
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 13 October 2022
Sec. T Cell Biology
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.948314
This article is part of the Research TopicInsights in T Cell Biology: 2022View all 7 articles
 Namin Wei1†
Namin Wei1† Yan Xu1†
Yan Xu1† Ya’nan Li1
Ya’nan Li1 Jingjing Shi2
Jingjing Shi2 Xuesong Zhang2
Xuesong Zhang2 Yaping You2
Yaping You2 Qianqian Sun1
Qianqian Sun1 Huaqiang Zhai1*
Huaqiang Zhai1* Yuanhui Hu2*
Yuanhui Hu2*Atherosclerosis (AS) is widespread and develops into circulatory system problems. T cells play an essential regulatory role in AS occurrence and development. So far, there is no bibliometric research on T cells and AS. To learn more about T cell and AS development, 4,381 records were retrieved from Web of Science™ Core Collection. Then, these records were scientometrically analyzed using CiteSpace and VOSviewer in terms of spatiotemporal distribution, author distribution, subject categories, topic distribution, references, and keywords. Our analysis provides basic information on research in the field, demonstrates that the field has stabilized over the past decade, and identifies potential partners for interested researchers. Current research hotspots in this field mainly include the inflammatory mechanism, immune mechanism, related diseases, and related cytokines of AS. B cell, mortality, inhibition, and monocyte represent the frontiers of research in this field, undergoing an explosive phase. We hope that this work will provide new ideas for advancing the scientific research and clinical application of T cell and AS.
Atherosclerosis (AS) is a chronic inflammatory disease with an autoimmune component that is regulated by innate and adaptive immunity (1–3). AS exists widely in countries all over the world and progresses into a circulatory system problem (4, 5). It is estimated that by 2030, more than 23 million people will die annually from AS (6). At present, the treatment of AS has been expanded from simple lipid-lowering, lipid-regulating and plaque stabilization to the prevention and control of immune damage and inflammation (2).
Studies have shown that atherosclerotic lesions contain a large number of immune cells, especially monocyte macrophages and T cells (7). Among them, the key to adaptive immune regulation lies in the regulation of T cells. T cells are activated in both cellular immunity and humoral immunity, and different T cell subtypes play different roles (8). Examples, Th1 cells secrete pro-inflammatory cytokines such as interferon (IFN) -γ and interleukin (IL) -12 to promote monocyte infiltration and macrophage activation, thus promoting AS (9). Th2 cells, secrete IL-4, IL-5, IL-10, and IL-13, and their anti-atherosclerotic effects remain controversial (10, 11). Regulatory T cells (Tregs) are immunosuppressive cells, which play a protective role in AS by inhibiting Th1/Th17 mediated pro-inflammatory response and down-regulating Dendritic Cell Presenting Antigen (12–14).
Bibliometrics is a branch of informatics that takes the literature system and bibliometric characteristics as the research object and conducts quantitative and qualitative analyses of literature. This method can quantitatively measure the contour distribution, relationship, and clustering of the research field (15) and has become one of the prevalent techniques for assessing academic work credibility, quality, and impact (16, 17). Specifically, the evaluation can comprise contributions and influence of different authors, countries/regions, institutions, disciplines, and journals, as well as assess the status, trends, and frontiers of research activities (18–20). VOSviewer and CiteSpace are commonly used bibliometric visualization tools for data analysis and visualization (21, 22). They are effective methods for evaluating the thematic development of structured content and can facilitate intuitive comprehension among readers (23).
Although this type of literature has been widely utilized in other fields in recent years, to our knowledge, so far, there is no bibliometric study in the field of T cell and AS. To fill this knowledge gap, this study is based on the Web of Science™ Core Collection (WoSCC). Relevant bibliometric data (annual articles, countries/regions, authors, institutions, disciplines, journals, references and keywords) for each T cell and AS research field were retrieved, and descriptive statistics were performed. This paper discusses the research status, hotspots, and frontiers of literature on T cell and AS and draws knowledge maps using CiteSpace and VOSviewer to serve as a reference for relevant future research.
Web of Science is the primary research platform for hard science, social sciences, arts, and humanities information, as well as the independent global citation database of the world’s most trusted publishers (24). To improve data representativeness and accessibility, we retrieved WoSCC. The following search terms were employed to retrieve literature from WoSCC regardless of language or document type: Topic = (“T-lymphocyte” OR “T Lymphocytes” OR “T-Lymphocyte” OR “Thymus-Dependent Lymphocytes” OR “Lymphocyte, Thymus-Dependent” OR “Lymphocytes, Thymus-Dependent” OR “Thymus Dependent Lymphocytes” OR “Thymus-Dependent Lymphocyte” OR “T-Cells” OR “T-Cell” OR “T Cell” OR “Cell, T” OR “Cells, T” OR “T Cells” OR “T Lymphocyte” OR “Lymphocyte, T” OR “Lymphocytes, T”) AND (“Atherosclerosis” OR “Atheroscleroses” OR “Atherogenesis”). The retrieved data were collected on February 20, 2022, to avoid any potential deviation due to daily updates. A total of 4,381 records comprising ten document types were obtained. Notably, 3,096 original research papers accounted for 70.669% of total records (Table 1). Review articles ranked second (n=978), accounting for 22.324% of the total records. The other eight document types met abstracts (n=184), editorial materials (n=98), proceedings papers (n=65), letters (n=21), book chapters (n=19), early access (n=18), corrections (n=4), and retracted publications (n=1). A total of 4,381 records were exported in the form of full records with cited references, saved as plain text files, and stored in download_.txt format. A total of 199,057 times cited, 122,704 citing articles, 181 h-index, and 45.440 average per item were obtained.
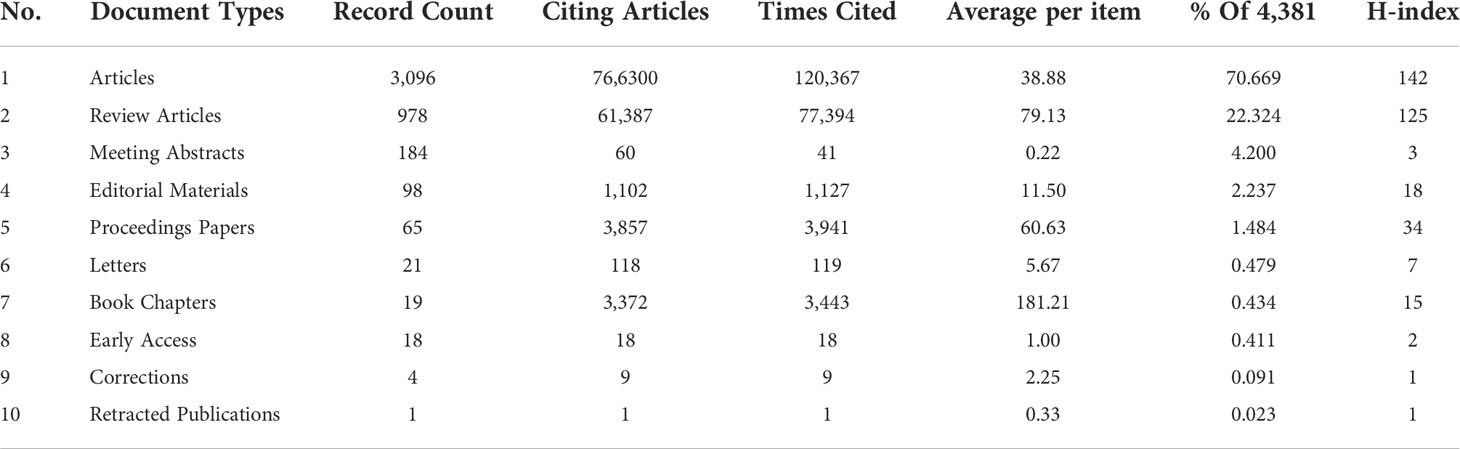
Table 1 Document types of the publications.
The Microsoft Office Excel 2019, VOSviewer (v.1.6.17), and CiteSpace (v.6.1.R3 Advanced) analyzed all 4,381 documents. VOSviewer (a bibliometric software) is a Java-based free software developed by Van Eck and Waltman of the center for science and technology studies (CWTS) of Leiden University in the Netherlands in 2009. It has a strong graphic ability and is suitable for processing large-scale data (22). CiteSpace was developed by Professor Chen Chaomei of Drexel University in the United States. It is a document visualization analysis software gradually developed for bibliometrics analyses and data visualization (21, 25). CiteSpace was deployed to visually display the basic knowledge and hotspots of T cell and AS and predict its research frontiers (26). The emergence and development of these two software have strongly promoted the research and application expansion of the entire information visualization field (27). Figure 1 shows the flowchart for search strategy and selection process in this study.
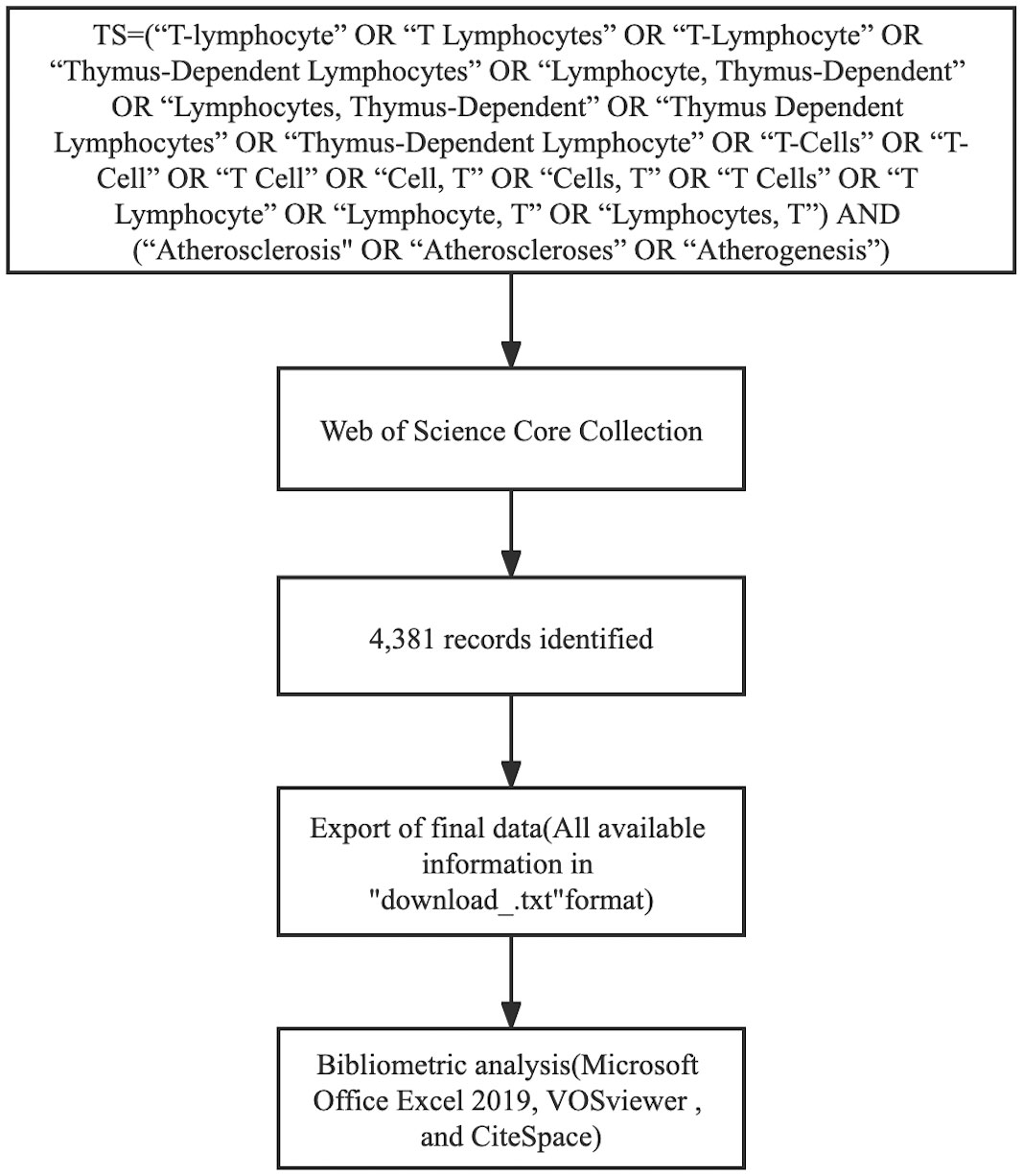
Figure 1 The flowchart illustrating the search strategy and selection process in T cell and AS.
The number of publications over a period can reflect the research speed and trend in this field (28). As depicted in Figure 2, there have been publications in this field since 2004, demonstrating that it has garnered interest. Since 2007, the number of publications has basically remained constant at 200. In 2014, 315 papers were published. In recent ten years, the number of articles published has been about 250, indicating that the field is relatively stable. Citations are growing rapidly and increasing annually.
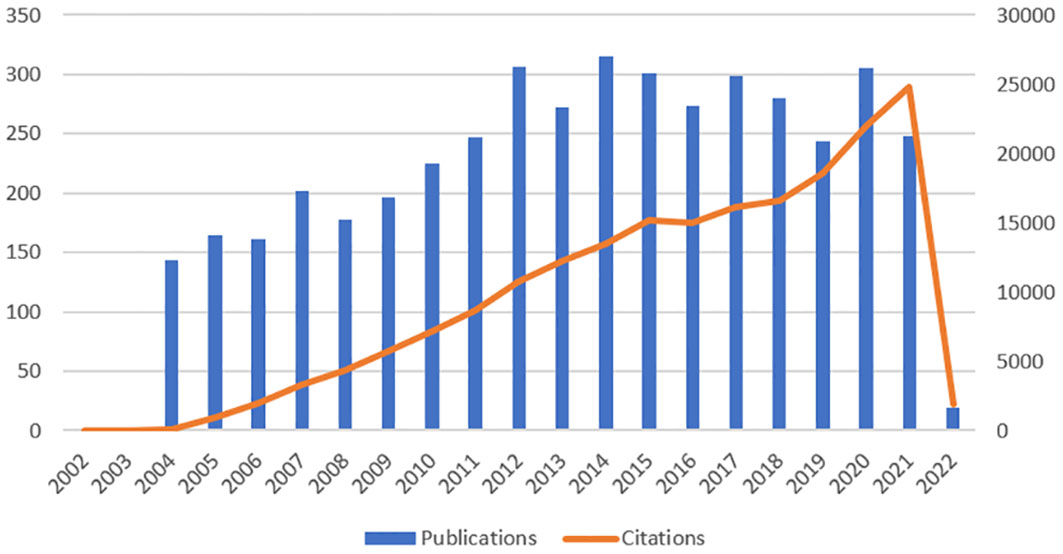
Figure 2 Trends in the growth of publications and the number of citations.
As revealed in Table 2, the largest number of published literature was from USA, China, and Germany, respectively, accounting for 32.938%, 15.156%, and 11.048% of the total reports. The total number of studies from the three countries accounted for more than half of the total reports, implying a high interest in research in T cell and AS. Studies from Sweden (96.390), USA (68.690), and Australia (60.770) had the highest average per item, indicating that the three countries started research on T cell and AS, and their results are relatively mature. Among the top 10 countries/regions in Table 2, the centrality of five countries is greater than or equal to 0.1. They are USA (0.61), Germany (0.19), England (0.19), China (0.14), and France (0.10), indicating that these countries play a crucial role in the research in this field.
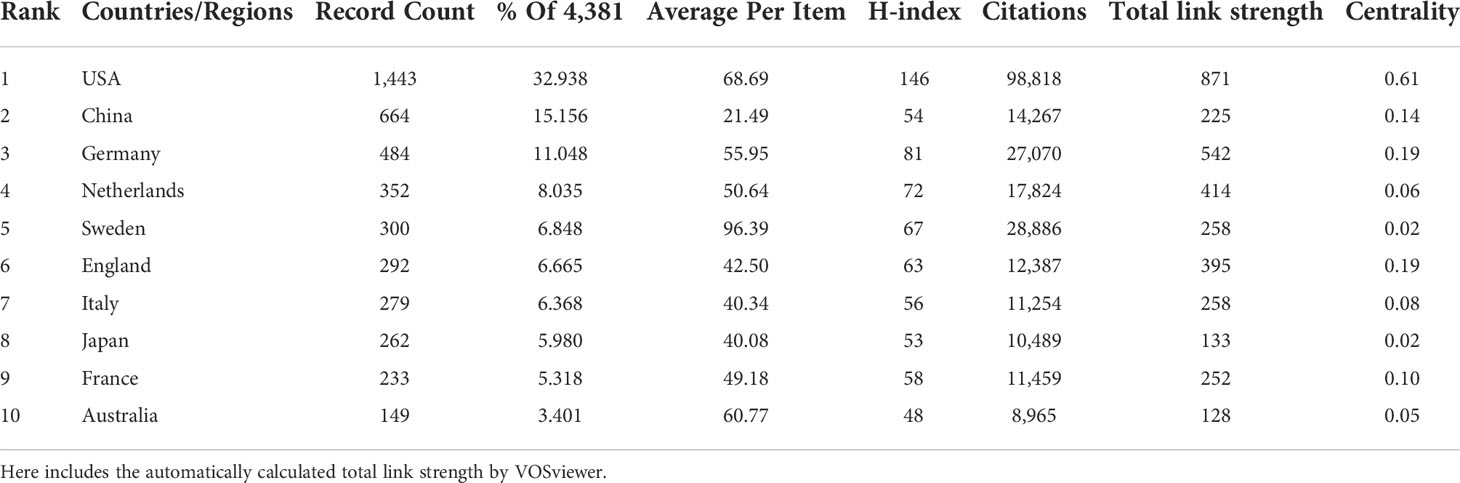
Table 2 Top 10 productive countries/regions in T cell and AS.
VOSviewer parameters were set as follows: Method (Linlog/modularity) and a minimum number of country documents: 5. The obtained results were retrieved from 85 countries, with 51 meeting the thresholds. Based on co-authorship analysis, VOSviewer classifies countries into different clusters. Nodes with different colors in the figure represent different clusters. The size of nodes represents the number of documents, and the thickness of lines represents the number of connections between nodes. Figure 3 displays the cooperation map of countries/regions in T cell and AS. Figure 3A shows that USA largely cooperated with Australia, Indonesia, Japan, New Zealand, Russia, Serbia, and Slovenia; China closely cooperated with England, Hungary, India, Mexico, Pakistan, Romania, and Turkey; Austria frequently cooperated with Croatia, Egypt, Finland, Iran, Lebanon, Qatar, Saudi Arabia, Switzerland, and Wales. Italy closely cooperated with Canada, Greece, Kazakhstan, Poland, Portugal, Scotland, Singapore, and South Korea. CiteSpace parameters were set as follows: time slice (2004–2022), years per slice (1), term source (entire selection), node type (country), and selection criteria (top N=50). Other parameters were left at the default settings. The purple-circled nodes in Figure 3B represent countries with high centrality. CiteSpace employs this indicator to measure the importance of countries in this field. From 2004 to 2022, the color changes from purple to yellow.
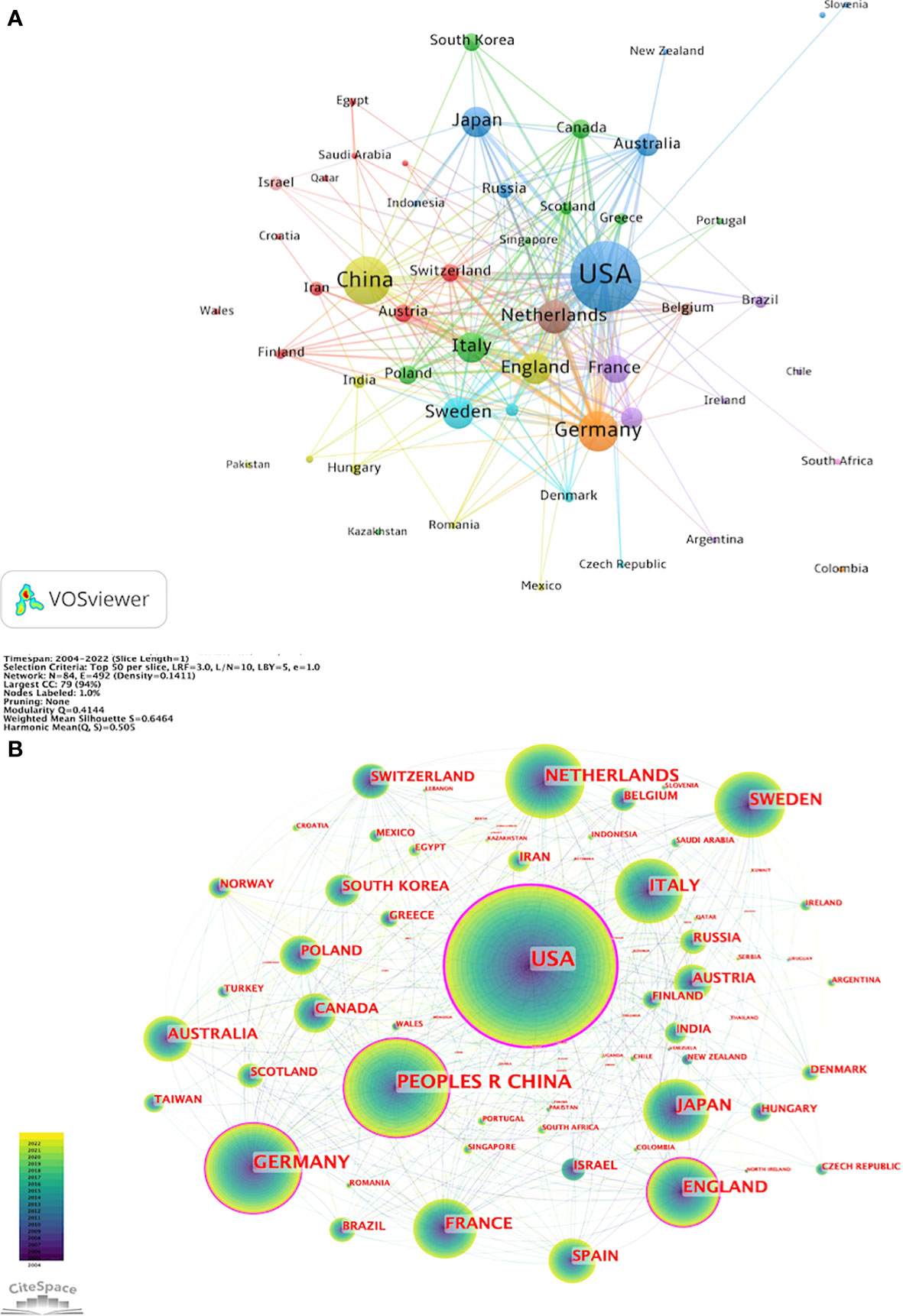
Figure 3 Cooperation map of countries/regions in T cell and AS. (A) A visual map for VOSviewer network. (B) A visual map for CiteSpace network.
Hansson GK from the Department of Medicine, Center for Molecular Medicine (G.K.H.) was the author with the most published articles, followed by Weber C from the Institute for Cardiovascular Prevention (IPEK), Ludwig Maximilians University and German Centre for Cardiovascular Research (DZHK) and Nilsson J from Department of Clinical Sciences Malmö, Lund University, Sweden (Table 3).
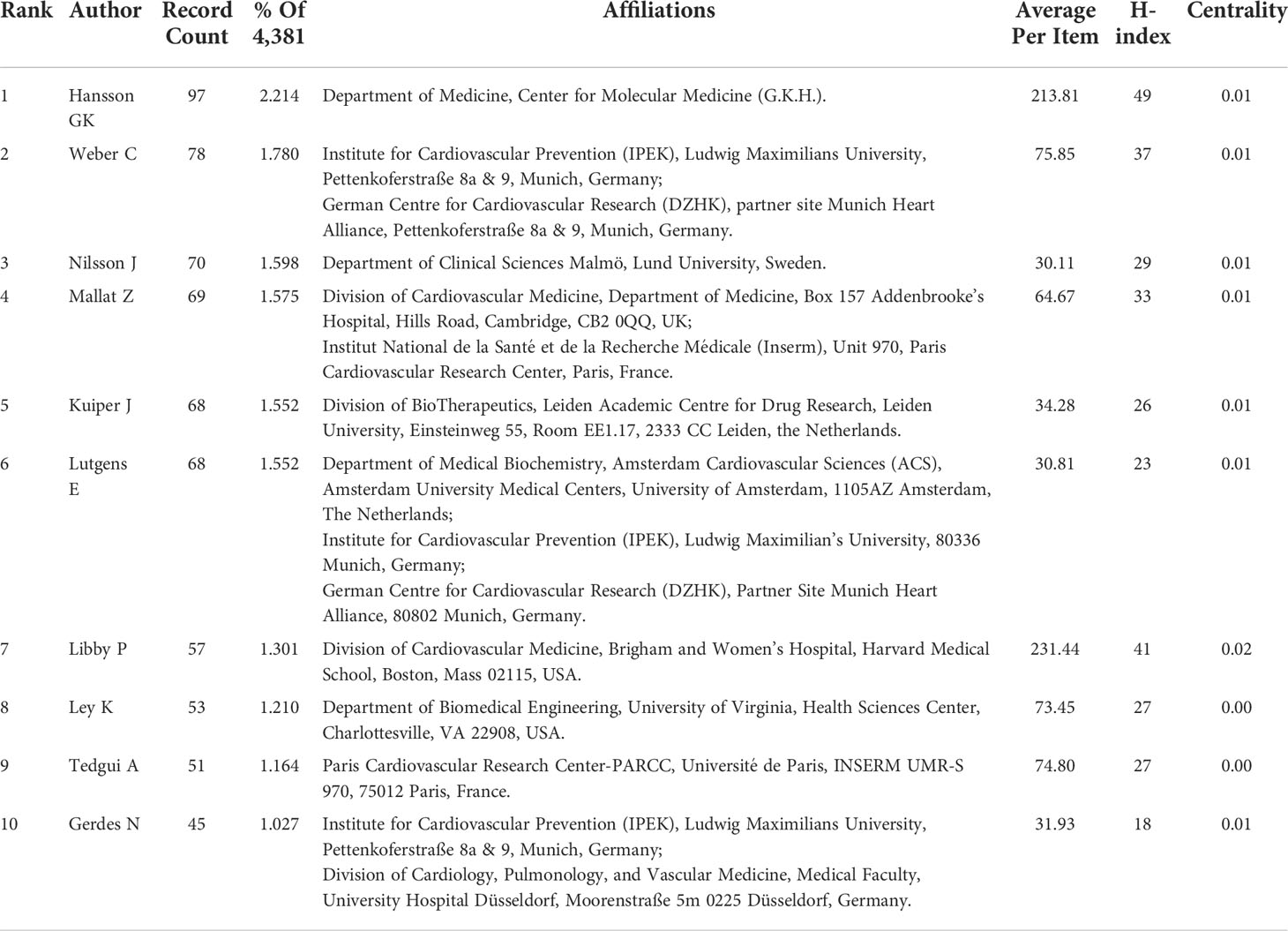
Table 3 Top 10 authors in T cell and AS.
VOSviewer parameters were set as follows: Method (Linlog/modularity) and a minimum number of documents of an author: 20. The obtained results were retrieved for 21,108 authors, and 35 met the thresholds. Based on co-authorship analysis, VOSviewer classifies authors into different clusters and colors them according to the time course in which they appear, superimposing time on the network of co-occurrence authors. Each node in Figure 4A represents each author, the size of the circle reflects the number of articles published by researchers, and the line connecting the circles represents the co-occurrence relationship between authors. As revealed in Figure 4A, different clusters represent cooperation among authors. Aukrust, Pal., Hansson, Goran K., Ketelhuth, Daniel F. J., Libby, Peter, Lichtman, Andrew H., Shi, Guo-Ping, Sukhova, and Galina K closely cooperated. Gerdes, Norbert, worked closely with Ley, Klaus, Lutgens, Esther, Weber, Christian, Winkels, Holger, Wolf, Dennis, Zernecke, Alma. Bjorkbacka, Harry, Chyu, Kuang-Yuh, Fredrikson, Gunilla Nordin, Nilsson, Jan, Shah, and Prediman K closely cooperated. Biessen, Erik A. L., worked closely with Bot, Ilze, Kuiper, Johan, Van Puijvelde, and Gijs H. M. Ait-Oufella, worked closely with Hafid, Binder, Christoph J., Mallat, Ziad, Tedgui, Alain. Bobik, and Alex, worked closely with Kyaw, Tin, Toh, and Ban-Hock. CiteSpace parameters were set as follows: time slice (2004–2022), years per slice (1), term source (entire selection), node type (author), and selection criteria (top N=50). Other parameters were left at the default settings. Figure 4B shows that a visual map of authors for CiteSpace network. The co-citation relationship is indicated by the line connecting the nodes. The size of the node is determined by the citations. The colors represent different years. From 2004 to 2022, the color changes from purple to yellow.
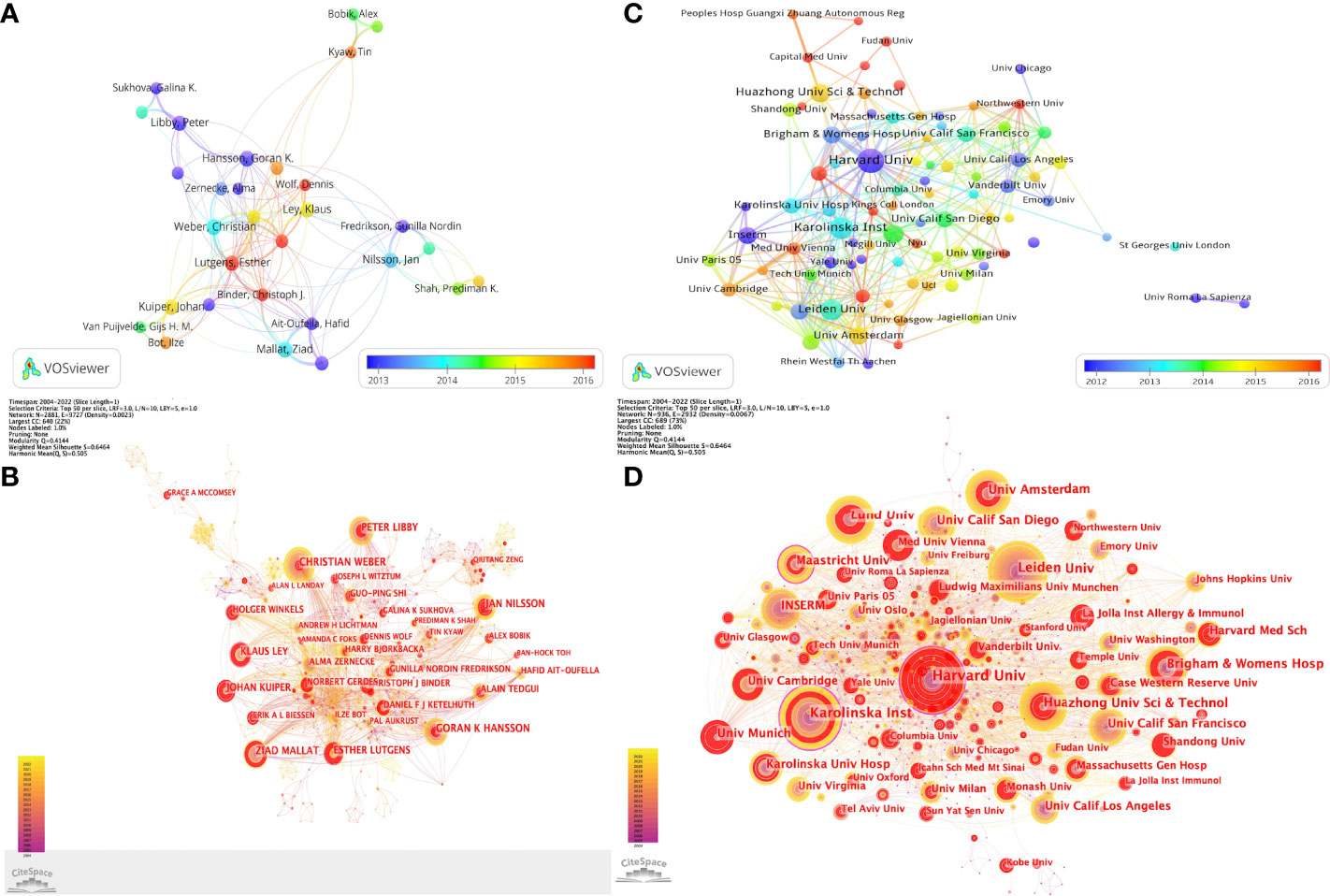
Figure 4 Collaboration networks among authors and among institutions in T cell and AS. (A) A visual map for VOSviewer network among authors. (B) A visual map for CiteSpace network among authors. (C) A visual map for VOSviewer network among institutions. (D) A visual map for CiteSpace network among institutions.
As presented in Table 4, Harvard University (460 papers) was the institution that published the most research papers, followed by University of California System (413 papers) and Karolinska Institutet (318 papers). Karolinska Institutet is the research institution with the highest average per item (133.420). Harvard University closely follows it with an average per item of 115.670 and University of California System with an average per item of 62.850. Among the top 10 institutions in T cell and AS, there are three institutions whose centrality is greater than or equal to 0.10, namely Harvard University (0.13), Karolinska Institute (0.12) and Maastricht University (0.10).
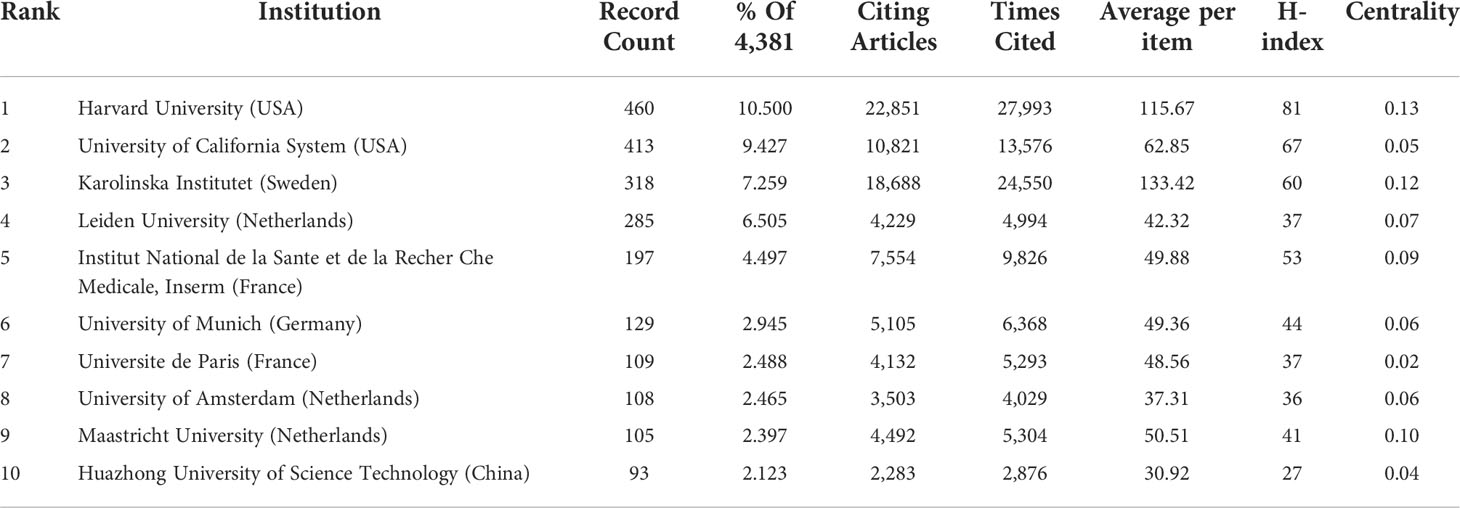
Table 4 Top 10 institutions in T cell and AS.
VOSviewer parameters were set as Method (Linlog/modularity) and a minimum number of documents of an institution: 20. The obtained results were retrieved from 3,455 institutions, and 91 met the thresholds. As demonstrated in Figure 4C, seven clusters were formed, with close cooperation among representatives of the constituent institutions of each cluster. Cluster 1 consisted of the following institutions: Harvard Univ, Icahn Sch Med Mt Sinai, Kings Coll London, Massachusetts Gen Hosp, Baylor Coll Med, Brigham & Women’s Hosp, Capital Med Univ, Fudan Univ, Harvard Med Sch, Huazhong Univ Sci & Technol, Nanjing Med Univ, NHLBI, NIAID, Peking Univ, Peoples Hosp Guangxi Zhuang Autonomous Reg, Shandong Univ, Shanghai Jiao Tong Univ, Sun Yat-Sen Univ, Temple Univ, Univ Florida, Univ Michigan, and Wuhan Univ closely collaborated. Cluster 2 contained the following institutions: Albert Einstein Coll Med, Case Western Reserve Univ, Cedars Sinai Med Ctr, Columbia Univ, Emory Univ, Johns Hopkins Univ, Lund Univ, Mcgill Univ, Monash Univ, Northwestern Univ, Stanford Univ, Univ Alabama Birmingham, Univ Calif Los Angeles, Univ Calif San Francisco, Univ Chicago, Univ Minnesota, Univ Vermont, Univ Washington, and Vanderbilt Univ closely collaborated. Cluster 3 comprised the following institutions: Hannover Med Sch, Heidelberg Univ, Leiden Univ, Ludwig Maximilians Univ Munchen, Maastricht Univ, Rhein Westfal Th Aachen, Tech Univ Munich, Univ Amsterdam, Univ Groningen, Univ Maastricht, Univ Med Ctr Utrecht, Univ Munich, Univ Sao Paulo, Univ Ulm, and Yale Univ closely collaborated. Cluster 4 included the following institutions: Boston Univ, Ist Super Sanita, Nyu, St Georges Univ London, Tel Aviv Univ, Ucl, Univ Calif Davis, Univ Cattolica Sacro Cuore, Univ Milan, Univ New S Wales, Univ Penn, Univ Roma La Sapienza, Univ Sydney, and Univ Zurich closely collaborated. Cluster 5 consisted of the following institutions: Austrian Acad Sci, Inserm, Karolinska Inst, Karolinska Univ Hosp, Med Univ Vienna, Univ Cambridge, Univ Oslo, and Univ Paris closely collaborated. Cluster 6 contained the following institutions: La Jolla Inst Allergy & Immunol, La Jolla Inst Immunol, Univ Calif San Diego, Univ Freiburg, Univ Tokyo, and Univ Virginia closely collaborated. Cluster 7 comprised the following institutions: Jagiellonian Univ, Univ Glasgow, Univ Naples Federico Ii, and Univ Oxford closely collaborated. CiteSpace parameters were set as follows: time slice (2004–2022), years per slice (1), term source (entire selection), node type (institution), and selection criteria (top N=50). Other parameters were left at the default settings. Figure 4D shows that a visual map of institutions for CiteSpace network. Through the number of connections, we can see that the links between various institutions are relatively close. We can also clearly see that the nodes with purple outer circles and larger nodes are important participating institutions in T cell and AS.
Regarding the number of published papers, Cardiac Cardiovascular Systems and Peripheral Vascular Disease and Immunology were the top three disciplines (Table 5). Additional subjects in the literature include Biochemistry Molecular Biology (18.535%), Hematology (11.276%), Cell Biology (10.454%), Medicine Research Experimental (9.792%), Pharmacology Pharmacy (7.784%), Multidisciplinary Sciences (7.464%), Endocrinology Metabolism (5.387%), Infectious Diseases (3.675%), and other subjects.
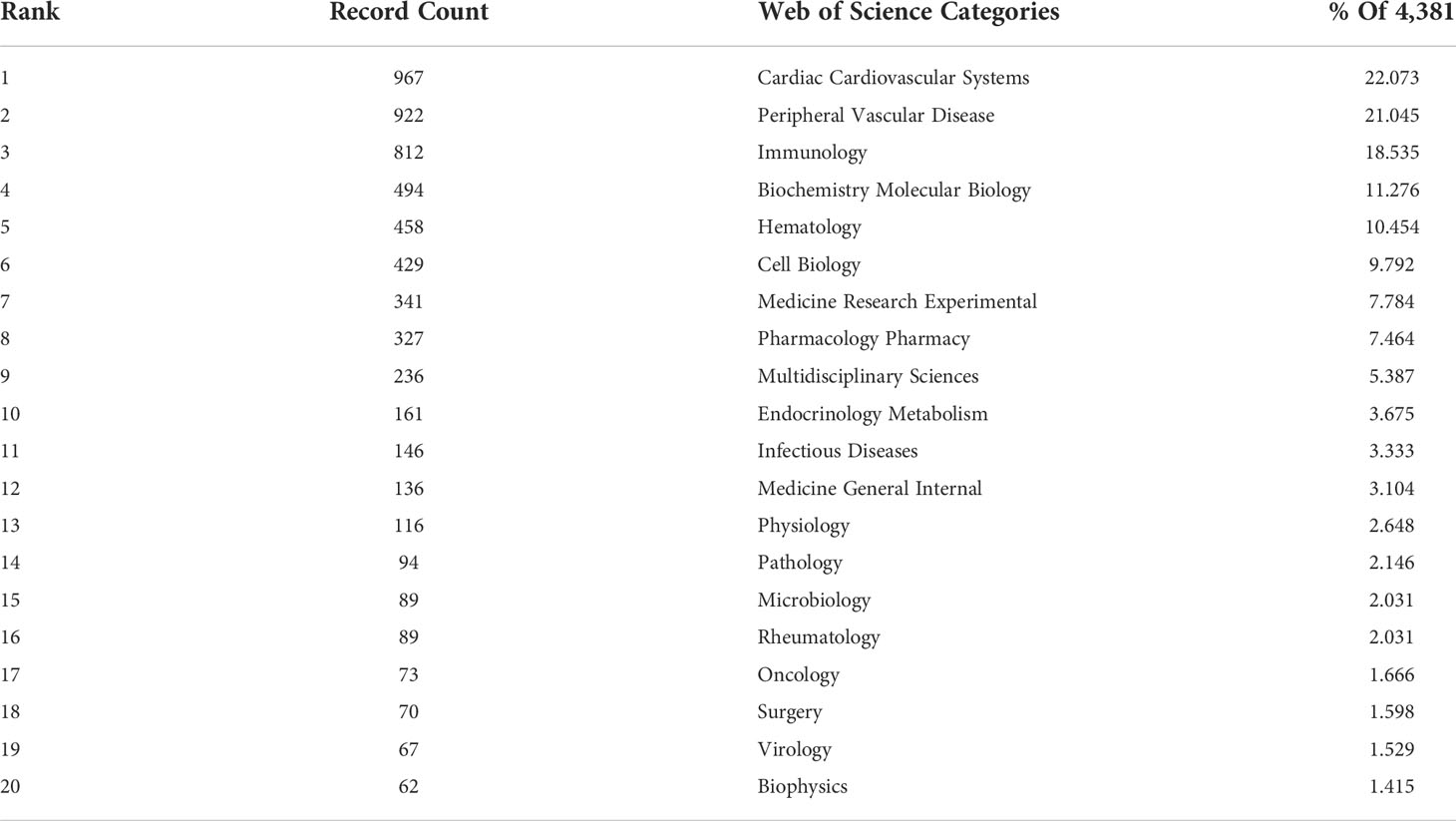
Table 5 Top 20 categories in T cell and AS.
As listed in Table 6, Arteriosclerosis Thrombosis and Vascular Biology was the journal with the highest number of publications in T cell and AS, followed by Atherosclerosis (179 publications), Plos One (139 publications), Circulation (131 publications), Cardiovascular Research (95 publications) and Circulation Research (95 publications). In co-citing journals, Circulation (39.918) was the journal with the highest impact factors (IF), followed by European Heart Journal (35.855), Circulation Research (23.213), and Cardiovascular Research (13.081). Among these journals, the IF of fifteen journals is greater than 10. Among them, the journal with the highest IF is New England Journal of Medicine (176.079), followed by Nature Reviews Immunology (108.555), Nature Medicine (87.241), Nature (69.504) and Science (63.741).
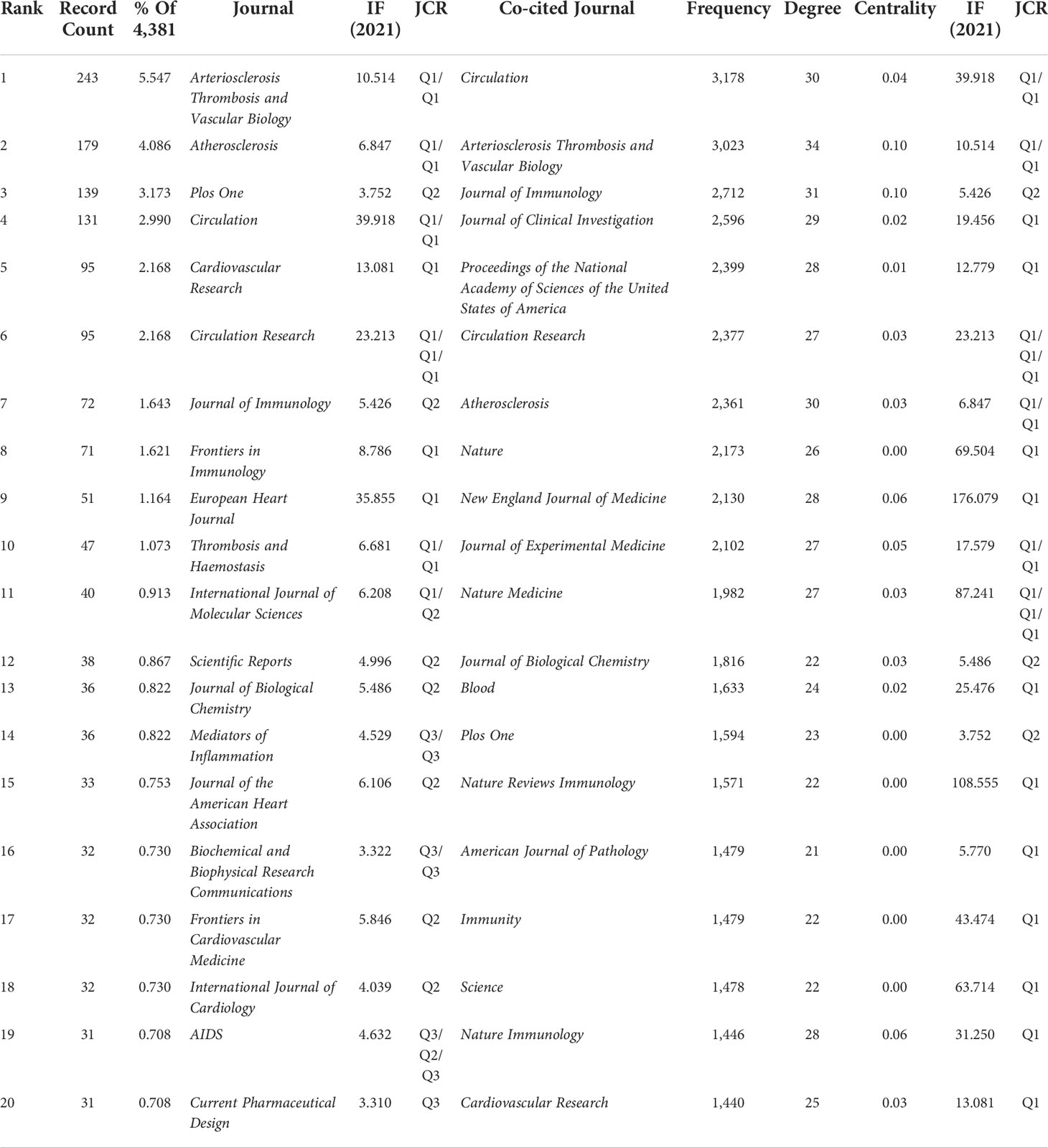
Table 6 Top 20 journals and co-cited journals in T cell and AS.
In Figure 5, dual map overlay of journals shows the distribution of topics. The citing journals are on the left, and the cited journals are on the right. The labels represent the disciplines covered by the journals, and the colored path represented the citation relationship. We can see the most important three paths. The two orange citation paths indicate that research in Molecular, Biology, Genetics journals and Health, Nursing, Medicine journals are frequently cited by Molecular/Biology/Immunology journals. The green citation path indicate that research in Molecular, Biology, Genetics journals is frequently cited by Medicine/Medical/Clinical journals.
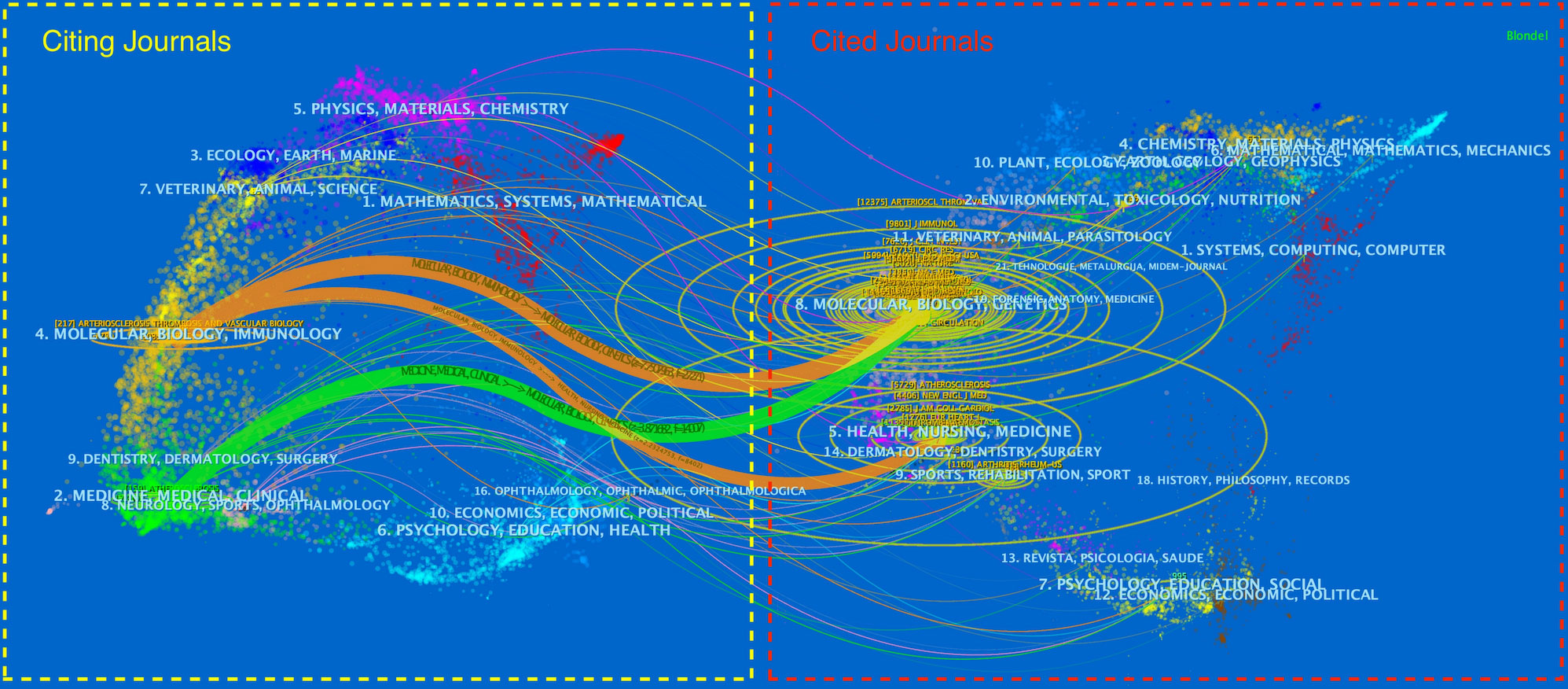
Figure 5 The dual-map overlay of journals in T cell and AS.
CiteSpace parameters were set as follows: time slicing (2004–2022), years per slice (1), node type (cited reference), selection criteria (top N=50), and no clipping. According to the set parameters, a network with 1,046 nodes, 4,674 connections, and 0.0086 density was obtained (Figure 6A). CiteSpace employs the purple-circled nodes to measure the importance of documents and determine the ten most-cited sources (Table 7). Co-citation analysis indicated that two references appeared in the reference list of a third citation article, establishing a co-citation relationship. The article “Inflammation, Atherosclerosis, and Coronary Artery Disease” (29) was the most cited, while “The immune system in atherosclerosis” (30) was the second most cited. The “Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease” (31) was the third most cited article. In CiteSpace, nodes with more than 0.1 mediation centrality become the key points (32). In Table 7, the centrality of “Depletion of FOXP3+ regulatory T cells promotes hypercholesterolemia and atherosclerosis” (35) was 0.11. Figure 6B presents the top 20 references with the strongest citation bursts. The strongest citation burst was for the 2005 article “Inflammation, Atherosclerosis, and coronary artery disease.” (29). This article has an intensity of 90.66.
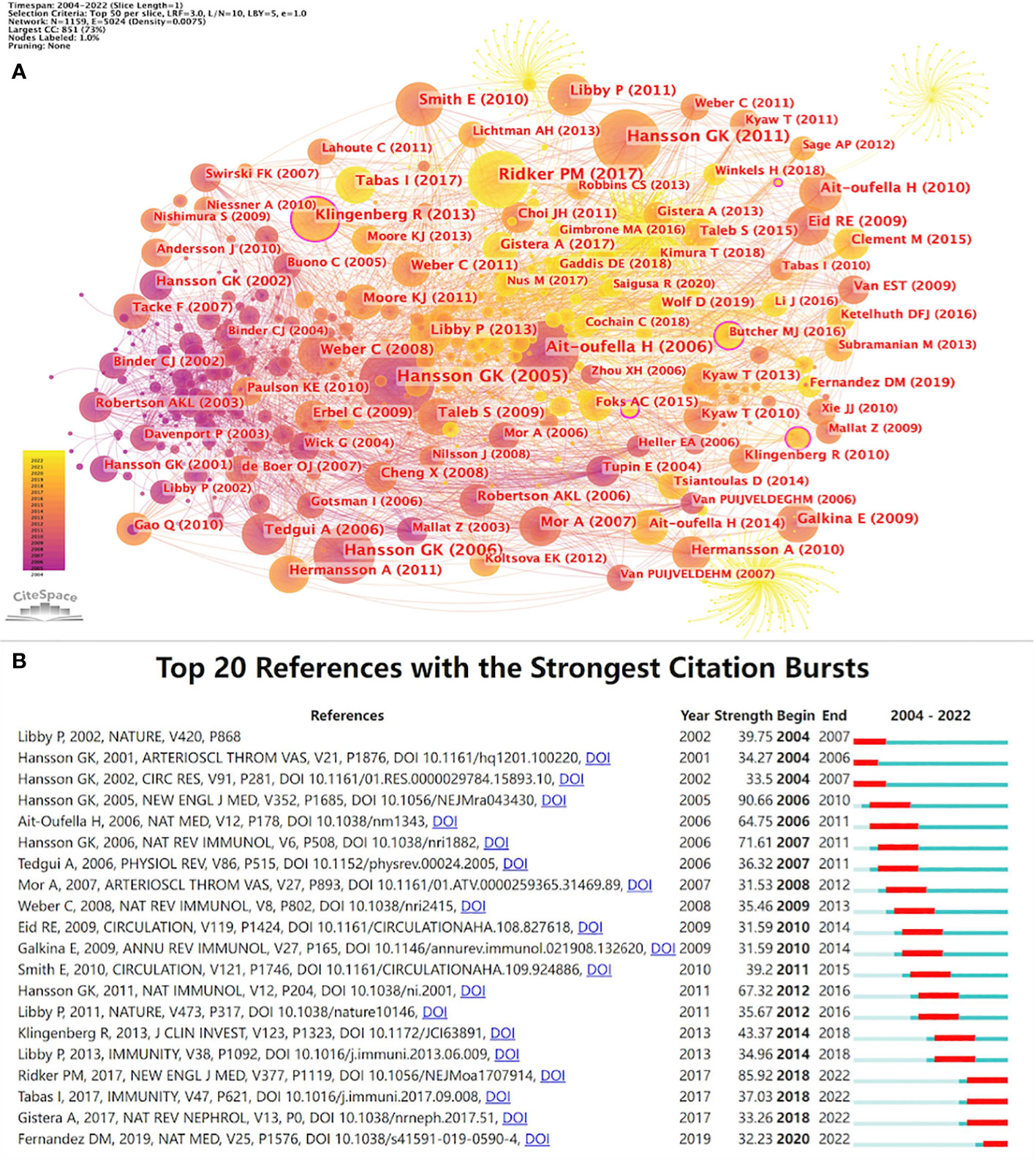
Figure 6 (A) References co-citation network in T cell and AS. (B) Top 20 references with the strongest citation bursts in T cell and AS.
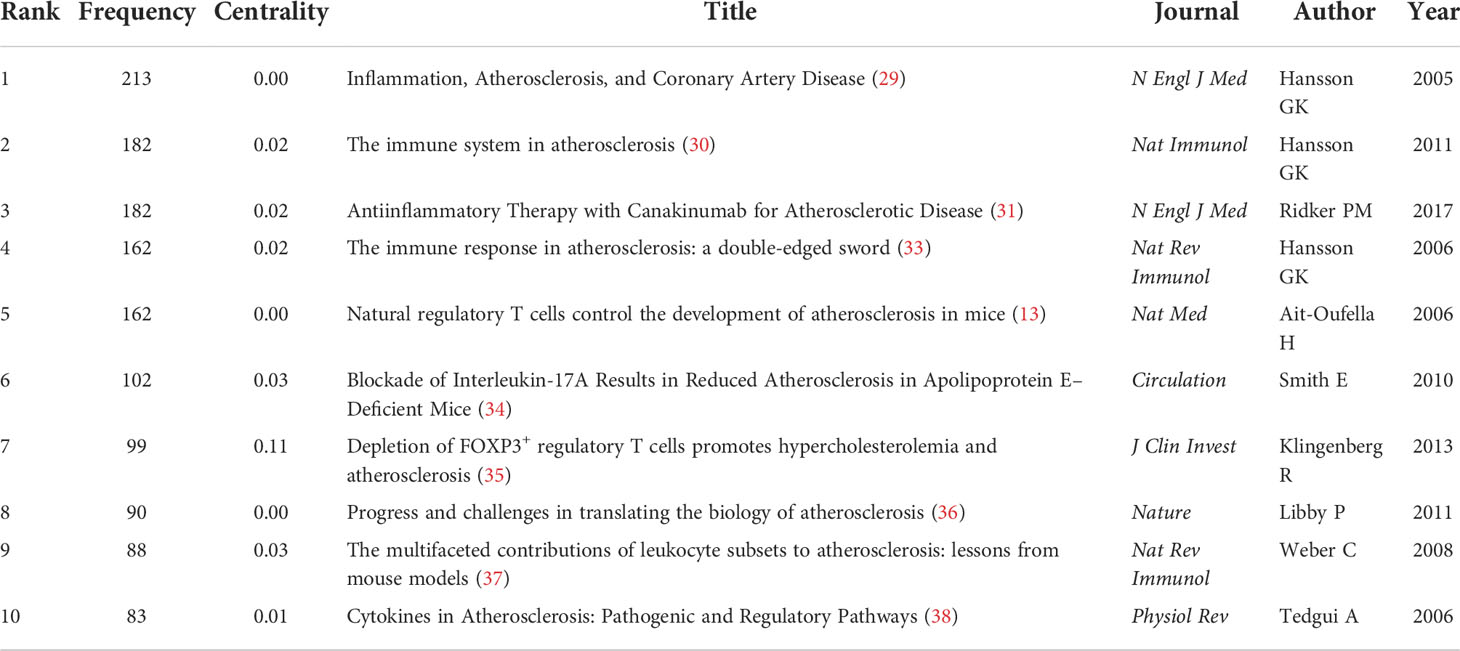
Table 7 Top 10 cited references of publications in T cell and AS.
Specifically, these are representative articles in T cell and AS. The article “Inflammation, Atherosclerosis, and Coronary Artery Disease” (29) is a review by Hansson GK published in The New England Journal of Medicine in 2005. This review highlights the importance of inflammation in the pathogenesis of atherosclerotic cardiovascular disease (ASCVD) from four aspects: the main characteristics of atherosclerotic lesions, the evolution of vulnerable plaques, and acute coronary syndrome (ACS), and treatment opportunities.
“The immune system in atherosclerosis” (30); this article is a review published in Nature Immunology by Hansson GK and Hermansson A in 2011. This review provides an overview of the role of innate and adaptive immune mechanisms in AS from ten aspects (LDL initiates vascular inflammation; a major role for innate immunity in atherosclerosis; adaptive immunity enters the scene; T lymphocytes: key participants in atherogenesis; role of helper T cell subsets; antigens of atherosclerosis; tolerance, and reactivity to LDL; metabolic regulation of immunity and inflammation; A difficult case for genetic epidemiology; atherosclerosis emphasizes the role of inflammation).
The article “Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease” (31) was published in The New England Journal of Medicine by Ridker PM et al. in 2017. The trial was a randomized, double-blind trial of canakinumab comparing three doses of canakinumab (50, 150, and 300 mg, given subcutaneously every three months) with a placebo. The results revealed that anti-inflammatory treatment with 150 mg canakinumab every three months, targeting the natural IL-1β immune pathway, resulted in a significantly lower recurrence rate of cardiovascular events than placebo, unrelated to reducing blood lipid level.
The centrality of the article “Depletion of FOXP3+ regulatory T cells promotes hypercholesterolemia and atherosclerosis” (35) is 0.11, indicating that the article is influential. This article was published by Klingenberg R et al. in Journal of Clinical Investigation in 2013. Through the chimeric DEREG/Ldlr–/– mouse model experiment, the authors confirmed that Foxp3+ Tregs have a substantial protective effect on AS, and the metabolism of plasma lipoprotein is partially regulated by immune regulation and showed that chronic inflammation could promote cardiovascular diseases (CVDs) by causing metabolic disorder. By mastering the articles with turning significance in this field, we can deeply study the research overview in this field.
As displayed in Table 8, in addition to atherosclerosis (2,696) and T cell (1,348), keywords with higher frequency in this study include inflammation (1,348), expression (774), regulatory T cells (699), activation (540), low-density lipoprotein (531), macrophage (469), coronary artery disease (446) and dendritic cells (432). Among these keywords, inflammation, activation, low-density lipoprotein, macrophage, coronary artery disease, and dendritic cells appeared more than 400 times, indicating that they are the focus of research.
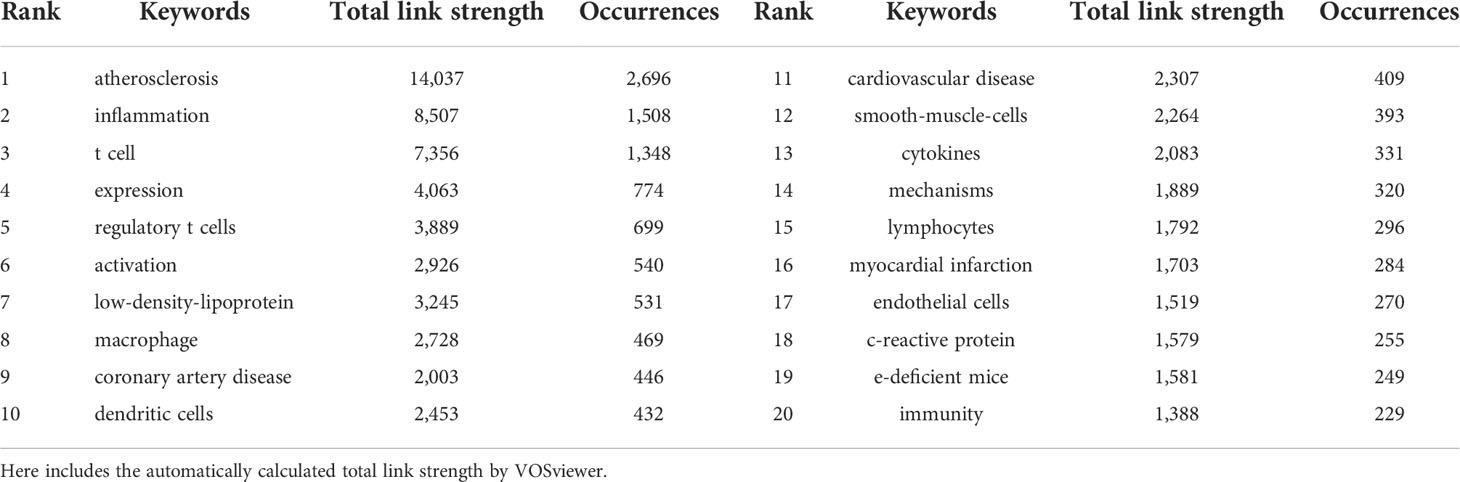
Table 8 Top 20 keywords in T cell and AS.
VOSviewer parameters were as follows: Method (Linlog/modularity) and a minimum number of occurrences of a keyword: 50. There were 11,731 keywords, with 142 keywords meeting the thresholds. For each of 142 keywords, the total strength of co-occurrence links with other keywords was calculated. Keywords with the greatest total link strength were selected. The keyword co-occurrence network graph (Figure 7A) displays that the thicker the connection between nodes, the higher the frequency of two keywords appearing together. Keywords formed four clusters, representing the four main research directions T cell and AS.
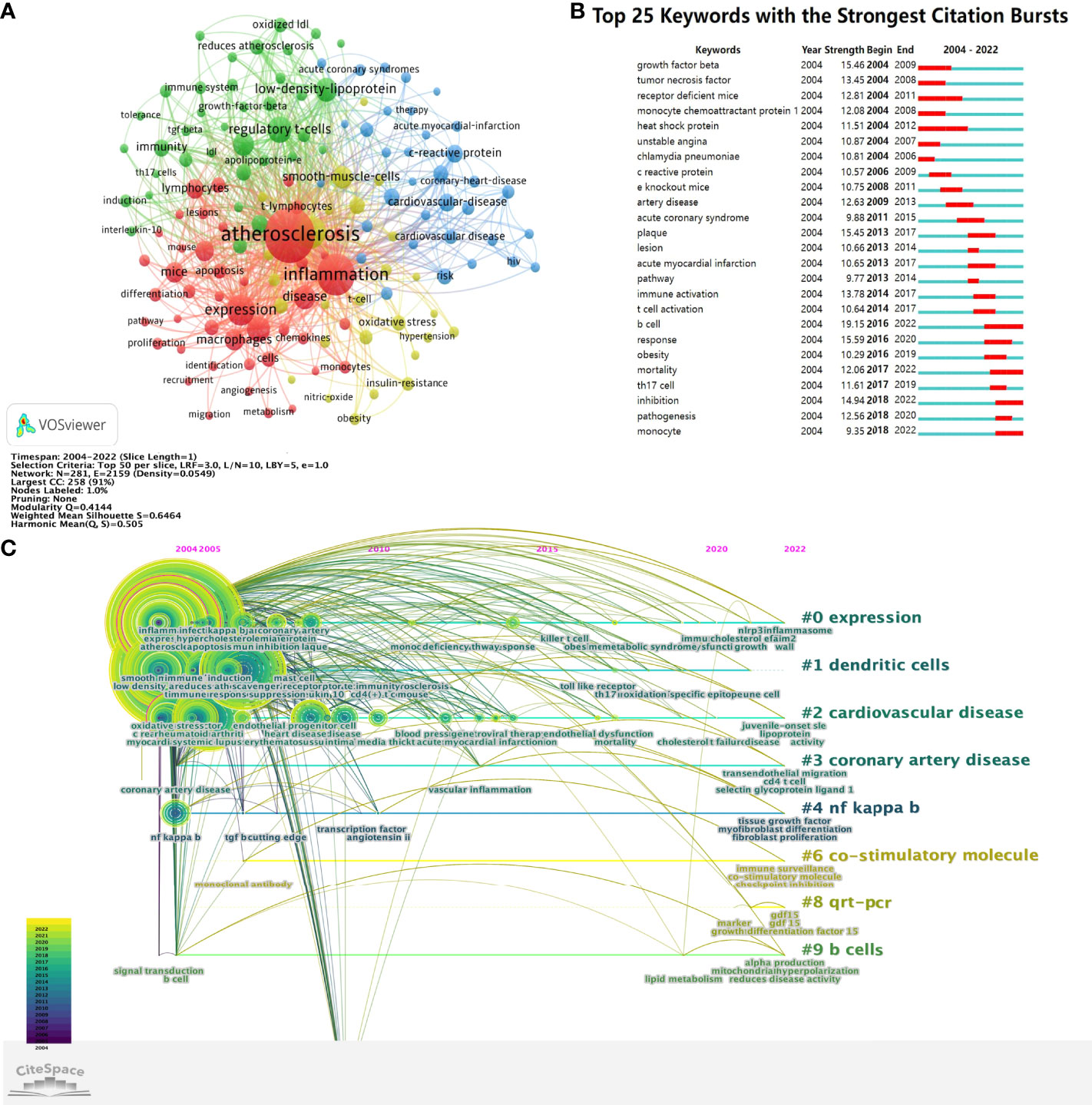
Figure 7 (A) The cluster of keywords in the studies of T cell and AS. (B) Top 25 keywords with the strongest citation bursts. (C) Timeline viewer related to T cell and AS.
The red cluster mainly includes atherosclerosis, inflammation, expression, macrophages, apoptosis, proliferation, angiogenesis, differentiation, monocytes, metabolism, migration, pathway, lymphocytes, t-lymphocytes, atherosclerotic lesions, recruitment, identification, activation, adhesion, atherogenesis, chemokines, cholesterol, deficiency, endothelium, hypercholesterolemia, immune, inhibition, lesions, leukocytes, macrophage, mechanisms, mice, pathogenesis, plaque, progression, protein, receptor, responses, and stains.
The green cluster mainly contains immunity, immune system, low-density-lipoprotein (LDL), IL-10, atherosclerosis reduction, TGF-β, regulatory t-cells (Tregs), apolipoprotein-e, tolerance, Th17 cells, induction, adaptive immunity, antibodies, autoimmunity, B-cells, CD4(+) T-cells, cytokines, deficient mice, dendritic cells, E-deficient mice, e-knockout mice, Foxp3+, transforming growth-factor-beta, human atherosclerotic plaques, immune-response, immunization, immunology, in-vivo, INF-γ, IL-17, oxidized LDL, receptor-deficient mice, and T cells.
The blue cluster mainly comprises cardiovascular disease, coronary heart disease, artery disease, coronary artery disease, cardiovascular events, heart disease, acute coronary syndrome, acute myocardial infarction, myocardial infarction, unstable angina, rheumatoid arthritis, HIV, stroke, and systemic-lupus-erythematosus.
The yellow cluster mainly consists of smooth muscle cells, endothelial cells, oxidative stress, endothelial dysfunction, gene expression, insulin resistance, T-cell, NO, MCP-1, TNF-α, NF-κB, TLRs, TNF, TNF-α, and INF-γ.
Based on the keywords co-citation network, we conducted the keywords emergent word detection. The top 25 keywords with the strongest citation bursts in T cell and AS are reported. As revealed in Figure 7B, the blue line denotes the time axis while the red segment on the blue time axis demonstrates the burst detection, indicating the start year, end year, and burst duration. Notably, B cell (19.150) had the strongest citation bursts, followed by a response (15.590), transforming growth factor-beta (15.460), plaque (15.450), inhibition (14.940), immune activation (13.780), tumor necrosis factor (13.450), receptor-deficient mice (12.810), artery disease (12.630), pathogenesis (12.560), and mortality (12.060). Based on the start time of emergence, it is revealed that transforming growth factor-beta, tumor necrosis factor, receptor-deficient mice, monocyte chemoattractant protein 1, heat shock protein, unstable angina, and chlamydia pneumoniae appeared early and were the subjects of early attention. B cell, mortality, inhibition, and monocyte are the current research frontiers in T cell and AS, and they are already in an explosive period.
Timeline viewer can show the dynamic evolution path of the research hotspots represented by the keywords, and explore the time characteristics of the research fields reflected by the clusters and the rise and fall process of the hotspot keywords research. Documents in the same cluster are placed on the same horizontal line, and the time is from left to right, from far to near. The number of documents in the same cluster highlights the abundance and importance of the research achievements in this cluster field. According to the CiteSpace parameters, a network with 281 nodes, 2,159 connections, and 0.0549 density was obtained (Figure 7C). Figure 7C intuitively shows the stage hotspots and development directions of T cell and AS research from the time dimension. Cluster ID is the number after clustering. The number is shown as # 0, # 1, # 2, etc. The larger the size of the cluster, the larger the number of members included in the cluster. Figure 7C shows eight clusters, which were expression, dendritic cells, cardiovascular disease, coronary artery disease, NF kappa b, co-stimulatory molecule, qrt-pcr, and b cells. From Figure 7C, we can see that the keywords involved in 2004 and 2005 are mainly inflammation, coronary artery disease, NF kappa b, singal transduction, b cell. The keywords involved in 2020-2022 are mainly NLRP3 inflammasome, toll-like receptors, transendothelial migration, cd4 t cell, selection glycoprotein ligand 1, fibroblast proliferation, mitochondrial hyperpolarization, checkpoint inhibition factor 15.
In this study, we analyzed T cell and AS documents and reviewed the research results and progress using CiteSpace and VOSviewer quantitative analysis software. The basic information of annual publication quantity, country, author, institution, discipline, and journal is quantitatively analyzed. According to the number of documents issued by T cell and AS, the number of documents published in this field from 2004 was 144, and the overall trend is increasing. The higher citations a paper has, the greater its impact on the field and the higher its quality. As Figure 2 displays, the number of citations in this field has annually increased. Based on the statistical analysis of the number of papers published by various countries/regions and institutions, it is possible to identify key countries/regions and research institutions that have published many T cell and AS documents and have greater influence and determine their cooperative relationship. USA, China, and Germany are the countries that mainly study T cell and AS. Sweden, USA, and Australia have relatively mature studies in T cell and AS. Among the top ten institutions, three are from the Netherlands, two are from the USA, and two are from France, with Harvard University being the institution with the most publications and the highest h-index. The cooperation between various countries and institutions is relatively close. Close cooperation and communication between countries and institutions are conducive to eliminating academic barriers and further developing T cell- and AS-related research.
From the top 10 authors, Hansson GK (97, 2.214%) is the most published author, followed by Weber C (78, 1.780%) and Nilsson J (70, 1.598%). It indicates that these three authors have made the most outstanding contribution in the field of T cell and AS. Professor Hansson GK from the Department of Medicine, Center for Molecular Medicine (G.K.H.) is the author with the highest h-index (39). H-index is a comprehensive quantitative index used to evaluate the quantity and level of academic output of researchers (40). Prof. Hansson GK reviewed the immune system’s role in AS and believed that immune response in AS is a double-edged sword (30, 33). Experimental and clinical knowledge of AS pathogenesis is elucidated from an immunological perspective (41, 42), and new treatments are sought (43). This was followed by Weber C from IPEK and Nilsson J from Department of Clinical Sciences Malmö, Lund University, Sweden. Weber C studied the critical role of chemokines in AS (44) and suggested that AS is a chronic inflammatory disease of arterial walls caused by chemokine-driven monocyte recruitment (45, 46). As small chemotactic cytokines, chemokines are key mediators and regulators of leukocyte trafficking during immune surveillance and inflammation (47, 48). Nilsson J has studied many important roles of regulatory T cells in AS, inhibiting autoimmunity development by controlling the activity of autoreactive T cells (49). The response of regulatory T cells to apolipoprotein B100-derived peptides reduces AS development and progression in mice (50, 51), and vaccination may be an effective strategy to prevent or regulate AS (52, 53). There are no authors whose centrality is greater than or equal to 0.10 among all authors, indicating that there are no authors with significant influence in this field.
According to the discipline distribution in Table 5, the discipline with the most articles about T cell and AS is Cardiac Cardiovascular Systems (967, 22.073%), Peripheral Vascular Disease (922, 21.045%), and Immunology (812, 18.535%). According to journal distribution in Table 6, the journals with the most articles on T cell and AS are Arteriosclerosis Thrombosis and Vascular Biology (243, 5.547%), followed by Atherosclerosis (179, 4.086%) and Plos One (139, 3.173%). Circulation and Arteriosclerosis Thrombosis and Vascular Biology were frequently co-cited. Among the top 20 in co-citing journals, 9 journals are located in Q1 JCR region, of which Circulation (39.918, Q1/Q1) has the highest IF. Among the top 20 in co-cited journals, 17 journals are in the JCR1 region, and 15 journals have IF greater than 10. The journal with the highest IF is New England Journal of Medicine (176.079). JCR profiles are journal-specific indicators related to impact factors, rankings, and quarters in categories (39). Analyzing the distribution of literature sources, it is helpful to find the core journals published in the relevant literature on T cell and AS and help scholars build scientific achievements. These indicate that many high quality and high impact journals are very interested in T cell and AS related research. These data will help future scholars select journals when submitting manuscripts related to T cell and AS. Figure 5 shows that papers published in Molecular, Biology, Genetics journals and Health, Nursing, Medicine journals are frequently cited in papers published in Molecular, Biology, Genetics journals and Medicine, Medical, Clinical journals. This means that current research on T cell and AS-related research is mainly focused on basic research and transitional medicine.
Most of the top ten references dealt with immune responses and inflammation, mainly because AS was previously thought to be due to the passive accumulation of cholesterol in the arterial wall (54). With increasing evidence that AS was gradually recognized as a chronic inflammatory disease in the late 1990s, innate and adaptive immune-inflammatory mechanisms are involved in all disease stages, in which T cells are critical in the immune response accompanying AS (55). The high burst signal of reference indicates the high intensity of interest and time interval (56). According to the 20 references with the strongest citation bursts, the most cited references in recent years is mainly related to the immune and inflammatory mechanism of AS. It was not until around 2000 that people realized that the inflammatory mechanism combined dyslipidemia with AS formation, and the dysfunction of inflammatory mediators inhibited AS formation in mice (54).
Analysis of high-frequency keywords reflects the hotspots in a particular research field. We used key co-occurrence analysis to determine the main directions and hotspots in T cell and AS, as well as to uncover the development and changes of its theme structure (57). Cluster analysis based on keywords, finally forming a cluster of four colors. Then, according to the analysis of the top 25 keywords with the strongest citation bursts, the research hotspots and frontiers in T cell and AS are determined, and its main contents are as follows:
According to keywords, the red cluster mainly clarifies the inflammatory mechanism of AS. It is well known that AS is a chronic inflammatory lesion of large and medium elastic arteries in the whole body (58), and inflammatory reaction runs through the whole process of AS occurrence and development (59). The study on the results of Canakinumab anti-inflammatory thrombosis (31), the cardiovascular inflammation reduction trial of non-specific anti-inflammatory treatment with methotrexate (60), and the cardiovascular outcome test of colchicine (61, 62) all exhibited anti-inflammatory effects. The potential value of inflammation in AS and coronary heart disease treatment. Currently, targeted therapeutic drugs for inflammatory factors have made preliminary progress, such as IL-1β; IL-6 is the most potential target for inflammatory targeted therapy of AS. By studying NF-κB, JAK/STAT, and other AS-related inflammatory signaling pathways can further understand AS pathogenesis. Studies have also revealed that powerful immunosuppressants or anti-inflammatory drugs may be attractive approaches for treating acute coronary syndromes, demonstrating that strategies to reduce inflammation may be a viable treatment for AS suppression (63). However, the role of inflammation in AS pathophysiology is complex, and the interaction mechanism between metabolic imbalance and immunomodulatory disorder continues to be further researched; thus, it is also the focus of current research.
The second cluster is mainly associated with the immune mechanism of AS. AS is the main pathological basis of ischemic heart, cerebrovascular and peripheral vascular diseases. The immune response is involved in each stage of AS—the formation of atherosclerotic plaques, the transformation from stable to unstable plaques, and the rupture of plaques (64). There is increasing evidence that innate and adaptive immunities can closely regulate AS occurrence (65). The innate immune response is the first line of defense of immune response and the basis of adaptive immune response. It mainly plays the role of scavenging damaged and apoptotic cells, antigen presentation, immunosuppression, and protecting the host from foreign microorganisms (66). Adaptive immune response, the center of immune memory and tolerance development, can recognize presented antigens and release antibodies (62). The main feature of AS is that endothelial injury releases adhesion molecules, triggers innate immune response dominated by monocytes and macrophages, and then dendritic cells and macrophages present antigens to cause adaptive immune response dominated by lymphocytes. The inflammatory mechanism of AS is based on numerous immunoactivity cells found in AS lesions, such AS congenital immune cells (monocytes, macrophages, dendritic cells, etc.), adaptive immune cells (T cells, B cells, etc.), and various cytokines produced. Examples include IL, tumor necrosis factor (TNF), interferon (IFN), transforming growth factor (TGF), colony-stimulating factor (CSF), and chemokines (67). Among them, pro-inflammatory cytokines such as TNF-α, IL-1β, monocyte chemoattractant protein-1 (MCP-1), IL-6, IL-1, IL-12, and type I IFN (IFN-γ, β) and accelerate AS progression; Anti-inflammatory cytokines such as IL-10 and TGF-β, Arginase-1 (Arg-1), forkhead or winged-helix transcription factor-3(FOXP3) and IL-5 improved AS development. In addition, antibodies secreted by immune cells (immunoglobulin E (IgE), IgG, and IgM) and other specific binding-related antigens (heat shock protein (HSP) and oxidized low-density lipoprotein (ox-LDL)) play an immunomodulatory role. Studies have revealed that blocking TGF-β signaling pathway in ApoE-/- mouse T cells promote AS (68). Therefore, AS occurrence and development can be delayed, reduced, or even reversed by further regulation of immune regulatory cells and cytokines from the perspective of inflammation and interruption of key targets of immune-inflammatory response (69).
In addition, the cluster involves model animals for studying AS. Clinical studies, population studies, and cell culture experiments have provided important clues to AS pathogenesis (70). However, experiments on animals are required to dissect the pathogenic steps and determine cause and effect. Under normal conditions, laboratory mice do not develop AS.
However, ApoE-/- mouse causes severe hypercholesterolemia and spontaneous AS. LDL-/- mouse also develops AS, especially in mice fed a high-fat diet. Generally, these knockout mice have been used to study the relationship between hypercholesterolemia and AS and evaluate the impact of other genes and gene products on these diseases. By mating these mice with knockout mice lacking immunoregulatory genes, it is possible to elucidate the role of immune and inflammatory mechanisms in AS (29). In summary, the immune system is critical in AS occurrence and development, and more immunotherapy strategies will be applied to treat AS-related diseases in the future. Further improving the theory of AS and the prognosis of patients with related diseases is one of the hotspots of current research.
The blue cluster mainly involves AS-related diseases. AS, the underlying pathological basis of cardiovascular and cerebrovascular diseases, is prevalent in the elderly, and its incidence increases with age, dominating global mortality and disability statistics (3). The pathological process of AS progresses slowly. It mainly demonstrates clinical symptoms when the coronary lumen is seriously narrowed, and acute thrombosis seriously blocks the blood flow. Blocking blood flow to the heart will lead to coronary heart disease, blocking blood flow to the brain will cause ischemic stroke, and reducing blood flow at the end of the limb will result in peripheral vascular disease. AS is prevalent in the elderly, and its incidence increases with age. In addition, studies have revealed that premature AS is one of the main reasons that affect the quality of life of patients with systemic lupus erythematosus (SLE) and leading to death in SLE patients, and there is an increasing trend (71). The increased prevalence of AS in SLE patients is thought to be due to a combination of traditional risk factors and autoimmune-mediated inflammatory responses (72).
The yellow cluster mainly involves AS-related cytokines. Various cytokines and related substances are involved in AS occurrence and development (73) and are critical in AS occurrence and development. Cytokines are a very diverse class of molecules, including more than 100 secretory factors, which can be divided into several categories: ILs, tumor necrosis factors (TNFs), interferons (IFNs), transforming growth factors (TGFs), colonies Stimulatory factor (CSF), and various chemokines (CXCL). The expression of cytokines can be abnormal before morphological changes of AS. Therefore, detecting cytokines can provide more effective information for discovery, diagnosis, and curative effect evaluation of AS-related diseases. Studies have revealed that most communication between monocytes/macrophages and vascular smooth muscle cells is through immune mediators (74), with TNF-α, IL-1β, IL-6, and MCP-1 in AS and plays a major role in arterial wall inflammation (75). With the deepening and development of research, inflammatory factors are critical in AS-related diseases. However, discovering new AS-associated cytokines and the related mechanisms remains challenging.
The first research frontier may be B cell. It is well known that the proliferation and activation status of B cells, in addition to T cells, are critical factors in CVD risk. B cells are involved in the systemic and local immune responses of AS arteries through antigen presentation, cytokine production, and immunoglobulin synthesis (76, 77). The specific relationship between B cells and AS depends largely on the subset of B cells and their functional targeting (78, 79). B cells were divided into B1 and B2 subsets. In mature B cells, B2 cells dominated.
B1 cells assume the natural defense function against common pathogens. Accumulating IgM antibodies derived from B1 cells in AS lesions can reduce the number of apoptotic cells and the necrotic core size to reduce the severity of inflammation and block the uptake of ox-LDL by macrophages (80), which has a protective effect on AS. Studies have indicated that transplantation of B cell-deficient bone marrow into irradiated LDLR-/- mice exacerbates AS (81). Subsequent studies further confirmed that the lack of B1a cells and the consequent decrease in IgM are the leading causes of the loss of B cell effect (82). This study also confirmed that IgM released by B1a cells protects the vascular wall by inhibiting necrotic core formation. In addition, studies have demonstrated that IgM inhibits ox-LDL uptake by macrophages, thereby inhibiting myeloid cell inflammation (83). Similarly, the response of IgM secreted by B1b cells to oxidation-specific epitopes also has a protective effect on AS (84). B2 cells are further divided into marginal zone B cells and follicular B cells. Marginal zone B cells play an anti-AS function, while follicular B cells aggravate AS (85, 86). Inhibiting B2 cells is protective against AS (87, 88).
In addition, there are regulatory B cells (Bregs), accounting for only a small part of B cells, but can still inhibit vascular inflammation by producing anti-inflammatory cytokine IL-10 to produce the effect of anti-AS (89).
In conclusion, the complex role of B cells in AS has not yet been fully and accurately understood. Therefore, it is very necessary to further explore the mechanism of B cells regulating AS to gain a more comprehensive understanding of AS. Simultaneously, B cell-targeted therapy of AS is an important research direction in the future.
The second research frontier may be mortality. Cardiovascular and cerebrovascular diseases caused by AS are now the leading cause of death worldwide, and morbidity and mortality are rising (90). Therefore, the related understanding of mortality will still be future research hotspot and frontier.
The third research frontier may be inhibition. The wide clinical application of immune checkpoint inhibitors (ICIs) increases the risk of immune-related adverse events in the cardiovascular system. In cancer patients, the adverse effects of ICIs on AS-related cardiovascular disease may lead to acute cardiovascular events (AVEs) such as myocardial infarction (91). Therefore, conducting predictive studies to increase clinician awareness of AVEs caused by ICIs through risk stratification is essential in preventing these adverse events.
The fourth research frontier may be monocytes. Monocytes are an important part of the body’s innate immune system and the leukocytes recruited at the early stage of AS lesions, which can further differentiate into macrophages to promote inflammation. Macrophages phagocytose ox-LDL accumulation in the vascular wall to form foam cells that initiate necrotic core formation in the plaque, further exacerbating atherosclerotic lesions. At present, human monocytes can be divided into three groups according to the expression of surface markers CD14 and CD16: classical (CD14++CD16-), intermediate (CD14++CD16+), and non-classical (CD14+CD16++) monocytes (92). Monocytes in mouse circulating blood include two main subtypes: Ly6C(hi) and Ly6C(low). Studies have revealed that hypercholesterolemia can trigger monocyte increase in mice. Reversing hypercholesterolemia in mice can prevent monocyte recruitment and reduce macrophages in plaques, suggesting that continuous monocyte recruitment is necessary for plaque maintenance and progress (93). The capture and rolling of circulating monocytes depend on a series of chemokines expressed by vascular endothelial cells, such as CCL5, CXCL1, and P-selectin. The entry of monocytes from the endothelium into AS plaques requires the participation of chemokines secreted by endothelial cells, macrophages, and smooth muscle cells. The most important three pairs of chemokine receptors-chemokines are CCR2-CCL2, CX3CR1-CX3CRL1, and CCR5-CCL5 (94). Combined inhibition of these three chemokine axes could prevent the increase of monocytes in hyperlipidemic mice and reduce the area of AS plaque in ApoE-/- mice by approximately 90% (95).
In summary, B cell, mortality, inhibition, and monocyte are the frontiers of research in this field and are currently in an explosive phase.
First, to ensure high-quality bibliometric analysis, the analysis of this study is based on the articles in WoSCC database, which is the most famous database of scientific publications on many research topics. Numerous studies have been omitted because they are published in non-SCI journals or other databases. Second, CiteSpace and VOSviewer cannot completely replace system retrieval. Third, bibliometrics cannot assess the quality of individual studies because citation metrics are time-dependent, implying that more recent articles may be less cited than earlier articles, mainly due to publication date (96). These limitations may slightly impact the overall results but are unlikely to change the main trends presented in this paper. Overall, our study provides a foundation for understanding research topics, hotspots, and development trends in T cell and AS.
Through detailed bibliometric analysis in T cell and AS, this study evaluates the literature information of different years, countries, institutions, authors, disciplines, and journals and analyzes the theme development and future research hotspots. Our study observed that the field began to garner attention in 2004. Our study provides basic information about research in this field and identifies potential partners for interested researchers. Current research hotspots mainly include the inflammatory mechanism, and immune mechanisms, related diseases, and related cytokines of AS. Currently, B cell, mortality, inhibition, and monocyte are the frontiers of research in this field and are currently emerging.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
NW and YX designed the study. YL, JS, and XZ collected the data. NW, YX, and YY re-examined the data. NW, YX, and QS analyzed the data. NW and YX wrote the manuscript. YH and HZ reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
The authors thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Moreno PR, Sanz J, Fuster V. Atherosclerosis. Curr Mol Med (2006) 6(5):437–8. doi: 10.2174/156652406778018662
2. Wu MY, Li CJ, Hou MF, Chu PY. New insights into the role of inflammation in the pathogenesis of atherosclerosis. Int J Mol Sci (2017) 18(10):2034. doi: 10.3390/ijms18102034
3. Roy P, Orecchioni M, Ley K. How the immune system shapes atherosclerosis: roles of innate and adaptive immunity. Nat Rev Immunol (2022) 22(4):251–65. doi: 10.1038/s41577-021-00584-1
4. Falk E. Pathogenesis of atherosclerosis. J Am Coll Cardiol (2006) 47(8 Suppl):C7–12. doi: 10.1016/j.jacc.2005.09.068
5. Libby P. The changing landscape of atherosclerosis. Nature (2021) 592(7855):524–33. doi: 10.1038/s41586-021-03392-8
6. Thomas H, Diamond J, Vieco A, Chaudhuri S, Shinnar E, Cromer S, et al. Global atlas of cardiovascular disease 2000-2016: The path to prevention and control. Glob Heart (2018) 13(3):143–63. doi: 10.1016/j.gheart.2018.09.511
7. Tabas I, Lichtman AH. Monocyte-macrophages and T cells in atherosclerosis. Immunity (2017) 47(4):621–34. doi: 10.1016/j.immuni.2017.09.008
8. Saigusa R, Winkels H, Ley K. T Cell subsets and functions in atherosclerosis. Nat Rev Cardiol (2020) 17(7):387–401. doi: 10.1038/s41569-020-0352-5
9. Wolf D, Ley K. Immunity and inflammation in atherosclerosis. Circ Res (2019) 124(2):315–27. doi: 10.1161/circresaha.118.313591
10. Winkels H, Ehinger E, Vassallo M, Buscher K, Dinh HQ, Kobiyama K, et al. Atlas of the immune cell repertoire in mouse atherosclerosis defined by single-cell RNA-sequencing and mass cytometry. Circ Res (2018) 122(12):1675–88. doi: 10.1161/CIRCRESAHA.117.312513
11. Lahoute C, Herbin O, Mallat Z, Tedgui A. Adaptive immunity in atherosclerosis: mechanisms and future therapeutic targets. Nat Rev Cardiol (2011) 8(6):348–58. doi: 10.1038/nrcardio.2011.62
12. Klingenberg R, Gerdes N, Badeau RM, Gisterå A, Strodthoff D, Ketelhuth DF, et al. Depletion of FOXP3+ regulatory T cells promotes hypercholesterolemia and atherosclerosis. J Clin Invest (2013) 123(3):1323–34. doi: 10.1172/JCI63891
13. Ait-Oufella H, Salomon BL, Potteaux S, Robertson AK, Gourdy P, Zoll J, et al. Natural regulatory T cells control the development of atherosclerosis in mice. Nat Med (2006) 12(2):178–80. doi: 10.1038/nm1343
14. Mor A, Planer D, Luboshits G, Afek A, Metzger S, Chajek-Shaul T, et al. Role of naturally occurring CD4+ CD25+ regulatory T cells in experimental atherosclerosis. Arterioscler Thromb Vasc Biol (2007) 27(4):893–900. doi: 10.1161/01.ATV.0000259365.31469.89
15. Ma D, Guan B, Song L, Liu Q, Fan Y, Zhao L, et al. A bibliometric analysis of exosomes in cardiovascular diseases from 2001 to 2021. Front Cardiovasc Med (2021) 8:734514. doi: 10.3389/fcvm.2021.734514
16. Ellegaard O, Wallin JA. The bibliometric analysis of scholarly production: How great is the impact? Scientometrics (2015) 105(3):1809–31. doi: 10.1007/s11192-015-1645-z
17. Rondanelli M, Perna S, Peroni G, Guido D. A bibliometric study of scientific literature in scopus on botanicals for treatment of androgenetic alopecia. J Cosmet Dermatol (2016) 15(2):120–30. doi: 10.1111/jocd.12198
18. Smith DR. Bibliometrics, dermatology and contact dermatitis. Contact Dermatitis (2008) 59(3):133–6. doi: 10.1111/j.1600-0536.2008.01405.x
19. Chandra SP, Singh A, Goyal N, Laythalling RK, Singh M, Kale SS, et al. Analysis of changing paradigms of management in 179 patients with spinal tuberculosis over a 12-year period and proposal of a new management algorithm. World Neurosurg (2013) 80(1-2):190–203. doi: 10.1016/j.wneu.2012.12.019
20. Pu QH, Lyu QJ, Su HY. Bibliometric analysis of scientific publications in transplantation journals from mainland China, Japan, south Korea and Taiwan between 2006 and 2015. BMJ Open (2016) 6(8):e011623. doi: 10.1136/bmjopen-2016-011623
21. Chen C. Searching for intellectual turning points: Progressive knowledge domain visualization. Proc Natl Acad Sci (2004) 101(Supplement 1):5303–10. doi: 10.1073/pnas.0307513100
22. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
23. Cobo MJ, López-Herrera AG, Herrera-Viedma E, Herrera F. Science mapping software tools: Review, analysis, and cooperative study among tools[J]. J Am Soc Inf Sci Technol (2014) 62(7):1382–402. doi: 10.1002/asi.21525
24. Liu X, Zhao S, Tan L, Tan Y, Wang Y, Ye Z, et al. Frontier and hot topics in electrochemiluminescence sensing technology based on CiteSpace bibliometric analysis. Biosens Bioelectron (2022) 201:113932. doi: 10.1016/j.bios.2021.113932
25. Chen C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol (2006) 57(3):359–77. doi: 10.1002/asi.20317
26. Perianesrodriguez LW A, Eck NJV. L egghe constructing bibliometric networks: A comparison between full and fractional counting. J Informetr (2016) 10(4):1178–95. doi: 10.1016/j.joi.2016.10.006
27. Zhang L, Ye X, Ye Y. Application comparison of information visualization software CiteSpace and VOSviewer. J Inf Resour Manage (2011) 01):95–8. doi: 10.13365/j.jirm.2011.01.017
28. Qin Y, Zhang Q, Liu Y. Analysis of knowledge bases and research focuses of cerebral ischemia-reperfusion from the perspective of mapping knowledge domain. Brain Res Bull (2020) 156:15–24. doi: 10.1016/j.brainresbull.2019.12.004
29. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med (2005) 352(16):1685–95. doi: 10.1056/NEJMra043430
30. Hansson GK, Hermansson A. The immune system in atherosclerosis. Nat Immunol (2011) 12(3):204–12. doi: 10.1038/ni.2001
31. Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med (2017) 377(12):1119–31. doi: 10.1056/NEJMoa1707914
32. Henry S. Co-Citation in the scientific literature: A new measure of the relationship between two documents. J Am Soc Inf Sci (1973) 24(4):265–7. doi: 10.1002/asi.4630240406
33. Hansson GK, Libby P. The immune response in atherosclerosis: A double-edged sword. Nat Rev Immunol (2006) 6(7):508–19. doi: 10.1038/nri1882
34. Smith E, Prasad KM, Butcher M, Dobrian A, Kolls JK, Ley K, et al. Blockade of interleukin-17A results in reduced atherosclerosis in apolipoprotein e-deficient mice. Circulation (2010) 121(15):1746–55. doi: 10.1161/circulationaha.109.924886
35. Klingenberg R, Gerdes N, Badeau RM, Gisterå A, Strodthoff D, Ketelhuth DF, et al. Depletion of FOXP3+ regulatory T cells promotes hypercholesterolemia and atherosclerosis. J Clin Invest (2013) 123(3):1323–34. doi: 10.1172/jci63891
36. Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature (2011) 473(7347):317–25. doi: 10.1038/nature10146
37. Weber C, Zernecke A, Libby P. The multifaceted contributions of leukocyte subsets to atherosclerosis: lessons from mouse models. Nat Rev Immunol (2008) 8(10):802–15. doi: 10.1038/nri2415
38. Tedgui A, Mallat Z. Cytokines in atherosclerosis: pathogenic and regulatory pathways. Physiol Rev (2006) 86(2):515–81. doi: 10.1152/physrev.00024.2005
39. Wang L, Feng W, Duan J, Liang J. Pharmacovigilance bibliometrics: Visualizing thematic development in the category of pharmacology and pharmacy in web of science. Front Pharmacol (2021) 12:731757. doi: 10.3389/fphar.2021.731757
40. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U.S.A. (2005) 102(46):16569–72. doi: 10.1073/pnas.0507655102
41. Gisterå A, Hansson GK. The immunology of atherosclerosis. Nat Rev Nephrol (2017) 13(6):368–80. doi: 10.1038/nrneph.2017.51
42. Andersson J, Libby P, Hansson GK. Adaptive immunity and atherosclerosis. Clin Immunol (2010) 134(1):33–46. doi: 10.1016/j.clim.2009.07.002
43. Klingenberg R, Hansson GK. Treating inflammation in atherosclerotic cardiovascular disease: emerging therapies. Eur Heart J (2009) 30(23):2838–44. doi: 10.1093/eurheartj/ehp477
44. van der Vorst EP, Döring Y, Weber C. Chemokines and their receptors in atherosclerosis. J Mol Med (2015) 93(9):963–71. doi: 10.1007/s00109-015-1317-8
45. Zernecke A, Shagdarsuren E, Weber C. Chemokines in atherosclerosis: An update. Arterioscler Thromb Vasc Biol (2008) 28(11):1897–908. doi: 10.1161/atvbaha.107.161174
46. Krohn R, Raffetseder U, Bot I, Zernecke A, Shagdarsuren E, Liehn EA, et al. Y-box binding protein-1 controls CC chemokine ligand-5 (CCL5) expression in smooth muscle cells and contributes to neointima formation in atherosclerosis-prone mice. Circulation (2007) 116(16):1812–20. doi: 10.1161/circulationaha.107.708016
47. Koenen RR, Weber C. Chemokines: established and novel targets in atherosclerosis. EMBO Mol Med (2011) 3(12):713–25. doi: 10.1002/emmm.201100183
48. Schober A, Bernhagen J, Weber C. Chemokine-like functions of MIF in atherosclerosis. J Mol Med (2008) 86(7):761–70. doi: 10.1007/s00109-008-0334-2
49. Nilsson J, Wigren M, Shah PK. Regulatory T cells and the control of modified lipoprotein autoimmunity-driven atherosclerosis. Trends Cardiovasc Med (2009) 19(8):272–6. doi: 10.1016/j.tcm.2010.02.010
50. Klingenberg R, Lebens M, Hermansson A, Fredrikson GN, Strodthoff D, Rudling M, et al. Intranasal immunization with an apolipoprotein b-100 fusion protein induces antigen-specific regulatory T cells and reduces atherosclerosis. Arterioscler Thromb Vasc Biol (2010) 30(5):946–52. doi: 10.1161/atvbaha.109.202671
51. Herbin O, Ait-Oufella H, Yu W, Fredrikson GN, Aubier B, Perez N, et al. Regulatory T-cell response to apolipoprotein B100-derived peptides reduces the development and progression of atherosclerosis in mice. Arterioscler Thromb Vasc Biol (2012) 32(3):605–12. doi: 10.1161/atvbaha.111.242800
52. Shah PK, Chyu KY, Dimayuga PC, Nilsson J. Vaccine for atherosclerosis. J Am Coll Cardiol (2014) 64(25):2779–91. doi: 10.1016/j.jacc.2014.10.018
53. Hansson GK, Nilsson J. Vaccination against atherosclerosis? induction of atheroprotective immunity. Semin Immunopathol (2009) 31(1):95–101. doi: 10.1007/s00281-009-0151-x
54. Libby P. Inflammation in atherosclerosis. Nature (2002) 420(6917):868–74. doi: 10.1038/nature01323
55. Libby P, Hansson GK. From focal lipid storage to systemic inflammation: JACC review topic of the week. J Am Coll Cardiol (2019) 74(12):1594–607. doi: 10.1016/j.jacc.2019.07.061
56. Kleinberg J. Bursty and hierarchical structure in streams. Data Min Knowl Discovery (2003) 7(4):373–97. doi: 10.1023/A:1024940629314
57. Guo S, Wang L, Xie Y, Luo X, Zhang S, Xiong L, et al. Bibliometric and visualized analysis of stem cells therapy for spinal cord injury based on web of science and CiteSpace in the last 20 years. World Neurosurg (2019) 132:e246–e58. doi: 10.1016/j.wneu.2019.08.191
58. Li B, Li W, Li X, Zhou H. Inflammation: A novel therapeutic Target/Direction in atherosclerosis. Curr Pharm Des (2017) 23(8):1216–27. doi: 10.2174/1381612822666161230142931
59. K L. Role of the adaptive immune system in atherosclerosis. Biochem Soc Trans (2020) 48(5):2273–81. doi: 10.1042/bst20200602
60. Ridker PM, Everett BM, Pradhan A, MacFadyen JG, Solomon DH, Zaharris E, et al. Low-dose methotrexate for the prevention of atherosclerotic events. N Engl J Med (2019) 380(8):752–62. doi: 10.1056/NEJMoa1809798
61. Tardif JC, Kouz S, Waters DD, Bertrand OF, Diaz R, Maggioni AP, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med (2019) 381(26):2497–505. doi: 10.1056/NEJMoa1912388
62. Bouabdallaoui N, Tardif JC, Waters DD, Pinto FJ, Maggioni AP, Diaz R, et al. Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the colchicine cardiovascular outcomes trial (COLCOT). Eur Heart J (2020) 41(42):4092–9. doi: 10.1093/eurheartj/ehaa659
63. Roy P, Orecchioni M, Ley K. How the immune system shapes atherosclerosis: roles of innate and adaptive immunity. Nat Rev Immunol (2022) 22(4):251–65. doi: 10.1038/s41577-021-00584-1
64. Sasaki N, Yamashita T, Kasahara K, Takeda M, Hirata K. Regulatory T cells and tolerogenic dendritic cells as critical immune modulators in atherogenesis. Curr Pharm Des (2015) 21(9):1107–17. doi: 10.2174/1381612820666141013142518
65. Herrero-Fernandez B, Gomez-Bris R, Somovilla-Crespo B, Gonzalez-Granado JM. Immunobiology of atherosclerosis: A complex net of interactions. Int J Mol Sci (2019) 20(21):5293. doi: 10.3390/ijms20215293
66. Zarif JC, Hernandez JR, Verdone JE, Campbell SP, Drake CG, Pienta KJ. A phased strategy to differentiate human CD14+monocytes into classically and alternatively activated macrophages and dendritic cells. BioTechniques (2016) 61(1):33–41. doi: 10.2144/000114435
67. Fatkhullina AR, Peshkova IO, Koltsova EK. The role of cytokines in the development of atherosclerosis. Biochem (Mosc) (2016) 81(11):1358–70. doi: 10.1134/s0006297916110134
68. Robertson AK, Rudling M, Zhou X, Gorelik L, Flavell RA, Hansson GK. Disruption of TGF-beta signaling in T cells accelerates atherosclerosis. J Clin Invest (2003) 112(9):1342–50. doi: 10.1172/jci18607
69. Ait-Oufella H, Sage AP, Mallat Z, Tedgui A. Adaptive (T and b cells) immunity and control by dendritic cells in atherosclerosis. Circ Res (2014) 114(10):1640–60. doi: 10.1161/circresaha.114.302761
70. Breslow JL. Mouse models of atherosclerosis. Science (1996) 272(5262):685–8. doi: 10.1126/science.272.5262.685
71. Li D, Yoshida K, Feldman CH, Speyer C, Barbhaiya M, Guan H, et al. Initial disease severity, cardiovascular events and all-cause mortality among patients with systemic lupus erythematosus. Rheumatol (Oxford) (2020) 59(3):495–504. doi: 10.1093/rheumatology/kez288
72. Cinoku II, Mavragani CP, Moutsopoulos HM. Atherosclerosis: Beyond the lipid storage hypothesis. Role Autoimmun Eur J Clin Invest (2020) 50(2):e13195. doi: 10.1111/eci.13195
73. Hong LZ, Xue Q, Shao H. Inflammatory markers related to innate and adaptive immunity in atherosclerosis: Implications for disease prediction and prospective therapeutics. J Inflamm Res (2021) 14:379–92. doi: 10.2147/jir.S294809
74. Ramel D, Gayral S, Sarthou MK, Augé N, Nègre-Salvayre A, Laffargue M. Immune and smooth muscle cells interactions in atherosclerosis: How to target a breaking bad dialogue? Front Pharmacol (2019) 10:1276. doi: 10.3389/fphar.2019.01276
75. Bobryshev YV, Ivanova EA, Chistiakov DA, Nikiforov NG, Orekhov AN. Macrophages and their role in atherosclerosis: Pathophysiology and transcriptome analysis. BioMed Res Int (2016) 2016:9582430. doi: 10.1155/2016/9582430
76. Ketelhuth DF, Hansson GK. Adaptive response of T and b cells in atherosclerosis. Circ Res (2016) 118(4):668–78. doi: 10.1161/circresaha.115.306427
77. Ma SD, Mussbacher M, Galkina EV. Functional role of b cells in atherosclerosis. Cells (2021) 10(2):270. doi: 10.3390/cells10020270
78. Tsiantoulas D, Sage AP, Mallat Z, Binder CJ. Targeting b cells in atherosclerosis: closing the gap from bench to bedside. Arterioscler Thromb Vasc Biol (2015) 35(2):296–302. doi: 10.1161/atvbaha.114.303569
79. Sage AP, Tsiantoulas D, Binder CJ, Mallat Z. The role of b cells in atherosclerosis. Nat Rev Cardiol (2019) 16(3):180–96. doi: 10.1038/s41569-018-0106-9
80. Hosseini H, Yi L, Kanellakis P, Cao A, Tay C, Peter K, et al. Anti-TIM-1 monoclonal antibody (RMT1-10) attenuates atherosclerosis by expanding IgM-producing B1a cells. J Am Heart Assoc (2018) 7(13):e008447. doi: 10.1161/jaha.117.008447
81. Major AS, Fazio S, Linton MF. B-lymphocyte deficiency increases atherosclerosis in LDL receptor-null mice. Arterioscler Thromb Vasc Biol (2002) 22(11):1892–8. doi: 10.1161/01.atv.0000039169.47943.ee
82. Kyaw T, Tay C, Krishnamurthi S, Kanellakis P, Agrotis A, Tipping P, et al. B1a b lymphocytes are atheroprotective by secreting natural IgM that increases IgM deposits and reduces necrotic cores in atherosclerotic lesions. Circ Res (2011) 109(8):830–40. doi: 10.1161/circresaha.111.248542
83. Gillotte-Taylor K, Boullier A, Witztum JL, Steinberg D, Quehenberger O. Scavenger receptor class b type I as a receptor for oxidized low density lipoprotein. J Lipid Res (2001) 42(9):1474–82. doi: 10.1016/S0022-2275(20)30281-9
84. Rosenfeld SM, Perry HM, Gonen A, Prohaska TA, Srikakulapu P, Grewal S, et al. B-1b cells secrete atheroprotective IgM and attenuate atherosclerosis. Circ Res (2015) 117(3):e28–39. doi: 10.1161/circresaha.117.306044
85. Clement RL, Daccache J, Mohammed MT, Diallo A, Blazar BR, Kuchroo VK, et al. Follicular regulatory T cells control humoral and allergic immunity by restraining early b cell responses. Nat Immunol (2019) 20(10):1360–71. doi: 10.1038/s41590-019-0472-4
86. Tsimikas S, Brilakis ES, Lennon RJ, Miller ER, Witztum JL, McConnell JP, et al. Relationship of IgG and IgM autoantibodies to oxidized low density lipoprotein with coronary artery disease and cardiovascular events. J Lipid Res (2007) 48(2):425–33. doi: 10.1194/jlr.M600361-JLR200
87. Kyaw T, Tay C, Hosseini H, Kanellakis P, Gadowski T, MacKay F, et al. Depletion of B2 but not B1a b cells in BAFF receptor-deficient ApoE mice attenuates atherosclerosis by potently ameliorating arterial inflammation. PloS One (2012) 7(1):e29371. doi: 10.1371/journal.pone.0029371
88. Ait-Oufella H, Herbin O, Bouaziz JD, Binder CJ, Uyttenhove C, Laurans L, et al. B cell depletion reduces the development of atherosclerosis in mice. J Exp Med (2010) 207(8):1579–87. doi: 10.1084/jem.20100155
89. Douna H, Amersfoort J, Schaftenaar FH, Kroon S, van Puijvelde GHM, Kuiper J, et al. Bidirectional effects of IL-10(+) regulatory b cells in ldlr (-/-) mice. Atherosclerosis (2019) 280:118–25. doi: 10.1016/j.atherosclerosis.2018.11.019
90. Peng R, Ji H, Jin L, Lin S, Huang Y, Xu K, et al. Macrophage-based therapies for atherosclerosis management. J Immunol Res (2020) 2020:8131754. doi: 10.1155/2020/8131754
91. Ball S, Ghosh RK, Wongsaengsak S, Bandyopadhyay D, Ghosh GC, Aronow WS, et al. Cardiovascular toxicities of immune checkpoint inhibitors: JACC review topic of the week. J Am Coll Cardiol (2019) 74(13):1714–27. doi: 10.1016/j.jacc.2019.07.079
92. Kim KW, Ivanov S, Williams JW. Monocyte recruitment, specification, and function in atherosclerosis. Cells (2020) 10(1):15. doi: 10.3390/cells10010015
93. Potteaux S, Gautier EL, Hutchison SB, van Rooijen N, Rader DJ, Thomas MJ, et al. Suppressed monocyte recruitment drives macrophage removal from atherosclerotic plaques of apoe-/- mice during disease regression. J Clin Invest (2011) 121(5):2025–36. doi: 10.1172/jci43802
94. Tacke F, Alvarez D, Kaplan TJ, Jakubzick C, Spanbroek R, Llodra J, et al. Monocyte subsets differentially employ CCR2, CCR5, and CX3CR1 to accumulate within atherosclerotic plaques. J Clin Invest (2007) 117(1):185–94. doi: 10.1172/jci28549
95. Combadière C, Potteaux S, Rodero M, Simon T, Pezard A, Esposito B, et al. Combined inhibition of CCL2, CX3CR1, and CCR5 abrogates Ly6C(hi) and Ly6C(lo) monocytosis and almost abolishes atherosclerosis in hypercholesterolemic mice. Circulation (2008) 117(13):1649–57. doi: 10.1161/circulationaha.107.745091
Keywords: T cell, atherosclerosis, CiteSpace, VOSviewer, bibliometrics, visualization
Citation: Wei N, Xu Y, Li Y'n, Shi J, Zhang X, You Y, Sun Q, Zhai H and Hu Y (2022) A bibliometric analysis of T cell and atherosclerosis. Front. Immunol. 13:948314. doi: 10.3389/fimmu.2022.948314
Received: 19 May 2022; Accepted: 30 September 2022;
Published: 13 October 2022.
Edited by:
Takashi MaruYama, National Institutes of Health (NIH), United StatesReviewed by:
Mehrnoosh Doroudchi, Shiraz University of Medical Sciences, IranCopyright © 2022 Wei, Xu, Li, Shi, Zhang, You, Sun, Zhai and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huaqiang Zhai, ano3MTFAcXEuY29t; Yuanhui Hu, aHVpeXVodWk1NUBzb2h1LmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.