 Amr Ehab El-Qushayri
Amr Ehab El-Qushayri Abdullah Reda
Abdullah Reda Jaffer Shah
Jaffer Shah
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol., 14 December 2022
Sec. Viral Immunology
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1094346
This article is part of the Research TopicCOVID and Emerging Infectious DiseasesView all 47 articles
In this paper we aimed to study the characteristics, laboratory data and outcomes of monkeypox virus (MPV) and COVID-19 co-infection. On 2nd October 2022, we used the search term “(“monkeypox virus” OR “MPV” OR “monkey pox” OR “monkeypox”) AND (“COVID-19” OR “COVID 19” OR “novel coronavirus” OR “SARS−CoV−2”)” in five databases to collect the relevant articles. We found three male patients, who had sex with men prior to the infection, had multiple comorbid conditions, were diagnosed with PCR, and were admitted to the hospital. The length of hospital stay was 4, 6, and 9 days. On admission, two cases had multiple vesicular lesions on various sites of the body associated with tonsillar inflammation, while the third case had genital ulcers and inguinal lymph node enlargement. All cases were managed in the hospital and recovered well. It might still be too early to establish solid evidence about the exact cause-effect association between SARS-CoV-2 and MPV co-infection and patient’s outcomes because of the current low sample size. Accordingly, future relevant investigations, estimating the risk ratio of this association are needed to formulate definite evidence.
COVID-19 still constitutes a remarkable burden on countries and their healthcare systems even with the remarkable advances in the vaccine industry. COVID-19 patients are liable to various complications, and those with co-morbidities and associated infections are usually the most vulnerable (1, 2). Recently, a multi-country outbreak of monkeypox virus (MPV) occurred and the World Health Organization declared it a Public Health Emergency of International Concern. Accordingly, certain concerns aroused regarding the outcomes of patients co-infected with COVID-19 and MPV.
To collect all the papers that reported COVID-19 and MPV co-infection, we searched in five databases: PubMed (131), Virtual Health Library (122), Google Scholar (75), Web of Science (79), and Scopus (108). On 2nd October 2022, we used the search term “(“monkeypox virus” OR “MPV” OR “monkey pox” OR “monkeypox”) AND (“COVID-19” OR “COVID 19” OR “novel coronavirus” OR “SARS−CoV−2”)” through all the databases and adapted it to fit the search process in each database. The literature search resulted in 3 articles reporting 3 cases of COVID-19 and MPXV co-infection (Table 1). All cases were male patients, who had sex with men prior to the infection, had multiple comorbid conditions, were diagnosed with PCR, and were admitted to the hospital. The length of hospital stay was 4, 6, and 9 days. On admission, two cases had multiple vesicular lesions on various sites of the body associated with tonsillar inflammation, while the third case had genital ulcers and inguinal lymph node enlargement. All cases were managed in the hospital and recovered well.
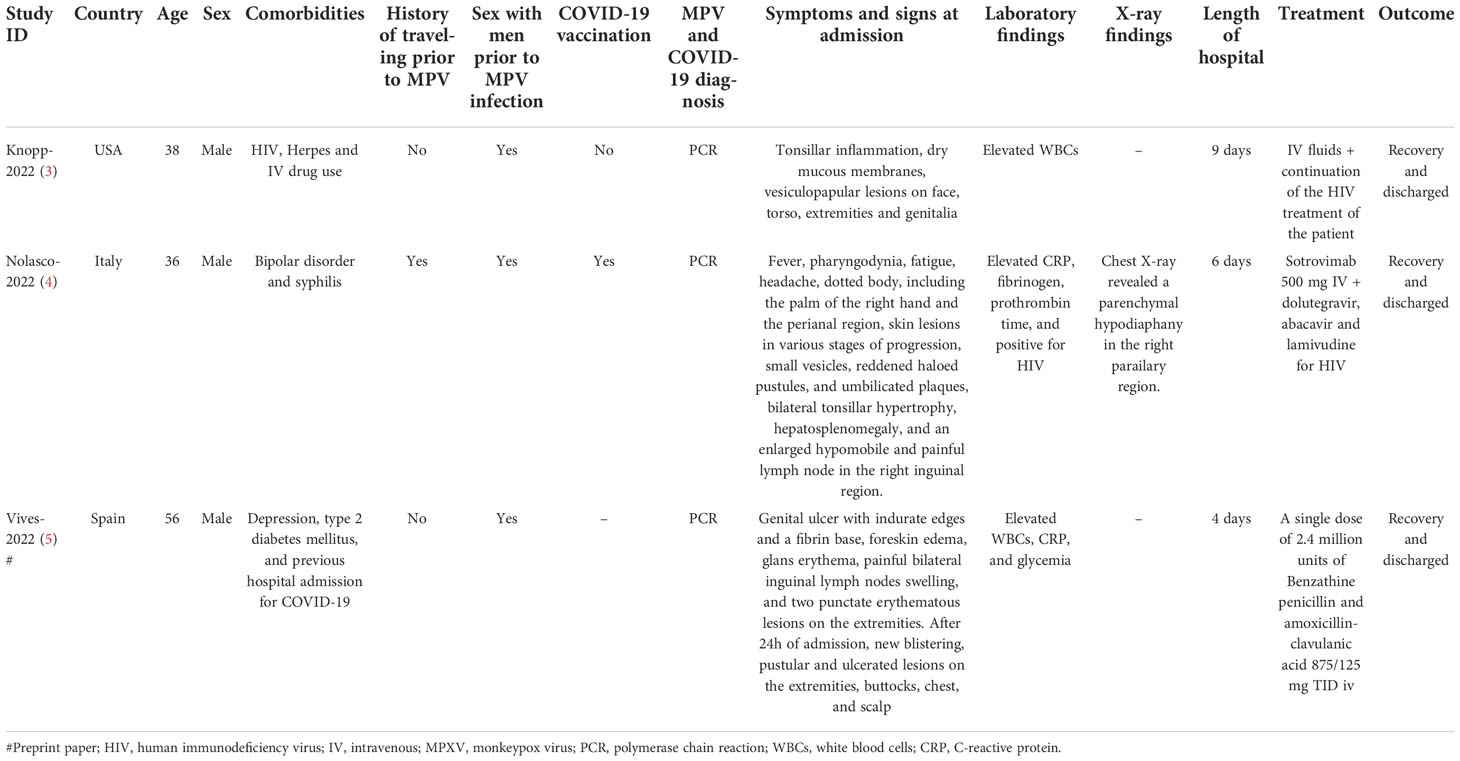
Table 1 Characteristics of patients with COVID-19 and MPV co-infection.
Our findings indicated that although all the included three cases with the co-infection were hospitalized, none of them developed severe outcomes and were discharged after a good recovery. Accordingly, these findings showed that patients having COVID-19 and MPV co-infection might not develop severe outcomes since all the included patients also had multiple comorbid conditions, which were previously reported as significant risk factors for developing severe COVID-19 outcomes (2). To our knowledge, COVID-19 infection presents usually with fever, cough, fever and smell and tasting disorders. However, the characteristic vesicular and ulcerative lesions in the genital lesions together with the enlargement of lymph nodes in our series are not common features of the disease and suggested co-infection with MPV based upon the manifestations reported in the published literature (6, 7). In our series of patients, elevated white blood cells was noticed in two of three patients, which confirms other comorbid infectious condition rather than COVID-19 that is not associated with WBCs rise in most cases (8). The estimated favorable outcomes are consistent with the findings of our previous report of 4080 MPV patients, where no mortality or intensive care unit admissions were estimated (6). In another report, the estimated case-fatality rate of MPV in non-endemic regions is 0.01% (9). The length of hospital stay was also not long among the included patients, ranging between 4 and 9 days. Besides, supportive management seems to be sufficient for these patients due to the mild course of the disease. Therefore, it can be suggested –until now- that MPV infection, whether alone or in combination with COVID-19 does not induce severe patient’s outcomes. However, it might still be too early to establish solid evidence about the exact cause-effect association between SARS-CoV-2 and MPV co-infection and patient’s outcomes because of the current low sample size. Accordingly, future relevant investigations, estimating the risk ratio of this association are needed to formulate definite evidence.
Another important aspect to consider is the overlapping of the clinical manifestations between the two infections since most MPV patients present with fever which is also common among COVID-19 patients. Although rash might significantly distinguish the two infections, some MPV patients might suffer from atypical undetectable lesions and others might suffer from associated rash-causing illnesses (5), making it difficult to establish a proper differential diagnosis. However, the current MPV outbreak characteristically spreads among men who have sex with men. Accordingly, a history of such sexual contact, together with laboratory-detecting MPV, might provide a sufficient differential diagnosis. Therefore, healthcare physicians should be aware of the best practices to establish a differential diagnosis and have adequate knowledge about the characteristics of MPV. Awareness campaigns are essential in this context since the disease, despite re-emerging, is novel in some countries and hard to identify by many healthcare providers (5).
Early detection of cases might also another factor responsible for the reduced severity of co-infection. Therefore, establishing an early proper diagnosis and detection of infections is vital in curbing the spread of these diseases. Moreover, inaugurating national surveillance programs targeting the most impacted populations and populations at risk of catching the infection is also important. Finally, one patient received COVID-19 vaccination, which might also be protective and responsible for the mild outcomes. However, one patient did not receive the vaccine and still had favorable outcomes, and no information was available for the other, indicating the need for future relevant investigations.
AE-Q was responsible for the idea and the study design. All authors extracted the data and shared in the writing of the full text and approval of final version before submission.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. El-Qushayri AE, Kamel AMA, Reda A, Ghozy S. Does dengue and COVID-19 co-infection have worse outcomes? A systematic review of current evidence. Rev Med Virol (2022) 32(5):e2339.
2. Størdal K, Ruiz PL, Greve-Isdahl M, Surén P, Knudsen PK, Gulseth HL, et al. Risk factors for SARS-CoV-2 infection and hospitalisation in children and adolescents in Norway: A nationwide population-based study. BMJ Open (2022) 12(3):e056549.
3. Mertoglu C, Huyut MT, Arslan Y, Ceylan Y, Coban TA. How do routine laboratory tests change in coronavirus disease 2019? Scand J Clin Lab Invest (2021) 81(1):24–33.
4. Sah R, Mohanty A, Abdelaal A, Reda A, Rodriguez-Morales AJ, Henao-Martinez AF. First monkeypox deaths outside Africa: no room for complacency. Ther Adv Infect Disease (2022) 9:20499361221124027.
5. Ali MR, Hasan MA, Rahman MS, Billah M, Karmakar S, Shimu AS, et al. Clinical manifestations and socio-demographic status of COVID-19 patients during the second-wave of pandemic: A Bangladeshi experience. J infect Public Health (2021) 14(10):1367–74.
6. Knopp B, Weiss H, Goldstein E, Parmar J. Co-Infection of COVID-19 and monkeypox: A case report from Florida, USA, 2022. Curr Res Emerg Med (2022) 2:1041.
7. Nolasco S, Vitale F, Geremia A, Tramuto F, Maida CM, Sciuto A, et al. First case of monkeypox virus, SARS-CoV-2 and HIV co-infection. J Infect.
8. Vives A, Vantman D, Rocco M, Muñoz CA, Alonso-Tarres C, Castañe ER, et al. Coinfection of monkeypox, COVID-19 and syphilis in a PrEP using MSM: A case report from Barcelona. (2022).
Keywords: COVID19, monkeypox, coinfection - disease, SARS- CoV2, infection
Citation: El-Qushayri AE, Reda A and Shah J (2022) COVID-19 and monkeypox co-infection: A rapid systematic review. Front. Immunol. 13:1094346. doi: 10.3389/fimmu.2022.1094346
Received: 10 November 2022; Accepted: 28 November 2022;
Published: 14 December 2022.
Edited by:
Pushpendra Singh, Johns Hopkins Medicine, United StatesReviewed by:
Baolin Liao, Guangzhou Medical University, ChinaCopyright © 2022 El-Qushayri, Reda and Shah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaffer Shah, amFmZmVyLnNoYWhAa2F0ZWIuZWR1LmFm
†These authors have contributed equally to this work
‡ORCID: Amr Ehab El-Qushayri, orcid.org/0000-0002-0967-797X
Abdullah Reda, orcid.org/0000-0002-2180-0029
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.