
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol. , 06 January 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1089621
This article is part of the Research Topic Novel Insights into the Pathology of Rheumatoid Arthritis: Emerging Role of Macrophage & T Cell Immunity View all 6 articles
 Zongpan Li1,2
Zongpan Li1,2 Xue-Qiang Wang1,2*
Xue-Qiang Wang1,2*Rheumatoid arthritis (RA) is a common systematic, chronic inflammatory, autoimmune, and polyarticular disease, causing a range of clinical manifestations, including joint swelling, redness, pain, stiffness, fatigue, decreased quality of life, progressive disability, cardiovascular problems, and other comorbidities. Strong evidence has shown that exercise is effective for RA treatment in various clinical domains. Exercise training for relatively longer periods (e.g., ≥ 12 weeks) can decrease disease activity of RA. However, the mechanism underlying the effectiveness of exercise in reducing RA disease activity remains unclear. This review first summarizes and highlights the effectiveness of exercise in RA treatment. Then, we integrate current evidence and propose biological mechanisms responsible for the potential effects of exercise on immune cells and immunity, inflammatory response, matrix metalloproteinases, oxidative stress, and epigenetic regulation. However, a large body of evidence was obtained from the non-RA populations. Future studies are needed to further examine the proposed biological mechanisms responsible for the effectiveness of exercise in decreasing disease activity in RA populations. Such knowledge will contribute to the basic science and strengthen the scientific basis of the prescription of exercise therapy for RA in the clinical routine.
Rheumatoid arthritis (RA) is a type of systematic, chronic inflammatory, autoimmune, and polyarticular disease that causes a range of clinical manifestations, including joint swelling, redness, pain, stiffness, fatigue, decreased quality of life, progressive disability, cardiovascular problems, and other comorbidities (1–3). RA affects 0.5%–1.0% of adults, with an annual incident rate of 5–50/100,000 person-years. The prevalence of RA in women is higher than that in men and increases with age (4–7). RA ranks 42nd among 291 conditions causing disability globally, accounting for 0.49% of the total years of living with disability (8). With the growing population and aging, the overall burden of RA, estimated by disability-adjusted life years, increased from 3.3 million in 1990 to 4.8 million in 2010 (9). Aside from the high disease burden, RA has substantial economic impact. The total average medical costs for individual RA patient ranged from US$ 5720 to US$ 5822, accounting for 8%–24% of the total medial costs, 8%–21% of physician visits, and 17%–88% of in-patient stays (10). In addition, the average number of days of absences due to RA ranges from 2.7 days/year to 30 days/year (11, 12).
Current practice involves the usage of disease-modifying drugs, and biological agents can substantially improve disease activity and minimize structural damage (13, 14). However, challenges in the current practice of RA management should be considered. Some patients remain difficult to treat or can barely achieve the targeted clinical remissions or low disease activity (15). Nonpharmacological treatments, such as exercise therapy, are promising approaches for symptom control and daily function improvement and widely used for patients with RA (16). Moreover, exercise intervention can effectively improve cardiorespiratory fitness, reduce the risk of commensurate cardiovascular disease, and decrease disease activity and severity in patients with RA (17). Thus, physical exercise therapy, as a cost-effective approach, in conjunction with drug therapy has been recommended by the European Alliance of Associations for Rheumatology (EULAR) in 2018 (18).
The clinical effect of exercise on RA has been extensively studied, and the results have been well synthesized by several reviews published from 1998 to 2022 (19–29). An expert review from Metsios et al. discussed the physiological mechanisms by which exercise alleviates inflammation, psychologic health, and cardiovascular risk in patients with RA and provided detailed description on how to incorporate exercises into RA management (30). Moreover, a systematic review from Sveaas et al. reported that high evidence supporting exercises are beneficial for reducing RA disease activity (31). However, to the best of our knowledge, the possible biological mechanisms of how exercise can decrease the RA disease activity have not been comprehensively reviewed. Such information would be essential for understanding the basic science, which can promote the administration of exercises in the routine management of RA.
To summarize the evidence regarding the clinical effect of exercise on RA, we conducted a literature search using the keywords (exercise, physical activity, clinical effect, and rheumatoid arthritis) in PubMed and Google scholar to identify related individual studies and review articles. As there are overlaps between the individual studies and review articles and some reviews have a specific focus (e.g., a certain type of exercise or clinical domain) (24, 29, 32, 33), we chose to review the individual original studies and provide an overall summary of the clinical effect of exercise for patients with RA (Table 1). A total of 30 related studies published between 1985 and 2019 were identified and reviewed, of which 27 were randomized controlled trials (RCTs (34–42, 44–59, 61, 62), 2 were non-RCTs (17, 60), and 1 was before-after trial (43).
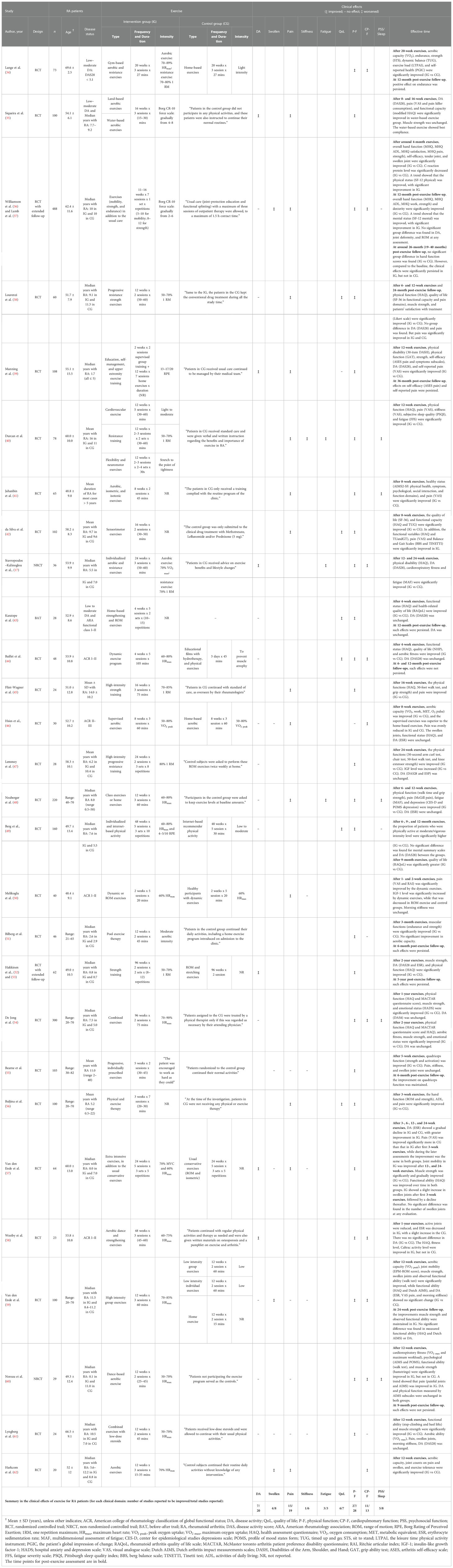
Table 1 Characteristics of Included Studies.
Exercise interventions are effective in improving physical ability (17, 34–45, 47–49, 51–61), alleviating pain (35–42, 45, 46, 48, 50, 56, 57, 62), and improving aerobic function (17, 34, 36, 37, 44, 46, 54, 58–60, 62) in patients with RA. In addition, exercise can be effective in improving quality of life (38, 42–44, 49, 56), mental health or sleep status (40, 41, 48, 54, 60), and fatigue (17, 40, 48) and does not aggravate disease activity (17, 35–39, 43, 44, 46–49, 52–54, 57–61) or severity of some conditions, including swollen joints (36, 37, 46, 55, 57, 59, 61, 62) and joint stiffness (40, 50, 55, 57, 59, 61). Exercise training for relatively longer periods can decrease disease activity or clinical severity (i.e., 12–96 weeks) (17, 35–37, 39, 40, 52, 53, 57, 58). The duration of an effective exercise ranges from 2 weeks to 96 weeks, suggesting even short-term exercises can be clinically beneficial for patients with RA. For safety considerations, most exercise protocols utilize moderate intensities for strengthening (i.e., 50%–70% one repetition maximum: 1 RM) and aerobic training (i.e., 50%–70% maximum heart rate: HRmax or peak oxygen uptake: VO2 max). However, several studies have shown that high-intensity strengthening (i.e., 1 RM ≥ 70%) and aerobic (i.e., HRmax or VO2 max ≥ 70%) exercises are effective for patients with RA, and no exercise-related adverse events have been reported (17, 34, 45, 47, 54, 59, 62). Hence, exercises with moderate-to-high intensities are clinically effective and safe for patients with RA. Exercise therapies seem effective and safe for patients with various stages of RA (i.e., duration 0.5–50 years). More importantly, exercises can effectively promote clinical remission in patients with relatively early RA stages (i.e., duration ≤ 5 years (39, 51–53). Hence, exercise therapies are safe and cost-effective approaches and provide a “window of opportunity” for the early management of RA in first-line treatment (63).
In summary, exercise is effective in alleviating pain, improving physical ability, aerobic function, quality of life, mental health, and sleep status and reducing fatigue in patients with RA. Exercise training for relatively longer periods is effective in reducing disease activity.
Exercise enables a range of biological responses, including the immune systems (64), inflammation (65), matrix metalloproteinase (MMP) (66), oxidative stress (67), and epigenetic adaptation (68). Exercise may reduce the RA disease activity from the following biological aspects: immune cells and immunity, inflammatory response and inflammatory factors, MMP, oxidative stress, and epigenetic expression (Figure 1).
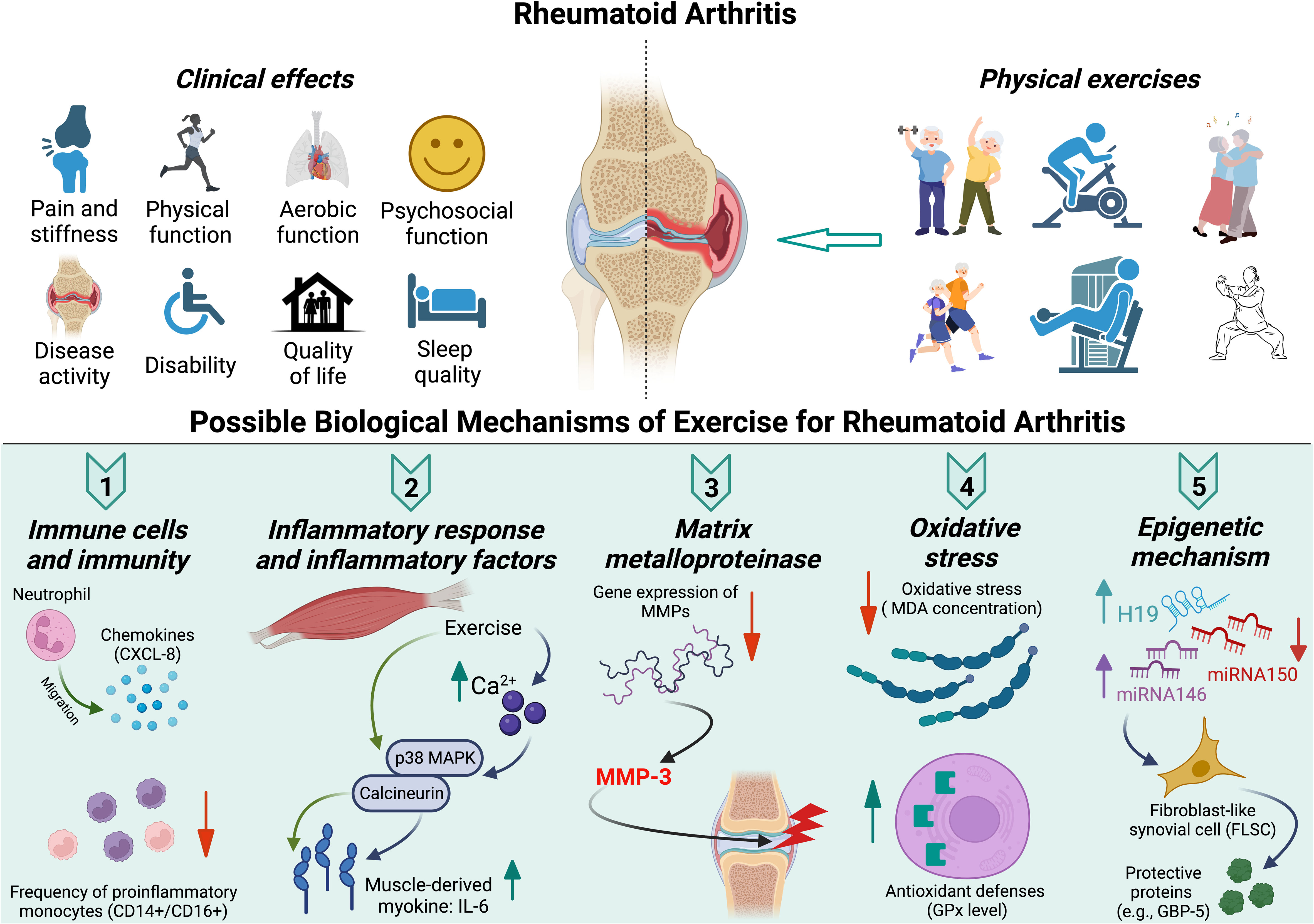
Figure 1 Clinical effects and possible biological mechanisms of exercise for rheumatoid arthritis.
RA is known as a chronic autoimmune disease, with a maladaptive tissue repair process elicited by multiple types of immune cells and malfunction of signaling networks (69). Exercise can profoundly affect the immune system, and causes regulation of immune functions (64), which may reduce the RA disease activity. A single bout of brief dynamic exercise (several minutes) causes an increase in the leukocyte count to 2 to 3 times, whereas prolonged exercise (0.5–3 hours) may increase the count of leukocytes up to fivefold (70, 71). Although the increase of leukocyte count is a common indicator of infection/inflammation, the increase can be returned to the pre-exercise level within 6–24 hours after cessation of the exercise (64). Particularly after endurance exercises, the lymphocyte count in blood would be falling 30–50% below pre-exercise level, reaching the clinically low level (i.e., < 1.0 x 109/L) (64, 70, 71). In addition, the neutrophils and lymphocytes can be predominantly mobilized by exercise (70, 71), and the exercise-mobilized cells have increased effector/cytotoxic functions (64).
Growing evidence has shown that exercise and habitual physical activity enhance the immune function of adaptive and innate cells in healthy adults (70, 72). Several studies have examined the effect of exercise on immune response in patients with RA. One study investigated the effect of an 8-week bicycle exercise on immune response in patients with RA and observed temporary increase in lymphoproliferative response during the acute phase of the exercise and no significant changes in the levels of blood mononuclear cell populations in the post-exercise resting state (73). Another study assessed immune responses to exercise in patients with RA and found no changes in lymphocyte proliferation and natural killer cells, suggesting that exercise does not enhance primary cell functions in RA (74). A more recent study that examined the effects of exercise training on immune function in stable patients with RA showed that the neutrophil migration toward chemokines (CXCL-8) was promoted and the frequency of proinflammatory monocytes (CD14+/CD16+) in the circulation was reduced after exercise (75). As RA is characterized by the dysfunctions of peripheral blood neutrophil migration and increased frequency of proinflammatory monocytes (69, 76), exercise may reduce RA disease activity by improving innate immune functions from the two above-mentioned aspects.
Once immune cells detect an infection or tissue injury, inflammation is triggered by the innate immune system (69). Certain inflammatory cytokines (e.g., interleukin: IL-6; and tumor necrosis factor alpha: TNF-α) are related to the pathogenesis and progression of RA (77). Clinically, inflammatory markers (i.e., c-reactive protein: CRP) and erythrocyte sedimentation rate (ESR) are routinely used in detecting and monitoring inflammation. In addition, ESR has been commonly used as a component in the calculation of disease activity (e.g., DA28-ESR) (78, 79). Evidence from RCTs has shown that exercise can effectively decrease inflammation/disease activity (i.e., exercise-induced decrease in ERS) in patients with RA (52, 57, 58). However, the biological mechanism of such effects remains unclear.
Although IL-6 is commonly viewed as a proinflammatory cytokine, accumulating evidence has shown that the muscle-derived IL-6, known as a type of myokine, has anti-inflammatory functions (80). Different from the signaling pathway of the expression of IL-6 in macrophages during sepsis (i.e., dependent upon the activation of NF-κB), the contraction of the skeletal muscle causes an increased cytosolic Ca2+ and increased activation of p38 MAPK/calcineurin, which facilitates the production of IL-6 but not of TNF (81). IL-6 is the first cytokine released into the blood during exercise (82). In general, inflammatory cytokine level decreases within a few hours after an exercise (83, 84). However, evidence of the acute effect of exercise on inflammatory response in patients with RA is inconsistent (85). Two observational studies examined the acute effect of a single-session exercise on inflammatory cytokine (e.g., IL-6) in patients with RA; one of the studies found no significant change in IL-6 (86), whereas the other observed IL-6 level sharply increased in the first one hour, then gradually decreased, and returned to pre-exercise level in 24 hours (87). Future studies are needed to clarify the role of muscle-derived IL-6 in the inflammatory response during exercise, and its potential anti-inflammatory function in RA populations.
Matrix metalloproteinase (MMP) constitutes a large group of zinc-dependent proteases that degrade the components of the extracellular matrix, including collagen, gelatin, casein, and elastin. Exercise may regulate MMP level by affecting their tissue inhibitor of metalloproteinase (TIMPs), transforming growth factor-β (TGF- β), or RNA expression of MMPs (88–90). Evidence shows that physical exercise training is effective in reducing MMP level in healthy men (91), sedentary women (92), individuals with metabolic syndrome (93), patients with coronary artery disease (94), patients with diabetes (95, 96), patients with multiple sclerosis (97), and female patients with postmenopausal osteoporosis (98). Overall, physical exercise can effectively reduce MMP level in different populations.
However, evidence regarding the effectiveness of exercise on MMP reduction in patients with RA is limited. Wang et al. obtained knee synovial tissues from patients with RA who underwent total knee replacement to examine whether mechanical stretching regulates MMP secretion; they found that mechanical stretching induced significant reduction in the messenger RNA expression levels of MMP-1 and MMP-13 (88). To the best of our knowledge, no in vivo study has explored the effectiveness of exercise in reducing MMP level in patients with RA. MMP-3 is produced in the joints, and it aggravates inflammation by activating a range of pro-MMPs and cleaving extracellular matrix components (99). Elevated serum MMP-3 level is positively associated with inflammatory mediators and the disease activity of RA (100–103) and is a crucial outcome for early RA (101–103). Thus, MMP-3 has been regarded as a reliable marker for disease activity, predictability of disease outcome, radiological monitoring, and therapeutic response for RA (104). Hence, it is important for future studies to examine the exercise-induced change in MMP-3 in RA patients and its potential role in explaining the biological mechanism of exercise-induced reduction in RA disease activity.
In RA, particularly at the early stage, oxidative stress may initiate and perpetuate the local and systemic inflammation process (105). Oxidative stress has detrimental effects on the structures and functions of cellular proteins and proteoglycans, via different processes (i.e., oxidation and nitrosylation) (106). The accumulated oxidized cellular components and damaged products may aggravate the synovial inflammation; and the damaged contents caused by oxidative stress can also be released into the extracellular spaces and increase cellular death (106).
Oxidative stress is characterized as elevated intracellular levels of reactive oxygen species (ROS), which can be indirectly measured by lipid peroxidation (e.g., malondialdehyde: MDA), protein oxidation or nitration (e.g., protein carbonyl), or DNA/RNA damage (e.g., 8-hydroxydeoxyguanosine: 8-oxo-dG) (107). Exercise-induced metabolic challenges result in elevated generation of ROS, and such exercise-related changes in the redox milieu are modulated by several factors of mitochondrial biogenesis (e.g., PGC-1α, mitogen-activated protein kinase, and SIRT1) (108). Evidence from animal and human studies suggests that exercise can effectively reduce oxidative stress and improve antioxidant defense. Findings from animal studies have shown that high-intensity aerobic exercise can effectively reduce oxidative stress (reduces MDA concentration) and improve antioxidant defenses (increases GPx) in rats (109, 110). Similar results have been obtained by studies on the effectiveness of physical exercise on oxidative stress (reduced rate and concentration of MDA; decreased 8-oxo-dG) and antioxidant defense system (increased GPx) in humans with or without diseases (111–114).
However, inconsistent results can be seen in RA populations. Wadley et al. reported that a single bout of moderate-intensity exercise increased the oxidative stress (increased protein carbonyls and nitric oxide metabolites) in RA patients, while the following 3-month exercise significantly decreased the RA disease activity, but without significant change in oxidative stress (115). In contrast, Tuna et al. found that the 30-minute aerobic exercise caused a significant reduction in MDA concentration immediately and 24 hours after the exercise in the RA group (116). It is important for future studies to further examine the effect of exercise on oxidative stress and antioxidant defenses in RA populations, and the related biological and molecular mechanisms of exercise, oxidative stress, and the resultant reduction in RA disease activity.
A range of aberrantly expressed noncoding RNAs (miRNA, lncRNA, and circRNA) were observed in RA. For instance, the expression levels of miRNA146a/b and H19 (lncRNA) are upregulated (117–119), but the miRNA-150-5p expression is downregulated in RA (120). Regular exercise induces genome-wide epigenetic modifications in skeletal muscles and adipose tissues in the human body, which are linked with altered expression of mRNA (121, 122). Such exercise-induced alteration in DNA methylation and mRNA expression are believed to improve the metabolic phenotypes and decrease the risk of disease (68).
Evidence has shown the effectiveness of exercise in the regulation of noncoding RNAs (123–125). Four studies reported that physical exercise downgraded the expression of miRNA146 in trained males (126), active males (127), amateur basketball players (128), and patients with chronic kidney diseases (129). Findings from an animal study suggested that a 4-week moderate endurance exercise reduced the expression of H19 in the hearts of rats with myocardial infarction (123). Van Craenenbroeck et al. reported that miRNA150 expression was upregulated after 10 minutes of endurance aerobic exercise in people with chronic kidney diseases (129). Despite these findings from non-RA populations, the effectiveness of exercise in regulating noncoding RNA expression in patients with RA remains unexplored.
Noncoding RNAs, including microRNAs (miRNAs), long noncoding RNAs (lncRNAs), and circular RNAs (circRNAs), play crucial roles in the regulation of inflammation, autoimmunity, and activation, differentiation, and polarization of immune cells (130). Epigenetic disorders can activate rheumatoid arthritis synovial fibroblasts (RASFs) (131), which promote inflammation and joint destruction in RA (132). In non-inflammatory joints of healthy individuals, normal SFs are differentiated from mesenchymal stromal/stem cells under normal genetic regulation. However, aberrant epigenetic alterations would promote the activation of SFs in inflammatory joints of patients with RA (131). A recent study from Haque et al. reported that in response to cytokine stimulation, the guanylate binding protein 5 (GBP-5) from RASFs is a potential target to restore cellular homeostasis, inflammation, and tissue destruction in RA (133).
In summary, future studies are needed to examine the effect of exercise on noncoding RNA expression in RA populations. It is also important to explore the potential role of epigenetic regulation in the biological mechanism of exercise for the reduction of RA disease activity.
The clinical effectiveness of exercise for RA treatment has been extensively studied. Substantial evidence has shown that exercise therapies of different types, durations, and intensities can be clinically effective for RA. More importantly, exercise for relatively longer periods can decrease the RA disease activity. This review discusses the possible biological mechanism of exercise for reducing RA disease activity from the following aspects: 1) immunity; 2) inflammatory response; 3) MMP; 4) oxidative stress; and 5) epigenetic mechanism. However, the related evidence is mainly based on evidence from non-RA populations. This may highlight the urgency for future studies to further examine the proposed biological mechanisms in RA populations.
Based on current evidence, the following directions regarding the exercise for reducing RA disease activity are proposed for further investigation in RA populations: 1) exercise may cause neutrophil migration toward chemokines (e.g., CXCL-8) and reduce the frequency of proinflammatory monocytes (e.g., CD14+/CD16+) in the circulation; 2) exercise may promote the production of muscle-derived myokine (IL-6), which may have anti-inflammatory functions; 3) exercise may induce reduction in the messenger RNA expression of MMPs(e.g., MMP-3); 4) exercise may reduce oxidative stress (reducesMDA concentration) and improve antioxidant defenses(increases GPx level); and 5) exercise may downregulate the expression of miRNA146 and H19 but upregulate miRNA150expression, which may relate to the production of protectiveproteins (e.g., GBP-5) for decreasing RA disease activity.
ZL and X-QW carried out the literature search, reviewed all the included articles, and drafted and edited the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by grants from the Shanghai Key Lab of Human Performance (Shanghai University of Sport) (11DZ2261100); the Shanghai Frontiers Science Research Base of Exercise and Metabolic Health; the Talent Development Fund of Shanghai Municipal (2021081); and the Shanghai Clinical Research Center for Rehabilitation Medicine (21MC1930200).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet (2010) 376:1094–108. doi: 10.1016/S0140-6736(10)60826-4
2. Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol (1998) 27 Suppl 1:S18–24. doi: 10.1016/s0720-048x(98)00038-2
3. Solomon DH, Goodson NJ, Katz JN, Weinblatt ME, Avorn J, Setoguchi S, et al. Patterns of cardiovascular risk in rheumatoid arthritis. Ann Rheum Dis (2006) 65:1608–12. doi: 10.1136/ard.2005.050377
4. Alamanos Y, Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev (2005) 4:130–6. doi: 10.1016/j.autrev.2004.09.002
5. Pedersen JK, Kjær NK, Svendsen AJ, Hørslev-Petersen K. Incidence of rheumatoid arthritis from 1995 to 2001: impact of ascertainment from multiple sources. Rheumatol Int (2009) 29:411–5. doi: 10.1007/s00296-008-0713-6
6. Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising?: results from Olmsted county, Minnesota, 1955-2007. Arthritis Rheum (2010) 62:1576–82. doi: 10.1002/art.27425
7. Carbonell J, Cobo T, Balsa A, Descalzo M, Carmona L, Group* SS. The incidence of rheumatoid arthritis in Spain: results from a nationwide primary care registry. Rheumatol (Oxford) (2008) 47:1088–92. doi: 10.1093/rheumatology/ken205
8. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet (2012) 380:2197–223. doi: 10.1016/S0140-6736(12)61689-4
9. Cross M, Smith E, Hoy D, Carmona L, Wolfe F, Vos T, et al. The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis (2014) 73:1316–22. doi: 10.1136/annrheumdis-2013-204627
10. Cooper N. Economic burden of rheumatoid arthritis: a systematic review. Rheumatol (Oxford) (2000) 39:28–33. doi: 10.1093/rheumatology/39.1.28
11. Liang MH, Larson M, Thompson M, Eaton H, Mcnamara E, Katz R, et al. Costs and outcomes in rheumatoid arthritis and osteoarthritis. Arthritis Rheum (1984) 27:522–9. doi: 10.1002/art.1780270507
12. Lubeck DP, Spitz PW, Fries JF, Wolfe F, Mitchell DM, Roth SH. A multicenter study of annual health service utilization and costs in rheumatoid arthritis. Arthritis Rheum (1986) 29:488–93. doi: 10.1002/art.1780290405
13. Boers M, van Tuyl L, van den Broek M, Kostense PJ, Allaart CF. Meta-analysis suggests that intensive non-biological combination therapy with step-down prednisolone (COBRA strategy) may also ‘disconnect’disease activity and damage in rheumatoid arthritis. Ann Rheum Dis (2013) 72:406–9. doi: 10.1136/annrheumdis-2012-202333
14. Weinblatt ME. Methotrexate in rheumatoid arthritis: a quarter century of development. Trans Am Clin Climatol Assoc (2013) 124:16–25.
15. Conigliaro P, Triggianese P, De Martino E, Fonti GL, Chimenti MS, Sunzini F, et al. Challenges in the treatment of rheumatoid arthritis. Autoimmun Rev (2019) 18:706–13. doi: 10.1016/j.autrev.2019.05.007
16. Cooney JK, Law R-J, Matschke V, Lemmey AB, Moore JP, Ahmad Y, et al. Benefits of exercise in rheumatoid arthritis. J Aging Res (2011) 2011:2011. doi: 10.4061/2011/681640
17. Stavropoulos-Kalinoglou A, Metsios GS, Van Zanten JJV, Nightingale P, Kitas GD, Koutedakis Y. Individualised aerobic and resistance exercise training improves cardiorespiratory fitness and reduces cardiovascular risk in patients with rheumatoid arthritis. Ann Rheum Dis (2013) 72:1819–25. doi: 10.1136/annrheumdis-2012-202075
18. Weijers JM, Rongen-van Dartel SA, Hoevenaars DM, Rubens M, Hulscher ME, van Riel PL. Implementation of the EULAR cardiovascular risk management guideline in patients with rheumatoid arthritis: Results of a successful collaboration between primary and secondary care. Ann Rheum Dis (2018) 77:480–3. doi: 10.1136/annrheumdis-2017-212392
19. Baillet A, Zeboulon N, Gossec L, Combescure C, Bodin LA, Juvin R, et al. Efficacy of cardiorespiratory aerobic exercise in rheumatoid arthritis: meta-analysis of randomized controlled trials. Arthritis Care Res (Hoboken) (2010) 62:984–92. doi: 10.1002/acr.20146
20. Cairns AP, McVeigh JG. A systematic review of the effects of dynamic exercise in rheumatoid arthritis. Rheumatol Int (2009) 30:147–58. doi: 10.1007/s00296-009-1090-5
21. Van den Ende C, Vliet Vlieland T, Munneke M, Hazes J. Dynamic exercise therapy in rheumatoid arthritis: a systematic review. Br J Rheumatol (1998) 37:677–87. doi: 10.1093/rheumatology/37.6.677
22. Sobue Y, Kojima T, Ito H, Nishida K, Matsushita I, Kaneko Y, et al. Does exercise therapy improve patient-reported outcomes in rheumatoid arthritis? a systematic review and meta-analysis for the update of the 2020 JCR guidelines for the management of rheumatoid arthritis. Mod Rheumatol (2022) 32:96–104. doi: 10.1080/14397595.2021.1886653
23. Hu H, Xu A, Gao C, Wang Z, Wu X. The effect of physical exercise on rheumatoid arthritis: An overview of systematic reviews and meta-analysis. J Adv Nurs (2021) 77:506–22. doi: 10.1111/jan.14574
24. Han A, Judd M, Welch V, Wu T, Tugwell P, Wells GA. Tai chi for treating rheumatoid arthritis. Cochrane Database Syst Rev (2004) 2004:CD004849. doi: 10.1002/14651858.CD004849
25. Lee M, Pittler M, Ernst E. Tai chi for rheumatoid arthritis: systematic review. Rheumatol (Oxford) (2007) 46:1648–51. doi: 10.1093/rheumatology/kem151
26. Sieczkowska SM, Smaira FI, Mazzolani BC, Gualano B, Roschel H, Pecanha T. Efficacy of home-based physical activity interventions in patients with autoimmune rheumatic diseases: a systematic review and meta-analysis. Semin Arthritis Rheum (2021) 51:576–87. doi: 10.1016/j.semarthrit.2021.04.004
27. Wessel J. The effectiveness of hand exercises for persons with rheumatoid arthritis: a systematic review. J Handb Ther (2004) 17:174–80. doi: 10.1197/j.jht.2004.02.006
28. Hammond A, Prior Y. The effectiveness of home hand exercise programmes in rheumatoid arthritis: a systematic review. Br Med Bull (2016) 119:49–62. doi: 10.1093/bmb/ldw024
29. Hurkmans E, van der Giesen FJ, Vlieland TPV, Schoones J, Van den Ende EC. Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis. Cochrane Database Syst Rev (2009) 2009:CD006853. doi: 10.1002/14651858.CD006853.pub2
30. Metsios GS, Stavropoulos-Kalinoglou A, Kitas GD. The role of exercise in the management of rheumatoid arthritis. Expert Rev Clin Immunol (2015) 11:1121–30. doi: 10.1586/1744666X.2015.1067606
31. Sveaas SH, Smedslund G, Hagen KB, Dagfinrud H. Effect of cardiorespiratory and strength exercises on disease activity in patients with inflammatory rheumatic diseases: a systematic review and meta-analysis. Br J Sports Med (2017) 51:1065–72. doi: 10.1136/bjsports-2016-097149
32. Rongen-van Dartel S, Repping-Wuts H, Flendrie M, Bleijenberg G, Metsios G, van Den Hout W, et al. Effect of aerobic exercise training on fatigue in rheumatoid arthritis: a meta-analysis. Arthritis Care Res (Hoboken) (2015) 67:1054–62. doi: 10.1002/acr.22561
33. Salmon VE, Hewlett S, Walsh NE, Kirwan JR, Cramp F. Physical activity interventions for fatigue in rheumatoid arthritis: a systematic review. Phys Ther Rev (2017) 22:12–22. doi: 10.1080/10833196.2016.1277454
34. Lange E, Kucharski D, Svedlund S, Svensson K, Bertholds G, Gjertsson I, et al. Effects of aerobic and resistance exercise in older adults with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res (Hoboken) (2019) 71:61–70. doi: 10.1002/acr.23589
35. Siqueira US, Valente LGO, de Mello MT, Szejnfeld VL, Pinheiro MM. Effectiveness of aquatic exercises in women with rheumatoid arthritis: a randomized, controlled, 16-week intervention–the HydRA trial. Am J Phys Med Rehabil (2017) 96:167–75. doi: 10.1097/PHM.0000000000000564
36. Williamson E, McConkey C, Heine P, Dosanjh S, Williams M, Lamb SE. Hand exercises for patients with rheumatoid arthritis: an extended follow-up of the SARAH randomised controlled trial. BMJ Open (2017) 7:e013121. doi: 10.1136/bmjopen-2016-013121
37. Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, et al. Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet (2015) 385:421–9. doi: 10.1016/S0140-6736(14)60998-3
38. Lourenzi FM, Jones A, Pereira DF, JHCAd S, RNV F, Natour J. Effectiveness of an overall progressive resistance strength program for improving the functional capacity of patients with rheumatoid arthritis: a randomized controlled trial. Clin Rehabil (2017) 31:1482–91. doi: 10.1177/0269215517698732
39. Manning VL, Hurley MV, Scott DL, Coker B, Choy E, Bearne LM. Education, self-management, and upper extremity exercise training in people with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res (Hoboken) (2014) 66:217–27. doi: 10.1002/acr.22102
40. Durcan L, Wilson F, Cunnane G. The effect of exercise on sleep and fatigue in rheumatoid arthritis: a randomized controlled study. J Rheumatol (2014) 41:1966–73. doi: 10.3899/jrheum.131282
41. Jahanbin I, Moghadam MH, Nazarinia MA, Ghodsbin F, Bagheri Z, Ashraf AR. The effect of conditioning exercise on the health status and pain in patients with rheumatoid arthritis: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery (2014) 2:169–76.
42. da Silva KNG, Teixeira L, Imoto AM, Atallah AN, Peccin MS, Trevisani VFM. Effectiveness of sensorimotor training in patients with rheumatoid arthritis: a randomized controlled trial. Rheumatol Int (2013) 33:2269–75. doi: 10.1007/s00296-013-2706-3
43. Göksel Karatepe A, Günaydin R, Türkmen G, Kaya T. Effects of home-based exercise program on the functional status and the quality of life in patients with rheumatoid arthritis: 1-year follow-up study. Rheumatol Int (2011) 31:171–6. doi: 10.1007/s00296-009-1242-7
44. Baillet A, Payraud E, Niderprim V-A, Nissen MJ, Allenet B, Francois P, et al. A dynamic exercise programme to improve patients’ disability in rheumatoid arthritis: a prospective randomized controlled trial. Rheumatol (Oxford) (2009) 48:410–5. doi: 10.1093/rheumatology/ken511
45. Flint-Wagner HG, Lisse J, Lohman TG, Going SB, Guido T, Cussler E, et al. Assessment of a sixteen-week training program on strength, pain, and function in rheumatoid arthritis patients. J Clin Rheumatol (2009) 15:165–71. doi: 10.1097/RHU.0b013e318190f95f
46. Lin-Fen Hsieh M, Shih-Ching Chen M, Chih-Cheng Chuang M. Supervised aerobic exercise is more effective than home aerobic exercise in female Chinese patients with rheumatoid arthritis. J Rehabil Med (2009) 41:332–7. doi: 10.2340/16501977-0330
47. Lemmey AB, Marcora SM, Chester K, Wilson S, Casanova F, Maddison PJ. Effects of high-intensity resistance training in patients with rheumatoid arthritis: A randomized controlled trial. Arthritis Rheum (2009) 61:1726–34. doi: 10.1002/art.24891
48. Neuberger GB, Aaronson LS, Gajewski B, Embretson SE, Cagle PE, Loudon JK, et al. Predictors of exercise and effects of exercise on symptoms, function, aerobic fitness, and disease outcomes of rheumatoid arthritis. Arthritis Rheum (2007) 57:943–52. doi: 10.1002/art.22903
49. Van den Berg M, Ronday H, Peeters A, Le Cessie S, van der Giesen F, Breedveld F, et al. Using internet technology to deliver a home-based physical activity intervention for patients with rheumatoid arthritis: A randomized controlled trial. Arthritis Rheum (2006) 55:935–45. doi: 10.1002/art.22339
50. Melikoglu MA, Karatay S, Senel K, Akcay F. Association between dynamic exercise therapy and IGF-1 and IGFBP-3 concentrations in the patients with rheumatoid arthritis. Rheumatol Int (2006) 26:309–13. doi: 10.1007/s00296-005-0605-y
51. Bilberg A, Ahlmen M, Mannerkorpi K. Moderately intensive exercise in a temperate pool for patients with rheumatoid arthritis: a randomized controlled study. Rheumatol (Oxford) (2005) 44:502–8. doi: 10.1093/rheumatology/keh528
52. Häkkinen A, Sokka T, Kotaniemi A, Hannonen P. A randomized two-year study of the effects of dynamic strength training on muscle strength, disease activity, functional capacity, and bone mineral density in early rheumatoid arthritis. Arthritis Rheum (2001) 44:515–22. doi: 10.1002/1529-0131(200103)44:3<515::AID-ANR98>3.0.CO;2-5
53. Häkkinen A, Sokka T, Hannonen P. A home-based two-year strength training period in early rheumatoid arthritis led to good long-term compliance: a five-year followup. Arthritis Rheum (2004) 51:56–62. doi: 10.1002/art.20088
54. de Jong Z, Munneke M, Zwinderman AH, Kroon HM, Jansen A, Ronday KH, et al. Is a long-term high-intensity exercise program effective and safe in patients with rheumatoid arthritis?: results of a randomized controlled trial. Arthritis Rheum (2003) 48:2415–24. doi: 10.1002/art.11216
55. Bearne L, Scott D, Hurley M. Exercise can reverse quadriceps sensorimotor dysfunction that is associated with rheumatoid arthritis without exacerbating disease activity. Rheumatol (Oxford) (2002) 41:157–66. doi: 10.1093/rheumatology/41.2.157
56. Buljina AI, Taljanovic MS, Avdic DM, Hunter TB. Physical and exercise therapy for treatment of the rheumatoid hand. Arthritis Rheum (2001) 45:392–7. doi: 10.1002/1529-0131(200108)45:4<392::AID-ART353>3.0.CO;2-2
57. Van den Ende C, Breedveld F, Le Cessie S, Dijkmans B, De Mug A, Hazes J. Effect of intensive exercise on patients with active rheumatoid arthritis: a randomised clinical trial. Ann Rheum Dis (2000) 59:615–21. doi: 10.1136/ard.59.8.615
58. Westby MD, Wade JP, Rangno KK, Berkowitz J. A randomized controlled trial to evaluate the effectiveness of an exercise program in women with rheumatoid arthritis taking low dose prednisone. J Rheumatol (2000) 27:1674–80.
59. Van den Ende C, Hazes J, Le Cessie S, Mulder W, Belfor D, Breedveld F, et al. Comparison of high and low intensity training in well controlled rheumatoid arthritis. results of a randomised clinical trial. Ann Rheum Dis (1996) 55:798–805. doi: 10.1136/ard.55.11.798
60. Noreau L, Martineau H, Roy L, Belzile M. Effects of a modified dance-based exercise on cardiorespiratory fitness, psychological state and health status of persons with rheumatoid arthritis. Am J Phys Med Rehabil (1995) 74:19–27. doi: 10.1097/00002060-199501000-00004
61. Lyngberg KK, Harreby M, Bentzen H, Frost B, Danneskiold-Samsøe B. Elderly rheumatoid arthritis patients on steroid treatment tolerate physical training without an increase in disease activity. Arch Phys Med Rehabil (1994) 75:1189–95. doi: 10.1016/0003-9993(94)90003-5
62. Harkcom TM, Lampman RM, Banwell BF, Castor CW. Therapeutic value of graded aerobic exercise training in rheumatoid arthritis. Arthritis Rheum (1985) 28:32–9. doi: 10.1002/art.1780280106
63. Burmester GR, Pope JE. Novel treatment strategies in rheumatoid arthritis. Lancet (2017) 389:2338–48. doi: 10.1016/S0140-6736(17)31491-5
64. Simpson RJ, Kunz H, Agha N, Graff R. Exercise and the regulation of immune functions. Prog Mol Biol Transl Sci (2015) 135:355–80. doi: 10.1016/bs.pmbts.2015.08.001
65. Metsios GS, Moe RH, Kitas GD. Exercise and inflammation. Best Pract Res Clin Rheumatol (2020) 34:101504. doi: 10.1016/j.berh.2020.101504
66. da Cunha Nascimento D, de Cassia Marqueti Durigan R, Tibana RA, Durigan JLQ, Navalta JW, Prestes J. The response of matrix metalloproteinase-9 and -2 to exercise. Sports Med (2015) 45:269–78. doi: 10.1007/s40279-014-0265-8
67. Radak Z, Chung HY, Koltai E, Taylor AW, Goto S. Exercise, oxidative stress and hormesis. Ageing Res Rev (2008) 7:34–42. doi: 10.1016/j.arr.2007.04.004
68. Ling C, Rönn T. Epigenetic adaptation to regular exercise in humans. Drug Discovery Today (2014) 19:1015–8. doi: 10.1016/j.drudis.2014.03.006
69. Weyand CM, Goronzy JJ. The immunology of rheumatoid arthritis. Nat Immunol (2021) 22:10–8. doi: 10.1038/s41590-020-00816-x
70. Walsh NP, Gleeson M, Shephard RJ, Gleeson M, Woods JA, Bishop N, et al. Position statement part one: immune function and exercise. Exerc Immunol Rev (2011) 17:6–63.
71. Simpson RJ. The effects of exercise on blood leukocyte numbers. In: Gleeson M, Bishop NC, Walsh NP, editors. Exercise immunology. Oxford, UK, New York, USA: Routledge (2013). p. 64–105.
72. Nieman DC, Henson D, Gusewitch G, Warren BJ, Dotson RC, Butterworth DE, et al. Physical activity and immune function in elderly women. Med Sci Sports Exerc (1993) 25:823–31. doi: 10.1249/00005768-199307000-00011
73. Baslund B, Lyngberg K, Andersen V, Halkjaer Kristensen J, Hansen M, Klokker M, et al. Effect of 8 wk of bicycle training on the immune system of patients with rheumatoid arthritis. J Appl Physiol (1985) (1993) 75:1691–5. doi: 10.1152/jappl.1993.75.4.1691
74. Rall LC, Roubenoff R, Cannon JG, Abad LW, Dinarello CA, Meydani SN. Effects of progressive resistance training on immune response in aging and chronic inflammation. Med Sci Sports Exerc (1996) 28:1356–65. doi: 10.1097/00005768-199611000-00003
75. Bartlett DB, Willis LH, Slentz CA, Hoselton A, Kelly L, Huebner JL, et al. Ten weeks of high-intensity interval walk training is associated with reduced disease activity and improved innate immune function in older adults with rheumatoid arthritis: a pilot study. Arthritis Res Ther (2018) 20:1–15. doi: 10.1186/s13075-018-1624-x
76. Wright HL, Moots RJ, Bucknall RC, Edwards SW. Neutrophil function in inflammation and inflammatory diseases. Rheumatol (Oxford) (2010) 49:1618–31. doi: 10.1093/rheumatology/keq045
77. McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol (2007) 7:429–42. doi: 10.1038/nri2094
78. Inoue E, Yamanaka H, Hara M, Tomatsu T, Kamatani N. Comparison of disease activity score (DAS) 28-erythrocyte sedimentation rate and DAS28-c-reactive protein threshold values. Ann Rheum Dis (2007) 66:407–9. doi: 10.1136/ard.2006.054205
79. Van der Heijde D, van't Hof MA, Van Riel P, Theunisse L, Lubberts EW, van Leeuwen MA, et al. Judging disease activity in clinical practice in rheumatoid arthritis: first step in the development of a disease activity score. Ann Rheum Dis (1990) 49:916–20. doi: 10.1136/ard.49.11.916
80. Muñoz-Cánoves P, Scheele C, Pedersen BK, Serrano AL. Interleukin-6 myokine signaling in skeletal muscle: a double-edged sword? FEBS J (2013) 280:4131–48. doi: 10.1111/febs.12338
81. Benatti FB, Pedersen BK. Exercise as an anti-inflammatory therapy for rheumatic diseases–myokine regulation. Nat Rev Rheumatol (2015) 11:86–97. doi: 10.1038/nrrheum.2014.193
82. Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev (2008) 88:1379–406. doi: 10.1152/physrev.90100.2007
83. Ostrowski K, Rohde T, Asp S, Schjerling P, Pedersen BK. Pro-and anti-inflammatory cytokine balance in strenuous exercise in humans. J Physiol (1999) 515:287–91. doi: 10.1111/j.1469-7793.1999.287ad.x
84. Febbraio MA, Pedersen BK. Muscle-derived interleukin-6: mechanisms for activation and possible biological roles. FASEB J (2002) 16:1335–47. doi: 10.1096/fj.01-0876rev
85. Balchin C, Tan AL, Golding J, Bissell L-A, Wilson OJ, McKenna J, et al. Acute effects of exercise on pain symptoms, clinical inflammatory markers and inflammatory cytokines in people with rheumatoid arthritis: a systematic literature review. Ther Adv Musculoskelet Dis (2022) 14:1759720X221114104. doi: 10.1177/1759720X221114104
86. Knudsen LS, Christensen IJ, Lottenburger T, Svendsen MN, Nielsen HJ, Nielsen L, et al. Pre-analytical and biological variability in circulating interleukin 6 in healthy subjects and patients with rheumatoid arthritis. Biomarkers (2008) 13:59–78. doi: 10.1080/13547500701615017
87. Pereira Nunes Pinto AC, Natour J, De Moura Castro CH, Eloi M, Lombardi Junior I. Acute effect of a resistance exercise session on markers of cartilage breakdown and inflammation in women with rheumatoid arthritis. Int J Rheum Dis (2017) 20:1704–13. doi: 10.1111/1756-185X.13204
88. Wang P, Yang L, You X, Singh GK, Zhang L, Yan Y, et al. Mechanical stretch regulates the expression of matrix metalloproteinase in rheumatoid arthritis fibroblast-like synoviocytes. Connect Tissue Res (2009) 50:98–109. doi: 10.1080/03008200802348625
89. Kwak HB, Kim JH, Joshi K, Yeh A, Martinez DA, Lawler JM. Exercise training reduces fibrosis and matrix metalloproteinase dysregulation in the aging rat heart. FASEB J (2011) 25:1106–17. doi: 10.1096/fj.10-172924
90. Koskinen SO, Heinemeier KM, Olesen JL, Langberg H, Kjaer M. Physical exercise can influence local levels of matrix metalloproteinases and their inhibitors in tendon-related connective tissue. J Appl Physiol (1985) (2004) 96:861–4. doi: 10.1152/japplphysiol.00489.2003
91. Urso ML, Pierce JR, Alemany JA, Harman EA, Nindl BC. Effects of exercise training on the matrix metalloprotease response to acute exercise. Eur J Appl Physiol (2009) 106:655–63. doi: 10.1007/s00421-009-1063-0
92. Fiotti N, Deiuri E, Altamura N, Moretti M, Toigo G, Giansante C. Body composition and muscular strength changes after moderate activity: association with matrix metalloproteinase polymorphisms. Arch Gerontol Geriatr (2009) 49 Suppl 1:83–94. doi: 10.1016/j.archger.2009.09.016
93. Roberts CK, Won D, Pruthi S, Kurtovic S, Sindhu RK, Vaziri ND, et al. Effect of a short-term diet and exercise intervention on oxidative stress, inflammation, MMP-9, and monocyte chemotactic activity in men with metabolic syndrome factors. J Appl Physiol (1985) (2006) 100:1657–65. doi: 10.1152/japplphysiol.01292.2005
94. Niessner A, Richter B, Penka M, Steiner S, Strasser B, Ziegler S, et al. Endurance training reduces circulating inflammatory markers in persons at risk of coronary events: impact on plaque stabilization? Atherosclerosis (2006) 186:160–5. doi: 10.1016/j.atherosclerosis.2005.06.047
95. Kadoglou N, Vrabas I, Sailer N, Kapelouzou A, Fotiadis G, Noussios G, et al. Exercise ameliorates serum MMP-9 and TIMP-2 levels in patients with type 2 diabetes. Diabetes Metab (2010) 36:144–51. doi: 10.1016/j.diabet.2009.11.004
96. Lucotti P, Monti LD, Setola E, Galluccio E, Gatti R, Bosi E, et al. Aerobic and resistance training effects compared to aerobic training alone in obese type 2 diabetic patients on diet treatment. Diabetes Res Clin Pract (2011) 94:395–403. doi: 10.1016/j.diabres.2011.08.002
97. Zimmer P, Bloch W, Schenk A, Oberste M, Riedel S, Kool J, et al. High-intensity interval exercise improves cognitive performance and reduces matrix metalloproteinases-2 serum levels in persons with multiple sclerosis: A randomized controlled trial. Mult Scler (2018) 24:1635–44. doi: 10.1177/1352458517728342
98. Filipović T, Gopčević K, Dimitrijević S, Hrković M, Backović A, Lazović M. Effects of 12-week exercise program on enzyme activity of serum matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 in female patients with postmenopausal osteoporosis: A randomized control study. BioMed Res Int (2020) 2020:9758289. doi: 10.1155/2020/9758289
99. Wu JJ, Lark MW, Chun LE, Eyre DR. Sites of stromelysin cleavage in collagen types II, IX, X, and XI of cartilage. J Biol Chem (1991) 266:5625–8. doi: 10.1016/S0021-9258(19)67640-4
100. Shinozaki M, Inoue E, Nakajima A, Hara M, Tomatsu T, Kamatani N, et al. Elevation of serum matrix metalloproteinase-3 as a predictive marker for the long-term disability of rheumatoid arthritis patients in a prospective observational cohort IORRA. Mod Rheumatol (2007) 17:403–8. doi: 10.1007/s10165-007-0608-5
101. Tchetverikov I, Lard L, DeGroot J, Verzijl N, TeKoppele J, Breedveld F, et al. Matrix metalloproteinases-3,-8,-9 as markers of disease activity and joint damage progression in early rheumatoid arthritis. Ann Rheum Dis (2003) 62:1094–9. doi: 10.1136/ard.62.11.1094
102. Posthumus MD, Limburg PC, Westra J, van Leeuwen MA, van Rijswijk MH. Serum matrix metalloproteinase 3 in early rheumatoid arthritis is correlated with disease activity and radiological progression. J Rheumatol (2000) 27:2761–8.
103. Ally MM, Hodkinson B, Meyer PW, Musenge E, Tikly M, Anderson R. Serum matrix metalloproteinase-3 in comparison with acute phase proteins as a marker of disease activity and radiographic damage in early rheumatoid arthritis. Mediators Inflammation (2013) 2013:183653. doi: 10.1155/2013/183653
104. Lerner A, Neidhöfer S, Reuter S, Matthias T. MMP3 is a reliable marker for disease activity, radiological monitoring, disease outcome predictability, and therapeutic response in rheumatoid arthritis. Best Pract Res Clin Rheumatol (2018) 32:550–62. doi: 10.1016/j.berh.2019.01.006
105. Fonseca L, Nunes-Souza V, Goulart MOF, Rabelo LA. Oxidative stress in rheumatoid arthritis: What the future might hold regarding novel biomarkers and add-on therapies. Oxid Med Cell Longev (2019) 2019:7536805. doi: 10.1155/2019/7536805
106. Phull A-R, Nasir B, ul Haq I, Kim SJ. Oxidative stress, consequences and ROS mediated cellular signaling in rheumatoid arthritis. Chem Biol Interact (2018) 281:121–36. doi: 10.1016/j.cbi.2017.12.024
107. Powers SK, Nelson WB, Hudson MB. Exercise-induced oxidative stress in humans: Cause and consequences. Free Radic Biol Med (2011) 51:942–50. doi: 10.1016/j.freeradbiomed.2010.12.009
108. Radak Z, Zhao Z, Koltai E, Ohno H, Atalay M. Oxygen consumption and usage during physical exercise: the balance between oxidative stress and ROS-dependent adaptive signaling. Antioxid Redox Signal (2013) 18:1208–46. doi: 10.1089/ars.2011.4498
109. Gomes MJ, Pagan LU, Lima AR, Reyes DR, Martinez PF, Damatto FC, et al. Effects of aerobic and resistance exercise on cardiac remodelling and skeletal muscle oxidative stress of infarcted rats. J Cell Mol Med (2020) 24:5352–62. doi: 10.1111/jcmm.15191
110. Paes L, Lima D, Matsuura C, de Souza M, Cyrino F, Barbosa C, et al. Effects of moderate and high intensity isocaloric aerobic training upon microvascular reactivity and myocardial oxidative stress in rats. PloS One (2020) 15:e0218228. doi: 10.1371/journal.pone.0218228
111. Franzke B, Schober-Halper B, Hofmann M, Oesen S, Tosevska A, Henriksen T, et al. Age and the effect of exercise, nutrition and cognitive training on oxidative stress–the Vienna active aging study (VAAS), a randomized controlled trial. Free Radic Biol Med (2018) 121:69–77. doi: 10.1016/j.freeradbiomed.2018.04.565
112. Kozakiewicz M, Rowiński R, Kornatowski M, Dąbrowski A, Kędziora-Kornatowska K, Strachecka A. Relation of moderate physical activity to blood markers of oxidative stress and antioxidant defense in the elderly. Oxid Med Cell Longev (2019) 2019:5123628. doi: 10.1155/2019/5123628
113. Lima AH, Correia MA, Soares AH, Farah BQ, Forjaz CL, Silva AS, et al. Acute effects of walking and combined exercise on oxidative stress and vascular function in peripheral artery disease. Clin Physiol Funct Imaging (2018) 38:69–75. doi: 10.1111/cpf.12384
114. Fatouros IG, Jamurtas AZ, Villiotou V, Pouliopoulou S, Fotinakis P, Taxildaris K, et al. Oxidative stress responses in older men during endurance training and detraining. Med Sci Sports Exerc (2004) 36:2065–72. doi: 10.1249/01.mss.0000147632.17450.ff
115. Wadley AJ, van Zanten JJ, Stavropoulos-Kalinoglou A, Metsios GS, Smith JP, Kitas GD, et al. Three months of moderate-intensity exercise reduced plasma 3-nitrotyrosine in rheumatoid arthritis patients. Eur J Appl Physiol (2014) 114:1483–92. doi: 10.1007/s00421-014-2877-y
116. Tuna Z, Duger T, Atalay-Guzel N, Aral A, Basturk B, Haznedaroglu S, et al. Aerobic exercise improves oxidant-antioxidant balance in patients with rheumatoid arthritis. J Phys Ther Sci (2015) 27:1239–42. doi: 10.1589/jpts.27.1239
117. Stuhlmüller B, Kunisch E, Franz J, Martinez-Gamboa L, Hernandez MM, Pruss A, et al. Detection of oncofetal h19 RNA in rheumatoid arthritis synovial tissue. Am J Pathol (2003) 163:901–11. doi: 10.1016/S0002-9440(10)63450-5
118. Yang Z, Wang J, Pan Z, Zhang Y. miR-143-3p regulates cell proliferation and apoptosis by targeting IGF1R and IGFBP5 and regulating the Ras/p38 MAPK signaling pathway in rheumatoid arthritis. Exp Ther Med (2018) 15:3781–90. doi: 10.3892/etm.2018.5907
119. Guo T, Ding H, Jiang H, Bao N, Zhou L, Zhao J. miR-338-5p regulates the viability, proliferation, apoptosis and migration of rheumatoid arthritis fibroblast-like synoviocytes by targeting NFAT5. Cell Physiol Biochem (2018) 49:899–910. doi: 10.1159/000493222
120. Chen Z, Wang H, Xia Y, Yan F, Lu Y. Therapeutic potential of mesenchymal cell–derived miRNA-150-5p–expressing exosomes in rheumatoid arthritis mediated by the modulation of MMP14 and VEGF. J Immunol (2018) 201:2472–82. doi: 10.4049/jimmunol.1800304
121. Rönn T, Volkov P, Davegårdh C, Dayeh T, Hall E, Olsson AH, et al. A six months exercise intervention influences the genome-wide DNA methylation pattern in human adipose tissue. PloS Genet (2013) 9:e1003572. doi: 10.1371/journal.pgen.1003572
122. Nitert MD, Dayeh T, Volkov P, Elgzyri T, Hall E, Nilsson E, et al. Impact of an exercise intervention on DNA methylation in skeletal muscle from first-degree relatives of patients with type 2 diabetes. Diabetes (2012) 61:3322–32. doi: 10.2337/db11-1653
123. Farsangi SJ, Rostamzadeh F, Sheikholeslami M, Jafari E, Karimzadeh M. Modulation of the expression of long non-coding RNAs H19, GAS5, and MIAT by endurance exercise in the hearts of rats with myocardial infarction. Cardiovasc Toxicol (2021) 21:162–8. doi: 10.1007/s12012-020-09607-0
124. Domańska-Senderowska D, Laguette M-JN, Jegier A, Cięszczyk P, September AV, Brzeziańska-Lasota E. MicroRNA profile and adaptive response to exercise training: a review. Int J Sports Med (2019) 40:227–35. doi: 10.1055/a-0824-4813
125. Fernández-Sanjurjo M, de Gonzalo-Calvo D, Fernández-García B, Díez-Robles S, Martínez-Canal Á, Olmedillas H, et al. Circulating microRNA as emerging biomarkers of exercise. Exerc Sport Sci Rev (2018) 46:160–71. doi: 10.1249/JES.0000000000000148
126. Nielsen S, Åkerström T, Rinnov A, Yfanti C, Scheele C, Pedersen BK, et al. The miRNA plasma signature in response to acute aerobic exercise and endurance training. PloS One (2014) 9:e87308. doi: 10.1371/journal.pone.0087308
127. Sawada S, Kon M, Wada S, Ushida T, Suzuki K, Akimoto T. Profiling of circulating microRNAs after a bout of acute resistance exercise in humans. PloS One (2013) 8:e70823. doi: 10.1371/journal.pone.0070823
128. Li Y, Yao M, Zhou Q, Cheng Y, Che L, Xu J, et al. Dynamic regulation of circulating microRNAs during acute exercise and long-term exercise training in basketball athletes. Front Physiol (2018) 9:282. doi: 10.3389/fphys.2018.00282
129. Van Craenenbroeck AH, Ledeganck KJ, Van Ackeren K, Jürgens A, Hoymans VY, Fransen E, et al. Plasma levels of microRNA in chronic kidney disease: patterns in acute and chronic exercise. Am J Physiol Heart Circ Physiol (2015) 309:H2008–16. doi: 10.1152/ajpheart.00346.2015
130. Wang J, Yan S, Yang J, Lu H, Xu D, Wang Z. Non-coding RNAs in rheumatoid arthritis: from bench to bedside. Front Immunol (2020) 10:3129. doi: 10.3389/fimmu.2019.03129
131. Araki Y, Mimura T. The mechanisms underlying chronic inflammation in rheumatoid arthritis from the perspective of the epigenetic landscape. J Immunol Res (2016) 2016:6290682. doi: 10.1155/2016/6290682
132. Mor A, Abramson SB, Pillinger MH. The fibroblast-like synovial cell in rheumatoid arthritis: a key player in inflammation and joint destruction. Clin Immunol (2005) 115:118–28. doi: 10.1016/j.clim.2004.12.009
Keywords: exercise, clinical effect, biological mechanism, rheumatoid arthritis, review
Citation: Li Z and Wang X-Q (2023) Clinical effect and biological mechanism of exercise for rheumatoid arthritis: A mini review. Front. Immunol. 13:1089621. doi: 10.3389/fimmu.2022.1089621
Received: 04 November 2022; Accepted: 16 December 2022;
Published: 06 January 2023.
Edited by:
Tsutomu Takeuchi, Keio University School of Medicine, JapanReviewed by:
Brian J. Andonian, Duke University, United StatesCopyright © 2023 Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xue-Qiang Wang, d2FuZ3h1ZXFpYW5nQHN1cy5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.