
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol., 16 September 2022
Sec. Cancer Immunity and Immunotherapy
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.984132
This article is part of the Research TopicRecent advances and challenges in cancer immunotherapies for patients with autoimmune diseasesView all 11 articles
 Roxane Mari1*
Roxane Mari1* Mathilde Guerin1
Mathilde Guerin1 Cécile Vicier1
Cécile Vicier1 Jochen Walz2
Jochen Walz2 Nathalie Bonnet3
Nathalie Bonnet3 Géraldine Pignot2
Géraldine Pignot2 Gwenaelle Gravis1
Gwenaelle Gravis1Background: Immune checkpoint inhibitors deeply modified metastatic renal cell carcinoma’s management, and confront us to adverse events that we were not used to with conventional anti-cancer therapies. We report the case of a patient who received nivolumab as second-line treatment of a metastatic clear cell renal cell carcinoma and who developed bullous pemphigoid four years after nivolumab introduction, with persistent exacerbations even after its discontinuation.
Case presentation: A 66-year-old man was diagnosed with lung metastasis eight years after radical nephrectomy for a clear cell renal cell carcinoma. He firstly received an anti-angiogenic agent combination, and then received anti-programmed death 1 (PD1) nivolumab as second-line treatment. Nivolumab led to prolonged disease control, but after four years of exposure the patient developed skin lesions consistent with bullous pemphigoid. After seven years of nivolumab administration and perfect disease stability, nivolumab was discontinued and surveillance was proposed. Despite nivolumab discontinuation, the patient continued to develop bullous pemphigoid exacerbations. Metastatic renal cell carcinoma was still perfectly stable more than two years after immune checkpoint discontinuation with no further anti-cancer therapy.
Discussion: We report the case of a refractory bullous pemphigoid which occurred four years after nivolumab introduction and lasted despite nivolumab discontinuation, in a patient whose metastatic renal cell carcinoma is still controlled after more than two years without any anticancer treatment. This highlights the potential association between immune-related adverse events and response to immune checkpoint inhibitors, and underlines the occurrence of late-onset and long-lasting immune-related adverse events even after discontinuation of treatment, which must encourage us to remain vigilant in the long term.
Kidney cancer, among which renal cell carcinoma (RCC) is the most common form, represents the 7th most common cancer in men, and the 10th most common cancer in women (1). Metastatic renal cell carcinoma’s management has been deeply modified by the approvement of immune checkpoint inhibitors (ICI). Nivolumab, an anti-programmed death 1 (PD1) monoclonal antibody, was firstly used as monotherapy for advanced clear cell renal cell carcinoma (ccRCC) who experienced progression after antiangiogenic therapy (2). It was secondly approved as first-line treatment for ccRCC in association with ipilimumab – another ICI that targets the Cytotoxic-T-Lymphocyte-Antigen 4 protein (CTLA4) – for intermediate and poor risk patients (3), and then in association with the tyrosine kinase inhibitor (TKI) cabozantinib, regardless of the patient risk (4). Pembrolizumab, another PD1 monoclonal antibody, has also been approved as first-line treatment in this setting, in association with the TKI axitinib or lenvatinib (5, 6). These new agents, whose mechanism of action is based on anti-tumor immunity enhancing, present a very specific safety profile, resulting in several immune-related adverse events (irAE) whose management is very different from those we were used to (7). Since the first approval of ipilimumab in advanced melanoma in 2011 (8), the knowledge of ICI’s safety profile is evolving rapidly over time consequently to the duration of utilization and the increasing number of tumors in which they are used.
We report the case of a refractory bullous pemphigoid (BP) following nivolumab discontinuation in metastatic ccRCC with durable response.
In 2001, a 58-year-old Caucasian man had radical nephrectomy for pT3N0 ccRCC, Fuhrman grade III. In 2009, lung metastasis was histologically proven. The patient had a favorable risk metastatic ccRCC, according to the IMDC (International Metastatic RCC Database Consortium). He was enrolled in a clinical trial and received a combination of sunitinib and trebananib (AMG 386) – a recombinant fusion protein which neutralizes interaction between angiopoietin-1/2 and its receptor (9). Trebananib was stopped in 2012 for toxicity, and sunitinb was maintained until progression in 2013. The patient was then included in the Checkmate 025 trial (NCT01668784) which compared second line treatment by nivolumab versus everolimus, and received nivolumab.
In April 2014, he presented a single lung injury treated by stereotactic radiation and nivolumab continuation. In 2017, after four years of well-tolerated nivolumab administration, the patient developed pruriginous skin lesions. The histologic analysis of the cutaneous biopsy was compatible with BP. This hypothesis was reinforced by the presence of anti-basal membrane antibodies in the patient’s serum. Oral corticosteroid therapy with prednisone was introduced and then progressively decreased. In May 2020, after seven years of nivolumab administration and perfect disease stability, nivolumab was discontinued and surveillance was proposed. In October 2020, as systemic corticosteroids had been decreased to 10 mg per day, the patient presented new pruriginous skin lesions associated with cutaneous blisters, which biopsy and direct immunofluorescence revealed a junctional bullous auto-immune dermatitis, concordant with the BP diagnosis that had previously been established (Figure 1). Serum analysis revealed anti basal membrane (>80 UR/mL), antiBP180 (27 UR/mL, N <20) and anti BP230 (50 UR/mL, N < 20) antibodies, consistent with this diagnosis. Oral corticosteroid therapy was thus increased, and then very progressively decreased. In October 2021, as anti PD1 had been stopped for more than one year, the patient presented a new BP exacerbation, and oral corticosteroid therapy was reintroduced (60 mg per day), and then replaced by Methotrexate in December 2021. In the meantime, regular follow up of the ccRCC was continued, and computed tomography scan continued to show perfect stability of the disease at the last follow-up in August 2022. BP is relatively controlled by Methotrexate, even if he still presents pruritis than requires prolonged symptomatic treatment (Figure 2).
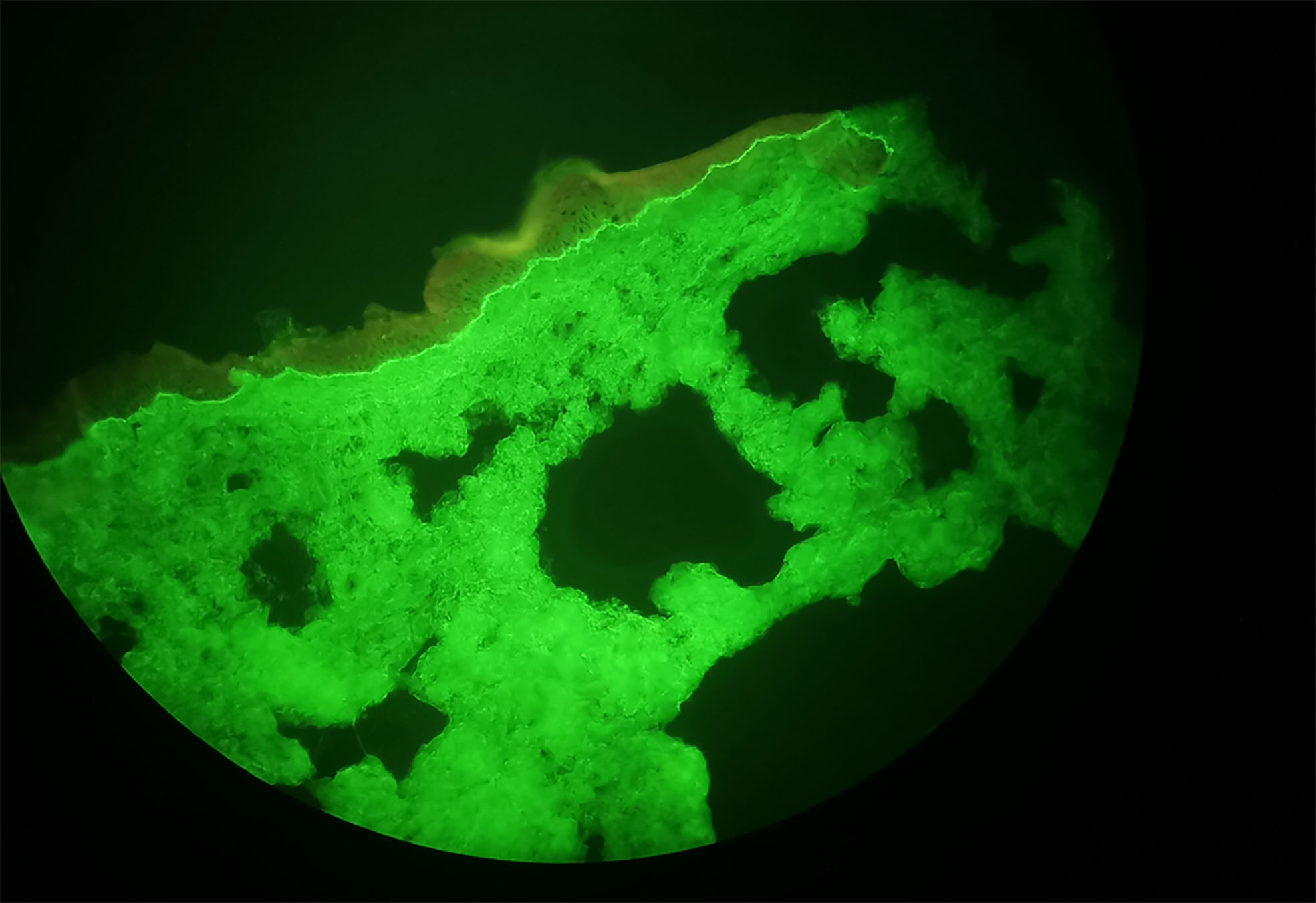
Figure 1 Direct Immunofluorescence consistent with Bullous Pemphigoid Diagnosis.

Figure 2 Diagnosis and Treatments Timeline.
We report the case of a durable disease control even after ICI discontinuation, in a patient treated for a lung metastatic ccRCC for more than twelve years, and who presented a junctional bullous auto-immune dermatitis four years after nivolumab introduction. He had no history of auto-immune disease, and had not taken any other treatment likely to trigger this BP, which suggest that it could be an irAE. He continued to present BP exacerbations despite oral corticosteroid therapy and nivolumab discontinuation for 18 months, and was offered methotrexate treatment, which finally seems to control the BP. To date, his metastatic ccRCC is still perfectly controlled more than two years after nivolumab discontinuation.
The arrival of immunotherapy has profoundly changed our way to manage cancer therapy toxicities, and irAE are now well-known side effects of ICI. In the phase III CheckMate 025 trial, irAE were described in approximately 79% of patients receiving nivolumab for TKI refractory metastatic RCC, with 19% being grade 3 or 4 (2). Pruritus was the second most observed treatment adverse-event (14% of patients), and cutaneous rash was the sixth (10% of patients).
Regardless of the type of cancer, cutaneous toxicities are one of the most common irAE, observed in one third of the treated patients, mainly in the form of pruriginous rash (10). Vitiligo is another well-known cutaneous adverse event, most frequently observed in melanoma but also reported in other cancer types, with an estimated overall incidence of 7,5% for nivolumab (11). The occurrence of vitiligo has been shown to be associated with tumor response to ICI in some cases, especially in melanoma but also in cases of non-small cell lung cancer (NSCLC) or RCC (12–14).
Autoimmune bullous cutaneous disorder, such as BP, are less common cutaneous irAE, but several cases of immune induced BP have been described, especially in melanoma and NSCLC (15).
BP is an acquired skin disorder in which auto antibodies led to subepidermal detachment of the epidermis from the underlying dermis. This results in cutaneous blisters, often preceded by an initial non-bullous phase of pruritus and non-specific maculopapular eruption. Direct immunofluorescence classically shows linear deposits of IgG and C3 at the dermoepidermal junction. Circulating antibodies directed against BP180 and BP230 – two hemidesmosomal structural proteins – may be found in serous samples.
Whereas classic BP is idiopathic, some BP are triggered by drugs such as antibiotics, non-steroidal anti-inflammatory drugs, diuretic, hypoglycemic agents. These drug-induced BP usually resolve after withdrawal of the causative agent (16). Immune-related BP mechanism is unclear, but PD1 pathway’s blockade may increase antibodies production against the hemidesmosomal protein BP180, through a process that may be T-cell and B-cell induced. Some cases of immune related BP associated with tumor response have been described, especially in melanoma and NSCLC (15, 17), but to our knowledge this is the first case of durable disease control associated with BP in RCC. It has been suggested that BP180 may be a common antigen, found both in the dermo-epidermal junction and on the surface of malignant melanocytic tumor cells and NSCLC cells, and that this cross-reactivity between tumor neoantigens and normal tissue antigens may explain the association between immune related BP and tumor response (18, 19). However, we did not find any data concerning BP180 expression by renal cancer cells.
More generally, the association between irAE and efficacy of ICI has already been reported, especially in melanoma, in which a pooled analysis of 576 patients treated with nivolumab for advanced melanoma showed a significant overall response rate improvement in patients who experienced irAE (20). It has also been reported in NSCLC, with improved overall and progression-free survivals in patients who had experienced irAE (21, 22), and this association was particularly reported for immune related thyroid dysfunction, which is consistent with other studies (23, 24). Furthermore, late adverse events might be associated with better response rate and overall survival, as it has been shown in a recent study which compared outcomes in patients with NSCLC and other types of cancer, and showed better outcomes in patients who experienced irAE occurring more than 3 months after ICI initiation, compared to patients whose irAE occurred earlier (25). Concerning RCC, some studies also reported an association between the occurrence of irAE and efficacy of ICI, resulting in improved overall and progression-free survival (26, 27). However, to our knowledge, specific association between cutaneous irAE, and more specifically immune induced bullous disease, has not been reported yet.
For our patient, this cutaneous irAE occurred four years after nivolumab introduction, and lasted even after ICI discontinuation, underlining the fact that irAEs can occur tardily, and that long-lasting irAEs can persist despite ICI discontinuation. Some cases are reported concerning late irAEs that had occurred several months after the introduction of ICI. For example, a case was described concerning a patient treated for a metastatic ccRCC who experienced immune-related renal toxicity after 19 months of nivolumab, and who maintained clinical response even after ICI discontinuation (28). Another patient, treated by nivolumab for platinum refractory laryngeal carcinoma, firstly presented pseudo-progression followed by progressively complete response achieved after 16 courses of nivolumab. A grade 1 interstitial pneumonitis was simultaneously identified, that lead to ICI discontinuation after 18 courses. He then experienced grade 2 immune-related colitis 5 months after ICI discontinuation. Complete response was still maintained 18 months after nivolumab discontinuation (29). Another case was reported concerning a patient who presented reappearance of immune-related colitis one year after ICI discontinuation, underlying the potential of delayed and prolonged alteration of gastro-intestinal immune response (30). These cases underline the fact that irAE can occur after prolonged exposure to ICI, and can last even after ICI discontinuation, suggesting that the PD1 occupancy on T cells could remain for months after ICI exposure (31).
We herein report the case of a refractory BP which occurred four years after nivolumab introduction and lasted despite nivolumab discontinuation in a patient whose metastatic ccRCC is still controlled after more than two years without any anticancer treatment. As previously reported, this could highlight the potential association between irAE and response to ICI. It also underlines the existence of late-onset and long-lasting irAEs even after discontinuation of treatment, which should encourage clinicians to remain vigilant over the long term.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
GG and RM: conception and manuscript writing. RM, MG, CV, JW, NB, GP and GG: final approval. GG, MG and CV: Patient’s management.
The authors acknowledge the patient for allowing us to publish the report of his case.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Escudier B, Porta C, Schmidinger M, Rioux-Leclercq N, Bex A, Khoo V, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2019) 30(5):706–20. doi: 10.1093/annonc/mdz056
2. Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med (2015) 373(19):1803–13. doi: 10.1056/NEJMoa1510665
3. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med (2018) 378(14):1277–90. doi: 10.1056/NEJMoa1712126
4. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med (2021) 384(9):829–41. doi: 10.1056/NEJMoa2026982
5. Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med (2019) 380(12):1116–27. doi: 10.1056/NEJMoa1816714
6. Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med (2021) 384(14):1289–300. doi: 10.1056/NEJMoa2035716
7. Champiat S, Lambotte O, Barreau E, Belkhir R, Berdelou A, Carbonnel F, et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol (2016) 27(4):559–74. doi: 10.1093/annonc/mdv623
8. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med (2010) 363(8):711–23. doi: 10.1056/NEJMoa1003466
9. Atkins MB, Gravis G, Drosik K, Demkow T, Tomczak P, Wong SS, et al. Trebananib (AMG 386) in combination with sunitinib in patients with metastatic renal cell cancer: An open-label, multicenter, phase II study. J Clin Oncol (2015) 33(30):3431–8. doi: 10.1200/JCO.2014.60.6012
10. Sibaud V. Dermatologic reactions to immune checkpoint inhibitors. Am J Clin Dermatol (2018) 19(3):345–61. doi: 10.1007/s40257-017-0336-3
11. Dai J, Belum VR, Wu S, Sibaud V, Lacouture ME. Pigmentary changes in patients treated with targeted anticancer agents: A systematic review and meta-analysis. J Am Acad Dermatol (2017) 77(5):902–910.e2. doi: 10.1016/j.jaad.2017.06.044
12. Hua C, Boussemart L, Mateus C, Routier E, Boutros C, Cazenave H, et al. Association of vitiligo with tumor response in patients with metastatic melanoma treated with pembrolizumab. JAMA Dermatol (2016) 152(1):45–51. doi: 10.1001/jamadermatol.2015.2707
13. Billon E, Walz J, Brunelle S, Thomassin J, Salem N, Guerin M, et al. Vitiligo adverse event observed in a patient with durable complete response after nivolumab for metastatic renal cell carcinoma. Front Oncol (2019) 9:1033. doi: 10.3389/fonc.2019.01033
14. Uenami T, Hosono Y, Ishijima M, Kanazu M, Akazawa Y, Yano Y, et al. Vitiligo in a patient with lung adenocarcinoma treated with nivolumab: A case report. Lung Cancer (2017) 109:42–4. doi: 10.1016/j.lungcan.2017.04.019
15. Naidoo J, Schindler K, Querfeld C, Busam K, Cunningham J, Page DB, et al. Autoimmune bullous skin disorders with immune checkpoint inhibitors targeting PD-1 and PD-L1. Cancer Immunol Res (2016) 4(5):383–9. doi: 10.1158/2326-6066.CIR-15-0123
16. Vassileva S. Drug-induced pemphigoid: bullous and cicatricial. Clin Dermatol (1998) 16(3):379–87. doi: 10.1016/S0738-081X(98)00008-X
17. Rofe O, Bar-Sela G, Keidar Z, Sezin T, Sadik CD, Bergman R. Severe bullous pemphigoid associated with pembrolizumab therapy for metastatic melanoma with complete regression. Clin Exp Dermatol (2017) 42(3):309–12. doi: 10.1111/ced.13042
18. Krenacs T, Kiszner G, Stelkovics E, Balla P, Teleki I, Nemeth I, et al. Collagen XVII is expressed in malignant but not in benign melanocytic tumors and it can mediate antibody induced melanoma apoptosis. Histochem Cell Biol (2012) 138(4):653–67. doi: 10.1007/s00418-012-0981-9
19. Papay J, Krenacs T, Moldvay J, Stelkovics E, Furak J, Molnar B, et al. Immunophenotypic profiling of nonsmall cell lung cancer progression using the tissue microarray approach. Appl Immunohistochem Mol Morphol (2007) 15(1):19–30. doi: 10.1097/01.pai.0000213143.32030.f5
20. Weber JS, Hodi FS, Wolchok JD, Topalian SL, Schadendorf D, Larkin J, et al. Safety profile of nivolumab monotherapy: A pooled analysis of patients with advanced melanoma. J Clin Oncol (2017) 35(7):785–92. doi: 10.1200/JCO.2015.66.1389
21. Haratani K, Hayashi H, Chiba Y, Kudo K, Yonesaka K, Kato R, et al. Association of immune-related adverse events with nivolumab efficacy in non-Small-Cell lung cancer. JAMA Oncol (2018) 4(3):374–8. doi: 10.1001/jamaoncol.2017.2925
22. Grangeon M, Tomasini P, Chaleat S, Jeanson A, Souquet-Bressand M, Khobta N, et al. Association between immune-related adverse events and efficacy of immune checkpoint inhibitors in non-small-cell lung cancer. Clin Lung Cancer (2019) 20(3):201–7. doi: 10.1016/j.cllc.2018.10.002
23. Osorio JC, Ni A, Chaft JE, Pollina R, Kasler MK, Stephens D, et al. Antibody-mediated thyroid dysfunction during T-cell checkpoint blockade in patients with non-small-cell lung cancer. Ann Oncol (2017) 28(3):583–9. doi: 10.1093/annonc/mdw640
24. Kim HI, Kim M, Lee SH, Park SY, Kim YN, Kim H, et al. Development of thyroid dysfunction is associated with clinical response to PD-1 blockade treatment in patients with advanced non-small cell lung cancer. Oncoimmunology (2017) 7(1):e1375642. 10.1080/2162402X.2017.1375642
25. Hsiehchen D, Naqash AR, Espinoza M, Von Itzstein MS, Cortellini A, Ricciuti B, et al. Association between immune-related adverse event timing and treatment outcomes. Oncoimmunology (2022) 11(1):2017162. doi: 10.1080/2162402X.2021.2017162
26. Elias R, Yan F, Singla N, Levonyack N, Formella J, Christie A, et al. Immune-related adverse events are associated with improved outcomes in ICI-treated renal cell carcinoma patients. JCO (2019) 37(7_suppl):645–5. doi: 10.1200/JCO.2019.37.7_suppl.645
27. Ishihara H, Takagi T, Kondo T, Homma C, Tachibana H, Fukuda H, et al. Association between immune-related adverse events and prognosis in patients with metastatic renal cell carcinoma treated with nivolumab. Urol Oncol (2019) 37(6):355.e21–355.e29. doi: 10.1016/j.urolonc.2019.03.003
28. Pesola G, Murianni V, Rebuzzi SE, Banna GL, Cerbone L, Catalano F, et al. Durable response after immunotherapy discontinuation for delayed and severe immune-related adverse events: A case report. Immunotherapy (2021) 13(17):1379–86. doi: 10.2217/imt-2021-0085
29. Kondo T, Nakatsugawa M, Okubo M, Nakamura H, Yunaiyama D, Wakiya M, et al. Laryngeal cancer with lung metastases showing long-term complete response and delayed immune-related adverse event after nivolumab discontinuation. Ear Nose Throat J (2021), 1–6. doi: 10.1177/01455613211031025
30. Horisberger K, Portenkirchner C, Rickenbacher A, Biedermann L, Gubler C, Turina M. Long-term immune-related adverse events after discontinuation of immunotherapy. Immunotherapy (2021) 13(9):735–40. doi: 10.2217/imt-2020-0320
31. Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol (2010) 28(19):3167–75. doi: 10.1200/JCO.2009.26.7609
Keywords: renal cell carcinoma, immunotherapy, bullous pemphigoid, durable response, late adverse event
Citation: Mari R, Guerin M, Vicier C, Walz J, Bonnet N, Pignot G and Gravis G (2022) Durable disease control and refractory bullous pemphigoid after immune checkpoint inhibitor discontinuation in metastatic renal cell carcinoma: A case report. Front. Immunol. 13:984132. doi: 10.3389/fimmu.2022.984132
Received: 01 July 2022; Accepted: 02 September 2022;
Published: 16 September 2022.
Edited by:
Fiona Simpson, The University of Queensland, AustraliaReviewed by:
Melih Simsek, Bezmiâlem Vakıf Üniversitesi, TurkeyCopyright © 2022 Mari, Guerin, Vicier, Walz, Bonnet, Pignot and Gravis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roxane Mari, bWFyaXJAaXBjLnVuaWNhbmNlci5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.