
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 02 February 2023
Sec. Cytokines and Soluble Mediators in Immunity
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1115894
This article is part of the Research Topic Women in Cytokines and Soluble Mediators in Immunity View all 63 articles
 Sylvester Klöcker Grønbæk1*
Sylvester Klöcker Grønbæk1* Julie Høgh1Andreas Dehlbæk Knudsen1Michael Huy Cuong Pham2Per Ejlstrup Sigvardsen2Andreas Fuchs2Jørgen Tobias Kühl2Lars Køber2,3
Julie Høgh1Andreas Dehlbæk Knudsen1Michael Huy Cuong Pham2Per Ejlstrup Sigvardsen2Andreas Fuchs2Jørgen Tobias Kühl2Lars Køber2,3 Jan Gerstoft1,3
Jan Gerstoft1,3 Thomas Benfield4
Thomas Benfield4 Sisse Rye Ostrowski3,5Klaus Fuglsang Kofoed2,3,6
Sisse Rye Ostrowski3,5Klaus Fuglsang Kofoed2,3,6 Susanne Dam Nielsen1,3*
Susanne Dam Nielsen1,3*Introduction: People living with HIV (PLWH) are at twice the risk of developing cardiovascular diseases and have more than four times higher odds of aortic aneurysm (AA) than the uninfected population. However, biomarkers of AA in PLWH are yet to be discovered. We aimed to investigate whether circulating biomarkers reflecting platelet activation, hemostasis and endothelial disruption, i.e. sCD40L, D-dimer, syndecan-1, and thrombomodulin, were associated with AA in PLWH.
Methods: Five hundred seventy one PLWH from the Copenhagen Comorbidity in HIV Infection (COCOMO) study ≥40 years of age with an available contrast-enhanced CT scan as well as available biomarker analyses were included. The biomarkers were analyzed on thawed plasma. For each biomarker, we defined high level as a concentration in the upper quartile and low level as a concentration below the upper quartile. For D-dimer, the cut-off was defined as the lower limit of detection. Using unadjusted and adjusted logistic and linear regression models, we analyzed associations between AA and sCD40L, D-dimer, syndecan-1, and thrombomodulin, respectively in PLWH.
Results: PLWH had median (IQR) age 52 years (47-60), 88% were male, median (IQR) time since HIV diagnosis was 15 years (8-23), and 565 (99%) were currently on antiretroviral treatment. High level of sCD40L was associated with lower odds of AA in both unadjusted (odds ratio, OR, 0.23 (95% CI 0.07-0.77; P=0.017)) and adjusted models (adjusted OR, aOR, 0.23 (95% CI 0.07-0.78; P=0.019)). Detectable level of D-dimer was associated with higher odds of AA in both unadjusted (OR 2.76 (95% CI 1.34-5.67; P=0.006)) and adjusted models (aOR 2.22 (95% CI 1.02-4.85; P=0.045)).
Conclusions: SCD40L was associated with lower odds of AA whereas D-dimer was independently associated with higher odds of AA in PLWH. This calls for further investigations into specific biomarkers to aid early diagnosis of AA in PLWH.
As the median age of people living with HIV (PLWH) increases (1), so does the burden of age-related comorbidities (2). The risk of incident cardiovascular diseases (CVD) in PLWH is twice that of uninfected individuals (3), with myocardial infarction, stroke, and coronary artery disease being the most frequent manifestations (4). In a previous study by our group, HIV infection was associated with a 4.5 increased odds ratio (OR) of having aortic aneurysms (AA) compared to uninfected controls (5). AA is a rare but potentially severe manifestation of CVD, as the mortality rate of a ruptured abdominal AA may be as high as 80% (6). The European Society of Cardiology recommends screening of populations with a high risk of abdominal AA (7), because most AA are asymptomatic and diagnosed incidentally (8).
The initial phase of the pathogenesis of AA is not fully understood, but studies have suggested endothelial cell injury to contribute (9, 10). Associations have been found between AA, in the majority of studies in patients undergoing surgery for AA, and a marker of platelet activation, soluble CD40L (sCD40L) (11, 12), a marker of hemostasis, D-dimer (13–17), and the markers of endothelial disruption, syndecan-1 (18–20) and soluble thrombomodulin (21, 22), respectively. Importantly, all of these biomarkers have been reported to be elevated in PLWH compared to uninfected controls (23–28).
Possible associations between these biomarkers and AA have yet to be established but could aid in the early identification of high-risk patients. So far, no studies on the association between AA and markers of platelet activation, hemostasis, and endothelial disruption, respectively, in PLWH have been published. Thus, we investigated whether sCD40L, D-dimer, syndecan-1, and thrombomodulin (the biomarkers) are associated with AA in a large cohort of well-treated PLWH. We hypothesized that each of the biomarkers would be independently associated with AA in PLWH.
The Copenhagen Comorbidity in HIV Infection (COCOMO) study is a non-interventional cohort study that aims to assess non-AIDS comorbidities in PLWH. Inclusion criteria were age above 18 years and a positive HIV test. Between March 2015 and December 2016, 1099 PLWH living in the greater Copenhagen area were included. Procedures for recruitment and collection of data have previously been described elsewhere (29). A combined thoracic and abdominal contrast-enhanced computed tomography (CT) scan was offered to all COCOMO participants. In this study, we included COCOMO participants who were ≥40 years of age, had a contrast-enhanced CT performed, and had biomarkers measured in plasma.
Written informed consent was obtained from all participants. Ethical approval was obtained by the Regional Ethical Committee of Copenhagen (COCOMO: H-8-2014-004). The study was carried out in accordance with the Declaration of Helsinki.
A physical examination including measurement of blood pressure and anthropometrics was performed by trained clinical staff. Venous blood was collected non-fasting. Blood for plasma samples (EDTA anti-coagulated) was stored on ice until centrifugation in a cold centrifuge at 4˚C, and cryovials were transferred to liquid nitrogen within 72 hours (29). Extensive questionnaires included questions regarding medication, medical history, and smoking. From medical records, HIV-specific data such as transmission mode, duration of HIV infection, type of antiretroviral therapy, and hepatitis B and C status were obtained. Hepatitis B virus co-infection was defined as positive hepatitis B virus surface-antigen and hepatitis C virus co-infection as positive hepatitis C virus RNA. Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg and/or current use of antihypertensive medication according to Joint National Committee guidelines (30).
Contrast-enhanced thoracic and abdominal CT examinations including contrast-enhanced CT angiography were performed using a 320-detector CT scanner (Aquilion ONE, ViSION Edition, Canon Medical Systems, Otawara, Japan) at Rigshospitalet University Hospital, Copenhagen, Denmark.
Aortic analyses were performed by two trained examiners on contrast-enhanced CT images. Maximal and minimal inner aortic diameter was measured at seven anatomical points of the aorta, in four of which maximal outer diameter of the aorta was measured as well (5). According to the European Society of Cardiology guidelines, aortic aneurysms were defined as ≥50% increase in aortic diameter compared to the expected normal diameter or an infrarenal diameter of ≥30 mm (7). This resulted in the definition of AA as diameter of ascending aorta ≥45 mm and/or diameter of descending aorta ≥35 mm and/or diameter of suprarenal aorta ≥30 mm and/or diameter of the infrarenal aorta ≥30 mm (31).
Plasma concentrations of sCD40L, soluble syndecan-1, and thrombomodulin, were analyzed on thawed plasma using Luminex® Human Discovery Assays (R&D Systems, UK, Europe) in a 1:2 dilution, according to the manufacturer’s instructions, at the Department of Clinical Immunology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark. Plasma concentrations of D-dimer were measured as routine biochemistry on fresh blood samples at Department of Clinical Biochemistry, Copenhagen University Hospital, Herlev, Copenhagen, Denmark (29).
Continuous data were reported using means and standard deviations for normal deviates and medians with interquartile ranges for variables not normally distributed, as appropriate. For categorical data, frequency counts and percentages of subjects within each category were reported. Logistic regression analyses were applied where the dependent variable was binary and linear regression where the dependent variable was continuous.
As the primary outcome, we investigated the association between AA and high levels of sCD40L, syndecan-1, and thrombomodulin and detectable level of D-dimer one at a time using simple and multivariable logistic regression. For each biomarker, we created a dichotomous variable defining high level of the biomarker as a concentration in the upper quartile and low level as a concentration below the upper quartile. We used the third quartile as cut-off in the dichotomous variables for sCD40L, syndecan-1 and thrombomodulin to make the effect estimates more easily interpretable. For D-dimer, the cut-off was defined as the lower limit of detection (290 ng/mL (Fibrin Equivalent Units, FEU)), creating a dichotomous variable with detectable versus undetectable as most of the measurements were below the lower limit of detection. We created two predefined models; model 1 adjusted for age (per decade) and sex and model 2 adjusted for traditional risk factors that were significant in previous analyses on AA in PLWH (5) (age, sex, BMI category, hypertension, and smoking (current/previous/never)). Furthermore, in sensitivity analyses, we investigated the associations between AA, sCD40L, and (one at a time) use of aspirin, use of statins, weekly alcohol intake, and hypertension. As a sensitivity analysis, we included all four biomarkers into a single analysis with AA.
Additionally, continuous variables were used in pre-specified, secondary analyses to make sure any linear associations between exposure and outcome would not be overlooked. We adjusted for the same predefined models 1 and 2. Moreover, in sensitivity analyses, we investigated associations between aortic diameter (maximum outer diameter of ascending, descending, suprarenal, and infrarenal aorta) and high versus low levels of the biomarkers. Lastly, in sensitivity analyses, we examined associations between aortic wall thickness (maximal outer minus maximal inner diameter of ascending, descending, suprarenal, and infrarenal aorta) and high versus low levels of the biomarkers.
P-values <0.05 were considered statistically significant, and all P-values were two-sided. R (version 4.1.0 (2021-05-18)) was used for all statistical analyses (32).
We included 571 participants aged 40 years or older with available contrast-enhanced CT and biomarker measurements. As reported previously, 43 aneurysms were found in 39 PLWH (6.8%). The median (IQR) age of PLWH was 52 years (47-60) and 88% were male (Table 1). The median (IQR) time since HIV diagnosis was 15 years (8-23) and 565 (99%) were currently on antiretroviral therapy (Table 1). Participant characteristics, HIV-specific variables, and biomarkers are listed in Table 1.
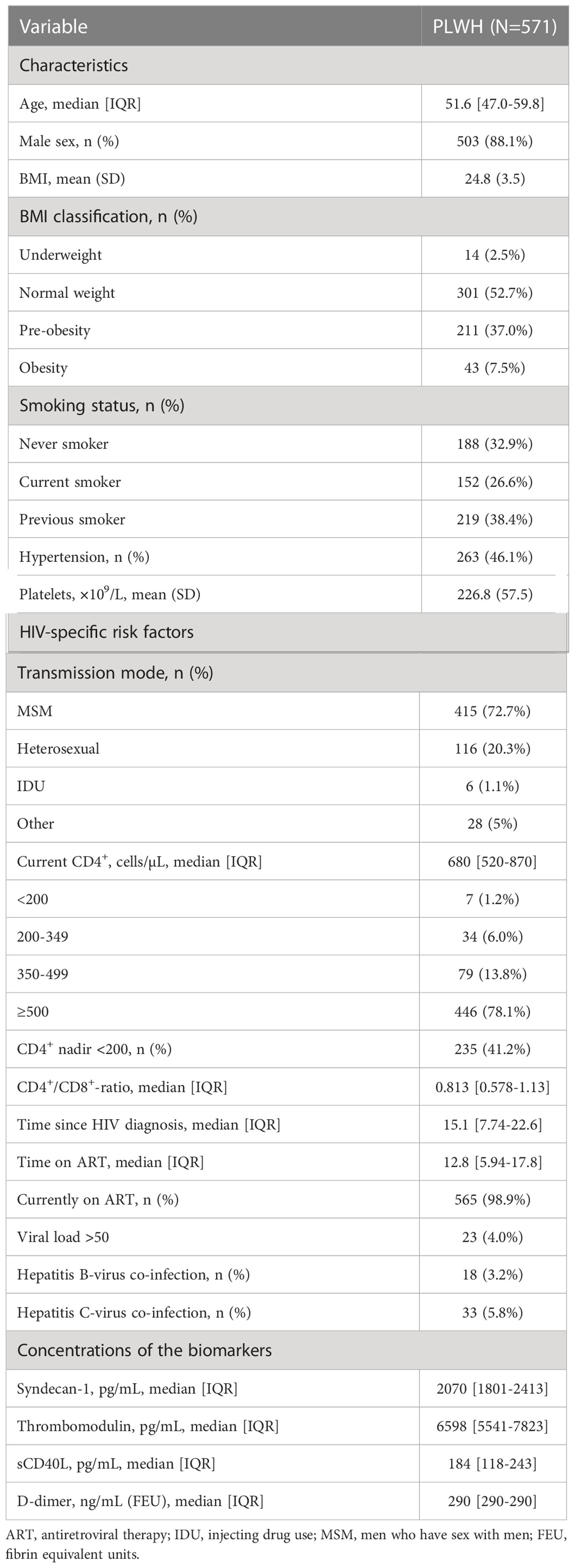
Table 1 Participant characteristics, HIV-specific risk factors, and concentrations of the biomarkers.
We found high levels of sCD40L to be associated with lower odds of AA; univariably with OR 0.23 (95% CI 0.07-0.77; P=0.017) and adjusted odds ratio, aOR, 0.23 (95% CI 0.07-0.78; P=0.019) adjusted in model 2 (Table 2). In a sensitivity analysis, further adjustment of model 2 for use of aspirin did not significantly alter the association between high level of sCD40L and AA (aOR 0.25 (95% CI 0.07-0.87); P=0.029). In other sensitivity analyses, use of statins, weekly alcohol intake, and hypertension were not associated with AA and sCD40L.
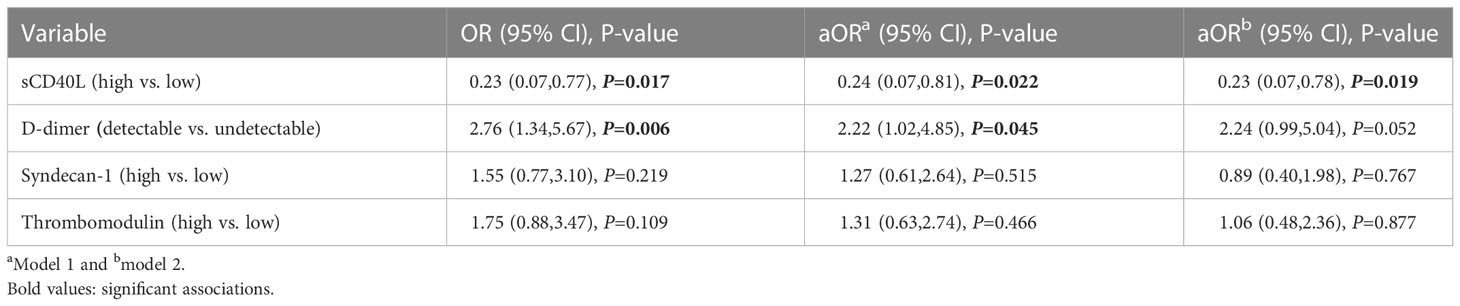
Table 2 Associations between AA and high levels of the biomarkers.
Detectable level of D-dimer was associated with higher odds of AA, both univariably (OR 2.76 (95% CI 1.34-5.67; P=0.006)) and adjusted in model 1 (aOR 2.22 (95% CI 1.02-4.85; P=0.045)). Adjusting for traditional risk factors in model 2 did not change the parameter estimate, (aOR 2.24 (95% CI 0.99-5.04; P=0.052). There were aortic aneurysms among PLWH with undetectable D-dimer.
Syndecan-1 and thrombomodulin were not associated with AA (Table 2).
Including all four biomarkers into a single analysis did not significantly alter the associations compared to the individual associations between the biomarkers and AA.
In exploratory analyses with the biomarkers as continuous variables, a doubling in sCD40L concentration was associated with lower odds of AA; univariably with OR 0.81 (95% CI 0.66,0.98; P=0.028) and aOR 0.76 (95% CI 0.62-0.95; P=0.014) adjusted in model 2. A twofold increase in D-dimer concentration was associated with higher odds of AA; univariably with OR 1.51 (95% CI 1.22-1.86; P<0.001) and aOR 1.41 (95% CI 1.08-1.84; P=0.010) adjusted in model 2. Syndecan-1 was not significantly associated with AA. A twofold increase in thrombomodulin concentration was univariably associated with higher odds of AA (OR 1.82 (95% CI 1.02-3.26; P=0.043) but not in adjusted models (Table 3). Analyses of high versus low levels and with continuous variables are shown in Figure 1.
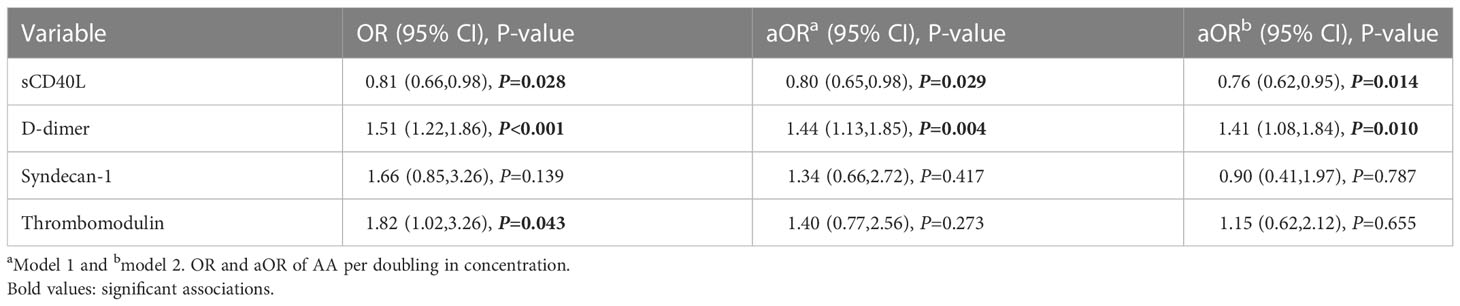
Table 3 Associations between AA and the biomarkers as continuous variables.

Figure 1 Primary (high vs. low variable) and exploratory (continuous variable, aOR associated with doubling of biomarker) analyses of the association between AA and the biomarkers in PLWH adjusted for age, sex, hypertension, smoking status, and BMI category.
The mean (SD) aortic diameters are presented in Figure 2 and Table 4. Diameter in ascending aorta 34.54 mm (4.30); in descending aorta 26.36 mm (2.70); in suprarenal aorta 24.97 mm (2.82); and in infrarenal aorta 21.65 mm (3.17). In sensitivity analyses, high level of sCD40L was associated with smaller suprarenal aortic diameter (0.46 mm (95% CI 0.01-0.91; P=0.045)) adjusted in model 2 but not univariably (0.40 mm (95% CI 0.14-0.93; P=0.144)). Detectable level of D-dimer was associated with larger infrarenal aortic diameter; univariably 1.11 mm (95% CI 0.38-1.84; P=0.003) and 0.97 mm (95% CI 0.30-1.63; P=0.004) adjusted in model 2. High level of syndecan-1 was univariably associated with larger diameter of the ascending aorta (1.04 mm (95% CI 0.23-1.85; P=0.012)) and with larger infrarenal aortic diameter (0.95 mm (95% CI 0.36-1.55; P=0.002)). High level of thrombomodulin was associated with larger infrarenal aortic diameter; univariably 1.41 mm (95% CI 0.82-2.00; P<0.0001) and 0.89 mm (95% CI 0.38-1.41; P<0.001) adjusted in model 2. Furthermore, high level of thrombomodulin was univariably associated with larger diameter of the ascending aorta (1.12 mm (95% CI 0.30-1.92; P=0.007)) and with larger suprarenal aortic diameter (0.68 mm (95% CI 0.14-1.21; P=0.024)) (Table 4 and Figure 2).
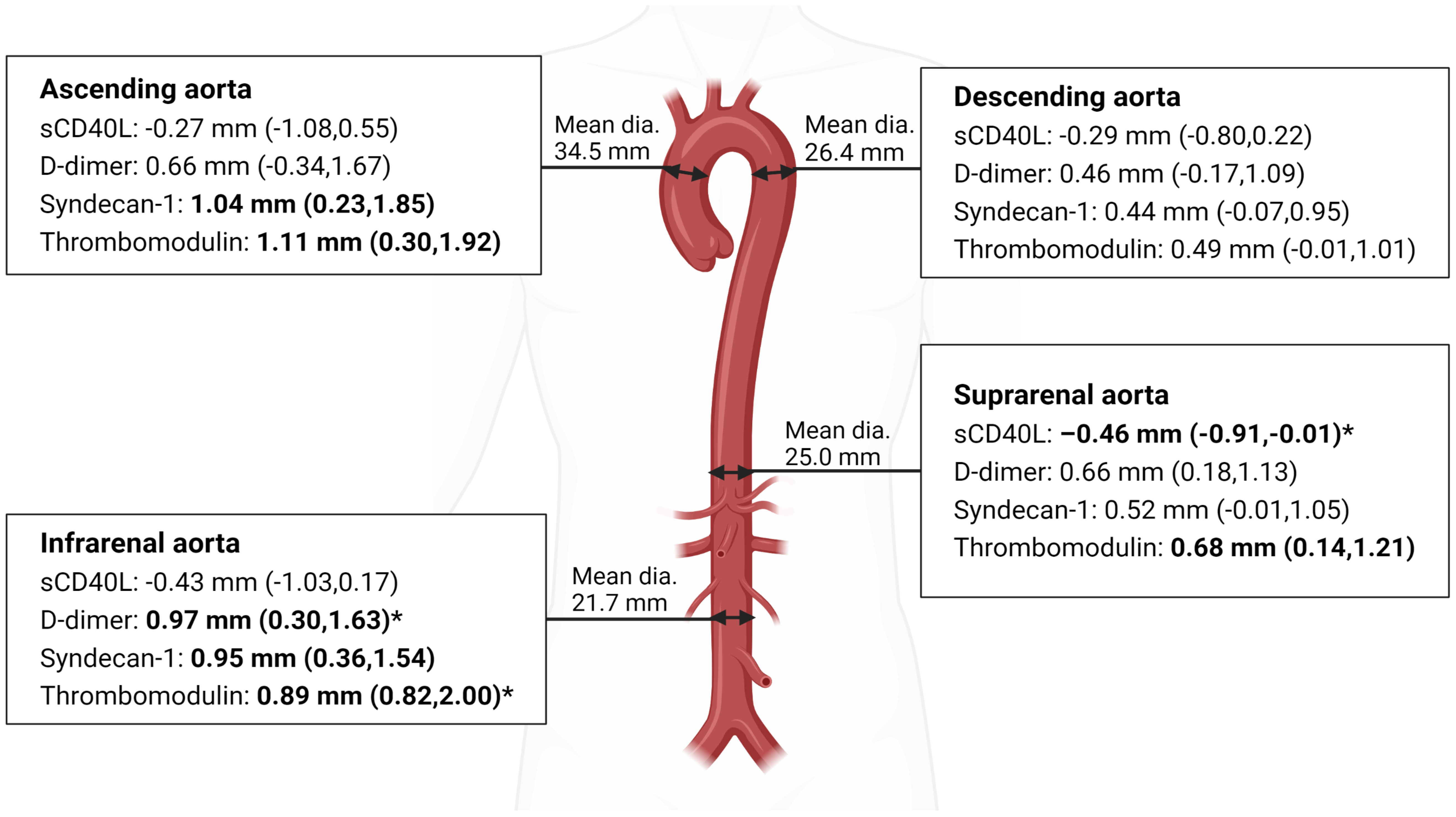
Figure 2 Aortic diameter measured as maximum outer diameter. Mean diameter and larger or smaller diameter in mm (95% CI) associated with high level of the biomarker. Bold text: significant associations. *Adjusted for age, sex, hypertension, smoking status, and BMI category. (Made with biorender.com).
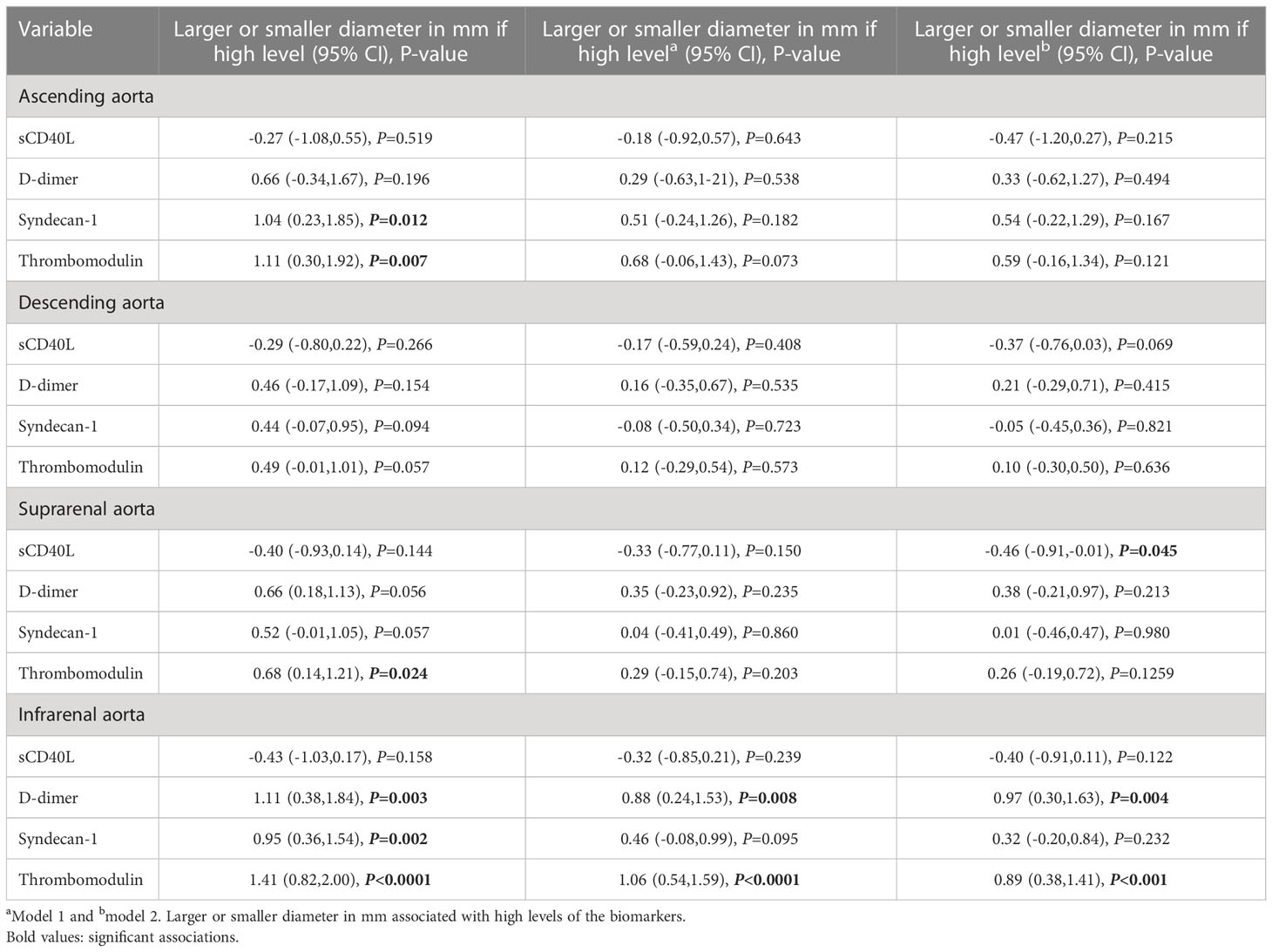
Table 4 Associations between aortic diameter and the biomarkers.
The mean (SD) aortic wall thickness was: in ascending aorta 2.28 mm (0.59); in descending aorta 2.32 mm (0.60); in suprarenal aorta 2.22 mm (0.76); and in infrarenal aorta 2.09 mm (0.81). In sensitivity analyses, high level of sCD40L was not associated with aortic wall thickness. Detectable level of D-dimer was associated with greater infrarenal aortic wall thickness; univariably 0.46 mm (95% CI 0.36-0.56; P<0.001) and 0.41 mm (95% CI 0.30-0.51; P<0.001) adjusted in model 2. High level of syndecan-1 was univariably associated with greater infrarenal aortic wall thickness (0.16 mm (95% CI 0.01-0.31; P<0.040)). High level of thrombomodulin was associated with greater infrarenal aortic wall thickness; univariably 0.27 mm (95% CI 0.12-0.42; P<0.001) and 0.18 mm (95% CI 0.03-0.33; P=0.018) adjusted in model 2.
In a large cohort of well-treated PLWH, we found high level of sCD40L to be associated with lower odds of AA and D-dimer above 290 ng/mL (FEU) to be associated with higher odds of AA. The same associations were found in analyses with biomarkers treated as continuous analyses.
The primary source of sCD40L is activated platelets (33). A study reported decreased platelet counts in HIV-negative AA patients compared to controls (34), and it is possible that lower platelet count in the PLWH with AA may contribute to the inverse association between AA and sCD40L, since platelets are critical for vascular endothelial integrity and health (35). Other studies have reported aspirin to suppress (36) or block (37) the release of sCD40L from platelets. Furthermore, hypertension is associated with higher concentration of sCD40L (26), statins reduce sCD40L in CVD patients (38, 39), and alcohol is proposed to partially activate platelets (40) resulting in decreased sCD40L production. However, our analyses showed no such associations, so this cannot explain the contrast to previous reports of sCD40L being increased in plasma from HIV-negative patients with abdominal AA compared to matched controls (11) and the lacking finding of associations between sCD40L and AA (41).
In line with the emerging focus on the role of endothelial cells in AA pathogenesis (9, 10), we hypothesized that the biomarkers may be involved in the pathogenesis prior to the aortic diameter exceeding the aneurysmal limit. Therefore, we performed sensitivity analyses regarding associations between aortic diameter and the biomarkers. We found sCD40L to be negatively associated with suprarenal aortic diameter, while, at present, studies regarding associations between aortic diameter and sCD40L have not been published. Another measurement of interest is the aortic wall thickness, which studies have suggested the incorporation of into the risk analysis of AA (42, 43). Therefore, we investigated associations between wall thickness and the biomarkers but found no association with sCD40L.
D-dimer, an important marker of hemostasis, has been reported elevated in HIV-negative patients with abdominal AA compared to controls without abdominal AA (13–17). Furthermore, a study reported D-dimer to be 49% higher in PLWH on ART aged 45-76 years than in population controls (adjusted percent difference) (27). In line with these findings, our results highlight D-dimer as a possible biomarker, not only associated with abdominal AA, but all AA in PLWH. However, adjusting for known risk factors resulted in an only borderline significant parameter estimate, perhaps caused by an insufficient sample size, as plasma from 83 patients lacked measurement of D-dimer. The reported association between D-dimer and larger infrarenal aortic diameter is consistent with a previous study (44) and suggests a possible role of D-dimer as an indicator of larger infrarenal aortic diameter. Additionally, the reported associations between D-dimer and greater infrarenal aortic wall thickness may indicate increased fibrinolytic activity in the infrarenal aorta. However, as D-dimer is a general marker of fibrinolysis and not disease-specific, combination with other biomarkers may increase the specificity.
A previous study reported concentrations of syndecan-1, a key constituent of the endothelial glycocalyx and a regulator of inflammation, to be elevated in aortic tissue, though not in plasma, from patients with ascending AA compared to matched controls (18). Additionally, a study reported elevated syndecan-1 in PLWH compared to uninfected controls (23). Syndecan-1 is a key constituent of glycocalyx on most endothelial cells in the body, and its soluble form is generated by shedding from the endothelial glycocalyx indicative of damage to endothelial cells (45). As suggested by a previous study (18), it is possible that increased local shedding of syndecan-1 from the aneurysm is masked by the total pool of the biomarker, resulting in non-significant associations with AA in this study. Furthermore, since we only measured syndecan-1 in plasma and not aortic tissue, this may altogether explain why we do not reproduce the previously found association. Syndecan-1 being univariably associated with larger diameter in ascending and infrarenal aorta suggests an association between larger aortic diameter and endothelial disruption.
Another biomarker shed from endothelial cells indicating endothelial cell injury (46), is soluble thrombomodulin, which has been reported elevated in serum from HIV-negative patients with abdominal AA compared to healthy controls (21, 22). Moreover, several studies have reported thrombomodulin to be elevated in PLWH compared to uninfected controls (24, 25). We found thrombomodulin to be univariably associated with AA when kept as a continuous variable, but not when used as a dichotomous variable. However, this finding was not significant when adjusted for known risk factors in our predefined models and we considered it to be an incidental finding. A potential reason why we found no independent association between thrombomodulin and AA in PLWH is the above-mentioned possible masking of shedding from the aneurysm by the shedding from all endothelial cells. The reported association between thrombomodulin and larger infrarenal aortic diameter suggests thrombomodulin as a possible marker of aortic diameter, though at present, no studies regarding this association have been published. Moreover, as with syndecan-1, the association between thrombomodulin and greater infrarenal aortic diameter indicates an association between larger aortic diameter and endothelial disruption. However, further studies into these associations are required.
The patients in the majority of the previous studies were undergoing surgery for AA, meaning that the diameters of the aneurysms were larger than those in our study, in which the vast majority of aneurysms had diameters below the surgical threshold. A study reported the size of abdominal AA to be associated with concentration of D-dimer (47), while another study suggested endothelin-1 (ET-1), which is released from endothelial cells in response to among other factors vascular injury, as a marker of aneurysm diameter (48). Though such associations have not presently been reported regarding the other biomarkers, it is possible that the smaller diameters of the aneurysms in our study precluded the use of these biomarker concentrations to identify AA, and may, thus, partly explain the negative inverse association between sCD40L and AA and the lack of associations between AA and high levels of syndecan-1 and thrombomodulin, respectively.
A limitation of this study is its cross-sectional design, making it difficult to investigate causal relationships between the biomarkers and AA. Moreover, the cohort is predominantly male and in fact, all AA were found in men. Strengths include a large cohort of well-treated PLWH and the opportunity to adjust for known risk factors for AA. Lastly, the prevalence of AA is high, making it possible to investigate associations with AA.
In conclusion, in this large cohort of well-treated PLWH, we found high sCD40L to be associated with lower odds of AA, and we confirmed previous findings of the association between high D-dimer and higher odds of AA. Furthermore, thrombomodulin and D-dimer were associated with larger aortic diameter and sCD40L with smaller aortic diameter. These findings regarding sCD40L and AA call for further investigation into its utilization as a biomarker of AA in PLWH. D-dimer holds promise as a possible marker, though not specific of AA, why further examinations of specific biomarkers remain necessary to aid in the early diagnosis of AA in PLWH.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Regional Ethical Committee of Copenhagen. The patients/participants provided their written informed consent to participate in this study.
Design of the COCOMO study was carried out by SN et.al (29). and data collection was performed by the COCOMO-team from the Viro-Immunology Research Group. SO contributed to the Luminex® analysis and interpretation of the analysed biomarkers. Statistical analysis plan and design of this sub study was written by SG under supervision by SN and JH. Statistical analyses, interpretation of data, and writing of the manuscript was performed by SKG under supervision by SN, JH and AK. Review of the manuscript was performed by MP, PS, AF, JK, LK, JG, TB, SO, and KK. All authors contributed to the article and approved the submitted version.
This work was supported by Rigshospitalet Research Council, Region Hovedstaden, Novo Nordisk Foundation, Augustinus Foundation, Gilead Sciences and Lundbeck Foundation. The study was designed, conducted, analyzed, and written by the authors without involvement of any commercial party.
We acknowledge the contribution from all patients enrolled in the COCOMO study and the work of the COCOMO-team.
SG has received a grant from Rigshospitalet Research Council; AK has received a grant from The Danish Heart Foundation and a grant from the European Commission EU 7th Framework Grant ID no. 603266; LK has received speakers honorarium form AstraZeneca, Bayer, Boehringer, Novartis and Novo; TB reports grants from Novo Nordisk Foundation, Lundbeck Foundation, Simonsen Foundation, GSK, Pfizer, Gilead, Kai Hansen Foundation and Erik and Susanna Olesen’s Charitable Fund, personal fees from GSK, Pfizer, Boehringer Ingelheim, Gilead, MSD, Pentabase ApS, Becton Dickinson, Janssen and Astra Zeneca all outside the submitted work; SN has received unrestricted research grants from Novo Nordisk Foundation, Lundbeck Foundation, Augustinus Foundation, Rigshospitalet Research Council and advisory board activity for Gilead and GSK/ViiV. All unrelated to this manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
PLWH, People living with HIV; CVD, Cardiovascular diseases; AA, Aortic aneurysms; sCD40L, Soluble CD40 ligand; FEU, Fibrin Equivalent Units; ET-1, Endothelin-1; OR, Odds ratio; aOR, Adjusted odds ratio; CI, Confidence interval; SD, Standard deviation.
1. Smit M, Brinkman K, Geerlings S, Smit C, Thyagarajan K, van Sighem AV, et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect Dis (2015) 15(7):810–8. doi: 10.1016/S1473-3099(15)00056-0
2. Gebo KA. Epidemiology of HIV and response to antiretroviral therapy in the middle aged and elderly. Aging Health (2008) 4(6):615. doi: 10.2217/1745509X.4.6.615
3. Shah ASV, Stelzle D, Ken Lee K, Beck EJ, Alam S, Clifford S, et al. Global burden of atherosclerotic cardiovascular disease in people living with HIV: Systematic review and meta-analysis. Circulation (2018) 138(11):1100–12. doi: 10.1161/CIRCULATIONAHA.117.033369
4. Neuhaus J, Angus B, Kowalska JD, La Rosa A, Sampson J, Wentworth D, et al. Risk of all-cause mortality associated with non-fatal AIDS and serious non-AIDS events among adults infected with HIV. AIDS (2010) 24(5):697. doi: 10.1097/QAD.0b013e3283365356
5. Høgh J, Pham MHC, Knudsen AD, Thudium RF, Gelpi M, Sigvardsen PE, et al. HIV Infection is associated with thoracic and abdominal aortic aneurysms: a prospective matched cohort study. Eur Heart J (2021) 42(30):2924–31. doi: 10.1093/eurheartj/ehab348
6. Kent KC. Clinical practice. abdominal aortic aneurysms. N Engl J Med (2014) 371(22):2101–8. doi: 10.1056/NEJMcp1401430
7. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J (2014) 35(41):2873–926. doi: 10.1093/eurheartj/ehu281
8. Mathur A, Mohan V, Ameta D, Gaurav B, Haranahalli P. Aortic aneurysm. J Transl Intern Med (2016) 4(1):35–41. doi: 10.1515/jtim-2016-0008
9. Franck G, Dai J, Fifre A, Ngo S, Justine C, Michineau S, et al. Reestablishment of the endothelial lining by endothelial cell therapy stabilizes experimental abdominal aortic aneurysms. Circulation (2013) 127(18):1877–87. doi: 10.1161/CIRCULATIONAHA.113.001677
10. Siasos G, Mourouzis K, Oikonomou E, Tsalamandris S, Tsigkou V, Vlasis K, et al. The role of endothelial dysfunction in aortic aneurysms. Curr Pharm Des (2015) 21(28):4016–34. doi: 10.2174/1381612821666150826094156
11. Touat Z, Ollivier V, Dai J, Huisse MG, Bezeaud A, Sebbag U, et al. Renewal of mural thrombus releases plasma markers and is involved in aortic abdominal aneurysm evolution. Am J Pathol (2006) 168(3):1022–30. doi: 10.2353/ajpath.2006.050868
12. Kusters PJH, Seijkens TTP, Beckers L, Lievens D, Winkels H, De Waard V, et al. CD40L deficiency protects against aneurysm formation. Arterioscler Thromb Vasc Biol (2018) 38:1076–85. doi: 10.1161/ATVBAHA.117.310640
13. Golledge J, Tsao PS, Dalman RL, Norman PE. Circulating markers of abdominal aortic aneurysm presence and progression. Circulation (2008) 118(23):2382–92. doi: 10.1161/CIRCULATIONAHA.108.802074
14. Sidloff DA, Stather PW, Choke E, Bown MJ, Sayers RD. A systematic review and meta-analysis of the association between markers of hemostasis and abdominal aortic aneurysm presence and size. J Vasc Surg (2014) 59(2):528–35. doi: 10.1016/j.jvs.2013.10.088
15. Golledge J, Muller R, Clancy P, McCann M, Norman PE. Evaluation of the diagnostic and prognostic value of plasma d-dimer for abdominal aortic aneurysm. Eur Heart J (2011) 32(3):354–64. doi: 10.1093/eurheartj/ehq171
16. Takagi H, Manabe H, Kawai N, Goto S, Umemoto T. Plasma fibrinogen and d-dimer concentrations are associated with the presence of abdominal aortic aneurysm: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg (2009) 38(3):273–7. doi: 10.1016/j.ejvs.2009.05.013
17. Vega De Ceniga M, Esteban M, Barba A, Estallo L, Blanco-Colio LM, Martin-Ventura JL. Assessment of biomarkers and predictive model for short-term prospective abdominal aortic aneurysm growth-a pilot study. Ann Vasc Surg (2014) 28(7):1642–8. doi: 10.1016/j.avsg.2014.02.025
18. Ntika S, Tracy LM, Franco-Cereceda A, Björck HM, Krizhanovskii C. Syndecan-1 expression is increased in the aortic wall of patients with type 2 diabetes but is unrelated to elevated fasting plasma glucagon-like peptide-1. Biomedicines (2021) 9(6):697. doi: 10.3390/biomedicines9060697
19. Wen J, Wang P, Smith SV, Haller CA, Chaikof EL. Syndecans are differentially expressed during the course of aortic aneurysm formation. J Vasc Surg (2007) 46(5):1014–25. doi: 10.1016/j.jvs.2007.06.022
20. Xiao J, Angsana J, Wen J, Smith SV, Park PW, Ford ML, et al. Syndecan-1 displays a protective role in aortic aneurysm formation by modulating T cell-mediated responses. Arterioscler Thromb Vasc Biol (2012) 32(2):386–96. doi: 10.1161/ATVBAHA.111.242198
21. Budzyń M, Gryszczyńska B, Majewski W, Krasiński Z, Kasprzak MP, Formanowicz D, et al. The association of serum thrombomodulin with endothelial injuring factors in abdominal aortic aneurysm. BioMed Res Int (2017) 2017:2791082. doi: 10.1155/2017/2791082
22. Brunelli T, Prisco D, Fedi S, Rogolino A, Farsi A, Marcucci R, et al. High prevalence of mild hyperhomocysteinemia in patients with abdominal aortic aneurysm. J Vasc Surg (2000) 32(3):531–6. doi: 10.1067/mva.2000.107563
23. Meneses GC, Cavalcante MG, Da Silva Junior GB, Martins AMC, Da Justa Pires Neto R, Libório AB, et al. Endothelial glycocalyx damage and renal dysfunction in HIV patients receiving combined antiretroviral therapy. AIDS Res Hum Retroviruses (2017) 33(7):703–10. doi: 10.1089/aid.2016.0284
24. Leucker TM, Weiss RG, Schär M, Bonanno G, Mathews L, Jones SR, et al. Coronary endothelial dysfunction is associated with elevated serum PCSK9 levels in people with HIV independent of low-density lipoprotein cholesterol. J Am Heart Assoc (2018) 7(19):e009996. doi: 10.1161/JAHA.118.009996
25. De Larrañaga GF, Bocassi AR, Puga LM, Alonso BS, Benetucci JA. Endothelial markers and HIV infection in the era of highly active antiretroviral treatment. Thromb Res (2003) 110(2–3):93–8. doi: 10.1016/S0049-3848(03)00291-3
26. Falasca K, Reale M, Di Nicola M, Ucciferri C, Zecca IA, Santilli F, et al. Circulating CD40 ligand, dickkopf-1 and p-selectin in HIV-infected patients. HIV Med (2019) 20(10):681–90. doi: 10.1111/hiv.12789
27. Neuhaus J, Jacobs DR, Baker JV, Calmy A, Duprez D, La Rosa A, et al. Markers of inflammation, coagulation and renal function are elevated in adults with HIV infection. J Infect Dis (2010) 201(12):1788. doi: 10.1086/652749
28. Haugaard AK, Lund TT, Birch C, Rönsholt F, Trøseid M, Ullum H, et al. Discrepant coagulation profile in HIV infection: elevated d-dimer but impaired platelet aggregation and clot initiation. AIDS (2013) 27(17):2749–58. doi: 10.1097/01.aids.0000432462.21723.ed
29. Ronit A, Haissman J, Kirkegaard-Klitbo DM, Kristensen TS, Lebech AM. Benfield T, et al. Copenhagen comorbidity in HIV infection (COCOMO) study: a study protocol for a longitudinal, non-interventional assessment of non-AIDS comorbidity in HIV infection in Denmark. BMC Infect Dis (2016) 16(1):713. doi: 10.1186/s12879-016-2026-9
30. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA (2014) 311(5):507–20. doi: 10.1001/jama.2013.284427
31. Lindholt JS, Rasmussen LM, Søgaard R, Lambrechtsen J, Steffensen FH, Frost L, et al. Baseline findings of the population-based, randomized, multifaceted Danish cardiovascular screening trial (DANCAVAS) of men aged 65-74 years. Br J Surg (2019) 106(7):862–71. doi: 10.1002/bjs.11135
33. Aloui C, Prigent A, Sut C, Tariket S, Hamzeh-Cognasse H, Pozzetto B, et al. The signaling role of cd40 ligand in platelet biology and in platelet component transfusion. Int J Mol Sci (2014) 15(12):22342–64. doi: 10.3390/ijms151222342
34. Milne AA, Adam DJ, Murphy WG, Ruckley CV. Effects of asymptomatic abdominal aortic aneurysm on the soluble coagulation system, platelet count and platelet activation. Eur J Vasc Endovasc Surg (1999) 17(5):434–7. doi: 10.1053/ejvs.1998.0790
35. Nachman RL, Rafii S. Platelets, petechiae, and preservation of the vascular wall. N Engl J Med (2008) 359(12):1261. doi: 10.1056/NEJMra0800887
36. Enomoto Y, Adachi S, Matsushima-Nishiwaki R, Doi T, Niwa M, Akamatsu S, et al. Thromboxane A(2) promotes soluble CD40 ligand release from human platelets. Atherosclerosis. (2010) 209(2):415–21. doi: 10.1016/j.atherosclerosis.2009.10.024
37. Nannizzi-Alaimo L, Alves VL, Phillips DR. Inhibitory effects of glycoprotein IIb/IIIa antagonists and aspirin on the release of soluble CD40 ligand during platelet stimulation. Circulation (2003) 107(8):1123–8. doi: 10.1161/01.CIR.0000053559.46158.AD
38. Li J, Zhao SP, Peng DQ, Xu ZM, Zhou H. Early effect of pravastatin on serum soluble CD40L, matrix metalloproteinase-9, and c-reactive protein in patients with acute myocardial infarction. Clin Chem (2004) 50(9):1696–9. doi: 10.1373/clinchem.2003.030940
39. Schönbeck U, Gerdes N, Varo N, Reynolds RS, Horton DB, Bavendiek U, et al. Oxidized low-density lipoprotein augments and 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitors limit CD40 and CD40L expression in human vascular cells. Circulation (2002) 106(23):2888–93. doi: 10.1161/01.CIR.0000043029.52803.7B
40. Salem RO, Laposata M. Effects of alcohol on hemostasis. Am J Clin Pathol (2005) 123(Suppl 1):S96–105. doi: 10.1309/113N8EUFXYUECCNA
41. Flondell-Sité D, Lindblad B, Kölbel T, Gottsäter A. Cytokines and systemic biomarkers are related to the size of abdominal aortic aneurysms. Cytokine (2009) 46:211–5. doi: 10.1016/j.cyto.2009.01.007
42. Shang EK, Nathan DP, Woo EY, Fairman RM, Wang GJ, Gorman RC, et al. Local wall thickness in finite element models improves prediction of abdominal aortic aneurysm growth. J Vasc Surg (2015) 61(1):217–23. doi: 10.1016/j.jvs.2013.08.032
43. Shang EK, Nathan DP, Sprinkle SR, Fairman RM, Bavaria JE, Gorman RC, et al. Impact of wall thickness and saccular geometry on the computational wall stress of descending thoracic aortic aneurysms. Circulation (2013) 128(11 Suppl 1):S157–62. doi: 10.1161/CIRCULATIONAHA.112.000200
44. Laughlin GA, Allison MA, Jensky NE, Aboyans V, Wong ND, Detrano R, et al. Abdominal aortic diameter and vascular atherosclerosis: the multi-ethnic study of atherosclerosis. Eur J Vasc Endovasc Surg (2011) 41(4):481–7. doi: 10.1016/j.ejvs.2010.12.015
45. Bartlett AH, Hayashida K, Park PW. Molecular and cellular mechanisms of syndecans in tissue injury and inflammation. Mol Cells (2007) 24(2):153–66.
46. Martin FA, Murphy RP, Cummins PM. Thrombomodulin and the vascular endothelium: insights into functional, regulatory, and therapeutic aspects. Am J Physiol Heart Circ Physiol (2013) 304(12):H1585–97. doi: 10.1152/ajpheart.00096.2013
47. Yamazumi K, Ojiro M, Okumura H, Aikou T. An activated state of blood coagulation and fibrinolysis in patients with abdominal aortic aneurysm. Am J Surg (1998) 175(4):297–301. doi: 10.1016/S0002-9610(98)00014-2
Keywords: HIV, PLWH, aortic aneurysm, sCD40L, D-dimer (DD), syndecan-1, thrombomodulin (TM)
Citation: Grønbæk SK, Høgh J, Knudsen AD, Pham MHC, Sigvardsen PE, Fuchs A, Kühl JT, Køber L, Gerstoft J, Benfield T, Ostrowski SR, Kofoed KF and Nielsen SD (2023) Aortic aneurysms and markers of platelet activation, hemostasis, and endothelial disruption in people living with HIV. Front. Immunol. 14:1115894. doi: 10.3389/fimmu.2023.1115894
Received: 04 December 2022; Accepted: 23 January 2023;
Published: 02 February 2023.
Edited by:
Diana Boraschi, Shenzhen Institute of Advanced Technology (SIAT) (CAS), ChinaCopyright © 2023 Grønbæk, Høgh, Knudsen, Pham, Sigvardsen, Fuchs, Kühl, Køber, Gerstoft, Benfield, Ostrowski, Kofoed and Nielsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne Dam Nielsen, c3VzYW5uZS5kYW0ucG91bHNlbkByZWdpb25oLmRr; Sylvester Klöcker Grønbæk, c3lsdmVzdGVyLmtsb2Vja2VyLmdyb2VuYmFla0ByZWdpb25oLmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.