 Inger Johanne Fenne
Inger Johanne Fenne Guro Askildsen Oftebro1
Guro Askildsen Oftebro1 Christian Vestergaard
Christian Vestergaard- 1Study of Medicine, Faculty of Health, Aarhus University, Aarhus, Denmark
- 2Department of Dermato-Venereology, Aarhus University Hospital, Aarhus, Denmark
Introduction: Bullous pemphigoid (BP) can be treated using systemic and topical glucocorticoids and/or other immunomodulatory agents. However, the long-term use of systemic glucocorticoids causes severe adverse side effects. This study was aimed at investigating whether the early initiation of corticosteroid-sparing therapy (CST) in BP patients results in better outcomes than late or no CST.
Method: We retrospectively identified all BP patients referred to the tertiary center, of the Department of Dermatology and Venerology, Aarhus University Hospital, Denmark, from 2015 to 2021. Patients’ demographics, comorbidities, treatment, remission of BP, length of admission, relapse, and 1-year mortality were recorded. All patients who received CST were dichotomised into two groups: initiated with CST <28 or >28 days. The groups were compared using t-tests. Additionally, all patients who received CST were compared with those who received systemic glucocorticoids alone. Our cohort was compared with that of a previous study (2006–2013) performed in our department. In 2015, we revised our BP treatment guidelines to include the early initiation of CST.
Results: On comparing the group of patients initiated with CST <28 versus >28 days, we found no significant differences in the complications or mortality between the groups (p = 0.63 and p=0.79, respectively). The <28 days group had a lower rate of relapse (p < 0.05). On comparing data from this study with those from the previous study, conducted before we revised our treatment guideline, we found a reduced initial dose of prednisolone and reduced admission time in this study. No significant differences were found between patients treated with CST and those treated with systemic glucocorticoids alone.
Conclusion: The rate of complications and 1-year mortality did not differ significantly between the two subgroups in this study. The relapse rate was lower in the CST <28 days group than in the CST >28 days group. The initial dose of prednisolone and admission time were reduced in this study compared with those in the previous study performed before the implementation of a local treatment guideline recommending the early initiation of CST.
1 Introduction
Bullous pemphigoid (BP) is an autoimmune blistering disease that predominantly affects individuals aged >65 years1 and is characterized by tense subepithelial blisters and generalized pruritic urticarial plaques arising from normal or erythematosus skin (1) (Figure 1). In one-third of BP patients, the oral and/or anogenital mucosa is also affected. However, one-fifth of patients do not develop blisters; in such patients, the diagnosis is made by direct immunofluorescence of skin biopsy staining for deposits of IgG at the dermo-epidermal border1. Standard therapies include topical and systemic corticosteroids and other immunomodulatory agents. The outcome and prognosis of the disease are correlated with the disease severity. Long-term monitoring is often required, as well as hospitalization in severe cases.

Figure 1 Admitted BP patient with characteristic tense subepithelial blisters and pruritic urticarial plaques.
BP is caused by autoantibodies targeting the hemidesmosomal proteins, BP230 (BPAG1) and BP180 (also termed BPAG2 and type XVII collagen). These proteins are components of the dermo-epidermal junction and are important components of the adhesion complexes that promote epithelial-stromal adhesion (2). The binding of antibodies to antigens promotes inflammation by activating the complement system and mast cells. Activated inflammatory cells produce proteolytic enzymes that damage the dermo-epidermal junction. Consequently, subepithelial blisters develop.
The prodromal phase of BP is characterized by pruritus and/or urticarial lesions and detection of circulating autoantibodies in the blood1. As the disease progresses, bullae may develop, which are often located on the flexor surface of the trunk, abdomen, forearms, and medial thighs and in the axillae. The fluid in the bullae is clear, and the bullae can persist for days before leaving erosions and crusts that heal without scarring. Unlike other blistering diseases, such as pemphigus vulgaris, the Nikolsky sign is negative in typical cases of BP whereas the Asboe–Hansen sign is positive (3). Damaged skin can lead to secondary Staphylococcus or Streptococcus infections, which can be fatal in elderly patients, in case of sepsis1.
The first-line treatment for BP is systemic corticosteroids; however, the choice of treatment also depends on the disease severity and patients’ comorbidities. In mild cases, potent topical steroids are sufficient, whereas in moderate-to-severe disease, systemic immunosuppressive treatments may be needed, including systemic corticosteroids at dosages of up to 0.5 to 0.75 mg/kg/day for the severe form of BP. This consensus on BP treatment with lower doses of systemic corticosteroids was developed by an international panel of experts in the field of autoimmune blistering disorders (4). Higher doses of glucocorticoids may be more effective in disease control but are not advisable because of the associated risk of adverse effects and increased 1-year mortality (5, 6).
A Finnish study from 2016 indicated that an early initiation of corticosteroid-sparing therapy (CST) and limitation of the systemic steroid dose to a maximum of 0.75 mg/kg/day may increase the survival of BP patients (7). The local guidelines at the Department of Dermatology at Aarhus University Hospital were revised in 2015 to recommend the systematic introduction of CST to BP patients within the first day of admission, in addition to the regular dose of prednisolone 0.5–0.75 mg/kg/day. If the patient did not tolerate prednisolone, tetracycline was administered. Azathioprine 0.5–2.5 mg/kg/day is often used as a steroid-sparing drug. Alternatively, other steroid-sparing drugs such as methotrexate, mycophenolate mofetil, or cyclosporine may be used depending on the individual patient and discretion of the treating doctor. In treatment-refractory cases, intravenous immunoglobulins, plasmapheresis, or rituximab may be administered.
To differentiate between different clinical severities of BP, two scoring systems have been developed: the Autoimmune Bullous Skin Disorder Intensity Score (ABSIS) and the Bullous Pemphigoid Disease Area Index (BPDAI) (8, 9). The BPDAI was developed by the International Pemphigoid Committee and is based on three subcomponents: cutaneous blisters, erythema/urticaria, and mucosal blisters/erosions (8). ABSIS uses a combination of the percentage of body surface involved and a subsequent weighting factor based on whether a lesion is exudative, dry, or re-epithelialized (9). However, these two scoring systems are not always employed in clinics as they are rather comprehensive and, therefore, more suitable for research purposes.
This study aimed to retrospectively describe the demographics, comorbidities, treatment (pre-hospitalization medications; glucocorticoids, including doses; and steroid-sparing drugs), and treatment outcomes (remission, length of admission, relapse, and 1-year mortality) in a cohort of all BP patients referred to a tertiary centre (Department of Dermatology, Aarhus University Hospital) from 2015 to 2021. We hypothesized that consistent application of the new local guidelines (early initiation of CST) in the department would improve the survival rate, lower the rate of complications, and lower the rate of relapse, thereby lowering the number of readmission and length of admission. In this manner, the new guidelines can be evaluated to provide valuable information about the effects of current steroid-sparing treatments. Our secondary objective was to compare our findings regarding comorbidities and pre-hospitalization medications with existing literature to contribute to the understanding of possible associations and epidemiology of BP.
2 Materials and methods
2.1 Design and patients
In this retrospective case-series study, the medical records of all referred patients diagnosed with BP at the Department of Dermatology and Venerology, Aarhus University Hospital, from 2015 to 2021 were investigated (Figure 2). The cohort was a heterogeneous group of patients, some referred from general practitioners as having suspected BP and some from private dermatology practitioners. Patients were identified using the ICD10 system. The diagnoses included in this study were BP (DL 12.0), unspecified pemphigoid (DL 12.9), and other pemphigoids (DL 12.8). The project was reported to the Regional (Region Midtjylland) Record of Research Projects (registration number: 1-16-02-44-22).
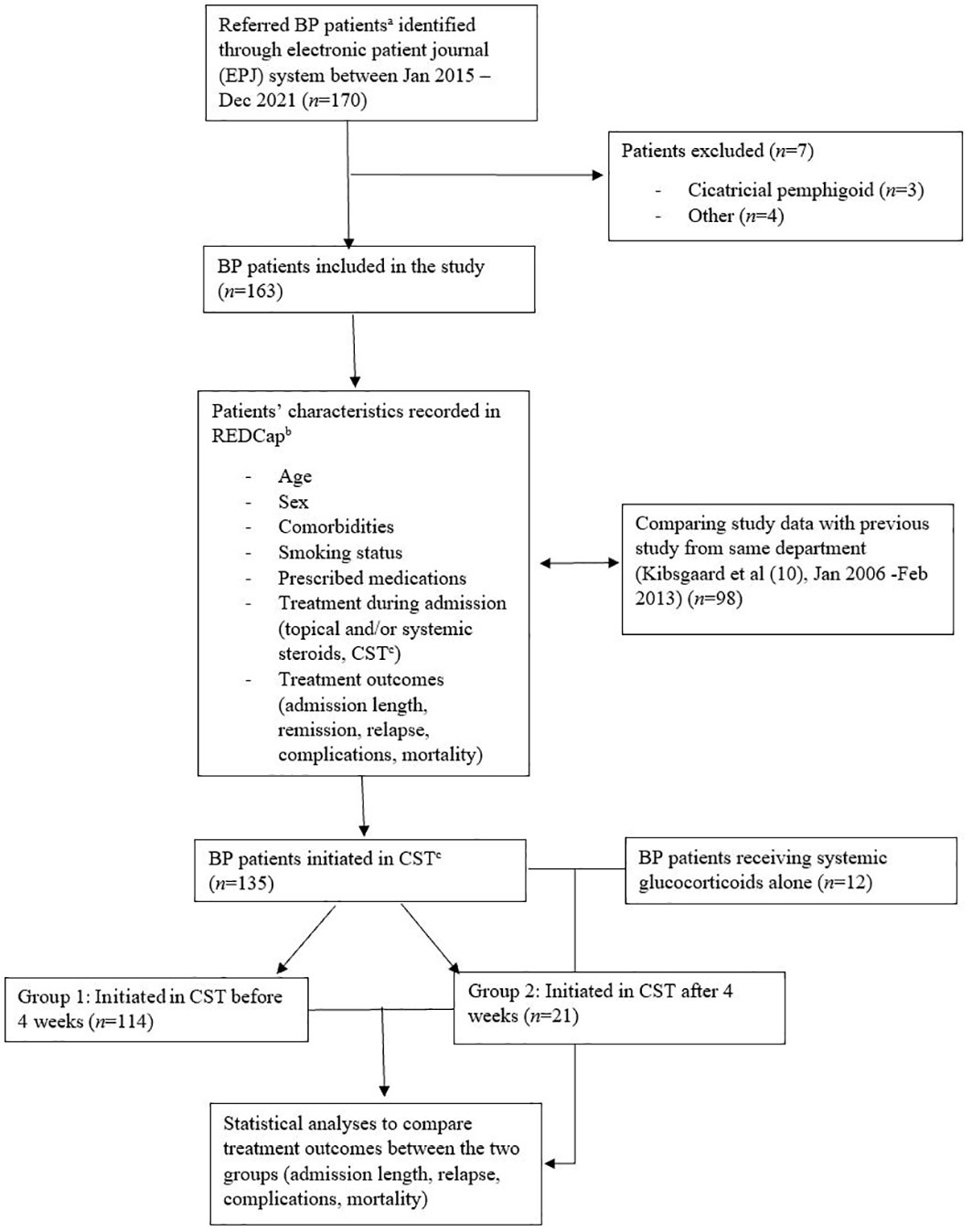
Figure 2 Flow chart of study design and patients. aReferred to the Department of Dermatology and Venerology at Aarhus University Hospital; bThe Research Electronic Data Capture; cCorticosteroid-sparing therapy (CST).
Patient characteristics (age, comorbidities, smoking, and prescribed medicines), treatment during admission, and treatment outcomes (admission length, remission, relapse, and mortality) were recorded using the Research Electronic Data Capture (REDCap) data management platform. Patients were included if characteristic clinical presentations such as bullae and pruritus were found; skin biopsies revealed subepidermal clusters of eosinophils and/or bullae; and/or direct immunofluorescence (IF) showed linear deposits of IgG, IgA, or complement C3 along the basement membrane zone. Patients with primary mucosal involvement were excluded, as this suggested a cicatricial pemphigoid.
The treatment of the referred patients was based on the local guidelines of the Department of Dermatology at Aarhus University Hospital. First-line therapies included potent topical glucocorticoids in combination with prednisolone if needed. Prednisolone was usually administered as 0.5–0.75 mg/kg/day and updosed until effect (no appearance of new blisters). If the patient did not tolerate systemic corticosteroids, tetracycline was administered. Local treatment guidelines recommend the initiation of CST on the day of admission. According to these guidelines, CST can include azathioprine, methotrexate, mycophenolate mofetil, or cyclosporine. In treatment-refractory cases, intravenous immunoglobulins, plasmapheresis, or rituximab can be administered.
2.2 Variables
To assess the outcomes, multiple data from medical records were included in our study. Data such as treatment and dosage, length of admission, readmission, relapse, remission, complications after diagnosis (sepsis and/or diabetes), and 1-year mortality were included. The length of admission was used as a proxy for the disease course, as patients were normally discharged when new bullae did not appear for a minimum of 2 days and primary skin lesions started to re-epithelialize. Frequent clinical control following a fixed scheme after discharge was common practice, and in this manner, relapse or remission was recorded. Remission was defined as the absence of bullae and/or urticaria. Readmission within the first year of diagnosis was interpreted as relapse of BP.
2.3 Data analysis
We used means and standard deviations (SDs) for all continuous variables and percentages for all categorical variables. To test our hypothesis that the early initiation of CST is related to treatment outcomes, all patients that received CST were secondarily dichotomised into two groups. The first group included patients receiving CST within 4 weeks (<28 days), and the second group included patients who received CST after 4 weeks (>28 days). We investigated the association between earlier initiation of CST and treatment outcomes versus late initiation. Furthermore, we compared all patients receiving CST with those who received prednisolone alone. The treatment outcomes were defined as the number of days admitted, relapse rate, rate of complications (sepsis and/or diabetes), and 1-year mortality. To compare the groups (CST before versus after 4 weeks groups and CST versus prednisolone alone group), we used t-tests, which was a two-sample equal variance (homoscedastic) test based on the assumption that the groups originated from the same population. p-values <0.05 were considered statistically significant.
3 Results
3.1 Patients
Between 01/01/2015 and 31/12/2021, a total of 170 patients were identified. Of these patients, three who were retrospectively diagnosed with cicatricial pemphigoid were excluded, along with four patients who were excluded for other reasons. Finally, 163 patients were included in the study (Figure 2).
The age at BP diagnosis ranged from 27 to 100 years with a mean ± SD age of 79 ± 10 years. Of the 163 patients, 94 (58%) were men and 69 (42%) were women (Table 1).
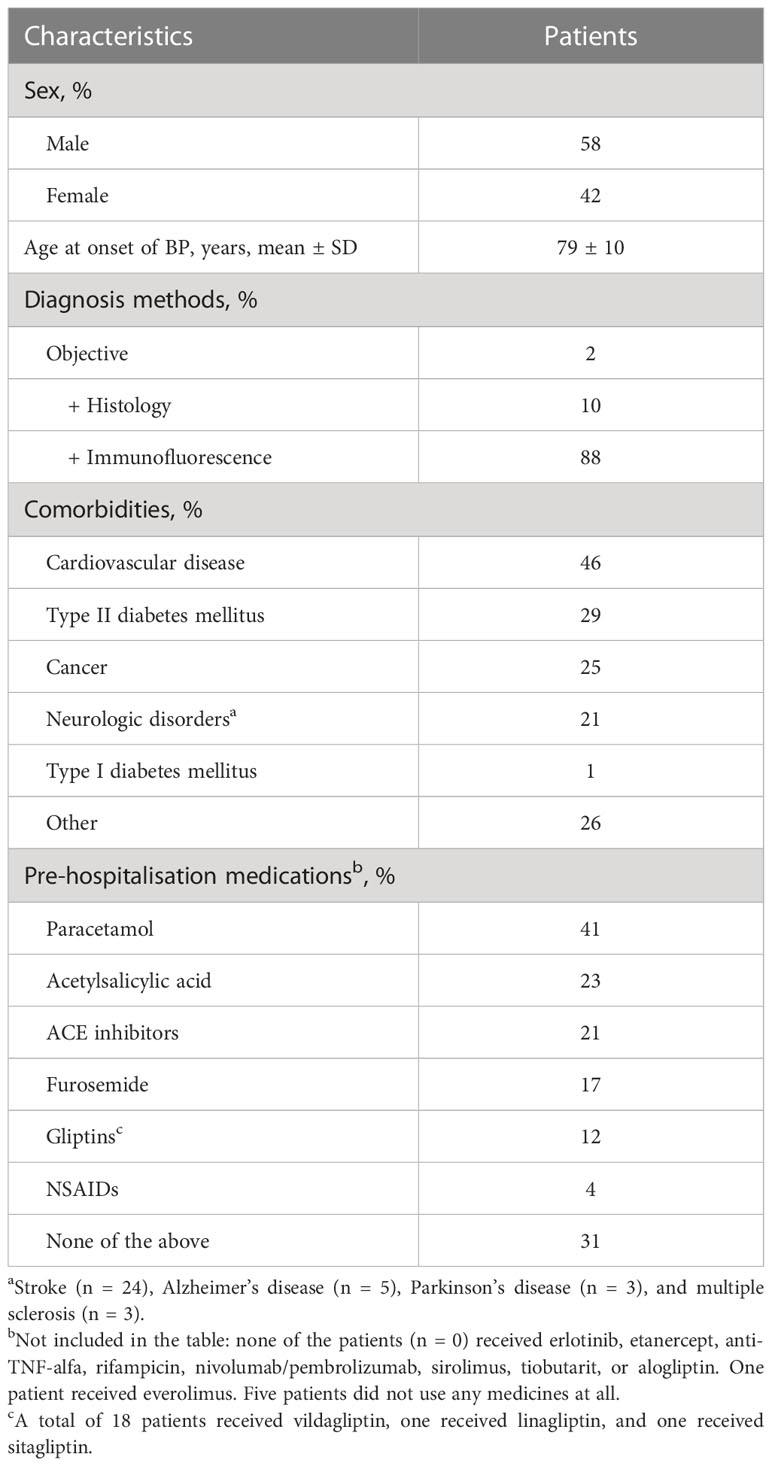
Table 1 Baseline characteristics of patients admitted with bullous pemphigoid (n = 163) during the study period (Jan 2015–Dec 2021).
BP diagnosis was based on clinical, histological, and immunofluorescence in 143 (88%) of the 163 patients.
As for comorbidities, the most common comorbidity was cardiovascular diseases (CVDs), which was present in 75 patients (46%), followed by type II diabetes mellitus (DM), which was present in 48 patients (29%), and neurological disorders, including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, and stroke, which was present in 35 patients (21%) (Table 1).
Before hospitalization, the patients were most commonly treated with paracetamol (41%), acetylsalicylic acid (23%), angiotensin-converting-enzyme (ACE) inhibitors (21%), furosemide (17%), and gliptins (12%). None of the included patients were treated with nivolumab, erlotinib, etanercept, rifampicin, or sirolimus at the time of admission (Table 1). These drugs have been associated with the development of BP (2).
3.2 Treatment outcomes
Of the 163 patients, 106 (65%) were initiated with systemic glucocorticoids. The initial doses ranged from 5 to 50 mg, with a mean ± SD of 25 ± 11 mg (Table 2). Of the remaining 57 patients who were not initiated on systemic glucocorticoids at time of the first visit, 23 (40%) were initiated subsequently. We found that 131 (80%) of the 163 patients were initially treated with topical glucocorticoid group 4; 30 and 20% were treated with group 3 and 2 steroids, respectively. Whether the topical treatment was used only on the lesions or whole body (except face and anogenital region) varied based on clinical severity and doctor’s discretion. In addition to topical steroids, some patients also received systemic steroids and/or CST.
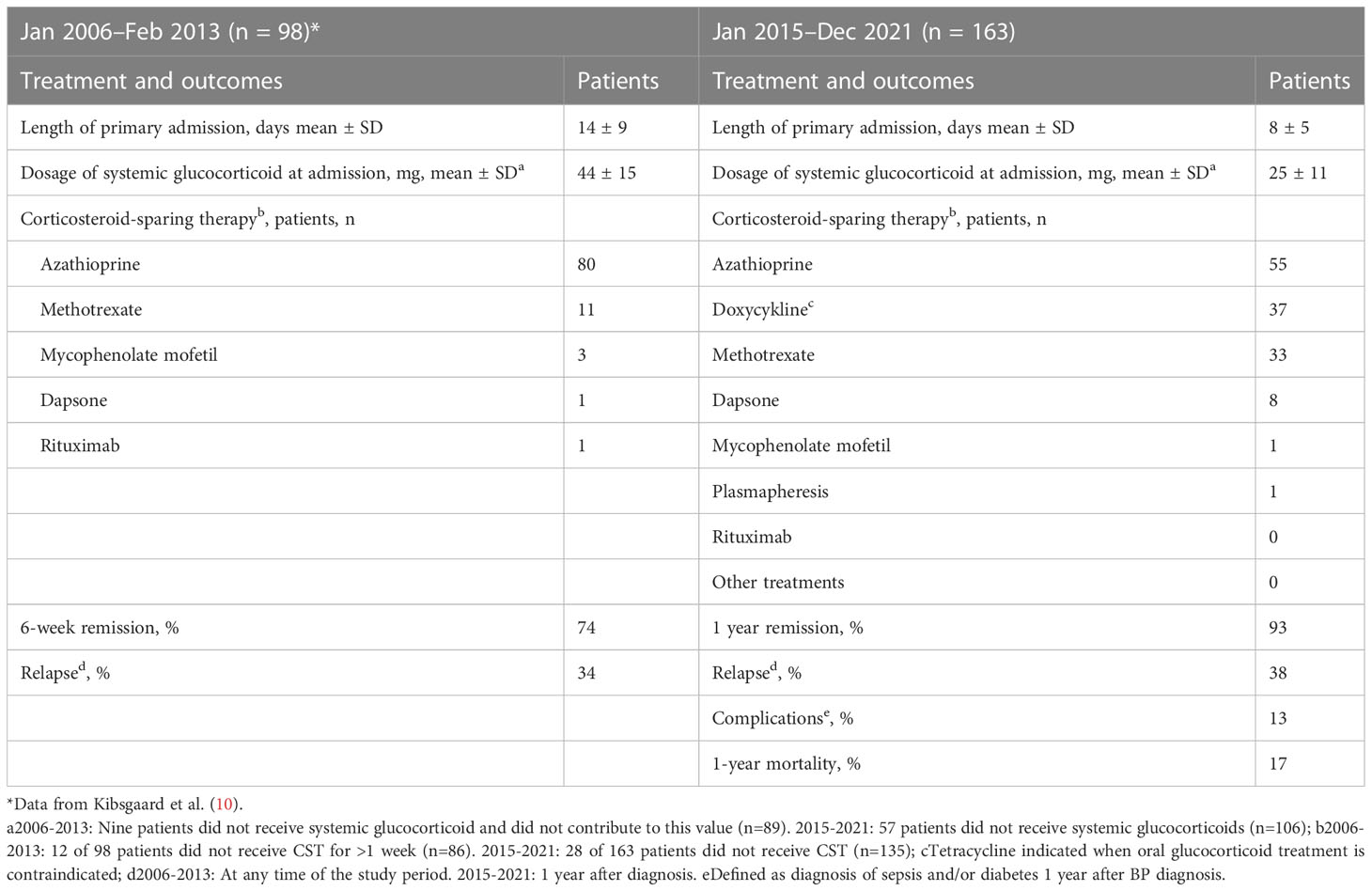
Table 2 Comparison of treatment and treatment outcomes in patients with bullous pemphigoid at the Department of Dermatology and Venereology at Aarhus University Hospital in two different time periods.
Of the 163 patients, 135 (83%) were initiated on CST. The choice of CST was based on an individual assessment by taking into consideration comorbidities (CVD or existing/prior neoplasm), kidney and liver function, age, and performance status. Azathioprine was the most frequently used CST (n = 55), followed by doxycycline (n = 37) and methotrexate (n = 33; Table 2). Eight patients received dapsone as adjuvant CST. One patient was treated with mycophenolate mofetil and one with plasmapheresis. None of the patients were treated with rituximab during the study period. The number of days from diagnosis until the initiation of CST ranged from 0 to 719 days, with a mean of 3 days. For admitted patients, the number of days ranged from 0 to 120 days, with a mean of 1 day. For the non-admitted patients, the number of days ranged from 0 to 719 days, with a mean of 8 days (Figure 3).
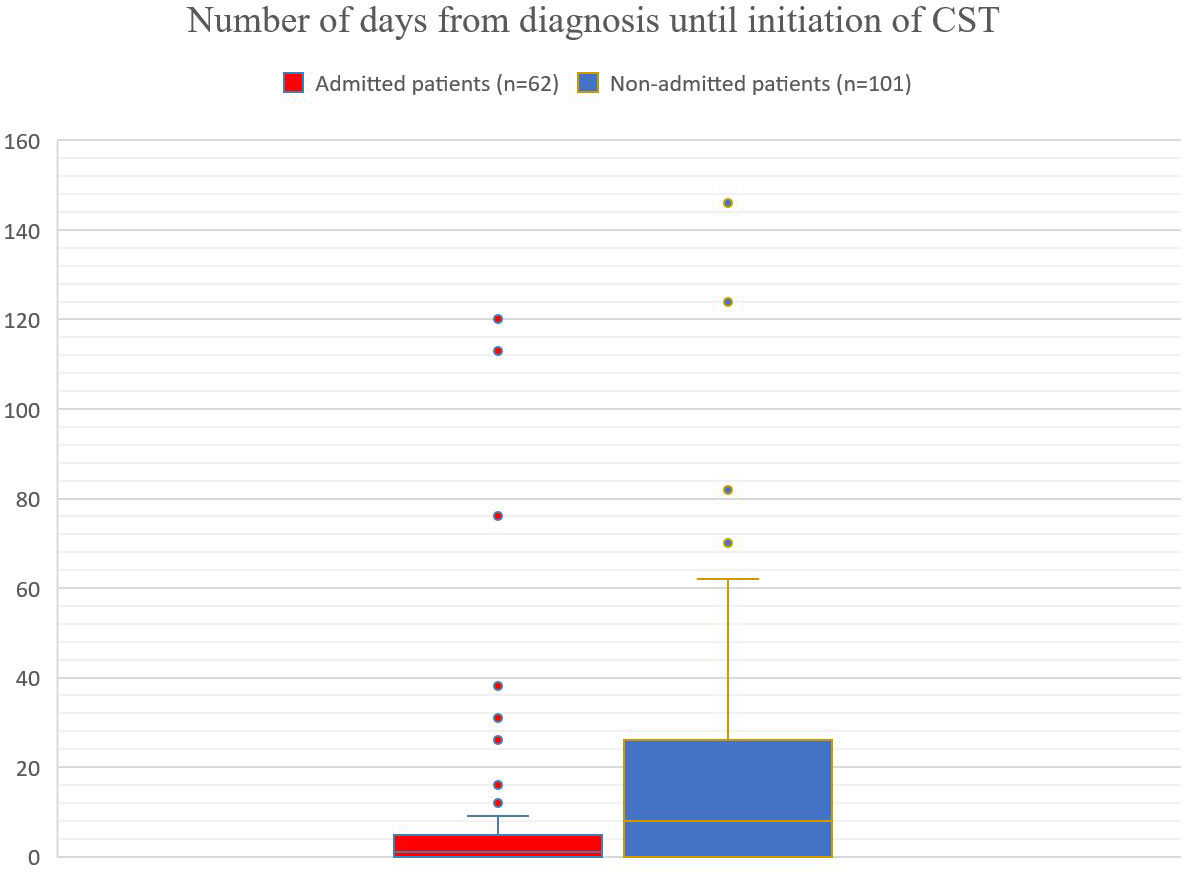
Figure 3 Admitted patients (red): mean of 1 day, number of days ranged from 0 to 120 days, with an upper quartile (75th percentile) of 5 days. Non-admitted patients (blue): mean of 8 days, number of days ranged from 0 to 719 days, with an upper quartile (75th percentile) of 26 days.
At the time of diagnosis 62 (38%) out of the 163 patients were admitted to the hospital because of the severity of their BP disease. The number of days admitted ranged from 1 to 26, days with a mean ± SD of 8 ± 5 days (Table 2). Within the first year after BP diagnosis, 15 (24%) of the 62 admitted patients were readmitted. Of the 163 patients, 151 (93%) were classified as having remission of the disease within the first year and 141 (87%) did not have complications such as sepsis or diabetes after diagnosis. Overall, 17% of the patients died within the first year after diagnosis.
We found that 114 (84%) of those 135 patients initiated on CST were initiated on CST within 28 days (early initiation of CST) and 21 (16%) were initiated after 28 days (late initiation of CST).
In the CST <28 days group, the number of days admitted ranged from 1 to 26 days, with a mean ± SD of 8 ± 5 days, whereas in the CST >28 days group, this number ranged from 1 to 13 days, with a mean ± SD of 8 ± 5 days (p = 0.49). The rates of complications (sepsis and/or diabetes 1 year after diagnosis) were 15% and 19% (p = 0.63), the relapse rates were 38% and 62% (p < 0.05), and the 1-year mortality was 17% and 14% (p = 0.79) in the CST <28 days and CST >28 days groups, respectively (Table 3).
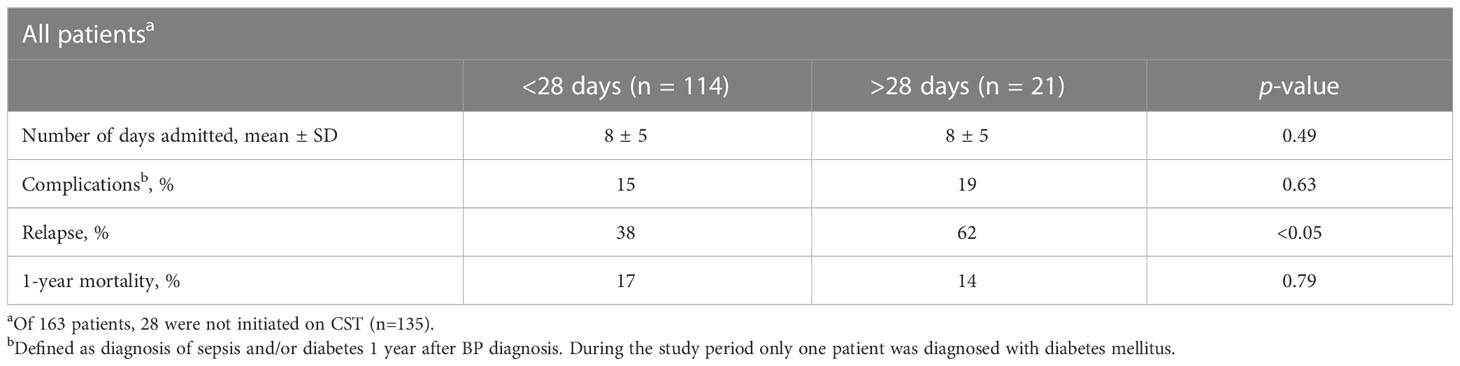
Table 3 Treatment outcomes stratified by the number of days until the initiation of CST.
Only 12 patients (7%) were treated with prednisolone alone, whereas 135 (83%) were treated with CST. Compared with the CST group in which 46% of the patients were admitted to the hospital, none of those treated with prednisolone alone were admitted. The relapse rates were 33% and 42% (p = 0.55), the rates of complications were 8% and 16% (p = 0.50), and the 1-year mortality was 33% and 16% (p = 0.14) in the prednisolone alone and CST groups, respectively. None of the abovementioned data were statistically different between the prednisolone alone and CST groups.
4 Discussion
The rate of complications and 1-year mortality did not differ significantly between the groups that initiated early (<28 weeks) or late (>28 weeks) corticosteroid-sparing therapy (CST). Instead, we found a minor increase in 1-year mortality in the <28-days group (17% vs. 14%, p = 0.79). However, the relapse rate was significantly different between the groups (p < 0.05), where those initiated early on CST had fewer relapses. This suggests a positive effect of the early initiation of steroid-sparing drugs. However, the relapse rate may be biased by patient compliance and disease severity; therefore, the outcome must be interpreted with caution.
Considering our cohort and its rather small size (compared with other cohorts of more prevalent diseases), finding significant results can be challenging. By performing a quick power calculation of our two subgroups and outcome relapse, the minimum powerful sample size was 134. As we had a cohort of 135 patients initiated on CST, there were theoretically enough patients to provide our study with statistical power.
There were 163 BP patients referred to the Department of Dermatology and Venerology from 2015 to 2021. This is an increase compared with an almost identical study by Kibsgaard et al. conducted from 2006 to 2013 within the same department (10). Kibsgaard et al. reported that 98 BP patients were referred to the Department of Dermatology during a 7-year study period from 2006 to 2013 (10). The increased number of BP patients could be due to several factors, including a continuously increasing proportion of the elderly population and/or better diagnostics of BP. Additionally, the same trend of an increasing incidence of BP patients has been observed in several other countries the last decades (11, 12). Moreover, other causal factors such as a higher prevalence of neurological diseases have been shown to increase the risk of developing BP (13). The same inclusion criteria were used in Kibsgaard et al.’s study and this study. Therefore, the increased number of referred BP patients may reflect an actual increase in the incidence of BP in the Danish population.
In this study, 38% of the referred patients were admitted to the hospital because of the severity of their BP disease. This was not only due to high disease activity and need for intensive therapy with intravenous treatments in some cases but also because of comorbidities, as all the admitted patients were initiated on CST to reduce the use of systemic steroids.
The time from BP diagnosis to the initiation of CST varied from 0 to 719 days, with a mean of 3 days (Figure 3). In the group of admitted patients, the mean was only 1 day, and 75% of the admitted patients were initiated on CST within 5 days. On the other hand, in the group of non-admitted patients, the mean was 8 days, and 75% of the patients were initiated within almost 4 weeks (26 days). Thus, the admitted patients experienced earlier initiation of CST. This supports more strictly application of our treatment guidelines in patients admitted to our inpatient ward compared with those treated in our outpatient clinic. There should be no differences in the handling of admitted/non-admitted patients.
We found no difference in treatment outcomes when comparing the group of BP patients treated with prednisolone alone and those treated with prednisolone in combination with CST (early and late initiation). Although it was a higher mortality in the prednisolone alone group, this was of no significance (p = 0.14). This might reflect the fact that only 12 patients were treated with prednisolone alone, and it was impossible to obtain statistical significance. On the other hand, this again reflects that we adhered to our local treatment guidelines for the initiation of CST in BP patients.
The time of admission was shorter in this study (mean [± SD]: 8 [± 5] days) than in the study by Kibsgaard et al. (mean [± SD]: 14 [± 9] days) (Table 2). This reduction in admission time may indicate more effective management of the acute phase of the disease. Furthermore, we found a decreased initial dose of prednisolone (from a mean ± SD of 44 ± 15 mg in Kibsgaard et al.’s study to 25 ± 11 mg in this study). However, we did not find any changes in the overall remission or relapse (34% in Kibsgaard et al.’s study, 38% in this study) of BP between the two study periods.
The 1-year mortality of 17.2% in this study was similar to that of 16.7% reported in a study from Finland conducted by Försti et al. (7). Finland is comparable with Denmark in several aspects, particularly demographics (for instance, having an older age structure), the incidence of BP, and treatment methods for BP. The 1-year mortality for citizens aged >70 years was approximately 5.4% in 2018 in Denmark2. Thus, BP patients have an increased mortality rate compared with the general population of the same age group, which has been confirmed in several studies, including this study (14–16).
Considering the epidemiological aspects of this study, there was a decreased rate of CVDs of 46% versus 70% in Kibsgaard et al.’s study (10). Few studies have demonstrated an association between CVD and BP. However, Kibsgaard et al.’s study and Försti et al.’s of 198 BP patients (7) both found CVD as the most common comorbidity. This was also observed in the present study. Recent studies have demonstrated BP association with hypertension (17, 18). Lee et al. found a significant adjusted odds ratio of 2.03 [95% CI 1.24–3.32] of BP when having hypertension (18). The present study did not differentiate between different types of CVD; therefore, the proportion of patients with hypertension was unknown. However, the possible association between specific forms of CVD and BP is an interesting aim for further research.
In this study, CVD was the most common comorbidity, followed by type II DM (29%), cancer (25%), and neurological diseases (21%). There are hypotheses of cross-reactions against BP230 isotopes, where the autoantibody binds to both antigens expressed in neurological tissues and the basement membrane of human skin (19). This suggests an association between BP and neurodegenerative disorders. A larger case–control study from Denmark revealed a significantly increased frequency of multiple sclerosis (MS) among BP patients, with a risk of developing MS more than five times higher than that in the background population (19). As this was a retrospective descriptive study and not a follow-up study, we could not conclude any association between MS and BP based on our findings. Three patients of our cohort had MS as a comorbidity at the time of BP diagnosis.
As mentioned earlier, several drugs have been reported to increase the risk of developing BP, including antihypertensive drugs, anti-inflammatory drugs, diuretics, antirheumatic drugs, vaccines, and gliptins. The most frequent drugs used in our cohort were paracetamol (41%), acetylsalicylic acid (23%), and ACE inhibitors (21%). This may be explained by the advanced age and multiple comorbidities of our patients. In our cohort, 12% of the patients used gliptins, in total 18 received vildagliptin, one received linagliptin, and one received sitagliptin. In the last years of BP research, the use of dipeptidyl peptidase-4 inhibitors (particularly vildagliptin and linagliptin) for the treatment of DM has been investigated and has shown to be significantly associated with BP (20). The Danish Endocrine Society suggests alogliptin, linagliptin, and sitagliptin as first-line drugs if there is indication for using gliptins in the treatment of DM. Therefore, it is interesting that 18 out of 20 of our gliptin users were prescribed vildagliptin. Vildagliptin has in several studies been shown to have the highest association with BP compared with other gliptins (21). Lastly, there has been an increase in the use of non-insulin, glucose-lowering drugs such as gliptins the last decade in Denmark, and in 2021, 7.5% of the type II DM population in Denmark used gliptins (22). In comparison, we found 42% of our type II DM BP patients using gliptins. In conclusion, our results may support the rising evidence of gliptin-associated BP.
The strengths of this study were a long study period and the substantial percentage of patients (almost 90%) with a BP diagnosis based on histology, direct IF, and clinical presentation. The limitations of this study were the lack of assessment of BP severity, for example, using the ABSIS or BPDAI disease scores, which could have provided more specific information on the disease stage, and hence, the possible effect of early initiation of CST. Therefore, the results must be interpreted with caution. Furthermore, we could have confirmed the BP diagnosis by performing serological tests for autoantibodies against BP180 and/or BP230. Consequently, we have now adapted this as a routine practice in our department. Another limitation that may have affected our results was selection bias, as our department consulted the most severe cases within a limited geographic region. However, the fact that the same standard guidelines were used and that, in this study, these guidelines were followed quite consequently by the department specialists indicates the strength of this study and its results.
5 Conclusion
The rate of complications and 1-year mortality did not differ significantly between the groups that initiated early (<28 weeks) or late (>28 weeks) CST. However, the rate of relapse was lower in the group with early initiation of CST. When comparing the outcomes of patients treated with prednisolone alone with those of patients treated with CST, we found no difference.
Furthermore, we found that the initial dose of prednisolone and admission time were reduced in this study compared with those reported in a similar study conducted before the implementation of a local treatment guideline recommending the early initiation of CST. Thus, the initial prednisolone dose was reduced after a change in the treatment guidelines for BP patients; however, further studies are needed to clarify whether the reduced prednisolone dose lowers the risk of adverse outcomes and mortality in these patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
RB, AF, CV conceived of the study, made the design, and coordinated the study. AF provided all patient data. GO collected the epidemiological data. GO and IF performed the interpretation of data. IF performed the statistical analysis, interpreted the results, and composed the discussion. RB, AF, CV contributed to drafting and critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We highly appreciate all contributors to this project at the Department of Dermato-Venereology at Aarhus University Hospital. We also deeply appreciate the work of doctor Detlef Zillikens, and his mutual contribution to our understanding and handling of autoimmune blistering disorders of the skin.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
- ^ Lægehåndbogen at Sundhed.dk. Pemfigoid (2022). https://www.sundhed.dk/sundhedsfaglig/laegehaandbogen/hud/tilstande-og-sygdomme/bulloese-tilstande/pemfigoid/ [Accessed May 1, 2022].
- ^ «Number of deaths» from Statistic Denmark. (2018). https://www.dst.dk/en/Statistik/emner/borgere/befolkning/doedsfald [Accessed February 23, 2023].
References
1. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet (2013) 381(9863):320–32. doi: 10.1016/S0140-6736(12)61140-4
2. Moro F, Fania L, Sinagra JLM, Salemme A, Di Zenzo G. Bullous pemphigoid: trigger and predisposing factors. Biomolecules (2020) 10(10):1–2. doi: 10.3390/biom10101432
3. Hammers CM, Stanley JR. Mechanisms of disease: pemphigus and bullous pemphigoid. Annu Rev Pathol (2016) 11:175–97. doi: 10.1146/annurev-pathol-012615-044313
4. Borradori L, Van Beek N, Feliciani C, Tedbirt B, Antiga E, Bergman R, et al. Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European academy of dermatology and venereology (EADV). J Eur Acad Dermatol Venereol (2022) 36(10):1689–704. doi: 10.1111/jdv.18220
5. Joly P, Roujeau JC, Benichou J, Picard C, Dreno B, Delaporte E, et al. A comparison of oral and topical corticosteroids in patients with bullous pemphigoid. N Engl J Med (2002) 346(5):321–7. doi: 10.1056/NEJMoa011592
6. Rzany B, Partscht K, Jung M, Kippes W, Mecking D, Baima B, et al. Risk factors for lethal outcome in patients with bullous pemphigoid: low serum albumin level, high dosage of glucocorticosteroids, and old age. Arch Dermatol (2002) 138(7):903–8. doi: 10.1001/archderm.138.7.903
7. Försti AK, Jokelainen J, Timonen M, Tasanen K. Risk of death in bullous pemphigoid: a retrospective database study in Finland. Acta Derm Venereol (2016) 96(6):758–61. doi: 10.2340/00015555-2347
8. Murrell DF, Daniel BS, Joly P, Borradori L, Amagai M, Hashimoto T, et al. Definitions and outcome measures for bullous pemphigoid: recommendations by an international panel of experts. J Am Acad Dermatol (2012) 66(3):479–85. doi: 10.1016/j.jaad.2011.06.032
9. Pfütze M, Niedermeier A, Hertl M, Eming R. Introducing a novel autoimmune bullous skin disorder intensity score (ABSIS) in pemphigus. Eur J Dermatol (2007) 17(1):4–11. doi: 10.1684/ejd.2007.0090
10. Kibsgaard L, Bay B, Deleuran M, Vestergaard C. A retrospective consecutive case-series study on the effect of systemic treatment, length of admission time, and co-morbidities in 98 bullous pemphigoid patients admitted to a tertiary centre. Acta Derm Venereol (2015) 95(3):307–11. doi: 10.2340/00015555-1925
11. Persson MSM, Harman KE, Vinogradova Y, Langan SM, Hippisley-Cox J, Thomas KS, et al. Incidence, prevalence and mortality of bullous pemphigoid in England 1998-2017: a population-based cohort study. Br J Dermatol (2021) 184(1):68–77. doi: 10.1111/bjd.19022
12. Thorslund K, Seifert O, Nilzén K, Grönhagen C. Incidence of bullous pemphigoid in Sweden 2005-2012: a nationwide population-based cohort study of 3761 patients. Arch Dermatol Res (2017) 309(9):721–7. doi: 10.1007/s00403-017-1778-4
13. Langan SM, Groves RW, West J. The relationship between neurological disease and bullous pemphigoid: a population-based case-control study. J Invest Dermatol (2011) 131(3):631–6. doi: 10.1038/jid.2010.357
14. Brick KE, Weaver CH, Lohse CM, Pittelkow MR, Lehman JS, Camilleri MJ, et al. Incidence of bullous pemphigoid and mortality of patients with bullous pemphigoid in Olmsted county, Minnesota, 1960 through 2009. J Am Acad Dermatol (2014) 71(1):92–9. doi: 10.1016/j.jaad.2014.02.030
15. Joly P, Baricault S, Sparsa A, Bernard P, Bédane C, Duvert-Lehembre S, et al. Incidence and mortality of bullous pemphigoid in France. J Invest Dermatol (2012) 132(8):1998–2004. doi: 10.1038/jid.2012.35
16. Cortés B, Marazza G, Naldi L, Combescure C, Borradori L. Mortality of bullous pemphigoid in Switzerland: a prospective study. Br J Dermatol (2011) 165(2):368–74. doi: 10.1111/j.1365-2133.2011.10413.x
17. Shen WC, Chiang HY, Chen PS, Lin YT, Kuo CC, Wu PY. Risk of all-cause mortality, cardiovascular disease mortality, and cancer mortality in patients with bullous pemphigoid. JAMA Dermatol (2022) 158(2):167–75. doi: 10.1001/jamadermatol.2021.5125
18. Lee S, Rastogi S, Hsu DY, Nardone B, Silverberg JI. Association of bullous pemphigoid and comorbid health conditions: a case-control study. Arch Dermatol Res (2021) 313(5):327–32. doi: 10.1007/s00403-020-02100-2
19. Kibsgaard L, Rasmussen M, Lamberg A, Deleuran M, Olesen AB, Vestergaard C. Increased frequency of multiple sclerosis among patients with bullous pemphigoid: a population-based cohort study on comorbidities anchored around the diagnosis of bullous pemphigoid. Br J Dermatol (2017) 176(6):1486–91. doi: 10.1111/bjd.15405
20. Tasanen K, Varpuluoma O, Nishie W. Dipeptidyl peptidase-4 inhibitor-associated bullous pemphigoid. Front Immunol (2019) 10. doi: 10.3389/fimmu.2019.01238
21. Arai M, Shirakawa J, Konishi H, Sagawa N, Terauchi Y. Bullous pemphigoid and dipeptidyl peptidase 4 inhibitors: a disproportionality analysis based on the Japanese adverse drug event report database. Diabetes Care (2018) 41(9):e130–e2. doi: 10.2337/dc18-0210
Keywords: bullous pemphigoid, steroid-sparing treatment, immunomodulatory treatment, glucocorticoids, relapse, mortality, cardiac disease
Citation: Fenne IJ, Askildsen Oftebro G, Vestergaard C, Frølunde AS and Bech R (2023) Effect of early initiation of steroid-sparing drugs in patients with bullous pemphigoid. Front. Immunol. 14:1176284. doi: 10.3389/fimmu.2023.1176284
Received: 28 February 2023; Accepted: 15 June 2023;
Published: 06 July 2023.
Edited by:
Enno Schmidt, University of Lübeck, GermanyReviewed by:
Daisuke Tsuruta, Osaka City University, JapanBranka Marinovic, University Hospital Centre Zagreb, Croatia
Aikaterini Patsatsi, Aristotle University of Thessaloniki, Greece
Copyright © 2023 Fenne, Askildsen Oftebro, Vestergaard, Frølunde and Bech. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inger Johanne Fenne, MjAxNjEwMTU1QHBvc3QuYXUuZGs=