
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol., 27 October 2022
Sec. Cancer Immunity and Immunotherapy
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.970823
This article is part of the Research TopicExpert Opinions and Perspectives in Immune checkpoint inhibitors for cancer: 2022View all 5 articles
 Manuel Olmos1,2,3
Manuel Olmos1,2,3 Rainer Lutz1,2,3
Rainer Lutz1,2,3 Tjark-Ole Büntemeyer1,2,3Jacek Glajzer1,2,3Christopher-Philipp Nobis1,2,3
Tjark-Ole Büntemeyer1,2,3Jacek Glajzer1,2,3Christopher-Philipp Nobis1,2,3 Jutta Ries1,2,3Tobias Möst1,2,3
Jutta Ries1,2,3Tobias Möst1,2,3 Markus Eckstein2,4
Markus Eckstein2,4 Markus Hecht2,3,5
Markus Hecht2,3,5 Antoniu-Oreste Gostian2,3,6
Antoniu-Oreste Gostian2,3,6 Michael Erdmann2,3,7Yannick Foerster1,2,3
Michael Erdmann2,3,7Yannick Foerster1,2,3 Marco Kesting1,2,3
Marco Kesting1,2,3 Manuel Weber1,2,3*
Manuel Weber1,2,3*Background: Prognosis of patients with recurrent or metastatic head and neck cancer is generally poor. Adjuvant immunotherapy (IT) featuring immune checkpoint inhibition (ICI) is standard of care in advanced stage head and neck squamous cell carcinoma (HNSCC) and cutaneous squamous cell carcinoma (CSCC). ICI response rates in CSCC are described as higher than in HNSCC. IT is constantly shifting into earlier disease stages which confronts the surgeon with immunotherapeutically pre-treated patients. It is therefore becoming increasingly difficult to assess which patients with symptomatic tumor disease and a lack of curative surgical option might benefit from salvage surgery.
Case presentations: The following 6 cases describe therapeutic decision-making regarding ICI and (salvage) surgery in patients with advanced stage HNSCC or CSCC. Cases A and B focus on neoadjuvant ICI followed by salvage surgery. In Cases C and D salvage surgery was performed after short-term stabilization with partial response to ICI. The last two cases (Cases E and F) address the surgical approach after failure of ICI. All cases are discussed in the context of the current study landscape and with focus on individual decision-making. For better understanding, a timetable of the clinical course is given for each case.
Conclusions: ICI is rapidly expanding its frontiers into the neoadjuvant setting, frequently confronting the surgeon with heavily pretreated patients. Salvage surgery is a viable therapeutic concept despite the rise of systemic treatment options. Decision-making on surgical intervention in case of a salvage surgery remains an individual choice. For neoadjuvant ICI monitoring regarding pathological tumor response or tumor necrosis rate, we suggest correlation between the initial biopsy and the definite tumor resectate in order to increase its significance as a surrogate marker. Scheduling of neoadjuvant ICI should be further investigated, as recent studies indicate better outcomes with shorter time frames.
Incidence rates for head and neck cancer have decreased in recent decades for laryngeal and nasopharyngeal cancer, while they have increased for oral/hypopharyngeal cancer and lip/oral cavity cancer (1). The prognosis of patients with recurrent or metastatic (R/M) HNSCC is generally poor and treatment often associated with high morbidity (2). Primary’s grading, margins and lymph node ratio significantly influence risk of recurrence which occurs in more than half of advanced stage patients (stage III or IV) within 3 years of definitive treatment (2–4). Therefore, the search for innovative treatment options in advanced cases is becoming more and more important. To date, surgical tumor resection and neck dissection combined with radio(chemo)therapy are considered the most effective treatments options for HNSCC in advanced cases (5). In case of locoregional recurrence, salvage surgery or re-irradiation are available (6, 7). The introduction of immunotherapy (IT) featuring immune checkpoint inhibition (ICI) recently provided a further treatment option for advanced solid cancers, including HNSCC (8). As of now, immunotherapy in the recurrent or metastatic (R/M) setting is generally characterized by relatively low response rates of 13.3%, compared with response rates of up to 44% reported for neoadjuvant treatment (9–13). Timing and scheduling of ICI might be crucial for therapy outcome. In this regard, several preclinical and clinical studies indicate that ICI might be more effective at earlier disease states (14–16). Additionally, experimental studies demonstrate that immune responses in the head and neck area are reduced after cervical lymph node dissection (17). For HNSCC neoadjuvant immunotherapeutic treatment is under intense investigation in large clinical trials (NCT03708224, NCT03129061, and NCT03944915). In particular checkmate-141 and KEYNOTE-048 were practice changing trials resulting in the approval of Nivolumab and Pembrolizumab (PD-L1 CPS≥ 1) as first line therapy for patients with R/M HNSCC (9, 18). Completed and published phase II studies describe neoadjuvant use of Pembrolizumab as safe, reporting pathologic response in 44% of patients and a lower 1-year relapse rate compared to historical in patients with high-risk pathology (11, 12). The result of the consecutive phase III study (Keynote-689, NCT03765918) is pending and highly anticipated. Given the current study landscape, a paradigm shift from induction chemotherapy to neoadjuvant ICI may soon occur (19–21).
Cutaneous squamous cell carcinoma (CSCC) is the second most common skin cancer and has seen rising incidence in recent years (22, 23). Many factors are known to increase the risk of CSCC, with cumulative sun exposure being of greatest importance, leading to CSCC developing predominantly in the head-and-neck area (24). In addition, immunosuppression is known to play an important role in the development of CSCC (25, 26). Most cases are cured by complete surgical excision (27, 28). However, a substantial number of patients subsequently develop either metastatic or locally advanced CSCC not amenable to curative surgery or curative radiotherapy. For better understanding, these cases are referred to as advanced CSCC in the following. According to the National Comprehensive Cancer Network (NCCN) Guidelines V2.2021, systemic ICI with Cemiplimab or Pembrolizumab is recommended only for complicated cases of advanced CSCC when curative radiotherapy or surgery is not available (28). Regarding neoadjuvant ICI for CSCC of the head and neck, recently published Phase II trial results report that administration is safe. Complete pathologic response (cPR) was observed in 55% of the patients with additional 15% of patients showing major pathologic response (MPR, 10% viable tumor) (29, 30). Interestingly, response rates are described as higher compared to ICI in HNSCC (31–33).
In highly advanced or recurrent cases of both HNSCC and CSCC and at the transition from the curative to the R/M setting salvage surgery can be considered as an alternative or addition to re-irradiation in selected cases (34, 35). With an increasing number of long-term responders on immunotherapy in the R/M setting there is a growing number of patients with tumor-derived symptoms and quest for surgical intervention. In addition, ICI is constantly shifting to earlier stages of disease, confronting the surgeon with immunotherapeutically pre-treated patients. In the context of this development, it is becoming increasingly difficult to assess which patients with symptomatic tumor disease and no curative surgical option could benefit from salvage surgery.
Individual decision-making for surgical therapy in the context of IT using ICI will be discussed on the basis of the following 6 cases. In addition, we will provide a review of the current literature in order to facilitate future therapeutic decisions for surgeons.
PubMed and Scopus were comprehensively searched in January 2022 using the keywords HNSCC, cSCC, immunotherapy and salvage surgery. The individual keywords HNSCC and cSCC were combined with immunotherapy and salvage surgery. It was then updated in February 2022 and limited to a publication date within the last 15 years. The search returned 18 results on PubMed, 6 on Scopus. Subsequently, the results were supplemented by a manual search. For better comprehension, a table of current human studies on neoadjuvant immunotherapy of HNSCC is attached (Table 1).
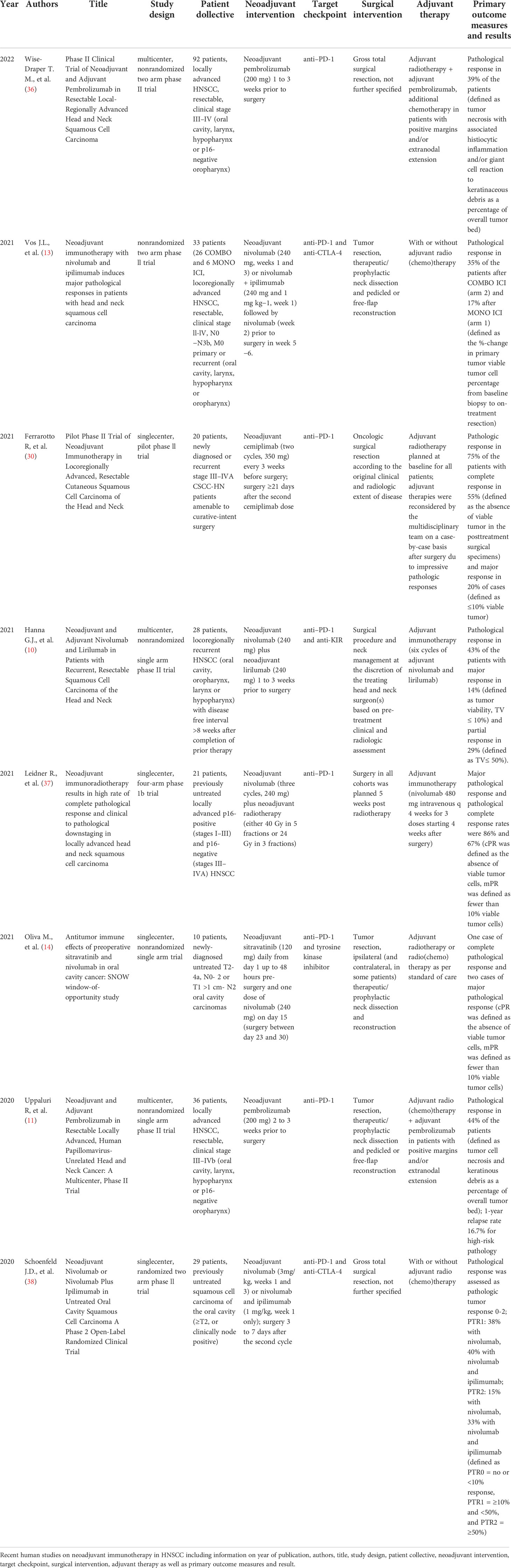
Table 1 Human studies on neoadjuvant Immunotherapy in HNSCC.
The following two cases describe successful combination of neoadjuvant ICI and salvage surgery:
Patient A presented at the end of October 2021 with pain in the right maxilla and restricted mouth opening. Subsequent computed tomography (CT) and biopsy confirmed the diagnosis OSCC of the left maxilla (cT4b cN1; HPV/p16 negative). Immunohistochemical staining of the biopsy revealed a tumor proportion score (TPS, stained tumor cells/tumor cells) of 15%, inflammatory cell score (IC-Score, stained inflammatory cells/tumor surface) of 0,5% and a combined positive score (CPS, (stained tumor cells + stained mononuclear immune cells)/tumor cells)) of 15. A single dose of Pembrolizumab 200 mg was administered on October 2021, 15 days prior to surgery. Operation included radical tumor resection with lip-split mandibulotomy as demonstrated in Figures 1A, B, and bilateral selective neck dissection level I-V left and I-III right (Figure 1C). CAD-CAM assisted (Figure 1D) microvascular reconstruction was used for defect coverage. Pathological assessment revealed: ypT4a pN1 (1/63) L0 V0 Pn0with positive margins to the medial maxillary sinus wall (70% vital tumor cells, 30% regressive change; pathologic tumor response (pTR) can therefore be classified as pTR-1 (10%-49%) (11)). Subsequently, immunohistochemical assessment of the tumor mass was performed. Methods were identical to our previously published case report on neoadjuvant IT (39). A significant factor increase was observed in TPS, IC-Score, CPS and immune cell infiltration (CD8/mm2), comparing initial biopsy and final tumor resection (Figures 2A–D). Adjuvant RCT was recommended by the tumor board starting in February 2022. Last follow-up took place in early-April 2022 and showed no signs of tumor recurrence (Figure 1E).
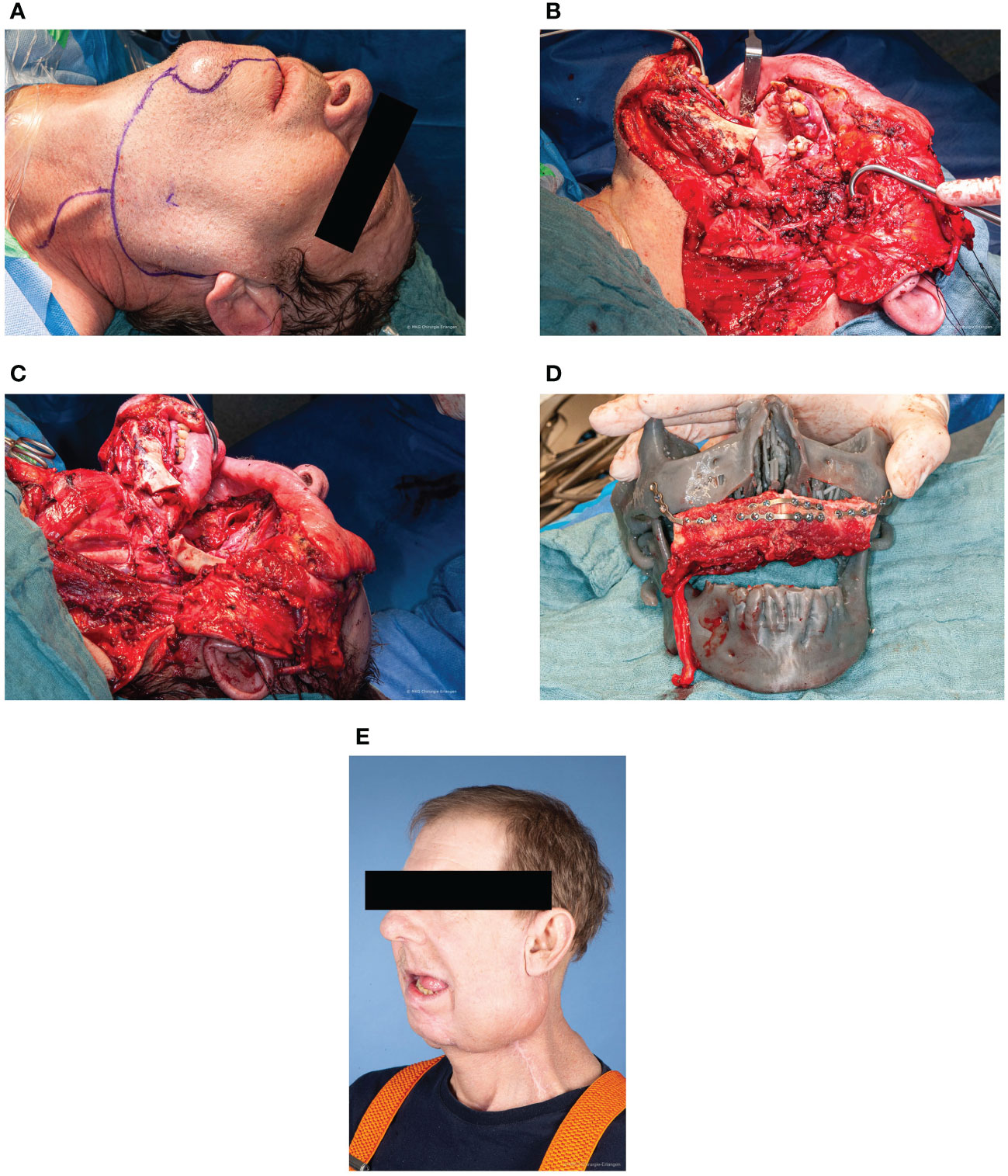
Figure 1 Case A (A) Preoperative sketching of the surgical incision. Photo taken under intubation anaesthesia. Preauricular and submandibular approach with temporary lip-split mandibulotomy. (B) Intraoperative view of the tumor on the left maxilla. Situs after successful access via preauricular and submandibular with temporary lip-split mandibulotomy with view of the tumor in the maxilla. (C) Intraoperative view after bilateral neck dissection and radical tumor resection. Neck dissection level I-V left and I-III right with vascular presentation on both sides. Radical tumor resection by way of bilateral maxillectomy. (D) CAD-CAM assisted microvascular double flap reconstruction. In domo planned and printed surgical model for sagittal positioning of the microvascular 2-segment fibula transplant. An additional microvascular latissimus dorsi graft was used for enoral soft tissue reconstruction. (E) Last follow-up in early-April 2022 - 5 months postoperative. No signs of tumor recurrence. Functionally satisfying rehabilitation with good mouth opening.
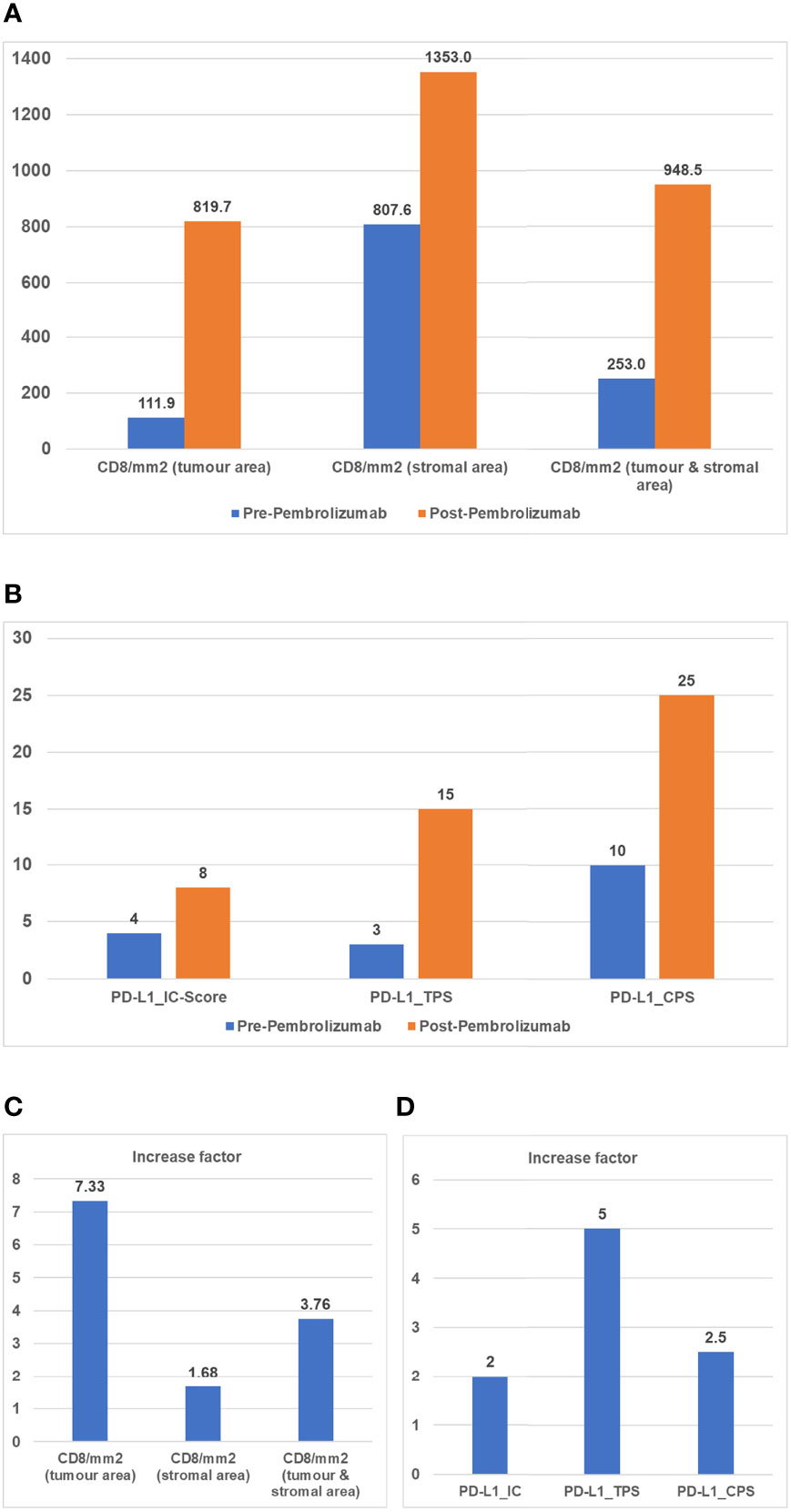
Figure 2 (A) CD8 density (mm2) (Cytotoxic T cell marker) during treatment. Points of interest/sample collection: initial biopsy (blue); final resection after Pembrolizumab (orange). Charts show: CD8+ cells per mm2 in tumor area; CD8+ cells per mm2 in stroma area; CD8 mm2 combined tumor and stroma area. (B) Immune scores during treatment. Points of interest/sample collection: initial biopsy (blue); final resection after Pembrolizumab (orange). Charts show: TC, tumor cells; TPS, tumor proportion score (stained tumor cells/tumor cells); IC-Score, inflammatory cell score (stained inflammatory cells/tumor surface); CPS, combined positivity score [(stained tumor cells + stained mononuclear immune cells)/tumor cells]. (C) Increase factor in CD8 density (mm2). Increase factor between initial biopsy and final resection in terms of CD8/mm2 tumor area, CD8/mm2 stromal area and CD8/mm2 tumor and stromal area. (D) Increase factor in Immune scores. Increase factor between initial biopsy and final resection in terms of immune scores. IC-Score, inflammatory cell score (stained inflammatory cells/tumor surface); TPS, tumor proportion score (stained tumor cells/tumor cells); CPS, combined positivity score [(stained tumor cells + stained mononuclear immune cells)/tumor cells].
Patient B presented with OSCC of the right mandible in early January 2021. In detail, histopathological examination resulted in focally moderately differentiated squamous cell carcinoma with extensive necrosis. Staging CT revealed multiple ipsilateral lymph node metastases at level 1-5 (40), partial contact (> 180°) with the internal carotid artery at the skull base and metastasis in the right upper lobe of the lung; cT4a N3b M1 (HPV/p16 negative). Neoadjuvant ICI (TPS 100%, IC 0.5%, CPS 100) was administered in mid-January with Pembrolizumab 200 mg, 17 days prior to surgery. Preoperative restaging after neoadjuvant therapy revealed local tumor progression and predominantly size-progressive necrotic lymph nodes in level I-IV on the right. Surgery took place at the beginning of February including partial mandibulectomy, bilateral level I-V neck dissection and microvascular flap reconstruction. Histologic assessment confirmed clear margin resection for OSCC ypT4a pN3b (7/41) L0 V0 Pn0 [40% vital tumor cells, 60% regressive change; pTR-2 (≥50%) (11)]. Postoperative CT to clarify an atypical awakening process showed multifocal cerebral infarcts with proximal complete occlusion of the right external carotid artery the patient was transferred to the intensive care unit of the neurology department for early neurological rehabilitation. After significant improvement of the general condition, adjuvant radiotherapy (64 Gy total dose) was initiated in June 2021. The last follow-up took place in late-February 2022 and showed no signs of tumor recurrence.
The occurrence of peri-/postoperative cerebrovascular apoplexy following neoadjuvant ICI in Case B is not considered a side effect of IT, but a general complication due to the length and complexity of surgery.
The following two cases describe the combined administration and feasibility of ICI and salvage surgery in the R/M setting. Surgery was performed after partial response to ICI or delay of tumor progression:
The patient was initially treated with a squamous cell carcinoma of the left oropharynx in mid-2014 by primary RCT (72 Gy total dose; cisplatin and 5-FU). Mid-2017, OSCC of the left buccal area was diagnosed. It was treated surgically by resection and microvascular flap reconstruction as well as bilateral neck dissection due to radiologically enlarged cervical lymph nodes (pT1 pN0 G2 R0; HPV/p16 negative). Adjuvant therapy was not carried out. In late-2018, the patient was diagnosed with bladder cancer which was treated by primary surgical resection (pT2 G3) and adjuvant RCT (59 Gy total dose; carboplatin and 5-FU). Shortly afterwards, biopsy of the left maxillary premolar area and buccal mucosa revealed recurrence of OSCC (rcT4 rcN2b cM0 G2). The patient was treated by definitive RCT (66 Gy and carboplatin+5-FU). Due to overall poor prognosis of re-irradiation in advanced OSCC/HNSCC this was followed by four months of ICI with Pembrolizumab 200mg (TPS 2%, IC 3%, CPS 5). After four months and initial improvement of the clinical condition, systemic therapy was switched from Pembrolizumab to Paclitaxel and Cetuximab due to tumor progression. The patient’s clinical condition progressively deteriorated, with abscess and multiple skin fistulas on the left paramandibular side due to cutaneous metastasis (Figure 3A). In order to improve the clinical condition, the decision was made to carry out salvage surgery. Tumor resection with hemimandibulectomy and partial resection of the left buccal region/maxilla was performed (Figure 3B) followed by microvascular flap reconstruction (Figure 3C). Histology revealed a tumor mass of approximately 6.5 cm poorly differentiated OSCC with bone infiltration (rpT4a L0 V0 Pn0 G3 R0). Close margin resection with minimal 0.2 cm margins was achieved. Despite close margin resection, CT in January 2021 showed early local recurrence and multiple predominantly new bi-pulmonary consolidations. The patient died of tumor-toxic multi-organ failure in April 2021.
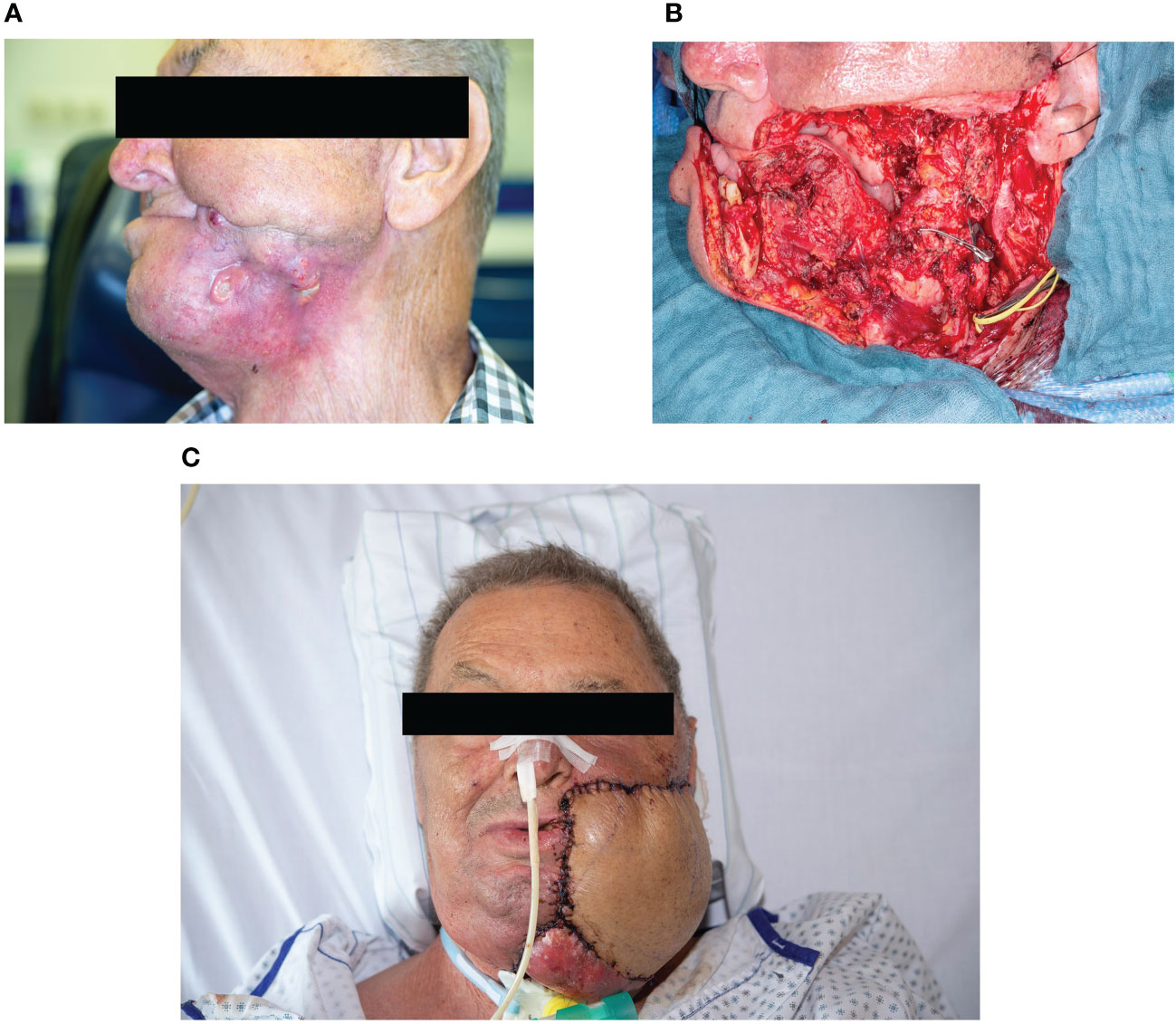
Figure 3 Case C (A) Abscess and multiple skin fistulas on the left paramandibular side due to cutaneous metastasis under IT. Photo taken during tumor aftercare from the left-hand side. (B) Salvage surgery. Tumor resection with hemimandibulectomy of the left side and partial resection of the left buccal region/maxilla. (C) Reconstruction with two microvascular grafts. Microvascular double flap reconstruction with anterior lateral thigh and latissimus dorsi flap.
After resection and radiotherapy of multiple CSCC of the head and neck region from 2008 to 2019, Patient D presented with field changes of the scalp in Mai 2019. In August 2019, ICI was initiated with palliative intent by administration of 2 doses of Cemiplimab by the Department of Dermatology. In the course, regression of all lesions was observed except for one parietal and one lateral-cervical lesion. The interdisciplinary tumor board recommended salvage surgery to treat the persistent lesions. Salvage surgery took place in September 2019 by radical tumor resection and microvascular flap reconstruction. Subsequent histology revealed ulcerated, poorly differentiated cutaneous squamous cell carcinoma (cervical R0, parietal R1). The postoperative result was found to be aesthetically and functionally good. Due to progression of lesions of other localization and R1 resection of the parietal lesion, experimental use of intralesional mRNA TLR agonist was decided as part of the CureVac trial (cohort A, NCT03291002). The administration took place from November 2019 to February 2020. After discontinuation of IT due to further progress, an extensive recurrence of the outer skin occipital-left measuring 7 cm with arrosion of the skull calvaria and the dura mater as well as an in-transit metastasis was diagnosed in May 2021 (Figure 4A). Salvage surgery with was performed in June 2021 by radical tumor resection including resection of the calvarium and dura mater and defect coverage with a microvascular flap in collaboration with the Department of Neurosurgery (rpT3 rpN0 L0 V0 G3 Pn0) (Figures 4B, C). Last CT and tumor aftercare in August 2021 showed no signs of recurrence (Figures 4D, E). Further aftercare takes place close to home according to patient’s choice.
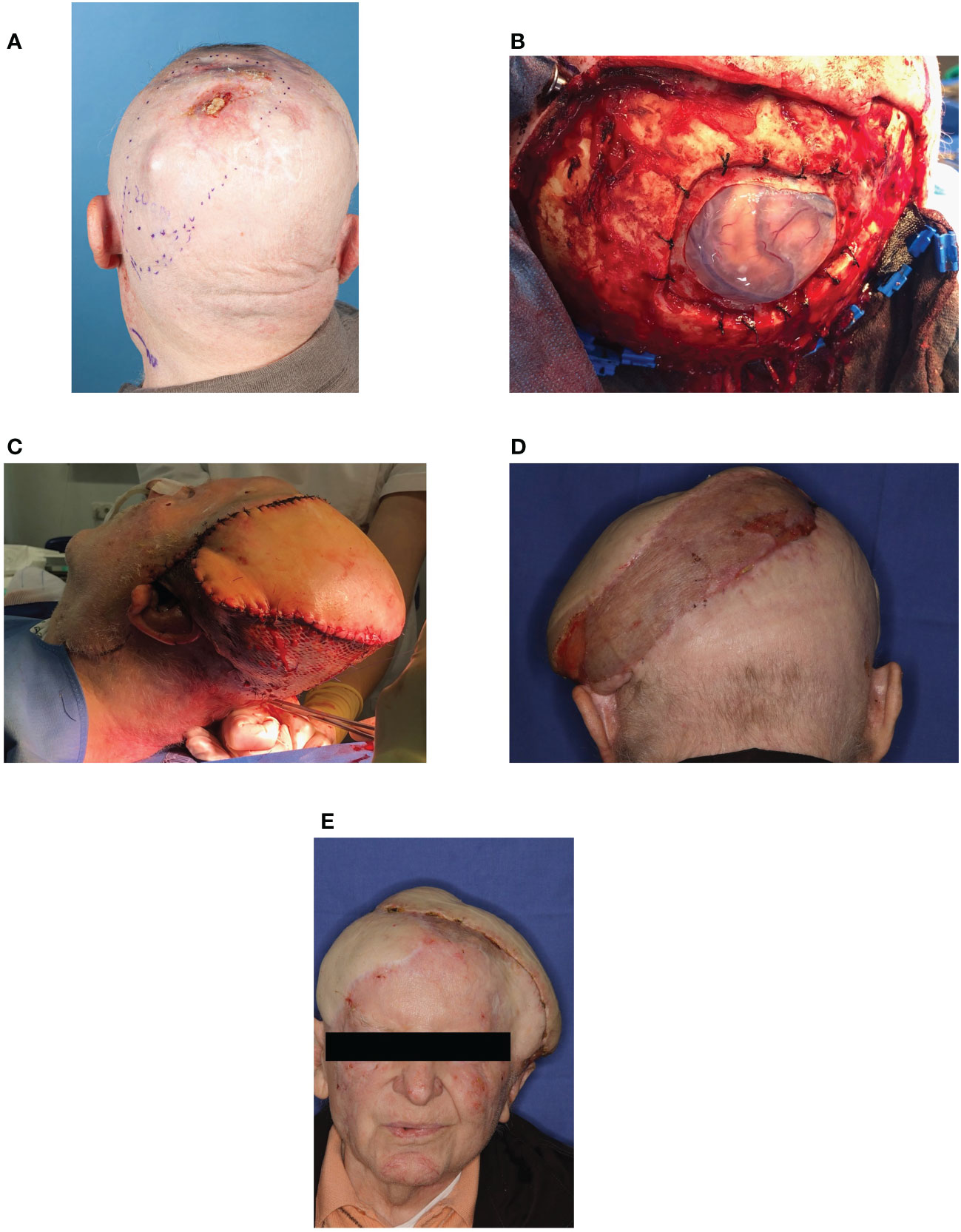
Figure 4 Case D (A) Recurrence of the outer skin with in-transit metastasis. Extensive recurrence of the outer skin located occipital-left and measuring 7 cm with arrosion of the skull calvaria and the dura mater as well as an in-transit metastasis. (B) Salvage surgery. Salvage surgery with palliative intent by radical tumor resection including resection of the calvarium and dura mater. (C) Reconstruction with microvascular graft. Defect coverage with a microvascular latissimus dorsi graft in collaboration with the Department of Neurosurgery. (D) Last follow-up in August-2021 - 2 months postoperative. No signs of tumor recurrence. Further follow-up care takes place near home at the patient’s request. (E) For further information see Figure 4D.
The following two cases describe the implementation of salvage surgery after failure of (chemo/radio-) immunotherapy:
Patient E presented in mid-May 2017 with OSCC of the left floor of the mouth. In late May 2017, primary surgical therapy was performed by means of partial mandibulectomy, floor of the mouth reconstruction and level I-III right and I-V left neck dissection (pT2 pN0 (0/37) L0 V0 Pn0 cM0 with close margins; HPV/p16 negative). Re-resection due to close margins was performed shortly after. Postoperative interstitial brachytherapy with 50 Gy total dose was administered. In early March 2018, CT scan revealed urgent suspicion of a recurrence with pharyngeal location close to the ramus mandibulae. Biopsy showed a poorly differentiated basaloid squamous cell carcinoma (G3). The interdisciplinary tumor board decided on a primary RCT starting at the end of June with a total dose of 50.4 Gy and 5-FU as well as cisplatin due to possible infiltration of the prevertebral fascia. Staging-CT 4 months after RCT initiation showed size regressive oropharyngeal carcinoma however multiple new lymph node and lung metastases which were subsequently treated by stereotactic radiation with 36 Gy total dose. Due to the generally poor prognosis with re-irradiation, additional IT with Pembrolizumab was initiated in November 2018. Based on a significant deterioration of the clinical condition with strong growth of submental and submandibular metastases under IT, palliative resection of metastases and microvascular flap reconstruction was performed in February 2019. Immunotherapy was continued. The patient died 4 months later with unknown cause of death.
In April 2019 Patient F presented with G3 OSCC of the tongue base (cT4a cN3b cM0; HPV/p16 negative). Induction chemo-immunotherapy was initiated as part of the CheckRad-CD8 study (NCT03426657) (41); for exact schedule see Table 2f. Four weeks after completion of therapy, control FDG-PET/CT revealed a tongue base carcinoma that had progressed in size and metabolism under induction chemo-immunotherapy, as well as progressive lymph node metastases. Based on tumor progression, tumor board decided on a salvage surgical procedure. At the end of June, partial mandibulectomy, bilateral neck dissection level I-V and subsequent reconstruction was carried out by an interdisciplinary team of ENT and maxillofacial surgeons (ypT4a ypN3b (2/77) cM0 L1 V0 Pn1 with close margins). In addition, and due to close margin resection, adjuvant RCT with 60 Gy total dose and cisplatin/5-FU was administered from early August to early November 2019. The follow-up CT at the beginning of December showed no local recurrence of the floor of the mouth, but three pulmonary foci of progressive size. After close follow-up, it was decided in mid-February 2020 to repeat chemotherapy according to the TPExtreme regimen (Table 2f) due to strong progression of pulmonary metastasis. Further progression of lung lesions with cavern formation was diagnosed in February 2021. Supportive-palliative procedure was recommended and carried out near home.
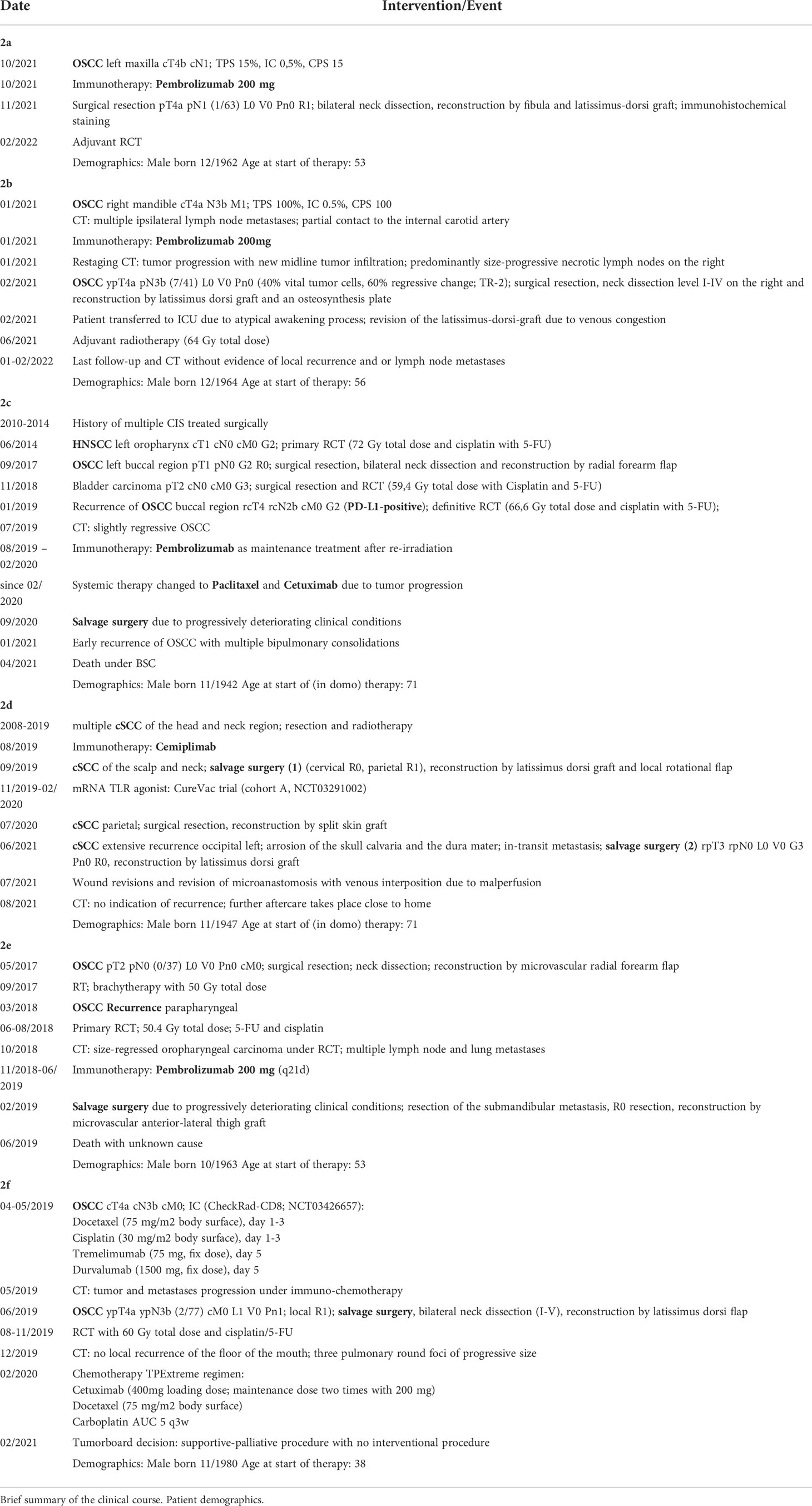
Table 2 Time history.
Apart from those described, no ADRs occurred over the course of the cases described.
Cases A and B, as well as our previously published case report on neoadjuvant immunotherapy (39), show that neoadjuvant ICI can be performed successfully and should be evaluated in selected cases. Nevertheless, the optimal timing for neoadjuvant ICI remains unclear. Uppaluri et al. recommend a time frame of 13-22 days prior to surgery (11). In the ongoing and highly anticipated Keynote-689 trial, Pembrolizumab 200 mg is administered on day 1 of a 21-day cycle for 2 cycles (NCT03765918). Regarding our cases, Pembrolizumab 200 mg was given 15 (Case A), 17 (Case B) and 19 days (39) before surgery. – Reason was not to delay the planned surgery and to stick to the seemingly biologically reasonable time frame given in the literature available at the time (11). Recently, Liu et al. investigated the sole timing of ICI in relation to resection of the primary tumor and its impact on the efficacy of ICI in an animal study. First step was to demonstrate the significantly greater therapeutic efficacy of neoadjuvant compared to adjuvant ICI to eradicate distant metastases following primary tumor resection of breast cancer. Different metastatic burden at the time of treatment was eliminated as a factor by varying the schedule of neoadjuvant and adjuvant ICI administration. Furthermore, investigation on the optimal scheduling between neoadjuvant immunotherapy and surgery showed that short duration (4-5 days instead of 10 days) between first administration of neoadjuvant ICI and resection of the primary tumor yielded in optimal results in overall and relapse-free survival. Interestingly, adding 4 adjuvant doses had no benefit on overall survival and instead lead to an increase in immune related adverse events (15, 16). Comparing the studies described in Table 1 regarding the publication date and the administration period, it can be observed that more recent studies, e.g. Wise-Draper et al. (36) work according to a shorter administration schedule as described by Liu et al. (16).
Although timing of neoadjuvant ICI differed significantly from the optimal administration schedule proposed by Liu et al. (16), all cases presented, as well as the previously published case, can be classified as pTR-2 9 [Cases B and (39)] or pTR-1 (Case A) according to the histologic response classification proposed by Uppaluri et al. (11). PTR ≥1 correlates with better clinical outcome, as shown by the aforementioned author (11).
To date, all studies on neoadjuvant ICI in OSCC/HNSCC consider pathological tumor response as an important target criterion for response to therapy. How reliable and feasible is this surrogate marker in the context of other available outcome criteria such as overall survival, immune cell infiltration and radiological response?
In a recently published review, Menzies et al. report high pathological and radiological response rates with impressive recurrence-free survival (RFS) and OS with neoadjuvant therapy in melanoma. The degree of pTR was found to strongly correlate with RFS and OS, allowing the early endpoint to be used as a surrogate marker for survival in future clinical trials (42). This statement is in line with Uppaluri et al. who suggest pTR as a biomarker for response to neoadjuvant ICI and a lower rate of disease relapse (11). The hypothesis is currently being tested in an ongoing phase III trial (NCT03765918). Additionally, pTR seems to be associated with tumor PD-L1 expression and high disease-free survival (DFS) in intermediate-risk patients as stated by Wise-Draper et al. (36, 43). Although Menzies et al. report a correlation between radiological and pathological response, radiological response seems to be inconsistent and unsuitable as a marker for neoadjuvant therapy due to the short time frame and the possibility of radiologic flare as stated by Leidner et al. (37, 42, 44). A recent study by Vos et al. proposes [18F] FDG-PET for pathological response assessment in early neoadjuvant ICI, however radiological flare is also present in PET-CT (45). Regardless, it should be considered that ICI’s effect on the primary tumor site and on potential lymph node metastases may differ (46). Besides radiological and pathological response, the role of immune biomarkers and circulating tumor DNA (ctDNA) seems to be emerging for the assessment of (neoadjuvant) ICI. PD-L1 immune cell area and intratumoral CD8+ cell density have previously been identified as significant positive predictors of pathologic complete response (pCR) (41, 47). Interestingly, the immunohistochemical assessment of Case A showed a strong increase in all immunohistochemical parameters examined, including immune cell infiltration (Figures 4A–C), despite showing lowest pTR of the three described cases of neoadjuvant ICI. For ctDNA, DNA released from damaged or apoptotic tumor cells, correlation with increased risk of recurrence has been described for several other malignancies (48, 49). Due to its high sensitivity for tumor recurrence (50), it could play a role in the future in HNSCC/OSCC, both for estimating the molecular tumor burden and for progression monitoring. Another promising approach presented by Rozeman et al. shows that both tumor mutation burden and a high interferon-gamma-related gene expression score (IFN-Y score) are associated with a high pathological response and a low risk of relapse in melanomas treated with ipilimumab plus nivolumab. A recent review also mentions tumor mutational burden and IFN-Y score as promising prognostic and predictive markers, highlighting the tumor microenvironment as a potential source for identifying new biomarkers (51, 52).
Currently, pTR/pCR seems to be the most reliable and practical surrogate marker for neoadjuvant ICI response available. However, the significance of pTR/pCR with regard to the necrosis rate of the initial biopsy has received little to no attention in previous publications. As demonstrated in Case B, initial biopsy taken ahead of neoadjuvant therapy may already show extensive necrosis and thus relativize the significance of any pTR/pCR determined on the basis of the definite tumor resectate. As a solution, we propose to relate the pTR/pCR to the necrosis rate of the initial biopsy and thus increase its significance as previously applied by Vos et al. (13). Nevertheless, improvement of the current criteria for pathological response (residual viable tumor (RVT)) seems necessary as they were developed in the context of induction chemotherapy showing pathologic changes completely different to those of neoadjuvant immunotherapy (53). A promising approach seems to be the immune-related pathologic response criteria (irPRC) recently published by Cottrell et al. (53). According to the Authors, the observed discrepancy between CT imaging and pathological assessment of the residual tumor is explained by the area of immune-mediated tumor clearance referred to as regression bed. The regression bed is further characterized by tumor infiltrating lymphocytes with macrophages and tertiary lymphoid structures, tumor cell death or cholesterol clefts and tissue repair parameters, specifically neovascularization and proliferative fibrosis. To account for these changes, the irPRC are defined as irRVT = viable tumor area/total tumor bed area, whereby the total tumor bed area = regression bed + RVT + necrosis (53).
Surgical therapy with curative intent is indicated for early stage HNSCC (7, 54, 55). In advanced cases, surgical tumor resection and neck dissection combined with radio(chemo)therapy are considered the most effective treatment options to date (5). Cases A, B and (39) outline the feasibility and potential effects of neoadjuvant ICI in recurrent or advanced HNSCC/OSCC prior to definitive surgical tumor treatment. ICI has not led to any delay in surgical procedures.
Shibata et al. describe a trend shift away from classical induction chemotherapy towards ICI for treatment of head and neck tumors (21). In case of immunotherapeutic approach, various explanatory models can be discussed for the significantly higher response rates in the neoadjuvant compared to the R/M setting (9–11). Response to ICI depends on local T cell infiltration (47, 56). As of now, most strategies focus on modulating tumor microenvironment in order to improve the overall efficacy of IT, not taking into consideration the possible role of tumor-draining lymph nodes and the immunomodulatory role of surgery prior to and after ICI. Since performing neck dissection results in higher rates of overall and disease-free survival (57) it plays a crucial role in surgical therapy of HNSCC. However, lack of lymphatic and potentially immunologically significant structures could have an impact on the efficacy of checkpoint inhibitors, thus explaining significantly higher response rates with neoadjuvant treatment prior to removal of lymphatic structures.
Two recent Phase III trials (MSLT-II and DeCOG-CLND; NCT00297895 and NCT02434107) demonstrated that completion lymph node dissection (CLND) for high risk melanoma treatment was not associated with better distant metastasis-free survival (DMFS) and OS outcomes (58, 59). In addition, the need for CLND to obtain better information on staging was disproved (60). In this regard, Eggermont, A.M.M. describes the paradigm shift from historical elective regional lymph node dissection (ELND) to sentinel lymph node dissection (SLND) plus CLND to sentinel lymph node dissection (SLND) alone in melanoma therapy as ground-breaking for the therapy of other entities, justified by a high response rate to immune checkpoint inhibition in melanoma (61). So far, the trend away from lymphadenectomy combined with ICI shifting to neoadjuvant is mainly limited to melanoma therapy (62). In other tumor entities accessible by ICI, such as HNSCC/OSCC, SLND as alternative for ELND remains controversial and should be further investigated in future trials. Recently, studies on murine HNSCC models by Saddawi-Konefka et al. showed that regional lymphablation eliminates the tumor response to ICI leading to worse overall survival (63). In addition, ELND led to repolarization of the tumor microenvironment and peripheral-immune compartments. The authors were able to map the murine cervical lymphatic system which allowed a precise modelling of lymphatic ablative therapy (ELND) (63). Animals were treated with different combinations of ELND and ICI without surgical treatment of the primary tumor site. Anti-CTLA4 or anti-PD-L1 treatment was administered 10 days after ELND or control skin incision. In this experimental layout, ELND counteracted the anti-PD-1 and anti-CTLA4 dependent reduction in primary tumor mass. Comparative analysis revealed a predominantly lymphocytic infiltrate and a less infiltrative cancer pattern in the primary tongue tumors of control animals compared to ELND animals under anti-CTLA4 ICI. Animals with ELND showed significantly increased CD45- cells, Myeloid derived suppressor cells (MDSCs) and M2-Type macrophages as well as a decrease in in CD8 and CD4 T-cell infiltration (63). These data support the potential use of ICI in a neoadjuvant setting with available lymphatic structures and motivate further investigation of SLND for cN0 HNSCC.
With regard to single-agent ICI, a recent meta-analysis by Masarwy et al. found no superiority of one particular anti-PD-1/PD-L1 agent over another (64). As of now, the addition of CTLA-4 antibodies (Case F) to standard anti PD-L1 ICI seems feasible without achieving significantly better results (64). The completed phase 2 study by Schoenfeld et al. investigated the administration of Nivolumab compared to Nivolumab and Ipilimumab (CTLA-4 antibody) and reported feasible use and promising response rates in the neoadjuvant setting for both cases. However, no significant difference was found between both study arms (38). Correspondingly, the IMCISION study showed that both Nivolumab alone and Nivolumab + Ipilimumab can be used successfully without significant differences in pathological response (65). Administering an additional tumor (immune-) microenvironment modulating drug, e.g. a tyrosine kinase inhibitor, could increase ICI efficacy. Oliva et al. reported a profound clinical and pathological response to preoperative Sitravatinib and Nivolumab, although the restricted patient number and lack of single-agent arms limit the study and necessitate further investigation (14). There is promising potential for drugs targeting the tumor microenvironment as immunological preconditioning in combination with classical immune checkpoint inhibition and should therefore be further explored.
Regarding the association of HPV and HNSCC, recent studies suggest that HPV-positive tumors of the oropharynx tumors respond significantly better to immunotherapy than HPV-negative ones (66, 67). In addition, the Keynote-012 and Checkmate-141 trials indicate a better response to ICI in HPV-positive tumors (9, 68). With the presence of functional HPV-specific PD-1+ TCF-1+ CD45RO+ stem-like CD8 T cells with proliferative capacity, Eberhardt et al. recently demonstrated that the cellular machinery to respond to PD-1 blockade exists in HPV-positive head and neck cancer (69). Nevertheless, HNSCC should be considered as a heterogeneous group of tumors. As Hübbers C.U. and Akgül B. noted, in contrast to the proven prognostic relevance of biologically active HPV infection in squamous cell carcinoma of the oropharynx, no such definite association was found for OSCC (70). The decision-making in case of the presented patients was not influenced by this due to a consistently negative HPV status.
Given these rapidly changing and exciting new frontiers, where does surgery situate itself? Is salvage surgery a viable option for patients in a palliative situation after failure of ICI or at stable disease state under immunotherapeutic treatment?
The clinical course of Cases E and F shows that salvage surgery can be performed successfully after ICI failure and can lead to an improvement in clinical condition. Since studies on salvage surgery in stable disease states under ICI and its effect on quality of life (QOL) are currently lacking, Cases C and D demonstrate the clinical feasibility and possible benefits.
In view of the current study landscape, salvage surgery for locoregional recurrence is considered controversial. According to Horn et al, who prospectively studied Salvage surgery with microvascular reconstruction for recurrent OSCC, it is a viable treatment option with acceptable morbidity and high success rate (34, 35). Similar results were reported by Patil et al. for patients with resectable locoregional recurrence without the option of curative re-irradiation (71, 72). Hamoir et al. and Saba et al. are more critical of salvage surgery due to high risk of recurrence at 30-40% and the significant risk of complications which is up to 67% (73, 74). All authors emphasise the urgency of new studies regarding the potentially synergistic effects of ICI and salvage surgery. Our Cases C, D, E and F demonstrate the feasibility and the improvement of clinical conditions through salvage surgery with limited complications even with complex surgical procedures requiring up to two microvascular flaps. If patients are ineligible for surgical therapy, all other treatment options should be considered. As stated by Altay-Langguth et al., radioimmunotherapy (re-irradiation with Nivolumab) might offer an effective treatment option in pre-irradiated patients (75).
Surgical debulking, whose effects on tumor progression have been controversial so far, could have alternative effects under immunotherapeutic treatment (76–78). Patients who opt for salvage surgery have most likely already undergone surgical resection of the primary tumor, including neck dissection. This procedure may have significant impact on the efficacy of checkpoint inhibitors as discussed earlier. In contrast to the potential negative impact of surgical lymphadenectomy on systemic ICI success, reduction of tumor mass in case of recurrence could play an important role in the efficacy of ICI in heavily pre-treated patients. Oppel et al. describe the emergence of ICI resistant tumor cell clones as a similar mechanism to classical chemotherapy resistance based on additionally acquired genetic alterations (76, 79). To avoid this, it is proposed to reduce genetic heterogeneity prior to molecular targeting, which could reduce the statistical probability of tumor recurrence triggered by resistant clones. Tumor debulking is suggested as a non-specific remedy for this, as currently successfully applied in clinical treatment of ovarian cancer (76). Additionally, initial experimental studies describe surgical debulking as a promoter for macrophage recruitment and therefore as a potential trigger for tumor phagocytosis in combination with ICI (77). However, increased macrophage infiltration in OSCC in the absence of ICI could also contribute to tumor progression (80, 81). Khong et al. observed a similar immunomodulatory effect of incomplete tumor debulking alone and investigated the proportion of CD4+ and CD8+ T cells in the postoperative tumor microenvironment of mice with malignant mesothelioma. Further research demonstrated that this postoperative tumor microenvironment is amenable to immunomodulatory drugs such as TLR7 agonists and anti-CD40, resulting in improved outcomes and tumor regression in 25% of cases (78).
Regarding recurrent HNSCC in particular Ritter at al. describe the feasibility of function preserving tumor debulking combined with brachytherapy and a simultaneous Cetuximab-Paclitaxel protocol as second-line treatment. Adding the Cetuximab-Paclitaxel protocol to standard tumor debulking and brachytherapy resulted in significantly higher disease-free survival and overall survival (82). Yet, the specific relationship between tumor debulking and additional systemic therapy remains unclear.
As Case D demonstrates, salvage surgery led to a significant improvement in quality of life and disease-free survival. The current tumor follow-up showed no signs of recurrence. Although this case cannot be considered a direct case of tumor debulking due to its R0 situation, the present field cancerization allows a similar conclusion. In addition, Cases C, E and F demonstrate the potentially life-prolonging and quality of life improving effect of salvage surgery in the context of immunotherapeutic treatment in selected cases.
ICI is rapidly expanding its frontiers into the neoadjuvant setting. However, the benefits of neoadjuvant ICI over conventional therapy of advanced head and neck cancer with surgical resection and adjuvant RCT has not yet been demonstrated in prospective phase 3 trials. Phase 2 studies with small patient collectives show that neoadjuvant ICI could improve the prognosis of advanced head and neck cancer. Yet, timing and surrogate markers for response remain unclear. For neoadjuvant ICI monitoring regarding pathological tumor response or tumor necrosis rate, we suggest correlation between the initial biopsy and the definite tumor resectate in order to increase its significance as a surrogate marker. Scheduling of neoadjuvant ICI should be further investigated, as recent studies indicate better outcomes with shorter time frames.
The currant multimodal treatment including immunotherapy after failure of primary surgery and RCT frequently confronts the surgeon with heavily pretreated patients and tumor progression. Salvage surgery remains a feasible therapy concept despite an increasing amount of systemic second- and third-line treatment options. Decision-making on surgical intervention in case of a salvage surgery remains, to this day, an individual choice.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of the Friedrich-Alexander University Erlangen-Nuremberg. Application number: 22-183-Br. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MW, MO, MK, RL, C-PN, TM, MH, A-OG, MiE, YF, T-OB, and JG participated in the examination and treatment of one or more of the patients and collected the data. MaE participated in the pathological diagnosis. MO and MW discussed the case and data. MO and MW wrote the manuscript. JR, RL, and T-OB aided with manuscript writing and language prettification. JR significantly contributed to the figure design. All authors read and approved the final manuscript.
MW has consulting contracts with the pharmaceutical companies Sanofi and Bristol Myers Squibb. MiE participated in an advisory board by Bristol Myers Squibb.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
HNSCC, Head and neck squamous cell carcinoma; IT, Immunotherapy; R/M, recurrent or metastatic; CSCC, Cutaneous squamous cell carcinoma; NCCN, National Comprehensive Cancer Network; cPR, Complete pathologic response; MPR, Major pathologic response; CT, Computed tomography; OSCC, Oral squamous cell carcinoma; TPS, Tumor proportion score; IC-Score, Inflammatory cell score; CPS, Combined positive score; pTR, Pathologic tumor response; RCT, Radiochemotherapy; RVT, residual viable tumor; ICI, Immune checkpoint inhibition; irPRC, Immune-related pathologic response criteria; MDSCs, Myeloid derived suppressor cells; TCF-1, T cell factor-1.
1. Aupérin A. Epidemiology of head and neck cancers: An update. Curr Opin Oncol (2020) 32(3):178–86. doi: 10.1097/CCO.0000000000000629
2. Shaikh H, Karivedu V, Wise-Draper TM. Managing recurrent metastatic head and neck cancer. Hematol Oncol Clin North Am (2021) 35(5):1009–20. doi: 10.1016/j.hoc.2021.05.009
3. Weckx A, Riekert M, Grandoch A, Schick V, Zöller JE, Kreppel M, et al. Time to recurrence and patient survival in recurrent oral squamous cell carcinoma. Oral Oncol (2019) 94:8–13. doi: 10.1016/j.oraloncology.2019.05.002
4. Lydiatt WM, Patel SG, O’Sullivan B, Brandwein MS, Ridge JA, Migliacci JC, et al. Head and neck cancers-major changes in the American joint committee on cancer eighth edition cancer staging manual. CA Cancer J Clin (2017) 67(2):122–37. doi: 10.3322/caac.21389
5. National Comprehensive Cancer Center. NCCN clinical practice guidelines in oncology; head and neck cancers (2022). Available at: www.nccn.org (Accessed January 20, 2022).
6. Specenier PM, Vermorken JB. Current concepts for the management of head and neck cancer: Chemotherapy. Oral Oncol (2009) 45(4-5):409–15. doi: 10.1016/j.oraloncology.2008.05.014
7. German Cancer Society, German Cancer Aid, AWMF. German Guideline program in oncology: oral cavity cancer long version 3.0 (2021). Available at: https://www.leitlinienprogramm-onkologie.de/leitlinien/mundhoehlenkarzinom/ (Accessed 11.11.2021).
8. Ferris RL. Immunology and immunotherapy of head and neck cancer. J Clin Oncol (2015) 33(29):3293–304. doi: 10.1200/JCO.2015.61.1509
9. Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med (2016) 375(19):1856–67. doi: 10.1056/NEJMoa1602252
10. Hanna GJ, ONeill A, Shin K-Y, Wong K, Jo VY, Quinn CT, et al. Neoadjuvant and adjuvant nivolumab and lirilumab in patients with recurrent, resectable squamous cell carcinoma of the head and neck. Clin Cancer Res (2021). doi: 10.1200/JCO.2021.39.15_suppl.6053
11. Uppaluri R, Campbell KM, Egloff AM, Zolkind P, Skidmore ZL, Nussenbaum B, et al. Neoadjuvant and adjuvant pembrolizumab in resectable locally advanced, human papillomavirus-unrelated head and neck cancer: A multicenter, phase II trial. Clin Cancer Res (2020) 26(19):5140–52. doi: 10.1158/1078-0432.CCR-20-1695
12. Uppaluri R, Campbell KM, Egloff AM, Zolkind P, Skidmore ZL, Nussenbaum B, et al. Correction: Neoadjuvant and adjuvant pembrolizumab in resectable locally advanced, human papillomavirus-unrelated head and neck cancer: A multicenter, phase II trial. Clin Cancer Res (2021) 27(1):357. doi: 10.1158/1078-0432.CCR-20-4484
13. Vos JL, Elbers JBW, Krijgsman O, Traets JJH, Qiao X, Leun der van AM, et al. Neoadjuvant immunotherapy with nivolumab and ipilimumab induces major pathological responses in patients with head and neck squamous cell carcinoma. Nat Commun (2021) 12(1):7348. doi: 10.1038/s41467-021-26472-9
14. Oliva M, Chepeha D, Olson DVAP, Prawira A, Spreafico A, Diaz-Mejia J, et al. Antitumor immune effects of preoperative sitravatinib and nivolumab in oral cavity cancer: SNOW window-of-opportunity study. J Immunother Cancer (2021) 9(10):e003476. doi: 10.1136/jitc-2021-003476
15. Liu J, Blake SJ, Yong MCR, Harjunpää H, Ngiow SF, Takeda K, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov (2016) 6(12):1382–99. doi: 10.1158/2159-8290.CD-16-0577
16. Liu J, O’Donnella J, Yana J, Madore S, Allena MJ, Smyth MWL, et al. Timing of neoadjuvant immunotherapy in relation to surgery is crucial for outcome. Oncoimmunology (2019) 8(5):e1581530. doi: 10.1080/2162402X.2019.1581530
17. Buettner M, Bode U. Lymph node dissection–understanding the immunological function of lymph nodes. Clin Exp Immunol (2012) 169(3):205–12. doi: 10.1111/j.1365-2249.2012.04602.x
18. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet (2019) 394(10212):1915–28. doi: 10.1016/S0140-6736(19)32591-7
19. Cohen EE, Karrison TG, Kocherginsky M, Mueller J, Egan R, Huang CH, et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol (2014) 32(25):2735–43. doi: 10.1200/JCO.2013.54.6309
20. Haddad R, O'Neill A, Rabinowits G, Tishler R, Khuri F, Adkins D, et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): A randomised phase 3 trial. Lancet Oncol (2013) 14(3):257–64. doi: 10.1016/S1470-2045(13)70011-1
21. Shibata H, Saito S, Uppaluri R. Immunotherapy for head and neck cancer: A paradigm shift from induction chemotherapy to neoadjuvant immunotherapy. Front Oncol (2021) 11:727433. doi: 10.3389/fonc.2021.727433
22. Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (Keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol (2015) 151(10):1081–6. doi: 10.1001/jamadermatol.2015.1187
23. Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma: Incidence, risk factors, diagnosis, and staging. J Am Acad Dermatol (2018) 78(2):237–47. doi: 10.1016/j.jaad.2017.08.059
24. Stratigos AJ, Garbe C, Dessinioti C, Lebbe C, Bataille V, Bastholt L, et al. European Interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 1. epidemiology, diagnostics and prevention. Eur J Cancer (2020) 128:60–82. doi: 10.1016/j.ejca.2020.01.007
25. Lindelöf B, Sigurgeirsson B, Gäbel H, Stern RS. Incidence of skin cancer in 5356 patients following organ transplantation. Br J Dermatol (2000) 143(3):513–9. doi: 10.1111/j.1365-2133.2000.03703.x
26. Cordaro A, Dobbs TD, Gibson JA, Whitaker S, Whitaker IS. Skin cancer screening in organ transplant centres in the united kingdom: A national survey. Eur J Dermatol (2020) 30(4):372–6. doi: 10.1684/ejd.2020.3845
27. Cranmer LD, Engelhardt C, Morgan SS. Treatment of unresectable and metastatic cutaneous squamous cell carcinoma. Oncologist (2010) 15(12):1320–8. doi: 10.1634/theoncologist.2009-0210
28. National Comprehensive Cancer Center. NCCN clinical practice guidelines in oncology; squamous cell skin cancer (2021). Available at: www.nccn.org (Accessed November 9, 2021).
29. Gross N, Ferrarotto R, Nagarajan P, Bell D, El-Naggar A, Johnson JM, et al. Phase II study of neoadjuvant cemiplimab prior to surgery in patients with stage III/IV (M0) cutaneous squamous cell carcinoma of the head and neck (CSCC-HN). Ann Oncol (2019) 30. doi: 10.1093/annonc/mdz394.071
30. Ferrarotto R, Amit M, Nagarajan P, Rubin ML, Yuan Y, Bell D, et al. Pilot phase II trial of neoadjuvant immunotherapy in locoregionally advanced, resectable cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res (2021) 27(16):4557–65. doi: 10.1158/1078-0432.CCR-21-0585
31. Gellrich FF, Hüning S, Beissert S, Eigentler T, Stockfleth E, Gutzmer R, et al. Medical treatment of advanced cutaneous squamous-cell carcinoma. J Eur Acad Dermatol Venereol (2019) 33 Suppl 8:38–43. doi: 10.1111/jdv.16024
32. Grob JJ, Joshi A, Bauman JR, et al. Pembrolizumab monotherapy for recurrent or metastatic cutaneous squamous cell carcinoma: A single-arm phase II trial (KEYNOTE-629). J Clin Oncol (2020) 38(25):2916–25. doi: 10.1200/JCO.19.03054
33. Bauml JM, Aggarwal C, Cohen RB. Immunotherapy for head and neck cancer: where are we now and where are we going? Ann Transl Med (2019) 7(Suppl 3):S75. doi: 10.21037/atm.2019.03.58
34. Horn D, Bodem J, Freudlsperger C, Zittel S, Weichert W, Hoffmann J, et al. Outcome of heavily pretreated recurrent oral squamous cell carcinoma after salvage resection: A monocentric retrospective analysis. J Craniomaxillofac Surg (2016) 44(8):1061–6. doi: 10.1016/j.jcms.2016.05.005
35. Horn D, Zittel S, Moratin J, Metzger K, Ristow O, Krisam J, et al. Prospective feasibility analysis of salvage surgery in recurrent oral cancer in terms of quality of life. Oral Oncol (2020) 102:104580. doi: 10.1016/j.oraloncology.2020.104580
36. Wise-Draper TM, Gulati S, Palackdharry S, Hinrichs BH, Worden FP, Old MO, et al. Phase II clinical trial of neoadjuvant and adjuvant pembrolizumab in resectable local-regionally advanced head and neck squamous cell carcinoma. Clin Cancer Res (2022) 28(7):1345–52. doi: 10.1158/1078-0432.CCR-21-3351
37. Leidner R, Crittenden M, Young K, Xiao H, Wu Y, Couey MA, et al. Neoadjuvant immunoradiotherapy results in high rate of complete pathological response and clinical to pathological downstaging in locally advanced head and neck squamous cell carcinoma. J Immunother Cancer (2021) 9(5):e002485. doi: 10.1136/jitc-2021-002485
38. Schoenfeld JD, Hanna GJ, Jo VY, Rawal B, Chen Y-H, Catalano PS, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in untreated oral cavity squamous cell carcinoma: A phase 2 open-label randomized clinical trial. JAMA Oncol (2020) 6(10):1563–70. doi: 10.1001/jamaoncol.2020.2955
39. Olmos M, Glajzer J, Büntemeyer T-O, Frohwitter G, Ries J, Eckstein M, et al. Neoadjuvant immunotherapy of oral squamous cell carcinoma: Case report and assessment of histological response. Front Oncol (2021) 11:720951. doi: 10.3389/fonc.2021.720951
40. Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A, et al. Neck dissection classification update: Revisions proposed by the American head and neck society and the American academy of otolaryngology-head and neck surgery. Arch Otolaryngol Head Neck Surg (2002) 128(7):751–8. doi: 10.1001/archotol.128.7.751
41. Hecht M, et al. Safety and efficacy of single cycle induction treatment with cisplatin/docetaxel/ durvalumab/tremelimumab in locally advanced HNSCC: First results of CheckRad-CD8. J ImmunoTher Cancer (2020) 8(2):e001378. doi: 10.1136/jitc-2020-001378
42. Menzies AM, Tetzlaff MT, van Wiel BA, Lo S, Tarhini AA, Thomas E, et al. Pathological response and survival with neoadjuvant therapy in melanoma: A pooled analysis from the international neoadjuvant melanoma consortium (INMC). Nat Med (2021) 27(2):301–9. doi: 10.1038/s41591-020-01188-3
43. Wise-Draper TM, Wise-Draper T, et al. (2021). Annual American society of clinical oncology annual meeting. J Clin Oncol 39:6006–6006. doi: 10.1200/JCO.2021.39.15_suppl.6006
44. Cao C, Le A, Bott M, Yang C-FJ, Gossot D, Melfi F, et al. Meta-analysis of neoadjuvant immunotherapy for patients with resectable non-small cell lung cancer. Curr Oncol (2021) 28(6):4686–701. doi: 10.3390/curroncol28060395
45. Vos JL, Zuur CL, Smit LA, Boer JP, Al‑Mamgani A, Brekel den van MWM, et al. [(18)F]FDG-PET accurately identifies pathological response early upon neoadjuvant immune checkpoint blockade in head and neck squamous cell carcinoma. Eur J Nucl Med Mol Imaging (2022) 49(6):2010–22. doi: 10.1007/s00259-021-05610-x
46. Merlino DJ, Johnson JM, Tuluc M, Gargano S, Stapp R, Harshyne L, et al. Discordant responses between primary head and neck tumors and nodal metastases treated with neoadjuvant nivolumab: Correlation of radiographic and pathologic treatment effect. Front Oncol (2020) 10:566315. doi: 10.3389/fonc.2020.566315
47. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJM, Robert L, et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature (2014) 515(7528):568–71. doi: 10.1038/nature13954
48. Tie J, Wang Y, Tomasetti C, Li L, Springer S, Kinde I, et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci Transl Med (2016) 8(346):346ra92. doi: 10.1126/scitranslmed.aaf6219
49. Said R, Guibert N, Oxnard GR, Tsimberidou AM. Circulating tumor DNA analysis in the era of precision oncology. Oncotarget (2020) 11(2):188–211. doi: 10.18632/oncotarget.27418
50. Qiu B, Guo W, Zhang F, Lv F, Ji Y, Peng Y, et al. Dynamic recurrence risk and adjuvant chemotherapy benefit prediction by ctDNA in resected NSCLC. Nat Commun (2021) 12(1):6770. doi: 10.1038/s41467-021-27022-z
51. Rozeman EA, Krijgsman O, Hoefsmit EP, Reijers ILM, Saw RPM, Dimitriadis P, et al. Survival and biomarker analyses from the OpACIN-neo and OpACIN neoadjuvant immunotherapy trials in stage III melanoma. Nat Med (2021) 27(2):256–63. doi: 10.1038/s41591-020-01211-7
52. Gavrielatou N, Doumas S, Economopoulou P, Foukas PG, Psyrri A. Biomarkers for immunotherapy response in head and neck cancer. Cancer Treat Rev (2020) 84:101977. doi: 10.1016/j.ctrv.2020.101977
53. Cottrell TR, Thompson ED, Forde PM, Stein JE, Duffield AS, Anagnostou V, et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for quantitative immune-related pathologic response criteria (irPRC). Ann Oncol (2018) 29(8):1853–60. doi: 10.1093/annonc/mdy218
54. Montero PH, Patel SG. Cancer of the oral cavity. Surg Oncol Clin N Am (2015) 24(3):491–508. doi: 10.1016/j.soc.2015.03.006
55. Rodgers HW Jr., Weinstock MA, Feldman SR, Coldiron BM. Management of squamous cell carcinoma of the floor of mouth. Head Neck (1993) 15(1):16–9. doi: 10.1002/hed.2880150104
56. Kümpers C, Grätz V, Langan EA, Jokic M, Haase O, Perner S. Immune cell infiltration of the primary tumor, not PD-L1 status, is associated with improved response to checkpoint inhibition in metastatic melanoma. Front Med (Lausanne) (2019) 6:27. doi: 10.3389/fmed.2019.00027
57. D'Cruz AK, Vaish R, Kapre N, Dandekar M, Gupta S, Hawaldar R, et al. Elective versus therapeutic neck dissection in node-negative oral cancer. N Engl J Med (2015) 373(6):521–9. doi: 10.1056/NEJMoa1506007
58. Leiter U, Stadler R, Mauch C, Hohenberger W, Brockmeyer NH, Berking C, et al. Final analysis of DeCOG-SLT trial: No survival benefit for complete lymph node dissection in patients with melanoma with positive sentinel node. J Clin Oncol (2019) 37(32):3000–8. doi: 10.1200/JCO.18.02306
59. Faries MB, Thompson JF, Cochran AJ, Andtbacka RH, Mozzillo N, Zager JS, et al. Completion dissection or observation for sentinel-node metastasis in melanoma. N Engl J Med (2017) 376(23):2211–22. doi: 10.1056/NEJMoa1613210
60. Verver D, van Klaveren D, van Akkooi ACJ, Rutkowski P, Powell BWEM, Robert C, et al. Risk stratification of sentinel node-positive melanoma patients defines surgical management and adjuvant therapy treatment considerations. Eur J Cancer (2018) 96:25–33. doi: 10.1016/j.ejca.2018.02.022
61. Eggermont AMM. The impact of the immunotherapy revolution on lymph nodal surgery. Bull Cancer (2020) 107(6):640–1. doi: 10.1016/j.bulcan.2019.05.013
62. Ascierto PA, Eggermont AMM. Neoadjuvant therapy in melanoma: The next step? Lancet Oncol (2018) 19(2):151–3. doi: 10.1016/S1470-2045(18)30016-0
63. Saddawi-Konefka R, O’Farrell A, Faraji F, Clubb L, Allevato MM, Jensen SM, et al. Lymphatic-preserving treatment sequencing with immune checkpoint inhibition unleashes cDC1-dependent antitumor immunity in HNSCC. Nat Commun (2022) 13(1):4298. doi: 10.1038/s41467-022-31941-w
64. Masarwy R, Kampel L, Horowitz G, Gutfeld O, Muhanna N. Neoadjuvant PD-1/PD-L1 inhibitors for resectable head and neck cancer: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg (2021) 147(10):871–8. doi: 10.1001/jamaoto.2021.2191
65. Zuur CL, Elbers JBW, Vos JL, van der Leun A, Qiao X, Karakullukcu B, et al. Feasibility and toxicity of neoadjuvant nivolumab with or without ipilimumab prior to extensive (salvage) surgery in patients with advanced head and neck cancer (the IMCISION trial, NCT03003637). J Clin Oncol (2019) 37(15_suppl):2575–5. doi: 10.1200/JCO.2019.37.15_suppl.2575
66. Wang M, Zhai X, Li J, Guan J, Xu S, Li YY, et al. The role of cytokines in predicting the response and adverse events related to immune checkpoint inhibitors. Front Immunol (2021) 12:670391. doi: 10.3389/fimmu.2021.670391
67. Galvis MM, Borges GA, Oliveira Bueno T, Toledo Porto I, Castilho Moraes R, Guerra ENS, et al. Immunotherapy improves efficacy and safety of patients with HPV positive and negative head and neck cancer: A systematic review and meta-analysis. Crit Rev Oncol Hematol (2020) 150:102966. doi: 10.1016/j.critrevonc.2020.102966
68. Seiwert TY, Burtness B, Mehra R, Weiss J, Berger R, Eder JP, et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): an open-label, multicentre, phase 1b trial. Lancet Oncol (2016) 17(7):956–65. doi: 10.1016/S1470-2045(16)30066-3
69. Eberhardt CS, Prokhnevska N, Obeng RC, Im SJ, Kissick HT, Nasti TH, et al. Functional HPV-specific PD-1(+) stem-like CD8 T cells in head and neck cancer. Nature (2021) 597(7875):279–84. doi: 10.1038/s41586-021-03862-z
70. Hübbers CU, Akgül B. HPV and cancer of the oral cavity. Virulence (2015) 6(3):244–8. doi: 10.1080/21505594.2014.999570
71. Patil VM, Noronha V, Thiagarajan S, Joshi A, Chandrasekharan A, Talreja V, et al. Salvage surgery in head and neck cancer: Does it improve outcomes? Eur J Surg Oncol (2020) 46(6):1052–8. doi: 10.1016/j.ejso.2020.01.019
72. Foster CC, Fan M, Lee NY, Yom SS, Heaton CM, Deraniyagala R, et al. Is it worth it? consequences of definitive head and neck reirradiation. Semin Radiat Oncol (2020) 30(3):212–7. doi: 10.1016/j.semradonc.2020.02.002
73. Hamoir M, Holvoet E, Ambroise J, Lengelé B, Schmitz S. Salvage surgery in recurrent head and neck squamous cell carcinoma: Oncologic outcome and predictors of disease free survival. Oral Oncol (2017) 67:1–9. doi: 10.1016/j.oraloncology.2017.01.008
74. Saba NF, Mendenhall WM, Hutcheson K, Suárez C, Wolf G, Ferlito A. Salvage surgery for squamous cell carcinoma of the head and neck in the era of immunotherapy: Is it time to clarify our guidelines? Cancer (2018) 124(21):4163–4. doi: 10.1002/cncr.31717
75. Altay-Langguth A, Balermpas P, Brandts C, Balster S, Ghanaati S, Winkelmann R, et al. Re-irradiation with concurrent and maintenance nivolumab in locally recurrent and inoperable squamous cell carcinoma of the head and neck: A single-center cohort study. Clin Trans Radiat Oncol (2021) 28:71–8. doi: 10.1016/j.ctro.2021.03.004
76. Oppel F, Görner M, Sudhoff H. The potential of tumor debulking to support molecular targeted therapies. Front Oncol (2020) 10:801. doi: 10.3389/fonc.2020.00801
77. Zhu H, Leiss L, Yang N, Li X, Cheshier SH, Weissman IL, et al. Surgical debulking promotes recruitment of macrophages and triggers glioblastoma phagocytosis in combination with CD47 blocking immunotherapy. Oncotarget (2017) 8(7):12145–57. doi: 10.18632/oncotarget.14553
78. Khong A, Cleaver AL, Alatas MF, Wylie BC, Connor T, Fisher SA, et al. The efficacy of tumor debulking surgery is improved by adjuvant immunotherapy using imiquimod and anti-CD40. BMC Cancer (2014) 14:969. doi: 10.1186/1471-2407-14-969
79. Sabnis AJ, Bivona TG. Principles of resistance to targeted cancer therapy: Lessons from basic and translational cancer biology. Trends Mol Med (2019) 25(3):185–97. doi: 10.1016/j.molmed.2018.12.009
80. Weber M, Büttner-Herold M, Hyckel P, Moebius P, Distel L, Ries J, et al. Small oral squamous cell carcinomas with nodal lymphogenic metastasis show increased infiltration of M2 polarized macrophages–an immunohistochemical analysis. J Craniomaxillofac Surg (2014) 42(7):1087–94. doi: 10.1016/j.jcms.2014.01.035
81. Weber M, Iliopoulos C, Moebius P, Büttner-Herold M, Amann K, Ries J, et al. Prognostic significance of macrophage polarization in early stage oral squamous cell carcinomas. Oral Oncol (2016) 52:75–84. doi: 10.1016/j.oraloncology.2015.11.001
Keywords: salvage surgery, HNSCC, OSCC, CSCC, immunotherapy, checkpoint inhibition, anti-PD 1, neoadjuvant
Citation: Olmos M, Lutz R, Büntemeyer T-O, Glajzer J, Nobis C-P, Ries J, Möst T, Eckstein M, Hecht M, Gostian A-O, Erdmann M, Foerster Y, Kesting M and Weber M (2022) Case report: Patient specific combination of surgery and immunotherapy in advanced squamous cell carcinoma of the head and neck – a case series and review of literature. Front. Immunol. 13:970823. doi: 10.3389/fimmu.2022.970823
Received: 16 June 2022; Accepted: 10 October 2022;
Published: 27 October 2022.
Edited by:
Varun Sasidharan Nair, Helmholtz Association of German Research Centers (HZ), GermanyCopyright © 2022 Olmos, Lutz, Büntemeyer, Glajzer, Nobis, Ries, Möst, Eckstein, Hecht, Gostian, Erdmann, Foerster, Kesting and Weber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Weber, bWFudWVsLndlYmVyQHVrLWVybGFuZ2VuLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.