 Violette Dirix1Philippe Collart2Anne Van Praet1
Violette Dirix1Philippe Collart2Anne Van Praet1 Maya Hites3
Maya Hites3 Nicolas Dauby4,5Sabine Allard6
Nicolas Dauby4,5Sabine Allard6 Judith Racapé7
Judith Racapé7 Mahavir Singh8
Mahavir Singh8 Camille Locht9
Camille Locht9 Françoise Mascart1*
Françoise Mascart1* Véronique Corbière1
Véronique Corbière1- 1Laboratory of Vaccinology and Mucosal Immunity, Université Libre de Bruxelles (U.L.B.), Brussels, Belgium
- 2Biostatistiques du Pôle Santé (BIOPS), Université Libre de Bruxelles (U.L.B.), Brussels, Belgium
- 3Clinique des maladies infectieuses et tropicales, Hôpital Erasme, Université Libre de Bruxelles (U.L.B.), Brussels, Belgium
- 4Department of Infectious Diseases, Centre Hospitalier Universitaire Saint-Pierre, Université Libre de Bruxelles (U.L.B.), Brussels, Belgium
- 5Institute for Medical Immunology, Université Libre de Bruxelles (U.L.B.), Brussels, Belgium
- 6Dienst Interne Geneeskunde - Infectiologie, Universitair Ziekenhuis Brussel (UZ Brussel), Vrije Universiteit Brussel (VUB), Brussels, Belgium
- 7Biomedical Research Center, Erasme Hospital, Brussels, Belgium
- 8Lionex Diagnostics and Therapeutics, Braunschweig, Germany
- 9Univ. Lille, CNRS, Inserm, CHU Lille, Institut Pasteur de Lille, U1019 – UMR9017 – CIIL – Center for Infection and Immunity of Lille, Lille, France
Active tuberculosis (aTB) remains a major killer from infectious disease, partially due to delayed diagnosis and hence treatment. Classical microbiological methods are slow and lack sensitivity, molecular techniques are costly and often unavailable. Moreover, available immuno-diagnostic tests lack sensitivity and do not differentiate between aTB and latent TB infection (LTBI). Here, we evaluated the performance of the combined measurement of different chemokines/cytokines induced by two different stage-specific mycobacterial antigens, Early-secreted-antigenic target-6 (ESAT-6) and Heparin-binding-haemagglutinin (HBHA), after a short in vitro incubation of either peripheral blood mononuclear cells (PBMC) or whole blood (WB). Blood samples were collected from a training cohort comprising 22 aTB patients, 22 LTBI subjects and 17 non-infected controls. The concentrations of 13 cytokines were measured in the supernatants. Random forest analysis identified the best markers to differentiate M. tuberculosis-infected from non-infected subjects, and the most appropriate markers to differentiate aTB from LTBI. Logistic regression defined predictive abilities of selected combinations of cytokines, first on the training and then on a validation cohort (17 aTB, 27 LTBI, 25 controls). Combining HBHA- and ESAT-6-induced IFN-γ concentrations produced by PBMC was optimal to differentiate infected from non-infected individuals in the training cohort (100% correct classification), but 2/16 (13%) patients with aTB were misclassified in the validation cohort. ESAT-6-induced-IP-10 combined with HBHA-induced-IFN-γ concentrations was selected to differentiate aTB from LTBI, and correctly classified 82%/77% of infected subjects as aTB or LTBI in the training/validation cohorts, respectively. Results obtained on WB also selected ESAT-6- and HBHA-induced IFN-γ concentrations to provided discrimination between infected and non-infected subjects (89%/90% correct classification in the training/validation cohorts). Further identification of aTB patients among infected subjects was best achieved by combining ESAT-6-induced IP-10 with HBHA-induced IL-2 and GM-CSF. Among infected subjects, 90%/93% of the aTB patients were correctly identified in the training/validation cohorts. We therefore propose a two steps strategy performed on 1 mL WB for a rapid identification of patients with aTB. After elimination of most non-infected subjects by combining ESAT-6 and HBHA-induced IFN-γ, the combination of IP-10, IL-2 and GM-CSF released by either ESAT-6 or HBHA correctly identifies most patients with aTB.
Introduction
Tuberculosis (TB) remains a leading cause of death in the world, responsible for high morbidity and mortality worldwide with about 10 million new cases in 2020 and 1.5 million deaths (1). Diagnosis and hence appropriate treatment are often delayed due to the wide spectrum of clinical manifestations of active TB (aTB) and to the non-availability of sensitive and specific tests providing a rapid and accurate diagnosis (2, 3). In addition to classical clinical manifestations of aTB, this disease may occur as subclinical TB without suggestive symptoms, or as extrapulmonary TB often pauci-symptomatic in immunocompromised individuals, so that diagnosis strictly based on clinical signs or symptoms is illusive (2). The classical diagnostic method remains the identification of M. tuberculosis by direct smear microscopy or by culture that are both low in sensitivity and/or slow. Early diagnosis of infectious cases by sputum microscopy is only possible in approximately 50% of cases. Moreover, people with subclinical TB may likely be missed if TB culture is not performed and this is often the case in asymptomatic individuals. Molecular techniques such as GeneXpert are more sensitive but they are costly and often unavailable in primary-care settings.
Immuno-diagnosis was therefore identified as a promising approach for diagnosis of aTB. However, the commercially available tests, the interferon-γ-release assays (IGRA), based on the release of IFN-γ by blood cells in response to their in vitro stimulation with mycobacterial peptides corresponding to antigens encoded in the genomic region of difference (RD)-1 (the early-secreted-antigenic-target-6 (ESAT-6), and the culture-filtrate-protein-10 (CFP-10)), have a relatively high false negative rate in patients with aTB (4–6). In addition, these IGRAs, initially developed to diagnose latent TB infection (LTBI), are positive both in LTBI and in patients with aTB (7). The differential diagnosis of LTBI and aTB is therefore not possible with commercial IGRAs. New generation IGRAs were developped to improve the diagnosis of aTB. They are based either on recent studies indicating that the M. tuberculosis specific CD8+ T cell responses are positively correlated with the bacterial load and recent exposure to M. tuberculosis for the QuantiFERON-TB Gold Plus, or by inclusion of L-alanine dehydrogenase as an additional antigen for the LIOFeron TB/LTBI (8, 9). The added value of these improvements for the diagnosis of aTB and its differential diagnosis with LTBI was however not confirmed until now (8).
Therefore, several studies aimed to identify other proteins from M. tuberculosis as potential candidates to distinguish aTB from LTBI and they often also extend the cytokine measurements beyond IFN-γ to improve differential diagnosis. These studies generally first identify markers of M. tuberculosis infection, before applying one or several biomarkers to differentiate aTB from LTBI. Among the numerous proteins evaluated, the mycobacterial heparin-binding haemagglutinin (HBHA, Rv0475) appears as one of the most promising antigens to differentiate LTBI from aTB, but only few studies assessed HBHA-induced cytokines other than IFN-γ (10–12). In contrast, the potential added value of various cytokines induced by the peptides of the commercial IGRAs has been investigated, but with conflicting outcomes, as highlighted by a recent meta-analysis (13).
We previously reported on a combined HBHA- and ESAT-6-IGRA performed on either peripheral blood mononuclear cells (PBMC) or whole blood (WB) to diagnose LTBI and to partially differentiate LTBI from aTB (14–16). Even though this combined IGRA provided a better discrimination between LTBI and aTB than any other available in vitro test, it remained imperfect. In this study, we therefore measured cytokines/chemokines other than IFN-γ released in response to HBHA and to ESAT-6 and evaluated the potential added value of a combined analysis of cytokine/chemokine secretion for the differential diagnosis and especially for the diagnosis of aTB.
Material and Methods
Ethics Statement
The study protocol P2011/113 was approved by the ethics committee of ULB-Hôpital Erasme, Brussels, Belgium, and informed written consent was obtained from all participants.
Study Protocol
A panel of 13 different chemokines and cytokines induced by two different mycobacterial antigens after a short-term in vitro stimulation of blood cells was measured. Results obtained by in vitro stimulation of PBMC were analyzed in parallel with those obtained by stimulating diluted WB. The two antigens, HBHA and ESAT-6, were selected as they are secreted at different stages of the mycobacterial metabolism, in order to cover the whole spectrum of M. tuberculosis infection (17, 18). A training cohort was constituted to select the most promising cytokines or chemokines and their best combination to differentiate infected from non-infected subjects and then to identify patients with aTB among infected individuals. The accuracy of the selected combinations was further evaluated on samples from an independent validation cohort.
The Training and the Validation Cohorts
To ensure the reproducibility of the results and to limit the influence of a possible inclusion bias, two independent cohorts were evaluated. The training or discovery cohort comprised 61 individuals prospectively enrolled as being potentially M. tuberculosis infected (LTBI or aTB) or not (non-infected controls). For most of them (n=51), residual supernatants from stimulated PBMC or WB used in a previous study were used (16). Ten additional individuals (six controls, three LTBI, one aTB) were newly included. Samples from this cohort allowed us to identify the most suitable markers to first differentiate infected from non-infected subjects and then to differentiate aTB from LTBI subjects. These findings were then confirmed in a validation cohort that was independent from the training cohort and comprised 69 subjects included in a previous study (16). Residual supernatants from this cohort were used to confirm the diagnostic performance of the best combinations of markers identified on the training cohort (Table 1).
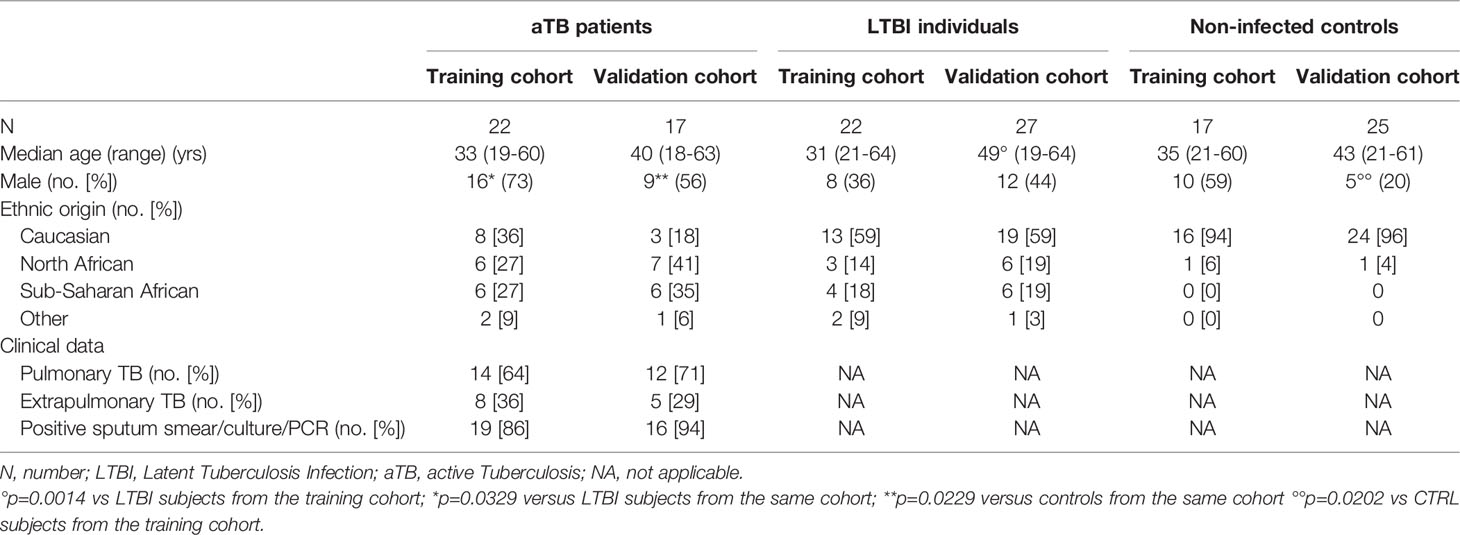
Table 1 Demographic and clinical data from the training and validation cohorts.
For both cohorts, the individuals were classified in three different groups, non-infected controls, LTBI subjects and patients with aTB, based on classical criteria as reported (19). Briefly, both non-infected controls and LTBI subjects were healthy with a negative or positive (induration size of 10 mm in case of risk factor and of 15 mm for the others) tuberculin skin test (TST) respectively. LTBI subjects also had a chest radiograph with no signs of aTB infection. Active TB diagnosis was based on microbiological proof for most patients, comprising both pulmonary and extrapulmonary aTB (Table 1). Based on these criteria, the training cohort comprised 17 non-infected controls, 22 LTBI subjects and 22 aTB patients, whereas the validation cohort comprised 25 non-infected controls, 27 LTBI subjects and 17 aTB patients. The main demographic data of the subjects included in this study for the two cohorts are reported in Table 1. Differences between the median ages and the sex ratios of the individuals included in the two cohorts were minor (Table 1). The proportion of subjects originating from endemic countries was lower for controls than for infected individuals (p ≤ 0.05) and was the most elevated among aTB patients (Table 1).
Induction of Chemokine and Cytokine Secretions
PBMC and diluted WB were in vitro stimulated as reported elsewhere (16, 19). Briefly, 1.106 PBMC, suspended in 500 μl culture medium (RPMI with 1 ng/ml IL-7), or 250 μl WB diluted 1:1 in IL-7-enriched-AIMV medium, were incubated during 24hrs at 37°C (5% CO2) with HBHA purified from Mycobacterium bovis BCG as described (20) (1 μg for PBMC and 2 μg for WB) or with recombinant ESAT-6 (2.5 μg) provided by Lionex (Diagnostics & Therapeutics GmbH, Braunschweig, Germany), before supernatant collection. Cells incubated in antigen-free medium and incubated with staphylococcal enterotoxin B (SEB, Sigma-Aldrich, Bornem, Belgium; 0.5 and 1 μg/ml for the PBMC and diluted WB stimulation, respectively) served as negative and positive controls, respectively.
Chemokine and Cytokine Concentration Measurements
The concentrations of 13 chemokines or cytokines were measured by multiparameter-based immunoassays (Milliplex human cytokine/chemokine kits-Merck, Belgium) according to the manufacturer’s instructions: granulocyte macrophage colony-stimulation factor (GM-CSF), Growth related oncogene (GRO), IFN-γ, interleukin (IL)-1β, IL-2, IL-6, IL-8, IL-10, IL-17A, IFN-γ-induced protein 10 (IP-10), Macrophage inflammatory protein (MIP)-1α, soluble CD40 ligand (sCD40L), and Tumor necrosis factor-alpha (TNF-α). Culture supernatants were diluted using dilution factors specific to each analyte in order to obtain concentrations within an interpretable range. Results were analysed with a Bio-Plex® MAGPIX™ Multiplex reader, Bio-Plex Manager™ MP Software and Bio-Plex Manager 6.1 Software (BIO-RAD laboratories, Nazareth Eke, Belgium). If detectable, the analyte concentrations obtained in the antigen-free conditions were subtracted from those obtained with antigen stimulation. To allow statistical analyses with continuous variables, the concentrations below the detection limit were allocated the arbitrary value of half of the threshold of detection, whilst results exceeding the assay’s upper limit of detection were attributed the concentration corresponding to this limit. The laboratory scientist performing the sample analysis was blinded to the clinical and other laboratory data.
Statistical Analysis
Differences in the concentrations of chemokines/cytokines between groups of subjects were analysed using the Mann-Whitney U test. The diagnostic abilities of individual parameters were first assessed by receiver operator characteristics (ROC) curve analysis and the areas under the curve (AUC) were calculated (GraphPad Prism version 7.03, GraphPad Software, La Jolla California USA, www.graphpad.com). The host marker selection was further evaluated by random forest analysis (random Forest package version 4.6-14) and the predictive abilities of combinations of markers were investigated by logistic regression using R (R-4.0.3, R Foundation for Statistical Computing, Vienna, Austria). Results were graphically represented with the linear predictor of the logistic regression. The tests were considered statistically significant when the p-value was < 0.05.
Results
Selection of PBMC-Produced Markers to Identify M. tuberculosis-Infected Subjects
We first investigated the ability of an individual marker, or a combination of markers, to differentiate M. tuberculosis-infected from non-infected individuals in the training cohort using ESAT-6 and HBHA for in vitro stimulation. Cytokine/chemokine concentrations were generally significantly higher for infected than non-infected subjects (Supplementary Table 1). The diagnostic accuracy of each individual marker was assessed by ROC curve analyses and most AUCs were higher than 0.7. We then performed random forest analyses including the 13 analytes secreted in response to ESAT-6 and HBHA to select the optimal combination to differentiate infected from non-infected subjects. The best discrimination was obtained by HBHA-induced IFN-γ, GM-CSF and IL-2, combined with ESAT-6-induced IFN-γ and IL-8 (Supplementary Figure 1A).
These markers were further evaluated in different combinations by logistic regression analysis for the training cohort. This analysis identified the combination of HBHA- and ESAT-6-induced IFN-γ as optimal to differentiate infected from non-infected subjects with 95% correct classification of the individuals (Figure 1A). Three non-infected subjects were misclassified. This combination was further applied on the validation cohort. In this case, 88% of the subjects were correctly classified with four controls and four infected subjects (two LTBI subjects and two patients with aTB) misclassified (Figures 1B, 2A).
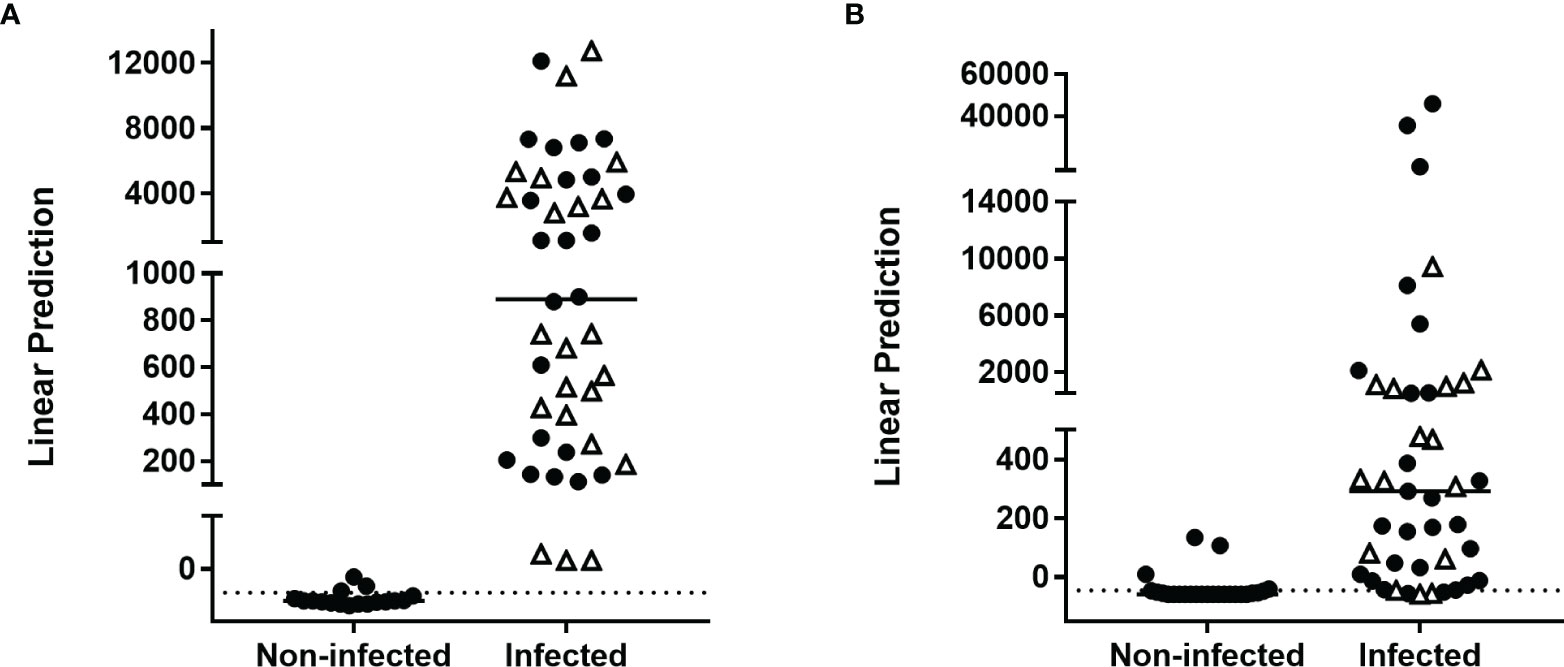
Figure 1 Combination of M. tuberculosis-specific immune markers allowing the distinction between M. tuberculosis-infected versus non-infected subjects in the PBMC assay. HBHA-IFN-γ and ESAT-6-IFN-γ were the markers selected by logistic regression analysis to be combined for the PBMC-based assay to discriminate M. tuberculosis-infected from non-infected subjects. Patients with aTB are indicated by open triangles. Results are represented with their linear predictor for the validation (A) and training (B) cohorts. The horizontal lines represent the medians and the dotted lines arbitrary cut-offs.
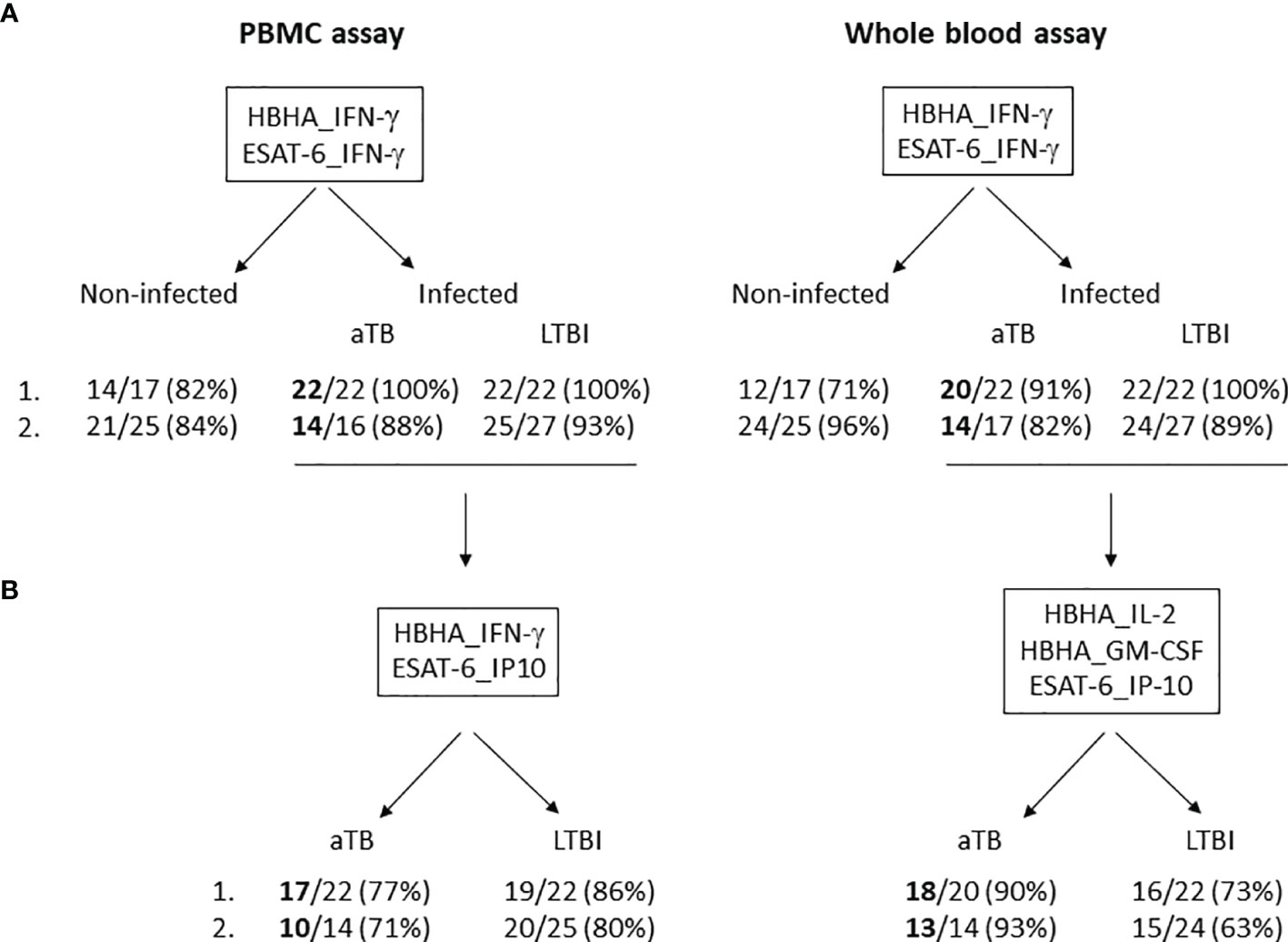
Figure 2 Two-step algorithm for the identification of aTB and LTBI among M. tuberculosis-infected subjects by using a combination of cytokines/chemokines induced by two stage-specific mycobacterial antigens in a PBMC- and WB-based assays. (A) M. tuberculosis-infected subjects, including aTB patients as well as LTBI subjects, were discriminated from non-infected subjects by using a combination of HBHA-IFN-γ and ESAT-6-IFN-γ in a PBMC- (left panel) and a WB-based assay (right panel) in a training (1.) and a validation cohort (2.). The numbers of well-classified subjects are indicated, as well as their percentages. (B) Patients with aTB were discriminated from LTBI subjects by using a combination of HBHA-IFN-γ and ESAT-6-IP-10 in a PBMC-based assay (left panel) or of HBHA-IL2, HBHA-GM-CSF and ESAT-6-IP-10 in a WB-based assay (right panel) in a training (1.) and a validation cohort (2.). Only the M. tuberculosis-infected subjects well-classified in (A) were taken into account for this discrimination between aTB and LTBI. The numbers of well-classified subjects are indicated, as well as their percentages.
Selection of PBMC-Produced Markers to Differentiate aTB From LTBI
A second random forest analysis including the same markers was performed to select the optimal combination to differentiate aTB from LTBI in the training cohort. ESAT-6-induced IP-10, IL-8, and HBHA-induced IP-10, IFN-γ, and TNF-α were selected (Supplementary Figure 1B) and combinations of these cytokines/chemokines were evaluated by logistic regression analysis. The most discriminant combination was ESAT-6-induced IP-10 combined with HBHA-induced IFN-γ, which provided a correct classification of 82% of the individuals: three LTBI subjects were classified as aTB, whereas five patients with aTB were classified as LTBI (Figure 3A). The clinical characteristics of the five aTB patients who were misclassified are reported in Table 2 (n°1 to n°5). The accuracy of this combination was further evaluated on the validation cohort. As in the validation cohort, two aTB patients and two LTBI subjects were misclassified by the first combination of markers (see Figure 1B), all LTBI and aTB individuals were included in this analysis. Seventy-four percent of the infected subjects were correctly classified with five LTBI subjects classified as aTB and six patients with aTB classified as LTBI (Figure 3B). The clinical characteristics of the misclassified aTB are reported in Table 3 (n°1 to 6). Two of them were already missed with the initial combination aiming to discard non-infected controls (n°1 and 2). The five misclassified LTBI subjects were considered at risk to reactivate the infection based on previously defined criteria (21) (Figure 3B, open circle).
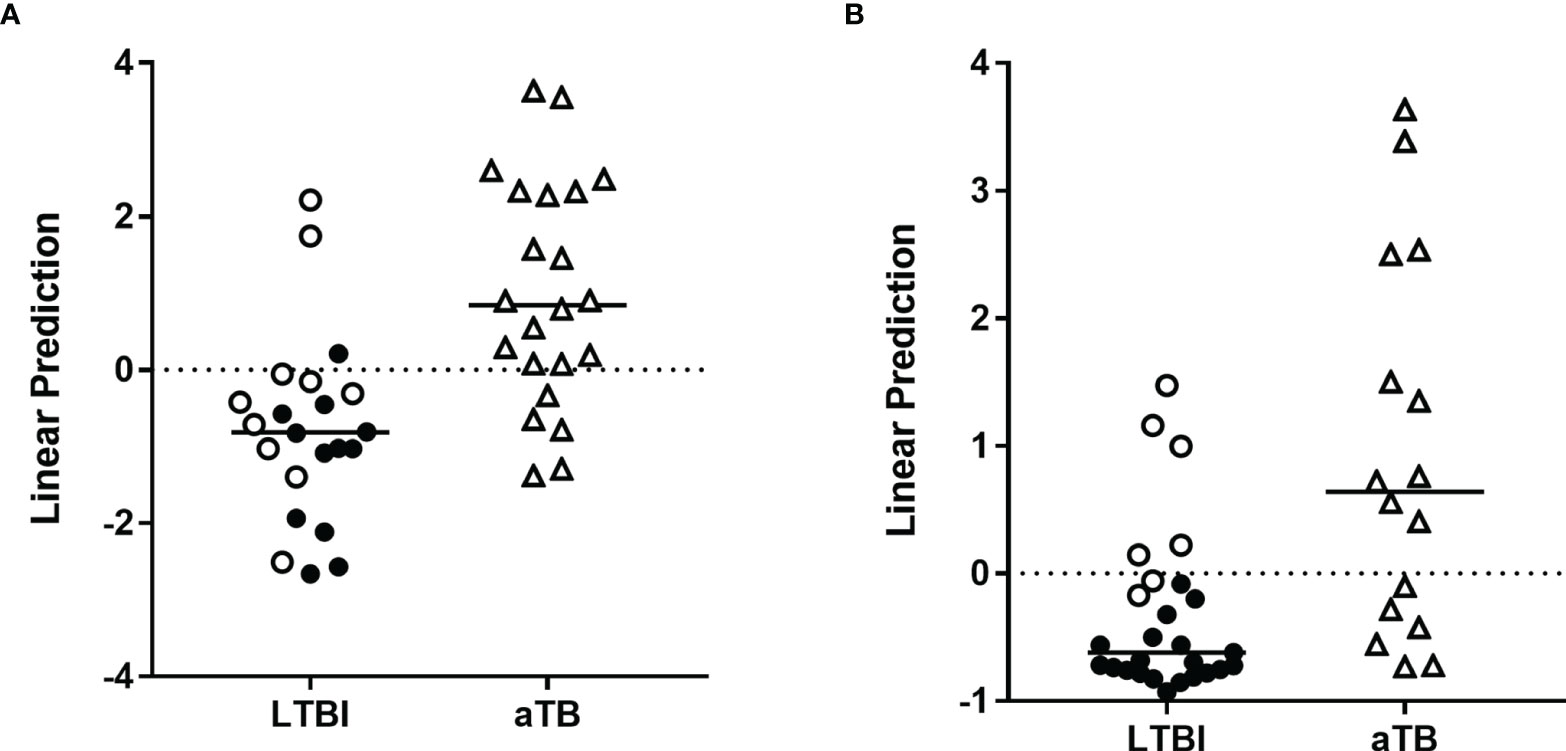
Figure 3 Combination of M. tuberculosis-specific immune markers allowing the distinction between LTBI and aTB in the PBMC assay. HBHA-IFN-γ and ESAT-6-IP-10 were the markers selected by logistic regression analysis to be combined for the PBMC-based assay to discriminate aTB from LTBI. Patients with aTB are indicated by open triangles and LTBI subjects at risk to reactivate the infection by open circles. Results are represented with their linear predictor for the validation (A) and training (B) cohorts. The horizontal lines represent the medians and the dotted lines arbitrary cut-offs.
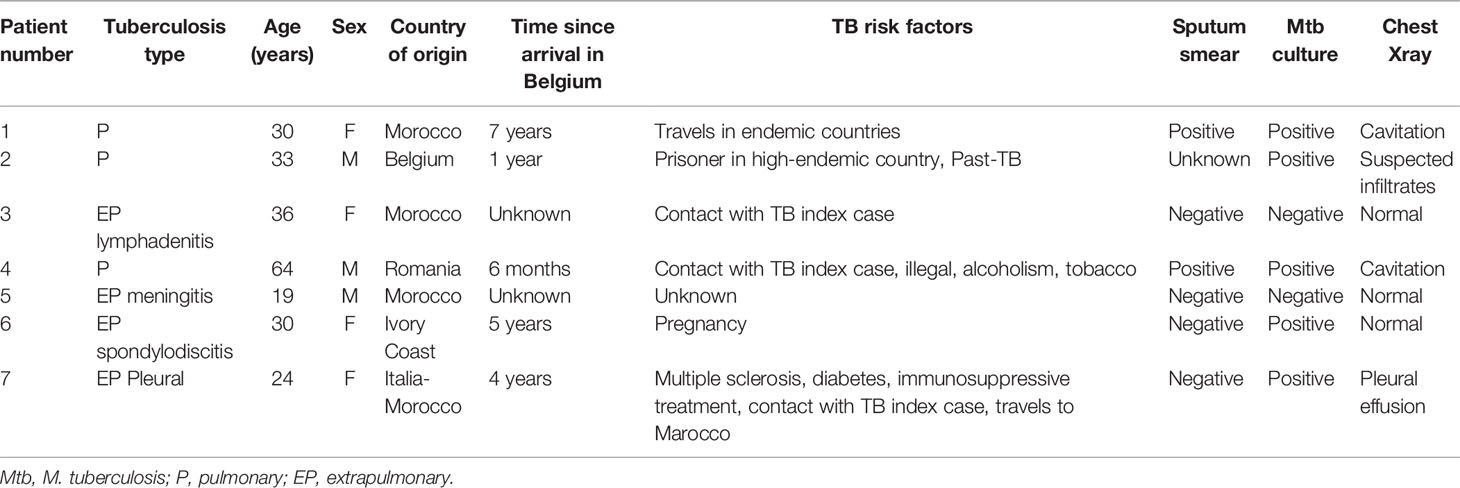
Table 2 Demographic and clinical data of the misclassified aTB patients from the training cohort.
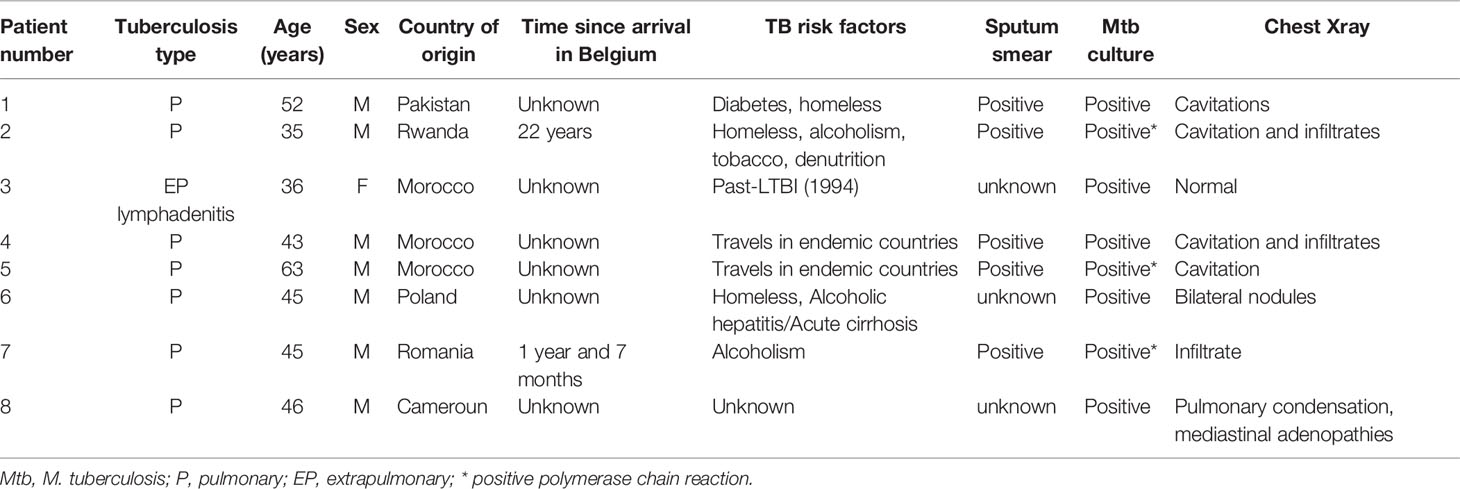
Table 3 Demographic and clinical data of the misclassified aTB patients from the validation cohort.
A good performance of the differential diagnosis between aTB and LTBI was thus possible in most cases by combining ESAT-6-induced IP-10 to HBHA-induced IFN-γ. However, this combination did not allow us to identify the two aTB patients who were initially misclassified as non-infected controls. The two-steps approach with a first identification of infected subjects, followed by a differential diagnosis between aTB and LTBI among infected individuals remains thus recommended as illustrated in Figure 2, panel A and B respectively. This two-steps approach resulted for the two cohorts in a correct identification of 36/38 aTB patients as infected (Figure 2A), with 27 of them as aTB patients (Figure 2B).
Selection of WB Markers to Identify M. tuberculosis-Infected Subjects
The same approach was applied for the WB assays. Similar to the PBMC, cytokine concentrations were generally significantly higher in infected than in non-infected individuals. ROC curves analyses differentiated infected from non-infected subjects with AUCs generally higher than 0.7 (Supplementary Table 2). Random forest analyses of the 13 analytes secreted in response to ESAT-6 and HBHA classified HBHA-induced IL-2, TNF-α and IFN-γ, together with ESAT-6-induced IL-8, TNF-α, IP-10 and IFN-γ as the optimal markers (Supplementary Figure 1C).
Logistic regression analysis on the results obtained for the training cohort identified three promising combinations of markers to be used to rule-out infection: HBHA- and ESAT-6-induced IFN-γ, HBHA- and ESAT-6-induced TNF-α, HBHA-induced IL-2 and ESAT-6-induced TNF-α. The first combination provided the best results on both cohorts. Eighty-nine percent and 90% of the subjects were correctly classified as infected or not in the training and validation cohorts, respectively (Figures 4A, B). Five controls and two aTB were misclassified in the training cohort as well as one control, three LTBI and three aTB in the validation cohort (Figures 2A, 3A, B). Three misclassified controls and two misclassified aTB patients with the WB assay were also misclassified in the PBMC assay. The clinical characteristics of the misclassified aTB patients are provided in Table 2 (n°5 and n°6) for the training cohort and in Table 3 (n°1, n°2 and n°7) for the validation cohort.
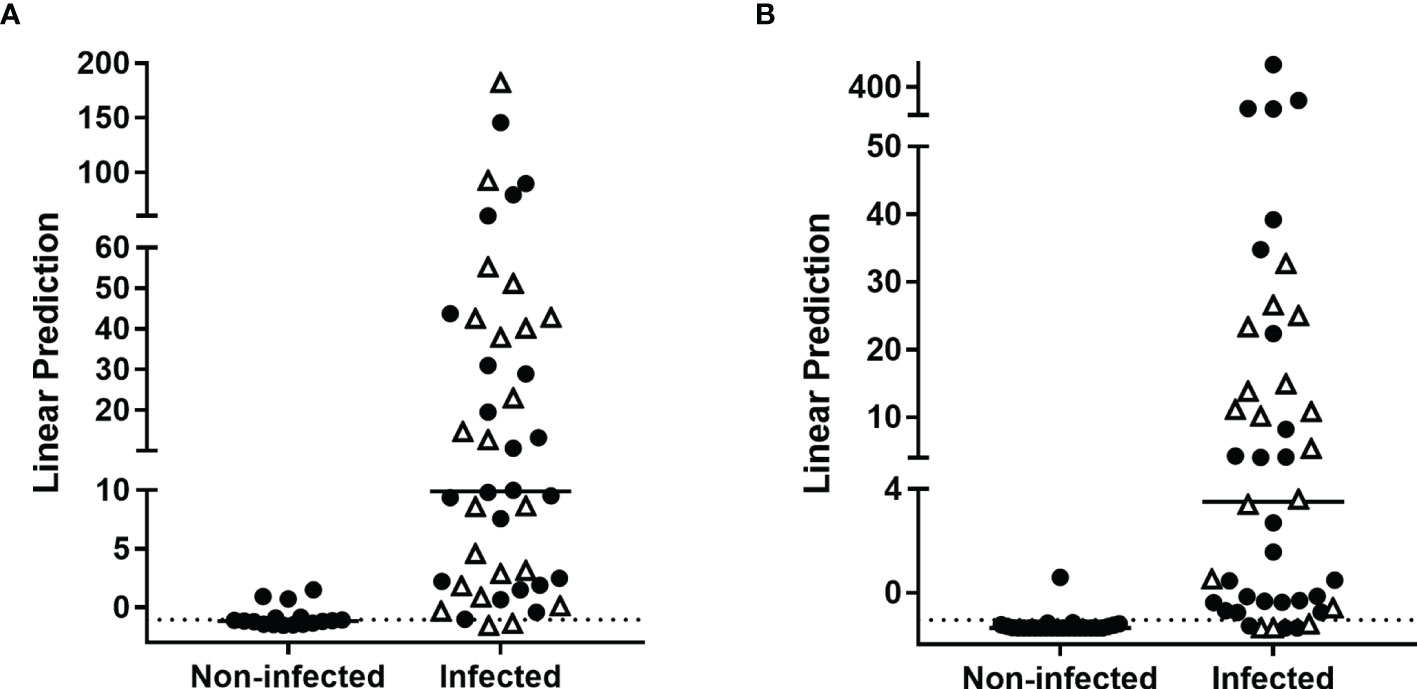
Figure 4 Combination of M. tuberculosis-specific immune markers allowing the distinction between M. tuberculosis-infected versus non-infected subjects in the WB assay. HBHA-IFN-γ and ESAT-6-IFN-γ were the markers selected by logistic regression analysis to be combined for the WB-based assay to discriminate M. tuberculosis-infected from non-infected subjects. Patients with aTB are indicated by open triangles. Results are represented with their linear predictor for the validation (A) and training (B) cohorts. The horizontal lines represent the medians and the dotted lines arbitrary cut-offs.
Selection of WB Markers to Differentiate aTB From LTBI
A second Random forest analysis was performed to identify the best markers to differentiate aTB from LTBI in the training cohort. All infected individuals were included in this analysis as a few patients with aTB were not identified as infected by the previous combination. ESAT-6-induced IP-10, and HBHA-induced IL-8, IL-2 and GM-CSF were identified as the best markers to differentiate aTB from LTBI (Supplementary Figure 1D). The optimal combination provided by further logistic regression was ESAT-6-induced IP-10 combined with HBHA-induced IL-2 and GM-CSF, which allowed us to correctly classify 82% of the subjects (Figure 5A). Among the misclassified subjects, only two were aTB patients (Table 2, n°4 and n°7), while the other six were LTBI subjects.
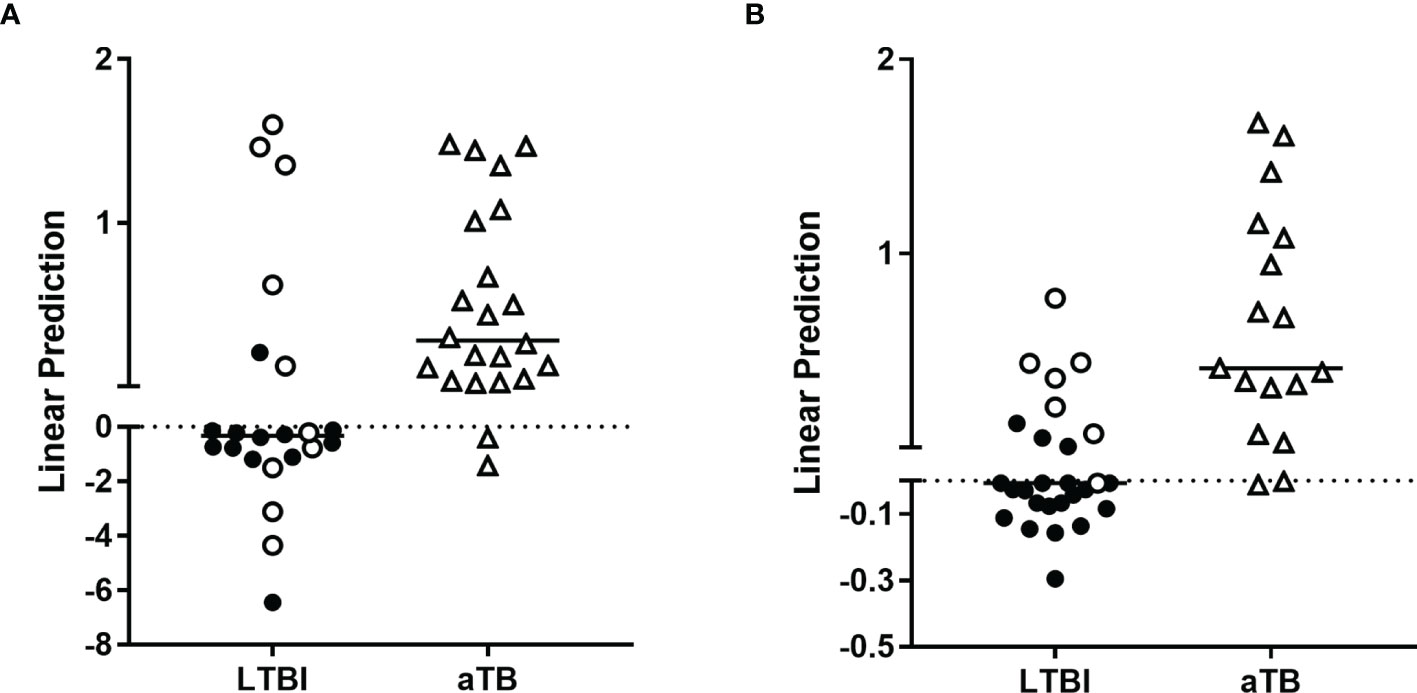
Figure 5 Combination of M. tuberculosis-specific immune markers allowing the distinction between LTBI and aTB in the WB assay. HBHA-IL2, HBHA-GM-CSF and ESAT-6-IP-10 were the host markers selected by logistic regression analysis to be combined for the WB-based assay to discriminate aTB from LTBI. Patients with aTB are indicated by open triangles and LTBI subjects at risk to reactivate the infection by open circles. Results are represented with their linear predictor for the validation (A) and training (B) cohorts. The horizontal lines represent the medians and the dotted lines arbitrary cut-offs.
In the validation cohort, this combination correctly classified 75% of the subjects (Figure 5B). As for the training cohort, only two aTB patients were misclassified (Table 3, n°1 and n°8), whereas the other nine misclassified subjects were LTBI subjects.
Good differential diagnosis between aTB and LTBI was thus possible in most cases by combining ESAT-6-induced IP-10 to HBHA-induced IL-2 and GM-CSF. However, this combination did not allow us to identify all the aTB patients who were initially misclassified as non-infected controls. Applying the two-steps approach to first identify infected subjects and then to identify aTB patients among infected individuals resulted globally for the two cohorts in a correct identification of 31/34 aTB patients.
This combination misclassified several LTBI subjects but most of them (11/15) were considered as being at risk to reactivate their infection.
Discussion
TB control could be significantly improved if simple and rapid triage or rule-out tests were available to first exclude non-infected subjects and then differentiate as much as possible aTB from LTBI. The development of triage tests designed for use by first-contact health care providers as a rule-out test of TB was reported by the World Health Organization as a high priority need for TB control (22). This strategy would limit the number of individuals requiring a confirmatory test. High sensitivity is needed for this approach to avoid missing patients with aTB. In contrast, the specificity of this triage test approach may be lower, as the patients initially selected by the triage test will benefit from more in-depth evaluation of their status. Blood-based immunological tests might be appropriate as triage tests. We previously reported that secretion of IFN-γ by PBMC or WB in response to in vitro stimulation with HBHA is a biomarker for LTBI contrasting with ESAT-6-induced IFN-γ secretion that is more characteristic of aTB (14, 15). Therefore, we suggested that combining IFN-γ secretion in response to HBHA and to ESAT-6 would help to differentiate LTBI from aTB and allows to stratify LTBI subjects in different groups associated with risks of reactivation of the infection (16, 21). In this study, we evaluated combinations of cytokines/chemokines released in response to these two antigens for improved identification of aTB patients, which could then be proposed as a triage test to select patients likely presenting aTB for further investigations to confirm the diagnosis. We propose a two-step approach consisting of first identifying infected subjects and then differentiating aTB from LTBI among infected individuals. Aiming to provide an easy test, we searched for optimal cytokine/chemokine combinations secreted by 24 hours-stimulated WB. However, this approach might not be sensitive enough for patients with lymphopenia or important inflammatory syndrome associated with high levels of plasma proteins that could inhibit cellular immune responses. It might also not be suitable for frozen material. We therefore also evaluated optimal cytokine/chemokine combinations secreted after 24 hours of in vitro-stimulated PBMC.
Among the 13 measured cytokines/chemokines secreted in response to HBHA and ESAT-6 and their various combinations to identify M. tuberculosis-infected patients, the best results were obtained both on WB and on PBMC by combining IFN-γ concentrations secreted in response to HBHA and to ESAT-6, as previously shown (15, 16). This approach allowed us to discard for further analysis most non-infected controls, 82%/71% in the training cohort and 84%/96% in the validation cohort, in the PBMC and WB assays, respectively. Misclassified controls were most often doubtful rather than being clearly positive. In addition, among the 10 misclassified controls in the PBMC and/or WB assay for both cohorts, five were health care workers potentially exposed to aTB patients, and four reported frequent travel to high TB endemic countries. Although these individuals were classified as non-infected, based on a negative TST result as recommended in Belgium (23), we cannot formally exclude that they developed immune responses to mycobacterial antigens as a consequence of exposure to M tuberculosis. They represented a minority of the enrolled controls that should benefit from further investigation (medical visit, chest radiograph, eventually followed by microbiological analysis of sputum samples) to exclude an ongoing M. tuberculosis infection. On the other hand, most infected individuals and especially most aTB patients were correctly identified and were selected for further investigations (100%/91% and 88%/82% in the training cohort in the validation cohort, in the PBMC and WB assays, respectively). Among the five misclassified aTB patients either in the PBMC or the WB assay in both cohorts, two had extra-pulmonary TB (one meningitis and one spondylodiscitis in a pregnant women) with obvious symptoms, while the other three had symptomatic pulmonary TB with severe denutrition and serious abnormalities on chest radiographs (Tables 2 and 3).
As a second step, we searched for the best combination of cytokines/chemokines secreted by the two stage-specific mycobacterial antigens to allow us to identify patients with aTB among infected individuals. Results were slightly different between the PBMC and WB assays. For PBMC stimulation, the best combination was HBHA-induced IFN-γ and ESAT-6-induced IP-10 that allowed us to correctly identify 77% and 71% of aTB patients in the training and validation cohorts, respectively. The interest of ESAT-6-induced IP-10 for diagnosis of M. tuberculosis infection was previously reported but with little added value compared to IFN-γ, except for patients with immune deficiencies (24). ESAT-6-induced IP-10 was not reported to provide differential diagnosis between aTB and LTBI. However, we show here that, when combined with HBHA-induced IFN-γ, it improves the differentiation between aTB and LTBI. This differentiation allowed us to identify ¾ of the patients with aTB, which is an improvement over previous studies. In addition, most misclassified aTB patients were shown to be infected in the first stage analysis and will therefore receive clinical attention.
Globally, eight LTBI subjects were misclassified as aTB. Seven of them were considered in a previous study as being at risk to reactivate their infection, based on their high ESAT-6-induced IFN-γ secretion (21). Latency is considered as a spectrum of different stages of activity of persistent mycobacteria, from totally quiescent to persistently multiplying (17, 18). This latter stage is the highest risk stage and therefore may not be possible to be differentiated from subclinical TB using immunological biomarkers. We may therefore hypothesize that these 8/49 misclassified LTBI subjects might have subclinical TB. Therefore, these individuals should be prioritized for more extensive evaluation for a possible aTB.
For WB stimulation, the best discrimination between aTB and LTBI was obtained by combining HBHA-induced IL-2 and GM-CSF with ESAT-6-induced IP-10. This allowed us to identify 90% and 93% of the aTB patients among infected individuals from the training and validation cohorts, respectively. The main advantages of the WB assay are the relatively small blood volume required (feasible on 1 mL WB) and easiness to perform. The good sensitivity should allow us to propose these tests as a triage test for aTB as the recommended sensitivity is to be at least 90% (22), and should help to limit the number of individuals who require confirmatory tests. One third of the LTBI subjects were misclassified and would require the confirmatory test. However, as for LTBI subjects misclassified with the PBMC assay, most of them were considered at risk to reactivate the infection and should therefore be prioritized for further evaluation of their status.
The sensitivities achieved with these combinations are similar to those reported in a few other studies aiming to define combinations of biomarkers that provide diagnostic test accuracy consistent with WHO specifications for a rule-out test for aTB. These studies that were recently summarized (25), are based on combinations of various serum markers, mostly cytokines/chemokines (26–28), sometimes combined with antibodies against a TB antigen to raise the specificity for TB (29). We chose in our study to measure cytokines/chemokines released in response to mycobacterial antigens to increase the specificity for TB. A few studies already addressed this question by measuring chemokines/cytokines induced by the peptides from the QuantiFERON, with different marker selections among the studies (13). Our results are difficult to compare to these studies, as we selected combinations of chemokines/cytokines induced by two different stage-specific mycobacterial antigens, ESAT-6 and HBHA, in order to cover a wide range of the M. tuberculosis metabolism. ESAT-6 is highly expressed during bacterial multiplication, while HBHA is a latency-associated antigen, whose gene is upregulated in hypoxic conditions and in cells harboring M. tuberculosis during latency (30–32). Not surprisingly, the selected combinations to differentiate aTB from LTBI were different between the PBMC and WB assays, since during acute inflammation plasma proteins may modify cellular immune responses.
Strengths of our study are that the biomarkers identified in the training cohort were validated in an independent validation cohort, both for the PBMC and the WB assays, and that these biomarkers are easy to measure in most laboratories. In addition, as blood and not sputum-based biomarkers, they are suitable to identify both pulmonary and extra-pulmonary TB who were both included in our cohorts. A limitation of this study results from the relatively low numbers of individuals in each cohort and from the heterogeneity of the cohorts that comprised both patients with pulmonary and extra-pulmonary TB. Moreover, we did not include in our cohorts TB-like diseases, which may perhaps represent more relevant negative controls for the evaluation of biomarkers to diagnose aTB. Inclusion of TB-like diseases was unfortunately not possible, because no screening for LTBI is performed in these patients in Belgium so that correct classification of these patients would have been difficult.
Based on the results of this pilot study performed in a low TB incidence country, we propose a two-steps algorithm to identify patients who are highly suspected to present aTB and should be further investigated (Figure 2). This algorithm warrants further evaluation on larger cohorts of subjects both in low and high TB endemic countries to confirm its robustness as triage test for aTB. Albeit not as simple as recommended to be a point of care test (22), it has the advantage of being relatively easy to perform on small blood volumes, to provide acceptable identification of aTB patients, and to be less expensive than systems biology approaches that have identified diagnostic signatures to discriminate aTB from LTBI (33, 34).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of ULB-Hôpital Erasme, Brussels, Belgium. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
VD designed the study, analyzed the data and wrote a first draft of the manuscript. PC performed the complete statistical analysis of the data. AP performed all the experimental work. MH, ND, and SA included patients, provided clinical data and reviewed the manuscript. JR did the initial statistical analysis. MS prepared ESAT-6 antigens. CL coordinated the preparation of antigens and critically reviewed the manuscript. FM designed the study, interpreted the data, and drafted the final manuscript. VC designed the study, analyzed and interpreted the data, collected clinical data, drafted figures and tables and critically reviewed the manuscript. All the authors contributed to this article and approved the submitted version.
Funding
This work was supported by the Fonds National de la Recherche Scientifique (FNRS—PDR T.0147.13), by the European Community within the Seventh Framework Program (FP7) NEWTBVAC (grant HEALTH-2009-2.3.2-2), and within the Horizon2020 program TBVAC2020 (grant agreement 643381), and by Innoviris Brussels.
Conflict of Interest
The author MS is employed by Lionex Diagnostics and Therapeutics, Braunschweig, Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all the volunteers who participated in this study and the clinicians involved in the recruitment of patients, particularly Dr C Martin, S Henrard, J Coussement, S Debulpaep, A. Drowart. We thank Dr C Wyndham-Thomas and E. Selis for their help in subject’s classification, A. Godefroid and S. Islane for their technical help, and M. Loyens and E. Petit for HBHA purification.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.842604/full#supplementary-material
References
1. World Health Organization. WHO Global Tuberculosis Report (2021). Available at: http://www.who.int/tb/publications/global_report/en/ (Accessed November 1, 2021).
2. Drain PK, Bajema KL, Dowdy D, Dheda K, Naidoo K, Schumacher SG. Incipient and Subclinical Tuberculosis: A Clinical Review of Early Stages and Progression of Infection. Clin Microbiol Rev (2018) 31(4):e00021–18. doi: 10.1128/CMR.00021-18
3. Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E. A Systematic Review of Rapid Diagnostic Tests for the Detection of Tuberculosis Infection. Health Technol Assess (2007) 11:1–196. doi: 10.3310/hta11030
4. De Visser V, Sotgiu G, Lange C, Aabye MG, Bakker M, Bartalesi F, et al. False-Negative Interferon-γ Release Assay Results in Active Tuberculosis: A TBNET Study. Eur Respir J (2015) 45:279–83. doi: 10.1183/09031936.00120214
5. Santos JA, Duarte R, Nunes C. Host Factors Associated to False Negative and Indeterminate Results in an Interferon-γ Release Assay in Patients With Active Tuberculosis. Pulmonology (2019) 26(6):353–62. doi: 10.1016/j.pulmoe.2019.11.001
6. Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB, et al. Interferon-γ Release Assays for the Diagnosis of Active Tuberculosis: A Systematic Review and Meta-Analysis. Eur Respir J (2011) 37:100 –111. doi: 10.1183/09031936.00114810
7. Lange C, Pai M, Drobniewsli F, Migliori GB. Interferon-γ Release Assays for the Diagnosis of Active Tuberculosis: Sensible or Silly? Eur Respir J (2009) 33:1250–3. doi: 10.1183/09031936.00019709
8. Shafeque A, Bigio J, Hogan CA, Pai M, Banaei N. Fourth-Generation QuantiFERON-TB Gold Plus: What Is the Evidence? J Clin Microbiol (2020) 58(9):e01950–19. doi: 10.1128/JCM.01950-19
9. Della Bella C, Spinicci M, Ainwaisri HFM, Bartalesi F, Tapinassi S, Mencarini J, et al. LIOFeron®TB/LTBI: A Novel and Reliable Test for LTBI and Tuberculosis. J Infect Dis (2020) 91:177–81. doi: 10.1016/j.ijid.2019.12.012
10. Molicotti P, Bua A, Cubeddu M, Cannas S, Delogu G, Zanetti S. Tuberculosis Patients Are Characterized by a Low-IFN-γ/High-TNF-α Response to Methylated HBHA Produced in M. Smegmatis. Diagn Microbiol Infect Dis (2011) 71(4):449–52. doi: 10.1016/j.diagmicrobio.2011.08.010
11. Loxton AG, Black GF, Stanley K, Walzl G. HBHA Induces IFN-γ+ IL-2+ IL-17+ T Cells During Multifunctional CD4+ T Cells During Latent But Not Active Tuberculosis Disease. Clin Vaccine Immunol (2012) 19(5):746–51. doi: 10.1128/CVI.00047-12
12. Dreesman A, Corbière V, Dirix V, Smits K, Debulpaep S, De Schutter I, et al. Age-Stratified T Cell Responses in Children Infected With Mycobacterium Tuberculosis. Front Immunol (2017) 8:1059. doi: 10.3389/fimmu.2017.01059
13. Qiu B, Liu Q, Li Z, Song H, Xu D, Ji Y, et al. Evaluation of Cytokines as a Biomarker to Distinguish Active Tuberculosis From Latent Tuberculosis Infection: A Diagnostic Meta-Analysis. BMJ Open (2020) 10:e039501. doi: 10.1136/bmjopen-2020-039501
14. Hougardy JM, Schepers K, Place S, Drowart A, Lechevin V, Verscheure V, et al. Heparin-Binding-Hemagglutinin-Induced IFN-γ Release as a New Diagnostic Tool for Latent Tuberculosis. PloS One (2007) 10:e926. doi: 10.1371/journal.pone.0000926
15. Mascart F, Locht C. Integrating Knowledge of Mycobacterium Tuberculosis Pathogenesis for the Design of Better Vaccines. Expert Rev Vaccines (2015) 14(12):1573–85. doi: 10.1586/14760584.2015.1102638
16. Dirix V, Dauby N, Hites M, Watelet E, Van Praet A, Godefroid A, et al. Optimal Detection of Latent M. Tuberculosis Infection by Combined HBHA and ESAT-6-Whole Blood Interferon-γ-Release Assays. J Clin Microbiol (2022) in press.
17. Lin PL, Flynn JL. The End of the Binary Era: Revisiting the Spectrum of Tuberculosis. J Immunol (2018) 201(9):2541–8. doi: 10.4049/jimmunol.1800993
18. Boom WH, Schaible UE, Achkar JM. The Knows and Unknows of Latent Mycobacterium Tuberculosis Infection. J Clin Invest (2021) 131(3):e136222. doi: 10.1172/JCI136222
19. Wyndham-Thomas C, Corbière V, Dirix V, Smits K, Domont F, Libin M, et al. Key Role of Effector Memory CD4+ T Lymphocytes in a Short-Incubation Heparin-Binding Hemagglutinin Gamma Interferon Release Assay for Detection of Latent Tuberculosis. Clin Vaccine Immunol (2014) 21(3):321–8. doi: 10.1128/CVI.00651-13
20. Corbière V, Segers J, Desmet R, Lecher S, Loyens M, Petit E, et al. Natural T Cell Epitope Containing Methyl Lysines on Mycobacterial Heparin-Binding Hemagglutinin. J Immunol (2020) 204:1715–23. doi: 10.4049/jimmunol.1901214
21. Corbière V, Pottier G, Bonkain F, Schepers K, Verscheure V, Lecher S, et al. Risk Stratification of Latent Tuberculosis Defined by Combined Interferon Gamma Release Assays. PloS One (2012) 7(8):e43285. doi: 10.1371/journal.pone.0043285
22. Denkinger CM, Kik SV, Cirillo DM, Casenghi M, Shinnick T, Weyer K, et al. Defining the Needs for Next Generation Assays for Tuberculosis. J Infect Dis (2015) 211(Suppl 2):S29–38. doi: 10.1093/infdis/jiu821
23. Fonds Des Affections Respiratoires. Tuberculose. Available at: http://www.fares.be (Accessed December 15th 2021).
24. Ruhwald M, Aabye MG, Ravn P. IP-10 Release Assays in the Diagnosis of Tuberculosis Infection: Current Status Ad Future Directions. Expert Rev Mol Diagn (2012) 12(2):175–87. doi: 10.1586/erm.11.97
25. Escalante P, Theel ES. Progress Towards Developing a Rapid Triage/Referral Test for Tuberculosis. Clin Chem (2020) 66(8):995–7. doi: 10.1093/clinchem/hvaa1
26. Chegou NN, Sutherland JS, Malherbe S, Crampin AC, Corstjens PLAM, Geluk A, et al. Diagnostic Performance of a Seven-Marker Serum Protein Biosignature for the Diagnosis of Active TB Disease in African Primary Healthcare Clinic Attendees With Signs and Symptoms Suggestive of TB. Thorax (2016) 71(9):785–94. doi: 10.1136/thoraxjnl-2015-20799925
27. De Groote MA, Sterling DG, Hraha T, Russell TM, Green LS, Wall K, et al. Discovery and Validation of Six-Marker Serum Protein Signature for the Diagnosis of Active Pulmonary Tuberculosis. J Clin Microbiol (2017) 55(10):3057–71. doi: 10.1128/JCM.00467-17
28. Delemarre EM, van Hoorn L, Bossink AWJ, Drylewicz J, Joosten SA, Ottenhoff THM, et al. Serum Biomarker Profile Including CCL1, CXCL10, VEGF, and Adenosine Deaminase Activity Distinguishes Active From Remotely Acquired Latent Tuberculosis. Front Immunol (2021) 12:725447. doi: 10.3389/fimmu.2021.725447
29. Ahmad R, Xie L, Pyle M, Suarez MF, Broger T, Steinberg D, et al. A Rapid Triage Test for Active Pulmonary Tuberculosis in Adult Patients With Persistent Cough. Sci Transl Med (2019) 11(515):eaaw8287. doi: 10.1126/scitranslmed.aaw8287
30. Mack U, Migliori GB, Sester M, Rieder HL, Ehlers S, Goletti D, et al. LTBI: Latent Tuberculosis Infection or Lasting Immune Responses to M. Tuberculosis? A TBNET Consensus Statement. Eur Respir J (2009) 33:956–73. doi: 10.1183/09031936.00120908
31. Iona E, Pardini M, Mustazzolu A, Piccaro G, Nisini R, Fattorini L, et al. Mycobacterium Tuberculosis Gene Expression at Different Stages of Hypoxia-Induced Dormancy and Upon Resuscitation. J Microbiol (2016) 54:565–72. doi: 10.1007/s12275-016-6150-4
32. Delogu G, Sanguinetti M, Posteraro B, Rocca S, Zanetti S, Fadda G. The hbhA Gene of Mycobacterium Tuberculosis Is Specifically Upregulated in the Lungs But Not in the Spleens of Aerogenically Infected Mice. Infect Immun (2006) 74:3006–11. doi: 10.1128/IAI.74.5.3006-3011.2006
33. Bloom CI, Graham CM, Berry MP, Rozakeas F, Redford PS, Wang Y, et al. Transcriptional Blood Signatures Distinguish Pulmonary Tuberculosis, Pulmonary Sarcoidosis, Pneumonias and Lung Cancers. PloS One (2013) 8(8):e70630. doi: 10.1371/journal.pone.0070630
Keywords: active tuberculosis, ESAT-6, HBHA, IFN-γ, IL-2, GM-CSF, IP-10
Citation: Dirix V, Collart P, Van Praet A, Hites M, Dauby N, Allard S, Racapé J, Singh M, Locht C, Mascart F and Corbière V (2022) Immuno-Diagnosis of Active Tuberculosis by a Combination of Cytokines/Chemokines Induced by Two Stage-Specific Mycobacterial Antigens: A Pilot Study in a Low TB Incidence Country. Front. Immunol. 13:842604. doi: 10.3389/fimmu.2022.842604
Received: 23 December 2021; Accepted: 11 February 2022;
Published: 10 March 2022.
Edited by:
Harriet Mayanja-Kizza, Makerere University, UgandaReviewed by:
Juraj Ivanyi, King’s College London, United KingdomAntónio Gil Castro, University of Minho, Portugal
Copyright © 2022 Dirix, Collart, Van Praet, Hites, Dauby, Allard, Racapé, Singh, Locht, Mascart and Corbière. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Françoise Mascart, ZnJhbmNvaXNlLm1hc2NhcnRAZXJhc21lLnVsYi5hYy5iZQ==