
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 22 May 2023
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1171649
This article is part of the Research TopicCommunity Series in Novel Biomarkers for Predicting Response to Cancer Immunotherapy, volume IIView all 19 articles
 Julien Ancel1,2*
Julien Ancel1,2* Valérian Dormoy1
Valérian Dormoy1 Béatrice Nawrocki Raby1
Béatrice Nawrocki Raby1 Véronique Dalstein1,3
Véronique Dalstein1,3 Anne Durlach1,3Maxime Dewolf2
Anne Durlach1,3Maxime Dewolf2 Christine Gilles4
Christine Gilles4 Myriam Polette1,3
Myriam Polette1,3 Gaëtan Deslée1,2
Gaëtan Deslée1,2Lung cancer remains the first cause of cancer-related death despite many therapeutic innovations, including immune checkpoint inhibitors (ICI). ICI are now well used in daily practice at late metastatic stages and locally advanced stages after a chemo-radiation. ICI are also emerging in the peri-operative context. However, all patients do not benefit from ICI and even suffer from additional immune side effects. A current challenge remains to identify patients eligible for ICI and benefiting from these drugs. Currently, the prediction of ICI response is only supported by Programmed death-ligand 1 (PD-L1) tumor expression with perfectible results and limitations inherent to tumor-biopsy specimen analysis. Here, we reviewed alternative markers based on liquid biopsy and focused on the most promising biomarkers to modify clinical practice, including non-tumoral blood cell count such as absolute neutrophil counts, platelet to lymphocyte ratio, neutrophil to lymphocyte ratio, and derived neutrophil to lymphocyte ratio. We also discussed soluble-derived immune checkpoint-related products such as sPD-L1, circulating tumor cells (detection, count, and marker expression), and circulating tumor DNA-related products. Finally, we explored perspectives for liquid biopsies in the immune landscape and discussed how they could be implemented into lung cancer management with a potential biological–driven decision.
Lung cancer represents the first cause of cancer‐related deaths worldwide with over 1.5 million deaths in 2018 and an incidence superior to 2 million (11.6%), largely represented by non-small cell lung cancer (NSCLC) (1). Lung cancer is diagnosed at a locally advanced or metastatic stage in most cases, leading to no curative options and poor outcomes (2). In recent decades, many innovative strategies have been designed, namely tyrosine kinase inhibitors (TKIs) targeting oncogenic drivers or immunotherapies (3). On the one hand, personalized medicine based on molecular targetable alterations has emerged from proof of concept to current clinical applications with restricted indications to a sub-population (4). On the other hand, immune checkpoint inhibitors (ICI) are now largely employed but obtain various response rates with fewer than 40% of responders among a population selected on programmed death-ligand 1 (PD-L1) expression (5).
Many biomarkers have been investigated through the last decades to improve clinical cancer management and patient outcomes. First, biomarkers designed to predict better, and longer responses have been proposed, such as PD-L1. PD-L1 expression in tumor biopsy is the strategy that allows identifying a subpopulation of patients benefiting from ICI. For example, patients with a high PD-L1 tumor proportion score (TPS ≥ 50%) benefit from ICI in first-line (vs platinum-based chemotherapy) (6–8). However, resistance and relapse fatally occur in most cases. Consequently, global age-standardized 5-year survival remains within the range of 10-20% and a limited increase of up to 5% has been observed (9), arguing the need to further refine and improve clinical lung cancer management. Therefore, other approaches have been explored in plasma or total blood. Soluble biomarkers have the advantages to allow real-time monitoring, repeatable, and easily feasible at every step of lung cancer (from the diagnosis throughout the progression of the disease) including non-evaluable radiographic diseases, named biological minimal residual diseases (MRD) (10). Liquid biopsy is now even integrated into clinical practice to research and/or monitor oncogenic addiction under TKI treatment (11). Circulating tumor-derived products are various and offer wide potential applications, especially in the ICI field (12). Inflammation-related biomarkers are particularly promising since inflammation is associated with a worse prognosis in solid tumors due to its effect on the immune modulation, into both tumor cells and its microenvironment, influencing disease-related outcomes (13). These biomarkers include immunoregulatory cells, soluble mediators, and a panel of features including absolute neutrophil, eosinophil, lymphocyte counts, or ratios (14). To date, no soluble biomarker has yet been approved and validated for the management of lung cancer patients, despite important recent technical advances. In this context, there is an emerging interest to identify one to predict ICI benefit, overcoming limitations due to tissue-based analysis (15).
Numerous serum-based biomarkers have already been explored or are currently under investigation. Among the most promising, the blood cell count of neutrophils, lymphocytes, and platelets have been associated with ICI efficacy with potential prognostic value (15). Other promising serum-based biomarkers include soluble PD-L1 (sPD-L1) (16), circulating tumor cells (CTCs) (17), blood tumor mutational burden (bTMB), or circulating tumor DNA (ctDNA) (18). Figure 1 – Graphical Abstract.
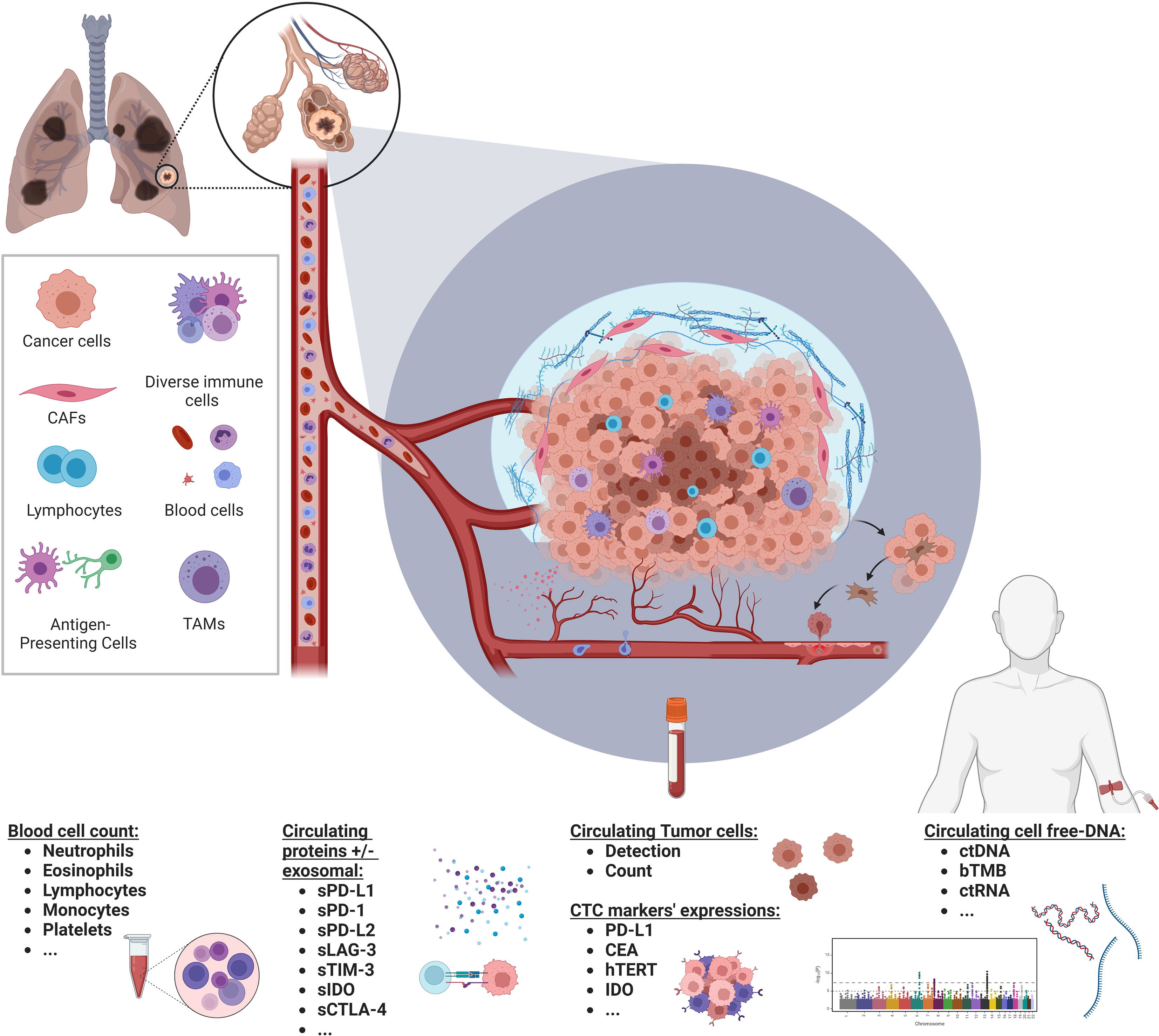
Figure 1 Soluble biomarkers in the immune landscape of NSCLC. Graphical abstract illustrating various types of soluble biomarkers with potential clinical relevance in the immunotherapy field in a non-small cell lung cancer context. Created with BioRender.com.
In this review, we discuss the potential relevance of such soluble biomarkers associated with clinical outcomes in NSCLC treated by ICI. We also analyzed their limitations precluding their implementation into clinical management. Finally, we selected active clinical trials exploring soluble biomarkers in NSCLC treated by ICI focusing on how their results could be integrated into clinical practice.
Systemic inflammation is a well-known related condition impacting tumor responses under ICI treatment in solid cancers (19). Cytokine profiles are thus modified in case of an inflammatory tumor with high IL-6 and TNF-α levels, affecting myelopoiesis (20), and resulting in a shift in blood-cell numerations. Neutrophils and other immune cells such as lymphocytes, platelets myeloid-derived suppressor cells, and monocytes also secrete proinflammatory cytokines (i.e. VEGF, IL-6/8, or TGF-beta) (21). Considering that these circulating immune cells also represent a broad part of ICI therapy effectors, immune cell count was evaluated in serum to predict ICI efficacy. Here under we review the impact of neutrophils, lymphocytes, and platelets, and their variation (Δ) in the case of longitudinal monitoring of clinical outcomes under ICI treatment.
Absolute neutrophil count (ANC), as a predictor for ICI response, has been investigated in many studies. The largest included 213 patients, retrospectively comparing biological profiles between long-term responders and non-long-term responders (22). Δ ANC decreased at 4 weeks and was associated with longer responses (p=0.018). In another large retrospective cohort of 191 patients, lower ANC at baseline was associated with better OS (p=0.048) with similar observations at first re-evaluation (23). All other studies were concordant with these results, despite ICI heterogeneity and thresholds. The principal ANC cut-off was 6.0 103/µL, whereas some authors proposed higher values until 7.5 103/µL (24). The main limitation for ANC integration in current practice to predict ICI outcomes remain a restricted number of studies. Moreover, ICI combined with chemotherapy could involve G-CSF stimulation, hardening Δ ANC interpretation in this context.
Absolute eosinophil count (AEC) was investigated in a few studies. The largest enrolled 191 patients, mostly treated with Nivolumab (n=100) and Pembrolizumab (n=58) (23). Interestingly, the authors reported an induced early increase in AEC, more frequently in responding patients, independently of PD-L1 and immune-related adverse events (p<0.001). Other studies tended to be negative regarding AEC as a predictor of ICI response. Otherwise, many parameters could influence AEC such as corticosteroids in premedication (for chemotherapy combination or palliative radiotherapy support). The interest of AEC thus appears limited for further studies to predict ICI response.
Absolute lymphocyte count (ALC) was extensively assessed, broadly co-evaluating lymphocyte ratio as described in the following sections. Murakami et al. conducted the largest study, with 213 patients, all treated with Nivolumab (22). ALC was not associated with ICI outcomes. Two other studies equally dimensioned with 203 and 191 patients respectively, were consistent despite various anti-PD-1 and anti-PD-L1 drugs: ALC did not differ according to ICI response (23, 25).
Flow cytometry (FC) allows a deep analysis of peripheral blood cell subpopulations such as myeloid-derived suppressor cells (MDSCs) and their sub-populations including monocytic myeloid-derived suppressor cells (M-MDSCs) and granulocytic MDSC (G-MDSCs) (26). Both tissular MDSCs and circulating subset play an important immunosuppressive role and negative effect on ICI in animal tumor models (27). Due to their immunosuppressive effects, MDSCs exhibit protumoral effects and associate with poorer prognosis. Thus, Bronte et al. reported in a meta-analysis pooling 14 studies (905 NSCLC patients) that high level of circulating M-MDSCs was associated with short PFS (HR=2.67, p<0.0001) and OS (HR=2.10, p<0.0001) (28). The proof of concept was established in a melanoma context treated by ICI (i.e ipilimumab) with a benefit from ICI in patients with low frequencies of M-MDSCs (29). In NSCLC, various reports are available in the ICI context. Feng et al. observed a rapid increase in NK cell fraction in 27 NSCLC patients responding to nivolumab, along with a reduction of G-MDSCs (30). Similar results were reported in a cohort of 132 NSCLC patients treated by anti-PD-1 therapy: lower levels of circulating M‐MDSCs, polymorphonuclear (PMN)‐MDSCs, and CD39+CD8+ T cells at baseline were associated with longer PFS and OS (31). In the same report, PD-L1 TPS was not correlated with the proportions of suppressive immune cells, including PMN-MDSCs and M-MDSCs, or with the clinical outcome. This was concordant with another report based on 22 NSCLC patients: patients with M-MDSC values upper than the median experienced shorter PFS (HR=2.51, p=0.046) and OS (HR=2.68, p=0.042) (32). FC could both assess pro and anti-tumor cell subsets such as regulatory T cells and MDSCs. Kim et al. thus proposed that the ratio between peripheral regulatory T cells to lox-1+ PMN MDSCs could predict the early response to ICI in NSCLC patients (33). Similarly, Youn et al. reported in 62 NSCLC patients that the NK cell-to-Lox-1+ PMN-MDSC ratio was significantly higher in patients benefiting from ICI (p<0.0001) (34). FC thus allows to standardize evaluation of immune cell subsets and potentially predicts clinical outcome for NSCLC patients treated by ICI. FC has become invaluable for biomarker research, providing detailed information on single cells in a heterogeneous population. However, only few clinical trials investigated FC interest in ICI context. Its validation and relevance at larger scale need to be further investigated.
As previously reviewed, the absolute count for circulating non-tumoral cells is not sufficient to predict clinical outcomes under the ICI regimen. Also, the markers of the systemic inflammatory response (such as plasma C-reactive protein (CRP) or hypoalbuminemia) have been shown to play a major role in cancer progression and aggressiveness (35). Many systemic inflammatory markers have thus been reported as prognostics markers in NSCLC, mainly based on the cell count ratio between two or more non-tumoral cell subsets. Among them, platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), and lymphocyte-to-monocyte ratio (LMR) have been previously proposed as prognostic markers (36–38). Moreover, the ratio between various subsets of cells could reflect the systemic inflammation with a lower intra- and inter-individual variation, especially during course of the treatment. As an additional hypothesis, the ratio between pro and anti-tumoral factors could also introduce precision and robustness to predict tumor immune sensibility. We review here the impact of neutrophils, lymphocytes, and platelets respective ratios, and their variation (Δ) for NSCLC patients treated by ICI.
Platelet to lymphocyte ratio (PLR) is a common ratio combining two parameters related to chronic inflammation. We reviewed 16 studies exploring PLR as a potential predictor of ICI response and survival. Ksienski’s report was the largest study published, retrospectively investigating PLR to predict ICI outcomes in 220 patients with NSCLC treated by Pembrolizumab in the frontline for 95% of them (39). In this study, patients with high PLR at baseline had worse OS (median: 4.0 vs 15.4 months, HR: 2.03, p=0.006), suggesting that PLR could predict ICI response and benefit. Interestingly, this study included only patients with high PD-L1 expression (TPS >50%) and thus highlighted that PLR may be independent of PD-L1 expression to predict ICI benefit. A recent meta-analysis published by Liu et al. integrated 15 studies focused on PLR in the ICI field of NSCLC (40). In this meta-analysis, the authors established that high PLR was associated with worse OS (HR: 1.49, p<0.001, I2 = 57.6%, p=0.003), driven by worse PFS (HR = 1.62, p<0 .001). To note, the I2 index reflects the degree of heterogeneity in a meta-analysis among included studies with higher heterogeneity for higher I2 indexes. Very interestingly, there was no association between PLR and OS in the group ≥ 200 when stratified by cut-off point (HR: 1.35, p=0.172). This discrepancy illustrates the heterogeneity in studies assessing PLR as a predictor of ICI response: the range for PLR cut-off varies from 144 to 441 and introduces a broad bias.
Another composite score based on three types of blood cell was also developed: the systemic immune inflammation index (SII) (SII = Platelet × Neutrophils/Lymphocytes counts). This index was first developed in the context of hepatocellular carcinoma (41). Larger studies then proposed that higher SII could predict worse clinical outcomes in various solid cancers, including NSCLC in terms of PFS, OS, and disease-free survival (DFS) (42, 43).
Only three studies investigated SII interest in NSCLC patients treated by ICI. One retrospective study of 44 patients treated by nivolumab monotherapy in the second line reported a significant association: low SII at baseline (<603.5) predicted longer PFS (HR=0.34, p=0.006) and OS (HR=0.16, p=0.005) and remained significant in a multivariate analysis (44). These results remain controversial, without association between SII at baseline (cut-off value of 730 and 792.07, respectively) and tumor response in two other studies (45, 46). Interestingly, these two studies both reported a significant prediction for dynamic change of SII throughout the ICI course of 6 weeks. Indeed, Fang et al. reported a shorter PFS for patients with an increased in SII from baseline (HR=1.731, p=0.027). Similarly, Jin Suh et al. observed a worse PFS for patients with a post-treatment SII ≥ 730 at 6 weeks (median: 2.8 vs 8.1 months, p=0.033). In earlier stages (stages I-IIIB), the same observations were done for NSCLC patients treated by chemoimmunotherapy: SII at baseline did not predict pathological response. However, on-treatment SII and a decrease of SII from baseline exhibited more frequently a major pathological response (p<0.01) (47).
SII predictive capacity was not specific to the ICI context, since similar results have been reported in EGFR mutant patients treated by TKIs (48–50). Considering inconsistent and non-specific results, SII is currently set aside to predict clinical issues for patients treated by ICI.
A few studies investigated lymphocyte-to-monocyte ratio (LMR) to predict ICI response. The largest one was a retrospective cohort of 262 patients mainly treated with Nivolumab (n=131) or Pembrolizumab (n=95). The patients with LMR < 2.12 at baseline were exposed to shorter OS (HR: 1.62, p=0.02) in multivariate analysis (51). In other available studies, low LMR was also associated with worse outcomes for patients with NSCLC under ICI regimens. These parameters remain rarely explored. A meta-analysis integrated 4 studies investigating this parameter: patients with low LMR had worse OS without heterogeneity (HR = 0.45, p <0 .001) (40). Finally, only one study compared PD-L1 and LMR abilities to predict ICI benefits with similar results. In Katayama et al. ‘s report, PD-L1 TPS was not significantly predictive for OS or PFS, while LMR > 1.5 was associated with better PFS and OS (HR: 0.418, p=0.004 and HR: 0.30, p<0.0001, respectively) (52). Of note and as a main limitation, LMR relevant cut-off was not consensual ranging from 1.5 to 2.12. This critical point needs to be elucidated in larger studies.
Nutrition and immune features share a close relationship and can both modify tumor aggressivity and prognosis in cancer patients (53). The nutritional status, the muscle mass, and the inflammatory status could reflect cancer-related cachexia and impact the immune system, leading to potential ineffective ICI (54). The prognostic nutritional index (PNI) is calculated as follows: [(10 × serum albumin (g/dL)) + (0.005 × total lymphocyte count)]. It is an efficient indicator for assessing the nutritional and immunological conditions of cancer patients. The parameters are routinely assessed in laboratory tests during clinical cancer management and are easily repeated. Numerous studies reported an association between baseline PNI and survival in various cancers, including NSCLC (55, 56). For example, PNI predicted both early-progression (OR=3.709, p=0.011) and shorter OS (HR= 7.596, p<0.001) for patients with lower PNI (significant cut-off value determined by ROC curve) (57). A meta-analysis dedicated to PNI included 12 studies, enrolling 13590 NSCLC patients treated by ICI (58). The Cut-off value for PNI ranged from 31.1 to 48. The findings demonstrated that patients treated by ICI with low PNI at baseline had both shorter OS (HR=2.24, 95% CI=1.57–3.20) and PFS (HR=1.61, 95% CI=1.37–1.88). Mahiat C. et al. explored systemic inflammation/nutritional status (including PNI) as predictive factors in 3 metastatic NSCLC cohorts treated in the first line by ICI monotherapy (n=75), ICI combined with chemotherapy (n=56), or chemotherapy alone (n=221). Their results supported that systemic inflammation/nutritional status could be associated with the outcomes independently of the treatment, and were therefore prognostic but not predictive (59). The ICI efficacy predicted by PNI also seemed independent of PD-L1 expression, since no association between PD-L1 TPS and PFS/OS was reported while a lower PNI was significantly associated with shorter PFS (HR: 1.704, p<0.05) (60). Consistent comparisons were reported in external NSCLC cohorts (57, 61). The non-specific prognosis was also supported by Sheng et al.: low PNI at baseline was predictive of worse survival in the EGFR mutated context (untreated by ICI) (62). Low levels of baseline PNI could thus be a significant predictor of worse clinical outcomes for patients treated with ICIs. However, its specificity with ICI and relevant cut-off remains unclear and needs to be assessed in further prospective and larger cohorts.
Neutrophil to lymphocyte ratio (NLR) and derived neutrophil to lymphocyte ratio (dNLR) were the broadest investigated features based on blood cell count. NLR assessed by absolute neutrophil count divided by absolute lymphocyte count is the most explored parameter as a potential predictor of clinical outcomes for NSCLC patients treated by ICI. NLR is a marker for the general immune response to various stress conditions (63, 64).
These studies are reviewed in Table 1. The most relevant and robust trial was LIPS-3, aiming to stratify the prognosis of patients treated by ICI. It retrospectively included 784 patients (201 in a training group and 583 in a validation group), all of them treated with Pembrolizumab in the frontline, thus with a TPS of PD-L1 ≥ 50% (85). Based on a threshold of 4, low NLR was associated with better OS in both cohorts, reaching 76.6% at 1 year. Interestingly, the authors proposed combining NLR with other factors such as PS-ECOG and corticosteroid pre-treatment to improve their prognostic score. As reviewed, a very large part of studies exploring NLR are consistent: low NLR at baseline was associated with better responses and clinical outcomes under an ICI regimen. However, patients and ICI are very heterogeneous, considering the line of pre-treatment, PS-ECOG, sub-type histology (squamous vs non-squamous), PD-L1 expression, or combination with chemotherapy. A recent meta-analysis aggregated 31 studies (40): high NLR was associated with shorter OS (HR 2.13, p<0.001) with significant heterogeneity (I2 = 83.8%, p<0 .001). Very similar results were observed for Δ NLR: increased NLR through ICI administration was associated with worse survival (HR = 1.77, p < 0.001, I2 = 79.5%, p <0.001). The sub-group analysis performed on the cut-off showed a significant association for the NLR threshold of 5 (HR=1.94, p<0.001), which remains the most employed cut-off, with a range from 2.8 to 5. Some studies compared and adjusted NLR levels with PD-L1 expression in multivariate analysis predicting PFS or OS for patients treated by ICI. Most of them were consistent, observing an independence between NLR and PD-L1 expression (51, 83, 95).

Table 1 Non-tumoral blood cell count biomarkers.
Derived neutrophil to lymphocyte ratio (dNLR), assessed by ANC/(WBC – ANC) was also proposed as a promising predictor of ICI responses in NSCLC. We thus reviewed 8 studies exploring dNLR, the largest one enrolling 466 patients (composed of a test set (n=161) and a validation set (n=305)) (101). The patients with high dNLR had independently worse OS (HR: 1.98, p=0.002) while PD-L1 was not significantly predictive of the clinical issue under the ICI regimen. All other studies were consistent and integrated into a meta-analysis published by Yang et al.: the pooled results supported that high dNLR predicted worse PFS (HR: 1.38, p<0.001) and shorter OS (HR: 1.65, p< 0.001) (104). Cut-off values were also different, ranging from 2.2 to 3.0. This meta-analysis showed that dNLR relevance remained significant, indifferently from the dNLR threshold. Moreover, dNLR was commonly associated with a parameter of a global score named LIPI, a predictor of ICI responses, and combined with LDH level. Just as exposed for NLR, the level of evidence is high for LIPI and dNLR but is not integrated into current clinical guidelines for ICI guidance in NSCLC management.
Although many other studies corroborated these observations, this easy and low-cost parameter remains unused in current clinical practice and does not even appear in clinical guidelines.
Petrova et al. explored both NLR and PLR in a cohort, comparing chemotherapy and ICI groups. Both NLR and PLR at baseline were significative predictors of OS in the chemotherapy groups (HR: 8.09, p<0.001 and HR: 2.91, p=0.025, respectively) and ICI groups (HR: 7.94, p<0.001 and HR: 5.08, p<0.001, respectively) in multivariate analysis. This suggests that nor NLR nor PLR are specific for survival in NSCLC treated by ICI (95). Regarding PFS, only NLR remained significant (HR = 4.47, p < 0.001), supporting more interest in NLR parameters in the ICI context.
Very few studies investigated these blood parameters for patients treated by ICI combined with chemotherapy, whereas chemo-immunotherapy became a large standard for many patients, especially when PD-L1 TPS ≤ 49% in the frontline. Moreover, the inclusion of ICI alone, mainly in a pre-treated context, is not easily transposed in a frontline context which represents a current challenge to predicting patient outcomes. The next step for these potential markers of ICI response remains certainly the establishment of a relevant cut-off to then validate the biological–driven decision in a prospective study.
Although PD-1/PD-L1 were described as membrane-associated molecules, various soluble derived products of ICI were described in the serum of cancer patients. Soluble PD-1/PD-L1 (sPD-1/sPD-L1) and exosomal PD-L1 (exoPD-L1) are both parts of the dynamic PD-1 pathway and immune response (105, 106). Their respective biological effects remain largely unknown. sPD-1 has been proposed to act as a decoy, blocking PD-1 immunosuppressive axis, and binding to PD-L1 and PD-L2 (107–109). sPD-L1 detection and/or high levels could thus be associated with ICI ineffectiveness. Although sPD-L1 effects are not elucidated, its clinical relevance in NSCLC was explored, especially in patients treated by ICI as a predictive biomarker for response and/or tumor progression.
sPD-L1 was the most investigated parameter with 9 reviewed studies focusing on ICI outcomes in NSCLC patients including a cohort of 119 NSCLC patients, with a control group of 29 healthy volunteers (110). Additional circulating parameters were explored such as PD-L1 levels on circulating immune cells, platelets, and platelet microparticles. Interestingly, circulating PD-L1+ leukocytes count was independent of tumor PD-L1 expression. Although some features such as PD-L1+ neutrophil count, or PD-L1+ PLTs count were associated with shorter PFS and OS, no differences were observed for patients with high vs low sPD-L1 (cut-off=12.94 pg/ml). Another study equally dimensioned with 233 NSCLC patients treated with Nivolumab or Pembrolizumab (details not provided), reported positive results (111): the patients with high sPD-L1 exhibited both shorter PFS (median: 57 days vs 177 days; p=0.011) and OS (median: 182 days vs not reached, p<0.001) than those in the low sPD-L1 group. In comparison with PD-L1 tissue expression, there was a significant but low correlation between tissue PD‐L1 TPS and circulating sPD‐L1 concentration (r=0.214, p=0.001). sPD-L1 remained an independent predictor of ICI outcome in a multivariate analysis for both PFS (HR: 1.910; p=0.061) and OS (HR: 2.073; p=0.034). In addition, sPD-L1 remained significant in a multivariate analysis for OS prediction after adjustment on PD-L1 tissue expression, illustrating its independence and valuable interest as a predictive marker of ICI benefit. In this report, the discrepancy could be explained by a high threshold of 90 pg/mL. Most other studies examined smaller cohort of patients resulting in lower statistical power and/or considered different cut-offs for sPD-L1 with a large range from 3.357 ng/mL (detection threshold/positivity) to 166 pg/mL (112). Δ sPD-L1 was also investigated with lower interest, as reviewed in Table 2. Finally, a meta-analysis updated in 2022 of 710 patients treated by surgery or ICI reported that high levels of sPD-L1 were correlated with worse OS (HR: 2.34; p<0.001) and PFS (HR: 2.35; p<0.001). The results were consistent when focusing on subgroups of patients treated by ICI for OS (HR: 2.40;p<0.001) (124, 125).
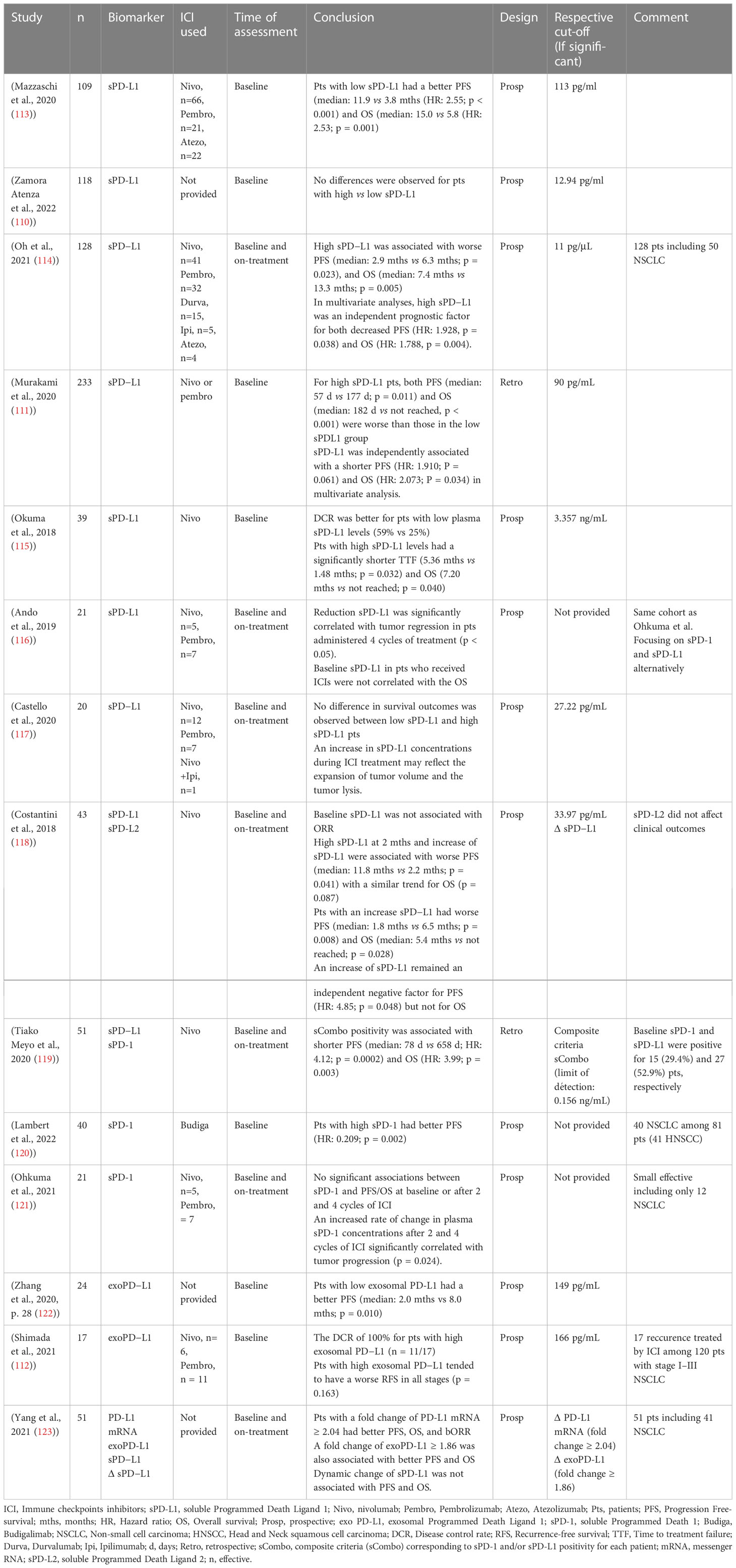
Table 2 Soluble-derived immune checkpoints-related products.
sPD-L2 may act as a decoy blocking the PD-1 immunosuppressive axis and leading to potential ICI inefficacy. Only one study explored the potential interest of sPD-L2 as a predictor of ICI response among 43 NSCLC patients treated with Nivolumab without any association with clinical outcomes (118, 125) (118, 125) (126). One study assessed serum mRNA PD-L1, reporting that patients with a fold change of PD-L1 mRNA ≥ 2.04 had better PFS, OS, and best objective response (123) (Table 2). Three studies also explored exoPD-L1, the largest cohort enrolling 42 NSCLC patients with contradictory results. Many other soluble markers might be of interest in this context such as sPD-L2, sLAG3, sTIM-3, or sIDO despite restricted reports (127).
Thus, all available studies currently suffer from limited effective with lower statistical power and/or retrospective designs. Although sPD-L1 was the most explored parameter with consistent meta-analysis, a relevant cut-off is not defined (high variation across publications). Considering sPD-L1 as a biomarker remains challenging according to its multi-biological and structural protein forms. Other parameters such as exosomal and mRNA-derived products introduced high challenges with technical difficulties, and high variabilities in methodologies, resulting in complex clinical applications.
Circulating tumor cells (CTCs) emerged as promising blood based-biomarkers in a large panel of solid cancers (128). CTCs are tumor cells that escaped from the primary tumor site and have extravasated into the blood circulation. CTCs detection is challenging because of their rarety. Nonetheless, recent technologies succeeded in extracting CTCs through enrichment and detection methods based on molecular markers and more especially on epithelial cell adhesion molecules but also on physical parameters (128). CTCs are thus also examined in lung cancer, especially in NSCLC, from early to advanced stages as a predictor of clinical outcomes (17). CTCs harbor a great interest in the cancer context with many potential clinical applications such as early diagnosis markers, prognostic evaluation, therapeutic response monitoring, drug sensitivity testing, and/or precision medication guidance (128, 129). Focusing on the NSCLC context, several studies already reported a global poor prognosis in patients with CTCs detection and/or high CTC enumeration (130), including early and resected NSCLC (131). Here, published studies are reviewed about CTC-related features associated with outcomes under ICI regimens for NSCLC patients.
CTC detection and absolute count were the most investigated parameter in the CTC field (132) with at least 8 studies focused on CTC enumeration with ICI treatment. The largest cohort included 104 patients, mainly treated with Nivolumab (133). Based on the CellSearch method, CTC detection was an independent predictive factor for worse PFS and OS at baseline (OR: 0.28, p=0.02), and on-treatment (OR: 0.07, p<0.01). However, this difference did not remain significant after adjustment with other co-factors including PD-L1 TPS (OR:0.22, p=0.08). Another published cohort by Guibert et al. (134) enrolled 96 patients with NSCLC all treated with Nivolumab. The patients with a high baseline CTC number ≥ 30/10mL were associated with worse OS (HR: 1.06; p=0.03) and PFS (HR: 1.05; p=0.02). All others were broadly consistent with these results, whereas we did not identify any meta-analysis focusing on CTC utility with ICI treatment. As reviewed in Table 3, the CTC cut-off also varies both on absolute number (0–30) and blood volume collected (3-10 mL), therefore introducing biases.

Table 3 Circulating tumor cells as biomarkers.
Additional techniques and analyses have been proposed to improve CTC relevance in the ICI context besides CTC detection and enumeration. Among them, PD-L1 expression by CTC was most explored (7 studies) with the hypothesis that PD-L1 expression by CTCs might be a valuable surrogate for PD-L1 tissue expression, in a dynamic and non-invasive approach, representing the whole landscape of the tumor heterogeneity. The largest study observed a higher baseline PD-L1+ CTC number (≥1%) in the “non-responders” group (PFS < 6 months, p=0.04) whereas PD-L1 TPS did not manage to predict ICI benefit in terms of PFS (134). No correlation was observed between tissues and CTC PD-L1 expression (r=0.04, p=0.77), and CTCs were more frequently found to be PD-L1 positive than tissues (83% vs 41%). Finally, PD-L1+ CTCs were seen in all patients at progression. Mondelo-Macía et al. reported no association for PD-L1+ CTCs, regardless of the technology employed (CellSearch and Parsortix systems) (137). A recent meta-analysis of 30 studies including various cancers reported global prognostic factors associated with PD-L1 CTC expression (144). Furthermore, Ouyang et al. reported that the baseline presence of PD-L1+ CTC was associated with better PFS (HR: 0.55, p=0.084, I2 = 61.1%, p=0.025) and with a trend for OS (HR: 0.61, p=0.067, I2 = 43%, p=0.135) when treated by ICI. In contrast, non-immune-based treatment (chemotherapy and/or TKI) was associated with worse PFS (HR: 1.85, p=0.005, I2 = 60.6%, p<0.001) and OS (HR: 2.44, p<0.001, I2 = 42.2%, p<0.043). These results suggested that PD-L1 CTC expression could endorse a certain specificity to predict outcomes with ICI treatment. However, PD-L1 CTC expression was not a significant predictor of PFS in the NSCLC context (HR: 1.3, p=0.341, I2 = 58.0%, p=0.011) with similar data for OS prediction.
CTCs seem highly promising for clinical cancer management, based on their non-invasive, easily repeatable, and dynamic real-time monitoring analysis (145). Additional CTC markers have been explored in NSCLC patients treated by ICI. In a cohort of 15 patients, high Carcinoembryonic antigen (CEA) and Human telomerase reverse transcriptase (hTERT) expression on CTC were associated with poor clinical response (p=0.017 and p=0.072, respectively) (142). In an equally dimensioned group treated by ICI, Indoleamine 2,3-dioxygenase (IDO)+ CTC detection was associated with shorter PFS (median: 2.5 vs 5.8 months, p=0.039) and OS (HR: 5.46, p=0.021). However, these results remain exploratory.
CTC use and transposability in daily practice remain very challenging. CTC detection remains very challenging with so-far only two FDA-approved methods (CellSearch and Parsortix) for specific cancer contexts and other numerous non-standardized techniques including ISET® (Isolation by Size of Epithelial Tumor cells) or numerous microfluidic systems. CellSearch is an FDA-approved system that demonstrated its clinical relevance in other solid cancer including breast (146), colorectal (147), and prostate cancers (148). The CellSearch method enriches cells using a magnetic ferrofluid containing antibodies against epithelial cell adhesion molecules (i.e EpCAM), before staining for cytokeratins (including cytokeratins 8, 18, and 19). This technology is not included in clinical practice, most probably because of its high cost. Moreover, there is no consensus for a relevant CTC threshold, also depending on the volume of blood collected. This critical point requires further investigation before additional consideration by the clinician. Innovative approaches are emerging such as Circulating tumor-derived endothelial cells (CTECs) that could predict acquired resistance to ICI (149). Other rare types of CTCs are suggested with non-elucidated and incertain clinical relevance (150). Aside from CTC-expressed immune-related biomarkers, other markers are also highly promising in reflecting tumor immune resistance (primary or acquired) such as those acquired through Epithelial-Mesenchymal Transition (EMT) for instance (151).
Plasma circulating tumor DNA (ctDNA) is a cell-free DNA product released by the tumor in the bloodstream. ctDNA interest is growing fast for solid tumor management. The detection and monitoring of ctDNA provide new opportunities for personalized cancer management. ctDNA is already used in clinical practice for detecting some targetable oncogenic driver such as EGFR of BRAF mutation but might have additional interest in the NSCLC context (152). Diverse technologies to analyze plasma ctDNA emerged and progressively integrated clinical practice. However, there is high variability and a lack of standardized techniques to detect ctDNA such as allele-specific PCR, digital PCR, multiplex PCR-based NGS, and whole-exome sequencing (WES) (153). Nonetheless, ctDNA-based clinical decision-making holds significant potential despite challenges and complexities, especially in the field of immunotherapy and lung cancer. We reviewed here published studies on ctDNA-related features associated with outcomes under ICI regimens for NSCLC patients (154).
Cell-free DNA can be estimated by various methods, most commonly using the maximum somatic allele frequency (MSAF), which is defined as the maximum allele frequency (AF) of all the tumor somatic mutations observed per sample by next-generation sequencing (NGS), and reflecting the ctDNA proportion in the blood. ctDNA and especially its variation and clearance have also been proposed as a potential surrogate of early tumor response and might predict responses to ICI (12). We identified 18 studies based on cell-free DNA detection and quantification of patients’ outcomes with NSCLC and under ICI (Table 4). The largest tested ctDNA levels as a potential relevant surrogate of early tumor response to ICI (168). ctDNA was detected using non-targetable mutation from the initial tumor biopsy by droplet digital PCR. A ctDNA decrease of over 30% at 4-6 weeks was correlated with an improved PFS and OS in 100 AC treated by ICI. In this cohort, patients with a tissue-positive PD‐L1 expression (TPS ≥ 1%) had a better PFS (HR: 0.46, p<0.001) and OS (HR: 0.57, p<0.05) than PD‐L1 negative patients. However, ctDNA demonstrated its independency from PD-L1 expression, significantly predicting OS both in PD-L1 positive and negative patients (HR: 0.37 and 0.47, p<0.05; respectively). Another equally dimensioned cohort of 97 patients treated by ICI also correlated with patient outcomes: an increase of ctDNA allele fraction at 1 month was associated with a 2-month PFS versus 14 months for patients with a decrease of AF. On another hand, PD-L1 TPS was not statistically predictive of ICI benefit, using either a cut-off of 1% or 50%, and was less predictive of response than ctDNA profiling (165). The largest report based on ctDNA was a pooled analysis of the randomized POPLAR and OAK studies by Chen et al. (161). This study assessed the clinical relevance of maximum somatic allele frequency (MSAF) which is an indicator of the proportion of tumor-derived plasma DNA. Atezolizumab was identified as beneficial when patients harbored lower MSAF levels (i.e., MSAF < 10.3%; HR: 0.59, p<0.001). In contrast, no difference was observed for patients with high MSAF levels between docetaxel and ICI groups (HR: 0.91, p=0.5). In this analysis, subgroup comparisons were performed especially regarding clinical confounding factors to determine the independency of ctDNA. Thus, the prediction of ICI interest by ctDNA remains significant both in Atezolizumab and Docetaxel arms after adjustment for baseline covariate (including age, sex, race, performance status, histology, number of metastatic sites, smoking history or number of prior therapies) with a more prominent effect in the Atezolizumab arm (HR=1.89, p<0.001 for Atezolizumab vs. HR=1.30, p=0.029 for docetaxel group). Finally, a meta-analysis was performed on 10 studies, including 1017 patients with NSCLC and treated by ICI (169). The baseline ctDNA detection was not associated with clinical outcomes, for OS, PFS, and ORR (respective HR: 1.18; 0.98, and 0.89). The longitudinal assessment and especially its early decrease was able to significantly predict ICI benefit regarding both OS, PFS, and ORR (respective HR: 0.19, 0.30, and 0.07).
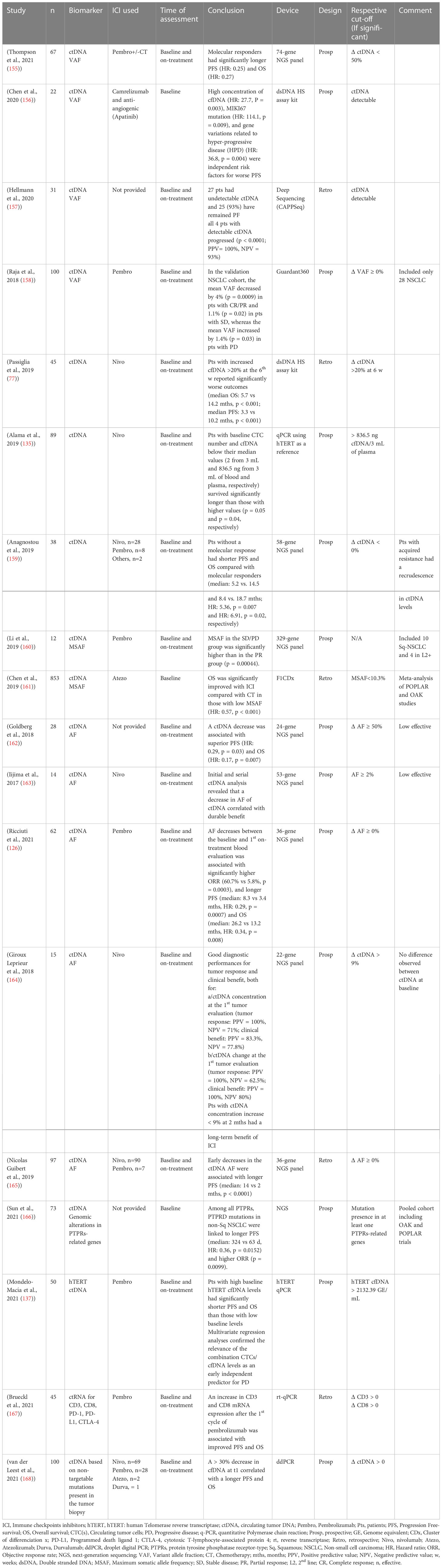
Table 4 Circulating tumor DNA as a biomarker.
Tumor mutation burden (TMB) is a marker of genomic instability. It reflects the production of immunological and inflammatory neoantigens, closely related to immunogenicity (170). The biological approaches support that high TMB reflects a tumor with a higher level of mutation and neoantigens productions, reflecting a so-called “hot-tumor”, which could potentially be predictive of ICI sensibility (171). Previous clinical trials reported positive results from tissue-based TMB analysis in NSCLC (172, 173). Blood TMB (bTMB) is a derived marker of ctDNA that might have the capacity to integrate and reflect tumor heterogeneity, and that we reviewed in a dedicated section (Table 5) according to a specific method of assessment and analysis.
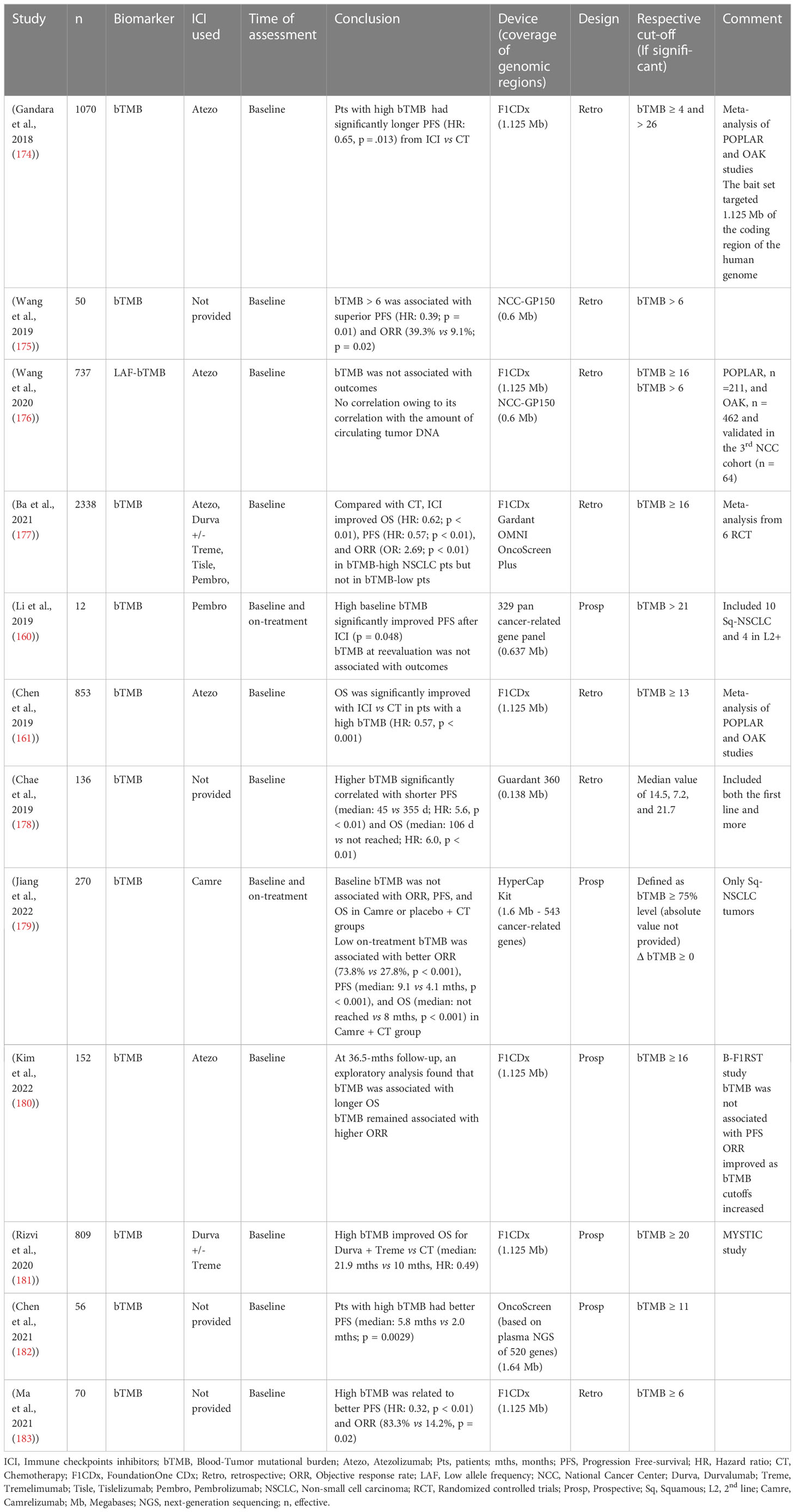
Table 5 Blood Tumor mutational burden.
The largest cohort included 809 patients with a NSCLC treated with Durvalumab +/- Tremelimumab (vs SOC) in the MYSTIC study (181). With a threshold of 20 mutations/Mb at baseline, the patients with high bTMB had better OS (HR: 0.49) when treated with Durvalumab and Tremelimumab. A level of bTMB > 16 mutations/Mb was associated with better OS in 153 patients treated with Atezolizumab from the BF1RST trial (at baseline, HR: 0.54, p<0.5) (180). Gandara et al, compared PD-L1 expression and bTMB levels to assess the potential overlap between these two parameters (174). Among 1070 patients (pooled from OAK and POPLAR trials), patients with high bTMB (>16 mutations/Mb) were not overrepresented among patients with the highest levels of PD-L1 (defined by a TPS ≥50% or ≥10% of tumor-infiltrating immune cells expressing PD-L1) with only 30 patients positive for both assays (19.2% of patients for bTMB and 29.1% for PD-L1 expression). These data demonstrated the independence between bTMB and PD-L1 expressions assessed by IHC. The supplemental analysis from the same publication also compared the clinical characteristics of the bTMB subgroups of patients from the OAK trial. bTMB > 16 mutations/Mb was associated with smoking history as already published, as a consequence of tobacco mutagen exposure (184). Additionally, high bTMB was also associated with high tumor stages (p<0.0001) or the number of metastases sites(p=0.0055), potentially impacting survival and prognosis. However, the baseline clinical features were well balanced between arms (Atezolizumab vs. Docetaxel) suggesting that bTMB might be an independent predictive marker of ICI efficacy.
Only one study addressed the potential relevance of longitudinal bTMB assessment (179): no correlation was found between clinical outcomes and baseline bTMB in 270 lung squamous carcinomas treated by Camrelizumab. However, low on-treatment bTMB significantly correlated with better PFS, OS, and ORR. This association was specific to the ICI regimen and was not observed in the chemotherapy control group. Finally, a meta-analysis pooled 2338 patients from 6 randomized controlled trials with bTMB assessment (177): patients with high bTMB and treated by ICI had improved ORR (HR:2.69, p<0.03), PFS (HGR: 0.57, p<0.01), and OS (HR: 0.62, p<0.01) in comparison with patients treated with chemotherapy. Inversely, no clinical benefit was observed with ICI regimens when patients had lower bTMB. More interestingly, subgroups analyses confirmed across all potential confounding factors (such as line of treatment, type of NGS panel with various among of genome covered, level of PD-L1 expression, and ICI regimen) that bTMB was able to independently predict clinical issues for NSCLC patients treated by ICI.
The interest in soluble biomarkers is also emerging in the earlier stages, including neoadjuvant conditions with many ICI trials in the peri-operative context (185). The NADIM trial enrolled 46 patients with a locally advanced stage IIIA NSCLC treated with neoadjuvant chemotherapy and Nivolumab (186). Tissue-based TMB and PD-L1 were significant predictors of OS. The patients with the lowest ctDNA at baseline had longer PFS (HR: 0.20, p=0.006), and OS (HR: 0.27, p=0.002). Moreover, the absence of ctDNA after neoadjuvant treatment was also associated with improved PFS (HR: 0.26, p=0.038) and OS (HR: 0.04, p=0.015). These results illustrated the feasibility and clinical relevance of detecting soluble biomarkers in every stage of NSCLC treated by ICI. Prospective dedicated studies are further needed to improve clinical outcomes under ICI regimen, considering randomization with pre-specified soluble biomarker expression and/or level at baseline.
ctDNA and its related biomarkers are highly promising for cancer management. However, many limitations remain unsolved.
The baseline level of ctDNA, and particularly of MSAF could be biased. An MSAF < 1% was associated with better OR in the BF1RST study. However, this result could be driven by better baseline values rather than by MSAF itself (180). Although the findings are broadly consistent, establishing bTMB cut-off values still requires further studies. For instance, the Keynote-189 trial used a 15 mutation/Mb while the MYSTIC study was based on a bTMB threshold of 20 mutation/Mb. Finally, OAK, B-F1RST, and POPLAR trials used an intermediate threshold of 16 mutations/Mb. Moreover, bTMB determination suffers from a major lack of standardization. Gold standard techniques involve a WES examination. Trying to reduce cost and time analysis, clinical studies were based on various NGS panels covering 150 to more than 500 genes and thus covering variable amounts of the genome (from 0.138 to 1.64 Mb of coding exome; the literature recommends at least 1 Mb of DNA for reliable assay) without clear cut-off for bTMB (187, 188).
These major reports highlight the need for a relevant bTMB cut-off before conducting a randomized controlled trial with a biological-driven treatment decision.
As reviewed previously, many circulating markers might help clinicians to predict ICI outcomes for NSCLC patients (189). We summarized here current active clinical trials investigating one or more soluble biomarkers in the ICI context for NSCLC and discussed how their results could introduce a change into clinical practice.
No active clinical trial is investigating (d)NLR in NSCLC despite its high potential. The BUDDY trial (NCT04059887) explores bTMB as a biomarker, whereas the endpoints do not drastically differ from the BF1RST study previously discussed. The NCT03373955 trial (non-randomized design) aims to construct an immune repertoire for patients treated with Atezolizumab, mainly based on T-cell repertoire and cfDNA. This approach might provide additional promising soluble markers.
The NCT04720339 prospectively enrolls NSCLC patients treated with Atezolizumab, assessing the predictive value for quantification of plasma cfDNA at the time of the first radiological evaluation and on clinical benefit. The ATLAS and CIRCULAR trials have similar secondary endpoints, based on Nivolumab-Ipilimumab or Pembrolizumab regimen (NCT04966676 and NCT04912687, respectively). Complementary results from observational studies are also expected with the same scope (NCT03892096; NCT04791215).
The COPE trial is an ambitious biological-driven protocol, where implementing sequential ctDNA to improve the management of patients with advanced cancer and therefore their survival is tested. AstraZeneca also supports a recruiting trial assessing the benefit of adjuvant concomitant chemotherapy plus Atezolizumab for resected NSCLC patients with post-operative detectable ctDNA (NCT04367311) named molecular residual disease (MRD). The clearance of ctDNA will also serve as a surrogate for DFS and OS. Some trials are also recruiting based on MRD positivity (detectable cfDNA) with other ICI regimens like Durvalumab + Tremelimumab (NCT04625699) also in post-operative context, post stereotactic radiotherapy for stage I (SCION trial - NCT04944173) or Pembrolizumab metastatic frontline (NCT05198154).
The terms of CTC use remain challenging. Many trials aim to use CTC as a surrogate of tumor response in ICI treatment through plasma clearance (NCT05091190; NCT03481101). The largest study dedicated to CTC in NSCLC is currently the IMMUNO-PREDICT trial, aiming to enroll about 200 patients with an NSCLC. Its main objective is to demonstrate the feasibility of the analysis of PD-L1 expression on CTC.
These active trials reflect the need to implement biomarkers into clinical management, especially with ICI treatment and in each NSCLC stage.
The experimental strategies do not converge on the same aims, challenges, and difficulties according to the stage of the disease. We discuss here how soluble biomarkers could be integrated into clinical practice with their respective potential interest. At the baseline evaluation, soluble biomarkers could thus allow the selection of the more appropriate treatment with a higher predictive value of clinical benefit (190). It could also predict patients with worse prognoses to propose more aggressive treatment and combine ICI with chemotherapy rather than ICI alone. At the early on-treatment phase, soluble biomarker variations could identify patients with biological progression and predict patients with a higher risk of progression to closely monitor the disease (191), and even identify patients with early-stage hyper progression (192). The prolonged monitoring of soluble biomarkers for patients treated by ICI also exhibits additional interest such as response assessment. The pseudo-progression or prediction of biological residual disease in long-term responders could also be identified with prolonged monitoring of soluble biomarkers (193) (Figure 2).
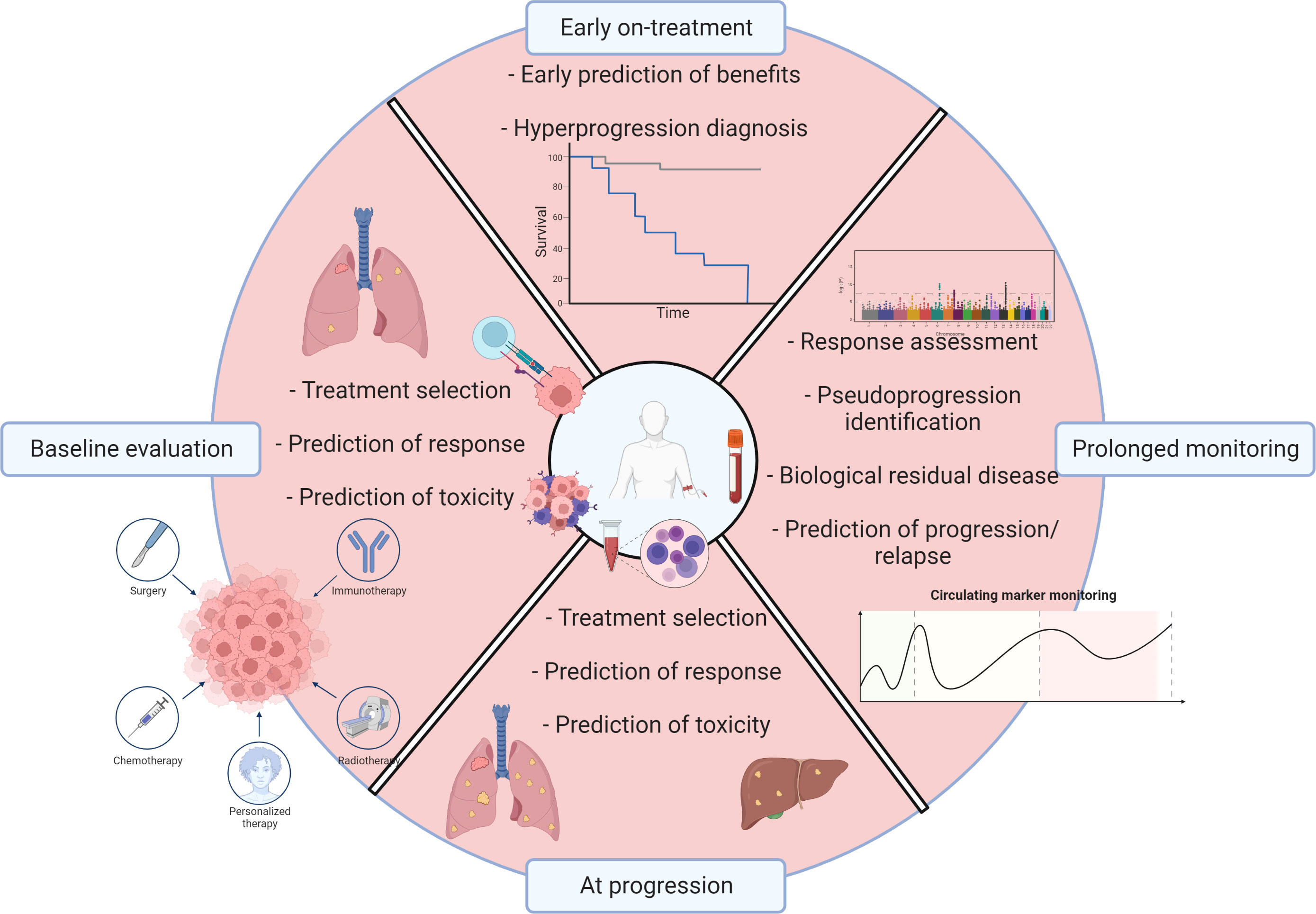
Figure 2 Perspectives for liquid biopsies into the immune landscape. Liquid biopsy for patients with NSCLC and treated by immunotherapy can improve many clinical challenges such as baseline evaluation, real-time monitoring, and prediction of response or progression. Created with BioRender.com.
Recent advances in lung cancer management are particularly impressive in ICI. However, only a sub-population benefits from immunotherapies. The currently available biomarkers, including tumor PD-L1 expression, remain largely perfectible. Liquid biopsy is now well-admitted into NSCLC with oncogenic addiction treated by TKIs showing promising results in the ICI field. Easy-to-use parameters derived from blood numerations and more complex scores and parameters can predict ICI outcomes for patients with NSCLC. However, each parameter harbors various limitations growing roots from a low level of evidence to technical difficulties before the integration into clinical practice. The design of specific and dedicated clinical trials is necessary to improve patient survival with biological-driven randomization and/or management.
JA, VDo, GD, and MP contributed to the conception and design of the study. JA wrote the first draft of the manuscript. JA, VDo, and VDa wrote sections of the manuscript. All authors contributed to the manuscript revision, and approved the submitted version.
With financial support from ITMO Cancer of Aviesan within the framework of the 2021-2030 Cancer Control Strategy, on funds administered by Inserm, from the University of Reims Champagne Ardenne (URCA), France and Reims University Hospitals, France.
The research effort associated with this review was funded in part by the Partenariat Hubert Curien-Tournesol. CG is a Senior Associate Researcher from FRS-FNRS (Belgium).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68:394–424. doi: 10.3322/caac.21492
2. Duma N, Santana-Davila R, Molina JR. Non-small cell lung cancer: epidemiology, screening, diagnosis, and treatment. Mayo Clin Proc (2019) 94:1623–40. doi: 10.1016/j.mayocp.2019.01.013
3. Reck M, Rabe KF. Precision diagnosis and treatment for advanced non-Small-Cell lung cancer. N Engl J Med (2017) 377:849–61. doi: 10.1056/NEJMra1703413
4. Korpanty GJ, Graham DM, Vincent MD, Leighl NB. Biomarkers that currently affect clinical practice in lung cancer: EGFR, ALK, MET, ROS-1, and KRAS. Front Oncol (2014) 4:204. doi: 10.3389/fonc.2014.00204
5. Prelaj A, Tay R, Ferrara R, Chaput N, Besse B, Califano R. Predictive biomarkers of response for immune checkpoint inhibitors in non-small-cell lung cancer. Eur J Cancer (2019) 106:144–59. doi: 10.1016/j.ejca.2018.11.002
6. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-Positive non-Small-Cell lung cancer. N Engl J Med (2016) 375:1823–33. doi: 10.1056/NEJMoa1606774
7. Sezer A, Kilickap S, Gümüş M, Bondarenko I, Özgüroğlu M, Gogishvili M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet (2021) 397:592–604. doi: 10.1016/S0140-6736(21)00228-2
8. Herbst RS, Giaccone G, de Marinis F, Reinmuth N, Vergnenegre A, Barrios CH, et al. Atezolizumab for first-line treatment of PD-L1–selected patients with NSCLC. N Engl J Med (2020) 383:1328–39. doi: 10.1056/NEJMoa1917346
9. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet (2018) 391:1023–75. doi: 10.1016/S0140-6736(17)33326-3
10. Marrugo-Ramírez J, Mir M, Samitier J. Blood-based cancer biomarkers in liquid biopsy: a promising non-invasive alternative to tissue biopsy. Int J Mol Sci (2018) 19:E2877. doi: 10.3390/ijms19102877
11. Canale M, Pasini L, Bronte G, Delmonte A, Cravero P, Crinò L, et al. Role of liquid biopsy in oncogene-addicted non-small cell lung cancer. Transl Lung Cancer Res (2019) 8:S265–79. doi: 10.21037/tlcr.2019.09.15
12. Rolfo C, Mack P, Scagliotti GV, Aggarwal C, Arcila ME, Barlesi F, et al. Liquid biopsy for advanced NSCLC: a consensus statement from the international association for the study of lung cancer. J Thorac Oncol (2021) 16:1647–62. doi: 10.1016/j.jtho.2021.06.017
13. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell (2010) 140:883–99. doi: 10.1016/j.cell.2010.01.025
14. Pan Y, Fu Y, Zeng Y, Liu X, Peng Y, Hu C, et al. The key to immunotherapy: how to choose better therapeutic biomarkers for patients with non-small cell lung cancer. biomark Res (2022) 10:9. doi: 10.1186/s40364-022-00355-7
15. Mitsuhashi A, Okuma Y. Perspective on immune oncology with liquid biopsy, peripheral blood mononuclear cells, and microbiome with non-invasive biomarkers in cancer patients. Clin Transl Oncol (2018) 20:966–74. doi: 10.1007/s12094-017-1827-7
16. Abu Hejleh T, Furqan M, Ballas Z, Clamon G. The clinical significance of soluble PD-1 and PD-L1 in lung cancer. Crit Rev Oncol Hematol (2019) 143:148–52. doi: 10.1016/j.critrevonc.2019.08.009
17. Qian H, Zhang Y, Xu J, He J, Gao W. Progress and application of circulating tumor cells in non-small cell lung cancer. Mol Ther - Oncolytics (2021) 22:72–84. doi: 10.1016/j.omto.2021.05.005
18. Punekar SR, Shum E, Grello CM, Lau SC, Velcheti V. Immunotherapy in non-small cell lung cancer: past, present, and future directions. Front Oncol (2022) 12:877594. doi: 10.3389/fonc.2022.877594
19. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer (2021) 21:345–59. doi: 10.1038/s41568-021-00347-z
20. Nakamura K, Smyth MJ. Myeloid immunosuppression and immune checkpoints in the tumor microenvironment. Cell Mol Immunol (2020) 17:1–12. doi: 10.1038/s41423-019-0306-1
21. Lim JU, Yoon HK. Potential predictive value of change in inflammatory cytokines levels subsequent to initiation of immune checkpoint inhibitor in patients with advanced non-small cell lung cancer. Cytokine (2021) 138:155363. doi: 10.1016/j.cyto.2020.155363
22. Murakami Y, Tamiya A, Taniguchi Y, Adachi Y, Enomoto T, Azuma K, et al. Retrospective analysis of long-term survival factors in patients with advanced non-small cell lung cancer treated with nivolumab. Thorac Cancer (2022) 13:593–601. doi: 10.1111/1759-7714.14303
23. Sibille A, Henket M, Corhay JL, Alfieri R, Louis R, Duysinx B. White blood cells in patients treated with programmed cell death-1 inhibitors for non-small cell lung cancer. Lung (2021) 199:549–57. doi: 10.1007/s00408-021-00474-2
24. Pu D, Xu Q, Zhou L-Y, Zhou Y-W, Liu J-Y, Ma X-L. Inflammation-nutritional markers of peripheral blood could predict survival in advanced non-small-cell lung cancer patients treated with PD-1 inhibitors. Thorac Cancer (2021) 12:2914–23. doi: 10.1111/1759-7714.14152
25. Yuan S, Xia Y, Shen L, Ye L, Li L, Chen L, et al. Development of nomograms to predict therapeutic response and prognosis of non-small cell lung cancer patients treated with anti-PD-1 antibody. Cancer Immunol Immunother (2021) 70:533–46. doi: 10.1007/s00262-020-02710-9
26. Weber R, Fleming V, Hu X, Nagibin V, Groth C, Altevogt P, et al. Myeloid-derived suppressor cells hinder the anti-cancer activity of immune checkpoint inhibitors. Front Immunol (2018) 9:1310. doi: 10.3389/fimmu.2018.01310
27. Orillion A, Hashimoto A, Damayanti N, Shen L, Adelaiye-Ogala R, Arisa S, et al. Entinostat neutralizes myeloid-derived suppressor cells and enhances the antitumor effect of PD-1 inhibition in murine models of lung and renal cell carcinoma. Clin Cancer Res (2017) 23:5187–201. doi: 10.1158/1078-0432.CCR-17-0741
28. Bronte G, Calabrò L, Olivieri F, Procopio AD, Crinò L. The prognostic effects of circulating myeloid-derived suppressor cells in non-small cell lung cancer: systematic review and meta-analysis. Clin Exp Med (2022). doi: 10.1007/s10238-022-00946-6
29. Meyer C, Cagnon L, Costa-Nunes CM, Baumgaertner P, Montandon N, Leyvraz L, et al. Frequencies of circulating MDSC correlate with clinical outcome of melanoma patients treated with ipilimumab. Cancer Immunol Immunother (2014) 63:247–57. doi: 10.1007/s00262-013-1508-5
30. Feng J, Chen S, Li S, Wu B, Lu J, Tan L, et al. The association between monocytic myeloid-derived suppressor cells levels and the anti-tumor efficacy of anti-PD-1 therapy in NSCLC patients. Transl Oncol (2020) 13:100865. doi: 10.1016/j.tranon.2020.100865
31. Koh J, Kim Y, Lee KY, Hur JY, Kim MS, Kim B, et al. MDSC subtypes and CD39 expression on CD8+ T cells predict the efficacy of anti-PD-1 immunotherapy in patients with advanced NSCLC. Eur J Immunol (2020) 50:1810–9. doi: 10.1002/eji.202048534
32. Bronte G, Petracci E, De Matteis S, Canale M, Zampiva I, Priano I, et al. High levels of circulating monocytic myeloid-derived suppressive-like cells are associated with the primary resistance to immune checkpoint inhibitors in advanced non-small cell lung cancer: an exploratory analysis. Front Immunol (2022) 13:866561. doi: 10.3389/fimmu.2022.866561
33. Kim HR, Park S-M, Seo S-U, Jung I, Yoon HI, Gabrilovich DI, et al. The ratio of peripheral regulatory T cells to lox-1+ polymorphonuclear myeloid-derived suppressor cells predicts the early response to anti-PD-1 therapy in patients with non-small cell lung cancer. Am J Respir Crit Care Med (2019) 199:243–6. doi: 10.1164/rccm.201808-1502LE
34. Youn J-I, Park S-M, Park S, Kim G, Lee H-J, Son J, et al. Peripheral natural killer cells and myeloid-derived suppressor cells correlate with anti-PD-1 responses in non-small cell lung cancer. Sci Rep (2020) 10:9050. doi: 10.1038/s41598-020-65666-x
36. Lin G-N, Peng J-W, Xiao J, Liu D-Y, Xia Z-J. Prognostic impact of circulating monocytes and lymphocyte-to-monocyte ratio on previously untreated metastatic non-small cell lung cancer patients receiving platinum-based doublet. Med Oncol (2014) 31:70. doi: 10.1007/s12032-014-0070-0
37. Gu X-B, Tian T, Tian X-J, Zhang X-J. Prognostic significance of neutrophil-to-lymphocyte ratio in non-small cell lung cancer: a meta-analysis. Sci Rep (2015) 5:12493. doi: 10.1038/srep12493
38. Gu X, Sun S, Gao X-S, Xiong W, Qin S, Qi X, et al. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: evidence from 3,430 patients. Sci Rep (2016) 6:23893. doi: 10.1038/srep23893
39. Ksienski D, Wai ES, Alex D, Croteau NS, Freeman AT, Chan A, et al. Prognostic significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio for advanced non-small cell lung cancer patients with high PD-L1 tumor expression receiving pembrolizumab. Transl Lung Cancer Res (2021) 10:355–67. doi: 10.21037/tlcr-20-541
40. Liu N, Mao J, Tao P, Chi H, Jia W, Dong C. The relationship between NLR/PLR/LMR levels and survival prognosis in patients with non-small cell lung carcinoma treated with immune checkpoint inhibitors. Med (Baltimore) (2022) 101:e28617. doi: 10.1097/MD.0000000000028617
41. Hu B, Yang X-R, Xu Y, Sun Y-F, Sun C, Guo W, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res (2014) 20:6212–22. doi: 10.1158/1078-0432.CCR-14-0442
42. Yang R, Chang Q, Meng X, Gao N, Wang W. Prognostic value of systemic immune-inflammation index in cancer: a meta-analysis. J Cancer (2018) 9:3295–302. doi: 10.7150/jca.25691
43. Huang W, Luo J, Wen J, Jiang M. The relationship between systemic immune inflammatory index and prognosis of patients with non-small cell lung cancer: a meta-analysis and systematic review. Front Surg (2022) 9:898304. doi: 10.3389/fsurg.2022.898304
44. Liu J, Li S, Zhang S, Liu Y, Ma L, Zhu J, et al. Systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio can predict clinical outcomes in patients with metastatic non-small-cell lung cancer treated with nivolumab. J Clin Lab Anal (2019) 33:e22964. doi: 10.1002/jcla.22964
45. Fang Q, Yu J, Li W, Luo J, Deng Q, Chen B, et al. Prognostic value of inflammatory and nutritional indexes among advanced NSCLC patients receiving PD-1 inhibitor therapy. Clin Exp Pharmacol Physiol (2023) 50:178–90. doi: 10.1111/1440-1681.13740
46. Suh KJ, Kim SH, Kim YJ, Kim M, Keam B, Kim TM, et al. Post-treatment neutrophil-to-lymphocyte ratio at week 6 is prognostic in patients with advanced non-small cell lung cancers treated with anti-PD-1 antibody. Cancer Immunol Immunother (2018) 67:459–70. doi: 10.1007/s00262-017-2092-x
47. Li C, Wu J, Jiang L, Zhang L, Huang J, Tian Y, et al. Correction to: the predictive value of inflammatory biomarkers for major pathological response in non-small cell lung cancer patients receiving neoadjuvant chemoimmunotherapy and its association with the immune-related tumor microenvironment: a multi-center study. Cancer Immunol Immunother (2023) 72:795. doi: 10.1007/s00262-022-03294-2
48. Ju Q, Huang T, Zhang Y, Wu L, Geng J, Mu X, et al. Systemic immune-inflammation index predicts prognosis in patients with different EGFR-mutant lung adenocarcinoma. Med (Baltimore) (2021) 100:e24640. doi: 10.1097/MD.0000000000024640
49. Li H, Wang G, Zhang H, Song X, Cao J, Zhang X, et al. Prognostic role of the systemic immune-inflammation index in brain metastases from lung adenocarcinoma with different EGFR mutations. Genes Immun (2019) 20:455–61. doi: 10.1038/s41435-018-0050-z
50. Chen D, Qin H, Deng G, Wang Q, Wang H, Liu X. Pre-radiotherapy systemic immune inflammation index associated with overall survival in patients with advanced EGFR mutant non-small cell lung cancer receiving thoracic radiotherapy. Clin Transl Oncol (2023) 25:226–35. doi: 10.1007/s12094-022-02936-2
51. Takada K, Takamori S, Yoneshima Y, Tanaka K, Okamoto I, Shimokawa M, et al. Serum markers associated with treatment response and survival in non-small cell lung cancer patients treated with anti-PD-1 therapy. Lung Cancer (2020) 145:18–26. doi: 10.1016/j.lungcan.2020.04.034
52. Katayama Y, Yamada T, Chihara Y, Tanaka S, Tanimura K, Okura N, et al. Significance of inflammatory indexes in atezolizumab monotherapy outcomes in previously treated non-small-cell lung cancer patients. Sci Rep (2020) 10:17495. doi: 10.1038/s41598-020-74573-0
53. Sun K, Chen S, Xu J, Li G, He Y. The prognostic significance of the prognostic nutritional index in cancer: a systematic review and meta-analysis. J Cancer Res Clin Oncol (2014) 140:1537–49. doi: 10.1007/s00432-014-1714-3
54. Madeddu C, Busquets S, Donisi C, Lai E, Pretta A, López-Soriano FJ, et al. Effect of cancer-related cachexia and associated changes in nutritional status, inflammatory status, and muscle mass on immunotherapy efficacy and survival in patients with advanced non-small cell lung cancer. Cancers (Basel) (2023) 15:1076. doi: 10.3390/cancers15041076
55. Tanaka S, Uchino J, Yokoi T, Kijima T, Goto Y, Suga Y, et al. Prognostic nutritional index and lung immune prognostic index as prognostic predictors for combination therapies of immune checkpoint inhibitors and cytotoxic anticancer chemotherapy for patients with advanced non-small cell lung cancer. Diagnostics (Basel) (2022) 12:423. doi: 10.3390/diagnostics12020423
56. Fang Q, Yu J, Luo J, Deng Q, Chen B, He Y, et al. Combination of baseline and variation of prognostic nutritional index enhances the survival predictive value of patients with advanced non-small cell lung cancer treated with programmed cell death protein 1 inhibitor. Clin Med Insights Oncol (2022) 16:11795549221137134. doi: 10.1177/11795549221137134
57. Liu N, Jiang A, Zheng X, Fu X, Zheng H, Gao H, et al. Prognostic nutritional index identifies risk of early progression and survival outcomes in advanced non-small cell lung cancer patients treated with PD-1 inhibitors. J Cancer (2021) 12:2960–7. doi: 10.7150/jca.55936
58. Ni L, Huang J, Ding J, Kou J, Shao T, Li J, et al. Prognostic nutritional index predicts response and prognosis in cancer patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Front Nutr (2022) 9:823087. doi: 10.3389/fnut.2022.823087
59. Mahiat C, Bihin B, Duplaquet F, Stanciu Pop C, Dupont M, Vander Borght T, et al. Systemic Inflammation/Nutritional status scores are prognostic but not predictive in metastatic non-Small-Cell lung cancer treated with first-line immune checkpoint inhibitors. Int J Mol Sci (2023) 24:3618. doi: 10.3390/ijms24043618
60. Shoji F, Takeoka H, Kozuma Y, Toyokawa G, Yamazaki K, Ichiki M, et al. Pretreatment prognostic nutritional index as a novel biomarker in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Lung Cancer (2019) 136:45–51. doi: 10.1016/j.lungcan.2019.08.006
61. Zaitsu J, Yamashita Y, Ishikawa A, Saito A, Kagimoto A, Mimura T, et al. Systemic inflammatory score predicts response and prognosis in patients with lung cancer treated with immunotherapy. Anticancer Res (2021) 41:3673–82. doi: 10.21873/anticanres.15158
62. Sheng J, Yang Y-P, Ma Y-X, Qin T, Hu Z-H, Hong S-D, et al. Low prognostic nutritional index correlates with worse survival in patients with advanced NSCLC following EGFR-TKIs. PloS One (2016) 11:e0147226. doi: 10.1371/journal.pone.0147226
63. Granot Z, Jablonska J. Distinct functions of neutrophil in cancer and its regulation. Mediators Inflammation (2015) 2015:701067. doi: 10.1155/2015/701067
64. Kaisar-Iluz N, Arpinati L, Shaul ME, Mahroum S, Qaisi M, Tidhar E, et al. The bilateral interplay between cancer immunotherapies and neutrophils’ phenotypes and Sub-populations. Cells (2022) 11:783. doi: 10.3390/cells11050783
65. Karantanos T, Karanika S, Seth B, Gignac G. The absolute lymphocyte count can predict the overall survival of patients with non-small cell lung cancer on nivolumab: a clinical study. Clin Transl Oncol (2019) 21:206–12. doi: 10.1007/s12094-018-1908-2
66. Diem S, Schmid S, Krapf M, Flatz L, Born D, Jochum W, et al. Neutrophil-to-Lymphocyte ratio (NLR) and platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer (2017) 111:176–81. doi: 10.1016/j.lungcan.2017.07.024
67. Khunger M, Patil PD, Khunger A, Li M, Hu B, Rakshit S, et al. Post-treatment changes in hematological parameters predict response to nivolumab monotherapy in non-small cell lung cancer patients. PloS One (2018) 13:e0197743. doi: 10.1371/journal.pone.0197743
68. Facchinetti F, Veneziani M, Buti S, Gelsomino F, Squadrilli A, Bordi P, et al. Clinical and hematologic parameters address the outcomes of non-small-cell lung cancer patients treated with nivolumab. Immunotherapy (2018) 10:681–94. doi: 10.2217/imt-2017-0175
69. Patil PD, Khunger M, Rakshit S, Stevenson J, Pennell NA, Elson P, et al. Pre-treatment hematological markers as a predictive biomarker for survival in patients with non-small cell lung cancer treated with nivolumab. JCO (2017) 35:11547–7. doi: 10.1200/JCO.2017.35.15_suppl.11547
70. Park W, Kwon D, Saravia D, Desai A, Vargas F, El Dinali M, et al. Developing a predictive model for clinical outcomes of advanced non-small cell lung cancer patients treated with nivolumab. Clin Lung Cancer (2018) 19:280–288.e4. doi: 10.1016/j.cllc.2017.12.007
71. Daher S, Lawrence YR, Dudnik E, Hanovich E, Urban D, Peled N, et al. Nivolumab in non-small cell lung cancer: real world long-term survival results and blood-based efficacy biomarkers. Front Oncol (2021) 11:625668. doi: 10.3389/fonc.2021.625668
72. Soyano AE, Dholaria BR, Marin-Acevedo JA, Diehl NN, Hodge D, Lou Y. Baseline peripheral blood biomarkers associated with clinical outcome of advanced lung cancer in patients treated with anti-PD-1 antibody. JCO (2017) 35:e20599–9. doi: 10.1200/JCO.2017.35.15_suppl.e20599
73. Bagley SJ, Kothari S, Aggarwal C, Bauml JM, Alley EW, Evans TL, et al. Pretreatment neutrophil-to-lymphocyte ratio as a marker of outcomes in nivolumab-treated patients with advanced non-small-cell lung cancer. Lung Cancer (2017) 106:1–7. doi: 10.1016/j.lungcan.2017.01.013
74. Rogado J, de la Maza MDF, Pacheco-Barcia V, Serra JM, Toquero P, Vera B, et al. P2.02-027 are inflammatory markers predictive of nivolumab efficacy in advanced non-Small-Cell lung cancer (NSCLC)? J Thorac Oncol (2017) 12:S2108–9. doi: 10.1016/j.jtho.2017.09.1205
75. Shiroyama T, Suzuki H, Tamiya M, Tamiya A, Tanaka A, Okamoto N, et al. Pretreatment advanced lung cancer inflammation index (ALI) for predicting early progression in nivolumab-treated patients with advanced non-small cell lung cancer. Cancer Med (2018) 7:13–20. doi: 10.1002/cam4.1234
76. Fukui T, Okuma Y, Nakahara Y, Otani S, Igawa S, Katagiri M, et al. Activity of nivolumab and utility of neutrophil-to-Lymphocyte ratio as a predictive biomarker for advanced non-Small-Cell lung cancer: a prospective observational study. Clin Lung Cancer (2019) 20:208–214.e2. doi: 10.1016/j.cllc.2018.04.021
77. Passiglia F, Galvano A, Castiglia M, Incorvaia L, Calò V, Listì A, et al. Monitoring blood biomarkers to predict nivolumab effectiveness in NSCLC patients. Ther Adv Med Oncol (2019) 11:1758835919839928. doi: 10.1177/1758835919839928
78. Russo A, Franchina T, Ricciardi GRR, Battaglia A, Scimone A, Berenato R, et al. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with nivolumab or docetaxel. J Cell Physiol (2018) 233:6337–43. doi: 10.1002/jcp.26609
79. Takeda T, Takeuchi M, Saitoh M, Takeda S. Neutrophil-to-lymphocyte ratio after four weeks of nivolumab administration as a predictive marker in patients with pretreated non-small-cell lung cancer: NLR in NSCLC 4 weeks after nivolumab. Thorac Cancer (2018) 9:1291–9. doi: 10.1111/1759-7714.12838
80. Amaral SR, Casal Moura M, Carvalho J, Chaves A, Jesus E, Sousa G. Prognostic significance of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in non-small cell lung cancer (NSCLC) treated with immune checkpoint inhibitors. Ann Oncol (2019) 30:i3. doi: 10.1093/annonc/mdz027.004
81. Dusselier M, Deluche E, Delacourt N, Ballouhey J, Egenod T, Melloni B, et al. Neutrophil-to-lymphocyte ratio evolution is an independent predictor of early progression of second-line nivolumab-treated patients with advanced non-small-cell lung cancers. PloS One (2019) 14:e0219060. doi: 10.1371/journal.pone.0219060
82. Ren F, Zhao T, Liu B, Pan L. Neutrophil–lymphocyte ratio (NLR) predicted prognosis for advanced non-small-cell lung cancer (NSCLC) patients who received immune checkpoint blockade (ICB). OTT (2019) 12:4235–44. doi: 10.2147/OTT.S199176
83. Pavan A, Calvetti L, Dal Maso A, Attili I, Del Bianco P, Pasello G, et al. Peripheral blood markers identify risk of immune-related toxicity in advanced non-small cell lung cancer treated with immune-checkpoint inhibitors. Oncologist (2019) 24:1128–36. doi: 10.1634/theoncologist.2018-0563
84. Banna GL, Signorelli D, Metro G, Galetta D, De Toma A, Cantale O, et al. Neutrophil-to-lymphocyte ratio in combination with PD-L1 or lactate dehydrogenase as biomarkers for high PD-L1 non-small cell lung cancer treated with first-line pembrolizumab. Transl Lung Cancer Res (2020) 9:1533–42. doi: 10.21037/tlcr-19-583
85. Banna GL, Cortellini A, Cortinovis DL, Tiseo M, Aerts JGJV, Barbieri F, et al. Corrigendum to “The lung immuno-oncology prognostic score (LIPS-3): a prognostic classification of patients receiving first-line pembrolizumab for PD-L1 ≥ 50% advanced non-small-cell lung cancer”: [ESMO open volume 6, issue 2, April 2021, 100078]. ESMO Open (2021) 6:100137. doi: 10.1016/j.esmoop.2021.100137
86. Banna GL, Tiseo M, Cortinovis DL, Facchinetti F, Aerts JGJV, Baldessari C, et al. Host immune-inflammatory markers to unravel the heterogeneous outcome and assessment of patients with PD-L1 ≥50% metastatic non-small cell lung cancer and poor performance status receiving first-line immunotherapy. Thorac Cancer (2022) 13:483–8. doi: 10.1111/1759-7714.14256
87. Peng L, Wang Y, Liu F, Qiu X, Zhang X, Fang C, et al. Peripheral blood markers predictive of outcome and immune-related adverse events in advanced non-small cell lung cancer treated with PD-1 inhibitors. Cancer Immunol Immunother (2020) 69:1813–22. doi: 10.1007/s00262-020-02585-w
88. Ayers KL, Ma M, Debussche G, Corrigan D, McCafferty J, Lee K, et al. A composite biomarker of neutrophil-lymphocyte ratio and hemoglobin level correlates with clinical response to PD-1 and PD-L1 inhibitors in advanced non-small cell lung cancers. BMC Cancer (2021) 21:441. doi: 10.1186/s12885-021-08194-9
89. Takeyasu Y, Yoshida T, Shibaki R, Matsumoto Y, Goto Y, Kanda S, et al. Differential efficacy of pembrolizumab according to metastatic sites in patients with PD-L1 strongly positive (TPS ≥ 50%) NSCLC. Clin Lung Cancer (2021) 22:127–133.e3. doi: 10.1016/j.cllc.2020.10.002
90. Russo A, Russano M, Franchina T, Migliorino MR, Aprile G, Mansueto G, et al. Neutrophil-to-Lymphocyte ratio (NLR), platelet-to-Lymphocyte ratio (PLR), and outcomes with nivolumab in pretreated non-small cell lung cancer (NSCLC): a Large retrospective multicenter study. Adv Ther (2020) 37:1145–55. doi: 10.1007/s12325-020-01229-w
91. Alessi JV, Ricciuti B, Alden SL, Bertram AA, Lin JJ, Sakhi M, et al. Low peripheral blood derived neutrophil-to-lymphocyte ratio (dNLR) is associated with increased tumor T-cell infiltration and favorable outcomes to first-line pembrolizumab in non-small cell lung cancer. J Immunother Cancer (2021) 9:e003536. doi: 10.1136/jitc-2021-003536
92. Chen S, Li R, Zhang Z, Huang Z, Cui P, Jia W, et al. Prognostic value of baseline and change in neutrophil-to-lymphocyte ratio for survival in advanced non-small cell lung cancer patients with poor performance status receiving PD-1 inhibitors. Transl Lung Cancer Res (2021) 10:1397–407. doi: 10.21037/tlcr-21-43
93. Lim JU, Kang HS, Yeo CD, Kim JS, Park CK, Kim JW, et al. Predictability of early changes in derived neutrophil-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in patients with advanced non-small cell lung cancer treated with immune checkpoint inhibitors. J Thorac Dis (2021) 13:2824–32. doi: 10.21037/jtd-20-3416
94. Jiang M, Peng W, Pu X, Chen B, Li J, Xu F, et al. Peripheral blood biomarkers associated with outcome in non-small cell lung cancer patients treated with nivolumab and durvalumab monotherapy. Front Oncol (2020) 10:913. doi: 10.3389/fonc.2020.00913
95. Petrova MP, Eneva MI, Arabadjiev JI, Conev NV, Dimitrova EG, Koynov KD, et al. 31015312. Biosci Trends (2020) 14:48–55. doi: 10.5582/bst.2019.01279
96. Xiong Q, Huang Z, Xin L, Qin B, Zhao X, Zhang J, et al. Post-treatment neutrophil-to-lymphocyte ratio (NLR) predicts response to anti-PD-1/PD-L1 antibody in SCLC patients at early phase. Cancer Immunol Immunother (2021) 70:713–20. doi: 10.1007/s00262-020-02706-5
97. Matsubara T, Takamori S, Haratake N, Toyozawa R, Miura N, Shimokawa M, et al. The impact of immune-inflammation-nutritional parameters on the prognosis of non-small cell lung cancer patients treated with atezolizumab. J Thorac Dis (2020) 12:1520–8. doi: 10.21037/jtd.2020.02.27
98. Rossi S, Toschi L, Finocchiaro G, Santoro A. Neutrophil and lymphocyte blood count as potential predictive indicators of nivolumab efficacy in metastatic non-small-cell lung cancer. Immunotherapy (2020) 12:715–24. doi: 10.2217/imt-2019-0154
99. Simonaggio A, Elaidi R, Fournier L, Fabre E, Ferrari V, Borchiellini D, et al. Variation in neutrophil to lymphocyte ratio (NLR) as predictor of outcomes in metastatic renal cell carcinoma (mRCC) and non-small cell lung cancer (mNSCLC) patients treated with nivolumab. Cancer Immunol Immunother (2020) 69:2513–22. doi: 10.1007/s00262-020-02637-1
100. Song P, Yang D, Cui X, Wang H, Si X, Zhang X, et al. NLCIPS: non-small cell lung cancer immunotherapy prognosis score. Cancer Manag Res (2020) 12:5975–85. doi: 10.2147/CMAR.S257967
101. Mezquita L, Auclin E, Ferrara R, Charrier M, Remon J, Planchard D, et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non-small cell lung cancer. JAMA Oncol (2018) 4:351–7. doi: 10.1001/jamaoncol.2017.4771
102. Seban R-D, Assié J-B, Giroux-Leprieur E, Massiani M-A, Soussan M, Bonardel G, et al. Association of the metabolic score using baseline FDG-PET/CT and dNLR with immunotherapy outcomes in advanced NSCLC patients treated with first-line pembrolizumab. Cancers (Basel) (2020) 12:E2234. doi: 10.3390/cancers12082234
103. Prelaj A, Rebuzzi SE, Pizzutilo P, Bilancia M, Montrone M, Pesola F, et al. EPSILoN: a prognostic score using clinical and blood biomarkers in advanced non-small-cell lung cancer treated with immunotherapy. Clin Lung Cancer (2020) 21:365–377.e5. doi: 10.1016/j.cllc.2019.11.017
104. Yang T, Hao L, Yang X, Luo C, Wang G, Lin Cai C, et al. Prognostic value of derived neutrophil-to-lymphocyte ratio (dNLR) in patients with non-small cell lung cancer receiving immune checkpoint inhibitors: a meta-analysis. BMJ Open (2021) 11:e049123. doi: 10.1136/bmjopen-2021-049123
105. Niu M, Liu Y, Yi M, Jiao D, Wu K. Biological characteristics and clinical significance of soluble PD-1/PD-L1 and exosomal PD-L1 in cancer. Front Immunol (2022) 13:827921. doi: 10.3389/fimmu.2022.827921
106. Bailly C, Thuru X, Quesnel B. Soluble programmed death ligand-1 (sPD-L1): a pool of circulating proteins implicated in health and diseases. Cancers (Basel) (2021) 13:3034. doi: 10.3390/cancers13123034
107. Khan M, Zhao Z, Arooj S, Fu Y, Liao G. Soluble PD-1: predictive, prognostic, and therapeutic value for cancer immunotherapy. Front Immunol (2020) 11:587460. doi: 10.3389/fimmu.2020.587460
108. Gong B, Kiyotani K, Sakata S, Nagano S, Kumehara S, Baba S, et al. Secreted PD-L1 variants mediate resistance to PD-L1 blockade therapy in non-small cell lung cancer. J Exp Med (2019) 216:982–1000. doi: 10.1084/jem.20180870
109. Sagawa R, Sakata S, Gong B, Seto Y, Takemoto A, Takagi S, et al. Soluble PD-L1 works as a decoy in lung cancer immunotherapy via alternative polyadenylation. JCI Insight (2022) 7:e153323. doi: 10.1172/jci.insight.153323
110. Zamora Atenza C, Anguera G, Riudavets Melià M, Alserawan De Lamo L, Sullivan I, Barba Joaquin A, et al. The integration of systemic and tumor PD-L1 as a predictive biomarker of clinical outcomes in patients with advanced NSCLC treated with PD-(L)1blockade agents. Cancer Immunol Immunother (2022) 71:1823–35. doi: 10.1007/s00262-021-03107-y
111. Murakami S, Shibaki R, Matsumoto Y, Yoshida T, Goto Y, Kanda S, et al. Association between serum level soluble programmed cell death ligand 1 and prognosis in patients with non-small cell lung cancer treated with anti-PD-1 antibody. Thorac Cancer (2020) 11:3585–95. doi: 10.1111/1759-7714.13721
112. Shimada Y, Matsubayashi J, Kudo Y, Maehara S, Takeuchi S, Hagiwara M, et al. Serum-derived exosomal PD-L1 expression to predict anti-PD-1 response and in patients with non-small cell lung cancer. Sci Rep (2021) 11:7830. doi: 10.1038/s41598-021-87575-3
113. Mazzaschi G, Minari R, Zecca A, Cavazzoni A, Ferri V, Mori C, et al. Soluble PD-L1 and circulating CD8+PD-1+ and NK cells enclose a prognostic and predictive immune effector score in immunotherapy treated NSCLC patients. Lung Cancer (2020) 148:1–11. doi: 10.1016/j.lungcan.2020.07.028
114. Oh SY, Kim S, Keam B, Kim TM, Kim D-W, Heo DS. Soluble PD-L1 is a predictive and prognostic biomarker in advanced cancer patients who receive immune checkpoint blockade treatment. Sci Rep (2021) 11:19712. doi: 10.1038/s41598-021-99311-y
115. Okuma Y, Wakui H, Utsumi H, Sagawa Y, Hosomi Y, Kuwano K, et al. Soluble programmed cell death ligand 1 as a novel biomarker for nivolumab therapy for non-small-cell lung cancer. Clin Lung Cancer (2018) 19:410–417.e1. doi: 10.1016/j.cllc.2018.04.014
116. Ando K, Hamada K, Watanabe M, Ohkuma R, Shida M, Onoue R, et al. Plasma levels of soluble PD-L1 correlate with tumor regression in patients with lung and gastric cancer treated with immune checkpoint inhibitors. Anticancer Res (2019) 39:5195–201. doi: 10.21873/anticanres.13716
117. Castello A, Rossi S, Toschi L, Mansi L, Lopci E. Soluble PD-L1 in NSCLC patients treated with checkpoint inhibitors and its correlation with metabolic parameters. Cancers (Basel) (2020) 12:E1373. doi: 10.3390/cancers12061373
118. Costantini A, Julie C, Dumenil C, Hélias-Rodzewicz Z, Tisserand J, Dumoulin J, et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology (2018) 7:e1452581. doi: 10.1080/2162402X.2018.1452581
119. Tiako Meyo M, Jouinot A, Giroux-Leprieur E, Fabre E, Wislez M, Alifano M, et al. Predictive value of soluble PD-1, PD-L1, VEGFA, CD40 ligand and CD44 for nivolumab therapy in advanced non-small cell lung cancer: a case-control study. Cancers (Basel) (2020) 12:E473. doi: 10.3390/cancers12020473
120. Lambert SL, Zhang C, Guo C, Turan T, Masica DL, Englert S, et al. Association of baseline and pharmacodynamic biomarkers with outcomes in patients treated with the PD-1 inhibitor budigalimab. J Immunother (2022) 45:167–79. doi: 10.1097/CJI.0000000000000408
121. Ohkuma R, Ieguchi K, Watanabe M, Takayanagi D, Goshima T, Onoue R, et al. Increased plasma soluble PD-1 concentration correlates with disease progression in patients with cancer treated with anti-PD-1 antibodies. Biomedicines (2021) 9:1929. doi: 10.3390/biomedicines9121929
122. Zhang C, Fan Y, Che X, Zhang M, Li Z, Li C, et al. Anti-PD-1 therapy response predicted by the combination of exosomal PD-L1 and CD28. Front Oncol (2020) 10:760. doi: 10.3389/fonc.2020.00760
123. Yang Q, Chen M, Gu J, Niu K, Zhao X, Zheng L, et al. Novel biomarkers of dynamic blood PD-L1 expression for immune checkpoint inhibitors in advanced non-Small-Cell lung cancer patients. Front Immunol (2021) 12:665133. doi: 10.3389/fimmu.2021.665133
124. Liao G, Zhao Z, Qian Y, Ling X, Chen S, Li X, et al. Prognostic role of soluble programmed death ligand 1 in non-small cell lung cancer: a systematic review and meta-analysis. Front Oncol (2021) 11:774131. doi: 10.3389/fonc.2021.774131
125. Cheng Y, Wang C, Wang Y, Dai L. Soluble PD-L1 as a predictive biomarker in lung cancer: a systematic review and meta-analysis. Future Oncol (2022) 18:261–73. doi: 10.2217/fon-2021-0641
126. Ricciuti B, Jones G, Severgnini M, Alessi JV, Recondo G, Lawrence M, et al. Early plasma circulating tumor DNA (ctDNA) changes predict response to first-line pembrolizumab-based therapy in non-small cell lung cancer (NSCLC). J Immunother Cancer (2021) 9:e001504. doi: 10.1136/jitc-2020-001504
127. Peng Y, Zhang C, Rui Z, Tang W, Xu Y, Tao X, et al. A comprehensive profiling of soluble immune checkpoints from the sera of patients with non-small cell lung cancer. J Clin Lab Anal (2022) 36:e24224. doi: 10.1002/jcla.24224
128. Lin D, Shen L, Luo M, Zhang K, Li J, Yang Q, et al. Circulating tumor cells: biology and clinical significance. Sig Transduct Target Ther (2021) 6:404. doi: 10.1038/s41392-021-00817-8
129. Deng Z, Wu S, Wang Y, Shi D. Circulating tumor cell isolation for cancer diagnosis and prognosis. eBioMedicine (2022) 83:104237. doi: 10.1016/j.ebiom.2022.104237
130. Jin F, Zhu L, Shao J, Yakoub M, Schmitt L, Reißfelder C, et al. Circulating tumour cells in patients with lung cancer universally indicate poor prognosis. Eur Respir Rev (2022) 31:220151. doi: 10.1183/16000617.0151-2022
131. Wankhede D, Grover S, Hofman P. Circulating tumor cells as a predictive biomarker in resectable lung cancer: a systematic review and meta-analysis. Cancers (Basel) (2022) 14:6112. doi: 10.3390/cancers14246112
132. Vasseur A, Kiavue N, Bidard F-C, Pierga J-Y, Cabel L. Clinical utility of circulating tumor cells: an update. Mol Oncol (2021) 15:1647–66. doi: 10.1002/1878-0261.12869
133. Tamminga M, de Wit S, Hiltermann TJN, Timens W, Schuuring E, Terstappen LWMM, et al. Circulating tumor cells in advanced non-small cell lung cancer patients are associated with worse tumor response to checkpoint inhibitors. J Immunother Cancer (2019) 7:173. doi: 10.1186/s40425-019-0649-2
134. Guibert N, Delaunay M, Lusque A, Boubekeur N, Rouquette I, Clermont E, et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer (2018) 120:108–12. doi: 10.1016/j.lungcan.2018.04.001
135. Alama A, Coco S, Genova C, Rossi G, Fontana V, Tagliamento M, et al. Prognostic relevance of circulating tumor cells and circulating cell-free DNA association in metastatic non-small cell lung cancer treated with nivolumab. J Clin Med (2019) 8:E1011. doi: 10.3390/jcm8071011
136. Park C-K, Oh H-J, Kim M-S, Koh B-G, Cho H-J, Kim Y-C, et al. Comprehensive analysis of blood-based biomarkers for predicting immunotherapy benefits in patients with advanced non-small cell lung cancer. Transl Lung Cancer Res (2021) 10:2103–17. doi: 10.21037/tlcr-21-100
137. Mondelo-Macía P, García-González J, León-Mateos L, Anido U, Aguín S, Abdulkader I, et al. Clinical potential of circulating free DNA and circulating tumour cells in patients with metastatic non-small-cell lung cancer treated with pembrolizumab. Mol Oncol (2021) 15:2923–40. doi: 10.1002/1878-0261.13094
138. Dall’Olio FG, Gelsomino F, Conci N, Marcolin L, De Giglio A, Grilli G, et al. PD-L1 expression in circulating tumor cells as a promising prognostic biomarker in advanced non-small-cell lung cancer treated with immune checkpoint inhibitors. Clin Lung Cancer (2021) 22:423–31. doi: 10.1016/j.cllc.2021.03.005
139. Dhar M, Wong J, Che J, Matsumoto M, Grogan T, Elashoff D, et al. Evaluation of PD-L1 expression on vortex-isolated circulating tumor cells in metastatic lung cancer. Sci Rep (2018) 8:2592. doi: 10.1038/s41598-018-19245-w
140. Ikeda M, Koh Y, Teraoka S, Sato K, Oyanagi J, Hayata A, et al. Longitudinal evaluation of PD-L1 expression on circulating tumor cells in non-small cell lung cancer patients treated with nivolumab. Cancers (Basel) (2021) 13:2290. doi: 10.3390/cancers13102290
141. Nicolazzo C, Raimondi C, Mancini M, Caponnetto S, Gradilone A, Gandini O, et al. Monitoring PD-L1 positive circulating tumor cells in non-small cell lung cancer patients treated with the PD-1 inhibitor nivolumab. Sci Rep (2016) 6:31726. doi: 10.1038/srep31726
142. Bao H, Bai T, Takata K, Yokobori T, Ohnaga T, Hisada T, et al. High expression of carcinoembryonic antigen and telomerase reverse transcriptase in circulating tumor cells is associated with poor clinical response to the immune checkpoint inhibitor nivolumab. Oncol Lett (2018) 15:3061–7. doi: 10.3892/ol.2017.7671
143. Papadaki MA, Sotiriou AI, Vasilopoulou C, Filika M, Aggouraki D, Tsoulfas PG, et al. Optimization of the enrichment of circulating tumor cells for downstream phenotypic analysis in patients with non-small cell lung cancer treated with anti-PD-1 immunotherapy. Cancers (Basel) (2020) 12:E1556. doi: 10.3390/cancers12061556
144. Ouyang Y, Liu W, Zhang N, Yang X, Li J, Long S. Prognostic significance of programmed cell death-ligand 1 expression on circulating tumor cells in various cancers: a systematic review and meta-analysis. Cancer Med (2021) 10:7021–39. doi: 10.1002/cam4.4236
145. Jiang A-M, Zheng H-R, Liu N, Zhao R, Ma Y-Y, Bai S-H, et al. Assessment of the clinical utility of circulating tumor cells at different time points in predicting prognosis of patients with small cell lung cancer: a meta-analysis. Cancer Control (2021) 28:10732748211050580. doi: 10.1177/10732748211050581
146. Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med (2004) 351:781–91. doi: 10.1056/NEJMoa040766
147. Negin BP, Cohen SJ. Circulating tumor cells in colorectal cancer: past, present, and future challenges. Curr Treat Options Oncol (2010) 11:1–13. doi: 10.1007/s11864-010-0115-3
148. Resel Folkersma L, Olivier Gómez C, San José Manso L, Veganzones de Castro S, Galante Romo I, Vidaurreta Lázaro M, et al. Immunomagnetic quantification of circulating tumoral cells in patients with prostate cancer: clinical and pathological correlation. Arch Esp Urol (2010) 63:23–31.
149. Zhang L, Zhang X, Liu Y, Zhang T, Wang Z, Gu M, et al. PD-L1+ aneuploid circulating tumor endothelial cells (CTECs) exhibit resistance to the checkpoint blockade immunotherapy in advanced NSCLC patients. Cancer Lett (2020) 469:355–66. doi: 10.1016/j.canlet.2019.10.041
150. Hu B, Gong Y, Wang Y, Xie J, Cheng J, Huang Q. Comprehensive atlas of circulating rare cells detected by SE-iFISH and image scanning platform in patients with various diseases. Front Oncol (2022) 12:821454. doi: 10.3389/fonc.2022.821454
151. Genna A, Vanwynsberghe AM, Villard AV, Pottier C, Ancel J, Polette M, et al. EMT-associated heterogeneity in circulating tumor cells: sticky friends on the road to metastasis. Cancers (Basel) (2020) 12. doi: 10.3390/cancers12061632
152. Bonanno L, Dal Maso A, Pavan A, Zulato E, Calvetti L, Pasello G, et al. Liquid biopsy and non-small cell lung cancer: are we looking at the tip of the iceberg? Br J Cancer (2022) 127:383–93. doi: 10.1038/s41416-022-01777-8
153. Peng Y, Mei W, Ma K, Zeng C. Circulating tumor DNA and minimal residual disease (MRD) in solid tumors: current horizons and future perspectives. Front Oncol (2021) 11:763790. doi: 10.3389/fonc.2021.763790
154. Cheng ML, Pectasides E, Hanna GJ, Parsons HA, Choudhury AD, Oxnard GR. Circulating tumor DNA in advanced solid tumors: clinical relevance and future directions. CA Cancer J Clin (2021) 71:176–90. doi: 10.3322/caac.21650
155. Thompson JC, Carpenter EL, Silva BA, Rosenstein J, Chien AL, Quinn K, et al. Serial monitoring of circulating tumor DNA by next-generation gene sequencing as a biomarker of response and survival in patients with advanced NSCLC receiving pembrolizumab-based therapy. JCO Precis Oncol (2021) 5:PO.20.00321. doi: 10.1200/PO.20.00321
156. Chen Y, Li X, Liu G, Chen S, Xu M, Song L, et al. ctDNA concentration, MIKI67 mutations and hyper-progressive disease related gene mutations are prognostic markers for camrelizumab and apatinib combined multiline treatment in advanced NSCLC. Front Oncol (2020) 10:1706. doi: 10.3389/fonc.2020.01706
157. Hellmann MD, Nabet BY, Rizvi H, Chaudhuri AA, Wells DK, Dunphy MPS, et al. Circulating tumor DNA analysis to assess risk of progression after long-term response to PD-(L)1 blockade in NSCLC. Clin Cancer Res (2020) 26:2849–58. doi: 10.1158/1078-0432.CCR-19-3418
158. Raja R, Kuziora M, Brohawn PZ, Higgs BW, Gupta A, Dennis PA, et al. Early reduction in ctDNA predicts survival in patients with lung and bladder cancer treated with durvalumab. Clin Cancer Res (2018) 24:6212–22. doi: 10.1158/1078-0432.CCR-18-0386
159. Anagnostou V, Forde PM, White JR, Niknafs N, Hruban C, Naidoo J, et al. Dynamics of tumor and immune responses during immune checkpoint blockade in non-small cell lung cancer. Cancer Res (2019) 79:1214–25. doi: 10.1158/0008-5472.CAN-18-1127
160. Li L, Wang Y, Shi W, Zhu M, Liu Z, Luo N, et al. Serial ultra-deep sequencing of circulating tumor DNA reveals the clonal evolution in non-small cell lung cancer patients treated with anti-PD1 immunotherapy. Cancer Med (2019) 8:7669–78. doi: 10.1002/cam4.2632
161. Chen Y-T, Seeruttun SR, Wu X-Y, Wang Z-X. Maximum somatic allele frequency in combination with blood-based tumor mutational burden to predict the efficacy of atezolizumab in advanced non-small cell lung cancer: a pooled analysis of the randomized POPLAR and OAK studies. Front Oncol (2019) 9:1432. doi: 10.3389/fonc.2019.01432
162. Goldberg SB, Narayan A, Kole AJ, Decker RH, Teysir J, Carriero NJ, et al. Early assessment of lung cancer immunotherapy response via circulating tumor DNA. Clin Cancer Res (2018) 24:1872–80. doi: 10.1158/1078-0432.CCR-17-1341
163. Iijima Y, Hirotsu Y, Amemiya K, Ooka Y, Mochizuki H, Oyama T, et al. Very early response of circulating tumour–derived DNA in plasma predicts efficacy of nivolumab treatment in patients with non–small cell lung cancer. Eur J Cancer (2017) 86:349–57. doi: 10.1016/j.ejca.2017.09.004
164. Giroux Leprieur E, Herbretau G, Dumenil C, Julie C, Giraud V, Labrune S, et al. Circulating tumor DNA evaluated by next-generation sequencing is predictive of tumor response and prolonged clinical benefit with nivolumab in advanced non-small cell lung cancer. Oncoimmunology (2018) 7:e1424675. doi: 10.1080/2162402X.2018.1424675
165. Nicolas G, Jones G, Beeler JF, Plagnol V, Morris C, Mourlanette J, et al. Targeted sequencing of plasma cell-free DNA to predict response to PD1 inhibitors in advanced non-small cell lung cancer. Lung Cancer (2019) 137:1–6. doi: 10.1016/j.lungcan.2019.09.005
166. Sun Y, Duan J, Fang W, Wang Z, Du X, Wang X, et al. Identification and validation of tissue or ctDNA PTPRD phosphatase domain deleterious mutations as prognostic and predictive biomarkers for immune checkpoint inhibitors in non-squamous NSCLC. BMC Med (2021) 19:239. doi: 10.1186/s12916-021-02075-5
167. Brueckl NF, Wirtz RM, Reich FPM, Veltrup E, Zeitler G, Meyer C, et al. Predictive value of mRNA expression and dynamic changes from immune related biomarkers in liquid biopsies before and after start of pembrolizumab in stage IV non-small cell lung cancer (NSCLC). Transl Lung Cancer Res (2021) 10:4106–19. doi: 10.21037/tlcr-21-587
168. van der Leest P, Hiddinga B, Miedema A, Aguirre Azpurua ML, Rifaela N, Ter Elst A, et al. Circulating tumor DNA as a biomarker for monitoring early treatment responses of patients with advanced lung adenocarcinoma receiving immune checkpoint inhibitors. Mol Oncol (2021) 15:2910–22. doi: 10.1002/1878-0261.13090
169. Wang H, Zhou F, Qiao M, Li X, Zhao C, Cheng L, et al. The role of circulating tumor DNA in advanced non-small cell lung cancer patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Front Oncol (2021) 11:671874. doi: 10.3389/fonc.2021.671874
170. Schumacher TN, Schreiber RD. Neoantigens in cancer immunotherapy. Science (2015) 348:69–74. doi: 10.1126/science.aaa4971
171. Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discovery (2019) 18:197–218. doi: 10.1038/s41573-018-0007-y
172. Hellmann MD, Ciuleanu T-E, Pluzanski A, Lee JS, Otterson GA, Audigier-Valette C, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med (2018) 378:2093–104. doi: 10.1056/NEJMoa1801946
173. Hellmann MD, Callahan MK, Awad MM, Calvo E, Ascierto PA, Atmaca A, et al. Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell (2018) 33:853–861.e4. doi: 10.1016/j.ccell.2018.04.001
174. Gandara DR, Paul SM, Kowanetz M, Schleifman E, Zou W, Li Y, et al. Blood-based tumor mutational burden as a predictor of clinical benefit in non-small-cell lung cancer patients treated with atezolizumab. Nat Med (2018) 24:1441–8. doi: 10.1038/s41591-018-0134-3
175. Wang Z, Duan J, Cai S, Han M, Dong H, Zhao J, et al. Assessment of blood tumor mutational burden as a potential biomarker for immunotherapy in patients with non-small cell lung cancer with use of a next-generation sequencing cancer gene panel. JAMA Oncol (2019) 5:696–702. doi: 10.1001/jamaoncol.2018.7098
176. Wang Z, Duan J, Wang G, Zhao J, Xu J, Han J, et al. Allele frequency-adjusted blood-based tumor mutational burden as a predictor of overall survival for patients with NSCLC treated with PD-(L)1 inhibitors. J Thorac Oncol (2020) 15:556–67. doi: 10.1016/j.jtho.2019.12.001
177. Ba H, Liu L, Peng Q, Chen J, Zhu Y-D. The relationship between blood-based tumor mutation burden level and efficacy of PD-1/PD-L1 inhibitors in advanced non-small cell lung cancer: a systematic review and meta-analysis. BMC Cancer (2021) 21:1220. doi: 10.1186/s12885-021-08924-z
178. Chae YK, Davis AA, Agte S, Pan A, Simon NI, Iams WT, et al. Clinical implications of circulating tumor DNA tumor mutational burden (ctDNA TMB) in non-small cell lung cancer. Oncologist (2019) 24:820–8. doi: 10.1634/theoncologist.2018-0433
179. Jiang T, Chen J, Xu X, Cheng Y, Chen G, Pan Y, et al. On-treatment blood TMB as predictors for camrelizumab plus chemotherapy in advanced lung squamous cell carcinoma: biomarker analysis of a phase III trial. Mol Cancer (2022) 21:4. doi: 10.1186/s12943-021-01479-4
180. Kim ES, Velcheti V, Mekhail T, Yun C, Shagan SM, Hu S, et al. Blood-based tumor mutational burden as a biomarker for atezolizumab in non-small cell lung cancer: the phase 2 b-F1RST trial. Nat Med (2022) 28:939–45. doi: 10.1038/s41591-022-01754-x
181. Rizvi NA, Cho BC, Reinmuth N, Lee KH, Luft A, Ahn M-J, et al. Durvalumab with or without tremelimumab vs standard chemotherapy in first-line treatment of metastatic non-small cell lung cancer: the MYSTIC phase 3 randomized clinical trial. JAMA Oncol (2020) 6:661–74. doi: 10.1001/jamaoncol.2020.0237
182. Chen X, Fang L, Zhu Y, Bao Z, Wang Q, Liu R, et al. Blood tumor mutation burden can predict the clinical response to immune checkpoint inhibitors in advanced non-small cell lung cancer patients. Cancer Immunol Immunother (2021) 70:3513–24. doi: 10.1007/s00262-021-02943-2
183. Ma Y, Li Q, Du Y, Cai J, Chen W, Zhao G, et al. Blood tumor mutational burden as a predictive biomarker in patients with advanced non-small cell lung cancer (NSCLC). Front Oncol (2021) 11:640761. doi: 10.3389/fonc.2021.640761
184. Wang X, Ricciuti B, Nguyen T, Li X, Rabin MS, Awad MM, et al. Association between smoking history and tumor mutation burden in advanced non-small cell lung cancer. Cancer Res (2021) 81:2566–73. doi: 10.1158/0008-5472.CAN-20-3991
185. Chmielewska I, Stencel K, Kalinka E, Ramlau R, Krawczyk P. Neoadjuvant and adjuvant immunotherapy in non-small cell lung cancer-clinical trials experience. Cancers (Basel) (2021) 13:5048. doi: 10.3390/cancers13205048
186. Provencio M, Serna-Blasco R, Nadal E, Insa A, García-Campelo MR, Casal Rubio J, et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non-Small-Cell lung cancer (NADIM phase II trial). J Clin Oncol (2022) 40(25):JCO2102660. doi: 10.1200/JCO.21.02660
187. Meri-Abad M, Moreno-Manuel A, García SG, Calabuig-Fariñas S, Pérez RS, Herrero CC, et al. Clinical and technical insights of tumour mutational burden in non-small cell lung cancer. Crit Rev Oncology/Hematology (2023) 182:103891. doi: 10.1016/j.critrevonc.2022.103891
188. Lam VK, Zhang J. Blood-based tumor mutation burden: continued progress toward personalizing immunotherapy in non-small cell lung cancer. J Thorac Dis (2019) 11:2208–11. doi: 10.21037/jtd.2019.05.68
189. Ancel J, Perotin J-M, Dewolf M, Launois C, Mulette P, Nawrocki-Raby B, et al. Hypoxia in lung cancer management: a translational approach. Cancers (Basel) (2021) 13:3421. doi: 10.3390/cancers13143421
190. Costantini A, Takam Kamga P, Dumenil C, Chinet T, Emile J-F, Giroux Leprieur E. Plasma biomarkers and immune checkpoint inhibitors in non-small cell lung cancer: new tools for better patient selection? Cancers (Basel) (2019) 11:E1269. doi: 10.3390/cancers11091269
191. Wang Q, He Y, Li W, Xu X, Hu Q, Bian Z, et al. Soluble immune checkpoint-related proteins in blood are associated with invasion and progression in non-small cell lung cancer. Front Immunol (2022) 13:887916. doi: 10.3389/fimmu.2022.887916
192. Zhou L, Zhang M, Li R, Xue J, Lu Y. Pseudoprogression and hyperprogression in lung cancer: a comprehensive review of literature. J Cancer Res Clin Oncol (2020) 146:3269–79. doi: 10.1007/s00432-020-03360-1
Keywords: liquid biopsy, soluble biomarkers, immunotherapy, non-small cell lung cancer (NSCLC), neutrophil lymphocyte ratio (NLR), circulating tumor (ctDNA), circulating tumor cell (CTC)
Citation: Ancel J, Dormoy V, Raby BN, Dalstein V, Durlach A, Dewolf M, Gilles C, Polette M and Deslée G (2023) Soluble biomarkers to predict clinical outcomes in non-small cell lung cancer treated by immune checkpoints inhibitors. Front. Immunol. 14:1171649. doi: 10.3389/fimmu.2023.1171649
Received: 22 February 2023; Accepted: 11 May 2023;
Published: 22 May 2023.
Edited by:
Jian Song, University Hospital Münster, GermanyReviewed by:
Yu Yao, The First Affiliated Hospital of Xi’an Jiaotong University, ChinaCopyright © 2023 Ancel, Dormoy, Raby, Dalstein, Durlach, Dewolf, Gilles, Polette and Deslée. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julien Ancel, amFuY2VsQGNodS1yZWltcy5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.