 Feifeng Wu
Feifeng Wu Cuifang Li
Cuifang Li Jueyi Mao
Jueyi Mao Junquan Zhu
Junquan Zhu Chuan Wen
Chuan Wen- Department of Pediatrics, The Second Xiangya Hospital, Central South University, Changsha, China
Background: Immune thrombocytopenia (ITP) is an autoimmune disease characterized by isolated thrombocytopenia. Recently, the pathophysiology and novel drugs of ITP have been the focus of researchers with plenty of publications emerging. Bibliometrics is the process of extracting measurable data through statistical analysis of published research studies to provide an insight into the trends and hotspots.
Objective: This study aimed to provide an insight into developing trends and hotspots in the field of ITP by bibliometric analysis.
Methods: By using three bibliometric mapping tools (bibliometrix R package, VOSviewer, CiteSpace), we summarized the overview information of retrieved publications, as well as the analysis of keyword co-occurrence and reference co-citation.
Results: A total of 3299 publications with 78066 citations on ITP research were included in the analysis. The keyword co-occurrence network identified 4 clusters relating to the diagnosis, pathophysiology, and treatment of ITP respectively. Then the reference co-citation analysis produced 12 clusters with a well-structured and highly credible clustering model, and they can be divided into 5 trends: second-line treatment, chronic ITP, novel therapy and pathogenesis, COVID-19 vaccine. Treg cells, spleen tyrosine kinase, and mesenchymal stem cells were the latest hotspots with strong burstness.
Conclusion: This bibliometric analysis provided a comprehensive insight into research hotspots and trends on ITP, which would enrich the review of the ITP research.
1 Introduction
Immune thrombocytopenia (ITP) is an autoimmune disease characterized by isolated thrombocytopenia. Patients may be asymptomatic at presentation, or they may present with mild mucocutaneous or life-threatening bleeding (1). The pathophysiology of ITP is complex and remains incompletely understood. The classical theory stated that platelet destruction and impaired megakaryocyte maturation were caused by autoantibodies (2). In addition, T-cell-mediated cytotoxicity toward platelets and megakaryocytes has been proven to be one of the important mechanisms (3, 4). In recent years, the pathogenesis of ITP has been further explored and found to be extensive, encompassing cellular immunity, humoral immunity, and bone marrow microenvironment (2). The emergence of new drugs, such as thrombopoietin receptor agonists (TPO-RAs), made the treatment of ITP no longer limited to immune suppression and splenectomy (5). The research aimed to explore a new pathology and treatment of ITP has gained increased attention with many publications.
The rapid progress and development of medical science in recent years have led to an exponential growth of academic papers every year, resulting in so-called information overload or filtering failure (6). Scholars often found it difficult to grasp the trends and hotspots of research in a huge literature base. Bibliometrics is the process of extracting measurable data through statistical analysis of published research studies and shows how the knowledge within a publication is used, providing a broad synthesis of a research field and demonstrating how it has changed over time, as well as identifying influential studies or scholars (6). It can not only enable researchers to gain a clearer overview of the research on a given topic but also identifies research abundancies, gaps, and trends of potential moderators (7). Thus, bibliometric analysis was wildly used in various fields in the last decade. Recently, Yang Ou et al. performed a bibliometric analysis of primary ITP from 2011 to 2021, which provided novel insights for researchers on future research trends and scientific decision-making (8). However, in the first decade of the 21st century, there have been some breakthroughs in the exploration of the pathogenesis and treatment of ITP, such as CD8+ T cells and TPO-RAs, and these documents were significant for understanding the lineage and direction of the field (3, 9). Encouraged by previous studies, we performed a bibliometric analysis of the literature concerning ITP for the last 20+ years (1999–2022), hoping to provide a comprehensive analysis of the research trends and hotspots.
2 Materials and methods
The data used in this study were retrieved from the Web of Science Core Collection database (WoSCC) on October 16, 2022. The search keyword query was: TI= “Idiopathic Thrombocytopenic Purpura*” OR “Immune Thrombocytopenic Purpura*” OR “Immune Thrombocytopenia*” OR “Werlhof* Disease” OR “Autoimmune Thrombocytopenia*” OR “Autoimmune Thrombocytopenic Purpura*” OR ITP. The database source was limited to the Web of Science Citation Index Expanded (SCI-Expanded) with a publication date from January 1, 1999, to October 16, 2022. Original articles and reviews were included as document types since they can represent the current status of research in a field (10, 11). The language was limited to English. Then, the “full record and cited references” of the retrieved documents were extracted in text files. Two of the authors reviewed all titles and abstracts independently to determine their eligibility. In case of disagreement, it was solved through discussion or further recourse to a third person. Before further bibliometric analysis, Python programming language was used for data cleaning, mainly to remove duplicates and replace synonyms. In addition, some results were presented in two parts to make them more rational: basic science papers (mainly including in vivo and in vitro experiments exploring the pathology and mechanisms of ITP) and clinical papers (mainly including guidelines, clinical trials, case reports, etc.).
Many bibliometric mapping software tools have been created and used by scholars. In this study, we chose the widely used tools for the analysis (12). For descriptive analysis, we used the bibliometrix R package (13) to analyze the amounts of publications, citations, and the trends of growth, as well as top authors, sources, cited sources, and their impact. We used several indicators, including the number of publications, the average number of citations, the h-index, and the g-index, to assess the impact of authors. The h-index is the highest number of papers that received h or more citations among a set of papers, while the g-index is the highest number g of papers that together received g2 or more citations (14, 15). Both two indicators can reflect the publication (quantity) and citation (quality). For network mapping, VosViewer (16) (version 1.6.18; http://www.VOSviewer.com/) was used to analyze the co-occurrence of keywords and co-authorship between countries/regions. The networks of co-cited references and the burstness of keywords were analyzed by CiteSpace (17) (version 6.1.3; http://cluster.ischool.drexel.edu/~cchen/citespace/).
3 Results
3.1 The overview of publications
The search in the WoSCC database resulted in a total of 3,402 publications, including original articles and reviews, without duplications. After two authors assessed eligibility, 104 documents unrelated to ITP were excluded, and finally, 3299 articles were included in the analysis, comprising 808 basic research papers and 2491 clinical papers. The main information about all documents and the two subgroups was shown in Table 1. During the recent decades, both publications and citations had a steady increase, with annual publication numbers peaking in 2021 (Figure 1). The average growth rate of the literature was 3.27% over the last 20 years. The annual growth rate of basic science papers was higher than that of clinical papers at 8% and 2.31%, respectively. By 2021, the cumulative number of citations was 78066, and the average number of citations per document was 23.59, with similar citation frequencies between the two subgroups (21.1 and 24.4, respectively).
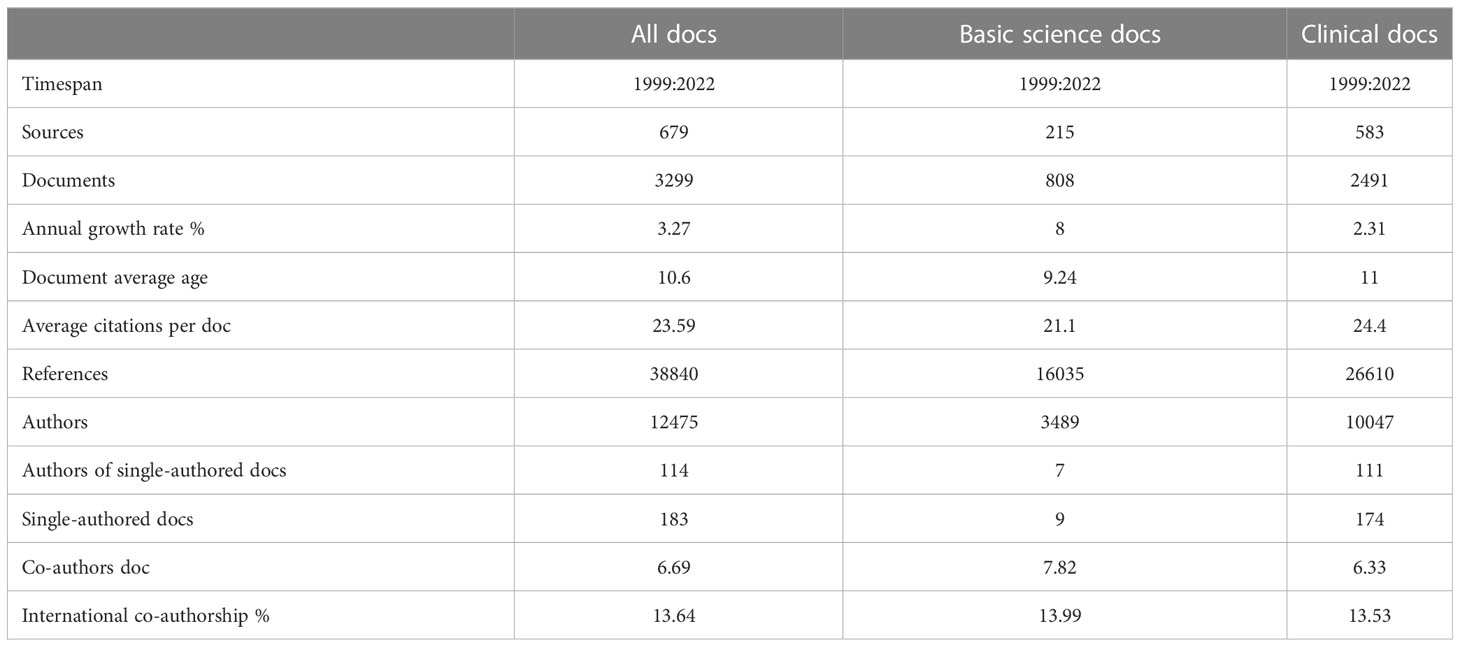
Table 1 Main information about data.
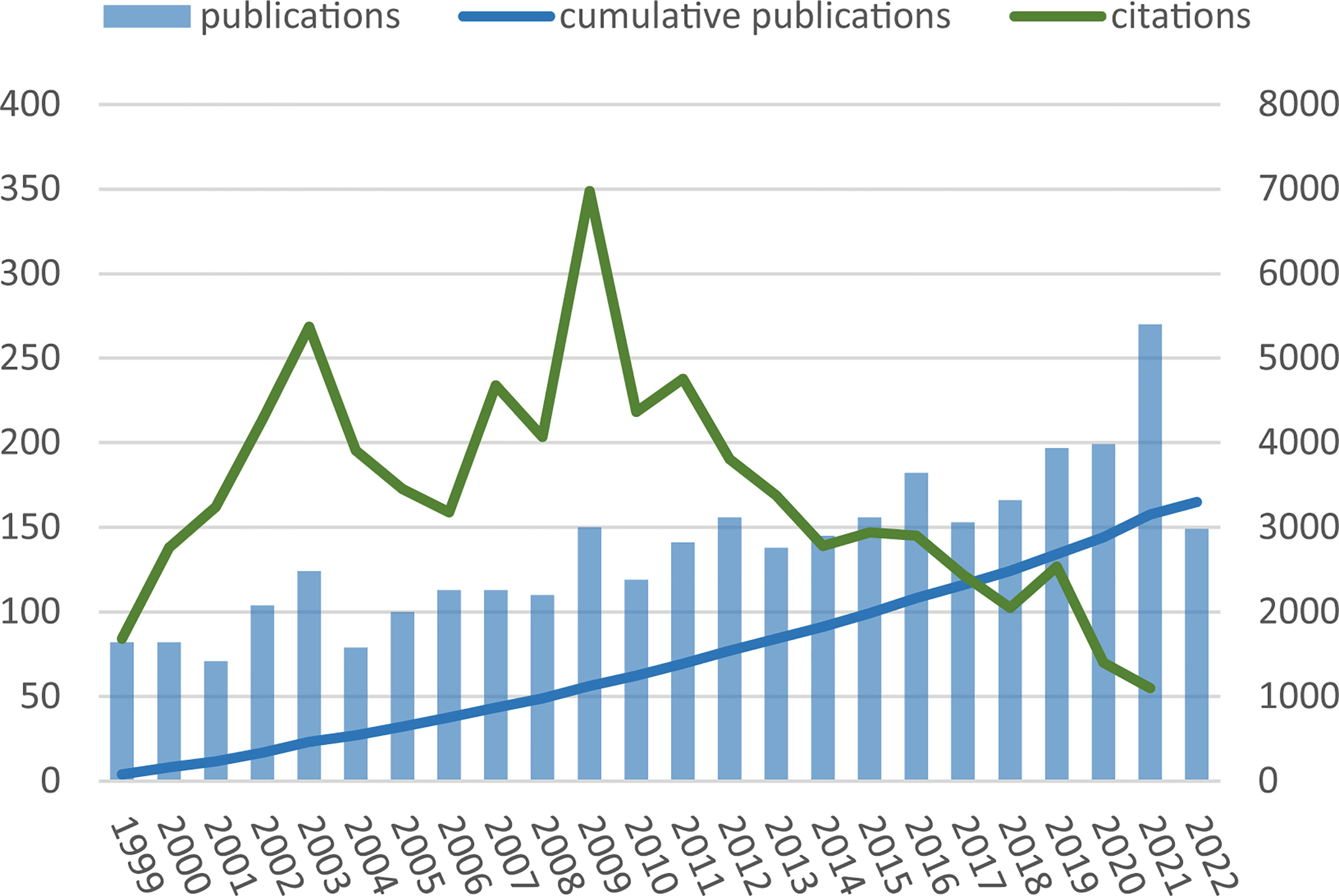
Figure 1 Annual publications and citations over time.
3.2 Authors, institutions, regions, and sources of publications
The total number of authors retrieved in the documents was 12,475, with an average of 6 authors per article. A total of 75.8% of the authors wrote only one article (Figure S1). The ten most productive and influential authors in the two groups were presented in Figure 2A. In general, the most-productive author in the basic science group was Hou M, who published 82 papers with 24 citations per doc and also had the highest g-index and h-index. On the other hand, Bussel JB published the highest number of clinical articles. The top authors’ production over time was presented in Figure 2B. The co-authorship network showed that Peng J and Hou M collaborated closely, and the two scholars focused on the pathogenesis of ITP (18–20). In addition, two collaborative groups centered around Bussel JB and Godeau B, respectively, significantly contributed to clinical trials and management guidelines (Figure 2D) (21, 22).
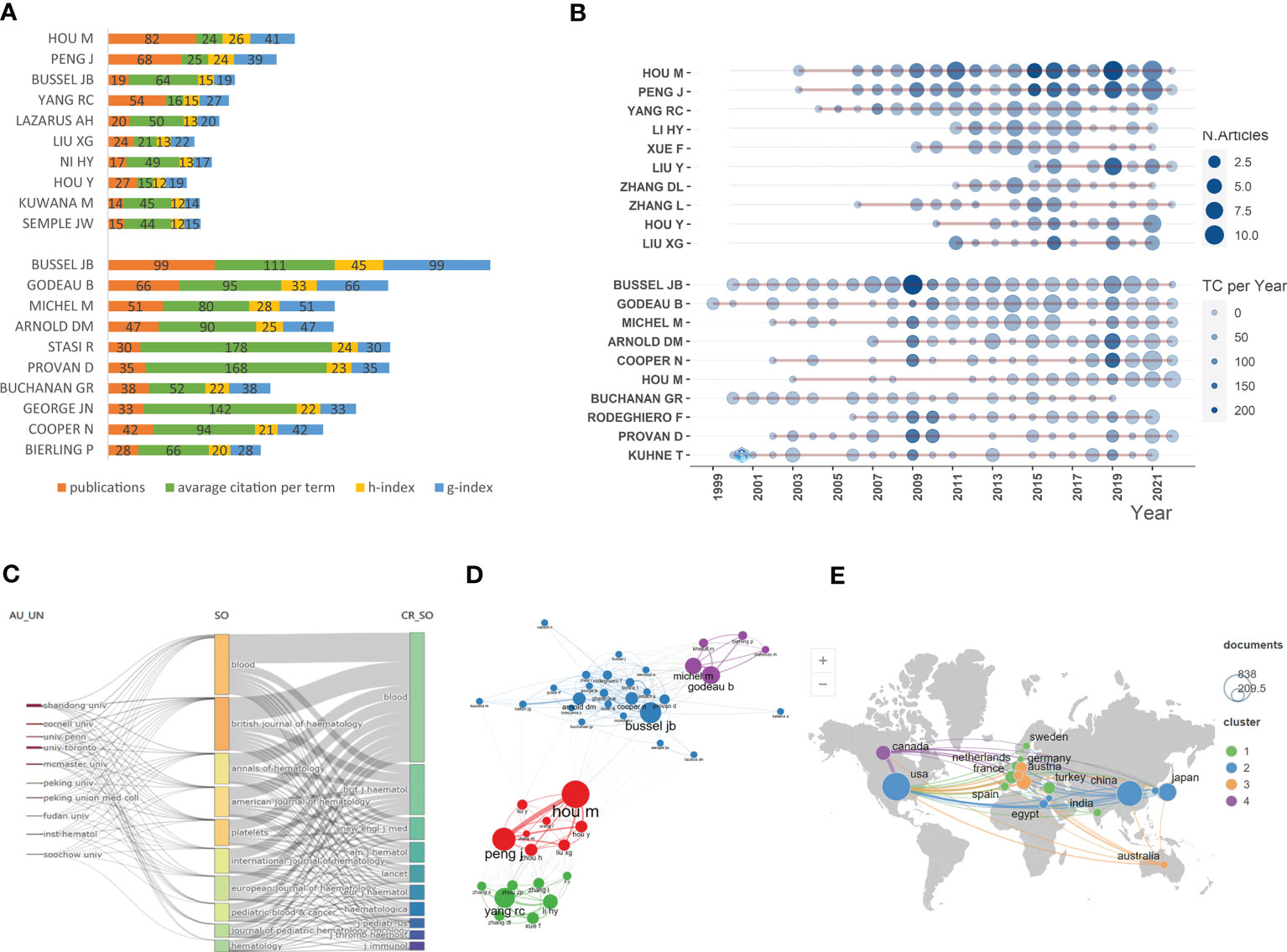
Figure 2 Descriptive statistical analyses of publications on ITP. (A) Publications and impact of the most-contributing authors in basic science papers (top) and clinical papers (bottom). (B) Top authors’ production over time in basic science papers (top) and clinical papers (bottom). (C) A Sankey diagram between institutions, sources and cited sources. (D) Co-authorship network of the authors in the field of ITP. (E) Global geographical distribution and network visualization map of country/region collaborations.
We also analyzed the main institutions and sources implicated in the field. As shown in Figure 2C, four of ten highly productive institutions were in China, with Shandong University topping the ranking, indicating that institutions in China played a crucial role in ITP research. A total of 3299 papers related to ITP were published in a wide range of 679 journals. Blood and British Journal of Haematology contributed a large portion of the ten journals with the greatest number of ITP-related articles, both of which belong to the Journal Citation Reports (JCR) “hematology” category. Meanwhile, references cited in the documents were mainly from the two journals. The top ten productive and locally cited sources were shown in Table S1, S2 respectively. According to the global geographical distribution and network visualization map, most papers were published by authors from North America and East Asia (Figure 2E). Further, the United States of America (USA) contributed the most published papers, followed by China and Japan. The international cooperation visualization map showed that USA collaborated most closely with China and Japan, while collaborations among other countries were scattered.
3.3 Keyword co-occurrence analysis
Author keywords, an essential part of an article given by the authors, can represent the research topic of a publication. To explore the research trends and hotspots, 279 out of 2610 keywords with a frequency of 5 and above were extracted for the co-occurrence analysis in VOSviewer. The 60 most frequently occurring keywords were shown in Table 2. In the network visualization, keywords could be classified into 4 clusters (Figure 3A). Cluster 1 (red) was the largest cluster mainly related to the diagnosis and manifestations of ITP, where the nodes were close to the center of the network (such as “bleeding,” “thrombocytopenia,” and “autoantibody”) and closely distributed. Cluster 2 (green) focused on basic research on the pathological mechanisms of ITP, including keywords such as “T cell subset,” “Treg cell,” “Th17 cell,” “interleukin,” “DNA methylation,” “apoptosis,” etc. Cluster 3 (blue) primarily referred to the management of ITP as evidenced by keywords “glucocorticoids,” “rituximab,” “spleen tyrosine kinase,” “splenectomy,” “eltrombopag,” etc. The last cluster (yellow) was small and only included a few keywords, such as “splenectomy.”
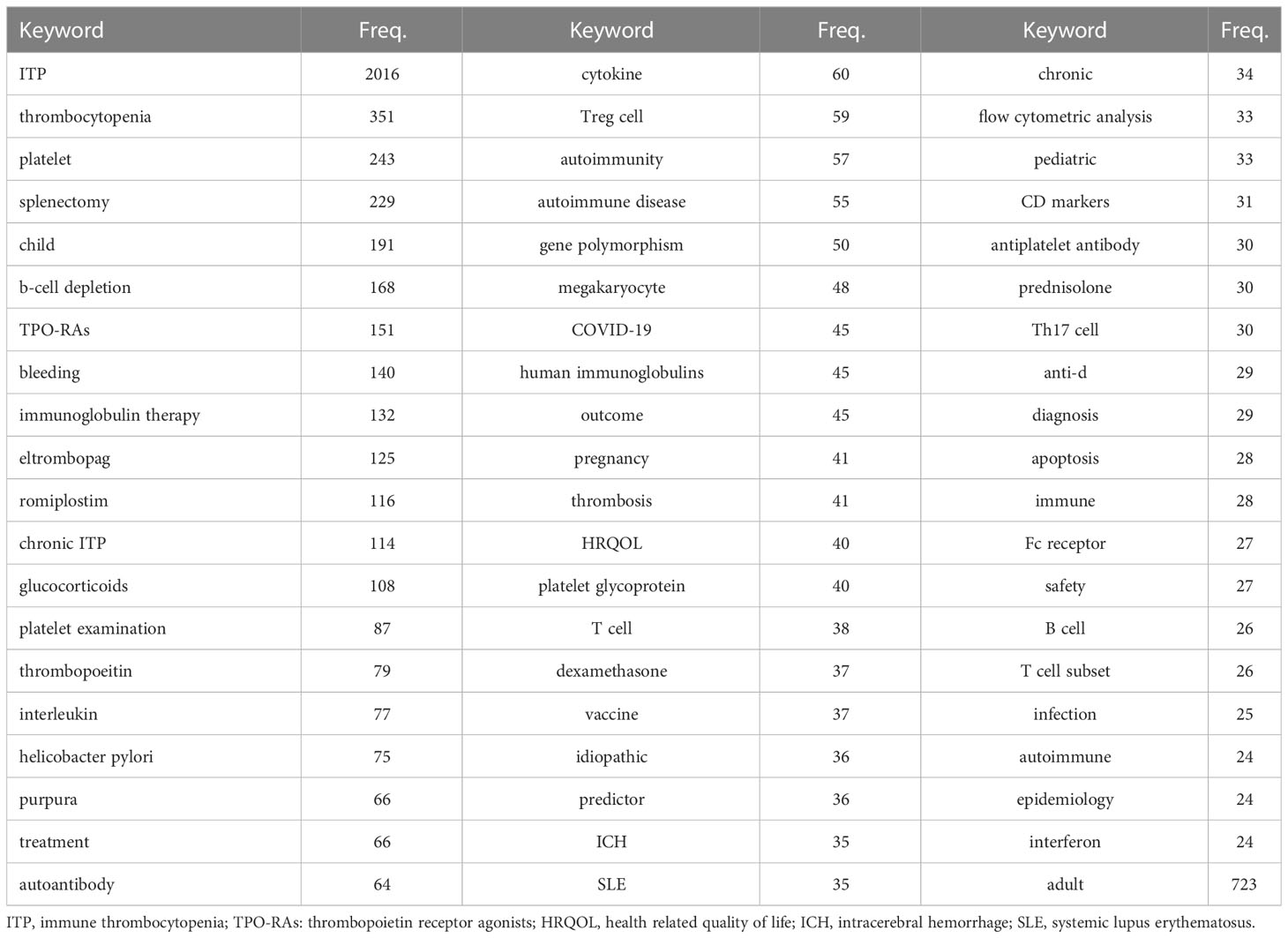
Table 2 High occurrences keywords in ITP research.
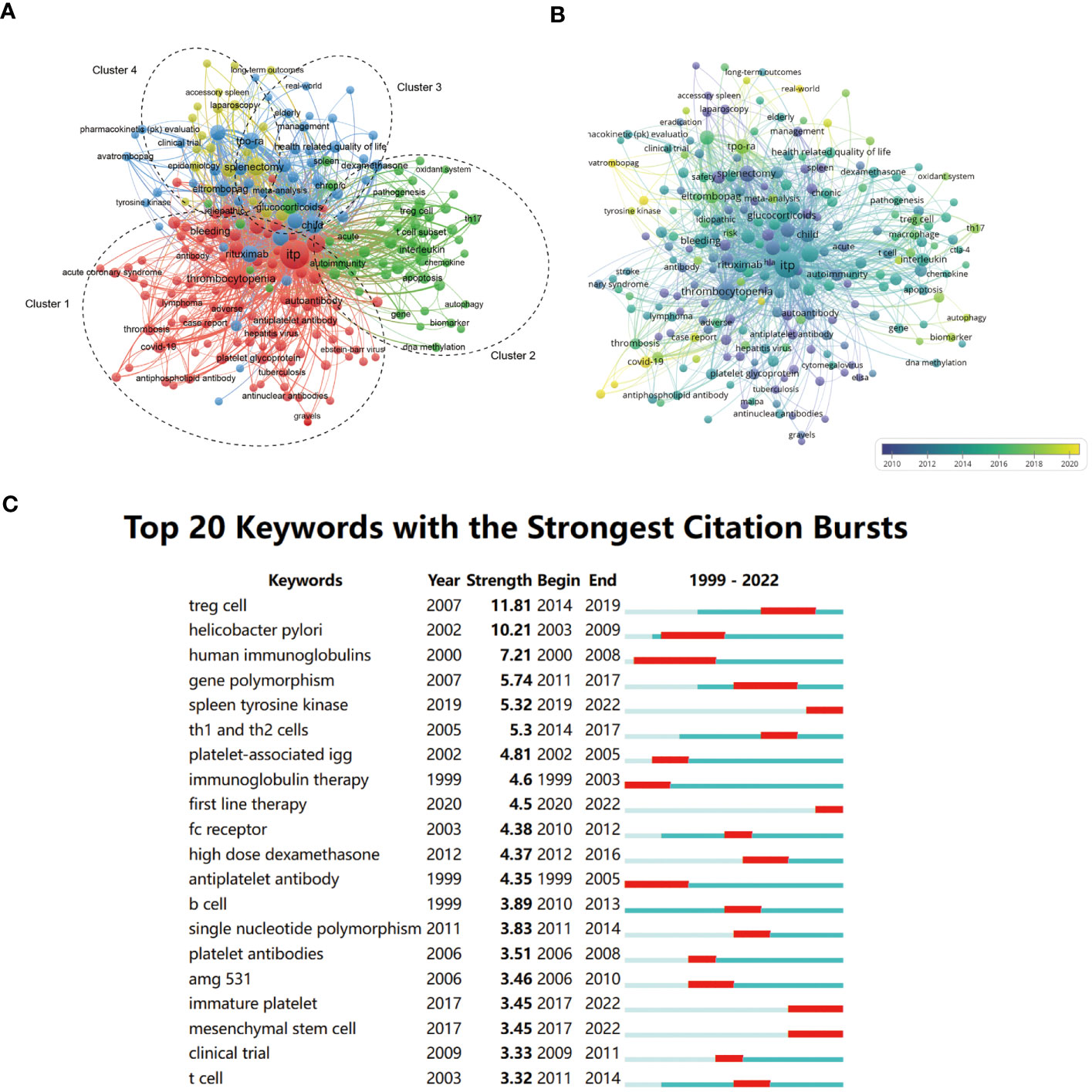
Figure 3 network visualization (A), overlay visualization (B), and top citation burst (C) of keyword co-occurrence analysis. (A) In the network visualization, items (nodes) are represented by different keywords. The size of the nodes is determined by the number of occurrences and the color represented the cluster to which the item belongs. In general, the closer two nodes are located to each other, the stronger their relatedness. All nodes are divided into four clusters (dotted circles). (B) An overlay visualization based on the average publication year. The size and position of the nodes are the same as (A). The color of the nodes represents the average publication year, and the corresponding relationship is shown in the legend. (C) The top 20 keywords with the strongest citation bursts. The red bold line represents the burst years.
We plotted the overlay visualization for the co-occurring author keyword network to analyze the trends of the study. The color of an item was determined by the average publication year, where colors ranged from blue (earlier) to green and yellow (latest). It showed that keywords such as “COVID-19,” “avatrombopag,” and “tyrosine kinase” were newly emerging research topics. “Th17 cell,” “TPO-RAs,” and “autophagy” were hotspots in latest five years. In addition, the analysis of burstness (Figure 3C) revealed that “Treg cell” was the keyword with the strongest burst in 2014–2019. When focusing on the last five years, more attention was paid to “spleen tyrosine kinase,” “first-line therapy,” “immature platelet,” and “mesenchymal stem cells.”
3.4 Reference co-citation analysis
In general, bibliometric outcomes included citation, co-citation, and co-occurrence. Co-citation is defined as when two published articles are cited together by another publication. We further extracted the co-citation network using CiteSpace (Figure 4). The network presented a high Q value (Q = 0.7426) and a t silhouette score (S = 0.9091), indicating a well-structured and highly credible clustering model (23). Finally, 12 clusters were identified and could be further classified into five research trends.
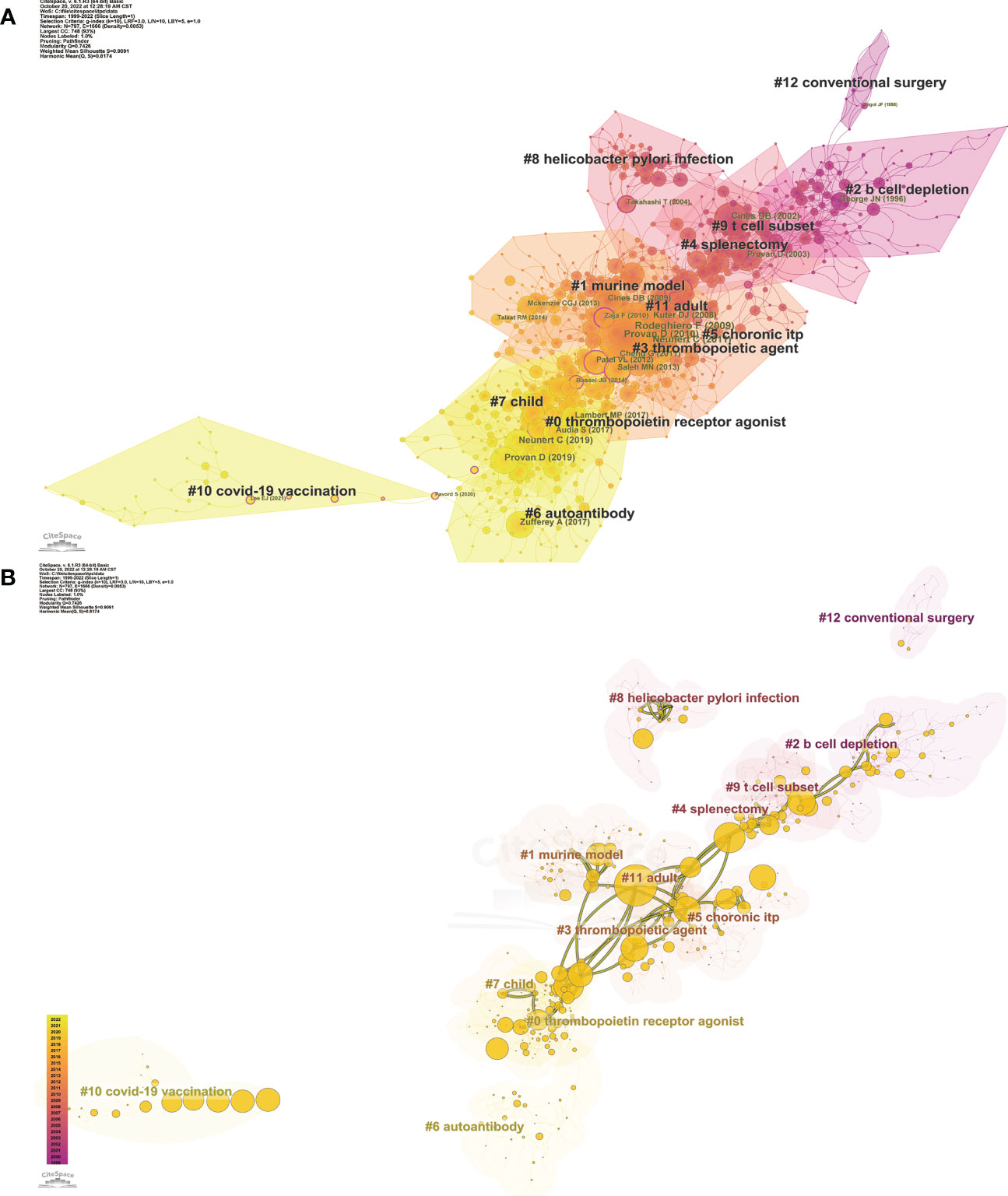
Figure 4 Co-citation references network (A) and correspondent betweenness centrality analysis (B) by CiteSpace. (A) The network with cluster visualization indicated different research hotspots. The nodes presented different references, the size and color of a node are determined by the co-citation frequency and publication year respectively. Annual citations of each reference are rendered as citation tree rings. The most recent citations correspond to the innermost rings. The network is decomposed into clusters of references based on the strengths of co-citation links. Clusters are numbered in descending order of their size. The largest one is numbered as #0, followed by #1, and so on. (B) The Visualization map with overlays of main paths (red) and core references (yellow) is organized by betweenness centrality, revealing the key hubs to connect different clusters. The centrality scores are normalized to the unit interval of [0,1], and the higher the score, the larger the node. The color of a link represented the earliest time slice in which the connection was first made.
The first trend started with cluster #12 conventional surgery and evolved to cluster #2 B cell depletion. The trend mainly included publications relating to the second-line treatment of ITP. It shared hotspots with and then gradually evolved to clusters #4, #5, and #9. Conventional splenectomy was once considered the first choice for drug-resistant chronic ITP (cITP). Many patients received surgery and achieved remission (24). In the 1990s, many scholars compared laparoscopic surgery with conventional surgery, suggesting the superiority of laparoscopic splenectomy in terms of rapid recovery and short hospital stay (25, 26). Otherwise, children with ITP were less likely to undergo splenectomy. However, due to the potential adverse effects including the operative complications and the risk of fatal bacterial infection (27), the place of splenectomy as the second-line treatment has been gradually challenged by other therapy approaches, such as B cell depletion (28).
The second trend was a topic concerning chronic ITP, including 4 clusters: #5 chronic ITP, #9 T cell subset. #4 splenectomy, and #8 Helicobacter pylori infection. Approximately 25% to 30% of adult patients developed cITP that was refractory to corticosteroids and splenectomy and other available treatments (28). The cause of cITP is not clear and may be related to some risk factors. Several groups have recently reported that eradication of Helicobacter pylori led to platelet recovery in patients with cITP, but little was known about the pathogenesis of cITP. Takahashi T et al. have further elucidated the role of molecular mimicry and cross-reactivity between PAIgG and H. pylori CagA protein (29). Even though the exact mechanism remained unclear, multiple guidelines have recommended eradication therapy of H. pylori in patients with cITP (30, 31). The immune imbalance of T cell subsets was the focus of pathogenic mechanism research and thought to be strongly associated with cITP. This was consistent with the hotspots of cluster 2 in the keyword network analysis. Among these studies, regulatory T cells (Treg cells), helper T cells (Th cells), and other T cell subsets were well studied (32).
Next, the two main trends were closely related to each other, where both the number and size of nodes significantly increased, suggesting that the research on ITP was in full swing with plenty of publications published and cited. The clusters here could be divided into clinical and basic research. The former included cluster #11 adult, #3 thrombopoietic agent, #7 child, and #0 TPO-RA, mainly including clinical trials and management guidelines for different patient groups. The latter included cluster #1 murine model and #6 autoantibody, suggesting that the pathogenesis of ITP has always been a focused area.
The last and latest trend discussed the topic of vaccination, which was introduced by a single cluster #10 COVID-19 vaccination. The COVID-19 pandemic has led to urgent development and widespread use of SARS-CoV-2 vaccines. Vaccines are crucial for protecting vulnerable groups, such as the old, the young, and the patients suffering from other diseases. Meanwhile, due to the potentially higher risk of adverse reactions, the indication of vaccination in this population has become the focus of public attention. Thrombocytopenia caused by vaccination was reported as early as the 20th century (33, 34). Recently, it has been reported that ITP may be identified de novo after SARS-CoV-2 vaccination, and the condition may worsen in part of preexisting ITP, especially in post-splenectomy patients and those with more refractory disease (35). Practical guidance has been formulated for the assessment and management of patients with ITP during the COVID-19 pandemic (36).
3.5 Developing trend analysis
Furthermore, we introduced temporal metrics, citation burstness, to measure the rate of change in a specific duration, thus, identifying emergent terms. The top 25 references with the strongest citation bursts were presented in Figure 5, in which the former items were all focused on guidelines for ITP from different organizations (31, 37, 38). In addition, reviews related to pathological mechanisms have recently also received more attention (39, 40). Among the basic research papers, the work that received a high citation burst for the first time illustrated the role of CD8+ cytotoxic T cells in platelet destruction, with important implications for elucidating the pathogenesis of ITP (3). The overlays of main paths and core references were presented in Figure 4B to analyze the developing trend. Nodes with high betweenness centrality generally connect different clusters and are considered key hubs, exerting a great influence on a network (7). Among these nodes, some references were highly connected to other nodes and positioned between different clusters, which could be seen as landmark works in the context of the research area of ITP. It was evidenced that the trend of ITP was based on the exploration of new therapies; meanwhile, research on related pathogenesis was always on the way. Throughout the development of ITP research, clinical and basic topics have been closely integrated and progressed together. There has been a remarkable temporal evolution in the treatment of ITP, from splenectomy and B-cell depletion therapy at the beginning of the 21st century to thrombopoietic agents and TPO-RAs in the last decade.
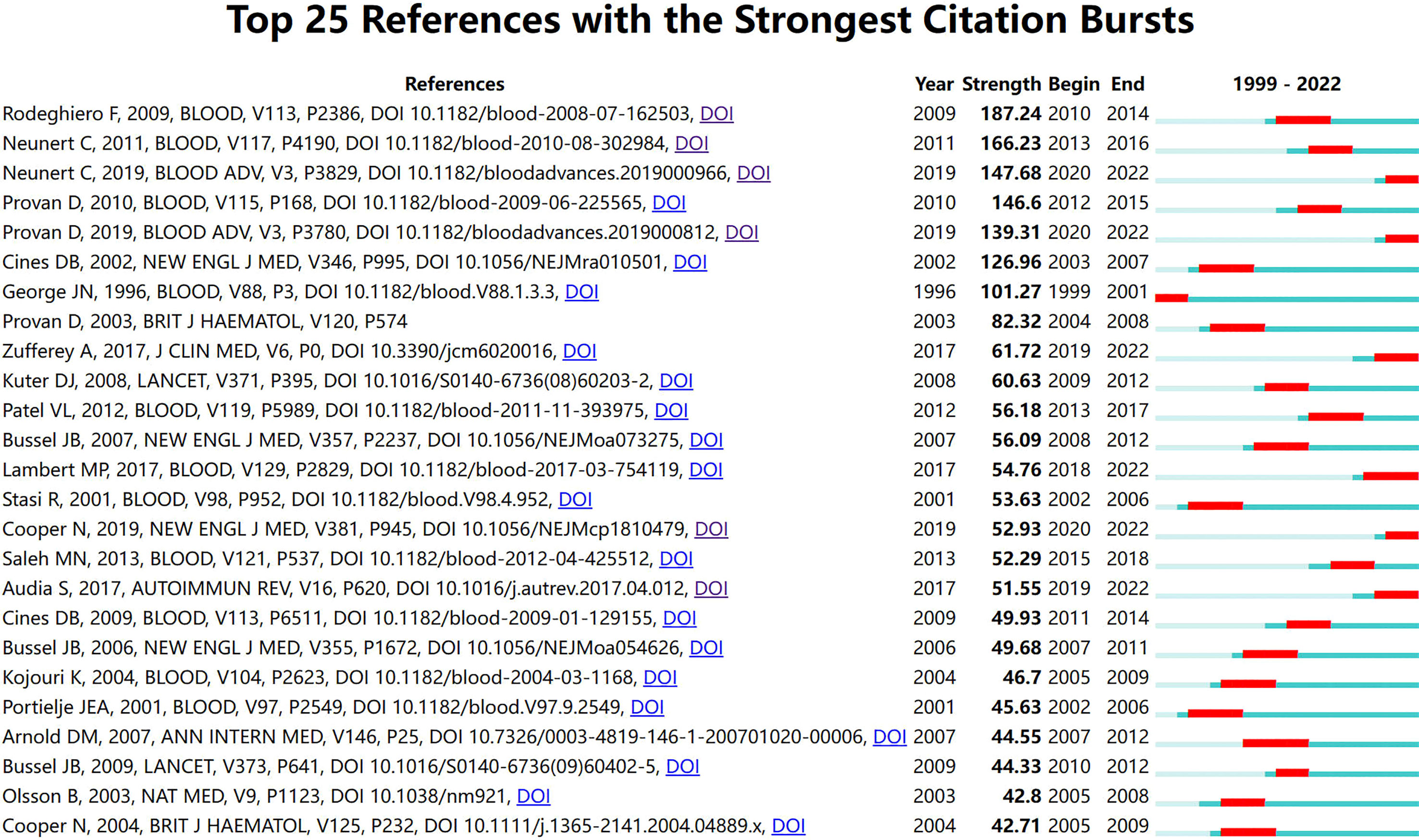
Figure 5 The top 25 references with the strongest citation bursts. The red bold line represents the burst years.
4 Discussion
Our research enriched the review of the research field of ITP. Based on the bibliometric analysis, it could be concluded that the study of novel therapy and pathogenesis of ITP were the main research hotspots. Beginning with the study showing that the infusion of plasma from patients with ITP to healthy volunteers would lead to thrombocytopenia (41), the study on the pathophysiology of ITP has never ceased. In the above-mentioned analysis, Treg cells and Th cells (mainly Th17 and Th1) were topics with high frequency and strong bursts, indicating that their role in ITP has been intensely investigated. The significance of Th17 cells was confirmed in a previous bibliometric analysis study about the ITP field in the last decade (8). Notably, our results showed that Treg cells also attracted much attention in T cell subsets. Since the first study suggested that lack of T cell suppression was responsible for platelet destruction, an impressive output of papers showed that T cell homeostasis played a predominant role (42). Treg cells, which were responsible for immune tolerance, have been studied the most during a long period, and these cells were deficient in ITP and failed to suppress the excessive auto-reactive T cells (43, 44). Furthermore, the imbalance of Th cells has been evidenced by an increasing polarization of Th1 and Th17 cells, as well as their cytokines (45). Increased Th17 cells and related cytokines have been evidenced in ITP patients and mice and correlated with the course of the disease and response to treatment (46–48).
A better understanding of the pathophysiology has promoted the development of new drugs. Over the decades, immunosuppression has been the essential method in traditional therapy of ITP, such as glucocorticoids and immunoglobulin. There are often some patients who are resistant to these treatments or suffer from the side effects of long-term medication. The decision regarding the second-line treatment for ITP has been debated for a long time. Recently, many new alternative drugs have emerged, among which TPO-RAs has been the most popular. As early as the 20th century, researchers began to explore novel therapy to replace or reduce the use of immunosuppressive drugs, such as the first-generation TPO mimetic drugs and recombinant human TPO. Although it did increase platelet counts, its clinical efficacy was limited as it may be neutralized by antibodies in patients (49). In 2008, the second-generation TPO mimetic drugs, eltrombopag and romiplostim, were licensed in the USA for the treatment of ITP, and since then, their use has progressively increased around the world (5, 50). TPO-RAs were well-tolerated and effective drugs for ITP with acceptable toxicity, which have been soon recommended by specialists as second-line therapy for ITP and even as first-line treatment in some patients (31, 51, 52). Besides, other new agents that function by preventing FcyR-mediated platelet destruction were also attractive and have been proven for clinical or advanced phase, including spleen tyrosine kinase (Syk) inhibitors, Bruton tyrosine kinase inhibitors (BTKIs), and neonatal Fc receptor inhibitors (2). Among them, Syk, one of the hot spots of research in recent years, was involved in FcγR-mediated platelet destruction and has been considered a therapeutic target for ITP (53). Its inhibitor Fostamatinib was approved by the FDA in 2018 as a new second-line agent for the treatment of ITP (54). Finally, mesenchymal stem cells (MSCs) have been highly studied in autoimmune diseases due to their immunomodulatory ability. Similarly, it has recently attracted attention in the ITP field (Figure 3C). Impaired bone marrow MSCs play an important role in the pathogenesis of ITP (55, 56). Meanwhile, the infusion of MSCs to patients with refractory ITP has also been supported by clinical evidence of encouraging efficacy (57, 58). Thus, MSCs have great potential in ITP, which is worthy of further exploration.
This study had some limitations. Compared to narrative reviews, bibliometric analysis can handle thousands of publications to comprehensively reveal the developing trends and topics of research. However, since the analysis method is based on the publications and their references, it is inevitably affected by various biases, such as publication bias and citation bias (59). The results may sometimes be biased in the keywords-based analysis because some keywords of papers are not as accurate. For example, regarding Th17 cells, a cell of high interest to scholars, the frequency of this keyword was only 30, which was much lower than the number of articles retrieved from the database. Second, the data analyzed in this study were only retrieved from the WoSCC, leading to the relative incompleteness of the retrieved publication. Nevertheless, the WoSCC has been broadly accepted among researchers and was considered a common tool for both retrieving and bibliometric analysis due to its high quality and integrity of data (60, 61). Besides, the article type and language of publications were limited, which might have led to the same concern.
Despite the limitations, this study also had strengths. First, this study provided a bibliometric analysis of the literature in the ITP field over the last 20 years, which would contribute to the understanding of research hotspots and developing trends in this field. Compared with previous research, we merged the synonyms in the keywords before the analysis, which could minimize the information omission caused by the scattered distribution of keywords due to synonyms. In addition, the analysis in this study was conjunctively achieved by three widely-used tools (CiteSpace, VOSviewer, and R package) for better visualization. Furthermore, the bibliometric outcomes of this study included citation, co-citation, and co-occurrence, and different types of visualization mapping were drew to comprehensively elucidate the research field. We studied multiple bibliometric indicators (for example, citations, g index, and h index were employed to evaluate the impact), temporal metrics, such as citation burstness, and structural metrics, such as betweenness centrality.
This bibliometric analysis provided a comprehensive insight into research hotspots and trends on ITP. Both publications and citations have witnessed a steady increase over the decades. USA, China, and Japan were the countries that studied ITP most and worked closely with each other. In the further analysis of 3299 publications, the research on pathophysiology and treatment of ITP was identified as the research hotspot, such as TPO-RAs, T cell subsets, etc. In addition, COVID-2019, Syk, and MSCs were emerging hot issues. Therefore, this study can help researchers better explore the development and trends of this field.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
FW: Formal analysis and writing-original draft. CL: Data curation and validation. JM: Software and methodology. JZ and YW: Conceptualization. CW: Reviewing and editing, supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1160048/full#supplementary-material
Abbreviations
ITP, immune thrombocytopenia; TPO-RAs, thrombopoietin receptor agonists; WoSCC, Web of Science Core Collection database; SCI-Expanded, Science Citation Index Expanded; cITP, chronic ITP; Treg cells, regulatory T cells; Th cells, helper T cells; Syk, spleen tyrosine kinase; BTKIs, Bruton tyrosine kinase inhibitors; MSCs, mesenchymal stem cells.
References
1. Cooper N, Ghanima W. Immune thrombocytopenia. N Engl J Med (2019) 381(10):945–55. doi: 10.1056/NEJMcp1810479
2. Provan D, Semple JW. Recent advances in the mechanisms and treatment of immune thrombocytopenia. EBioMedicine (2022) 76:103820. doi: 10.1016/j.ebiom.2022.103820
3. Olsson B, Andersson PO, Jernås M, Jacobsson S, Carlsson B, Carlsson LM, et al. T-Cell-mediated cytotoxicity toward platelets in chronic idiopathic thrombocytopenic purpura. Nat Med (2003) 9(9):1123–4. doi: 10.1038/nm921
4. Semple JW, Rebetz J, Maouia A, Kapur R. An update on the pathophysiology of immune thrombocytopenia. Curr Opin Hematol (2020) 27(6):423–9. doi: 10.1097/moh.0000000000000612
5. Ghanima W, Cooper N, Rodeghiero F, Godeau B, Bussel JB. Thrombopoietin receptor agonists: ten years later. Haematologica (2019) 104(6):1112–23. doi: 10.3324/haematol.2018.212845
6. Agarwal A, Durairajanayagam D, Tatagari S, Esteves SC, Harlev A, Henkel R, et al. Bibliometrics: tracking research impact by selecting the appropriate metrics. Asian J Androl (2016) 18(2):296–309. doi: 10.4103/1008-682x.171582
7. Sabe M, Pillinger T, Kaiser S, Chen C, Taipale H, Tanskanen A, et al. Half a century of research on antipsychotics and schizophrenia: a scientometric study of hotspots, nodes, bursts, and trends. Neurosci Biobehav Rev (2022) 136:104608. doi: 10.1016/j.neubiorev.2022.104608
8. Ou Y, Zhan Y, Zhuang X, Shao X, Xu P, Li F, et al. A bibliometric analysis of primary immune thrombocytopenia from 2011 to 2021. Br J Haematol (2023). doi: 10.1111/bjh.18692
9. Panzer S, Pabinger I. Eltrombopag in chronic idiopathic thrombocytopenic purpura. Lancet (2009) 373(9664):607–8. doi: 10.1016/s0140-6736(09)60377-9
10. Van Leeuwen TN, Visser MS, Moed HF, Nederhof TJ, Van Raan AFJ. The holy grail of science policy: exploring and combining bibliometric tools in search of scientific excellence. Scientometrics (2003) 57(2):257–80. doi: 10.1023/A:1024141819302
11. Chen C, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: a scientometric update (2000 - 2014). Expert Opin Biol Ther (2014) 14(9):1295–317. doi: 10.1517/14712598.2014.920813
12. Pan X, Yan E, Cui M, Hua W. Examining the usage, citation, and diffusion patterns of bibliometric mapping software: a comparative study of three tools. J Informetrics (2018) 12(2):481–93. doi: 10.1016/j.joi.2018.03.005
13. Aria M, Cuccurullo C. Bibliometrix: an r-tool for comprehensive science mapping analysis. J Informetrics (2017) 11(4):959–75. doi: 10.1016/j.joi.2017.08.007
14. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U.S.A. (2005) 102(46):16569–72. doi: 10.1073/pnas.0507655102
16. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
17. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U.S.A. (2004) 101 Suppl 1(Suppl 1):5303–10. doi: 10.1073/pnas.0307513100
18. Yang L, Wang L, Zhao CH, Zhu XJ, Hou Y, Jun P, et al. Contributions of TRAIL-mediated megakaryocyte apoptosis to impaired megakaryocyte and platelet production in immune thrombocytopenia. Blood (2010) 116(20):4307–16. doi: 10.1182/blood-2010-02-267435
19. Peng J, Liu C, Liu D, Ren C, Li W, Wang Z, et al. Effects of B7-blocking agent and/or CsA on induction of platelet-specific T-cell anergy in chronic autoimmune thrombocytopenic purpura. Blood (2003) 101(7):2721–6. doi: 10.1182/blood-2002-06-1666
20. Zhao HY, Ma YH, Li DQ, Sun T, Li LZ, Li P, et al. Low-dose chidamide restores immune tolerance in ITP in mice and humans. Blood (2019) 133(7):730–42. doi: 10.1182/blood-2018-05-847624
21. Mahévas M, Michel M, Godeau B. How we manage immune thrombocytopenia in the elderly. Br J Haematol (2016) 173(6):844–56. doi: 10.1111/bjh.14067
22. Bussel JB, Cheng G, Saleh MN, Psaila B, Kovaleva L, Meddeb B, et al. Eltrombopag for the treatment of chronic idiopathic thrombocytopenic purpura. N Engl J Med (2007) 357(22):2237–47. doi: 10.1056/NEJMoa073275
23. Shibata N, Kajikawa Y, Takeda Y, Matsushima K. Detecting emerging research fronts based on topological measures in citation networks of scientific publications. Technovation (2008) 28(11):758–75. doi: 10.1016/j.technovation.2008.03.009
24. Akwari OE, Itani KM, Coleman RE, Rosse WF. Splenectomy for primary and recurrent immune thrombocytopenic purpura (ITP). current criteria for patient selection and results. Ann Surg (1987) 206(4):529–41. doi: 10.1097/00000658-198710000-00014
25. Marassi A, Vignali A, Zuliani W, Biguzzi E, Bergamo C, Gianotti L, et al. Splenectomy for idiopathic thrombocytopenic purpura: comparison of laparoscopic and conventional surgery. Surg Endosc (1999) 13(1):17–20. doi: 10.1007/s004649900889
26. Friedman RL, Fallas MJ, Carroll BJ, Hiatt JR, Phillips EH. Laparoscopic splenectomy for ITP. the gold standard. Surg Endosc (1996) 10(10):991–5. doi: 10.1007/s004649900221
27. Eraklis AJ, Kevy SV, Diamond LK, Gross RE. Hazard of overwhelming infection after splenectomy in childhood. N Engl J Med (1967) 276(22):1225–9. doi: 10.1056/nejm196706012762203
28. Stasi R, Pagano A, Stipa E, Amadori S. Rituximab chimeric anti-CD20 monoclonal antibody treatment for adults with chronic idiopathic thrombocytopenic purpura. Blood (2001) 98(4):952–7. doi: 10.1182/blood.v98.4.952
29. Takahashi T, Yujiri T, Shinohara K, Inoue Y, Sato Y, Fujii Y, et al. Molecular mimicry by helicobacter pylori CagA protein may be involved in the pathogenesis of h. pylori-associated chronic idiopathic thrombocytopenic purpura. Br J Haematol (2004) 124(1):91–6. doi: 10.1046/j.1365-2141.2003.04735.x
30. Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP, Kuipers EJ, Axon AT, et al. Management of helicobacter pylori infection-the maastricht V/Florence consensus report. Gut (2017) 66(1):6–30. doi: 10.1136/gutjnl-2016-312288
31. Neunert C, Terrell DR, Arnold DM, Buchanan G, Cines DB, Cooper N, et al. American Society of hematology 2019 guidelines for immune thrombocytopenia. Blood Adv (2019) 3(23):3829–66. doi: 10.1182/bloodadvances.2019000966
32. Kuwana M, Kaburaki J, Kitasato H, Kato M, Kawai S, Kawakami Y, et al. Immunodominant epitopes on glycoprotein IIb-IIIa recognized by autoreactive T cells in patients with immune thrombocytopenic purpura. Blood (2001) 98(1):130–9. doi: 10.1182/blood.v98.1.130
33. Oski FA, Naiman JL. Effect of live measles vaccine on the platelet count. N Engl J Med (1966) 275(7):352–6. doi: 10.1056/nejm196608182750703
34. Grimaldi-Bensouda L, Michel M, Aubrun E, Leighton P, Viallard JF, Adoue D, et al. A case-control study to assess the risk of immune thrombocytopenia associated with vaccines. Blood (2012) 120(25):4938–44. doi: 10.1182/blood-2012-05-431098
35. Lee EJ, Beltrami-Moreira M, Al-Samkari H, Cuker A, DiRaimo J, Gernsheimer T, et al. SARS-CoV-2 vaccination and ITP in patients with de novo or preexisting ITP. Blood (2022) 139(10):1564–74. doi: 10.1182/blood.2021013411
36. Pavord S, Thachil J, Hunt BJ, Murphy M, Lowe G, Laffan M, et al. Practical guidance for the management of adults with immune thrombocytopenia during the COVID-19 pandemic. Br J Haematol (2020) 189(6):1038–43. doi: 10.1111/bjh.16775
37. Rodeghiero F, Stasi R, Gernsheimer T, Michel M, Provan D, Arnold DM, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood (2009) 113(11):2386–93. doi: 10.1182/blood-2008-07-162503
38. Neunert C, Lim W, Crowther M, Cohen A, Solberg L Jr, Crowther MA. The American society of hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood (2011) 117(16):4190–207. doi: 10.1182/blood-2010-08-302984
39. Zufferey A, Kapur R, Semple JW. Pathogenesis and therapeutic mechanisms in immune thrombocytopenia (ITP). J Clin Med (2017) 6(2):16. doi: 10.3390/jcm6020016
40. Audia S, Mahévas M, Samson M, Godeau B, Bonnotte B. Pathogenesis of immune thrombocytopenia. Autoimmun Rev (2017) 16(6):620–32. doi: 10.1016/j.autrev.2017.04.012
41. Harrington WJ, Minnich V, Hollingsworth JW, Moore CV. Demonstration of a thrombocytopenic factor in the blood of patients with thrombocytopenic purpura. J Lab Clin Med (1951) 38(1):1–10.
42. Ji X, Zhang L, Peng J, Hou M. T Cell immune abnormalities in immune thrombocytopenia. J Hematol Oncol (2014) 7:72. doi: 10.1186/s13045-014-0072-6
43. Han P, Hou Y, Zhao Y, Liu Y, Yu T, Sun Y, et al. Low-dose decitabine modulates T-cell homeostasis and restores immune tolerance in immune thrombocytopenia. Blood (2021) 138(8):674–88. doi: 10.1182/blood.2020008477
44. Aslam R, Hu Y, Gebremeskel S, Segel GB, Speck ER, Guo L, et al. Thymic retention of CD4+CD25+FoxP3+ T regulatory cells is associated with their peripheral deficiency and thrombocytopenia in a murine model of immune thrombocytopenia. Blood (2012) 120(10):2127–32. doi: 10.1182/blood-2012-02-413526
45. Qin J, Liu Q, Liu A, Leng S, Wang S, Li C, et al. Empagliflozin modulates CD4(+) T-cell differentiation via metabolic reprogramming in immune thrombocytopenia. Br J Haematol (2022) 198(4):765–75. doi: 10.1111/bjh.18293
46. Gu H, Chen Z, Shi X, Cui H, Qin X, Hu H, et al. Increased proportion of Th17/Treg cells at the new diagnosed stage of chronic immune thrombocytopenia in pediatrics: the pilot study from a multi-center. Eur J Pediatr (2021) 180(11):3411–7. doi: 10.1007/s00431-021-04121-z
47. Rocha AM, Souza C, Rocha GA, de Melo FF, Clementino NC, Marino MC, et al. The levels of IL-17A and of the cytokines involved in Th17 cell commitment are increased in patients with chronic immune thrombocytopenia. Haematologica (2011) 96(10):1560–4. doi: 10.3324/haematol.2011.046417
48. Zhang Y, Ma T, Zhou X, Chen J, Li J. Circulating level of Th17 cells is associated with sensitivity to glucocorticoids in patients with immune thrombocytopenia. Int J Hematol (2018) 107(4):442–50. doi: 10.1007/s12185-017-2392-0
49. Li J, Yang C, Xia Y, Bertino A, Glaspy J, Roberts M, et al. Thrombocytopenia caused by the development of antibodies to thrombopoietin. Blood (2001) 98(12):3241–8. doi: 10.1182/blood.v98.12.3241
50. Lambert MP, Gernsheimer TB. Clinical updates in adult immune thrombocytopenia. Blood (2017) 129(21):2829–35. doi: 10.1182/blood-2017-03-754119
51. Kuter DJ. The biology of thrombopoietin and thrombopoietin receptor agonists. Int J Hematol (2013) 98(1):10–23. doi: 10.1007/s12185-013-1382-0
52. Provan D, Arnold DM, Bussel JB, Chong BH, Cooper N, Gernsheimer T, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv (2019) 3(22):3780–817. doi: 10.1182/bloodadvances.2019000812
53. Crowley MT, Costello PS, Fitzer-Attas CJ, Turner M, Meng F, Lowell C, et al. A critical role for syk in signal transduction and phagocytosis mediated by fcgamma receptors on macrophages. J Exp Med (1997) 186(7):1027–39. doi: 10.1084/jem.186.7.1027
54. Connell NT, Berliner N. Fostamatinib for the treatment of chronic immune thrombocytopenia. Blood (2019) 133(19):2027–30. doi: 10.1182/blood-2018-11-852491
55. Rossi F, Tortora C, Palumbo G, Punzo F, Argenziano M, Casale M, et al. CB2 receptor stimulation and dexamethasone restore the anti-inflammatory and immune-regulatory properties of mesenchymal stromal cells of children with immune thrombocytopenia. Int J Mol Sci (2019) 20(5):1049. doi: 10.3390/ijms20051049
56. Zhang J, Zhu X, Xue J, Liu X, Long Zheng X, Chang Y, et al. Integrated mRNA and miRNA profiling revealed deregulation of cellular stress response in bone marrow mesenchymal stem cells derived from patients with immune thrombocytopenia. Funct Integr Genomics (2018) 18(3):287–99. doi: 10.1007/s10142-018-0591-2
57. Wang X, Yin X, Sun W, Bai J, Shen Y, Ao Q, et al. Intravenous infusion umbilical cord-derived mesenchymal stem cell in primary immune thrombocytopenia: a two-year follow-up. Exp Ther Med (2017) 13(5):2255–8. doi: 10.3892/etm.2017.4229
58. Fang B, Mai L, Li N, Song Y. Favorable response of chronic refractory immune thrombocytopenic purpura to mesenchymal stem cells. Stem Cells Dev (2012) 21(3):497–502. doi: 10.1089/scd.2011.0231
59. Urlings MJE, Duyx B, Swaen GMH, Bouter LM, Zeegers MP. Citation bias and other determinants of citation in biomedical research: findings from six citation networks. J Clin Epidemiol (2021) 132:71–8. doi: 10.1016/j.jclinepi.2020.11.019
60. Ding X, Yang Z. Knowledge mapping of platform research: a visual analysis using VOSviewer and CiteSpace. Electronic Commerce Res (2022) 22(3):787–809. doi: 10.1007/s10660-020-09410-7
Keywords: immune thrombocytopenia, bibliometric analysis, citespace, VOSviewer, research hotspot and trends
Citation: Wu F, Li C, Mao J, Zhu J, Wang Y and Wen C (2023) Knowledge mapping of immune thrombocytopenia: a bibliometric study. Front. Immunol. 14:1160048. doi: 10.3389/fimmu.2023.1160048
Received: 06 February 2023; Accepted: 21 April 2023;
Published: 03 May 2023.
Edited by:
Tomás José Gonzalez López, Burgos University Hospital, SpainReviewed by:
Deirdra Terrell, University of Oklahoma Health Sciences Center, United StatesRick Kapur, Sanquin Research, Netherlands
Copyright © 2023 Wu, Li, Mao, Zhu, Wang and Wen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chuan Wen, Y2h1YW53ZW5AY3N1LmVkdS5jbg==
†These authors have contributed equally to this work