
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 15 June 2022
Sec. Autoimmune and Autoinflammatory Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.889021
This article is part of the Research Topic Co-Morbidities in Primary Sjögren's Syndrome: Underlying Immunological Mechanism - Vol II View all 8 articles
 Theodoros Androutsakos1
Theodoros Androutsakos1 Theodoros A. Voulgaris2Athanasios-Dimitrios Bakasis1Maria-Loukia Koutsompina1
Theodoros A. Voulgaris2Athanasios-Dimitrios Bakasis1Maria-Loukia Koutsompina1 Loukas Chatzis1Ourania D. Argyropoulou1
Loukas Chatzis1Ourania D. Argyropoulou1 Vasilis Pezoulas3,4Dimitrios I. Fotiadis3,4George Papatheodoridis2
Vasilis Pezoulas3,4Dimitrios I. Fotiadis3,4George Papatheodoridis2 Athanasios G. Tzioufas1†
Athanasios G. Tzioufas1† Andreas V. Goules1*†
Andreas V. Goules1*†Background: Primary Sjögren syndrome (pSS) is a systemic autoimmune epithelitis, potentially affecting salivary epithelium, biliary epithelium, and hepatocytes. Common immunological mechanisms might cause clinically silent liver inflammation, and combined with non-alcoholic fatty liver disease (NAFLD), liver fibrosis (LF) may occur. No studies have explored the occurrence of LF in the context of NAFLD among pSS patients.
Methods: Consecutive pSS patients from the rheumatology outpatient clinic of the Department of Pathophysiology and individuals evaluated in the hepatology outpatient clinic for possible NAFLD serving as comparators underwent transient elastography (TE) to assess LF and liver steatosis (LS). All participants had no overt chronic liver disease. Clinical, demographic, and laboratory data were collected from all participants at the time of TE.
Results: Fifty-two pSS patients and 198 comparators were included in the study. The median age (range) of pSS and comparators was 62.5 (30–81) and 55 (19–86) years, respectively. Both groups had similar prevalence regarding type 2 diabetes mellitus, hyperlipidemia, and similar body mass index (BMI). Patients with pSS had less frequently high LS (S2, S3) (27% vs. 62%, p < 0.001) and significant LF (F2–4) [2 (3.8%) vs. 34 (17.2%), p = 0.014] than comparators. Univariable analysis showed that advanced LF was significantly associated with older age, higher LS, greater BMI, and disease status (comparators than pSS); of these, only age was identified as an independent LF risk factor in the multivariable logistic regression analysis.
Conclusion: Liver fibrosis among pSS patients is most likely not attributed to the disease per se.
Liver fibrosis (LF) is characterized by excessive deposition of fibrous tissue into hepatic parenchyma that may progress into cirrhosis and liver failure. The most common etiologies of LF include non-alcoholic fatty liver disease (NAFLD) and alcoholic fatty liver disease, viral infections, drugs, and other less common chronic liver diseases either metabolic or autoimmune such as hemochromatosis, Wilson’s disease, primary biliary cholangitis (PBC), and autoimmune hepatitis (AIH). More specifically, NAFLD comprises a major health problem worldwide with a rapidly rising incidence and a prevalence of approximately 25%–35% in the general population (1–4). The most common predisposing factors of NAFLD are obesity, metabolic syndrome, type 2 diabetes mellitus (T2DM) and hyperlipidemia, all of which display an increasing incidence (1, 5, 6). NAFLD is in fact an umbrella disease, including all manifestations of lipid accumulation in the liver, ranging from simple liver fat deposition in more than 5% of hepatocytes [non-alcoholic fatty liver (NAFL)] to liver necroinflammation [non-alcoholic steatohepatitis (NASH)], fibrosis, and cirrhosis (7, 8). Liver biopsy (LB) is still the gold standard for diagnosis and staging of liver fibrosis (LF) and liver steatosis (LS), but it is an expensive and invasive procedure with a high sampling error and a high risk of complications including pain, bleeding, and very rarely death (9–13). LF can be assessed by various non-invasive methods, with transient elastography (TE) being one of the most reliable when performed by an experienced operator (14–17). Similarly, the presence of fat in the liver parenchyma can be easily diagnosed by several imaging modalities including TE (9, 10).
On the other hand, primary Sjögren’s syndrome (pSS) is a systemic autoimmune disease characterized by chronic lymphocytic infiltration of exocrine glands and especially salivary and lachrymal glands, with the potential to affect almost any internal organ. Liver has been traditionally considered as one of the most commonly involved extra-glandular organ in the context of pSS, although the exact prevalence varies widely among different studies mainly due to the heterogeneity of the definition of hepatic disease. Sjögren’s syndrome-associated liver disease is clinically expressed as abnormal liver function tests, most likely due to PBC and/or AIH. Older studies supported that liver disease prevalence ranges between 5% and 27% (18–20), while more recent studies report even higher prevalence varying from 10% to 49% (21–23). Apart from pSS-associated PBC and AIH, LFT elevation among pSS patients could be attributed also to NAFLD, drug hepatotoxicity, and hepatitis B and C infections (21–27). Thus, the chronic and long-standing inflammatory state observed in the liver of pSS patients combined with other common comorbidities might promote the development of liver fibrosis in pSS sub-clinically and before overt liver involvement. Surprisingly, no epidemiologic or pathophysiological studies have been conducted to explore the association of LF and NAFLD in the context of pSS. The current study aims to investigate the prevalence of LF among pSS patients without overt liver disease, by performing TE, in comparison with NAFLD individuals, and after careful consideration of common comorbidities and potential confounders.
Consecutive pSS patients aged >18 years, who fulfilled the 2016 ACR/EULAR criteria and were followed in the rheumatology outpatient clinic of the Department of Pathophysiology at the General Hospital of Athens “Laiko” from June 1 to December 31 of 2021, were included in the current study. Individuals who were evaluated in the hepatology outpatient clinics of the Department of Pathophysiology and the Department of Gastroenterology at the General Hospital of Athens “Laiko” for possible NAFLD based on ultrasonographic criteria (higher echogenicity than renal cortex) served as the comparator group.
The exclusion criteria were as follows: (i) patients who were concomitantly diagnosed with other systemic autoimmune rheumatic disease or IgG4-related disorder; (ii) patients with incomplete laboratory testing, such as antinuclear antibody, anti-SSA/Ro, and anti-SSB/La, at diagnosis; (iii) patients who did not undergo minor salivary gland biopsy; (iv) patients who were under chemotherapy for solid or hematological malignancies; (v) patients with transaminasemia at the time of TE; (vi) patients with either medical history or laboratory tests suggesting non-NAFLD chronic liver diseases including chronic hepatitis B and C infections, heart failure, alcoholic or metabolic liver diseases, drug hepatotoxicity, as well as the presence of liver cirrhosis; and (vii) patients demonstrating hepatic structural abnormalities on ultrasonography that may affect TE. Transaminasemia was defined as the presence of alanine (ALT) and/or aspartate (AST) aminotransferases >3× the upper limit of normal (ULN) and alkaline phosphatase >2× ULN, while cirrhosis was diagnosed based on previous TE, radiographic, biochemical, or histological findings according to guidelines (28).
All participants underwent TE by a specialized operator blindly, to measure both liver stiffness for LF and controlled attenuation parameter (CAP) for LS. For LF, the following liver stiffness cutoffs were used: F0–F1: 2–7 kilopascals (kPa), F2: 7–10 kPa, F3: 10–14 kPa, and F4: >14 kPa. The LF stage of F0–F1 was considered as clinically insignificant and F2–F4 was considered as significant (29). For LS, the following CAP cutoffs were used: S0: 100–238 decibels/meter (dB/m), S1: 238–260 dB/m, S2: 260–290 dB/m, and S3: >290 dB/m. LS stage S0–S1 was classified as low and S2–S3 was classified as high (29). Patients were characterized as having diabetes if they were on antidiabetic treatment or if their blood sugar level during testing was >126 mg/dl or >200 mg/dl for fasting or non-fasting patient, respectively, and as hyperlipidemic if they were on hypolipidemic treatment or if their fasting cholesterol level was >200 mg/dl and/or LDL was >130 mg/dl after double checking at least 3 months apart (30, 31). In order to exclude concomitant liver diseases other than NAFLD, laboratory testing for exclusion of viral and autoimmune hepatitis was performed before TE, while alcohol-related liver disease was defined as liver damage attributed to alcohol overuse (more than 3 drinks on any day or more than 7 drinks per week for women and more than 4 drinks on any day or more than 14 drinks per week for men) according to national abuse and alcoholism guidelines (32). Demographic, clinical, and laboratory data were recorded for all participants, while for pSS patients, the immunologic profile, the cumulative dose and duration of methotrexate and prednisone, and the European League Against Rheumatism Sjögren's Syndrome Disease Activity Index (ESSDAI) at the time of diagnosis were additionally calculated and collected (33, 34). All systemic manifestations of pSS were defined based on the ESSDAI definitions and small airways as described previously (34, 35). Patients with pSS (study group) were compared with individuals with NAFLD (comparator group) in terms of LF and LS, and various subgroup analyses were performed.
All tests were routinely performed as standard of care, while the TE procedure was non-invasive. Therefore, ethical committee approval was unnecessary. All patients were explicitly informed about the nature of the study and the investigations performed, and they gave written consent for their participation and use of data for research purposes. The study was in compliance with the general protection rule regulation (GDPR) of the European Union.
Statistical analysis for numerical data was performed with Mann–Whitney or t-test after applying the Shapiro–Wilk normality test and categorical data by Fisher’s exact test when cell counts <5 patients or chi-square test with Yate’s correction accordingly. Multivariable logistic regression models were constructed for LF and LS to identify independent risk factors based on univariate analysis results between high and low fibrosis and steatosis participants, respectively. Correlations between liver fibrosis and steatosis with several parameters were also explored by either point biserial or Pearson coefficient. Statistical analysis was performed in Python 3.6 and GraphPad 7.0a.
As shown in Table 1, a total of 52 patients with pSS (49 female patients, 94.2%) and 198 comparators (104 female patients, 52.5%) underwent TE. The median age (range) of pSS and comparators was 62.5 (30–81) and 55 (19–86) years, respectively. The median disease durations (range) of pSS from disease onset and diagnosis were 8 (1–46) and 3 (1–37) years, respectively. Comparators and pSS patients had comparable prevalence regarding T2DM, hyperlipidemia, and body mass index (BMI) (Table 1). The distribution of LS grading S0, S1, S2, and S3 was 22 (42.3%), 16 (30.8%), 6 (11.5%), and 8 (15.4%) in pSS patients, and 50 (20%), 63 (25.2%), 56 (22.4%), and 81 (32.4%) among comparators, respectively. The distribution of LF grading F0–F1, F2, and F3 was 50 (96.2%), 1 (1.9%), and 1 (1.9%) in pSS patients, and 214 (85.6%), 25 (10%), and 11 (4.4%) in comparators, respectively. After classification according to TE and clinical significance, high LS was found in 27% (n = 14) of pSS patients in comparison with 62% (n = 123) of the comparator group, while significant LF was found in 3.8% (n = 2) of SS patients and 17.2% (n = 37) in the comparator group.
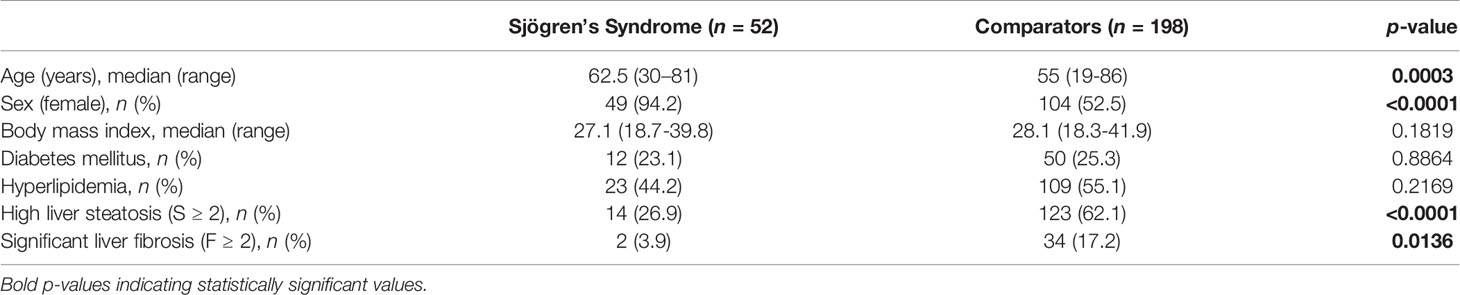
Table 1 Comparison between patients with pSS and comparators.
Given the low number of male pSS patients in our cohort and the fact that pSS is a female predominant disease, the female pSS patients (n = 49) were compared with matched female comparators (n = 39) according to age by randomly selecting those female comparators with an age range that of the median age of female pSS ± 5 years. No difference was identified in terms of T2DM, hyperlipidemia, and BMI between the 2 groups, except for higher LS in the comparators (64% vs. 24%, p = 0.004) accompanied by a strong trend for LF (15.4% vs. 4%) but not reaching statistical significance (Supplementary Table 1). In this line, female pSS patients with low LS (n = 37) had no difference in terms of LF or other confounders compared to low LS comparators (n = 46), except for age (pSS = 64 vs. Comparators = 57 years, p = 0.023) (Supplementary Table 2).
From the 250 participants, 214 had insignificant and 36 significant LF, of whom 2 belonged to the study group and 34 belonged to the comparators. In univariable analyses including T2DM, hyperlipidemia, BMI, age, sex, steatosis, and disease status (pSS or comparators), significant LF was significantly associated with older age, higher LS, greater BMI, and disease status (comparators than pSS) (Table 2). In multivariable analysis, age was identified as the only independent risk factor for LF (Table 3; Supplementary Figure 1). In this line, LF was significantly correlated with age as suggested by point biserial analysis (p = 0.005), but with a weak coefficient (r = 0.18) (Supplementary Figure 2)
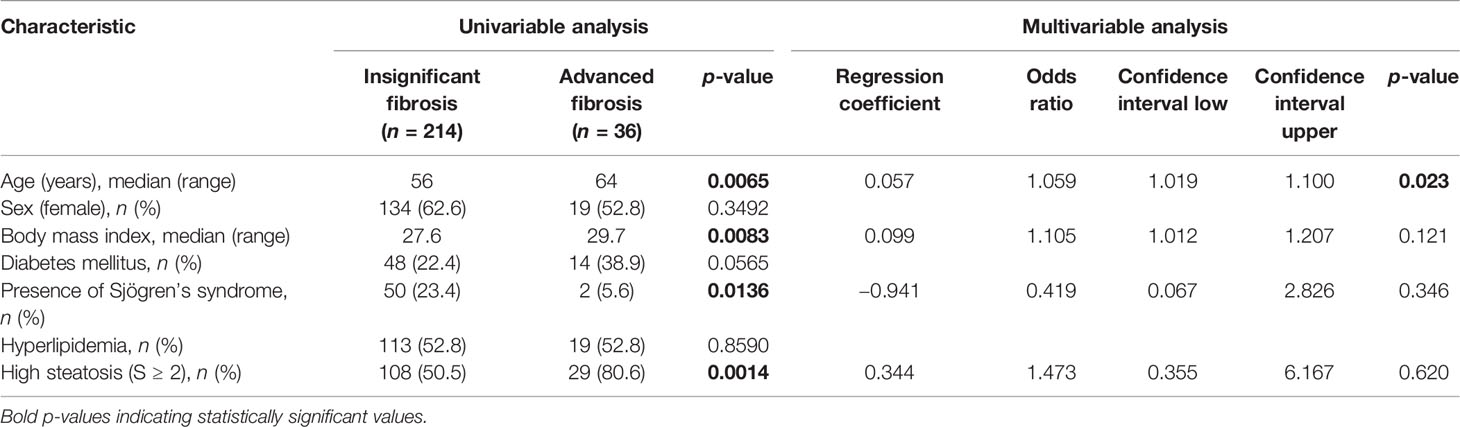
Table 2 Comparison between study participants with low and high liver fibrosis.
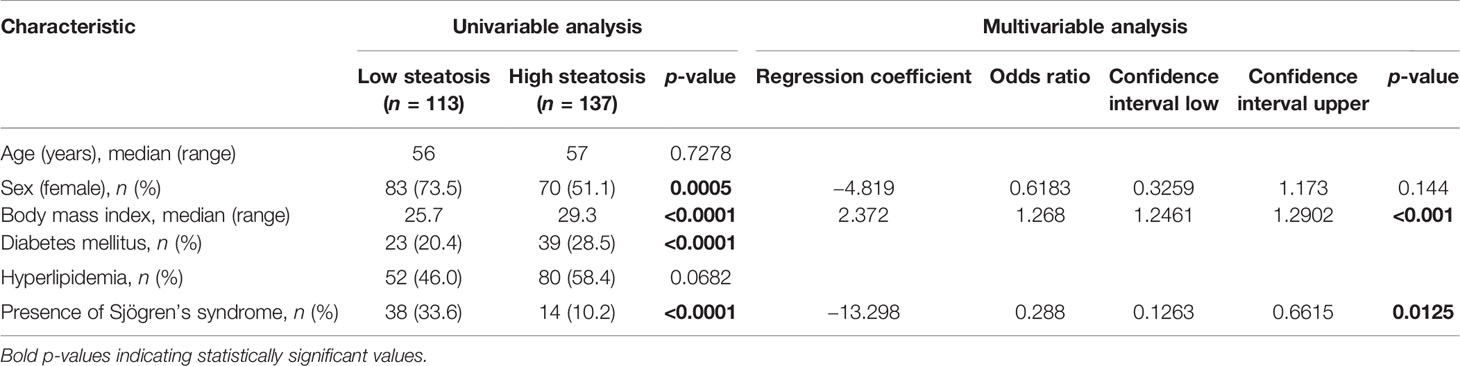
Table 3 Comparison between study participants with low and high steatosis.
From the 250 participants, 113 had low and 137 had high LS, of whom 14 belonged to the study group and 123 belonged to the comparators. In univariable analyses including age, sex, BMI, T2DM, hyperlipidemia, and disease status (pSS or comparators), high LS was significantly associated with sex, BMI, T2DM, and disease status (comparators than pSS) (Table 3). In multivariable analysis, BMI was positively correlated with high LS, while the presence of pSS was inversely associated with LS (Table 2; Supplementary Figure 3). Accordingly, LS was significantly correlated with BMI by point biserial analysis (p < 0.0001), but with a weak coefficient (r = 0.42) (Supplementary Figure 4)
Two pSS patients had significant LF; the first case referred to a 68-year-old female patient with a BMI of 29 kg/m2 and concomitant T2DM and arterial hypertension for 8 and 10 years, respectively, at the time of TE. She was diagnosed with pSS 8 years ago, complaining about persistent dry eyes and the laboratory workup revealed positive anti-nuclear antibodies (ANA) at a dilution of 1:160, positive anti-Ro/SSA autoantibodies, and a positive minor labial salivary gland biopsy. TE revealed stage 3 LS and stage 3 LF. She received proper treatment regarding her T2DM and arterial hypertension, and she never received methotrexate or prednisone for her primary disease. The second case referred to a 61-year-old female patient with a BMI of 33 kg/m2 at the time of TE. Her past medical history was otherwise unremarkable. She was diagnosed with pSS 11 years ago, based on dry mouth, dry eyes, Raynaud phenomenon, fatigue, and severe arthralgias of both hands. Laboratory tests were positive for ANA at a dilution of 1:160 exhibiting an anti-centromere antibody pattern at 1:1.280 while minor labial salivary biopsy was positive. She has been treated with methotrexate (cumulative dose of 7,800 mg) for a total of 11 years. TE revealed stage 2 LS and stage 2 LF.
Regarding SS patients with insignificant LF, the vast majority were female patients (47, 94%) with a median (range) age of 62.5 (30–81) years. The median disease duration (range) from diagnosis was 3 (1–37) years and that from pSS onset was 8 (1–46) years, while the median ESSDAI at disease diagnosis was 4 (0–20). The clinical manifestations of pSS patients with insignificant LF included oral dryness (88%, n = 44), ocular dryness (84%, n = 42), salivary gland enlargement (SGE) (22%, n = 11), arthritis (18%, n = 9), arthralgias (74%, n = 37), Raynaud’s phenomenon (31.8%, n = 19), interstitial lung involvement (10%, n = 5), small airways disease (6%, n = 3), interstitial renal disease (2% (n = 1), generalized lymphadenopathy (4%, n = 2), palpable purpura (14%, n = 14), and lymphoma (17%, n = 7); the autoantibody and laboratory profiles were as follows: anti-SSA antibodies (70%, n = 35), anti-SSB antibodies (58%, n = 29), rheumatoid factor (24%, n = 12), ANA antibodies (86%, n = 43), and low C4 (10%, n = 5). Sixteen of 50 patients (32%) were receiving corticosteroids at a median cumulative dose of 4,993 mg of prednisolone (range 610–94,800) for a median of 16.5 (range 8–272) months, and 9 patients (18%) were receiving methotrexate at a median cumulative dose of 3,130 mg (330–7,800) for a median of 63 (range 11–130) months. A total of 15 patients were receiving hydroxychloroquine at a median cumulative dose of 60 g (range 12–1,296 g) for a median of 10 (range 2–216) months. No correlations regarding treatment regimens were observed.
The fact that pSS affects liver frequently implies shared epitopes or epitope spreading across epithelial structures and particularly among salivary epithelium, biliary epithelium, and/or hepatocytes (27). In this case, a clinically silent chronic inflammatory process may evolve into liver parenchyma leading to LF (36–38). Fibrogenesis may be further promoted by several comorbidities or drugs, and therefore, it is reasonable to assume that LF might occur in higher prevalence among pSS patients compared to the general population. In the current study, LF and LS among pSS consecutive patients were assessed by TE, and a comparator group with individuals highly suspicious for NAFLD served as controls. The prevalence of significant LF among pSS reached 4% as opposed to 17% of the comparators, of whom 62% also showed a high degree of LS. The 2 groups also differed in terms of sex, age, and LS but not in other confounders of LF such as T2DM, hyperlipidemia, and BMI. However, in the multivariable analysis, only age and not LS was identified as an independent risk factor for LF, most likely due to the relatively low total number of individuals with significant LF. This particular association was further supported by the positive correlation between age and LF as attested through the point biserial analysis. Accordingly, subgroup analysis in female patients matched according to age between the 2 groups, and revealed a link between LF and LS as expected. Interestingly, in this specific cohort, high LS was positively associated with BMI and negatively associated with pSS; this negative association most likely represents a better control of pSS patients upon BMI or other comorbidities related to LS rather than an underlying protective pathogenetic mechanism. Taken together, it seems that pSS per se is not associated with significant LF or LS.
In our study, the prevalence of significant LF in pSS is similar to that of the general population (17). The estimated global prevalence of LF is approximately 5%, while NAFLD reaches 30% and thus pSS patients seem to display similar levels of LF and LS to the general population, most likely driven by classical risk factors (3, 6). In a previous study assessing the occurrence of LF in pSS patients, significant LF was found in 12% of cases after a disease duration period of 3.5 years, with low serum albumin, low white blood cell count, and high AST independently predicting significant LF (35). However, in that study, no comparator/control group was employed, and NAFLD/LS was not taken into account. At this point, we would like to emphasize that, since NAFLD is quite common in the general population, a control group of completely healthy individuals is not easy to be recruited. Furthermore, the reported association of significant LF with low white blood cell count could not be interpreted appropriately in the context of pSS (35). In comparison, pSS patients with insignificant LF in our cohort had similar disease duration, and were much older with more than a decade difference, and some of them received MTX and/or prednisone treatment, but still none developed clinically significant LF. On the contrary, the 2 pSS patients who presented with advanced LF had classical risk factors such as T2DM, high LS, or increased BMI, and one had been receiving MTX for many years, suggesting that pSS itself is most likely not associated with LF.
Our study has some limitations. Firstly, it is a retrospective study, since the TE was performed during the follow-up period and not at the time of pSS diagnosis; thus, it is by definition subject to selection and/or recall biases. Secondly, it is a single-center study on a fixed genetic background that may affect the outcome of both LF and LS. Thirdly, the number of recruited pSS patients and the disease duration may be relatively low—although the true disease course is longer—to study the fibrosis outcome of such a rare and long-standing process. Finally, the true effect of drugs cannot be easily evaluated, since apart from the cumulative dose and duration, specific drug combinations may interfere with the fibrogenesis procedure.
In conclusion, LF in pSS patients is most likely attributed to classical risk factors such as those in the general population and not to the disease per se, since pSS patients did not show an increased prevalence of LF compared to patients with NAFLD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
TA, GP, AG, and AT were involved in study design. M-LK, A-DB, LC, and OA collected patients’ data and blood samples. TV performed all transient elastographies. Data analysis and interpretation were performed by VP, DF, and AG. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.889021/full#supplementary-material
1. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology (2016) 64(1):73–84. doi: 10.1002/hep.28431
2. Li J, Zou B, Yeo YH, Feng Y, Xie X, Lee DH, et al. Prevalence, Incidence, and Outcome of Non-Alcoholic Fatty Liver Disease in Asia, 1999-2019: A Systematic Review and Meta-Analysis. Lancet Gastroenterol Hepatol (2019) 4(5):389–98. doi: 10.1016/s2468-1253(19)30039-1
3. Le MH, Yeo YH, Li X, Li J, Zou B, Wu Y, et al. 2019 Global Nafld Prevalence: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol (2021) S1542-3565(21)01280-5. doi: 10.1016/j.cgh.2021.12.002
4. Ciardullo S, Perseghin G. Prevalence of Nafld, Mafld and Associated Advanced Fibrosis in the Contemporary United States Population. Liver Int (2021) 41(6):1290–3. doi: 10.1111/liv.14828
5. Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic Steatohepatitis: A Review. JAMA (2020) 323(12):1175–83. doi: 10.1001/jama.2020.2298
6. Ayada I, van Kleef LA, Alferink LJM, Li P, de Knegt RJ, Pan Q. Systematically Comparing Epidemiological and Clinical Features of Mafld and Nafld by Meta-Analysis: Focusing on the Non-Overlap Groups. Liver Int (2022) 42(2):277–87. doi: 10.1111/liv.15139
7. Hui JM, Kench JG, Chitturi S, Sud A, Farrell GC, Byth K, et al. Long-Term Outcomes of Cirrhosis in Nonalcoholic Steatohepatitis Compared With Hepatitis C. Hepatology (2003) 38(2):420–7. doi: 10.1053/jhep.2003.50320
8. Bugianesi E, Leone N, Vanni E, Marchesini G, Brunello F, Carucci P, et al. Expanding the Natural History of Nonalcoholic Steatohepatitis: From Cryptogenic Cirrhosis to Hepatocellular Carcinoma. Gastroenterology (2002) 123(1):134–40. doi: 10.1053/gast.2002.34168
9. Easl-Easd-Easo Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J Hepatol (2016) 64(6):1388–402. doi: 10.1016/j.jhep.2015.11.004
10. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology (2018) 67(1):328–57. doi: 10.1002/hep.29367
11. Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD. Liver Biopsy. Hepatology (2009) 49(3):1017–44. doi: 10.1002/hep.22742
12. Intraobserver and Interobserver Variations in Liver Biopsy Interpretation in Patients With Chronic Hepatitis C. The French Metavir Cooperative Study Group. Hepatology (1994) 20(1 Pt 1):15–20. doi: 10.1002/hep.1840200104
13. Boyum JH, Atwell TD, Schmit GD, Poterucha JJ, Schleck CD, Harmsen WS, et al. Incidence and Risk Factors for Adverse Events Related to Image-Guided Liver Biopsy. Mayo Clin Proc (2016) 91(3):329–35. doi: 10.1016/j.mayocp.2015.11.015
14. Tapper EB, Loomba R. Noninvasive Imaging Biomarker Assessment of Liver Fibrosis by Elastography in Nafld. Nat Rev Gastroenterol Hepatol (2018) 15(5):274–82. doi: 10.1038/nrgastro.2018.10
15. Cassinotto C, Boursier J, Paisant A, Guiu B, Irles-Depe M, Canivet C, et al. Transient Versus Two-Dimensional Shear-Wave Elastography in a Multistep Strategy to Detect Advanced Fibrosis in Nafld. Hepatology (2021) 73(6):2196–205. doi: 10.1002/hep.31655
16. Tsai E, Lee TP. Diagnosis and Evaluation of Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis, Including Noninvasive Biomarkers and Transient Elastography. Clin Liver Dis (2018) 22(1):73–92. doi: 10.1016/j.cld.2017.08.004
17. Ginès P, Castera L, Lammert F, Graupera I, Serra-Burriel M, Allen AM, et al. Population Screening for Liver Fibrosis: Toward Early Diagnosis and Intervention for Chronic Liver Diseases. Hepatology (2022) 75(1):219–28. doi: 10.1002/hep.32163
18. Bloch KJ, Buchanan WW, Wohl MJ, Bunim JJ. Sjoegren's Syndrome. A Clinical, Pathological, and Serological Study of Sixty-Two Cases. Med (Baltimore) (1965) 44:187–231. doi: 10.1097/00005792-196505000-00001
19. Lindgren S, Manthorpe R, Eriksson S. Autoimmune Liver Disease in Patients With Primary Sjögren's Syndrome. J Hepatol (1994) 20(3):354–8. doi: 10.1016/s0168-8278(94)80007-3
20. Skopouli FN, Barbatis C, Moutsopoulos HM. Liver Involvement in Primary Sjögren's Syndrome. Br J Rheumatol (1994) 33(8):745–8. doi: 10.1093/rheumatology/33.8.745
21. Ramos-Casals M, Sánchez-Tapias JM, Parés A, Forns X, Brito-Zerón P, Nardi N, et al. Characterization and Differentiation of Autoimmune Versus Viral Liver Involvement in Patients With Sjögren's Syndrome. J Rheumatol (2006) 33(8):1593–9.
22. Montaño-Loza AJ, Crispín-Acuña JC, Remes-Troche JM, Uribe M. Abnormal Hepatic Biochemistries and Clinical Liver Disease in Patients With Primary Sjögren's Syndrome. Ann Hepatol (2007) 6(3):150–5. doi: 10.1016/S1665-2681(19)31920-9
23. Kaplan MJ, Ike RW. The Liver Is a Common Non-Exocrine Target in Primary Sjögren's Syndrome: A Retrospective Review. BMC Gastroenterol (2002) 2:21. doi: 10.1186/1471-230x-2-21
24. Ramos-Casals M, García-Carrasco M, Cervera R, Rosas J, Trejo O, de la Red G, et al. Hepatitis C Virus Infection Mimicking Primary Sjögren Syndrome. A Clinical and Immunologic Description of 35 Cases. Med (Baltimore) (2001) 80(1):1–8. doi: 10.1097/00005792-200101000-00001
25. Jorgensen C, Legouffe MC, Perney P, Coste J, Tissot B, Segarra C, et al. Sicca Syndrome Associated With Hepatitis C Virus Infection. Arthritis Rheum (1996) 39(7):1166–71. doi: 10.1002/art.1780390714
26. Ebert EC. Gastrointestinal and Hepatic Manifestations of Sjogren Syndrome. J Clin Gastroenterol (2012) 46(1):25–30. doi: 10.1097/MCG.0b013e3182329d9c
27. Sun Y, Zhang W, Li B, Zou Z, Selmi C, Gershwin ME. The Coexistence of Sjögren's Syndrome and Primary Biliary Cirrhosis: A Comprehensive Review. Clin Rev Allergy Immunol (2015) 48(2-3):301–15. doi: 10.1007/s12016-015-8471-1
28. Easl Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis - 2021 Update. J Hepatol (2021) 75(3):659–89. doi: 10.1016/j.jhep.2021.05.025
29. Eddowes PJ, Sasso M, Allison M, Tsochatzis E, Anstee QM, Sheridan D, et al. Accuracy of Fibroscan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology (2019) 156(6):1717–30. doi: 10.1053/j.gastro.2019.01.042
30. American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care (2018) 41(Suppl 1):S13–s27. doi: 10.2337/dc18-S002
31. Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr Pract (2017) 23(Suppl 2):1–87. doi: 10.4158/ep171764.Appgl
32. (NIAAA) NIoAAaA. Drinking Levels Defined (2022). Available at: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking.
33. Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren's Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol (2017) 69(1):35–45. doi: 10.1002/art.39859
34. Seror R, Bowman SJ, Brito-Zeron P, Theander E, Bootsma H, Tzioufas A, et al. Eular Sjögren's Syndrome Disease Activity Index (Essdai): A User Guide. RMD Open (2015) 1(1):e000022. doi: 10.1136/rmdopen-2014-000022
35. Lee SW, Kim BK, Park JY, Kim do Y, Ahn SH, Song J, et al. Clinical Predictors of Silent But Substantial Liver Fibrosis in Primary Sjogren's Syndrome. Mod Rheumatol (2016) 26(4):576–82. doi: 10.3109/14397595.2015.1113629
36. Delgado ME, Cárdenas BI, Farran N, Fernandez M. Metabolic Reprogramming of Liver Fibrosis. Cells (2021) 10(12):3604. doi: 10.3390/cells10123604
37. Caligiuri A, Gentilini A, Pastore M, Gitto S, Marra F. Cellular and Molecular Mechanisms Underlying Liver Fibrosis Regression. Cells (2021) 10(10):2759. doi: 10.3390/cells10102759
Keywords: non-alcoholic fatty liver disease, Sjögren’s syndrome, liver fibrosis, liver steatosis, transient elastography
Citation: Androutsakos T, Voulgaris TA, Bakasis A-D, Koutsompina M-L, Chatzis L, Argyropoulou OD, Pezoulas V, Fotiadis DI, Papatheodoridis G, Tzioufas AG and Goules AV (2022) Liver Fibrosis in Primary Sjögren’s Syndrome. Front. Immunol. 13:889021. doi: 10.3389/fimmu.2022.889021
Received: 03 March 2022; Accepted: 13 May 2022;
Published: 15 June 2022.
Edited by:
Marjan A. Versnel, Erasmus Medical Center, NetherlandsReviewed by:
Egidia Miftode, Grigore T. Popa University of Medicine and Pharmacy, RomaniaCopyright © 2022 Androutsakos, Voulgaris, Bakasis, Koutsompina, Chatzis, Argyropoulou, Pezoulas, Fotiadis, Papatheodoridis, Tzioufas and Goules. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreas V. Goules, YWdvdWxlc0BtZWQudW9hLmdy
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.