
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 16 March 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1107438
 Georg Christian Lodde1†
Georg Christian Lodde1† Frederik Krefting1†
Frederik Krefting1† Jan-Malte Placke1Lea Schneider1Melanie Fiedler2Ulf Dittmer2
Jan-Malte Placke1Lea Schneider1Melanie Fiedler2Ulf Dittmer2 Jürgen Christian Becker1,3,4Stefanie Hölsken5
Jürgen Christian Becker1,3,4Stefanie Hölsken5 Dirk Schadendorf1,4
Dirk Schadendorf1,4 Selma Ugurel1,4†Wiebke Sondermann1*†
Selma Ugurel1,4†Wiebke Sondermann1*†Background: The rate of seroconversion after COVID-19 vaccination in patients with moderate to severe psoriasis requiring systemic treatment is poorly understood.
Objectives: The aim of this prospective single-center cohort study performed between May 2020 and October 2021 was to determine the rate of seroconversion after COVID-19 vaccination in patients under active systemic treatment for moderate to severe psoriasis.
Methods: Inclusion criteria were systemic treatment for moderate to severe psoriasis, known COVID-19 vaccination status, and repetitive anti-SARS-CoV-2-S IgG serum quantification. The primary outcome was the rate of anti-SARS-CoV-2-S IgG seroconversion after complete COVID-19 vaccination.
Results: 77 patients with a median age of 55.9 years undergoing systemic treatment for moderate to severe psoriasis were included. The majority of patients received interleukin- (n=50, 64.9%) or tumor necrosis factor (TNF)-α inhibitors (n=16, 20.8%) as systemic treatment for psoriasis; nine patients (11.7%) were treated with methotrexate (MTX) monotherapy, and one patient each received dimethyl fumarate (1.3%), respectively apremilast (1.3%). All included patients completed COVID-19 vaccination with two doses over the course of the study. Serum testing revealed that 74 patients (96.1%) showed an anti-SARS-CoV-2-S IgG seroconversion. While all patients on IL-17A, -12 or -12/23 inhibitors (n=50) achieved seroconversion, three of 16 patients (18.8%) receiving MTX and/or a TNF-α inhibitor as main anti-psoriatic treatment did not. At follow-up, none of the patients had developed symptomatic COVID-19 or died from COVID-19.
Conclusions: Anti-SARS-CoV-2-S IgG seroconversion rates following COVID-19 vaccination in psoriasis patients under systemic treatment were high. An impaired serological response, however, was observed in patients receiving MTX and/or TNF-α inhibitors, in particular infliximab.
Psoriasis is a chronic inflammatory disease occurring worldwide which leads to typical erythematosquamous skin plaques and affects about 2-3% of the total Western population (1, 2). Already since the 1990s, there has been increasing scientific evidence that psoriasis is a systemic inflammatory disease associated with various comorbidities (3–5). Multiple epidemiological studies have shown an increased prevalence of cardiovascular risk factors, increased prevalence of arterial hypertension (6–11), and cardiovascular diseases like myocardial infarction (12–15) in psoriasis. In addition, a large body of evidence revealed that psoriasis is associated with obesity (7, 16–19), insulin resistance (20) and diabetes mellitus (6, 7, 11, 21, 22). Accordingly, various studies could show that psoriasis is closely related to metabolic syndrome (7, 16, 23–25). As a result of cardiovascular and cardiometabolic comorbidity, patients with severe psoriasis were shown to have a decreased life expectancy of up to 5 years (26, 27). Psoriasis is also frequently associated with psychological comorbidities. Altogether psoriasis has a massive negative impact on patients’ quality of life. In a US-based interview study, e.g. 98% of psoriasis patients reported that their emotional lives were impaired by their disease, 94% felt their social life was restricted and 68% perceived their careers to be hindered (28). Depending on the screening methodology, depressive symptoms are described to be present in up to 28-55% of psoriasis patients (6, 7). Social stigmatization due to easily visible skin manifestations is a strong predictor of depressive symptoms in psoriasis patients (29). However, there is emerging evidence that systemic inflammation may represent a pathophysiologic link between the diseases (30–32). For the above-mentioned reasons, patients with psoriasis, in particular with a severe form of the disease, have an urgent need for efficient therapies. Nowadays, systemic therapy options for moderate to severe psoriasis include conventional systemic agents such as dimethyl fumarate and methotrexate (MTX), the small molecule apremilast (phosphodiesterase-4 inhibitor), and various biologics (33). With the establishment of targeted cytokine inhibitors, the efficacy and tolerability of systemic therapies for the treatment of psoriasis patients has been massively increased (34). Unprecedented response rates of about 60% in terms of complete skin clearance are possible today with some of the newer biologics targeting interleukin (IL)-23 or IL-17 (35, 36). However, the first in group biologics licensed for psoriasis were tumor necrosis factor (TNF)-α inhibitors. In terms of safety profile, the incidence of severe adverse events in psoriasis patients receiving TNF-α inhibitors is low (37). Though, large cohort studies showed infliximab to be associated with an increased risk of serious infections (38). In addition, TNF-α inhibitors harbor a risk for reactivation of latent infections such as tuberculosis (39, 40). The rate of serious infections was shown to be higher especially for new users of infliximab and adalimumab (41). In contrast, therapy with anti-IL-12/23 antibodies and IL-17 inhibitors generally does not seem to increase the risk of serious infections (41).
Only very few reports in the literature so far have addressed the question to which extent immunomodulatory, respectively immunosuppressive therapies, such as those currently used to treat patients with psoriasis, influence the response to COVID-19 vaccines, which were shown to lead to serological responses in over 90% of healthy individuals (42, 43). For example, a recent study by Mahil et al. investigated psoriasis patients in the UK undergoing systemic therapy with MTX or targeted biological monotherapy. Functional humoral immunity to a single dose of BNT162b2 was shown to be impaired by MTX but not by targeted biologics, whereas cellular responses were unaffected (44, 45).
The aim of the present study was to determine the anti-SARS-CoV-2-S IgG seroconversion rate after COVID-19 vaccination in patients under active systemic treatment for moderate to severe psoriasis in order to expand the knowledge on this highly relevant topic.
This prospective single-center study of a consecutive sample of psoriasis patients under systemic treatment was performed from May 2020 until October 2021 at the Department of Dermatology, University Hospital Essen, Germany. Study outcome measures were anti-SARS-CoV-2-S IgG seroconversion and outcome of a potential COVID-19 disease. Data on patient characteristics, concomitant diseases, COVID-19 vaccination status, severity of psoriasis, systemic psoriasis therapy, and immunosuppressive comedication were collected. Leukocyte, neutrophil and lymphocyte counts were assessed at the time of first COVID-19 vaccination. Systemic treatment for psoriasis included biologics such as TNF-α inhibitors, IL-17A inhibitors, IL-23 inhibitors, the IL-12/23 inhibitor ustekinumab, the small molecule apremilast, as well as conventional therapies such as MTX and dimethyl fumarate. Concomitant diseases were evaluated using the modified Charlson Comorbidity Index (CCI) (46). Inclusion criteria were systemic treatment for moderate to severe psoriasis, completed COVID-19 vaccination corresponding to two sequential mRNA or viral vector vaccine applications, and repetitive anti-SARS-CoV-2-S IgG serum quantification (Figure 1). Anti-SARS-CoV-2-S IgG antibodies were measured at each time of consultation in our department.
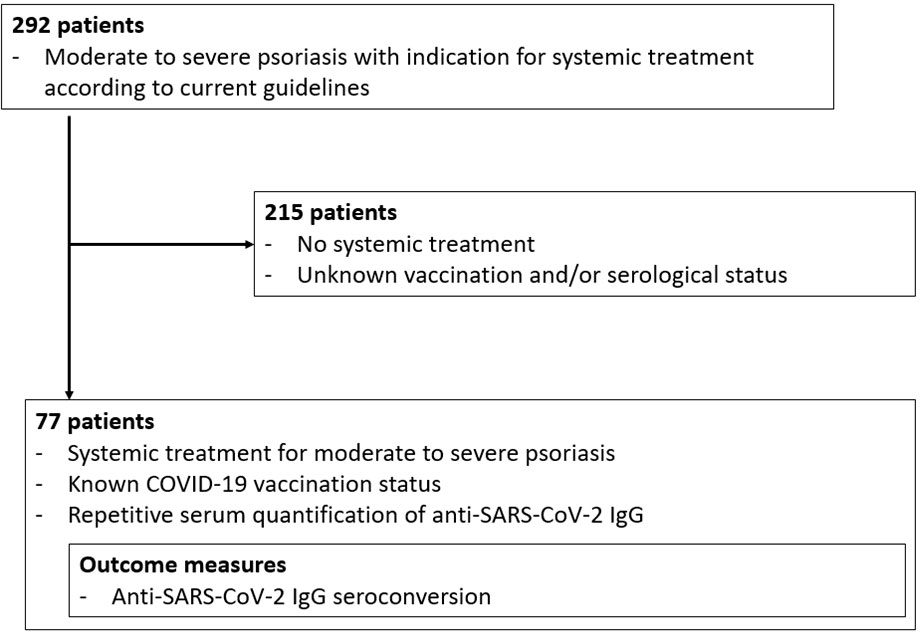
Figure 1 Patient flow chart.
Measurement of IgG antibodies against SARS-CoV-2 spike protein (anti-SARS-CoV-2-S IgG) in patients’ sera was performed with the chemiluminescence assays SARS-CoV-2 S1/S2 IgG or SARS-CoV-2 TrimericS IgG, DiaSorin, Saluggia, Italy. The chemiluminescence analyzer LIASION-XL (DiaSorin) was used following the manufacturer’s instructions. The first assay is semi-quantitative as at the start of the study no standardized fully quantitative assays were available. The second assay is quantitative and adjusted to the upcoming WHO standard. Values >15 AU/ml corresponding to 39 BAU/ml, and values ≥33.8 BAU/ml were considered positive after first or second vaccination, respectively. Sensitivity/specificity for each assay are 94.4%/98.6% and 96.9%/100%, respectively. For this study, only qualitative results were used to document seroconversion.
Descriptive statistical analyses were performed using SPSSv26.0 (IBM, Armonk, NY, USA). The follow up time was defined as the period between first serum testing and last patient visit. The study was approved by the institutional ethics committee of the University Duisburg-Essen (21-10141-BO). It was conducted in accordance with the Declaration of Helsinki.
Within the studied period, 77 of 292 consecutive psoriasis patients presenting at the Department of Dermatology, University Hospital Essen, met the inclusion criteria (Figure 1). At a median age of 55.9 years (range 23.8-86.3 years), the majority of patients had a modified CCI of 0 (n=46, 59.7%, Table 1). Sixty-six patients (85.7%) were treated with biologics (TNF-α inhibitors (n=16), IL-17A inhibitors (n=21), IL-23 inhibitors (n=21), or an IL-12/23 inhibitor (n=8); nine patients received MTX (11.7%), one patient was treated with dimethyl fumarate (1.3%), and one patient received the phosphodiesterase-4 inhibitor apremilast. At the end of data collection in October 2021, after a median follow-up time of 12.7 months, none of the patients had developed a symptomatic COVID-19 disease or died from COVID-19. The mean time between the second vaccination and analysis of antibody levels was 3.9 weeks (range 0.4-23.0 weeks). None of the patients had been vaccinated more than 6 months before antibody analysis (mean time period between first vaccination and analysis: 12.2 weeks, range: 4.1-25.9 weeks).
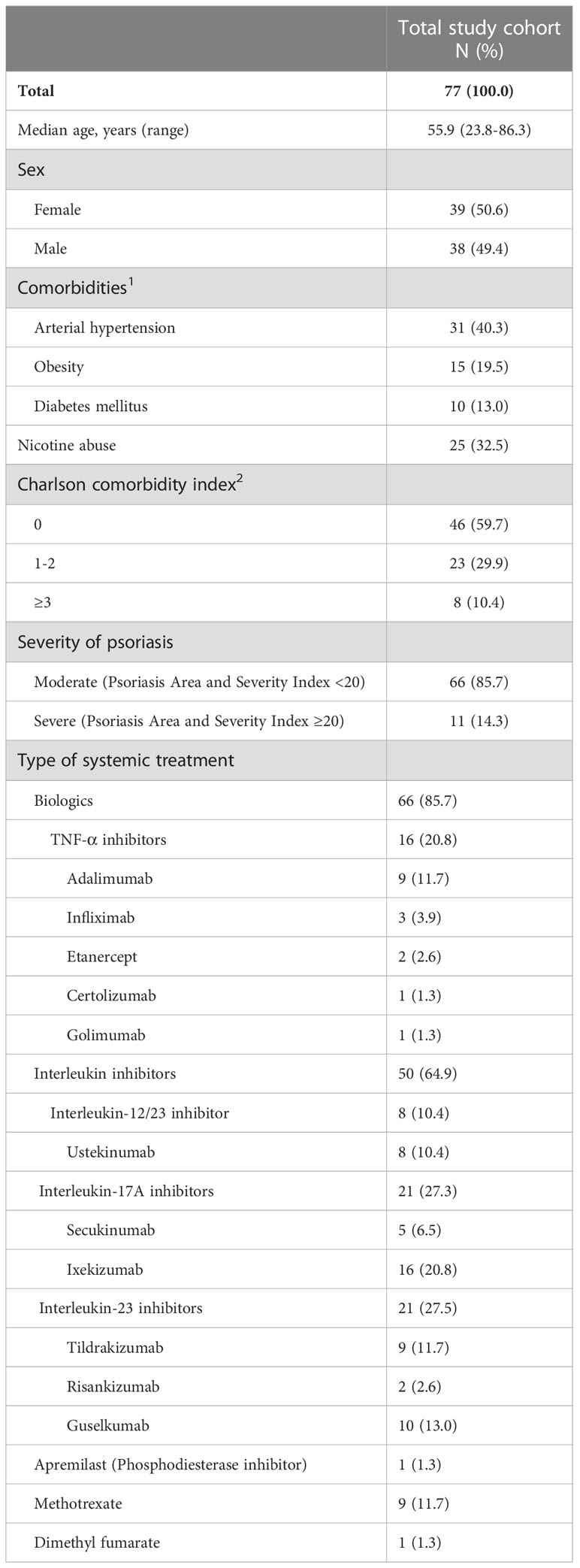
Table 1 Patient characteristics.
After completed COVID-19 vaccination (corresponding to two sequential mRNA or viral vector vaccine applications), 74/77 patients (96.1%) achieved anti-SARS-CoV-2-S IgG seroconversion (Table 2). Seroconversion was reached in 64/66 patients treated with biologics. Three of these 64 patients received additional immunosuppressive comedication with MTX 5-10 mg per week in the context of psoriasis treatment (Table 2). COVID-19 vaccination led to seroconversion in 8/9 patients treated with MTX as main systemic psoriasis treatment, in 1/1 patient under therapy with dimethyl fumarate, and in 1/1 patient treated with apremilast (Table 2).
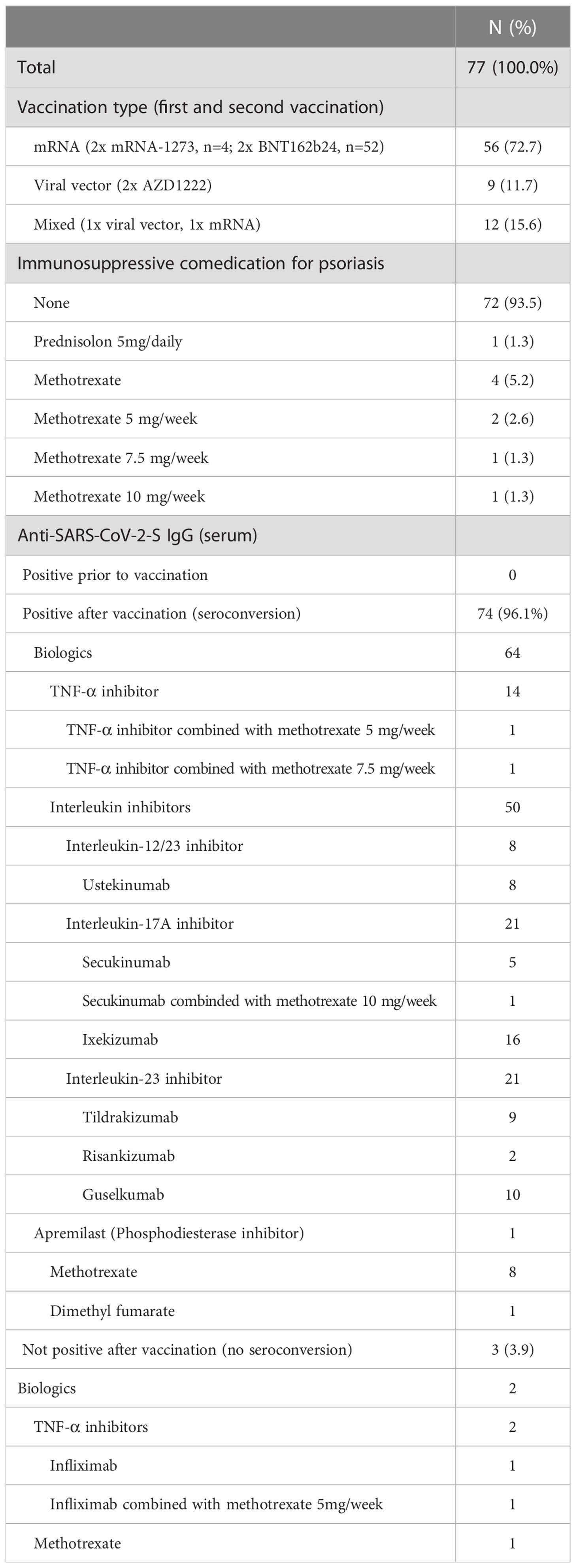
Table 2 COVID-19 vaccination and seroconversion.
In 3/77 completely vaccinated patients (3.9%) anti-SARS-CoV-2-S IgG antibodies could not be detected in sufficient amount in repeated serological tests after vaccination (anti-SARS-CoV-2-S IgG <33.8 BAU/ml) (Table 2).
The first patient without seroconversion, a 56-year-old female, was under therapy with the TNF-α inhibitor infliximab 5mg/kg Q7W i.v. and MTX 5 mg per week p.o. as an additional treatment. At the time of the first COVID-19 vaccination, she received her 46th infliximab infusion. The interval between infliximab treatments was shortened from 8 to 7 weeks due to increasing arthralgia towards the end of the interval. The patient had no further relevant comorbidities (CCI 0). At the time of the first COVID-19 vaccination, laboratory parameters including lymphocytes, leukocytes and neutrophils were within the normal range. Repeated laboratory controls performed until the end of follow-up did not reveal any pathological parameters. After two vaccinations, the patient’s absolute anti-SARS CoV-2-S IgG was 25.7 BAU/ml.
The second patient failing seroconversion, a 57-year-old female, also received infliximab 5 mg/kg Q8W. In the past, the patient also had comedication with low-dose MTX, which was discontinued 9 months ago due to lymphopenia. At the time of the first COVID-19 vaccination, the patient received her 59th infliximab infusion. The patient had no further relevant comorbidities (CCI 0). At the time of the first vaccination, the patient had decreased lymphocytes (0.90/nl). The lymphocyte counts remained decreased until the end of follow-up. After two vaccinations, the patient’s absolute anti-SARS CoV-2-S IgG was 26.5 BAU/ml.
The third patient failing seroconversion, an 86-year-old female, was treated with MTX 10 mg s.c. weekly. MTX treatment was initiated 4 weeks before the first COVID-19 vaccination. Lymphocytes, leukocytes and neutrophils were within normal ranges. The patient also suffered from diabetes mellitus type II, arterial hypertension and peripheral arterial occlusive disease of the lower legs. After two vaccinations, the patient’s absolute anti-SARS CoV-2-S IgG was 15.1 BAU/ml.
In the descriptive statistical comparison of the responder and non-responder group, no substantial differences were found. However, the median age of patients without seroconversion was slightly higher compared to patients with serological response (56.9 vs 55.6 years, Table 3). Of 13 patients receiving MTX as their main treatment, respectively comedication for psoriasis, 15.4% (n=2) failed to achieve seroconversion and of 16 patients receiving a TNF-α inhibitor as their main treatment for psoriasis 12.5% (n=2) did not reach seroconversion. The median values for leukocytes, neutrophils, and lymphocytes were similar in both groups at the time of the first COVID-19 vaccination (Table 3). However, patients who failed seroconversion (n=3) had lower median lymphocyte counts compared to patients who achieved seroconversion (1.6/nL (range 0.9-2.8) vs. 1.8/nL (range 0.6-3.8)).

Table 3 Characteristics of patients with and without anti-SARS-CoV-2-S IgG seroconversion.
One of the main intentions of the presented work was to shed more light on the question whether the systemic agents currently used for the treatment of patients with moderate to severe psoriasis negatively affect the serological response to COVID-19 vaccines. Our results showed that 96.1% of patients responded to COVID-19 vaccination in the sense of a seroconversion. The rate of seroconversion was found to be slightly reduced in patients receiving MTX and/or TNF-α inhibitors compared to those under therapy with dimethyl fumarate, apremilast and biologics targeting IL-17 or IL-12/23.
Serological response rates to COVID-19 vaccines have been reported to exceed 90% in healthy individuals (42, 43), and neutralizing antibody levels were shown to be highly predictive of immunologic protection from symptomatic SARS-CoV-2 infection (47). Yet, neutralizing assays are complex and time-consuming. For reasons of practicability, we did not assess neutralizing antibody levels but IgG antibodies against the SARS-CoV-2 spike protein. However, data from the literature found a strong correlation between IgG and neutralizing antibodies at least within a 6-month period after the second dose of vaccination (48). In our cohort, none of the patients had been vaccinated more than 6 months before the analysis of antibodies. In addition to the measured high rates of seroconversion, the fact that no patient of our cohort reported an infection by SARS-CoV-2, COVID-19, or even died from COVID-19 confirmed that an effective protection was established by the vaccinations in nearly all cases. To the best of our knowledge, only very few comparable data were published. Mahil et al. (44, 49) for example measured the serological response of COVID-19 vaccines in 67 psoriasis patients on active systemic treatment. The authors reported that all patients showed seroconversion after completed vaccination consisting of two doses, which fits in well with our findings (44, 49). Other studies also presented similar findings (50–56). The main results of other studies that also investigated the serological response to COVID-19 vaccination in psoriasis patients are summarized in Table 4
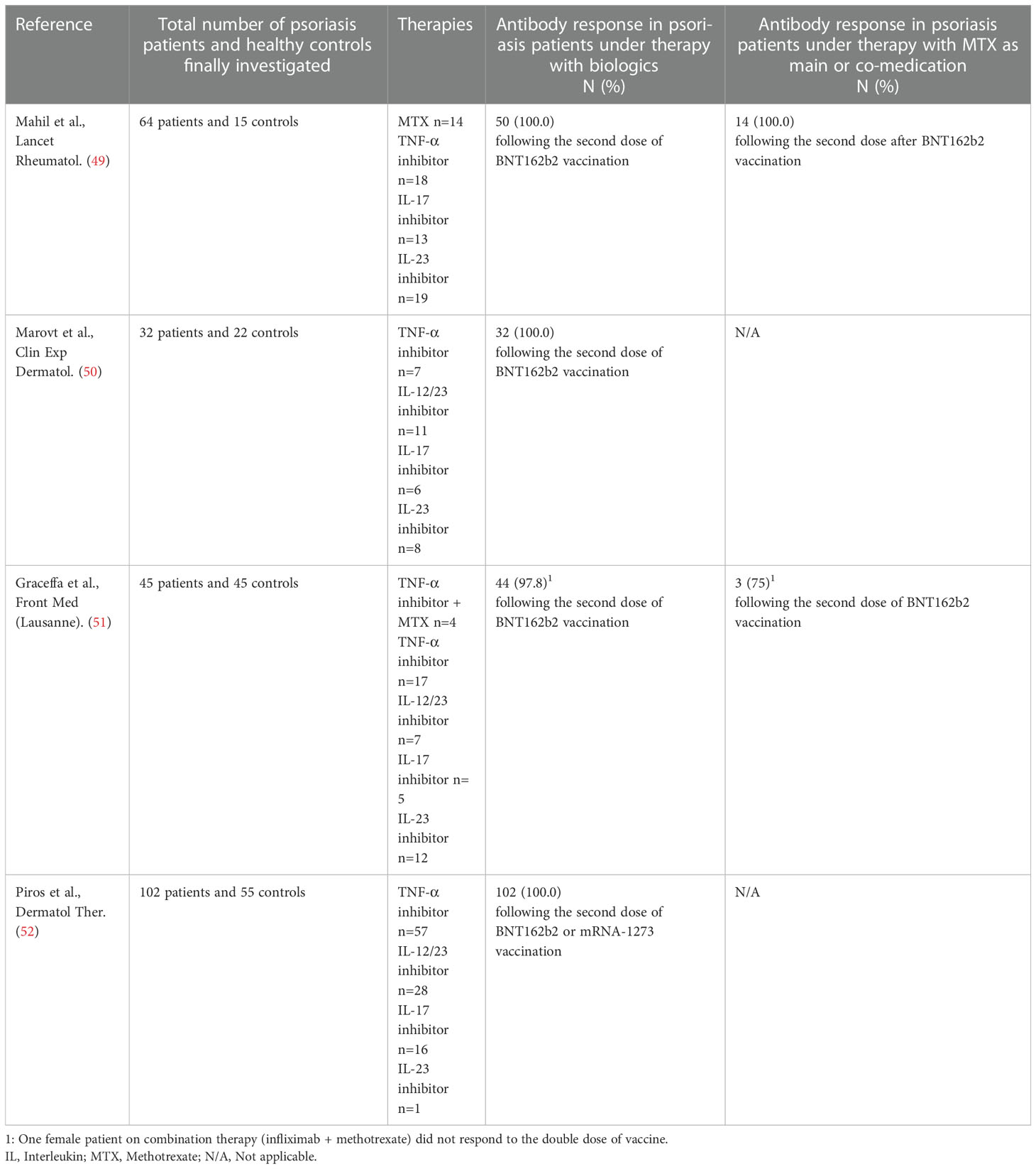
Table 4 Results of other studies investigating the serological response to COVID-19 vaccination in psoriasis patients.
Two of three patients without seroconversion received MTX. MTX is a widely used immunosuppressant for the treatment of various immune-mediated inflammatory diseases. Its safety profile includes leucopenia/pancytopenia and proneness to infections (57). In previous studies, it has been shown that the response to COVID-19 vaccination can be negatively affected by MTX (58–60). In our cohort, patients who received MTX as their main systemic psoriasis treatment or as comedication showed an impaired seroconversion rate of only 84.6% after COVID-19 vaccination. Haberman et al. even found a strongly decreased anti-SARS-CoV-2 seroconversion rate of 62.2% in patients with immune-mediated inflammatory diseases receiving MTX (59). This negative effect of MTX on seroconversion rates is also known from other types of vaccines such as influenza, pneumococcal or tetanus (60–65).
Additionally, two of the three patients who did not achieve seroconversion after COVID-19 vaccination were under therapy with TNF-α inhibitors (n=1, infliximab monotherapy; n=1, infliximab plus MTX low-dose). As already stated above, TNF-α inhibitors, and especially infliximab, have an inferior safety profile in comparison with the newer cytokine inhibitors targeting IL-17 and IL-12/23, which is mainly due to a higher number of severe infections under TNF-α inhibitors (37, 38, 41) suggesting an impact on the immunologic surveillance of infectious diseases. The effect of TNF-α inhibitors on the immune system has already been reflected in decreased response rates observed in various studies on different vaccinations in the past (66–71). For example, reduced immune responses could be observed after influenza (68, 69), pneumococcal (70), and hepatitis B vaccinations (71) in patients receiving infliximab in comparison to therapy-naive patients.
It should be noted, that one of the serological non-responding patients was 86 years old, raising the question whether age may have an impact on COVID-19 vaccine response in psoriasis patients. Although our study only involved one older-aged patient with failed seroconversion, data from the literature indicate that older patients exhibit weaker or delayed immune responses to COVID-19 vaccines compared to younger patients (72). The aforementioned patient also had different concomitant diseases such as diabetes mellitus. Evidence regarding the efficacy of COVID-19 vaccines in patients with underlying diseases in general is still limited (73).
In our cohort, patients who failed seroconversion (n=3) had a lower median lymphocyte count compared to patients who achieved seroconversion. Avivi et al. reported statistically significantly lower seroconversion rates upon COVID-19 vaccination in patients with lymphopenia (74). However, it has to be considered that in our study the sample size of patients with failure of seroconversion was very low.
General limitations of our study include the relatively small number of patients, a high selection bias due to recruitment of patients from our highly specialized psoriasis center and the monocentric design. Furthermore, this study lacks a control group, neutralizing assays and cellular data such as B cell numbers as well as a quantification of T cell responses. Due to the highly dynamic development of new SARS-CoV-2 diagnostics, two test generations were used in this prospective longitudinal study. While the first assay used was semi-quantitative, the second assay was quantitative and adjusted to the upcoming WHO standard. As a result, it was not possible to present consistent quantitative data of antibody levels.
In the meantime, three vaccine doses against SARS-CoV-2 are widely considered as standard immunization and e.g. in Germany a fourth dose is even recommended for particular subgroups at risk (75). Thus, it would be of high interest to also investigate the seroconversion rates of patients with psoriasis under active systemic treatment systematically under these adapted conditions. There is already some data showing that initial non-responders can often achieve seroconversion in response to further vaccination, which is consistent with our own recent clinical experiences (76, 77).
For patients who do not mount antibody responses to COVID-19 despite repeated vaccination, a passive immunization against SARS-CoV-2 with neutralizing monoclonal antibodies is possible (78). Currently, the combinations of casirivimab/imdevimab (Ronapreve®) and tixagevimab/cilgavimab (Evusheld®) are approved by the European Medicines Agency for passive immunization against COVID-19 (79, 80). However, in vitro studies show that casirivimab/imdevimab does not result in relevant neutralization against the currently circulating Omicron variants (81–83). For this reason, the currently published German S1 guideline on SARS-CoV-2 pre-exposure prophylaxis recommends only the use of tixagevimab/cilgavimab for passive immunization, as in particular in-vitro studies of cilgavimab demonstrated the ability to neutralize omicron variants (78, 81–83).
The vast majority of psoriasis patients receiving systemic treatment achieved a seroconversion in response to two COVID-19 vaccinations. Seroconversion rate for patients under therapy with modern cytokine inhibitors targeting IL-17 or IL-23 was 100%. An impaired serological response was observed in patients who received MTX and/or TNF-α inhibitors, respectively. Larger real-world studies are needed to confirm our preliminary findings.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics committee of the University Duisburg-Essen (21-10141-BO). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization: SU, WS, GL, FK. Methodology: SU, MF, WS, GL, FK. Formal analysis: MF, SU, WS, GL, FK. Resources: UD, DS, WS, SU, GL, FK. Data curation, GL, SU, WS, FK. Writing - original draft preparation: GL, SU, WS, FK. Writing and editing: GL, FK, MF, UD, J-MP, JB, DS, WS, SU. Visualization: SU, GL, WS, FK. Supervision: WS. Project administration: GL, FK, SU, WS. All authors contributed to the article and approved the submitted version.
We thank all study participants and their families. GL was supported by the Deutsche Forschungsgemeinschaft (DFG, German 582 Research Foundation, RTG 2535, Knowledge- and data-driven personalization of medicine at the 583 point of care). J-MP was supported by the DFG in the framework of the DFG Clinician Scientist Program UMEA, FU 356/12-1.
GL has received travel support from Sun Pharma. FK has received travel support and/or personal fees from Novartis and Almirall. MF has given a paid lecture for Dia Sorin.
UD reports consulting fees from Biontech and Moderna, and advisory board honoraria from Moderna outside the submitted work. J-MP served as consultant and/or has received honoraria from Bristol-Myers Squibb and Novartis, and received travel support from Bristol-Myers Squibb, Novartis, Pierre Fabre and Therakos. JB declares speaker honoraria from Amgen and Sanofi; advisory board honoraria from 4SC, Almirall, Amgen, MerckSerono, Novartis, InProTher, and Sanofi; research funding from Alcedis, Bristol-Myers Squibb, HTG, IQVIA, and MerckSerono; travel support from 4SC and Incyte. DS reports grants or contracts from Amgen, Array/Pfizer, Bristol-Myers Squibb, MSD, Novartis and Roche; consulting fees from 4SC, Amgen, Array Biopharma, AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Haystick, Immunocore, InFlarX, Innocent, LabCorp, Merck Serono, MSD, Nektar, NeraCare, Novartis, OncoSec, Pfizer, Philogen, Pierre Fabre, Replimune, Roche, Sandoz, Sanofi/Regeneron, Sun Pharma; honoraria from Bristol-Myers Squibb, MSD/Merck, Merck Serono, Novartis, Roche, Sanofi and Sun Pharma; support for attendings meetings or travel support from Bristol-Myers Squibb, MSD, Merck Serono, Novartis, Pierre Fabre and Sanofi; participation on drug safety monitoring or advisory boards for 4SC, Amgen, Array Biopharma, AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Immunocore, InFlarX, Merck Serono, MSD, Nektar, NeraCare, Novartis, OncoSec, Pfizer, Philogen, Pierre Fabre, Replimune, Roche, Sandoz, Sanofi/Regeneron and SunPharma; leadership roles for DeCOG, German Cancer Society, Hiege-Stiftung, Deutsche Hautkrebsstiftung, NVKH e.V. and EuMelaReg. WS reports grants and/or personal fees and/or speaker honoraria from medi GmbH Bayreuth, Abbvie, Almirall, Amgen, Bristol-Myers Squibb, Celgene, GSK, Janssen, LEO Pharma, Lilly, MSD, Novartis, Pfizer, Roche, Sanofi Genzyme und UCB outside the submitted work. SU declares research support from Bristol Myers Squibb and Merck Serono; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, Merck Sharp & Dohme, and Pierre Fabre; outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Schafer I, Rustenbach SJ, Radtke M, Augustin J, Glaeske G, Augustin M. [Epidemiology of psoriasis in Germany–analysis of secondary health insurance data]. Gesundheitswesen (2011) 73:308–13. doi: 10.1055/s-0030-1252022
2. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker J. Psoriasis. Lancet (2021) 397:1301–15. doi: 10.1016/S0140-6736(20)32549-6
3. Mrowietz U, Steinz K, Gerdes S. Psoriasis: to treat or to manage? Exp Dermatol (2014) 23:705–9. doi: 10.1111/exd.12437
4. Boehncke WH. Systemic inflammation and cardiovascular comorbidity in psoriasis patients: Causes and consequences. Front Immunol (2018) 9:579. doi: 10.3389/fimmu.2018.00579
5. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The 'psoriatic march': a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol (2011) 20:303–7. doi: 10.1111/j.1600-0625.2011.01261.x
6. Kaye JA, Li L, Jick SS. Incidence of risk factors for myocardial infarction and other vascular diseases in patients with psoriasis. Br J Dermatol (2008) 159:895–902. doi: 10.1111/j.1365-2133.2008.08707.x
7. Miller IM, Ellervik C, Yazdanyar S, Jemec GB. Meta-analysis of psoriasis, cardiovascular disease, and associated risk factors. J Am Acad Dermatol (2013) 69:1014–24. doi: 10.1016/j.jaad.2013.06.053
8. Phan C, Sigal ML, Lhafa M, Barthelemy H, Maccari F, Esteve E, et al. Metabolic comorbidities and hypertension in psoriasis patients in france. comparisons with French national databases. Ann Dermatol Venereol (2016) 143:264–74. doi: 10.1016/j.annder.2015.06.024
9. Armesto S, Coto-Segura P, Osuna CG, Camblor PM, Santos-Juanes J. Psoriasis and hypertension: a case-control study. J Eur Acad Dermatol Venereol (2012) 26:785–8. doi: 10.1111/j.1468-3083.2011.04108.x
10. Cohen AD, Weitzman D, Dreiher J. Psoriasis and hypertension: a case-control study. Acta Derm Venereol (2010) 90:23–6. doi: 10.2340/00015555-0741
11. Qureshi AA, Choi HK, Setty AR, Curhan GC. Psoriasis and the risk of diabetes and hypertension: a prospective study of US female nurses. Arch Dermatol (2009) 145:379–82. doi: 10.1001/archdermatol.2009.48
12. Benson MM, Frishman WH. The heartbreak of psoriasis: a review of cardiovascular risk in patients with psoriasis. Cardiol Rev (2015) 23:312–6. doi: 10.1097/crd.0000000000000048
13. Coumbe AG, Pritzker MR, Duprez DA. Cardiovascular risk and psoriasis: beyond the traditional risk factors. Am J Med (2014) 127:12–8. doi: 10.1016/j.amjmed.2013.08.013
14. Armstrong EJ, Harskamp CT, Armstrong AW. Psoriasis and major adverse cardiovascular events: a systematic review and meta-analysis of observational studies. J Am Heart Assoc (2013) 2:e000062. doi: 10.1161/jaha.113.000062
15. Balci DD, Balci A, Karazincir S, Ucar E, Iyigun U, Yalcin F, et al. Increased carotid artery intima-media thickness and impaired endothelial function in psoriasis. J Eur Acad Dermatol Venereol (2009) 23:1–6. doi: 10.1111/j.1468-3083.2008.02936.x
16. Miller IM, Ellervik C, Zarchi K, Ibler KS, Vinding GR, Knudsen KM, et al. The association of metabolic syndrome and psoriasis: a population- and hospital-based cross-sectional study. J Eur Acad Dermatol Venereol (2015) 29:490–7. doi: 10.1111/jdv.12595
17. Miller IM, Skaaby T, Ellervik C, Jemec GB. Quantifying cardiovascular disease risk factors in patients with psoriasis: a meta-analysis. Br J Dermatol (2013) 169:1180–7. doi: 10.1111/bjd.12490
18. Setty AR, Curhan G, Choi HK. Obesity, waist circumference, weight change, and the risk of psoriasis in women: Nurses' health study II. Arch Intern Med (2007) 167:1670–5. doi: 10.1001/archinte.167.15.1670
20. Gyldenlove M, Storgaard H, Holst JJ, Vilsboll T, Knop FK, Skov L. Patients with psoriasis are insulin resistant. J Am Acad Dermatol (2015) 72:599–605. doi: 10.1016/j.jaad.2015.01.004
21. Lønnberg AS, Skov L, Skytthe A, Kyvik KO, Pedersen OB, Thomsen SF. Association of psoriasis with the risk for type 2 diabetes mellitus and obesity. JAMA Dermatol (2016) 152:761–7. doi: 10.1001/jamadermatol.2015.6262
22. Dubreuil M, Rho YH, Man A, Zhu Y, Zhang Y, Love TJ, et al. Diabetes incidence in psoriatic arthritis, psoriasis and rheumatoid arthritis: a UK population-based cohort study. Rheumatol (Oxford) (2014) 53:346–52. doi: 10.1093/rheumatology/ket343
23. Danielsen K, Wilsgaard T, Olsen AO, Eggen AE, Olsen K, Cassano PA, et al. Elevated odds of metabolic syndrome in psoriasis: a population-based study of age and sex differences. Br J Dermatol (2015) 172:419–27. doi: 10.1111/bjd.13288
24. Rodriguez-Zuniga MJM, Cortez-Franco F, Quijano-Gomero E. Association of psoriasis and metabolic syndrome in Latin America: A systematic review and meta-analysis. Actas Dermosifiliogr (2017) 108:326–34. doi: 10.1016/j.ad.2016.11.009
25. Parodi A, Aste N, Calvieri C, Cantoresi F, Carlesimo M, Fabbri P, et al. Metabolic syndrome prevalence in psoriasis: a cross-sectional study in the Italian population. Am J Clin Dermatol (2014) 15:371–7. doi: 10.1007/s40257-014-0074-8
26. Abuabara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Cause-specific mortality in patients with severe psoriasis: a population-based cohort study in the U.K. Br J Dermatol (2010) 163:586–92. doi: 10.1111/j.1365-2133.2010.09941.x
27. Gelfand JM, Troxel AB, Lewis JD, Kurd SK, Shin DB, Wang X, et al. The risk of mortality in patients with psoriasis: results from a population-based study. Arch Dermatol (2007) 143:1493–9. doi: 10.1001/archderm.143.12.1493
28. Pariser D, Schenkel B, Carter C, Farahi K, Brown TM, Ellis CN, et al. A multicenter, non-interventional study to evaluate patient-reported experiences of living with psoriasis. J Dermatolog Treat (2016) 27:19–26. doi: 10.3109/09546634.2015.1044492
29. Łakuta P, Marcinkiewicz K, Bergler-Czop B, Brzezińska-Wcisło L. The relationship between psoriasis and depression: A multiple mediation model. Body Image (2016) 19:126–32. doi: 10.1016/j.bodyim.2016.08.004
30. Hölsken S, Krefting F, Schedlowski M, Sondermann W. Common fundamentals of psoriasis and depression. Acta Derm Venereol (2021) 101:adv00609. doi: 10.2340/actadv.v101.565
31. Koo J, Marangell LB, Nakamura M, Armstrong A, Jeon C, Bhutani T, et al. Depression and suicidality in psoriasis: review of the literature including the cytokine theory of depression. J Eur Acad Dermatol Venereol (2017) 31:1999–2009. doi: 10.1111/jdv.14460
32. Cohen BE, Martires KJ, Ho RS. Psoriasis and the risk of depression in the US population: National health and nutrition examination survey 2009-2012. JAMA Dermatol (2016) 152:73–9. doi: 10.1001/jamadermatol.2015.3605
33. Nast A, Altenburg A, Augustin M, Boehncke WH, Härle P, Klaus J, et al. German S3-guideline on the treatment of psoriasis vulgaris, adapted from EuroGuiDerm - part 1: Treatment goals and treatment recommendations. J Dtsch Dermatol Ges (2021) 19:934–150. doi: 10.1111/ddg.14508
34. Kamata M, Tada Y. Efficacy and safety of biologics for psoriasis and psoriatic arthritis and their impact on comorbidities: A literature review. Int J Mol Sci (2020) 21:1690. doi: 10.3390/ijms21051690
35. Reich K, Warren RB, Lebwohl M, Gooderham M, Strober B, Langley RG, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med (2021) 385:142–52. doi: 10.1056/NEJMoa2102383
36. Warren RB, Blauvelt A, Poulin Y, Beeck S, Kelly M, Wu T, et al. Efficacy and safety of risankizumab vs. secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): results from a phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br J Dermatol (2021) 184:50–9. doi: 10.1111/bjd.19341
37. Kamata M, Tada Y. Safety of biologics in psoriasis. J Dermatol (2018) 45:279–86. doi: 10.1111/1346-8138.14096
38. Yiu ZZN, Ashcroft DM, Evans I, McElhone K, Lunt M, Smith CH, et al. Infliximab is associated with an increased risk of serious infection in patients with psoriasis in the U.K. and republic of Ireland: results from the British association of dermatologists biologic interventions register (BADBIR). Br J Dermatol (2019) 180:329–37. doi: 10.1111/bjd.17036
39. Gisondi P, Cazzaniga S, Chimenti S, Maccarone M, Picardo M, Girolomoni G, et al. Latent tuberculosis infection in patients with chronic plaque psoriasis: evidence from the Italian psocare registry. Br J Dermatol (2015) 172:1613–20. doi: 10.1111/bjd.13539
40. Doherty SD, Van Voorhees A, Lebwohl MG, Korman NJ, Young MS, Hsu S, et al. National psoriasis foundation consensus statement on screening for latent tuberculosis infection in patients with psoriasis treated with systemic and biologic agents. J Am Acad Dermatol (2008) 59:209–17. doi: 10.1016/j.jaad.2008.03.023
41. Penso L, Dray-Spira R, Weill A, Pina Vegas L, Zureik M, Sbidian E. Association between biologics use and risk of serious infection in patients with psoriasis. JAMA Dermatol (2021) 157:1056–65. doi: 10.1001/jamadermatol.2021.2599
42. Demonbreun AR, Sancilio A, Velez MP, Ryan DT, Saber R, Vaught LA, et al. Comparison of IgG and neutralizing antibody responses after one or two doses of COVID-19 mRNA vaccine in previously infected and uninfected individuals. EClinicalMedicine (2021) 38:101018. doi: 10.1016/j.eclinm.2021.101018
43. Dagan N, Barda N, Kepten E, Miron O, Perchik S, Katz MA, et al. BNT162b2 mRNA covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med (2021) 384:1412–23. doi: 10.1056/NEJMoa2101765
44. Mahil SK, Bechman K, Raharja A, Domingo-Vila C, Baudry D, Brown MA, et al. The effect of methotrexate and targeted immunosuppression on humoral and cellular immune responses to the COVID-19 vaccine BNT162b2: a cohort study. Lancet Rheumatol (2021) 3:e627–e37. doi: 10.1016/s2665-9913(21)00212-5
45. Boekel L. Immunity after COVID-19 vaccinations in immunocompromised patients with psoriasis. Lancet Rheumatol (2022) 4:e5–7. doi: 10.1016/S2665-9913(21)00360-X
46. Thomas SJ, Perez JL, Lockhart SP, Hariharan S, Kitchin N, Bailey R, et al. 1558O COVID-19 vaccine in participants (ptcpts) with cancer: Subgroup analysis of efficacy/safety from a global phase III randomized trial of the BNT162b2 (tozinameran) mRNA vaccine. Ann Oncol (2021) S1129:e5–7. doi: 10.1016/j.annonc.2021.08.1551
47. Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med (2021) 27:1205–11. doi: 10.1038/s41591-021-01377-8
48. Levin EG, Lustig Y, Cohen C, Fluss R, Indenbaum V, Amit S, et al. Waning immune humoral response to BNT162b2 covid-19 vaccine over 6 months. N Engl J Med (2021) 385:e84. doi: 10.1056/NEJMoa2114583
49. Mahil SK, Bechman K, Raharja A, Domingo-Vila C, Baudry D, Brown MA, et al. Humoral and cellular immunogenicity to a second dose of COVID-19 vaccine BNT162b2 in people receiving methotrexate or targeted immunosuppression: a longitudinal cohort study. Lancet Rheumatol (2022) 4:e42–52. doi: 10.1016/S2665-9913(21)00333-7
50. Marovt M, Dezelak P, Ekart R, Marko PB. Immune response to SARS-CoV-2 mRNA vaccine in patients with psoriasis treated with biologics. Clin Exp Dermatol (2022) 47:2041–3. doi: 10.1111/ced.15347
51. Graceffa D, Sperati F, Bonifati C, Spoletini G, Lora V, Pimpinelli F, et al. Immunogenicity of three doses of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologics. Front Med (Lausanne). (2022) 9:961904. doi: 10.3389/fmed.2022.961904
52. Piros EA, Cseprekal O, Gorog A, Hidvegi B, Medvecz M, Szabo Z, et al. Seroconversion after anti-SARS-CoV-2 mRNA vaccinations among moderate-to-severe psoriatic patients receiving systemic biologicals-prospective observational cohort study. Dermatol Ther (2022) 35:e15408. doi: 10.1111/dth.15408
53. Al-Janabi A, Littlewood Z, Griffiths CEM, Hunter HJA, Chinoy H, Moriarty C, et al. Antibody responses to single-dose SARS-CoV-2 vaccination in patients receiving immunomodulators for immune-mediated inflammatory disease. Br J Dermatol (2021) 185:646–8. doi: 10.1111/bjd.20479
54. Fagni F, Simon D, Tascilar K, Schoenau V, Sticherling M, Neurath MF, et al. COVID-19 and immune-mediated inflammatory diseases: effect of disease and treatment on COVID-19 outcomes and vaccine responses. Lancet Rheumatol (2021) 3:e724–e36. doi: 10.1016/S2665-9913(21)00247-2
55. Simon D, Tascilar K, Fagni F, Kleyer A, Kronke G, Meder C, et al. Intensity and longevity of SARS-CoV-2 vaccination response in patients with immune-mediated inflammatory disease: a prospective cohort study. Lancet Rheumatol (2022) 4:e614–e25. doi: 10.1016/S2665-9913(22)00191-6
56. Simon D, Tascilar K, Fagni F, Kronke G, Kleyer A, Meder C, et al. SARS-CoV-2 vaccination responses in untreated, conventionally treated and anticytokine-treated patients with immune-mediated inflammatory diseases. Ann Rheum Dis (2021) 80:1312–6. doi: 10.1136/annrheumdis-2021-220461
57. West J, Ogston S, Foerster J. Safety and efficacy of methotrexate in psoriasis: A meta-analysis of published trials. PloS One (2016) 11:e0153740. doi: 10.1371/journal.pone.0153740
58. Furer V, Eviatar T, Zisman D, Peleg H, Paran D, Levartovsky D, et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: a multicentre study. Ann Rheum Dis (2021) 80:1330–8. doi: 10.1136/annrheumdis-2021-220647
59. Haberman RH, Herati R, Simon D, Samanovic M, Blank RB, Tuen M, et al. Methotrexate hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. Ann Rheum Dis (2021) 80:1339–44. doi: 10.1136/annrheumdis-2021-220597
60. Friedman MA, Curtis JR, Winthrop KL. Impact of disease-modifying antirheumatic drugs on vaccine immunogenicity in patients with inflammatory rheumatic and musculoskeletal diseases. Ann Rheum Dis (2021) 80:1255–65. doi: 10.1136/annrheumdis-2021-221244
61. Adler S, Krivine A, Weix J, Rozenberg F, Launay O, Huesler J, et al. Protective effect of A/H1N1 vaccination in immune-mediated disease–a prospectively controlled vaccination study. Rheumatol (Oxford) (2012) 51:695–700. doi: 10.1093/rheumatology/ker389
62. Park JK, Lee MA, Lee EY, Song YW, Choi Y, Winthrop KL, et al. Effect of methotrexate discontinuation on efficacy of seasonal influenza vaccination in patients with rheumatoid arthritis: a randomised clinical trial. Ann Rheum Dis (2017) 76:1559–65. doi: 10.1136/annrheumdis-2017-211128
63. Buhler S, Jaeger VK, Adler S, Bannert B, Brummerhoff C, Ciurea A, et al. Safety and immunogenicity of tetanus/diphtheria vaccination in patients with rheumatic diseases-a prospective multi-centre cohort study. Rheumatol (Oxford) (2019) 58:1585–96. doi: 10.1093/rheumatology/kez045
64. Nived P, Saxne T, Geborek P, Mandl T, Skattum L, Kapetanovic MC. Antibody response to 13-valent pneumococcal conjugate vaccine is not impaired in patients with rheumatoid arthritis or primary sjogren's syndrome without disease modifying treatment. BMC Rheumatol (2018) 2:12. doi: 10.1186/s41927-018-0019-6
65. Rasmussen SL, Fuursted K, Nielsen KA, Laurberg NP, Sorensen MB, Fagerberg SK, et al. Pneumococcal antibody protection in patients with autoimmune inflammatory rheumatic diseases with varying vaccination status. Scand J Rheumatol (2020) 49:353–60. doi: 10.1080/03009742.2020.1732459
66. Wagner N, Assmus F, Arendt G, Baum E, Baumann U, Bogdan C, et al. Bundesgesundheitsblatt gesundheitsforschung gesundheitsschutz. Bundesgesundheitsbl (2019) 62:494–515. doi: 10.1007/s00103-019-02905-1
67. Miehsler W, Novacek G, Wenzl H, Vogelsang H, Knoflach P, Kaser A, et al. A decade of infliximab: The Austrian evidence based consensus on the safe use of infliximab in inflammatory bowel disease. J Crohns Colitis (2010) 4:221–56. doi: 10.1016/j.crohns.2009.12.001
68. Hagihara Y, Ohfuji S, Watanabe K, Yamagami H, Fukushima W, Maeda K, et al. Infliximab and/or immunomodulators inhibit immune responses to trivalent influenza vaccination in adults with inflammatory bowel disease. J Crohns Colitis (2014) 8:223–33. doi: 10.1016/j.crohns.2013.08.008
69. deBruyn J, Fonseca K, Ghosh S, Panaccione R, Gasia MF, Ueno A, et al. Immunogenicity of influenza vaccine for patients with inflammatory bowel disease on maintenance infliximab therapy: A randomized trial. Inflammation Bowel Dis (2016) 22:638–47. doi: 10.1097/MIB.0000000000000615
70. Fiorino G, Peyrin-Biroulet L, Naccarato P, Szabo H, Sociale OR, Vetrano S, et al. Effects of immunosuppression on immune response to pneumococcal vaccine in inflammatory bowel disease: a prospective study. Inflammation Bowel Dis (2012) 18:1042–7. doi: 10.1002/ibd.21800
71. Andrade P, Santos-Antunes J, Rodrigues S, Lopes S, Macedo G. Treatment with infliximab or azathioprine negatively impact the efficacy of hepatitis b vaccine in inflammatory bowel disease patients. J Gastroenterol Hepatol (2015) 30:1591–5. doi: 10.1111/jgh.13001
72. Schwarz T, Tober-Lau P, Hillus D, Helbig ET, Lippert LJ, Thibeault C, et al. Delayed antibody and T-cell response to BNT162b2 vaccination in the elderly, Germany. Emerg Infect Dis (2021) 27:2174–8. doi: 10.3201/eid2708.211145
73. Pal R, Bhadada SK, Misra A. COVID-19 vaccination in patients with diabetes mellitus: Current concepts, uncertainties and challenges. Diabetes Metab Syndr (2021) 15:505–8. doi: 10.1016/j.dsx.2021.02.026
74. Avivi I, Balaban R, Shragai T, Sheffer G, Morales M, Aharon A, et al. Humoral response rate and predictors of response to BNT162b2 mRNA COVID19 vaccine in patients with multiple myeloma. Br J Haematol (2021) 195:186–93. doi: 10.1111/bjh.17608
75. RKI. Epidemiologisches bulletin. STIKO: 24. aktualisierung der COVID-19-Impfempfehlung (2022). Available at: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2022/Ausgaben/50_22.pdf?:blob=publicationFile (Accessed 27, 2022).
76. Wieske L, van Dam KPJ, Steenhuis M, Stalman EW, Kummer LYL, van Kempen ZLE, et al. Humoral responses after second and third SARS-CoV-2 vaccination in patients with immune-mediated inflammatory disorders on immunosuppressants: a cohort study. Lancet Rheumatol (2022) 4:e338–e50. doi: 10.1016/s2665-9913(22)00034-0
77. Lee A, Wong SY, Chai LYA, Lee SC, Lee MX, Muthiah MD, et al. Efficacy of covid-19 vaccines in immunocompromised patients: systematic review and meta-analysis. Bmj (2022) 376:e068632. doi: 10.1136/bmj-2021-068632
78. AWMF. S1-leitlinie SARS-CoV-2 prä-expositionsprophylaxe 2022 (2022). Available at: https://www.awmf.org/uploads/tx_szleitlinien/092-002l_S1_SARS-CoV-2_Prae-Expositionsprophylaxe_2022-05_01.pdf (Accessed 22, 2022).
79. EMA. Ronapreve (casirivimab and imdevimab) an overview of ronapreve and why it is authorised in the EU (2022). Available at: https://www.ema.europa.eu/en/documents/overview/ronapreve-epar-medicine-overview_en.pdf (Accessed 22, 2022).
80. EMA. Evusheld (tixagevimab / cilgavimab) an overview of evusheld and why it is authorised in the EU (2022). Available at: https://www.ema.europa.eu/en/documents/overview/evusheld-epar-medicine-overview_en.pdf (Accessed 22, 2022).
81. Iketani S, Liu L, Guo Y, Liu L, Chan JF, Huang Y, et al. Antibody evasion properties of SARS-CoV-2 omicron sublineages. Nature (2022) 604:553–6. doi: 10.1038/s41586-022-04594-4
82. Bruel T, Hadjadj J, Maes P, Planas D, Seve A, Staropoli I, et al. Serum neutralization of SARS-CoV-2 omicron sublineages BA.1 and BA.2 in patients receiving monoclonal antibodies. Nat Med (2022) 28:1297–302. doi: 10.1038/s41591-022-01792-5
Keywords: COVID-19 vaccines, seroconversion, psoriasis, psoriasis treatment, biologics
Citation: Lodde GC, Krefting F, Placke J-M, Schneider L, Fiedler M, Dittmer U, Becker JC, Hölsken S, Schadendorf D, Ugurel S and Sondermann W (2023) COVID-19 vaccination in psoriasis patients receiving systemic treatment: A prospective single-center study. Front. Immunol. 14:1107438. doi: 10.3389/fimmu.2023.1107438
Received: 24 November 2022; Accepted: 22 February 2023;
Published: 16 March 2023.
Edited by:
Michele Maria Luchetti Gentiloni, Marche Polytechnic University, ItalyReviewed by:
Michael Sticherling, University Hospital Erlangen, GermanyCopyright © 2023 Lodde, Krefting, Placke, Schneider, Fiedler, Dittmer, Becker, Hölsken, Schadendorf, Ugurel and Sondermann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wiebke Sondermann, d2llYmtlLnNvbmRlcm1hbm5AdWstZXNzZW4uZGU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.