 Qian Wu
Qian Wu Yang Liu2†
Yang Liu2† Wei Wang
Wei Wang Yu Zhang
Yu Zhang Kui Liu
Kui Liu Song-Hua Chen
Song-Hua Chen Bin Chen
Bin Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 22 July 2022
Sec. Autoimmune and Autoinflammatory Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.938406
This article is part of the Research Topic Biomarkers and Therapeutic Strategies of Systemic Lupus Erythematosus View all 11 articles
Background: Systemic lupus erythematosus (SLE) patients are particularly susceptible to infections, such as pulmonary tuberculosis (PTB) and extrapulmonary tuberculosis (EPTB). This meta-analysis aimed to determine the incidence and prevalence of tuberculosis (TB) in SLE patients.
Methods: The Web of Science, PubMed, Cochrane Library, and Chinese National Knowledge Infrastructure databases were searched for articles of relevant studies published from the dates the databases were established until April 30, 2022. The I2 statistic and Q test were used to evaluate heterogeneity among the analysed studies. Random-effects models were utilised and subgroup analyses were conducted for analysis of the study data.
Results: A total of 35 studies with 46,327 SLE patients were eligible for analysis. The incidence and prevalence of TB among the SLE patients were 1.16 per 100 person-years (95% confidence interval (CI): 0.69-1.93) and 3.59% (95% CI: 2.57%-5.02%), respectively. The pooled prevalence of SLE-PTB and SLE-EPTB was 2.46% (95% CI: 1.73%-3.51%) and 1.42% (95% CI: 0.98%-2.06%), respectively. Subgroup analyses showed that the incidence of SLE-TB was higher in Africa and in countries with a high TB burden than in countries with a low TB burden. The prevalence of SLE-TB was elevated in Asia, in patients taking a mean daily dose of glucocorticoids ≥20 mg, in studies with small sample sizes (n <1000) and ended before 2001.
Conclusions: The available evidence suggests that both the incidence and prevalence of TB in SLE patients are high. This study provides a more specific understanding of SLE-TB, which can help health policymakers in the development of preventive strategies for reducing the SLE-TB burden.
Systemic lupus erythematosus (SLE) is a prototypical inflammatory autoimmune disease that involves multiple systems and is characterised by the accentuation of humoral immunity, excessive proliferation of B lymphocytes, and abnormal production of autoantibodies. The mechanisms underlying the aberrant immune responses associated with SLE remain elusive.
The findings of a previous meta-analysis suggest that adult patients with SLE have a 2-6 times higher risk of infection than that of the general population or healthy controls (1). Susceptibility to an extensive range of severe infections has become a major cause of morbidity and mortality in SLE patients, which imposes a serious public health burden (2, 3). The underlying reasons for this susceptibility to infections include impaired cellular immunity, defective phagocytic function, and use of glucocorticoids (GCs) and immunosuppressants (4).
Tuberculosis (TB) is a major infectious disease worldwide. In 2021, an estimated 9.87 million people developed TB and 1.50 million TB-related deaths were recorded (5). There is increasing evidence that SLE patients have an increased risk of developing pulmonary tuberculosis (PTB) or extrapulmonary tuberculosis (EPTB), particularly in countries with a high TB burden, including India, China, and South Africa (6–9). Despite the significance of this problem, no comprehensive systematic review and meta-analysis of published relevant studies has been conducted to ascertain the global incidence and prevalence of TB in SLE (SLE-TB) patients.
In recent years, studies have reported inconsistent results regarding the specific incidence and prevalence of SLE-TB (10–13). Therefore, a contemporary and comprehensive evaluation and update of the SLE-TB epidemiology data worldwide is necessary as it will provide a theoretical basis for TB screening and preventive treatment in SLE patients. In this meta-analysis, we systematically reviewed relevant literature to comprehensively quantify the incidence and prevalence of SLE-TB and offer insights into the potential factors responsible for heterogeneity in the reported estimates.
This meta-analysis was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement. The Web of Science, PubMed, Cochrane Library, and Chinese National Knowledge Infrastructure databases were searched for articles of relevant studies published from the dates of the inception of the databases to April 30, 2022. A search strategy was designed for each electronic database. For example, the following search strategy was applied in the PubMed database: (“Tuberculosis” OR “TB” OR “pulmonary tuberculosis” OR “PTB” OR “extrapulmonary tuberculosis” OR “EPTB”) AND (“systemic lupus erythematosus” OR “lupus” OR “SLE”). The database search was conducted with no restriction on regions and languages.
Studies that met the following criteria were included: (1) studies in which diagnostic verification was performed, SLE patients should be defined according to the American College of Rheumatology (ACR)-1982, ACR-1997 or International Classification of diseases, diagnosis of TB was made on the basis of clinical manifestations (fever, cough, sputum, dyspnea, hemoptysis, and weight loss), as well as radiological, bacteriological and histopathological evidence suggestive of TB; (2) studies that included relevant data on the incidence or prevalence of SLE-TB; (3) studies on adult patients with SLE; and (4) studies on patients diagnosed with TB after the onset of SLE. For studies with the same sample or duplicate populations, only the most recent study or the study with the largest sample size was included. Reviews, protocols, editorials, letters, and meeting abstracts were excluded.
After the primary literature search, all the articles were entered into the EndNote X7 software. First, the titles and abstracts of the articles were independently reviewed by two co-first authors and duplicate articles were excluded. Thereafter, the full texts of the remaining articles were reviewed and eligible articles were selected. Any disagreement during selection was resolved through a group discussion. The following characteristics of each eligible study were recorded: first author’s name, publication year, incidence of SLE-TB (number of SLE and SLE-TB patients, follow-up duration), prevalence of SLE-TB (or number of SLE and SLE-TB patients), the types of TB (PTB or EPTB), methods used for the diagnosis of SLE, mean daily dose of GCs, study period, country, region, TB burden, and study sites.
The I2 statistic and Q test were used to evaluate heterogeneity among the includes studies. The pooled incidence and prevalence of SLE-TB (with 95% confidence intervals [CIs]) was defined as the number of SLE-TB patients per 100 person-years and per 100 persons (%), respectively. A random-effects model was used for analysis if I2 was >50% and the P value for Q test was <0.10; a fixed-effects model was used if otherwise. To identify the possible source of heterogeneity among the studies, subgroup analysis was conducted according to region, TB burden, diagnostic criteria for SLE, sample size, and mean daily dose of GCs. Publication bias was assessed using the Egger’s and Begg’s tests. Sensitivity analysis was conducted by iteratively removing one study from the meta-analysis. All statistical analyses were conducted using R software (version 3.6.1; http://www.R-project.org) with the “meta” package. Statistical significance was set at P < 0.05.
After a comprehensive literature search, 2371 articles from the Web of Science (1,126), PubMed (998), Cochrane library (86), and Chinese National Knowledge Infrastructure (161) databases were initially retrieved. Of these, 1825 relevant studies were identified based on the abovementioned eligibility and exclusion criteria. After manually reviewing the full texts, 1736 studies were excluded. Finally, 35 eligible studies, including nine cohort and 26 cross-sectional studies with a total of 46,327 SLE patients were included in the meta-analysis (6–40) (Figure 1). Of the included studies, 25 were published in English, eight in Chinese, and two in Spanish. All included studies were published between 1982 and 2021. The sample sizes ranged from 141 to 10469 participants. The baseline and general characteristics of the included studies are shown in Tables 1, 2.
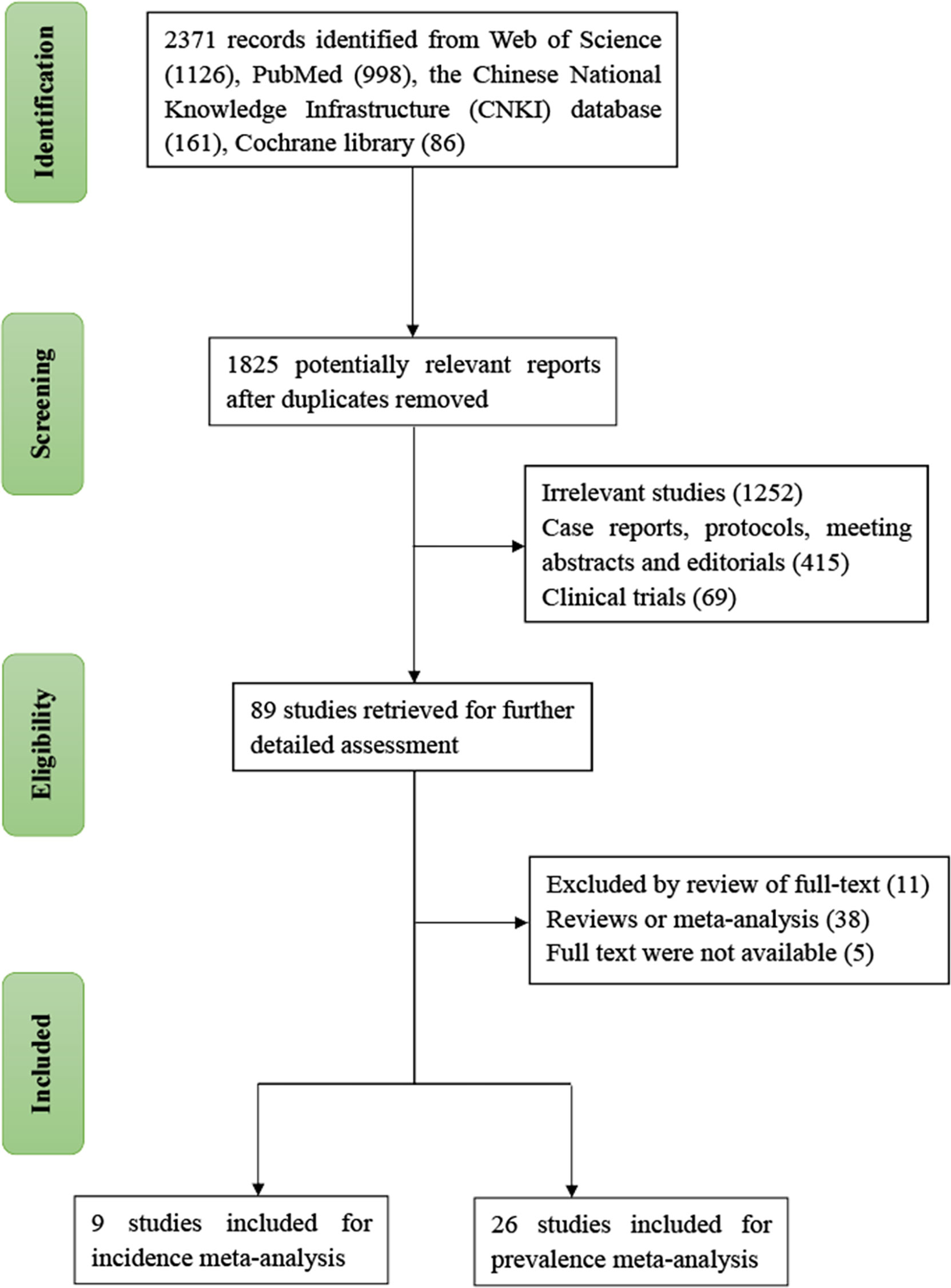
Figure 1 Flow chart of study selection.
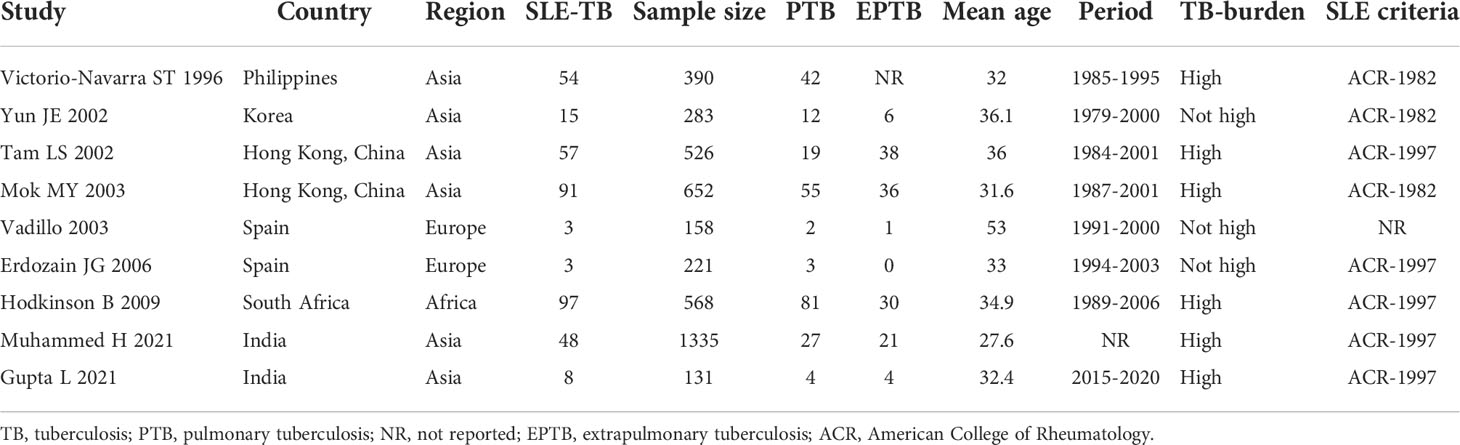
Table 1 Summary of the studies that reported the TB incidence among SLE patients.
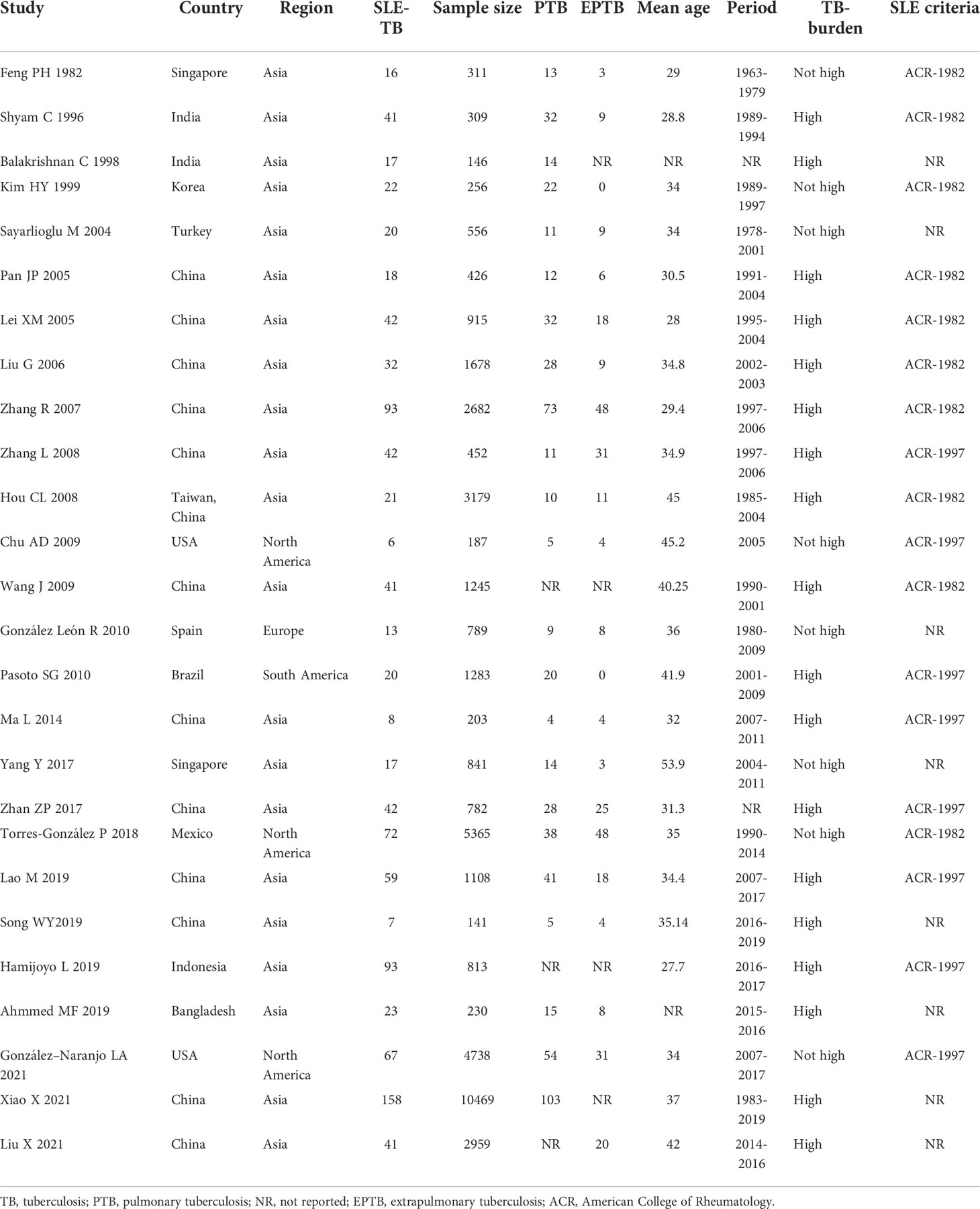
Table 2 Summary of the studies that reported the TB prevalence among SLE patients.
The incidence of TB in SLE patients was reported in nine studies, which included 4,264 SLE patients with 28,755 person-years of follow-up. The pooled estimate of the incidence of SLE-TB in these studies was 1.16 (95% CI: 0.69-1.93) per 100 person-years (Figure 2). Statistically significant heterogeneity was observed between the studies (I2 = 95.4%, τ2 = 0.53, P<0.01).
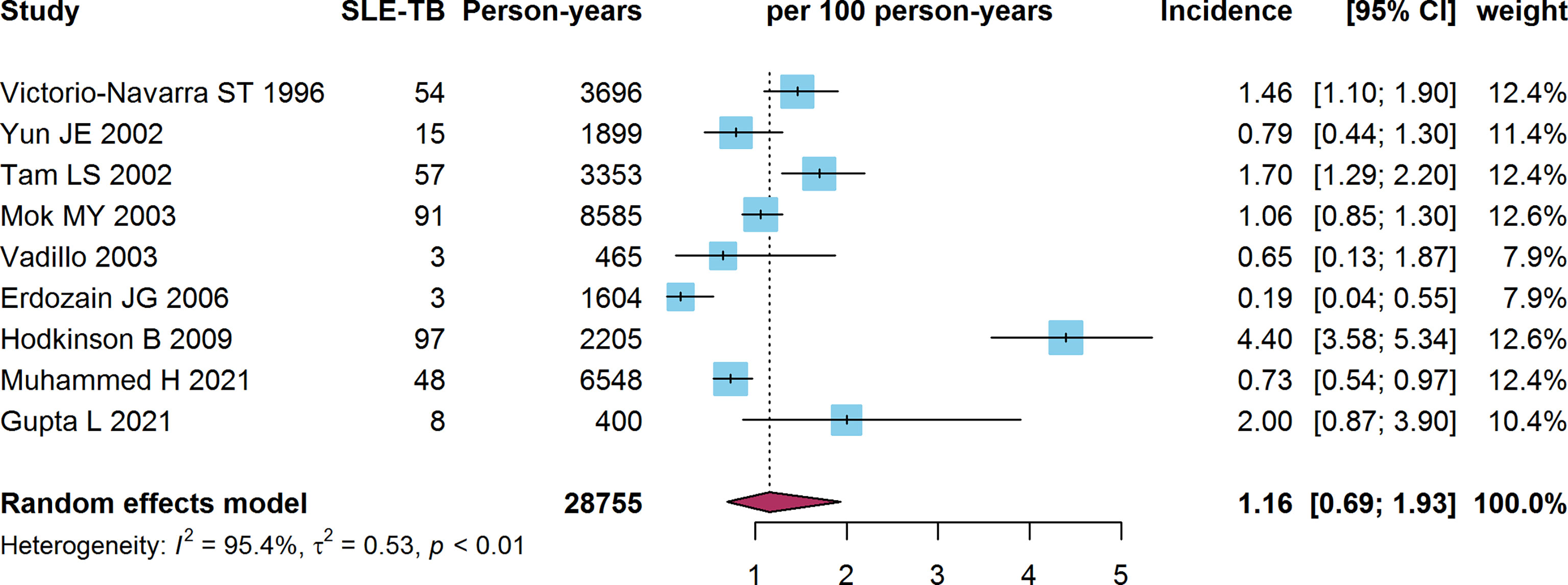
Figure 2 Forest plot of the SLE-TB incidence. SLE, systemic lupus erythematosus; TB, tuberculosis.
The subgroup meta-analysis stratified according to TB burden revealed that incidence of SLE-TB in countries with a high TB burden (1.60 per 100 person-years, 95% CI: 0.89-2.86) was higher than that in countries with a low TB burden (0.50 per 100 person-years, 95% CI: 0.22-1.17) (P=0.03). Only one of the studies was conducted in Africa. The pooled prevalence of SLE-TB in Africa was higher (4.40 per 100 person-years, 95% CI: 3.62-5.34) than that in Asia (1.18 per 100 person-years, 95% CI: 0.88-1.59) and Europe (0.35 per 100 person-years, 95% CI: 0.10-1.17) (P<0.01). However, the incidence of SLE-TB according to the 1982 criteria of the American College of Rheumatology (ACR-1982) or ACR-1997 did not differ between subgroups (P=0.79). Besides, no significant difference in the SLE-PTB incidence was observed when stratified according to study period of these studies (P=0.91) (Table 3)
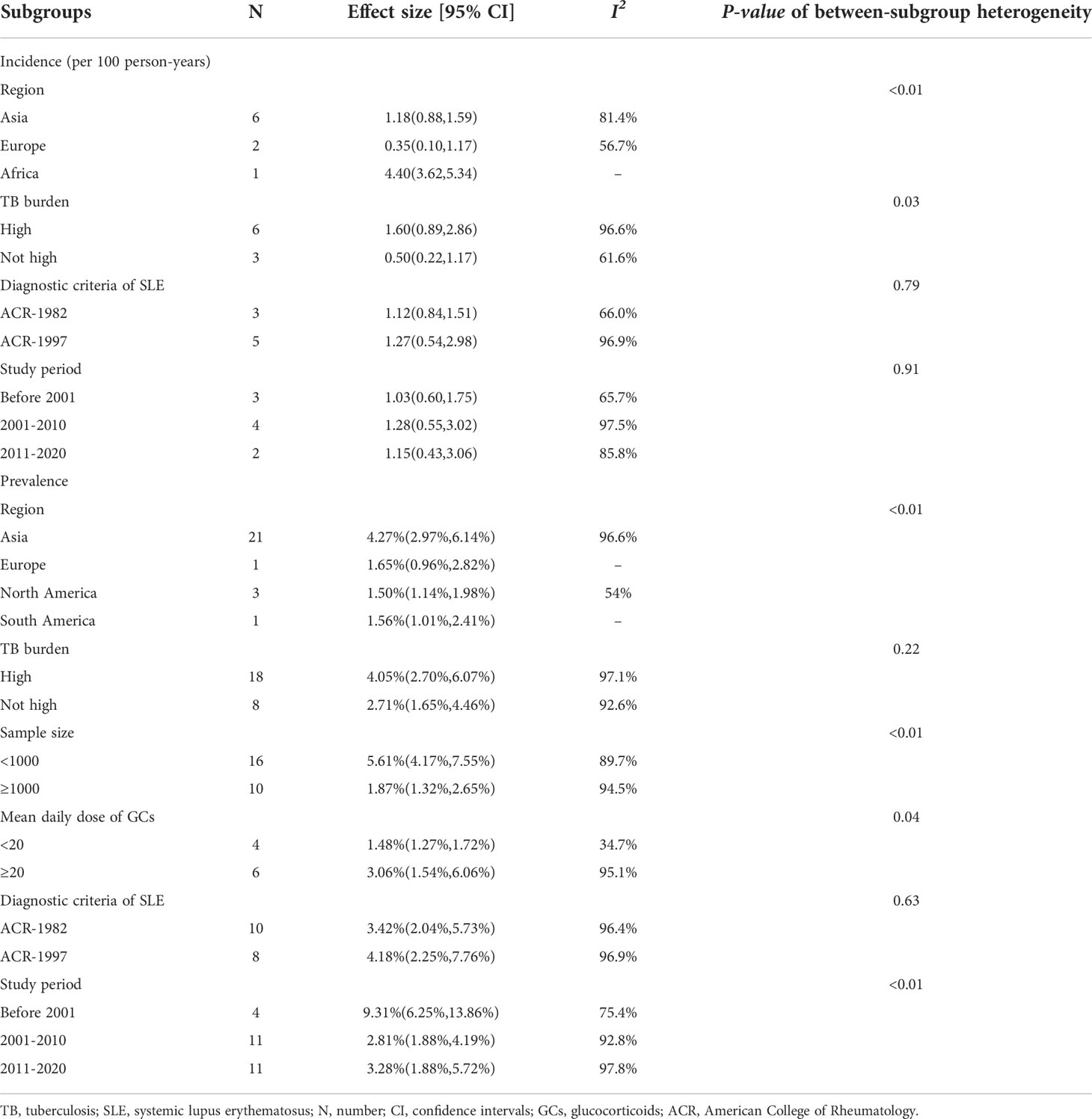
Table 3 Subgroup analysis of TB incidence and prevalence among SLE patients.
Sensitivity analysis revealed no significant changes in the overall estimates of the incidence of SLE-TB after omitting any study (Figure S1). The results of the Egger’s (t= -1.22, P=0.260) and Begg’s (z= -0.83, P=0.404) tests indicated no evidence of publication bias in the pooled incidence of SLE-TB (Figure S2).
The prevalence of TB in SLE patients was reported in 26 studies, which included 42,063 SLE patients. The pooled estimate of the prevalence of SLE-TB in the studies was 3.59% (95% CI: 2.57%-5.02%) (Figure 3). Heterogeneity among these studies was statistically significant (I2 = 96.6%, τ2 = 0.71, P<0.01). The prevalence of SLE-PTB was reported in 23 studies, which included 37,046 SLE patients. The pooled prevalence of SLE-PTB in the studies was 2.46% (95% CI: 1.73%-3.51%). There was high heterogeneity among these studies as well (I2 = 94.6%, τ2 = 0.68, P<0.01) (Figure S3). The prevalence of SLE-EPTB was reported in 20 studies with 27,851 SLE patients. The pooled prevalence of SLE-EPTB in the studies was 1.42% (95% CI: 0.98%-2.06%) and high heterogeneity was noted among the studies (I2 = 90.3%, τ2 = 0.60, P<0.01) (Figure S4).
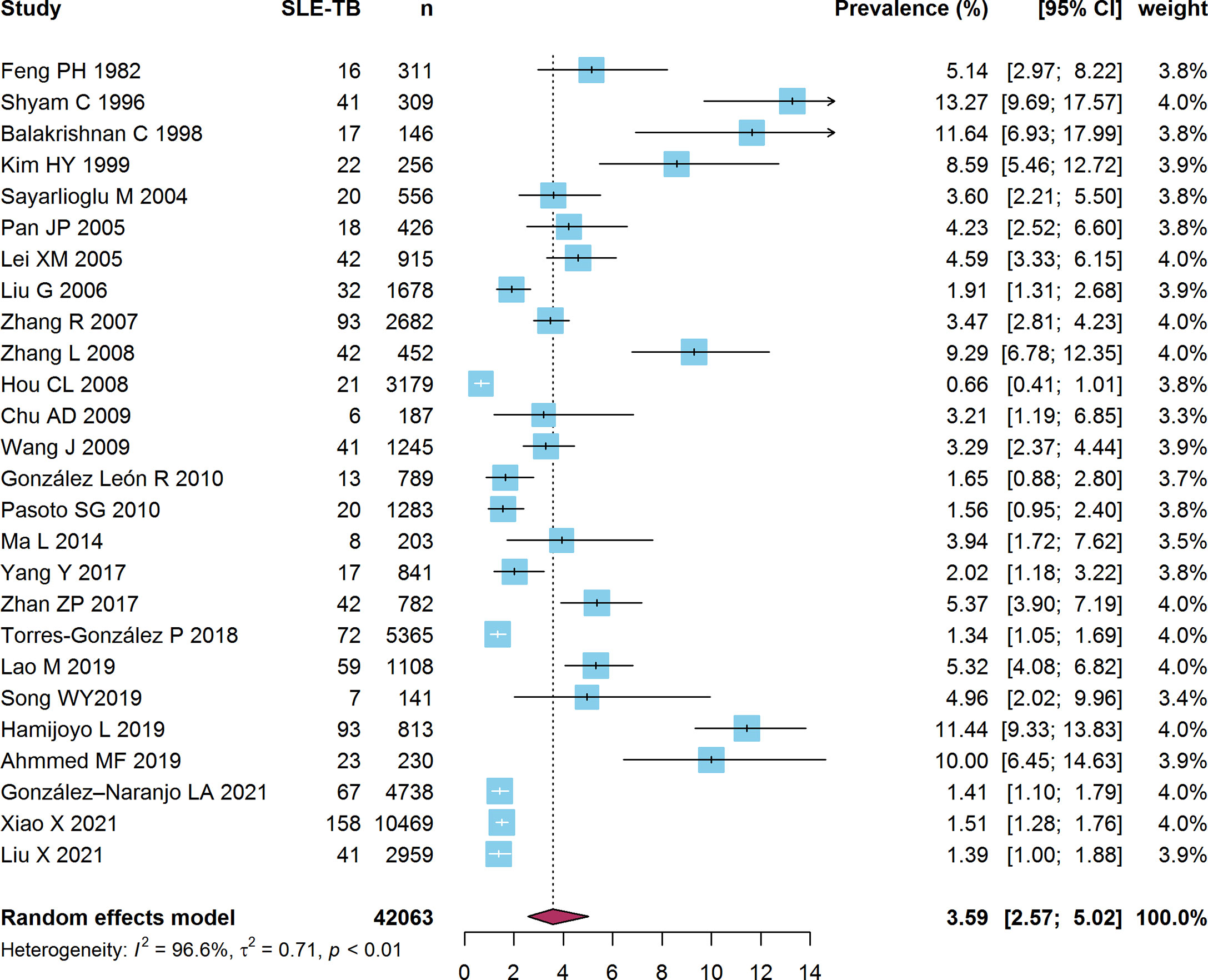
Figure 3 Forest plot of the SLE-TB prevalence. SLE, systemic lupus erythematosus; TB, tuberculosis.
Only one study each was conducted in Europe and South America. The pooled prevalence of SLE-TB in Asia was higher (4.27%, 95% CI: 2.97%-6.14%) than that in Europe (1.65%, 95% CI: 0.96%-2.82%), South America (1.56%, 95% CI: 1.01%-2.41%), and North America (1.50%, 95% CI: 1.14%-1.98%) (P<0.01). The subgroup meta-analysis stratified according to sample size showed that the prevalence of SLE-TB in studies with a small sample size (n <1000) (5.61%, 95% CI: 4.17%-7.55%) was three times higher than that in studies with a large sample size (n ≥1000) (1.87%, 95% CI: 1.32%-2.65%) (P<0.01). The pooled prevalence of SLE-TB among patients taking a mean daily dose of GCs ≥20 mg was higher (3.06%, 95% CI: 1.54%-6.06%) than that in patients taking a mean daily dose of GCs <20 mg (1.48%, 95% CI: 1.27%-1.72%) (P = 0.04). In terms of study period of these studies, the SLE-TB prevalence in studies ended before 2001 (9.31%, 95% CI: 6.25%-13.86%) was significantly higher than that in studies ended between 2001-2010 and 2011-2020 (P<0.01). However, no significant difference in the prevalence of SLE-PTB was observed when stratified according to TB burden (P=0.22) and diagnostic criteria of SLE (P=0.63) (Table 3).
Sensitivity analysis revealed no significant changes in the overall estimates of the prevalence of SLE-TB after omitting any study (Figure S5). The results of the Egger’s (t = 0.51, P = 0.615) and Begg’s (z = -0.20, P = 0.843) tests indicated no evidence of publication bias in the pooled prevalence of SLE-TB (Figure S6).
Previous studies conducted in different countries have shown that SLE patients had a 5-60-fold higher risk of TB than that of patients without (15, 17, 18, 33, 39). In this systematic review, we analysed data from 35 studies, which included 46,327 SLE patients from 13 countries across five continents. The results of the meta-analysis indicated that the incidence and prevalence of TB among SLE patients was 1.16 per 100 person-years (95% CI: 0.69-1.93) and 3.59% (95% CI: 2.57%-5.02%), respectively. Numerous studies have presented convincing biological evidence supporting a causal relationship between compromised immune defence systems and susceptibility to TB (41, 42). SLE patients exhibit atypical clinical manifestations of TB, including fever, arthralgia, pleurisy, peritonitis, and headache. Moreover, a retrospective study revealed that the radiological manifestations and laboratory results of TB in SLE patients are relatively atypical (35). In this regard, timely diagnosis and treatment of TB in SLE patients may be difficult to determine, reinforcing the need for disease surveillance in this population.
Several studies have demonstrated that SLE patients exhibit relatively frequent extrapulmonary involvement, indicating the reactivation of past infections rather than the occurrence of new primary infections (17, 27, 36). Conversely, the results of the present study revealed a relatively higher prevalence of SLE-PTB (2.46%, 95% CI: 1.73%-3.51%) than that of SLE-EPTB (1.42%, 95% CI: 0.98%-2.06%). Our findings conform with those of a retrospective case-control study in which PTB accounted for 46.3% of all cases, whereas EPTB and disseminated TB accounted for 16.4% and 37.3%, respectively (13).
The subgroup analyses in the present study revealed significant differences between the incidence and prevalence of SLE-EPTB in the five aforementioned continents. The variations among the studies conducted in these continents may be attributable to differences in the prevention strategies employed in the countries and the ethnic and sociodemographic statuses of the study participants (43, 44). Another possible explanation for the higher prevalence of SLE-TB in Asia than in Europe, South America, and North America could be the relatively larger proportion of high TB burden countries in Asia, such as India and China.
We found that the pooled incidence of TB was significantly higher in countries with a high TB burden. However, it should be noted that more than three-quarters of the studies included in this meta-analysis were conducted in endemic regions. Thus, large-scale, prospective, studies performed in several countries are required to obtain more reliable estimates of the global incidence of the SLE-TB.
A high cumulative and/or mean daily dose of GCs has been implicated as a predisposing factor for the development of TB in SLE patients (17, 21, 45). For example, a case-control study indicated that patients taking GCs have an approximately five-fold increased risk of developing TB compared to those who are not taking GCs (46). Consistent with these findings, we found that the pooled prevalence of SLE-TB in patients with a mean daily dose of GCs ≥20 mg was significantly higher than that in patients with a mean daily dose of GCs <20 mg. The exact mechanism of the effect of GC therapy in SLE patients has not been fully elucidated. However, it may involve the decline of cellular immune function through the inhibition of lymphocytes, monocyte macrophages, neutrophils, and eosinophils. Thus, administration of a minimum dose of GCs is recommended for better control of TB.
This systematic review had several limitations. First, the heterogeneity among the included studies was significant. This might have been caused by differences in populations and geographic regions. Therefore, the pooled incidence and prevalence of the diseases indicated in the results should be interpreted with caution. Second, previous studies have shown that the Systemic Lupus Erythematosus Disease Activity Index, use of immunosuppressants, duration of treatment, and presence of nephritis are risk factors for developing TB (9, 17, 44). Unfortunately, we were unable to retrieve sufficient information regarding these variables from most of the included studies. Third, there may be selection bias in the results owing to the retrospective nature of some of the included cohort studies. Thus, future, well-designed, prospective studies conducted using standardised methods of data collection and reporting are required to clarify the incidence of TB in SLE patients.
These limitations notwithstanding, this meta-analysis comprehensively summarises the current evidence regarding the global incidence and prevalence of TB in SLE patients, and provides a reference that can be used in the prevention and management of TB in SLE patients. Efforts to improve the understanding of SLE-TB and develop preventive strategies against it are required in the future.
The available evidence indicates that the incidence and prevalence of TB among SLE patients are significantly higher than those in the general population. More attention should be paid to strengthening strategies aimed at preventing TB and developing better treatments for SLE, especially in countries with a high TB burden and in patients taking a mean daily dose of GCs ≥20 mg.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
QW, YL and BC conceptualized the meta-analysis, QW and YL conducted the research and performed the statistical analysis. QW drafted the initial manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the National-Zhejiang Health commission Major S&T Project (Grant No. WKJ-ZJ-2118), Zhejiang Provincial Medical and Health Project (2021KY618 and 2020KY520).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.938406/full#supplementary-material
1. Pego-Reigosa JM, Nicholson L, Pooley N, Langham S, Embleton N, Marjenberg Z, et al. The risk of infections in adult patients with systemic lupus erythematosus: systematic review and meta-analysis. Rheumatol (Oxf Engl) (2021) 60:60–72. doi: 10.1093/rheumatology/keaa478
2. Goldblatt F, Chambers S, Rahman A, Isenberg DA. Serious infections in British patients with systemic lupus erythematosus: hospitalisations and mortality. Lupus (2009) 18:682–9. doi: 10.1177/0961203308101019
3. Iliopoulos AG, Tsokos GC. Immunopathogenesis and spectrum of infections in systemic lupus erythematosus. Semin Arthritis Rheum (1996) 25:318–36. doi: 10.1016/S0049-0172(96)80018-7
4. Juárez M, Misischia R, Alarcón GS. Infections in systemic connective tissue diseases: systemic lupus erythematosus, scleroderma, and polymyositis/dermatomyositis. Rheum Dis Clinics North America (2003) 29:163–84. doi: 10.1016/S0889-857X(02)00100-X
6. Hamijoyo L, Candrianita S, Rahmadi AR, Dewi S, Darmawan G, Suryajaya BS, et al. The clinical characteristics of systemic lupus erythematosus patients in Indonesia: a cohort registry from an Indonesia-based tertiary referral hospital. Lupus (2019) 28:1604–9. doi: 10.1177/0961203319878499
7. Wang J, Pan HF, Su H, Li XP, Xu and D.Q. Ye JH. Tuberculosis in systemic lupus erythematosus in Chinese patients. Trop Doct (2009) 39:165–7. doi: 10.1258/td.2008.080379
8. Shyam C, Malaviya AN. Infection-related morbidity in systemic lupus erythematosus: a clinico-epidemiological study from northern India. Rheumatol Int (1996) 16:1–3. doi: 10.1007/BF01419946
9. Hodkinson B, Musenge E, Tikly M. Osteoarticular tuberculosis in patients with systemic lupus erythematosus. QJM Mon J Assoc Phys (2009) 102:321–8. doi: 10.1093/qjmed/hcp015
10. Muhammed H, Jain A, Pattanaik SS, Chatterjee R, Naveen R, Kabeer H, et al. Clinical spectrum of active tuberculosis in patients with systemic lupus erythematosus. Rheumatol Int (2021) 41:2185–93. doi: 10.1007/s00296-021-04933-0
11. Gupta L, Aggarwal R, Naveen R, Lawrence A, Zanwar A, Misra DP, et al. High prevalence of active tuberculosis in adults and children with idiopathic inflammatory myositis as compared with systemic lupus erythematosus in a tuberculosis endemic country: Retrospective data review from a tertiary care centre in India. Mediterr J Rheumatol (2021) 32:134–42. doi: 10.31138/mjr.32.2.134
12. Liu X, Zhang L, Zhang F, Zeng X, Zhao Y, Wang Q, et al. Prevalence and risk factors of active tuberculosis in patients with rheumatic diseases: a multi-center, cross-sectional study in China. Emerg Microbes Infect (2021) 10:2303–12. doi: 10.1080/22221751.2021.2004864
13. González-Naranjo LA, Coral-Enríquez JA, Restrepo-Escobar M, Muñoz-Vahos CH, Jaramillo-Arroyave D, Vanegas-García AL, et al. Factors associated with active tuberculosis in Colombian patients with systemic lupus erythematosus: a case-control study. Clin Rheumatol (2021) 40:181–91. doi: 10.1007/s10067-020-05225-x
14. Feng PH, Tan TH. Tuberculosis in patients with systemic lupus erythematosus. Ann Rheum Dis (1982) 41:11–4. doi: 10.1136/ard.41.1.11
15. Victorio-Navarra ST, Dy EE, Arroyo CG, Torralba TP. Tuberculosis among Filipino patients with systemic lupus erythematosus. Semin Arthritis Rheum (1996) 26:628–34. doi: 10.1016/S0049-0172(96)80013-8
16. Kim HY, Im JG, Goo JM, Lee JK, Song JW, Kim SK. Pulmonary tuberculosis in patients with systematic lupus erythematosus. AJR Am J Roentgenol (1999) 173:1639–42. doi: 10.2214/ajr.173.6.10584813
17. Tam LS, Li EK, Wong SM, Szeto CC. Risk factors and clinical features for tuberculosis among patients with systemic lupus erythematosus in Hong Kong. Scand J Rheumatol (2002) 31:296–300. doi: 10.1080/030097402760375205
18. Yun JE, Lee SW, Kim TH, Jun JB, Jung S, Bae SC, et al. The incidence and clinical characteristics of mycobacterium tuberculosis infection among systemic lupus erythematosus and rheumatoid arthritis patients in Korea. Clin Exp Rheumatol (2002) 20:127–32.
19. Mok MY, Lo Y, Chan TM, Wong WS, Lau CS. Tuberculosis in systemic lupus erythematosus in an endemic area and the role of isoniazid prophylaxis during corticosteroid therapy. J Rheumatol (2005) 32:609–15. doi: 10.1097/01.rhu.0000158687.22004.18
20. Vadillo Font C, Hernández-García C, Pato E, Morado IC, Salido M, Júdez E, et al. [Incidence and characteristics of tuberculosis in patients with autoimmune rheumatic diseases]. Rev Clin Esp (2003) 203:178–82. doi: 10.1157/13045537
21. Sayarlioglu M, Inanc M, Kamali S, Cefle A, Karaman O, Gul A, et al. Tuberculosis in Turkish patients with systemic lupus erythematosus: increased frequency of extrapulmonary localization. Lupus (2004) 13:274–8. doi: 10.1191/0961203303lu529xx
22. Lei XM, Li SX. Clinical observation on systemic lupus erythematosus associated tuberculosis. Chin J Clin Healthcare (2005), 489–91. doi: 10.3969/j.issn.1672-6790.2005,06,004
23. Pan JP. The tuberculosis infection in patients with systemic lupus erythematosus. Chin J Rheumatol (2005), 100–1. doi: 10.3760/j:issn:1007-7480,2005.02.011
24. Erdozain JG, Ruiz-Irastorza G, Egurbide MV, Martinez-Berriotxoa A, Aguirre C. High risk of tuberculosis in systemic lupus erythematosus? Lupus (2006) 15:232–5. doi: 10.1191/0961203306lu2289xx
25. Liu G, Jiang L, Liu YX. Clinical analysis on 32 patients with systemic lupus erythematosus combined with tuberculosis. J Sichuan University (Med Sci Edition) (2006) 37:331–3. doi: 10.3969/ j.issn.1672-173/.2006.02.047
26. Zhang R, Liu G, Sun YL. Clinical analysis on 93 patients with systemic lupus erythematosus combined with tuberculosis. J South Med Univ (2007) 27:615–7.
27. Hou CL, Tsai YC, Chen LC, Huang JL. Tuberculosis infection in patients with systemic lupus erythematosus: pulmonary and extra-pulmonary infection compared. Clin Rheumatol (2008) 27:557–63. doi: 10.1007/s10067-007-0741-8
28. Zhang L, Wang DX, Ma L, Wu DH. A clinical study of tuberculosis infection in systemic lupus erythematosus. Chin J Internal Med (2008) 47:808–10.
29. Chu AD, Polesky AH, Bhatia G, Bush TM. Active and latent tuberculosis in patients with systemic lupus erythematosus living in the united states. J Clin Rheumatol Pract Rep Rheum Musculoskeletal Dis (2009) 15:226–9. doi: 10.1097/RHU.0b013e3181b0c85d
30. González León R, Garrido Rasco R, Chinchilla Palomares E, García Hernández FJ, Castillo Palma MJ, Sánchez Román J. Tuberculosis in a cohort of patients with systemic lupus erythematosus. Reumatol Clin (2010) 6:256–61. doi: 10.1016/j.reuma.2009,11.002
31. Pasoto SG, Borba EF, Bonfa E, Shinjo SK. Lupus pleuritis: a relevant risk factor for pulmonary tuberculosis. Lupus (2010) 19:1585–90. doi: 10.1177/0961203310375269
32. Ma L, Lin B, Wang LY, Wang DX, Li GY, Wang GC. Preventive therapy for iatrogenic active tuberculosis in systemic lupus erythematosus patients. Natl Med J China (2014) 94:3579–82. doi: 10.3760/cma.j.issn.0376-2491.2014.45.011
33. Yang Y, Thumboo J, Tan BH, Tan TT, Fong CHJ, Ng HS, et al. The risk of tuberculosis in SLE patients from an Asian tertiary hospital. Rheumatol Int (2017) 37:1027–33. doi: 10.1007/s00296-017-3696-3
34. Zhan ZP, Lao MX, Su F, Chen DY, Liang LQ, Yang XY. Clinical features of tuberculosis in patients with systemic lupus erythematosus. J Pract Med (2017) 33:3552–5. doi:10.3969/j.issn.1006-5725.2017,21.013
35. Lao M, Chen D, Wu X, Chen H, Qiu Q, Yang X, et al. Active tuberculosis in patients with systemic lupus erythematosus from southern China: a retrospective study. Clin Rheumatol (2019) 38:535–43. doi: 10.1007/s10067-018-4303-z
36. Torres-González P, Romero-Díaz J, Cervera-Hernández ME, Ocampo-Torres M, Chaires-Garza LG, Lastiri-González EA, et al. Tuberculosis and systemic lupus erythematosus: a case-control study in Mexico city. Clin Rheumatol (2018) 37:2095–102. doi: 10.1007/s10067-018-4109-z
37. Song WY, Guo ZJ, Wang B, Zhou T. Investigation on the incidence of hepatitis and tuberculosis in patients with systemic lupus erythematosus and methylprednisolone. Chin J Control Endemic Dis (2019) 34:263–264+330.
38. Xiao X, Da G, Xie X, Liu X, Zhang L, Zhou B, et al. Tuberculosis in patients with systemic lupus erythematosus-a 37-year longitudinal survey-based study. J Internal Med (2021) 290:101–15. doi: 10.1111/joim.13218
39. Balakrishnan C, Mangat G, Mittal G, Joshi VR. Tuberculosis in patients with systemic lupus erythematosus. J Assoc Phys India (1998) 46:682–3. doi: 10.1136/ard.41.1.11
40. Ahmmed MF, Islam MN, Ferdous S, Azad AK, Ferdous N. Tuberculosis in systemic lupus erythematosus patients. Mymensingh Med J MMJ (2019) 28:797–807.
41. Zandman-Goddard G, Shoenfeld Y. SLE and infections. Clin Rev Allergy Immunol (2003) 25:29–40. doi: 10.1385/CRIAI:25:1:29
42. Balbi GGM, Machado-Ribeiro F, Marques CDL, Signorelli F, Levy RA. The interplay between tuberculosis and systemic lupus erythematosus. Curr Opin Rheumatol (2018) 30:395–402. doi: 10.1097/BOR.0000000000000493
43. Lee J, Dhillon N, Pope J. All-cause hospitalizations in systemic lupus erythematosus from a large Canadian referral centre. Rheumatol (Oxford England) (2013) 52:905–9. doi: 10.1093/rheumatology/kes391
44. Dubula T, Mody GM. Spectrum of infections and outcome among hospitalized south africans with systemic lupus erythematosus. Clin Rheumatol (2015) 34:479–88. doi: 10.1007/s10067-014-2847-0
45. Noël V, Lortholary O, Casassus P, Cohen P, Généreau T, André MH, et al. Risk factors and prognostic influence of infection in a single cohort of 87 adults with systemic lupus erythematosus. Ann Rheum Dis (2001) 60:1141–4. doi: 10.1136/ard.60.12.1141
Keywords: systemic lupus erythematosus, tuberculosis, incidence, prevalence, glucocorticoids
Citation: Wu Q, Liu Y, Wang W, Zhang Y, Liu K, Chen S-H and Chen B (2022) Incidence and prevalence of tuberculosis in systemic lupus erythematosus patients: A systematic review and meta-analysis. Front. Immunol. 13:938406. doi: 10.3389/fimmu.2022.938406
Received: 07 May 2022; Accepted: 30 June 2022;
Published: 22 July 2022.
Edited by:
Jian Gao, Shanghai Children’s Medical Center, ChinaReviewed by:
Amita Aggarwal, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaCopyright © 2022 Wu, Liu, Wang, Zhang, Liu, Chen and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bin Chen, YmNoZW5AY2RjLnpqLmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.