonio Lalueza, University Hospital October 12, SpainReviewed by:
Andrew Weber, Northwell Health, United StatesDoreen E Szollosi, University of Saint Joseph, United States
Copyright © 2023 Arcani, Correard, Suchon, Kaplanski, Jean, Cauchois, Leprince, Arcani, Seguier, De Sainte Marie, Andre, Koubi, Rossi, Gayet, Gobin, Garrido, Weiland, Jouve, Couderc, Villani and Daumas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robin Arcani, cm9iaW4uYXJjYW5pQGFwLWhtLmZy
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship