 Mihaela Aldea1*Rakiba Belkhir2Emeline Colomba1Pierre Blanchard3Francois-Xavier Danlos1Angela Botticella3Mario Terlizzi3Eric Deutsch3,4Cecile Le Péchoux3David Planchard1Jean-Marie Michot5Benjamin Besse1
Mihaela Aldea1*Rakiba Belkhir2Emeline Colomba1Pierre Blanchard3Francois-Xavier Danlos1Angela Botticella3Mario Terlizzi3Eric Deutsch3,4Cecile Le Péchoux3David Planchard1Jean-Marie Michot5Benjamin Besse1 Antonin Levy3,4*
Antonin Levy3,4*- 1Department of Medical Oncology, International Center for Thoracic Cancers (CICT), Université Paris-Saclay, Gustave Roussy, Villejuif, France
- 2Rheumatology, Hôpital Bicêtre, Assistance Publique-Hôpitaux de Paris, FHU CARE, Le Kremlin-Bicêtre, France
- 3Department of Radiation Oncology, International Center for Thoracic Cancers (CICT), Université Paris-Saclay, Gustave Roussy, Villejuif, France
- 4INSERM U1030, Molecular Radiotherapy, Université Paris-Saclay, Villejuif, France
- 5DITEP (Département des Innovations Thérapeutiques et Essais Précoces), Université Paris-Saclay, Gustave Roussy, Villejuif, France
Radiotherapy can trigger immune-related out-of-field “abscopal” response. We report a patient with advanced NSCLC (non-small cell lung cancer) receiving long-term anti-PD1 (programmed cell death protein 1) who have developed out-of-field immune-related arthritis following pelvic irradiation.
Introduction
The “abscopal effect” was described decades ago, with the application of radiotherapy at one site leading to out-of-field response of a non-irradiated metastatic site. This phenomenon has possible underlying immune mechanisms, based on the stimulation of antigen release, immune cell recruitment, and memory (1). The synergism between radiotherapy and immune checkpoint blockers (ICBs) has shown activity, and is currently being investigated in immunoradiotherapy clinical trials (2, 3). In stage III unresectable non-small cell lung cancer (NSCLC), ICB use post curative intent concurrent thoracic chemoradiation is now the standard of care (PACIFIC trial). In the PACIFIC trial, increased severe adverse events were not reported with ICB, as compared to placebo (4).
Immune-related adverse effects (irAE) are observed with ICB; however, it remains unclear whether the addition of sequential radiotherapy after long-term ICB could promote out-of-field irAE occurrence. Here, we describe, for the first time, a potential radiation therapy-induced out-of-field irAE, in an advanced NSCLC patient undergoing long-term treatment with ICB.
Patient information
In March 2017, a male patient in his early 70s, with a history of tobacco smoking of 30 pack-years and no personal or family medical history, was diagnosed with advanced stage IV lung adenocarcinoma (PD-L1 <1%, CTNNB1 mutated), with two brain metastases. The patient had a synchronous locally advanced high-risk (Gleason 9, PSA = 27) prostate adenocarcinoma treated with LHRH (luteinizing hormone-releasing hormone) agonist from February 2017 (Figure 1A). The patient received brain stereotactic radiotherapy in May 2017. After three cycles of induction cisplatin-pemetrexed chemotherapy, he underwent a right superior lobectomy with lymphadenectomy in August 2017. In February 2018, the patient experienced oligo-recurrence with a new right adrenal and cerebellar lesion. Intravenous (IV) carboplatin (AUC 5 D1)–vinorelbine (30 mg/m2 D1 and D8, D1 = D21) chemotherapy was administered. However, due to progressive disease, IV nivolumab treatment (240 mg flat dose q2 weeks) commenced in June 2018. Due to an isolated adrenal oligoprogression, the patient underwent right adrenalectomy in February 2019 and continued nivolumab. In November 2020, following a significant PSA rise, choline PET-CT confirmed prostate cancer progression with a single left sacral bone metastasis. He received double site radiation therapy [prostate VMAT (volumetric modulated arc therapy) at a dose of 60 Gy in 20 fractions and sacrum stereotactic body radiotherapy (SBRT) at a dose of 35 Gy in 5 fractions] until 6 August 2021 (Figure 1B). From the last day of radiotherapy, he experienced invalidating poly-arthralgia predominantly of his lower limbs, with joint swelling and difficulty walking. The patient was referred to a rheumatology team. The blood samples only revealed a transient G3 lymphopenia without eosinophils variation (Figure 2D). Autoantibodies [including rheumatoid factor (RF), anti-citrullinated protein/peptide antibodies (ACPA), and total/soluble anti-nuclear antibodies (Anti-Ribosomes, -Sm, -SSA/Ro, - SSB/La, -U3-RNP, -centromere, -Scl-70, and -Jo-1)] were negative. Infectious analyses were negative; however, CRP was elevated (173 mg/L). X-rays were normal, joint ultrasounds revealed tenosynovitis (Figures 2A–C), and tendon sheath aspiration retrieved a sterile (and without crystals) inflammatory synovial fluid, with a white blood cell count of 13,000/µl (95% lymphocytes). Peripheral/central blood cultures and urine were sterile. Immune-related arthritis was suspected and steroids 20 mg/day was commenced on 27 August. Nivolumab and LHRH agonist were maintained with persistence of migrating arthralgia. Given poor efficacy of steroids, IV tocilizumab (162 mg per week) was initiated on December 2021 and symptoms improved with normalization of CRP. The patient is pursuing nivolumab and tocilizumab. His last radiological examination on 24 January 2022, including an FDG-PET/CT, showed no evolutive disease and no joint uptake.
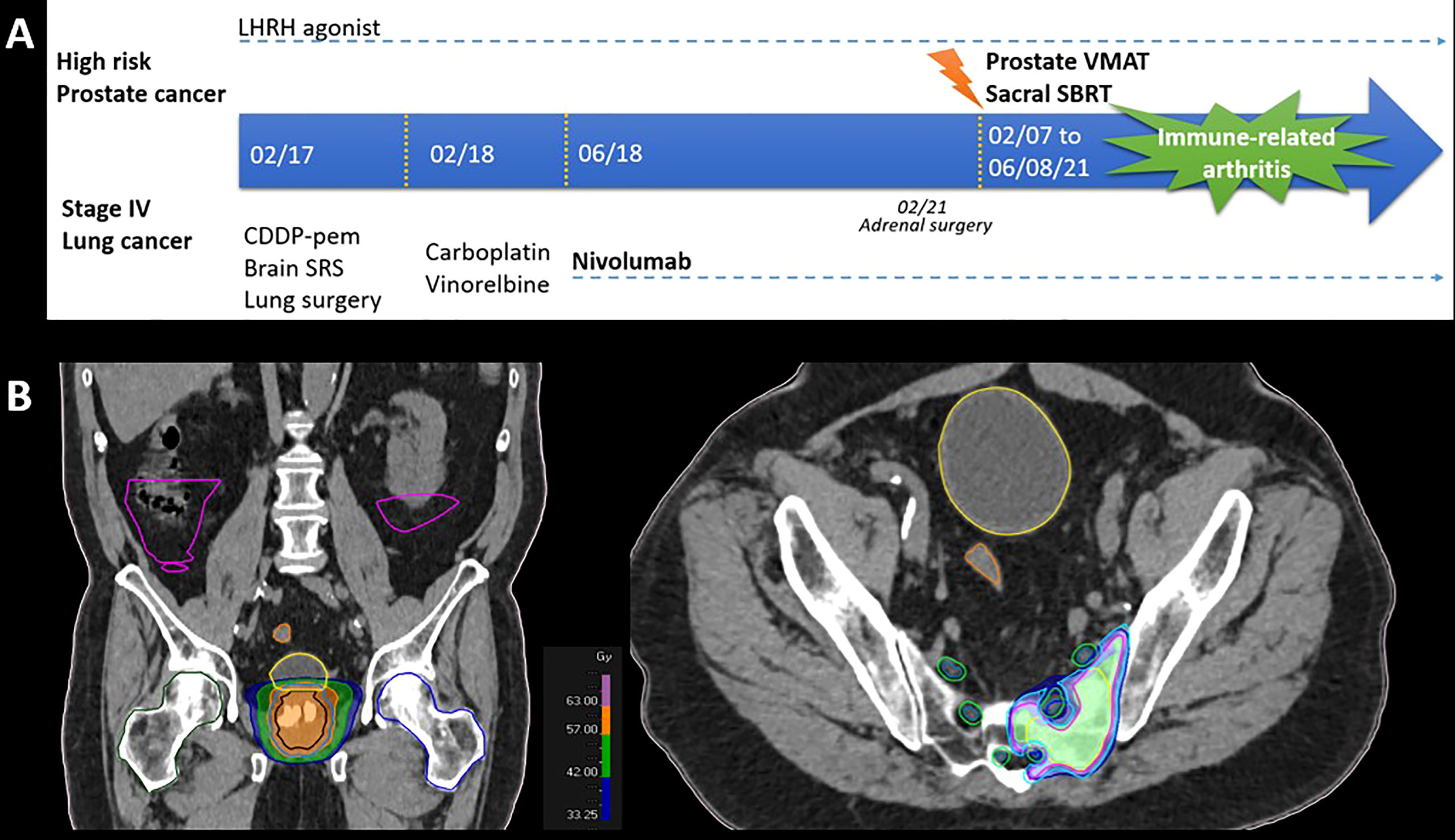
Figure 1 (A) Timelines and (B) radiation fields (images from the planning CT).
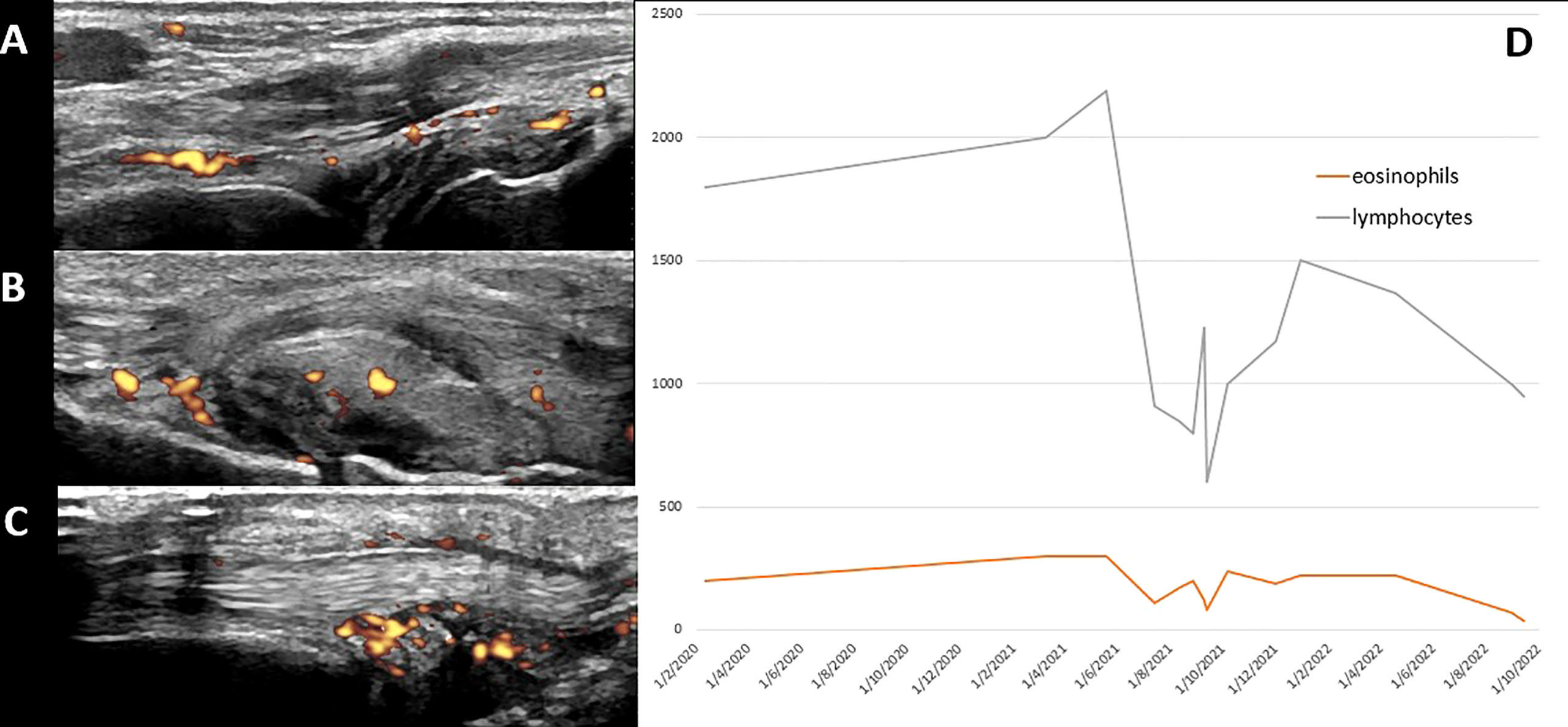
Figure 2 Diagnosis workup: ultrasound imaging (A: synovitis of the right wrist; B: synovitis of the right calcaneocuboid joint; C: tenosynovitis of the left extensor carpi ulnaris) and (D) plotting of blood counts.
Discussion
To the best of our knowledge, this is the first report of a radiotherapy-triggered out-of-field irAE occurring more than 3 years after commencing ICB. Although late-onset irAEs have been described in the absence of radiotherapy, late irAEs at 3 years or higher are uncommon. Arthralgia has generally been described in approximately 10% to 15% of patients. Median time to onset of immune-related arthritis was reported to be 70 days, ranging from 1 day to 650 days (5).
Concomitant immunoradiotherapy could theoretically increase toxicities (6). First randomized reports are however reassuring with no increase of unexpected adverse events when radiotherapy is combined to ICB (2, 7). There was no significant irAE increase in the PACIFIC (consolidation immunotherapy vs. placebo after thoracic chemoradiotherapy) trial (4). This remains to be confirmed as real-life data suggest higher rates of observed severe toxicities (8).
Prior ICB could increase radiation therapy toxicity. Radiation recall-induced ICB could be observed up to 2 years after the end of radiotherapy, matching the previously irradiated field (9). Prior irAEs could also be linked to an increased risk of radiation therapy side effects. In an analysis of 41 patients who had prior irAEs, 61% developed subsequent ≥grade 2 radiotherapy-induced radiation pneumonitis (10).
Whether this is an out-of-field irAE or simply an incidental event after radiotherapy with unusual late onset after ICB start would require further investigation, including possible surrogate biomarkers. Unfortunately, no translational research was performed in blood or tendon sheath aspiration. The diagnosis of immune-related arthritis was suspected after other arthritis causes were eliminated and given the observed timing after irradiation. However, immune non-related adverse events such as paraneoplastic syndrome cannot be totally excluded. It is also unknown if “curative” irradiation dose, schedule, and technique may have influenced the observed immune-related arthritis occurrence. In oligometastatic-ICB treated patients, maintaining ICB beyond progression and delivering stereotactic radiotherapy to oligoprogressive sites are under investigation. Particular attention should be paid in real-life practice and in future clinical trials (e.g., NCT02756793 and NCT04405401) where ICB starts prior to localized irradiation.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
Written informed consent was obtained from the individual AND for the publication of any potentially identifiable images or data included in this article
Author contributions
AL and MA: Conceptualization, Data curation, Formal analysis. AL and MA: Roles/Writing - original draft. All authors: Writing - review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mondini M, Levy A, Meziani L, Milliat F, Deutsch E. Radiotherapy-immunotherapy combinations - perspectives and challenges. Mol Oncol (2020) 14:1529–37. doi: 10.1002/1878-0261.12658
2. Theelen W, Chen D, Verma V, Hobbs BP, Peulen HMU, Aerts JGJV, et al. Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Respir Med (2021) 9:467–75. doi: 10.1016/S2213-2600(20)30391-X
3. Chargari C, Levy A, Paoletti X, Soria JC, Massard C, Weichselbaum RR, et al. Methodological development of combination drug and radiotherapy in basic and clinical research. Clin Cancer Res (2020) 26:4723–36. doi: 10.1158/1078-0432.CCR-19-4155
4. Spigel DR, Faivre-Finn C, Gray JE, Vicente D, Planchard D, Paz-Ares L, et al. Five-year survival outcomes from the PACIFIC trial: Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol (2022) 40(12):JCO2101308. doi: 10.1200/JCO.21.01308
5. Kostine M, Rouxel L, Barnetche T, Veillon R, Martin F, Dutriaux C, et al. Rheumatic disorders associated with immune checkpoint inhibitors in patients with cancer-clinical aspects and relationship with tumour response: A single-centre prospective cohort study. Ann Rheum Dis (2018) 77:393–8. doi: 10.1136/annrheumdis-2017-212257
6. Louvel G, Bahleda R, Ammari S, Le Péchoux C, Levy A, Massard C, et al. Immunotherapy and pulmonary toxicities: can concomitant immune-checkpoint inhibitors with radiotherapy increase the risk of radiation pneumonitis? Eur Respir J (2018) 51:1701737. doi: 10.1183/13993003.01737-2017
7. McBride S, Sherman E, Tsai CJ, Baxi S, Aghalar J, Eng J, et al. Randomized phase II trial of nivolumab with stereotactic body radiotherapy versus nivolumab alone in metastatic head and neck squamous cell carcinoma. J Clin Oncol (2021) 39:30–7. doi: 10.1200/JCO.20.00290
8. McDonald F, Mornex F, Garassino MC, Filippi AR, Christoph D, Haakensen VD, et al. 79MO PACIFIC-r: Real-world characteristics of unresectable stage III NSCLC patients treated with durvalumab after chemoradiotherapy. J Thorac Oncol (2021) 16:S738–9. doi: 10.1016/S1556-0864(21)01921-3
9. Deutsch E, Besse B, Le Pavec J, Le Péchoux C, Botticella A, Ammari S, et al. Can radiation-recall predict long lasting response to immune checkpoint inhibitors? Radiother Oncol (2021) 154:125–7. doi: 10.1016/j.radonc.2020.09.037
Keywords: radiation therapy, anti-PD(L)1, immunotherapy, toxicity, adverse (side) effects, immunoradiotherapy
Citation: Aldea M, Belkhir R, Colomba E, Blanchard P, Danlos F-X, Botticella A, Terlizzi M, Deutsch E, Le Péchoux C, Planchard D, Michot J-M, Besse B and Levy A (2022) Immune-related arthritis following pelvic radiation therapy in a patient with lung cancer receiving long-term immune checkpoint blocker treatment: Case report. Front. Immunol. 13:920130. doi: 10.3389/fimmu.2022.920130
Received: 14 April 2022; Accepted: 05 October 2022;
Published: 24 October 2022.
Edited by:
Udo S. Gaipl, University Hospital Erlangen, GermanyReviewed by:
Fernanda Herrera, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandKevin Sheng-Kai Ma, University of Pennsylvania, United States
Copyright © 2022 Aldea, Belkhir, Colomba, Blanchard, Danlos, Botticella, Terlizzi, Deutsch, Le Péchoux, Planchard, Michot, Besse and Levy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mihaela Aldea, TWloYWVsYS5BTERFQUBndXN0YXZlcm91c3N5LmZy; Antonin Levy, QW50b25pbi5MRVZZQGd1c3RhdmVyb3Vzc3kuZnI=