 Song Ouyang1,2
Song Ouyang1,2 Weifan Yin3*Qiuming Zeng1Bijuan Li4Jian Zhang5Weiwei Duan1Yi Li1Yong Liang2Jiaqi Wang2Hong Tan2Huan Yang1*
Weifan Yin3*Qiuming Zeng1Bijuan Li4Jian Zhang5Weiwei Duan1Yi Li1Yong Liang2Jiaqi Wang2Hong Tan2Huan Yang1*- 1Department of Neurology, Xiangya Hospital, Central South University, Changsha, China
- 2Medical Center of Neurology, The First Hospital of Changsha City, South China University, Changsha, China
- 3The Second Xiangya Hospital, Central South University, Changsha, China
- 4Department of Blood Transfusion, Xiangya Hospital, Central South University, Changsha, China
- 5Department of Pathology, University of Iowa, Iowa City, IA, United States
Background: Lymphoplasma exchange (LPE), a technique combining plasma exchange with leukapheresis, is emerging as promising treatment for autoimmune diseases. Data on the efficacy and safety of LPE in myasthenia gravis (MG) therapy are scarce. In this study, we aimed to comprehensively review the clinical efficacy, safety, and immunological characteristics of LPE therapy in MG patients.
Study Design and Methods: A Chinese cohort of 276 generalized MG patients in state of exacerbation, including impeding crisis, myasthenia crisis, and preparation for thoracic exsection between January 2014 and December 2020, were evaluated in this study.
Results: A total of 276 patients with a median age of 45.5 ± 16.7 years underwent a total of 635 LPE sessions. Clinical scales of Quantitative Myasthenia Gravis (QMG) scores, Myasthenia Gravis Specific Manual Muscle Testing (MMT) scores, activities of daily living (ADL) scores, and quality of life (QOL) scores were improved during 4 weeks’ follow-up. Adverse effects occurred in 20 out of 276 patients, with 14 patients having one adverse event each. Independent predictive factors for good response to LPE therapy were symptom onset before LPE therapy ≤3 days and age on LPE therapy <50 years of age. LPE decreased the serum levels of antibodies, immunoglobulins, and complements 4 weeks after the first replacement, with decreased levels of interleukin (IL)-17A and interferon (IFN)-γ and increased level of IL-10.
Conclusion: LPE is an effective treatment for MG patients in state of exacerbation and preparation for thymectomy. Early use of LPE on early-onset MG may have good therapeutic effects. The potential mechanism for LPE is the polarization of cytokines from IL-17A, IFN-γ, into IL-10.
Introduction
Myasthenia gravis (MG) is a chronic neurological autoimmune disease characterized by fluctuating weakness of voluntary muscles. It is a recurrent disease exacerbated by infection, irrational medication, or even harmful emotional stimulation. Most MG patients can maintain remission through treatment with oral glucocorticoids and immunosuppressants in an outpatient setting. However, for patients with impeding crisis or preparing for thymectomy, life-threatening exacerbations such as myasthenia crisis with respiratory fatigue and dysphagia may occur. In an acute exacerbation and in preparation for thoracic surgery, the main goal is rapidly eliminating antibodies so as to reduce damage of the neuromuscular junction. Recently, it has been acknowledged that immunoglobulins, plasma exchange (PE), and immunoadsorption are responsible for a short-term rapid disease remission (1).
The major pathogenic antibodies are anti-acetylcholine receptor (AchR) and anti-muscle-specific kinase (MusK) antibodies, accounting for approximately 80% and 7%–9%, respectively (2). Therapeutic PE has been reported to vigorously remove circulating autoantibodies and immune-competent substances (3), which are attributed to the direct separation of plasma from blood cells with membrane filtration or centrifugation, and reinfusion of the blood with plasma substitutes (4). For decades, PE has shown significant efficacy for acute exacerbation of MG, myasthenia crisis, and preparation for thymectomy in multiple clinical trials (4–6). In the international consensus guidance for MG management, PE has been recommended for impeding crisis and exacerbation of MG prior to the initiation of immunosuppressants (7).
Lymphoplasma exchange (LPE) was developed from traditional PE by combining it with lymphocyte monoculture. It involves removal of part of the patient’s plasma along with activated lymphocytes. LPE is deemed to be superior to PE in that it can not only eliminate inflammatory factors in the periphery but also remove immune-competent cells, such as T and B lymphocytes and platelets (8). Previous studies have shown that LPE therapy is beneficial for rheumatoid arthritis, Guillain–Barre syndrome, and systemic lupus erythematosus (8–10). However, in recent years, only a few studies on LPE therapy for autoimmune diseases have been reported. Our center previously reported that LPE had therapeutic effects on Guillain-Barre syndrome and pustular psoriasis of von Zumbusch (11, 12). Therapeutic LPE has been performed in very few clinical centers, and little is known about the indications and clinical responses to LPE in MG. In this article, we aimed to retrospectively analyze the clinical characteristics, immunological indices, and potential factors of LPE treatment on the outcome of MG exacerbations.
Materials and Methods
We searched the clinical database of Xiangya Hospital from January 1, 2014, to December 31, 2020, using the terms “MG diagnosis” and “LPE therapy.” We identified 321 potential MG patients and 276 patients satisfied with the following inclusion and exclusion criteria (13–15): (1) MG patients who have complete data on autoantibody tests (anti-AchR, anti-acetylcholinesterase [AchE], anti-ryanodine receptor [RyR], anti-Titin, and anti-MusK), cytokine measurement (IL-4, IL-10, IL-6, IL-17A, IL-23, and interferon [IFN]-γ), and clinical scales of QMG, MMT, ADL, and QOL scores were included in this study; (2) patients included were adults (aged older than 18 years) and in state of impeding or manifesting myasthenic crisis (Quantitative Myasthenia Gravis [QMG] score ≥20, or swallowing plus pulmonary score ≥4); (3) patients with tumors, not including malignant thymoma, were excluded from this analysis; (4) women who were pregnant, lactating, or planning pregnancy were excluded; and (5) patients with renal insufficiency or contraindications for immunoglobulin use were excluded, as it may lead to bias in treatment selection. The design of this study was shown in a flowchart (Figure 1). We collected data on the demographic characteristics, clinical features, treatment regimen, and comorbidities of patients included in the medical record system. According to the Myasthenia Gravis Foundation of America (MGFA) classification, the severity of the enrolled MG patients at onset varied from IIIa to V. QMG score improvement more than 3 points after LPE therapy was recognized as “significant improvement.”

Figure 1 The flowchart designed for this study.
For immune index evaluation, we recorded levels of immunoglobulins, cytokines, and complements (C3 and C4) from the clinical laboratory of our hospital at baseline and 1 month after the first replacement of LPE therapy. Concentrations of autoantibodies (anti-AchR, anti-AchE, anti-RyR, anti-Tintin) and cytokine were measured using enzyme-linked immunosorbent assay (ELISA), and levels of anti-MusK antibodies were detected using radioimmunoassay. The levels of immunoglobulins (IgA, IgM, and IgG) and complement (C3, C4) were measured using an automatic biochemical-immune analyzer (MY-B020, China). All participants provided written informed consent.
LPE was performed according to previously reported practices (11, 12, 16). Briefly, we used a COBE Spectra blood cell separator, installed a leukocyte pathway, and collected lymphocytes using density gradient centrifugation and optical colorimetry. For every session, we removed 25–30 ml/kg plasma along with 2–3 × 109 lymphocytes and replaced with equivalent fresh frozen plasma. The treatment regimen was one session a week. 193 patients completed two sessions of LPE treatment, and 83 patients completed three sessions of LPE treatment. All patients were administered prophylactic antiallergic drugs and calcium gluconate.
The studies involving human participants were reviewed and approved by the Medical Ethics Committee of Xiangya Hospital Central South University. We have obtained written informed consent from all study participants. All of the procedures were performed in accordance with the Declaration of Helsinki and relevant policies in China.
Statistical Analysis
Measurement data are expressed as mean ± standard deviation. Variance analysis was used to compare the mean values of the multiple samples. Student’s t-test was used to compare the mean values of the two independent samples. The Wilcoxon matched-pair signed-rank test was used to assess changes in QMG scores following LPE therapy. Statistical significance was set at p < 0.05. Univariate regression analysis was used to determine the individual variable risk factors for good clinical outcomes of LPE therapy (QMG score ≥ 50% of baseline), and all statistical analyses were performed using SPSS 22.0.
Results
Clinical Features of MG Patients With LPE Therapy
We identified 276 patients, including 166 females (60%) and 110 males (40%), who were aged between 18 and 72 years. The MGFA classification of MG patients before LPE therapy varied from classes IIIA to class V. The mean symptom duration was 24.6 ± 20.4 months. Approximately 10.9% of patients had thymic hyperplasia and 11.2% had thymoma. Of these patients, seventy-seven patients had thyroid diseases, such as hyperthyroidism (16.7%) and hypothyroidism (11.2%). During LPE, MG patients were medicated with glucocorticoids (93.5%), immunosuppressants (42.74%), or both (13.9%). The majority of antibodies were anti-AchR (89.8%) and anti-Musk antibodies (6.5%). Details of the baseline clinical characteristics are shown in Table 1.
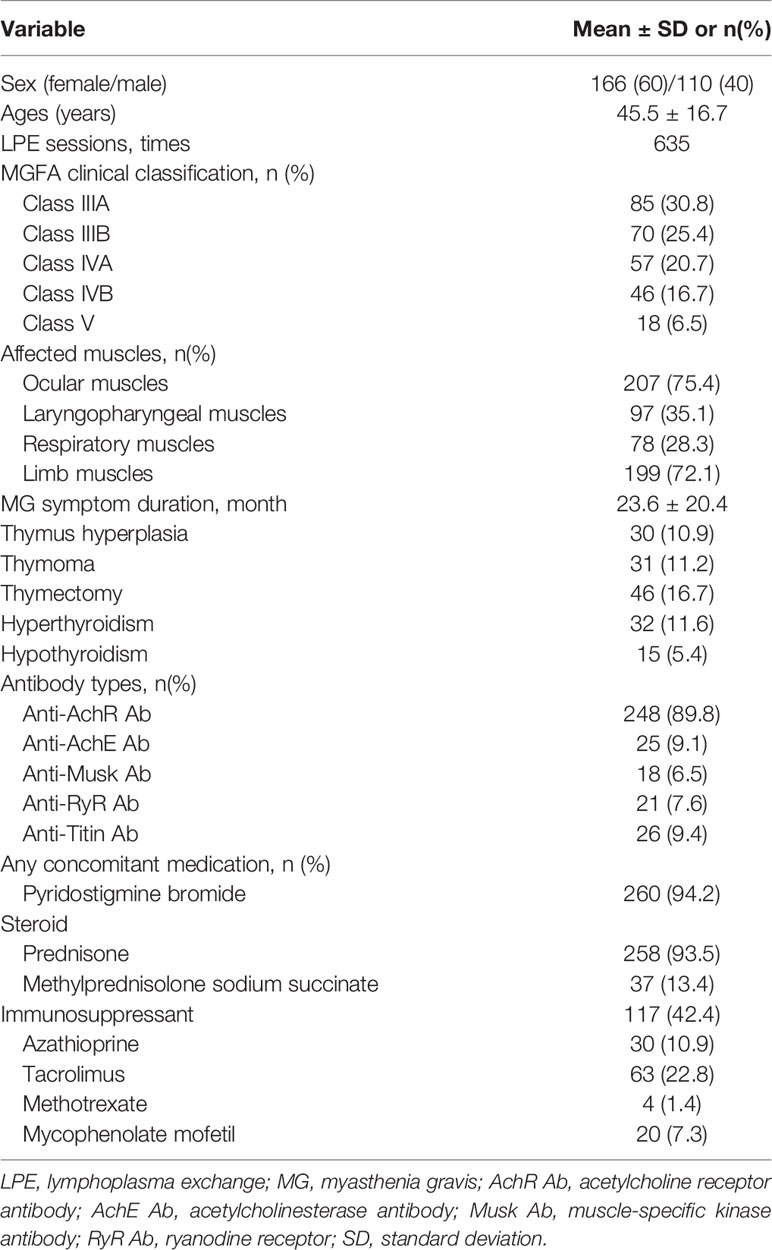
Table 1 Demographic baseline characteristics of patients with myasthenia gravis.
LPE Improved Clinical Symptoms in Generalized MG Patients
We monitored the scores of clinical scales at baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy for each patient. All patients fulfilled the QMG, MMT, ADL, and QOL scores, while only one hundred patients completed the Hamilton Depression Scale (HMDL). Before LPE therapy, the scores reflecting clinical symptoms were relatively high (QMG, 23.85 ± 4.83; MMT, 56.01 ± 13.02; MG-ADL, 10.69 ± 2.16; MG-QOL, 35.51 ± 8.09; and HMDL, 20.32 ± 26.17). One week after LPE therapy, the scores decreased gradually (QMG, 15.4 ± 4.57; MMT, 35.77 ± 10.75; MG-ADL, 8.10 ± 1.90; MG-QOL, 23.13 ± 6.62; and HMDL, 15.42 ± 4.67). All the scores further reduced 4 weeks after LPE therapy, with QMG, 6.97 ± 3.03; MMT, 14.57 ± 6.13; MG-ADL, 3.70 ± 1.86; MG-QOL, 10.82 ± 4.37; and HMDL, 8.88 ± 2.45. The detailed scores are shown in Figure 2.
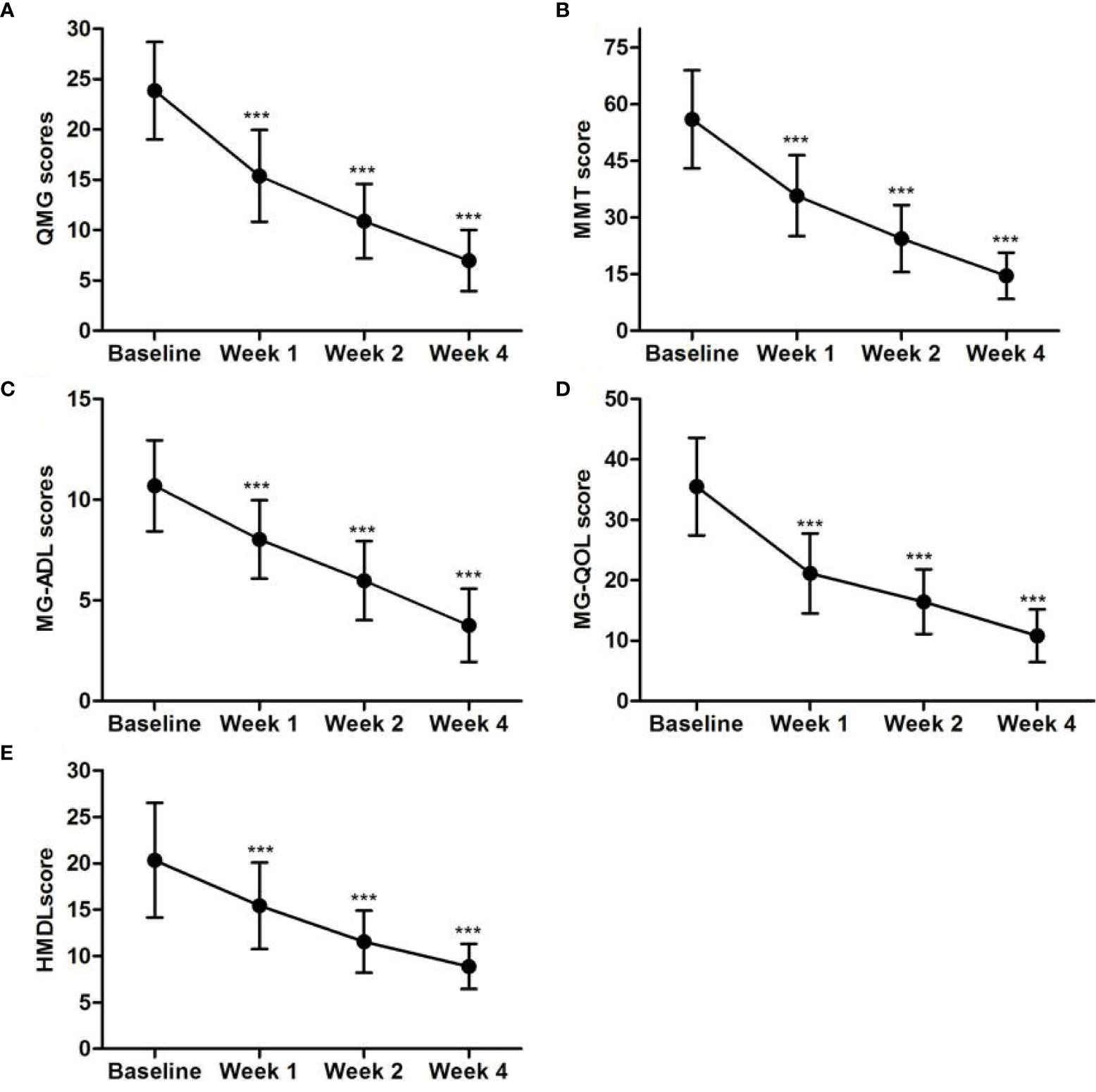
Figure 2 LPE improved clinical symptoms in generalized MG patients. The scores of QMG, MMT, MG-ADL, MG-QOL, and HMDL declined significantly 4 weeks after LPE therapy (n=276, ***p < 0.001). (A) QMG scores of MG patients of baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy. (B) MMT scores of MG patients of baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy. (C) MG-ADL scores of MG patients of baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy. (D) MG-QOL scores of MG patients of baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy. (E) HMDL scores of MG patients of baseline, week 1, week 2, and week 4 after the first replacement of LPE therapy.Note: LPE, lymphoplasma exchange; MG, myasthenia gravis; QMG, Quantitative Myasthenia Gravis; MMT, Myasthenia Gravis Specific Manual Muscle Testing; MG-ADL, Myasthenia Gravis Specific Activities of Daily Living scale; MG-QOL, myasthenia gravis quality of life; HMDL, Hamilton Depression Scale.
Predictive Factors for Outcome of LPE Therapy on MG Patients
In this study, 270 out of 276 patients responded to LPE with an improvement in QMG score ≥3 points. We divided the responsive patients into two groups: one group had a QMG score improvement of more than 50% of baseline and the other had improvement less than 50% of baseline. We studied the clinical factors that might influence the outcome of LPE therapy. Continuous variables, such as the age at onset, symptom duration before LPE therapy, antibody types, and concomitant medication, were converted into categorical variables according to the ratios of patient’s occurrence. Univariate logistic regression showed that age at LPE therapy <50 years (odds ratio [OR] = 2.35, p = 0.018), time between symptom onset and LPE therapy ≤3 days (OR = 3.289, p = 0.049), concomitant medication with glucocorticoids (OR = 1.238, p = 0.05), and advanced stage (stage IIIa to IV) (OR = 2.395, p = 0.041) were significantly associated with clinical improvement. The multivariable logistic regression analysis confirmed the time between symptom onset and LPE therapy ≤3 days (OR = 3.045 [1.231–8.465], p = 0.031) and age at LPE therapy <50 years (OR = 2.045 [0.931–4.465], p = 0.015) as independent predictive factors that significantly affected the clinical improvement of MG (Table 2).
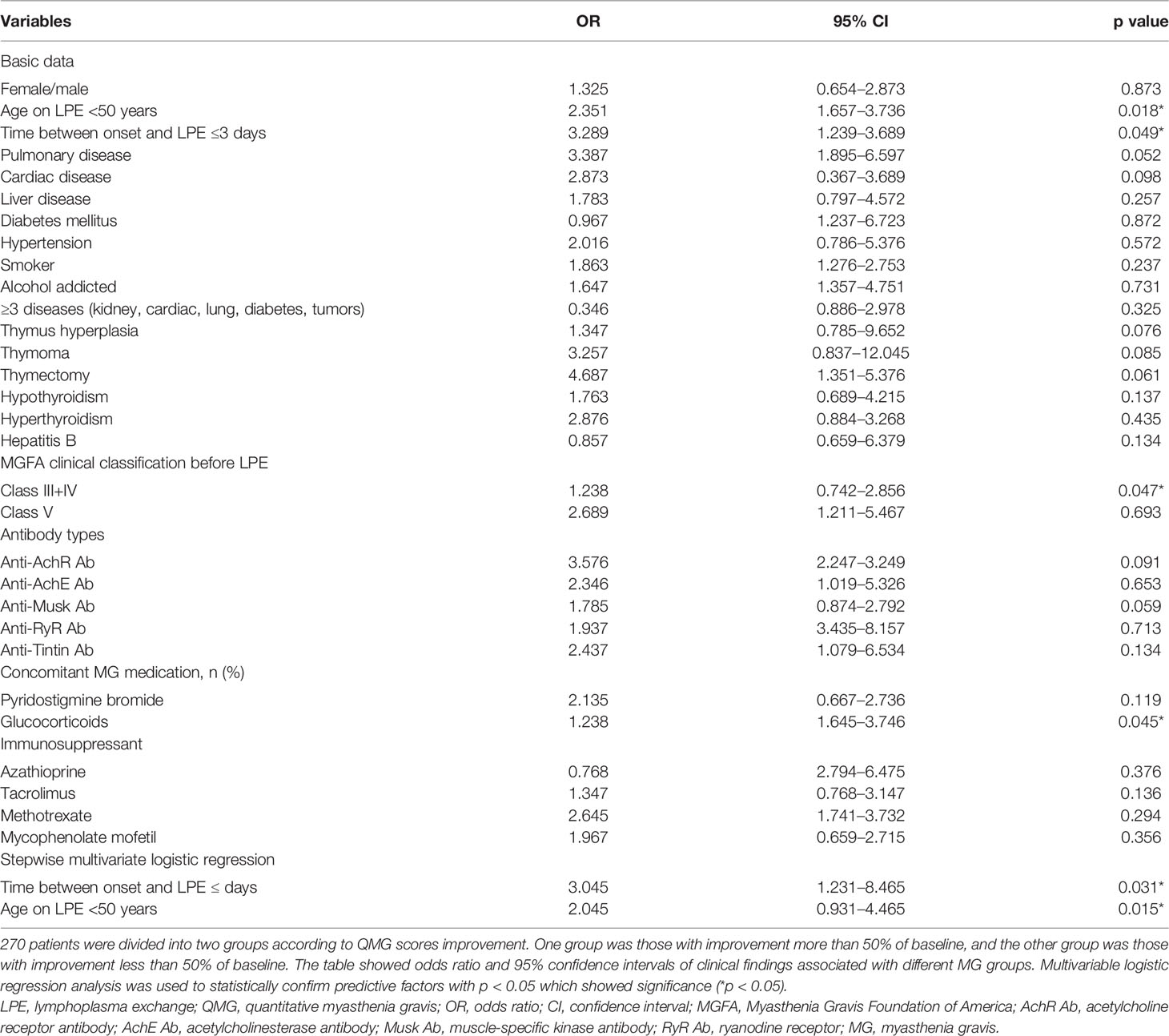
Table 2 Predictive factors affecting the outcome of LPE therapy on groups with QMG score improvement more than 50 percentage.
Effects of LPE on Serum Levels of Antibodies, Immunoglobulins, and Complements
Four weeks after the first session of LPE therapy, the levels of the anti-AchR antibody decreased significantly, compared with that before therapy (10.78 ± 9.62 vs. 18.75 ± 16.3 nmol/ml, p < 0.05, n = 248). Levels of anti-AchE, anti-Musk, anti-Ryr, and anti-Titin decreased after LPE therapy (Figure 3). Similarly, the levels of immunoglobulin (IgA, IgM, IgG) and complement (C3, C4) were significantly reduced compared with those before therapy (Figure 4).
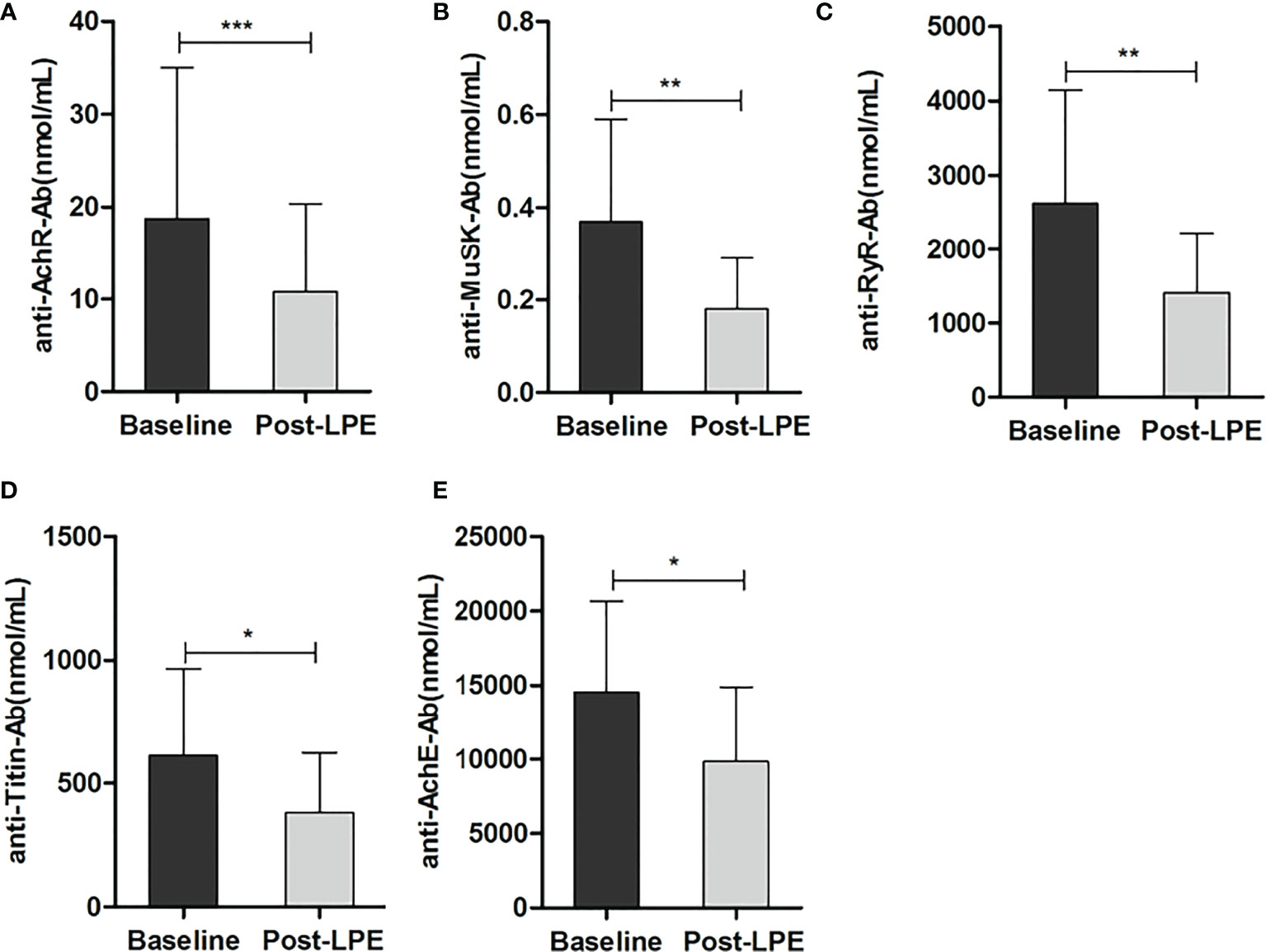
Figure 3 LPE reduced serum levels of autoantibodies after LPE therapy. (A) Effect of LPE on the anti-AchR antibody (n = 248). (B) Effect of LPE on anti-MusK antibody (n = 18). (C) Effect of LPE on the anti-RyR antibody (n = 21). (D) Effect of LPE on anti-Titin antibody(n = 26). (E) Effect of LPE on anti-AchE antibody (n = 25) (*p < 0.05, **p < 0.01, ***p < 0.001).LPE, lymphoplasma exchange; AchR Ab, acetylcholine receptor antibody; AchE Ab, acetylcholinesterase antibody; Musk Ab, anti-muscle-specific kinase antibody; RyR Ab, anti-ryanodine receptor; MG, myasthenia gravis.
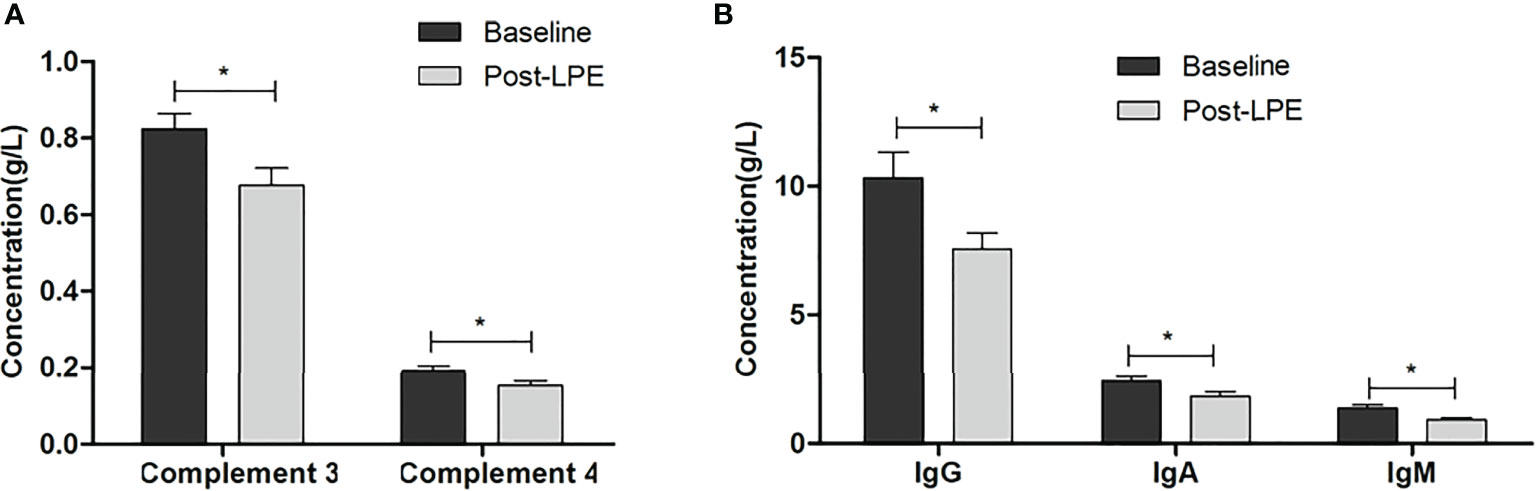
Figure 4 LPE reduced serum levels of immunoglobulins and complements after LPE therapy. (A) LPE reduced serum concentrations of complement C3 and C4 (n = 186). (B) LPE reduced serum concentrations of immunoglobulins (IgA, IgG, IgM) (n = 166) (*p < 0.05). LPE, lymphoplasma exchange.
Effects of LPE on Cytokines in Periphery
In 87 out of 273 MG patients, serum levels of interleukin (IL)-4, IL-10, IL-6, IL-17A, IL-23, and IFN-γ before and 4 weeks after the first session of LPE therapy were detected by ELISA. IL-17A, IFN-γ, and IL-23 decreased significantly after LPE, while IL-10 increased during therapy, and the levels of IL-4 and IL-6 did not change significantly during the LPE therapy (Figure 5).
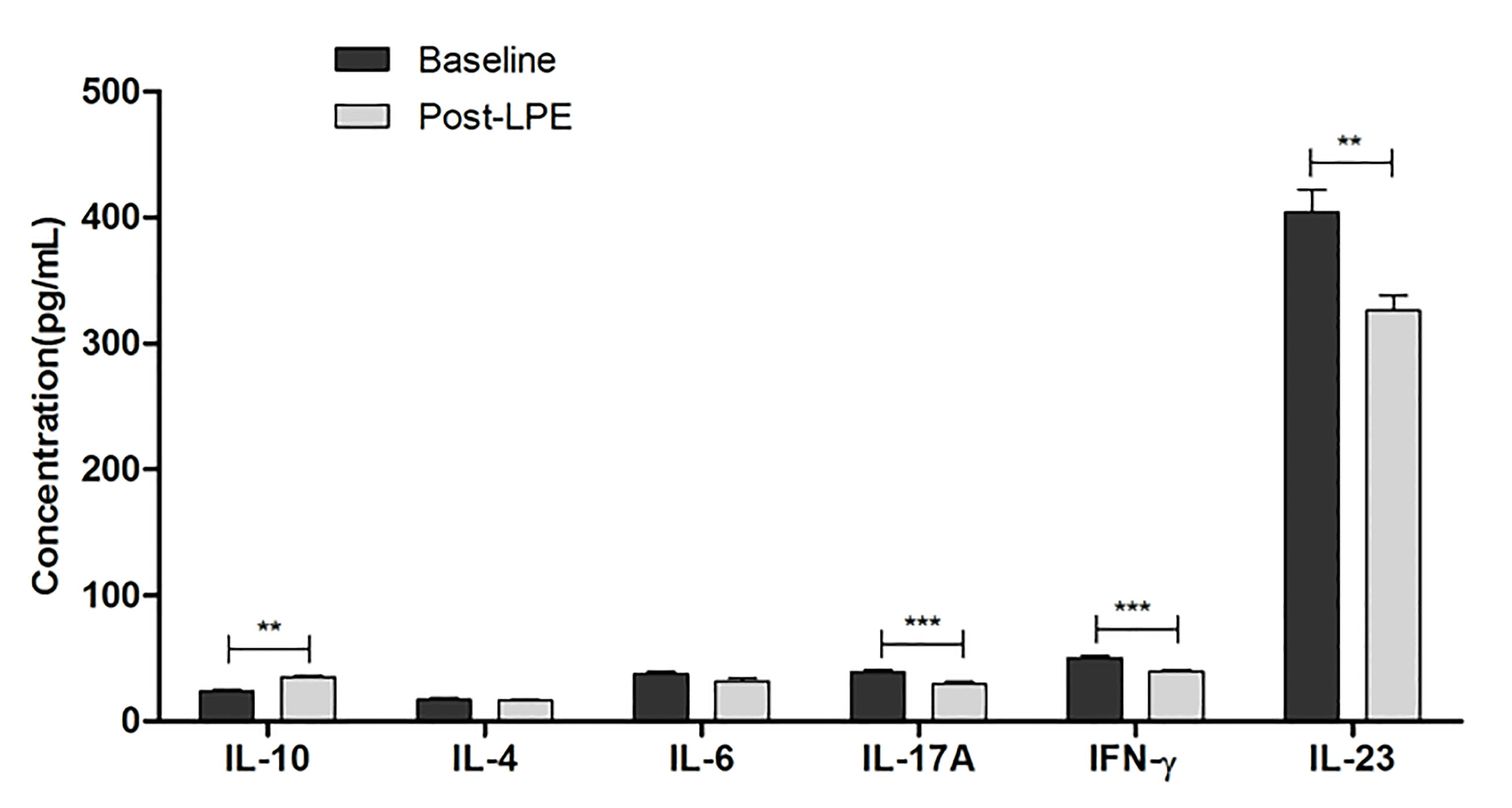
Figure 5 Serum levels of IL-4, IL-10, IL-6, IL-17A, IL-23, and IFN-γ before and after LPE therapy were detected in 87 MG patients. Cytokines were detected with ELISA from peripheral blood of MG patients and healthy controls (**p < 0.01, ***p < 0.001). ELISA, enzyme-linked immunosorbent assay; IL, interleukin; IFN, interferon; LPE, lymphoplasma exchange.
Adverse Effects of LPE
In 26 out of 635 single LPE sessions (4.1%), adverse effects occurred in 20 out of 276 patients (14 patients had one adverse event each). None of the patients had an adverse event of related death. The most common adverse effects were allergic reaction and hypocalcemia that occurred in three patients, respectively. After the first replacement of LPE, one patient experienced post-infusion systemic reactions, and one patient had vasovagal syncope. Local adverse events were infection and bleeding (two cases of bleeding and one case of infection due to vascular access, respectively). Emotional adverse effects occurred in two patients, both of which manifested as sleep disorders. Two patients experienced moderate hypotension and recovered after crystalloid infusion. Gastrointestinal symptoms occurred in four patients (one patient had diarrhea, another had nausea and vomiting), who were administered symptomatic treatment. One patient had systematic infection without sepsis, who manifested with fever and cough. This patient had a higher C-reactive protein, procalcitonin, and leukocyte ratio compared with that before LPE therapy. He recovered several days after antibiotic medication. One patient suffered from influenza after the second session of LPE treatment and recovered with symptomatic treatment. Non-specific symptoms (two patients with pain due to vascular access and two patients with headache) were also observed. Details of the adverse effects are shown in Table 3.
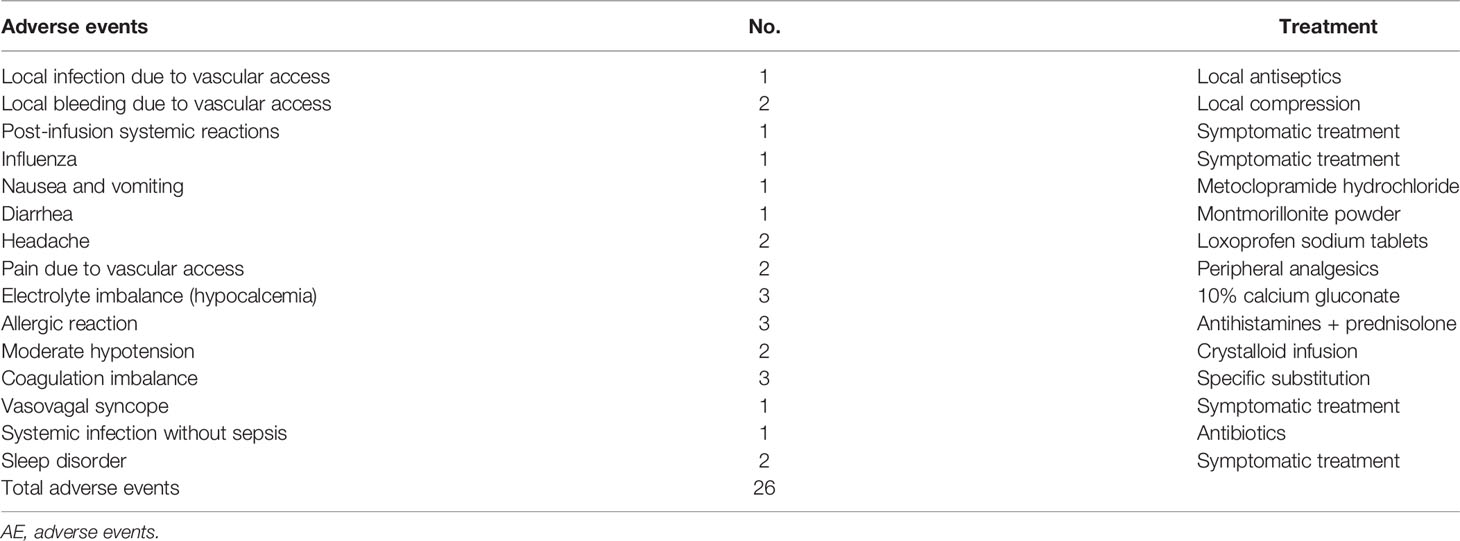
Table 3 Adverse events (AEs) during therapeutic lymphoplasma exchange (n = 635 sessions).
Discussion
We analyzed 635 single LPE sessions in 276 individual patients, which represent the largest retrospective cohort on LPE therapy to date. Previously, the investigators noticed encouraging therapeutic effects of LPE on several cases of acute systemic lupus erythematosus, rheumatoid arthritis, and acute renal allograft rejection (9, 10, 17). Recently, Luo et al. reported the therapeutic effects of LPE in only 12 cases of Guillain-Barre syndrome (8). Consistent with earlier reports, we concluded that LPE therapy improved MG exacerbation by recording a sustained clinical improvement with subjective and objective scales at 4 weeks post LPE therapy, which indicated good clinical management and daily activity (18, 19). Our findings of variations in immune indices could supplement the existing literature with new aspects.
In this study, we observed a reduction in complement, autoantibodies, and immunoglobulin levels 4 weeks after LPE therapy. This phenomenon is due to the direct elimination of immune substances and is in line with the findings of previous studies of PE but with minor differences (20). Compared to PE, LPE seems to sustain immune suppression for a longer duration. Liu et al. demonstrated that PE efficiently cleared autoantibodies and intercellular adhesion molecule-1 and evoked Treg cells in late-onset MG in the short term (21). Chien et al. also showed that PE had an excellent short effect, and it could adjust the ratio of T helper cells to T suppressor cells after a single session (22). In 2016, Guptill et al. conducted an integrated study of PE effects on immunoglobulins and IgG isotypes, which showed that AchR antibodies IgG, IgG1, and IgG2 were reduced below the reference range at 3 weeks post PE (23). We deduced that the reason for LPE having a longer immune suppression effect than PE was partly due to the reduction of activated lymphocytes along with plasma, although a detailed comparison between PE and LPE needs further elucidation.
Due to the retrospective nature of this study, we could not screen the T-cell subsets of all patients. Instead, we detected cytokines that may reflect related T helper cells. In the pathogenesis of MG, Th1 cells, which secrete IFN-γ, play a key role in the initiation of experimental autoimmune myasthenia gravis (EAMG) (24, 25). IL-4, a main cytokine secreted by Th2 cells, inhibits the proliferation of Th1 cells and exerts an inhibitory function on Th1 (26). Multiple clinical studies have used the ratio of Th1/Th2 to indicate the immune state during therapy for autoimmune diseases (27). Th17 cells, which secrete IL-17, participate in the progression of MG. Hosseini et al. reported that the increased frequency of Th17 cells was closely correlated with the clinical severity of MG patients (28). Treg play a crucial role in immune homeostasis. The frequency or functional deficiency of Treg may lead to an exacerbation of MG (5). IL-6 plays an important role in balancing Th17 and Treg cells by promoting Th17 and inhibiting Treg differentiation (29, 30). Immune treatment exerts its influence by regulating T helper cells and cytokine IL-10. Zhang et al. reported that PE benefits MG patients through cytokines (IL-2, IL-4, IL-10, and IFN-γ) and Treg (31). In multiple sclerosis, PE decreased IL-6 and increased TGF-β expression in patients (32). Our results of cytokine polarization indicated that LPE decreased proinflammatory cytokines IL-12, IL-17A, IFN-γ, and IL-23 but increased IL-10. Numerous studies have reported that plasma exchange exerts therapeutic effects by altering the polarization of cytokine profiles from Th1, Th2, to Th17 and Treg. IL-10, secreted by Treg, was increased after plasma exchange in multiple autoimmune diseases, such as myasthenia gravis (33), thrombotic thrombocytopenic purpura (34), and multiple sclerosis (35). LPE combines plasma exchange with removal of activated lymphocytes, so it has a similar mechanism with PE on cytokine polarization of IL-10 increase, while extending the time duration for immune tolerance. Our group has previously reported that LPE was effective in treatment of Guillain-Barre syndrome patients by directly removing immunoglobulin, complement, monocytes, and fibrinogen as well as polarizing T helper subsets from Th1, Th17 to Th2 and Treg profiles in the peripheral blood (21), which was consistent with our findings in MG patients. The duration for suppressive effects and the increase of IL-10 in our study might partly be due to the sequential use of glucocorticoids and immunosuppressants for long-term immunotherapy. We depicted a preliminary network of cytokines upon LPE effect. Further mechanisms still need to be elucidated.
Usmani et al. showed that PE had a 96% response rate to MG (36). Comparably, our study showed that the efficiency rate of LPE was 98%. Since both studies were in real-world practice, the reason for the high resolution rate may be the continued usage of glucocorticoids and immunosuppressants. It is important to know which patients will have a good response to LPE. In addition, response to PE was good when it was used early (37). We found that age at LPE therapy <50 years, symptom onset before LPE therapy ≤3 days, concomitant medication with glucocorticoids, and advanced stage were associated with clinical improvement. Symptom onset before LPE therapy ≤3 days and age during LPE therapy <50 years were independent predictive factors for a better response to LPE therapy, which may indicate that young patients may have few cardiopulmonary complications and that the earlier the LPE therapy, the better the outcome.
We documented 26 adverse effects during LPE therapy, including infection, non-specific symptoms, gastrointestinal disorders, coagulation imbalance, and allergic reactions, among others. No patient died secondary to adverse events. These adverse effects had similar events but lower rates than those recorded recently in the PE therapy of the intensive unit (38), which improved with symptomatic treatment. We examined systematic infections by measuring clinical manifestation (fever, cough, expectoration, etc.), blood biomedical indexes (leukocyte counts and ratio in blood routine, erythrocyte sedimentation rate, C-reactive protein, procalcitonin, and blood and urine culture), and radiological examination (chest and abdomen CT). The incidence of infection was relatively lower compared with that of plasma exchange (39). The reason for the relatively low rate of adverse effects may be due to the low frequency of LPE therapy once a week, and a fast benefit could be achieved in the short term for patients with severe symptoms.
Some limitations of our study must be highlighted. First, the observation time was inadequate to explore the long-term effects of LPE therapy. Second, the retrospective nature of this study was a limitation of our analysis. Comparative studies are warranted to provide a horizontal competition between a first-line therapy of PE, immunoglobulins, immune adsorption, etc. Third, our results were not stratified according to the severity of MG or differential autoantibody types.
In conclusion, LPE is an effective treatment for MG patients in state of exacerbation. Early use of LPE on early-onset MG may have good therapeutic effects. The potential mechanism for LPE is the polarization of cytokines IL-17A, IFN-γ, and IL-10. These findings need to be confirmed by randomized controlled trials and discussed in detail in further studies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by the Medical Ethics Committee of Xiangya Hospital Central South University. We have obtained written informed consent from all study participants. All of the procedures were performed in accordance with the Declaration of Helsinki and relevant policies in China.
Author Contributions
HY designed and funded the project. SO and WY performed, analyzed, and discussed the data, took major part in writing the manuscript, and funded the project. QZ discussed the data and provided financial support. BL performed the plasma exchange. JZ discussed the design as well as the data of the study. WD, YiL, JW, and HT took part in designing the research and discussing the data. YoL partly provided financial support. All authors contributed to the article and approved the submitted version.
Funding
The project described was supported by grants provided by the Natural Science Foundation of China (81771364 and 81801203), Science and Technology Innovation Guidance Project of Hunan Province (2020SK53009, 2020SK53008), and Changsha Municipal Natural Science Foundation (kq2007037).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rössling R, Prüss H. Apheresis in Autoimmune Encephalitis and Autoimmune Dementia. J Clin Med (2020) 9:2683. doi: 10.3390/jcm9092683
2. Osman C, Jennings R, El-Ghariani K, Pinto A. Plasma Exchange in Neurological Disease. Pract Neurol (2020) 20:92–9. doi: 10.1136/practneurol-2019-002336
3. Jiang Y, Tian X, Gu Y, Li F, Wang X. Application of Plasma Exchange in Steroid-Responsive Encephalopathy. Front Immunol (2019) 10:324. doi: 10.3389/fimmu.2019.00324
4. Milani M, Ostlie N, Wu H, Wang W, Conti-Fine BM. CD4+ T and B Cells Cooperate in the Immunoregulation of Experimental Autoimmune Myasthenia Gravis. J Neuroimmunol (2006) 179:152–62. doi: 10.1016/j.jneuroim.2006.07.004
5. Danikowski KM, Jayaraman S, Prabhakar BS. Regulatory T Cells in Multiple Sclerosis and Myasthenia Gravis. J Neuroinflammation (2017) 14:117. doi: 10.1186/s12974-017-0892-8
6. Mu L, Sun B, Kong Q, Wang J, Wang G, Zhang S, et al. Disequilibrium of T Helper Type 1, 2 and 17 Cells and Regulatory T Cells During the Development of Experimental Autoimmu- Ne Myasthenia Gravis. Immunology (2009) 128:e826–36. doi: 10.1111/j.1365-2567.2009.03089.x
7. Marinos CD. Treating Myasthenia on Consensus Guide: Helpful and Challenging But Still Unfinished Business. Neurology (2016) 87:350–1. doi: 10.1212/WNL.0000000000002796
8. Masuda M, Matsumoto M, Tanaka S, Nakajima K, Yamada N, Ido N, et al. Clinical Implication of Peripheral CD4+CD25+ Regulatory T Cells and Th17 Cells in Myasthenia Gravis Patients. J Neuroimmunol (2010) 225:123–31. doi: 10.1016/j.jneuroim.2010.03.016
9. Kleinman S, Nichols M, Strauss F, Goldfinger D. Use of Lymphoplasmapheresis or Plasmapheresis in the Management of Acute Renal Allograft Rejection. J Clin Apher (1982) 1:14–7. doi: 10.1002/jca.2920010105
10. Stojanov A, Milošević V, Dorđević G, Stojanov J. Quality of Life of Myasthenia Gravis Patients in Regard to Epidemiological and Clinical Characteristics of the Disease. Neurologist (2019) 24:115–20. doi: 10.1097/NRL.0000000000000238
11. Luo MC, Wang WF, Yin WF, Li Y, Li BJ, Duan WW, et al. Clinical Efficacy and Mechanism of Lymphoplasma Exchange in the Treatment of Guillain-Barre Syndrome. Cell Mol Biol(Noisy-le-grand) (2017) 63:106–15. doi: 10.14715/cmb/2017.63.10.17
12. Zhang M, Zhang Y, Zhu W, Kuang Y. Successful Use of Lymphoplasma Exchange in a Patient With Acute Generalized Pustular Psoriasis of Von Zumbusch. Dermatol Ther (2020) 33:e14092. doi: 10.1111/dth.14092
13. Bedlack RS, Simel DL, Bosworth H, Samsa G, Tucker-Lipscomb B, Sanders DB. Quantitative Myasthenia Gravis Score: Assessment of Responsiveness and Longitudinal Validity. Neurology (2005) 64:1968–70. doi: 10.1212/01.WNL.0000163988.28892.79
14. Sanders DB, Wolfe GI, Benatar M, Evoli A, Gilhus NE, Illa I, et al. International Consensus Guidance for Management of Myasthenia Gravis: Executive Summary. Neurology (2016) 87:419–25. doi: 10.1212/WNL.0000000000002790
15. Narayanaswami P, Sanders DB, Wolfe G, Benatar M, Cea G, Evoli A, et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology (2021) 96:114–22. doi: 10.1212/WNL.0000000000011124
16. Wang B, Li J, Xie HF, Chen ML, Li BJ, Shi W, et al. Striking Case of Febrile Ulceronecrotic Mucha-Habermann Disease Responding to Lymphoplasmapheresis and Methotrexate. J Dermatol (2020) 47:e430–1. doi: 10.1111/1346-8138.15598
17. Alanazy MH, Binabbad RS, Alromaih NI, Almansour RA, Alanazi SN, Alhamdi MF, et al. Severity and Depression can Impact Quality of Life in Patients With Myasthenia Gravis. Muscle Nerve (2020) 61:69–73. doi: 10.1002/mus.26719
18. Lemaire A, Parquet N, Galicier L, Boutboul D, Bertinchamp R, Malphettes M, et al. Plasma Exchange in the Intensive Care Unit: Technical Aspects and Complications. J Clin Apher (2017) 32:405–12. doi: 10.1002/jca.21529
19. Kim JY, Park KD, Richman DP. Treatment of Myasthenia Gravis Based on its Immunopathogenesis. J Clin Neurol (2011) 7:173–83. doi: 10.3988/jcn.2011.7.4.173
20. Jamshidian A, Abd-Nikfarjam B, Khademi Z, Shaygannejad V, Salehi M. Therapeutic Plasma Exchange may Adjust IL-6 and TGF-β Signals in Relapsed MS Patients Peripheral Blood. J Clin Apher (2020) 35:72–8. doi: 10.1002/jca.21755
21. Liu JF, Wang WX, Xue J, Zhao CB, You HZ, Lu JH, et al. Comparing the Autoantibody Levels and Clinical Efficacy of Double Filtration Plasmapheresis, Immunoadsorption, and Intravenous Immunoglobulin for the Treatment of Late-Onset Myasthenia Gravis. Ther Apher Dial (2010) 14:153–60. doi: 10.1111/j.1744-9987.2009.00751.x
22. Chien PJ, Yeh JH, Shih CM, Hsueh YM, Chen MC, Chiu HC. A Decrease in the Percentage of CD3+ Cells is Correlated With Clinical Improvement During Plasmapheresis in Patients With Myasthenia Gravis. Artif Organs (2013) 37:211–6. doi: 10.1111/j.1525-1594.2012.01531.x
23. Guptill JT, Juel VC, Massey JM, Anderson AC, Chopra M, Yi JS, et al. Effect of Therapeutic Plasma Exchange on Immunoglobulins in Myasthenia Gravis. Autoimmunity (2016) 49:472–9. doi: 10.1080/08916934.2016.1214823
24. Liu R, Hao J, Dayao CS, Shi FD, Campagnolo DI. T-Bet Deficiency Decreases Susceptibility to Experimental Myasthenia Gravis. Exp Neurol (2009) 220:366–73. doi: 10.1016/j.expneurol.2009.09.022
25. Suzuki Y, Onodera H, Tago H, Saito R, Ohuchi M, Shimizu M, et al. Altered Expression of Th1-Type Chemokine Receptor CXCR3 on CD4+ T Cells in Myasthenia Gravis Patients. J Neuroimmunol (2006) 172:166–74. doi: 10.1016/j.jneuroim.2005.10.001
26. Yang H, Zhang Y, Wu M, Li J, Zhou W, Li G, et al. Suppression of Ongoing Experimental Autoimmune Myasthenia Gravis by Transfer of RelB-Silenced Bone Marrow Dentritic Cells is Associated With a Change From a T Helper Th17/Th1 to a Th2 and FoxP3+ Regulatory T-Cell Profile. Inflammation Res (2010) 59:197–205. doi: 10.1007/s00011-009-0087-6
27. Takahashi N, Saitoh T, Gotoh N, Nitta Y, Alkebsi L, Kasamatsu T, et al. The Cytokine Polymorphisms Affecting Th1/Th2 Increase the Susceptibility to, and Severity of, Chronic ITP. BMC Immunol (2017) 18:26. doi: 10.1186/s12865-017-0210-3
28. Hosseini M, Robat-Jazi B, Shaygannejad V, Naffisi S, Mirmossayeb O, Rezaei A, et al. Increased Proportion of Tc17 and Th17 Cells and Their Significant Reduction After Thymectomy May Be Related to Disease Progression in Myasthenia Gravis. Neuroimmunomodulation (2017) 24:264–70. doi: 10.1159/000486037
29. Yao X, Kong Q, Xie X, Wang J, Li N, Liu Y, et al. Neutralization of Interleukin-9 Ameliorates Symptoms of Experimental Autoimmune Myasthenia Gravis in Rats by Decreasing Effector T Cells and Altering Humoral Responses. Immunology (2014) 143:396–405. doi: 10.1111/imm.12322
30. Zhang L, Liu J, Wang H, Zhao C, Lu J, Xue J, et al. Double Filtration Plasmapheresis Benefits Myasthenia Gravis Patients Through an Immunomodulatory Action. J Clin Neurosci (2014) 21:1570–4. doi: 10.1016/j.jocn.2013.11.046
31. Gilhus NE, Tzartos S, Evoli A, Palace J, Burns TM, Verschuuren JJGM. Myasthenia Gravis. Nat Rev Dis Primers (2019) 5:30. doi: 10.1038/s41572-019-0079-y
32. Mantegazza R, Bernasconi P, Cavalcante P. Myasthenia Gravis: From Autoantibodies to Therapy. Curr Opin Neurol (2018) 31:517–25. doi: 10.1097/WCO.0000000000000596
33. Shariatmadar S, Nassiri M, Vincek V. Effect of Plasma Exchange on Cytokines Measured by Multianalyte Bead Array in Thrombotic Thrombocytopenic Purpura. Am J Hematol (2005) 79(2):83–8. doi: 10.1002/ajh.20342
34. Yeh JH, Wang JH, Chien PJ, Shih CM, Chiu HC. Changes in Serum Cytokine Levels During Plasmapheresis in Patients With Myasthenia Gravis. Eur J Neurol (2009) 16(12):1318–22. doi: 10.1111/j.1468-1331.2009.02729.x
35. Jamshidian A, Gharagozloo M. Can Plasma Exchange Therapy Induce Regulatory T Lymphocytes in Multiple Sclerosis Patients? Clin Exp Immunol (2012) 168(1):75–7. doi: 10.1111/j.1365-2249.2011.04547.x
36. Usmani A, Kwan L, Wahib-Khalil D, Trivedi J, Nations S, Sarode R. Excellent Response to Therapeutic Plasma Exchange in Myasthenia Gravis Patients Irrespective of Antibody Status. J Clin Apher (2019) 34:416–22. doi: 10.1002/jca.21694
37. Zhang Y, Liu G, Jiang M, Chen W, Su Y. Efficacy of TherapeuticPlasma Exchange in Patients with Severe Refractory Anti-NMDA Receptor Encephalitis. Neurotherapeutics (2019) 16:828–37. doi: 10.1007/s13311-019-00725-4
38. Hatton RD. TGF-β in Th17 Cell Development: The truth Is Out There. Immunity (2011) 34:288–90. doi: 10.1016/j.immuni.2011.03.009
Keywords: myasthenia gravis (MG), lymphoplasma exchange (LPE), quantitative myasthenia gravis (QMG), autoimmune diseases, plasma exchange (PE)
Citation: Ouyang S, Yin W, Zeng Q, Li B, Zhang J, Duan W, Li Y, Liang Y, Wang J, Tan H and Yang H (2022) Lymphoplasma Exchange Improves Myasthenia Gravis Exacerbations: A Retrospective Study in a Chinese Center. Front. Immunol. 13:757841. doi: 10.3389/fimmu.2022.757841
Received: 12 August 2021; Accepted: 16 March 2022;
Published: 14 April 2022.
Edited by:
Anna Rostedt Punga, Uppsala University, SwedenReviewed by:
Nils Erik Gilhus, University of Bergen, NorwayYan Li, The First Affiliated Hospital of Sun Yat-sen University, China
Copyright © 2022 Ouyang, Yin, Zeng, Li, Zhang, Duan, Li, Liang, Wang, Tan and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huan Yang, NDAzODUwQGNzdS5lZHUuY24=; Weifan Yin, eWlud2VpZmFuMTk4NUBjc3UuZWR1LmNu