 Jéssica Castillo-Villalba1†
Jéssica Castillo-Villalba1† Sara Gil-Perotín1*†
Sara Gil-Perotín1*† Raquel Gasque-Rubio1Laura Cubas-Nuñez1Sara Carratalà-Boscà1
Raquel Gasque-Rubio1Laura Cubas-Nuñez1Sara Carratalà-Boscà1 Carmen Alcalá1
Carmen Alcalá1 Carlos Quintanilla-Bordás1
Carlos Quintanilla-Bordás1 Francisco Pérez-Miralles1Cristina Ferrer1Antonio Cañada Martínez2Jordi Tortosa3Luís Solís-Tarazona4
Francisco Pérez-Miralles1Cristina Ferrer1Antonio Cañada Martínez2Jordi Tortosa3Luís Solís-Tarazona4 Luisa Campos5
Luisa Campos5 Alberto Leivas5Begoña Laíz Marro3
Alberto Leivas5Begoña Laíz Marro3 Bonaventura Casanova1
Bonaventura Casanova1- 1Neuroimmunology Unit, Neurology Department and Health Research Institute, Hospital Universitario y Politécnico La Fe, Valencia, Spain
- 2Data Science, Biostatistics and Bioinformatics, Health Research Institute, Hospital Universitario y Politécnico La Fe, Valencia, Spain
- 3Clinical Laboratory, Hospital Universitario y Politécnico La Fe, Valencia, Spain
- 4Neurology Department, Hospital Dr. Peset, Valencia, Spain
- 5Scientific Department, The Binding Site Iberia, Barcelona, Spain
Cerebrospinal kappa free light chain (KFLC)-index is a marker of intrathecal immunoglobulin synthesis that aids in the diagnosis of multiple sclerosis (MS). However, little evidence exists on its prognostic role. Our aim is to analyze the relationship between KFLC-index and other MS biomarkers and to explore its prognostic role. This is a monocentric observational study in a cohort of 52 people with relapsing MS (pwRMS) performed on prospectively acquired clinical data and with retrospective evaluation of biomarkers. We measured KFLC-index, immunoglobulin intrathecal synthesis, cerebrospinal fluid (CSF) chitinase 3-like 1 (CHI3L1), and neurofilament light protein (NFL) and reviewed MRI to detect leptomeningeal contrast enhancement (LMCE). We compared time to Expanded Disability Status Scale (EDSS) 3 and to initiation of high-efficacy disease-modifying therapies (heDMTs) by multivariate Cox regression analysis. Median KFLC-index correlated with IgG/IgM indexes (p < 0.0001/p < 0.05) and IgG-oligoclonal bands (OCGBs) (p < 0.001). Patients with IgM-oligoclonal bands (OCMBs) had a higher KFLC-index (p = 0.049). KFLC-index was higher in patients with LMCE (p = 0.008) and correlated with CHI3L1 (p = 0.007), but disease activity had no effect on its value. Bivariate and multivariate analyses confirmed KFLC-index > 58 as an independent risk factor for reaching an EDSS of 3 (hazard ratio (HR) = 12.4; 95% CI = 1.1–147; p = 0.047) and for the need of treatment with heDMTs (HR = 3.0; 95% CI = 1.2–7.1; p = 0.0013). To conclude, our data suggest a potential prognostic role of the KFLC-index during the MS course.
Background
Multiple sclerosis (MS) has long been regarded as a T cell-mediated disease. However, increasing evidence supports the pathogenic role of B cells, through both the production of antibodies and the release of proinflammatory factors in the cerebrospinal fluid (CSF) (1). Antigen-directed affinity maturation and terminal differentiation of B cells contributing to immunoglobulin synthesis occur within perivascular infiltrates and meningeal ectopic lymphoid-like follicles and have been related to gray matter pathology and progressive disease (2–4).
Due to a predictive role in clinically isolated syndrome (CIS) conversion to MS, the examination of cerebrospinal IgG-oligoclonal bands (OCGBs) has been reintroduced in the latest MS diagnostic criteria (5). This paradigm change has focused attention on other biomarkers related to immunoglobulin syntheses, such as kappa free light chains (KFLCs) and IgM-oligoclonal bands (OCMBs). KFLC, a secreted remnant produced by plasma cells, whose values can be corrected for the blood–brain barrier permeability by use of the KFLC-index, has been described as a reliable marker of intrathecal IgG synthesis in MS (6–9), but there are scarce prognostic data on excess of KFLC in the long term. Alternatively, interest in OCMBs, present in 48% of people with MS (pwMS), has been recently renewed after increased research supporting a correlation with unfavorable disease courses in MS (10–13). Considering this background, the present single-center observational study in relapsing MS (RMS) patients aims to assess the potential relationship between KFLC-index and other neuroinflammatory biomarkers, such as OCMBs, and its value as a complementary tool to OCGBs and as a risk factor for neurological disability and treatment failure.
Materials and Methods
Participants
This is a single-center observational study in a cohort of 52 pwMS with a first demyelinating episode and definite diagnosis of RMS according to the 2017 McDonald criteria (5). A cohort of consecutive and unselected patients was recruited in the period comprised between 2010 and 2019 based on the availability of CSF at the time of disease onset. Clinical data were acquired prospectively, and biomarker and radiological data were analyzed retrospectively. Disability was estimated according to the Expanded Disability Status Scale (EDSS) at the time of lumbar puncture (LP) and in three-monthly visits during follow-up. The clinical study was approved by the Institutional Ethics Committee (reference number PI17/01544).
Definitions
A clinical attack or demyelinating event (relapse) was defined as an acute worsening of neurologic function lasting more than 24 h, not explained by fever or physical stress, and followed by a variable degree of recovery. MRI assessment of acute demyelination was required. CSF samples were contemporary to disease onset.
RMS patients were treated with disease-modifying therapies (DMTs) according to routine clinical practice. In general, a first-line DMT was offered unless any of the following circumstances occurred: i) two clinical attacks in a year, ii) a clinical attack and/or a new gadolinium-enhanced lesion (GEL), or iii) a disabling clinical attack with residual EDSS of at least 2 points in the pyramidal system. In these cases, and in those with treatment failure, high-efficacy DMTs (heDMTs) were preferred. We considered as heDMTs cladribine, fingolimod, natalizumab, ocrelizumab, rituximab, alemtuzumab, and hematopoietic stem cell transplantation (aHSCT). Treatment failure was considered in case of clinical relapse followed by MRI demonstrating GEL within 3 months from the flare.
Laboratory Analysis in the Cerebrospinal Fluid
Paired CSF and serum samples were collected simultaneously and stored at −80°C. Serum and CSF were tested to rule out infections, monoclonal serum OCB, or other inflammatory systemic diseases. IgG, IgM, and albumin were measured in CSF and serum with immuno-nephelometry, and Link index was calculated to obtain IgG and IgM indexes to correct the influence of blood–barrier permeability in the immunoglobulin concentration as per the following formula:
Ig index: (CSF Ig/serum Ig)/(CSF albumin/Serum albumin)
Detection of oligoclonal IgG and IgM bands was performed by isoelectric focusing and immunoblotting, as previously described (14). KFLC was measured by turbidimetry using the Freelite Mx immunoassay (The Binding Site, Birmingham, UK) on the automated analyzer Optilite (The Binding Site). Serum samples were diluted 1/10, and CSF samples were analyzed undiluted as recommended by the manufacturer. The lower limit of quantification (LOQ) for KFLC in the CSF was 0.03 mg/L. KFLC-index was calculated with reference to albumin CSF and serum albumin according to the following formula:
KFLC-index: (CSF KFLC/serum KFLC)/(CSF albumin/Serum albumin)
CSF NFL and chitinase 3-like 1 (CHI3L1) levels were assessed by ELISA using commercially available kits according to the manufacturer’s instructions (Uman Diagnostics AB, Umea, Sweden; and Quantikine ELISA kit, R&D Systems, Minneapolis, MN, USA, respectively). Samples were run in duplicate in a blind manner. The intra-assay variability was 5.8% for NFL and 5.13% for CHI3L1. The mean inter-assay coefficients of variation were 4.5% and 5.2%, respectively.
MRI Detection of Post-Gadolinium Leptomeningeal Enhancement
After CSF collection, 3-Tesla MRI acquisitions in all patients were analyzed. Sequences included pre-contrast T2-fluid-attenuated inversion recovery (T2-FLAIR) and post-contrast three-dimensional (3D) T2-FLAIR scans (1 × 1 mm) performed at least 10 min after IV injection of a single dose of gadolinium (Gd) (0.1 mmol/kg) and 3D T1 sequences (General Electric, Signa HDx, Boston, MA, USA) according to published scan acquisition parameters (15). Pre-contrast T2-FLAIR scans were available for all patients. Leptomeningeal contrast enhancement (LMCE) was defined as signal intensity within the subarachnoid space that was substantially greater than that of brain parenchyma on post-contrast 3D FLAIR images, excluding high-signal regions adjacent to dural venous sinuses, basal meninges, and large subarachnoid veins (15). For this manuscript, two trained raters (SG-P and SC-B) were involved in analyzing the images, and inter-rater variability was <1%.
Statistical Analysis
Continuous variables were reported as median with interquartile range (IQR) and categorical variables as absolute frequencies and percentages. Data did not distribute normally and were analyzed with non-parametric tests. Groups were compared with the Wilcoxon rank sum and Kruskal–Wallis tests, and correlations were performed with Spearman’s test. All associations were adjusted for sex, age, and disease duration. Bonferroni post-hoc adjustment was performed in the case of multiple comparisons. A two-sided p-value of less than 0.05 was considered to indicate statistically significant differences. Time to disability endpoints (EDSS score of 3) and initiation of heDMTs were compared using the Kaplan–Meier curves and a log-rank test. Patients who did not reach EDSS scores of >3 or who maintained first-line DMTs during follow-up were considered censored at the time of the last clinical assessment. We performed Cox proportional hazard regressions to estimate the hazard ratios (HRs) along with 95% CI as measures of association between test results and endpoints. Adjustments were made for potential confounding factors (sex, age, and EDSS at LP). Statistical analyses were performed using R studio 2021.09 (https://www.R-project.org/).
Results
Participant Characteristics
Fifty-two people with RMS (pwRMS) were enrolled in this study. Forty-two patients (81%) were women, and the median age at onset was 35 (25–45) years. Patients were followed up for a median of 58 (45–75) months. The median baseline disability score (EDSS) was 2.0 (1–2). Forty-two patients (81%) were experiencing clinical relapse, and 26 (50%) had GEL in the MRI at the time of CSF collection. Two patients were receiving first-line DMTs at the time of LP, one patient had received corticosteroids, and one had been treated with cyclophosphamide in the previous 2 months. Demographic and clinical data of all patients are summarized in Table 1.

Table 1 Demographic, clinical, and MRI data of pwMS in the study.
Kappa Free Light Chain-Index Association With Diagnostic and Prognostic Multiple Sclerosis Biomarkers
Median KFLC-index was 47.8 (14.3–130) and was significantly higher in pwMS with OCGBs as compared to those without (4.63 (0.03–11.76) and 73.14 (35.72–137.5); p < 0.0001, respectively). Likewise, the correlation with IgG index was strong (ρ = 0.872; p < 0.0001) (Figures 1A, B). In the receiver operating characteristic (ROC) analysis, a KFLC-index cutoff value of 12.8 predicted the presence of OCGBs with a sensitivity of 93% and a specificity of 80%, while a cutoff value of 17.2 was more specific (sensitivity 83% and specificity 90%). The area under the curve (AUC) was 0.952. A contingency analysis for both cutoff values showed a positive predictive value (PPV) of 94.7%/82% and a negative predictive value (NPV) of 80%/90%.
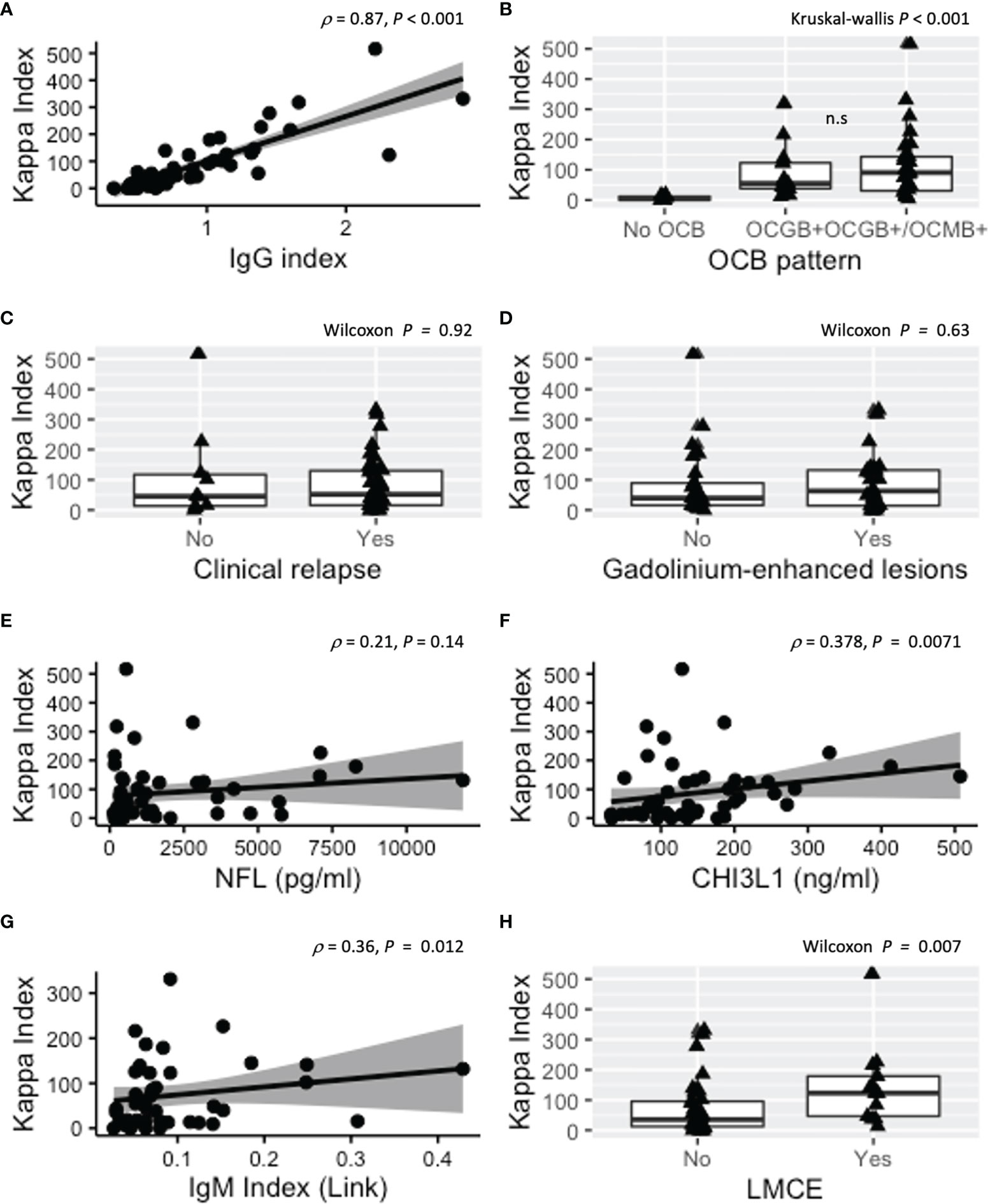
Figure 1 Association of KFLC-index with other diagnostic and prognostic MS biomarkers. (A) Correlation between KFLC-index and IgG index. (B) KFLC-index was significantly increased in the presence of OCGBs with respect to patients without intrathecal immunoglobulin synthesis. KFLC-index tended to be higher in the presence of both OCGBs and OCMBs but did not correlate with concurrence of clinical relapse (C) or presence of GEL (D). (E) KFLC-index did not correlate with CSF NFL but did weakly with CSF CHI3L1 and IgM index [(F, G), respectively]. (H) Patients with LMCE had higher median values of KFLC-index. Kappa index, kappa free light chain (KFLC) index; OCB, oligoclonal band; GEL, gadolinium-enhanced lesions; NFL, neurofilament light chain protein; CSF, cerebrospinal fluid; CHI3L1, chitinase 3-like 1; LMCE, leptomeningeal contrast enhancement; MS, multiple sclerosis. n.s., not significant.
During active disease, defined as relapse or presence of GEL in the MRI simultaneous to CSF collection, KFLC-index in our cohort was not significantly different from that in pwMS on remission (p = 0.92 and p = 0.63, respectively) (Figures 1C, D). Likewise, KFLC-index was not associated with sex (p = 0.76), age (p = 0.93), EDSS (p = 0.11), or DMTs at time of CSF collection (Kruskal–Wallis p = 0.59 with no differences between non-treated and treated with first-line DMTs or second-line DMTs). When we analyzed other cerebrospinal biomarkers such as neurofilament light protein (NFL) and chitinase 3-like 1 (CHI3L1), we only found a weak correlation between KFLC-index and CHI3L1 (ρ = 0.378; p = 0.007) (Figures 1E, F).
Twenty-nine patients (55.7%) had simultaneous OCGBs and OCMBs. KFLC-index was higher in pwMS with OCMBs (85.3 (17.9–141.4)) than in those without (37.8 (12.3–65.3); p = 0.049). The correlation between KFLC and IgM index was significant but less robust than with OCGBs (ρ = 0.36; p < 0.012) (Figure 1G). We sought for the discriminative potential of KFLC-index to detect both double-positive (OCGBs and OCMBs) patients, and we observed that pwMS with unique OCGB pattern had a lower median KFLC-index (54.9 (38.4–122.8)) as compared to those with OCGBs and OCMBs (90.6 (30.7–143.3)), but this difference did not reach statistical significance (p = 0.635) (Figure 1B).
Finally, as ectopic leptomeningeal follicles (eLFs) are thought to be involved in the intrathecal production of immunoglobulins, we studied the potential association between KFLC-index and LMCE, the radiological counterpart of eLFs. The presence of LMCE was observed in 13 patients (25%). Patients with LMCE had higher KFLC-index than patients without LMCE (123 (46.8–178.8) and (35.0 (12.4–96), respectively) (p = 0.008) (Figure 1H). There was a patient with LMCE and an outlier KFLC-index value of 516. After withdrawal from the analysis, the KFLC-index association with LMCE was still significant (p = 0.019).
Kappa Free Light Chain-Index as Prognostic Factor of Disability and Initiation of High-Efficacy Disease-Modifying Therapy
To explore time to disability endpoint (EDSS score of 3) and time to initiation of heDMTs, patients were stratified according to the most discriminative KFLC-index cutoff value. Seven patients (13.4%) had reached an EDSS score of 3 at the last data update. In the bivariate analysis, KFLC > 58 was a risk factor to reach EDSS of 3 (log-rank p = 0.036) (Figure 2A). Cox multivariate regression analysis (adjusted for sex and baseline age and EDSS) confirmed that KFLC-index > 58 was an independent risk factor for this outcome (HR) = 12.4, 95% CI = 1.1–147 and p = 0.047 (Figure 2B).
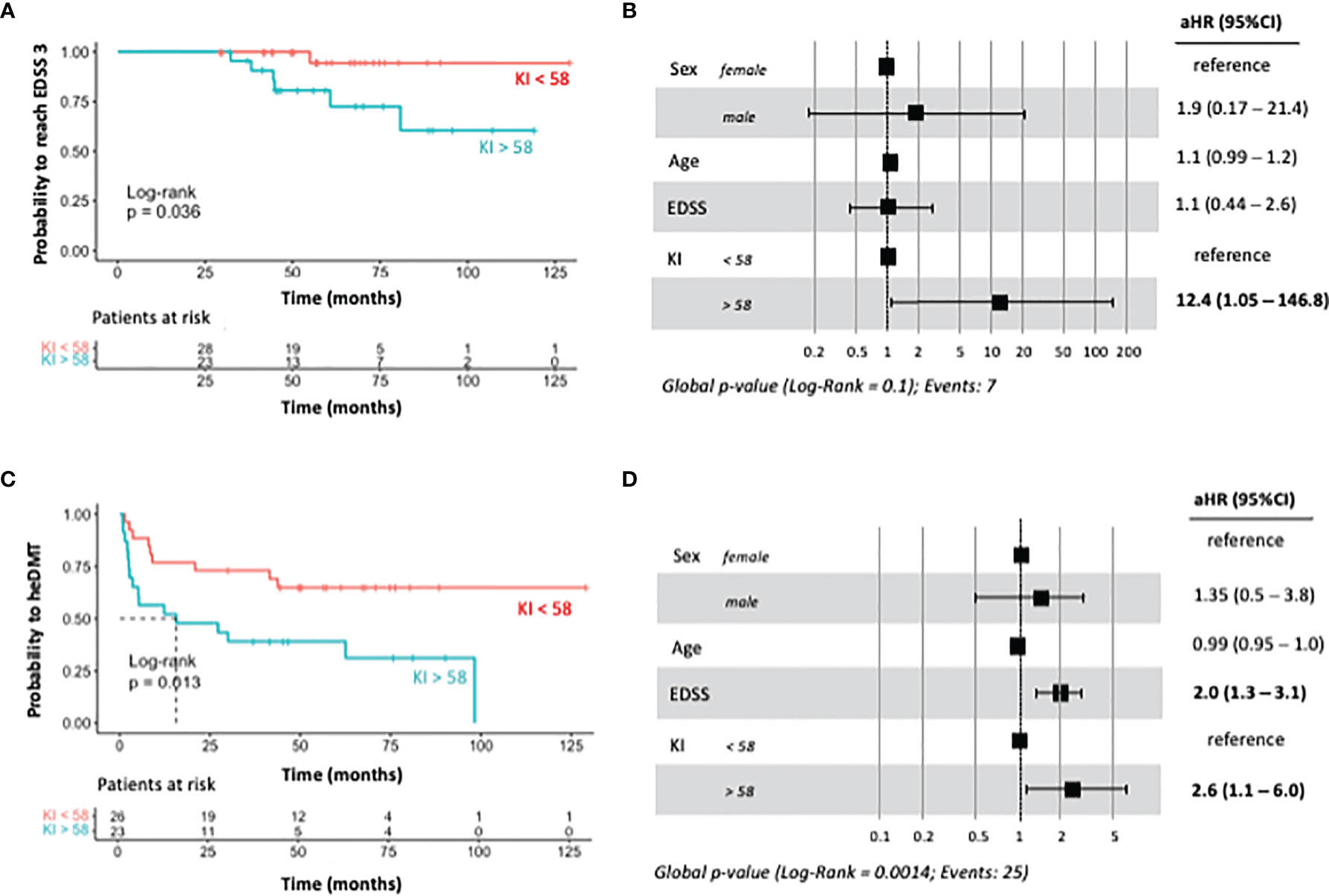
Figure 2 Bivariate and multivariate regression models for predicting the risk of reaching EDSS score of 3 and of treatment escalation. (A) Kaplan–Meier survival analysis showing the probability for reaching an EDSS of 3 stratified by KFLC-index value of 58. (B) Forest plot of multivariate analysis for the same disability endpoint adjusted for sex, baseline age, and baseline EDSS. (C) Kaplan–Meier survival analysis showing the probability for treatment escalation to heDMT stratified by KFLC-index value of 58. (D) Forest plot of multivariate analysis for the same disability endpoint adjusted for sex, baseline age, and baseline EDSS. KFLC-index, kappa free light chain index; EDSS, expanded disability severity score; heDMT, high-efficacy disease-modifying therapy.
The need for initiation of heDMTs during follow-up occurred in 25 patients (48%). The Kaplan–Meier survival analysis showed that pwMS with KFLC > 58 required heDMTs with a median time of 18 months (log-rank p = 0.013) and was an independent risk factor in the multivariate analysis (HR = 2.6; 95% CI = 1.1–6.0 p = 0.0014) (Figures 2C, D). Baseline EDSS was also an independent risk factor for treatment with heDMTs (HR 2.0, 95% CI 1.3– 3.1; p = 0.01).
Discussion
KFLC in the CSF is a product of immunoglobulin intrathecal synthesis and is measured with a quantitative and automated method, not dependent on technical interpretation. Here we showed that KFLCCSF/serum index is a feasible alternative to OCGBs and/or IgG index for MS diagnosis that is not significantly affected by concurrent radiological or clinical disease activity. Regarding long-term prognosis, KFLC-index correlated with CHI3L1, and its excess was related to the presence of OCMBs and LMCE, biomarkers associated with worse outcomes, progressive disease, and gray matter pathology. Additionally, KFLC-index above 58 was an independent risk factor for reaching an EDSS score of 3 and predicted the need for high-efficacy treatments during follow-up.
KFLC-index has been shown to be a sensitive marker of intrathecal immunoglobulin synthesis comparable to OCGB detection, the current “gold standard” (16). However, non-consensus has been reached about the most informative threshold value. Supplementary Table 1 summarizes the distinct studies addressing KFLC cutoff values. In our study, all patients fulfilled the criteria for RMS; thus, we performed ROC analysis in comparison with OCGBs, achieving a good sensitivity/specificity relation with a KFLC-index cutoff of 12.8. The specificity increased with a higher cutoff value, as may also be inferred by other groups’ reported results on CIS/MS patients. The discrepancies between different thresholds could be due to variability between the clinical cohorts included in the evaluation and/or different measurement techniques, although the best-performing cutoff value might depend on the specific diagnostic context.
In our cohort, KFLC-index was not related to inflammatory relapse or GEL, suggesting that there might not be a relationship between KFLC production and acute inflammatory activity in MS. These findings are in agreement with previous studies that showed no correlation between KFLC-index in pwRMS patients with GEL on MRI at the time of sampling (17, 18). However, another work described a significantly higher KFLC-index in patients presenting with myelitis or with >9 T2 lesions in the MRI (19).
The long-term prognostic role of KFLC is as yet widely unexplored. We showed that KFLC median values increased in the presence of OCMBs and correlated with the IgM index. KFLC might have the potential to detect IgM-producing cell clones commonly found in early inflammatory responses (20), similarly to what occurs during IgG synthesis, as has been suggested by Süße et al. (21). IgM intrathecal synthesis is associated with a shorter time between relapses and predicts earlier conversion to secondary progressive MS and higher neurological disability measured by EDSS (11, 13, 22). It also correlates with greater T2 lesion load and atrophy (23). Thus, our findings suggest that KFLC-index could play a potential role as an indirect indicator of intrathecal IgM synthesis that might predict worse outcomes in pwMS. CHI3L1 is a protein related to progressive disease and long-term disability in MS (24). Comabella et al. showed a correlation between OCMBs and CHI3L1 (25), and because our results suggest that KFLC-index is related to OCMBs, it might support a potential correlation with CHI3L1. Indeed, we found a weak correlation between KFLC-index and CHI3L1 cerebrospinal levels, but other studies have not confirmed this finding (17). Meningeal eLFs are reported to be the origin of intrathecal immunoglobulin production (2), although, to our knowledge, a potential link between eLFs and KFLC-index has not been described yet. In our cohort, the presence of at least one LMCE in the MRI was significantly associated with a higher KFLC-index. eLFs contribute to cortical demyelination and progression in MS (26), and therefore excess KFLC may also be a predictor of persistent cortical inflammation. This hypothesis strengthens the idea of an association between humoral and innate immune-inflammatory processes involved in the progression of disability.
While KFLC-index did not correlate to baseline EDSS, bivariate and multivariate analyses showed that a KFLC-index over 58 was a risk factor for reaching a disability score of 3 (EDSS) and increased the likelihood of treatment initiation with heDMTs. Similarly, an excess of KFLC-index has been associated with a higher probability of CIS conversion to MS (9), and patients with KFLC-index >100 at baseline had twice as high a probability of a second clinical attack within 12 months (27). Patients with higher baseline values of KFLC achieved EDSS-confirmed progression in shorter periods and showed a significant positive correlation with disability at follow-up, independently of the effects of age, OCB status at baseline, and DMT exposure (18, 28–30). Our conclusions should be interpreted cautiously due to study limitations such as low sample size, the low incidence in prognostic endpoints, and higher incidence of OCMBs as compared to other studies that might have introduced potential sources of bias. Also, the kinetics of CSF KFLC are not completely known and could be influenced by renal function, not investigated in this study.
Conclusions
Overall, this work indicates a potential link between KFLC, OCMBs, and eLFs and suggests an added prognostic value for KFLC measurement. This, added to a feasible implementation of the technique in most clinical laboratories, should prompt the performance of larger prospective studies.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the local (Hospital La Fe) Institutional Ethics Committee (reference number PI17/01544). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
BC is the head of the neuroimmunology laboratory. SG-P and BC designed the study, attended the patients, gathered and organized the clinical data, analyzed the data, wrote the manuscript, and revised the final draft. JC-V performed the biomarker analysis and wrote the manuscript. LC-N, RG-R, LS-T, and SC-B helped in gathering the biomarker and image data and revised the manuscript. FP-M, CA, and CQ-B attended the patients and helped in the registration of the clinical data. BM and JT helped to collect the analytical data and revised the manuscript. AM performed the statistical analysis. LC and AL revised the manuscript and gave statistical assistance. CF has been helping out in attending patients and in gathering of data. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This study has been funded by the Health Research Institute Carlos III (ISCIII), Ministry of Health (PI17/01544; PI020/01446), and FEDER funding. SG-P is financed by Juan Rodes Clinical Research Fellowship (ISCIII-JR20/00033).
Conflict of Interest
Authors LC and AL were employed by The Binding Site Iberia. The Binding Site has ceded the turbidimetry kits to measure KFLC for the present study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.827738/full#supplementary-material
Abbreviations
CHI3L1, chitinase 3-like 1; CIS, clinically isolated syndrome; CSF, cerebrospinal fluid; DMT, disease-modifying therapy; EDSS, Expanded Disability Status Scale; eLFs, ectopic leptomeningeal follicles; GEL, gadolinium-enhanced lesion; heDMT, high-efficacy disease-modifying therapy; KFLC, kappa free light chain; LMCE, leptomeningeal contrast enhancement; LP, lumbar puncture; MS, multiple sclerosis; NFL, neurofilament light protein; OCGBs, IgG-oligoclonal bands; OCMBs, IgM-oligoclonal bands; pwRMS, people with relapsing MS.
References
1. Sabatino JJ, Pröbstel AK, Zamvil SS. B Cells in Autoimmune and Neurodegenerative Central Nervous System Diseases. Nat Rev Neurosci (2019). doi: 10.1038/s41583-019-0233-2
2. Serafini B, Rosicarelli B, Magliozzi R, Stigliano E, Aloisi F. Detection of Ectopic B-Cell Follicles With Germinal Centers in the Meninges of Patients With Secondary Progressive Multiple Sclerosis. Brain Pathol (2004). doi: 10.1111/j.1750-3639.2004.tb00049.x
3. Prineas JW. Multiple Sclerosis: Presence of Lymphatic Capillaries and Lymphoid Tissue in the Brain and Spinal Cord. Science (1979). doi: 10.1126/science.424741
4. Magliozzi R, Howell OW, Nicholas R, Cruciani C, Castellaro M, Romualdi C, et al. Inflammatory Intrathecal Profiles and Cortical Damage in Multiple Sclerosis. Ann Neurol (2018). doi: 10.1002/ana.25197
5. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol (2018). doi: 10.1016/S1474-4422(17)30470-2
6. Kaplan B, Livneh A, Sela BA. Immunoglobulin Free Light Chain Dimers in Human Diseases. ScientificWorldJournal (2011). doi: 10.1100/tsw.2011.65
7. Van Der Heijden M, Kraneveld A, Redegeld F. Free Immunoglobulin Light Chains as Target in the Treatment of Chronic Inflammatory Diseases. Eur J Pharmacol (2006). doi: 10.1016/j.ejphar.2005.12.065
8. Hopper JE, Papagiannes E. Evidence by Radioimmunoassay That Mitogen-Activated Human Blood Mononuclear Cells Secrete Significant Amounts of Light Chain Ig Unassociated With Heavy Chain. Cell Immunol (1986). doi: 10.1016/0008-8749(86)90191-7
9. Villar LM, Espiño M, Costa-Frossard L, Muriel A, Jiménez J, Álvarez-Cermeño JC. High Levels of Cerebrospinal Fluid Free Kappa Chains Predict Conversion to Multiple Sclerosis. Clin Chim Acta (2012). doi: 10.1016/j.cca.2012.07.007
10. Pfuhl C, Grittner U, Gieß RM, Scheel M, Behrens JR, Rasche L, et al. Intrathecal IgM Production is a Strong Risk Factor for Early Conversion to Multiple Sclerosis. Neurology (2019). doi: 10.1212/WNL.0000000000008237
11. Oechtering J, Schaedelin S, Benkert P, Müller S, Achtnichts L, Vehoff J, et al. Intrathecal Immunoglobulin M Synthesis is an Independent Biomarker for Higher Disease Activity and Severity in Multiple Sclerosis. Ann Neurol (2021). doi: 10.1002/ana.26137
12. Fonderico M, Biagioli T, Lanzilao L, Bellinvia A, Fratangelo R, Pastò L, et al. Prognostic Role of Intrathecal IgM Synthesis in Multiple Sclerosis: Results From a Clinical Series. Mult Scler J (2021). doi: 10.1177/1352458520907913
13. Monreal E, Sainz de La Maza S, Costa-Frossard L, Walo-Delgado P, Zamora J, Fernández-Velasco JI, et al. Predicting Aggressive Multiple Sclerosis With Intrathecal IgM Synthesis Among Patients With a Clinically Isolated Syndrome. Neurol Neuroimmunol Neuroinflamm (2021). doi: 10.1212/NXI.0000000000001047
14. Villar LM, González-Porqué P, Masjuán J, Alvarez-Cermeño JC, Bootello A, Keir G. A Sensitive and Reproducible Method for the Detection of Oligoclonal IgM Bands. J Immunol Methods (2001). doi: 10.1016/S0022-1759(01)00492-6
15. Absinta M, Vuolo L, Rao A, Nair G, Sati P, Cortese ICM, et al. Gadolinium-Based MRI Characterization of Leptomeningeal Inflammation in Multiple Sclerosis. Neurology (2015). doi: 10.1212/WNL.0000000000001587
16. Presslauer S, Milosavljevic D, Brücke T, Bayer P, Hübl W. Elevated Levels of Kappa Free Light Chains in CSF Support the Diagnosis of Multiple Sclerosis. J Neurol (2008). doi: 10.1007/s00415-008-0954-z
17. Rosenstein I, Rasch S, Axelsson M, Novakova L, Blennow K, Zetterberg H, et al. Kappa Free Light Chain Index as a Diagnostic Biomarker in Multiple Sclerosis: A Real-World Investigation. J Neurochem (2021). doi: 10.1111/jnc.15500
18. Vecchio D, Crespi I, Virgilio E, Naldi P, Campisi MP, Serino R, et al. Kappa Free Light Chains Could Predict Early Disease Course in Multiple Sclerosis. Mult Scler Relat Disord (2019). doi: 10.1016/j.msard.2019.02.001
19. Gaetani L, Di Carlo M, Brachelente G, Valletta F, Eusebi P, Mancini A, et al. Cerebrospinal Fluid Free Light Chains Compared to Oligoclonal Bands as Biomarkers in Multiple Sclerosis. J Neuroimmunol (2020). doi: 10.1016/j.jneuroim.2019.577108
20. Duell F, Evertsson B, Al Nimer F, Sandin Å, Olsson D, Olsson T, et al. Diagnostic Accuracy of Intrathecal Kappa Free Light Chains Compared With OCBs in MS. Neurol Neuroimmunol Neuroinflamm (2020). doi: 10.1212/NXI.0000000000000775
21. Süße M, Feistner F, Grothe M, Nauck M, Dressel A, Hannich MJ. Free Light Chains Kappa can Differentiate Between Myelitis and Noninflammatory Myelopathy. Neurol Neuroimmunol Neuroinflamm (2020). doi: 10.1212/NXI.0000000000000892
22. Capuano R, Zubizarreta I, Alba-Arbalat S, Sepulveda M, Sola-Valls N, Pulido-Valdeolivas I, et al. Oligoclonal IgM Bands in the Cerebrospinal Fluid of Patients With Relapsing MS to Inform Long-Term MS Disability. Mult Scler J (2021). doi: 10.1177/1352458520981910
23. Durante L, Zaaraoui W, Rico A, Crespy L, Wybrecht D, Faivre A, et al. Intrathecal Synthesis of IgM Measured After a First Demyelinating Event Suggestive of Multiple Sclerosis is Associated With Subsequent MRI Brain Lesion Accrual. Mult Scler J (2012). doi: 10.1177/1352458511424589
24. Cantó E, Reverter F, Morcillo-Suárez C, Matesanz F, Fernández O, Izquierdo G, et al. Chitinase 3-Like 1 Plasma Levels are Increased in Patients With Progressive Forms of Multiple Sclerosis. Mult Scler J (2012). doi: 10.1177/1352458511433063
25. Comabella M, Fernández M, Martin R, Rivera-Vallvé S, Borrás E, Chiva C, et al. Cerebrospinal Fluid Chitinase 3-Like 1 Levels are Associated With Conversion to Multiple Sclerosis. Brain (2010). doi: 10.1093/brain/awq035
26. Magliozzi R, Howell O, Vora A, Serafini B, Nicholas R, Puopolo M, et al. Meningeal B-Cell Follicles in Secondary Progressive Multiple Sclerosis Associate With Early Onset of Disease and Severe Cortical Pathology. Brain (2007). doi: 10.1093/brain/awm038
27. Berek K, Bsteh G, Auer M, Di Pauli F, Grams A, Milosavljevic D, et al. Kappa-Free Light Chains in CSF Predict Early Multiple Sclerosis Disease Activity. Neurol Neuroimmunol Neuroinflamm (2021). doi: 10.1212/NXI.0000000000001005
28. Salavisa M, Paixão P, Ladeira AF, Mendes A, Correia AS, Viana JF, et al. Prognostic Value of Kappa Free Light Chains Determination in First-Ever Multiple Sclerosis Relapse. J Neuroimmunol (2020). doi: 10.1016/j.jneuroim.2020.577355
29. Pieri M, Storto M, Pignalosa S, Zenobi R, Buttari F, Bernardini S, et al. KFLC Index Utility in Multiple Sclerosis Diagnosis: Further Confirmation. J Neuroimmunol (2017). doi: 10.1016/j.jneuroim.2017.05.007
Keywords: ectopic lymphoid follicles, CHI3L1, high-efficacy disease-modifying therapies, prognostic factor, oligoclonal band
Citation: Castillo-Villalba J, Gil-Perotín S, Gasque-Rubio R, Cubas-Nuñez L, Carratalà-Boscà S, Alcalá C, Quintanilla-Bordás C, Pérez-Miralles F, Ferrer C, Cañada Martínez A, Tortosa J, Solís-Tarazona L, Campos L, Leivas A, Laíz Marro B and Casanova B (2022) High Levels of Cerebrospinal Fluid Kappa Free Light Chains Relate to IgM Intrathecal Synthesis and Might Have Prognostic Implications in Relapsing Multiple Sclerosis. Front. Immunol. 13:827738. doi: 10.3389/fimmu.2022.827738
Received: 02 December 2021; Accepted: 07 February 2022;
Published: 07 March 2022.
Edited by:
Joost Smolders, Erasmus Medical Center, NetherlandsReviewed by:
Jan Nils Lycke, University of Gothenburg, SwedenDejan Jakimovski, Buffalo Neuroimaging Analysis Center, United States
Copyright © 2022 Castillo-Villalba, Gil-Perotín, Gasque-Rubio, Cubas-Nuñez, Carratalà-Boscà, Alcalá, Quintanilla-Bordás, Pérez-Miralles, Ferrer, Cañada Martínez, Tortosa, Solís-Tarazona, Campos, Leivas, Laíz Marro and Casanova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara Gil-Perotín, c2FyYS5nYXJjaWFAdXYuZXM=
†These authors have contributed equally to this work