 Shuling Chen
Shuling Chen Xuezhen Zeng
Xuezhen Zeng Tianhong Su
Tianhong Su Han Xiao
Han Xiao Manxia Lin
Manxia Lin Zhenwei Peng
Zhenwei Peng Sui Peng3
Sui Peng3 Ming Kuang
Ming Kuang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 23 November 2022
Sec. Cancer Immunity and Immunotherapy
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1033000
This article is part of the Research Topic Tumor Ablation and Immunity View all 36 articles
Hepatocellular carcinoma (HCC) is the leading cause of cancer-related death worldwide. Local ablation, such as radiofrequency ablation, microwave ablation, cryoablation and irreversible electroporation, etc., are well established in elimination and control of HCC. However, high recurrence rate after local ablation remains the biggest challenge for HCC management. Novel and effective therapeutic strategies to improve long-term survival are urgently needed. Accumulating studies have reported the role of ablation in modulating the tumor signaling pathway and the immune microenvironment to both eliminate residual/metastatic tumor and promote tumor progression. Ablation has been shown to elicit tumor-specific immune responses by inducing massive cell death and releasing tumor antigen. Immunotherapies that unleash the immune system have the potential to enhance the anti-tumor immunity induced by ablation. Multiple combinatory strategies have been explored in preclinical and clinical studies. In this review, we comprehensively summarize the latest progress on different mechanisms underlying the effects of ablation on tumor cells and tumor microenvironment. We further analyze the clinical trials testing the combination of ablation and immunotherapies, and discuss the possible role of immunomodulation to boost the anti-tumor effects of ablation and prevent HCC recurrence.
Liver cancers rank as the sixth most common cancers and the fourth leading cause of cancer-related death, and remain to be one of the few human malignancies still trending upwards worldwide (1, 2). Nevertheless, with the advance of screening technology and increased awareness of cancer surveillance, more and more HCC could be detected at early stage, rendering curative therapeutics applicable. In the 2022 update of BCLC strategy for HCC management, local ablation still plays leading part among the recommended curative treatments for early-stage HCC (3). A vast range of percutaneous ablation techniques have changed over the past decades, enabling improved local control efficacy for more and more HCC patients. Study showed that approximately 10% of HCC tumors ≤ 2 cm developed intrahepatic metastasis, and about 27% of these tumors developed microvascular invasion, which leads to repeated recurrence in many HCC patients (4). Thus, adjuvant therapies that could prevent HCC recurrence after curative treatment could dramatically improve the prognosis. Of note, in the era of immunotherapy, ablative techniques are gaining more and more attention for their capability of boosting local and systemic immune effects, which makes combination strategy a promising weapon for HCC treatment. Herein, we summarized the current status and progress of various ablation and immunotherapy for HCC, discussed the rationale for their synergistic anti-tumor effects, and conceived the current trends and future prospects of their combination, hoping to shed light on future studies for ablative immunotherapy to yield a promising new era of HCC management.
Copious ablation therapeutics are feasible in clinic practice, among which radiofrequency ablation (RFA) remains the backbone of local ablation for early-stage HCC. Other ablative techniques including microwave ablation (MWA), cryoablation and irreversible electroporation (IRE) are also available for various HCC cases. However, more data is needed for other ablation choices to become the mainstay treatments of HCC. By and large, two indications for these ablative therapies are referred by guidelines, as first pick for single, very early tumors < 2 cm or as a substitute to resection in early-stage single tumors ≤ 4 cm, or 2–3 tumors ≤ 3 cm (5, 6). Typically, ablation destroys tumor by chemical, electrical or thermal technologies. RFA, MWA, laser and high intensity focused ultrasound (HIFU) ablation deliver focal hyper thermic injury to tumor cells (7, 8). Cryoablation (CRA) causes hypo thermic damage to ablated cells while IRE is a non-thermal ablative technique that destroys cell by changing cell permeability (8). Chemical ablations mostly use ethanol and acetic acid injections (9).
This section presents a brief retrospect of traditional ablative therapies for HCC, as well as newly emerging ablative techniques, and discusses their traditional anti-cancer effects.
RFA is the most widely adopted local ablation therapies for HCC because of its superiority to other ablative treatment in objective response rates and overall survival (10, 11). Moreover, survival rate of RFA is comparable to that of surgical resection in stratified patients (12). Being repeatable, more cost-effective, and less invasive, RFA has been recommended as the first-line therapy for early-stage HCC by AASLD and EASL guidelines (5, 6). Complete response rates range from 70% to 90% and a median overall survival of ~60 months have been reported (13, 14). Percutaneous RFA is performed by direct insert of electrodes into the tumor tissue under the guidance of ultrasound, computed tomography (CT) or magnetic resonance. High-frequency alternating current at 375–480 kHz from the electrodes generates temperatures between 60°C and 100°C to yield tumor necrosis (15). Traditional monopolar RFA is limited in tumors ≤ 2–3 cm or near vessels (16). Cytotoxic temperatures are hard to maintain when the ablated tumor is near large blood vessels because flowing blood would adsorb the heat energy, which is called heat sink effect6. Innovative techniques including multibipolar RFA are developed to improve ablation efficacy.
RFA destructs HCC cells by inducing hyperthermic injury, which causes rapid protein denaturation, cell membrane integrity loss, mitochondrial dysfunction, and inhibition of DNA replication (17, 18). In addition, indirect or delayed cellular damage play important parts in tumor damage after thermal ablation. Potential mechanisms includes induction of apoptosis, ischemia after vascular damage, ischemia–reperfusion injury, and release of lysosomal contents and cytokines from tumor cells and intruding inflammatory cells to stimulate further immune response (17).
However, high recurrence of HCC after RFA has been reported, with a 5-year recurrence rate of 50–70%, for which insufficient RFA (iRFA) is mainly to blame1. During RFA, three zones could be detected in heat-ablated lesions: central zone suffers from coagulative necrosis with temperature ≥ 50°C; transitional zone is exposed to sublethal heat stress and induces reversible cell damage; the surrounding liver tissue that is unaffected by sublethal heat6. iRFA endows HCC with a more malignant phenotype, leading to drug resistance and worse prognosis. Several mechanisms have been reported involved in HCC recurrence after iRFA. Activation of b-catenin, Akt, ERK1/2, HIF-1a/BNIP3, MAPK, and NF-kB signaling pathways as well as inhibition of STAT3 signaling pathways have been demonstrated to promote HCC progression after iRFA (19–25). Besides, ceRNA-mediated mechanisms including ASMTL-AS1/miR-342-3p/NLK/YAP axis and GAS6-AS2/miR-3619-5p/ARL2 axis are also uncovered (26, 27). Kuang’s team recently reported transcription and translation regulatory mechanisms working in HCC cells after iRFA. The sublethal heat treatment increased the level of stress-induced phosphoprotein 1 (STIP1) and heat shock protein 90 (HSP90), and promoted the formation of STIP1-HSP90 complex, which transferred epithelial transcription suppressor Snail1 into nucleus to modulate mesenchymal gene transcription (28). In addition, sublethal heat stress increased the m6A epigenetic modification of epidermal factor growth receptor (EGFR) and promoted its binding with YTHDF1, which enhanced the translation of EGFR mRNA, leading to the migration and invasion of HCC cells (29).
Endeavors to combat iRFA have been devoted recent years. Nanotechnology and artificial intelligence (AI) based radiomics have advanced greatly to counter iRFA. Deep learning radiomics improve the accuracy of imaging guided identification of ablation tumor boundaries and the accurate preoperative prediction of prognosis for RFA and surgery, facilitating the optimized decision making between them for HCC patients in early stage. Liu et al. retrospectively enrolled 419 patients examined by contrast-enhanced ultrasound (CEUS) within 1 week before RFA or surgical resection. The nomograms incorporating radiomics signatures and clinical variables for progression-free survival (PFS) prediction were built. The proposed radiomics models and nomograms yielded accurate preoperative prediction of PFS for RFA and liver resection (30). Jiang et al. designed a nanobubble conjugated with colony-stimulating factor 1 receptor (CSF-1R), called NBCSF-1R, for HCC margin detection, facilitating the determination of ablation margin (31). Further, the combination of systemic or immunotherapy would be a promising sally port to overwhelm HCC recurrence after iRFA.
MWA generates heat through electromagnetic waves with higher frequency (900–2,450 MHz), endowing it with several advantages over RFA, including higher temperature for larger ablation zone, shorter ablation time, and a lower susceptibility to heat-sink effects (32). MWA created electromagnetic field to force the polar molecules with intrinsic dipoles including predominantly water within the tissue to keep realigning with the oscillating electric field (32). MWA also destroy tumor cells via the aforementioned heat-ablated mechanisms of direct hyperthermic damage. However, MWA-induced pro-inflammatory cytokines including IL-1 and IL-6 is less compared with that from the other ablative technologies (33). Several trials found comparable treatment efficacy of MWA to RFA by reporting similar primary endpoint and local tumor progression at 2 years (33). However, phase III data is needed for recommending this treatment in early-stage HCC with high level of evidence.
IRE works through non-thermal manner. It delivers short electric pulses of high-voltage field current between two inserted electrodes and punches the cellular bilipid membrane to induce cell apoptosis (34). Its non-thermal mechanism lowers the risk of heat injury to the adjacent tissue. For this, heat sink effect poses little influence on the efficacy of IRE ablation. Therefore, IRE is better suitable for HCC located at risk anatomical position. Jean-Charles Nault et al. treated 58 patients with IRE and reported a complete ablation rate of 92%, and 70% of the cases got tumor progression-free survival at one year (35). In general, IRE could be an alternative for HCC not suitable for thermal ablation. Similar as WMA, large cohorts of patients with longer follow-up are needed to evaluate the long-range treatment efficacy of IRE.
Real world data is limited for other ablative techniques to date, including cryoablation, laser ablation and phototherapy. A multi-center RCT comparing RFA and CRA observed comparable results in overall survival and tumor-free survival while a retrospective study with large cohort reported greater advantage of CRA in HCC-specific survival in comparison to RFA (36, 37). Phototherapy including photodynamic therapy (PDT) and photothermal therapy (PTT) is a novel and promising cancer therapy. Phototherapy destroys tumor cells through photochemical or photophysical effects (38). Nevertheless, these techniques are way far from recommendation in daily clinical practice.
Accumulating studies have demonstrated the effect of ablation in shaping the immune microenvironment. Tumor neoantigen, cytokines and danger-associated molecular patterns (DAMPs) induced by ablative therapies are recognized as the source of immune activation (7, 39). Besides, ablation will also trigger physiological wound healing response that regulates and maintains immunological tolerance towards the damaged tissue (39). Different ablative therapies triggered various immune responses in the tumor immune microenvironment.
Among all the ablation therapies, RFA has been the most widely used percutaneous ablation in early-stage HCC. To investigate the dynamic changes of systemic immunity in HCC patients after RFA treatment, Rochigneux et al. collected PMBCs of 80 patients on the day before (D0), day after (D1) and month after RFA, and detected the frequencies and phenotypes of different immune cells. They found that an early dynamic (D0/D1) of activated NKp30+ natural killer (NK) cells was associated with decreased recurrence, while a late dynamic (D1/M1) of immature CD56bright NK cells and altered PD-L1+myeloid-derived dendritic cells (DCs) correlated with increased recurrence (40). Another study also showed that RFA treatment stimulated NK cell activation and differentiation, and the number of NK cells with high level of activatory NK receptors and enhanced cytotoxicity were significantly increased in peripheral blood of HCC patients after RFA treatment (41). In addition, CD4+ and CD8+ T cell response induced by ablation correlated with clinical outcomes (42, 43). Although RFA could enhance various tumor-associated antigens (TAA) -specific T cell responses which contributed to improved recurrence-free survival, this effect was not sufficient to prevent HCC recurrence completely due to the short lifetime of TAA-specific T cells (44, 45). In addition, the number of TAA-specific T cells was inversely correlated with the frequency of CD14+HLA-DR-/low monocytic myeloid-derived suppressor cells (M-MDSCs), suggesting the immunosuppression in tumor immune microenvironment (44). Similarly, another study showed that in post-RFA recurrent HCC, polymorphonuclear myeloid-derived suppressor cells (PMN-MDSCs) were accumulated in the tumor microenvironment to suppressed CD8+T cells, providing the immunosuppressive soil for tumor progression (46). Mechanistically, RFA-mediated heat treatment-induced methyltransferase 1 (METTL1) overexpression, which subsequently translationally upregulated transforming growth factor-beta 2 (TGF-β2) to induced PMN-MDSCs and suppressed CD8+T cell proliferation (46).
In addition to cytotoxic lymphocytes, accumulating studies have shown that ablation treatment could induce DC infiltration in tumor and activate DCs to evoke anti-tumor immune responses (47–49). Increased serum levels of tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), interferon-gamma (IFN-γ), and IL-2 were also observed, while the levels of Th2 cytokines including IL-4, IL-6 and IL-10 were markedly decreased (50, 51).
Vascular endothelial growth factor (VEGF) is an angiogenic factor that regulates angiogenesis by inducing proliferation, migration and permeability of endothelial cells. It has been reported that VEGF was increased in HCC patients after RFA treatment (52). VEGF also play a immunoregulatory role in tumor microenvironment by inducing MDSCs, regulatory T cells (Tregs), and mast cells, and inhibiting T cell function, differentiation and activation of DCs (53, 54).
As for other ablation therapies, cryoablation could induce inflammatory and coagulative responses in liver (55). Interestingly, study also found that elevation of circulating PD-L1/PD-1 in hepatitis B (HBV)-associated HCC patients after cryoablation correlated with poor prognosis (56). MWA significantly increased CD3+T cells, CD4+T cells and IL-2 in peripheral blood of HCC patients one month after treatment. In addition, IL-4 and IL-10 levels were decreased after MWA, indicating that MWA relieved immunosuppression in HCC patients (57). Besides, MWA increased T helper 17 cells (Th17) in HCC patients, and high frequency of circulating Th17 cells was associated with tumor recurrence (58). Study also found that the tumor-specific T cell response against TAAs was more frequent in patients with a long-time remission (> 1 year) after MWA compared to patients suffering from an early relapse, and correlated with improved PFS (59). Irreversible electroporation not only effectively eliminated HCC but also prevented tumor recurrence (60). On the one hand, IRE induced tumor cell necrosis and release of DAMPs including adenosine triphosphate (ATP), high mobility group box 1 (HMGB1) and calreticulin to stimulate anti-tumor immunity. On the other hand, IRE also alleviated immunosuppression by reducing Tregs and PD-1+ T cells (60).
Substantial evidence phenotypically showed that ablation induced immune cell changes and differential inflammatory cytokines and chemokines expression in peripheral blood or tumor microenvironment. In addition, ablation induces both protective anti-tumor immune response and immune tolerance. However, most studies have not yet explored the underlying mechanisms. It’s conceivable that DAMPs or inflammatory cytokines or chemokines induced by ablation may play the pivotal role in reshaping the immune microenvironment. Indeed, a few mechanistic studies reported that ablation affects the immune microenvironment indirectly through the regulation of cytokines or chemokines expression by residual tumor cells (46, 60). However, the complex regulatory network by ablation awaits further investigation in the future. Currently, efforts have been focused on developing adjuvant immunotherapy to synergistically shift the equilibrium out of inhibitory immune modulation and elicit sustainable immune response against tumor.
All ablation modalities generate tumor debris in situ, which provides antigen depot also known as cancer vaccine to stimulate immature DCs and naïve T cells that evoke antitumor immunity (7, 39). However, immune responses induced by ablative treatment are incapable of evoking robust sustainable immune effects. In addition, tumors evolved to create an immunosuppressive tumor immune microenvironment favorable for tumor progression. Developing approaches that counteract the immunosuppressive microenvironment potentially boost ablation-induced anti-tumor immune response (39).
Immunotherapy, either unleashes the own immune system or adoptively transfers cytotoxic cells to fight cancers provides the rationale for combination therapy. Different immune strategies have been tested in many studies, including adoptive cell therapy, immune checkpoint inhibitors (ICI), cytokines, etc. Currently, immunotherapies have been mostly used in advanced diseases, it’s also reasonable to use them in curative and adjuvant setting. Many clinical trials have been launched to investigate the safety and efficacy of combination of ablation and immunotherapy in HCC (Table 1).
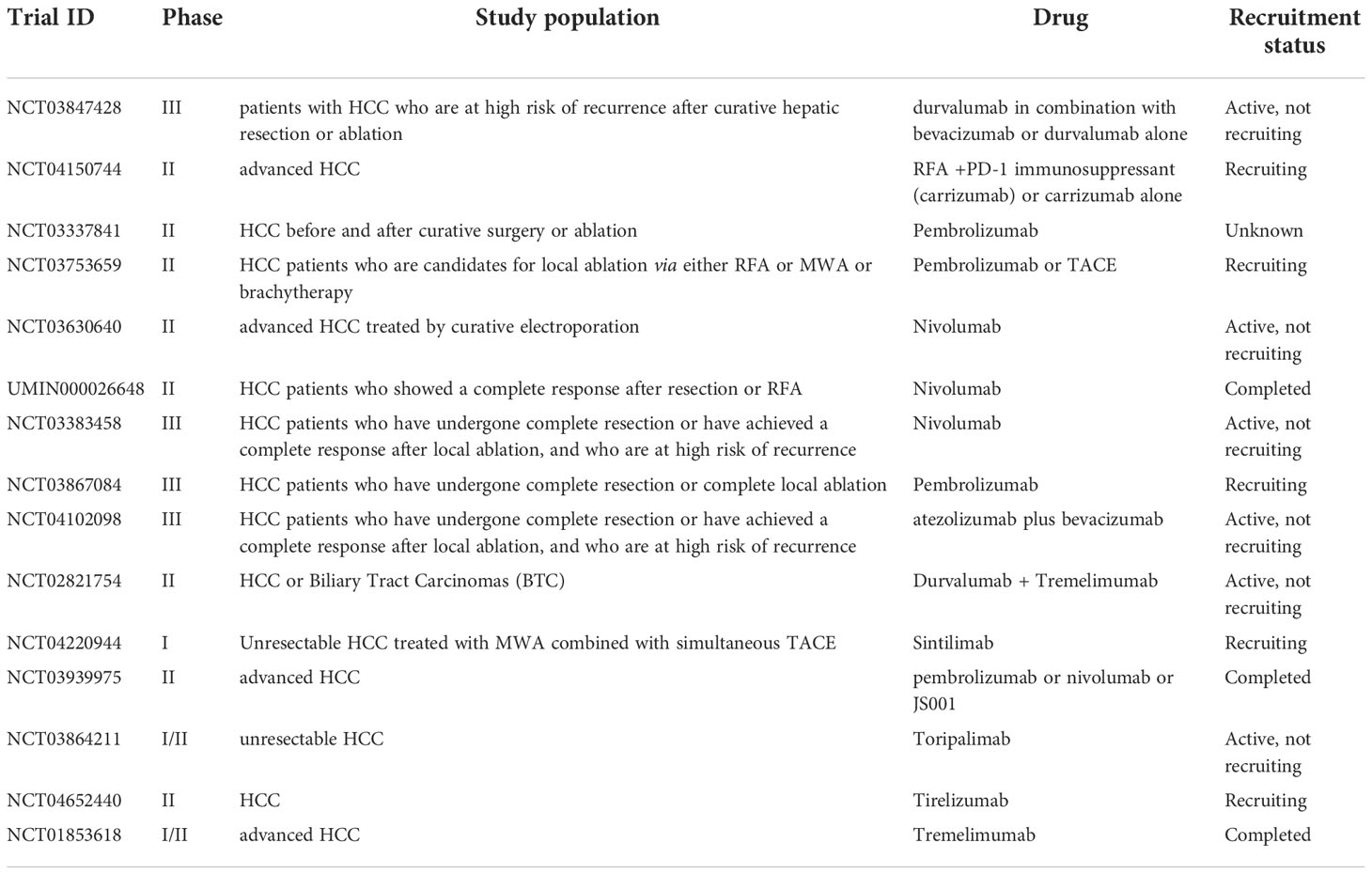
Table 1 Clinical trials evaluating the combination of ablation and immunotherapy in HCC.
Adoptive cell therapy is an immunotherapy that uses autologous immune cells which are modified or activated to evoke anti-tumor immunity and eliminate tumor cells. Cytokine-induced killer cells (CIK), tumor-infiltrating lymphocytes (TIL), chimeric antigen receptors (CAR)-T cells, DC vaccines are common forms of adoptive cell therapy.
CIK cells are a heterogeneous population of effector T cells, which come from patients’ peripheral blood mononuclear cells and can be expanded in vitro. CIK alone has been developed as cancer immunotherapy as it exhibits major histocompatibility complex (MHC)-unrestricted, safe, and effective anti-tumor activity (61). In the recent years, CIK has also been investigated as adjuvant therapy in treatment of HCC. Adjuvant therapy using cytokine-induced killer cells are derived from peripheral blood mononuclear cells (PBMCs) of HCC patients and activated by IL-2 and anti-CD3 antibody. To test the safety and feasibility of combination of RFA and adjuvant autologous RetroNectin activated killer (RAK) cells, 7 HCC patients were recruited in the trial. RAK cells were transfused to primary HCC patients intravenously after RFA. During a seven-month follow-up, no severe adverse events, recurrences or deaths were observed, suggesting the feasibility and safety of the combined therapeutic strategy to prevent HCC recurrence (62). In 2008, Weng et al. launched a clinical trial which recruited 85 HCC patients after transcatheter arterial chemoembolization and RFA. Autologous CIK cells were transfused to patients via hepatic artery. After infusion, CD3+, CD4+, CD56+, CD3+CD56+ cells, and CD4+/CD8+ ratio were significantly increased, resulting in a reduction of HCC recurrence (63). A study in Korea recruited 230 patients with HCC treated by surgical resection, radiofrequency ablation, or percutaneous ethanol injection, and patients were administered with control or CIK therapy respectively. The median time of recurrence-free survival was significantly improved from 30.0 months to 44 months (64). In another clinical trial, 62 patients diagnosed with HCC were treated with RFA alone or combined with CIK. The combination of sequential CIK with RFA improved progression-free survival, and reduced Hepatitis C (HCV) viral load in some patients (65). Consistently, a similar clinical trial also showed that autologous CIK cells after RFA treatment prolonged the RFS of HCC patients (66). These positive clinical results suggested the potential of this combined treatment in prevention of HCC recurrence (65).
The DC and T cell adoptive transfer have also been studied in HCC. In a phase II clinical trial, Peng et al. investigated the combination of neoantigen-based DC vaccination and adoptive T-cell transfer as adjuvant therapy after RFA or surgical resection of HCC patients. This combination therapy successfully induced neoantigen-specific immunity and prolonged disease-free survival in responders without severe side effects, indicating that neoantigen-based combination immunotherapy is feasible, safe, and has the potential to reduce HCC recurrence after curative treatment (67).
The development of ICIs has revolutionized the treatment of cancers and provides unprecedented extension of patient survival. Immune checkpoints are common part of the immune system which regulate T cell activity. ICIs achieved great success in treating various types of solid and liquid malignancies. ICIs work by releasing the inhibitory brakes of T cells and also activating other innate and adaptive immune cells, which orchestrate an effective immunity to eliminate tumors (68). Many studies have reported the positive results of ICIs as the first-line treatment in advanced cancers. And increasing studies have been investigating the efficacy of ICIs as combination with curative treatment (listed in Table 1).
In some trials, positive clinical results have been observed in advanced HCC patients who received cytotoxic T-lymphocyte-associated protein 4 (CTLA4) blockade (Tremelimumab) combined with RFA, accompanied by remarkably reduced HCV viral load. In addition, the combined treatment increased CD8+T cells infiltration in tumor (69). However, some of these patients also received cryoablation and/or transarterial chemoembolization (TACE). In another study, it showed that RFA induced anti-tumor immune response which was strongly enhanced by CTLA4 blockade, contributing to long-lasting tumor protection (70). For advanced HCC patients, anti-PD-1 (programmed cell death protein 1) antibody is one of the second-line therapies after sorafenib failure. Lyu et al. found that additional ablation increased response rate with tolerable toxicity and improved survival in these patients (71). Many trials are still under investigation and results of these trials will be public within the next few years.
In preclinical model, Huang et al. reported that the combination of MWA and anti-PD-1 antibody significantly ameliorated distant tumor growth and elevated Th1 cytokines in peripheral blood in mouse HCC model (72).
Multiple studies also investigated the efficacy of other adjuvant immunotherapies after ablation. CpG B oligonucleotides, a toll like receptor 9 agonists, has been tested in a rabbit VX2 hepatoma model. It showed that RFA alone could induce the secretion of Th1 cytokines, while CpG treatment increased IL-8 and IL-10 levels. In addition, the combination of CpG and RFA significantly reduced tumor burden and even prevented subsequent tumor metastasis, and thus improved survival (73).
Several chemokines were also used in cancer treatment for their ability to attract immune cells such as DC and cytotoxic T cells to augment anti-tumor immunity. It was reported that RFA alone could not only eradicate the treated ipsilateral tumors, but also inhibited the growth of contralateral non-RFA-treated tumors with increased T-cell infiltration. Additional injection of ECI301 (an active variant of CC chemokine ligand 3) after RFA significantly augmented RFA-induced anti-tumor immune responses and increased CCR1-expressing CD11c+ cells in peripheral blood and tumors. Deficiency of CCR1 impaired the accumulation of CD11C+, CD4+ and CD8+ cells in tumors, indicating that ECI301 augmented tumor-specific immune responses through CCR1-mediated DC accumulation in tumor (74).
The therapeutic strategies of HCC are evolving rapidly. The rationale for combination of ablation and immunotherapy is sound. Ablation promotes production of proinflammatory cytokines and antigens, which activated anti-tumor immunity. Tyrosine kinase inhibitors (TKIs) or immunotherapies, which modulates the tumor microenvironment by increasing effector T cell infiltration and decreasing immunosuppressive cells, further enhances anti-tumor immune response.
However, some issues need to be further investigated, including the timing of ICB administration, biomarkers that could predict therapeutic effects and management of adverse events. Immune profiling after ablation is essential for development of combination therapies that boost anti-tumor immunity (75).
In the recent years, various types of immunotherapies have come to the stage of HCC treatment, such as Lymphocyte-activation gene 3 (LAG-3), T cell Ig and ITIM domain (TIGIT) or T cell immunoglobulin domain and mucin domain-3 (TIM-3) blockade, chimeric antigen receptor T cell (CAR-T) therapy, adoptive cell therapies using NK cells, NKT cells, or γδ T cells, oncolytic virotherapy, cancer vaccines, etc (76, 77). These novel therapeutic strategies also show great potential to synergize with ablation in the treatment of primary and metastatic HCC. Increasing clinical trials are actively underway and may offer a paradigm shift in the management of HCC.
SC, XZ and TS wrote the manuscript. SC, HX, ML, ZP, SP, MK revised this manuscript. All authors contributed to the article and approved the submitted version.
This work is supported by State Key Program of National Natural Science of China (No. 82130083), The National Science Fund for Distinguished Young Scholars (No. 81825013), the National Science Fund for Young Scholars (No. 82003105), the National Natural Science Foundation of China (No. 82172047; No. 31970870), Natural Science Foundation of Guangdong Province (No. 2021A1515010450), Natural Science Foundation for Distinguished Youths of Guangdong Province (No. 2022B1515020060), the Joint Funds of the National Natural Science Foundation of China (No. U20A20370).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. Hepatocellular carcinoma. Nat Rev Dis Primers (2021) 7(1):6. doi: 10.1038/s41572-020-00240-3
2. Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet (2019) 394(10204):1145–58. doi: 10.1016/S0140-6736(19)30427-1
3. Reig M, Forner A, Rimola J, Ferrer-Fabrega J, Burrel M, Garcia-Criado A, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol (2022) 76(3):681–93. doi: 10.1016/j.jhep.2021.11.018
4. Nakashima O, Sugihara S, Kage M, Kojiro M. Pathomorphologic characteristics of small hepatocellular carcinoma: a special reference to small hepatocellular carcinoma with indistinct margins. Hepatology (1995) 22(1):101–5. doi: 10.1016/0270-9139(95)90359-3
5. European Association for the study of the liver. Electronic address, e.e.e. and l. European association for the study of the, EASL clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol (2018) 69(1):182–236. doi: 10.1016/j.jhep.2018.03.019
6. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology (2018) 67(1):358–80. doi: 10.1002/hep.29086
7. Chu KF, Dupuy DE. Thermal ablation of tumours: biological mechanisms and advances in therapy. Nat Rev Cancer (2014) 14(3):199–208. doi: 10.1038/nrc3672
8. Seror O. Ablative therapies: Advantages and disadvantages of radiofrequency, cryotherapy, microwave and electroporation methods, or how to choose the right method for an individual patient? Diagn Interv Imaging (2015) 96(6):617–24. doi: 10.1016/j.diii.2015.04.007
9. Clark TW, Soulen MC. Chemical ablation of hepatocellular carcinoma. J Vasc Interv Radiol (2002) 13(9 Pt 2):S245–52. doi: 10.1016/s1051-0443(07)61792-8
10. Lencioni RA, Allgaier HP, Cioni D, Olschewski M, Deibert P, Crocetti L, et al. Small hepatocellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology (2003) 228(1):235–40. doi: 10.1148/radiol.2281020718
11. Feng K, Yan J, Li X, Xia F, Ma K, Wang S, et al. A randomized controlled trial of radiofrequency ablation and surgical resection in the treatment of small hepatocellular carcinoma. J Hepatol (2012) 57(4):794–802. doi: 10.1016/j.jhep.2012.05.007
12. Mohkam K, Dumont PN, Manichon AF, Jouvet JC, Boussel L, Merle P, et al. No-touch multibipolar radiofrequency ablation vs. surgical resection for solitary hepatocellular carcinoma ranging from 2 to 5cm. J Hepatol (2018) 68(6):1172–80. doi: 10.1016/j.jhep.2018.01.014
13. Lee DH, Lee JM, Lee JY, Kim SH, Yoon JH, Kim YJ, et al. Radiofrequency ablation of hepatocellular carcinoma as first-line treatment: long-term results and prognostic factors in 162 patients with cirrhosis. Radiology (2014) 270(3):900–9. doi: 10.1148/radiol.13130940
14. Shiina S, Tateishi R, Arano T, Uchino K, Enooku K, Nakagawa H, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol (2012) 107(4):569–77. doi: 10.1038/ajg.2011.425
15. Breen DJ, Lencioni R. Image-guided ablation of primary liver and renal tumours. Nat Rev Clin Oncol (2015) 12(3):175–86. doi: 10.1038/nrclinonc.2014.237
16. Lehmann KS, Poch FG, Rieder C, Schenk A, Stroux A, Frericks BB, et al. Minimal vascular flows cause strong heat sink effects in hepatic radiofrequency ablation ex vivo. J Hepatobiliary Pancreat Sci (2016) 23(8):508–16. doi: 10.1002/jhbp.370
17. Nikfarjam M, Muralidharan V, Christophi C. Mechanisms of focal heat destruction of liver tumors. J Surg Res (2005) 127(2):208–23. doi: 10.1016/j.jss.2005.02.009
18. Fajardo LF, Egbert B, Marmor J, Hahn GM. Effects of hyperthermia in a malignant tumor. Cancer (1980) 45(3):613–23. doi: 10.1002/1097-0142(19800201)45:3<613::aid-cncr2820450331>3.0.co;2-e
19. Jia G, Li F, Tong R, Liu Y, Zuo M, Ma L, et al. C-Met/MAPK pathway promotes the malignant progression of residual hepatocellular carcinoma cells after insufficient radiofrequency ablation. Med Oncol (2020) 37(12):117. doi: 10.1007/s12032-020-01444-z
20. Zhang N, Li H, Qin C, Ma D, Zhao Y, Zhu W, et al. Insufficient radiofrequency ablation promotes the metastasis of residual hepatocellular carcinoma cells via upregulating flotillin proteins. J Cancer Res Clin Oncol (2019) 145(4):895–907. doi: 10.1007/s00432-019-02852-z
21. Xu WL, Wang SH, Sun WB, Gao J, Ding XM, Kong J, et al. Insufficient radiofrequency ablation-induced autophagy contributes to the rapid progression of residual hepatocellular carcinoma through the HIF-1alpha/BNIP3 signaling pathway. BMB Rep (2019) 52(4):277–82. doi: 10.5483/BMBRep.2019.52.4.263
22. Zhang N, Ma D, Wang L, Zhu X, Pan Q, Zhao Y, et al. Insufficient radiofrequency ablation treated hepatocellular carcinoma cells promote metastasis by up-regulation ITGB3. J Cancer (2017) 8(18):3742–54. doi: 10.7150/jca.20816
23. Zhang N, Wang L, Chai ZT, Zhu ZM, Zhu XD, Ma DN, et al. Incomplete radiofrequency ablation enhances invasiveness and metastasis of residual cancer of hepatocellular carcinoma cell HCCLM3 via activating beta-catenin signaling. PloS One (2014) 9(12):e115949. doi: 10.1371/journal.pone.0115949
24. Zhou T, Liu B, Wang Y, Wang W, Chang H, Li D, et al. Insufficient radiofrequency ablation promotes epithelial-mesenchymal transition mediated by interleukin-6/signal transducer and activator of transcription 3/Snail pathway in the H22 cells. J Cancer Res Ther (2020) 16(5):1112–8. doi: 10.4103/jcrt.JCRT_12_20
25. Kong J, Kong L, Kong J, Ke S, Gao J, Ding X, et al. After insufficient radiofrequency ablation, tumor-associated endothelial cells exhibit enhanced angiogenesis and promote invasiveness of residual hepatocellular carcinoma. J Transl Med (2012) 10:230. doi: 10.1186/1479-5876-10-230
26. Ma D, Gao X, Liu Z, Lu X, Ju H, Zhang N. Exosome-transferred long non-coding RNA ASMTL-AS1 contributes to malignant phenotypes in residual hepatocellular carcinoma after insufficient radiofrequency ablation. Cell Prolif (2020) 53(9):e12795. doi: 10.1111/cpr.12795
27. Li Z, Jiang M, Zhang T, Liu S. GAS6-AS2 promotes hepatocellular carcinoma via miR-3619-5p/ARL2 axis under insufficient radiofrequency ablation condition. Cancer Biother Radiopharm (2021) 36(10):879–87. doi: 10.1089/cbr.2019.3541
28. Su T, Liao J, Dai Z, Xu L, Chen S, Wang Y, et al. Stress-induced phosphoprotein 1 mediates hepatocellular carcinoma metastasis after insufficient radiofrequency ablation. Oncogene (2018) 37(26):3514–27. doi: 10.1038/s41388-018-0169-4
29. Su T, Huang M, Liao J, Lin S, Yu P, Yang J, et al. Insufficient radiofrequency ablation promotes hepatocellular carcinoma metastasis through N6-methyladenosine mRNA methylation-dependent mechanism. Hepatology (2021) 74(3):1339–56. doi: 10.1002/hep.31766
30. Liu F, Liu D, Wang K, Xie X, Su L, Kuang M, et al. Deep learning radiomics based on contrast-enhanced ultrasound might optimize curative treatments for very-early or early-stage hepatocellular carcinoma patients. Liver Cancer (2020) 9(4):397–413. doi: 10.1159/000505694
31. Jiang Q, Zeng Y, Xu Y, Xiao X, Liu H, Zhou B, et al. Ultrasound molecular imaging as a potential non-invasive diagnosis to detect the margin of hepatocarcinoma via CSF-1R targeting. Front Bioeng Biotechnol (2020) 8:783. doi: 10.3389/fbioe.2020.00783
32. Lubner MG, Brace CL, Hinshaw JL, Lee FT Jr. Microwave tumor ablation: mechanism of action, clinical results, and devices. J Vasc Interv Radiol (2010) 21(8 Suppl):S192–203. doi: 10.1016/j.jvir.2010.04.007
33. Ahmad F, Gravante G, Bhardwaj N, Strickland A, Basit R, West K, et al. Renal effects of microwave ablation compared with radiofrequency, cryotherapy and surgical resection at different volumes of the liver treated. Liver Int (2010) 30(9):1305–14. doi: 10.1111/j.1478-3231.2010.02290.x
34. Hsiao CY, Huang KW. Irreversible electroporation: A novel ultrasound-guided modality for non-thermal tumor ablation. J Med Ultrasound (2017) 25(4):195–200. doi: 10.1016/j.jmu.2017.08.003
35. Sutter O, Calvo J, N'Kontchou G, Nault JC, Ourabia R, Nahon P, et al. Safety and efficacy of irreversible electroporation for the treatment of hepatocellular carcinoma not amenable to thermal ablation techniques: A retrospective single-center case series. Radiology (2017) 284(3):877–86. doi: 10.1148/radiol.2017161413
36. Wang C, Wang H, Yang W, Hu K, Xie H, Hu KQ, et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma. Hepatology (2015) 61(5):1579–90. doi: 10.1002/hep.27548
37. Xu J, Noda C, Erickson A, Mokkarala M, Charalel R, Ramaswamy R, et al. Radiofrequency ablation vs. cryoablation for localized hepatocellular carcinoma: A propensity-matched population study. Anticancer Res (2018) 38(11):6381–6. doi: 10.21873/anticanres.12997
38. Li X, Lovell JF, Yoon J, Chen X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat Rev Clin Oncol (2020) 17(11):657–74. doi: 10.1038/s41571-020-0410-2
39. van den Bijgaart RJE, Schuurmans F, Futterer JJ, Verheij M, Cornelissen LAM, Adema GJ. Immune modulation plus tumor ablation: Adjuvants and antibodies to prime and boost anti-tumor immunity in situ. Front Immunol (2021) 12:617365. doi: 10.3389/fimmu.2021.617365
40. Rochigneux P, Nault JC, Mallet F, Chretien AS, Barget N, Garcia AJ, et al. Dynamic of systemic immunity and its impact on tumor recurrence after radiofrequency ablation of hepatocellular carcinoma. Oncoimmunology (2019) 8(8):1615818. doi: 10.1080/2162402X.2019.1615818
41. Zerbini A, Pilli M, Laccabue D, Pelosi G, Molinari A, Negri E, et al. Radiofrequency thermal ablation for hepatocellular carcinoma stimulates autologous NK-cell response. Gastroenterology (2010) 138(5):1931–42. doi: 10.1053/j.gastro.2009.12.051
42. Hiroishi K, Eguchi J, Baba T, Shimazaki T, Ishii S, Hiraide A, et al. Strong CD8(+) T-cell responses against tumor-associated antigens prolong the recurrence-free interval after tumor treatment in patients with hepatocellular carcinoma. J Gastroenterol (2010) 45(4):451–8. doi: 10.1007/s00535-009-0155-2
43. Nobuoka D, Motomura Y, Shirakawa H, Yoshikawa T, Kuronuma T, Takahashi M, et al. Radiofrequency ablation for hepatocellular carcinoma induces glypican-3 peptide-specific cytotoxic T lymphocytes. Int J Oncol (2012) 40(1):63–70. doi: 10.3892/ijo.2011.1202
44. Mizukoshi E, Yamashita T, Arai K, Sunagozaka H, Ueda T, Arihara F, et al. Enhancement of tumor-associated antigen-specific T cell responses by radiofrequency ablation of hepatocellular carcinoma. Hepatology (2013) 57(4):1448–57. doi: 10.1002/hep.26153
45. Zerbini A, Pilli M, Penna A, Pelosi G, Schianchi C, Molinari A, et al. Radiofrequency thermal ablation of hepatocellular carcinoma liver nodules can activate and enhance tumor-specific T-cell responses. Cancer Res (2006) 66(2):1139–46. doi: 10.1158/0008-5472.CAN-05-2244
46. Zeng X, Liao G, Li S, Liu H, Zhao X, Li S, et al. Eliminating METTL1-mediated accumulation of PMN-MDSCs prevents hepatocellular carcinoma recurrence after radiofrequency ablation. Hepatology (2022). doi: 10.1002/hep.32585
47. den Brok MH, Sutmuller RP, Nierkens S, Bennink EJ, Frielink C, Toonen LW, et al. Efficient loading of dendritic cells following cryo and radiofrequency ablation in combination with immune modulation induces anti-tumour immunity. Br J Cancer (2006) 95(7):896–905. doi: 10.1038/sj.bjc.6603341
48. Dromi SA, Walsh MP, Herby S, Traughber B, Xie J, Sharma KV, et al. Radiofrequency ablation induces antigen-presenting cell infiltration and amplification of weak tumor-induced immunity. Radiology (2009) 251(1):58–66. doi: 10.1148/radiol.2511072175
49. Zerbini A, Pilli M, Fagnoni F, Pelosi G, Pizzi MG, Schivazappa S, et al. Increased immunostimulatory activity conferred to antigen-presenting cells by exposure to antigen extract from hepatocellular carcinoma after radiofrequency thermal ablation. J Immunother (2008) 31(3):271–82. doi: 10.1097/CJI.0b013e318160ff1c
50. Ali MY, Grimm CF, Ritter M, Mohr L, Allgaier HP, Weth R, et al. Activation of dendritic cells by local ablation of hepatocellular carcinoma. J Hepatol (2005) 43(5):817–22. doi: 10.1016/j.jhep.2005.04.016
51. Ji L, Gu J, Chen L, Miao D. Changes of Th1/Th2 cytokines in patients with primary hepatocellular carcinoma after ultrasound-guided ablation. Int J Clin Exp Pathol (2017) 10(8):8715–20. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6965388/.
52. Guan Q, Gu J, Zhang H, Ren W, Ji W, Fan Y. Correlation between vascular endothelial growth factor levels and prognosis of hepatocellular carcinoma patients receiving radiofrequency ablation. Biotechnol Biotechnol Equip (2015) 29(1):119–23. doi: 10.1080/13102818.2014.981776
53. Yang J, Yan J, Liu B. Targeting VEGF/VEGFR to modulate antitumor immunity. Front Immunol (2018) 9:978. doi: 10.3389/fimmu.2018.00978
54. Vitale G, Dicitore A, Gentilini D, Cavagnini F. Immunomodulatory effects of VEGF: Clinical implications of VEGF-targeted therapy in human cancer. Cancer Biol Ther (2010) 9(9):694–8. doi: 10.4161/cbt.9.9.11691
55. Jansen MC, van Hillegersberg R, Schoots IG, Levi M, Beek JF, Crezee H, et al. Cryoablation induces greater inflammatory and coagulative responses than radiofrequency ablation or laser induced thermotherapy in a rat liver model. Surgery (2010) 147(5):686–95. doi: 10.1016/j.surg.2009.10.053
56. Zeng Z, Shi F, Zhou L, Zhang MN, Chen Y, Chang XJ, et al. Upregulation of circulating PD-L1/PD-1 is associated with poor post-cryoablation prognosis in patients with HBV-related hepatocellular carcinoma. PloS One (2011) 6(9):e23621. doi: 10.1371/journal.pone.0023621
57. Zhang H, Hou X, Cai H, Zhuang X. Effects of microwave ablation on T-cell subsets and cytokines of patients with hepatocellular carcinoma. Minim Invasive Ther Allied Technol (2017) 26(4):207–11. doi: 10.1080/13645706.2017.1286356
58. Zhou Y, Xu X, Ding J, Jing X, Wang F, Wang Y, et al. Dynamic changes of T-cell subsets and their relation with tumor recurrence after microwave ablation in patients with hepatocellular carcinoma. J Cancer Res Ther (2018) 14(1):40–5. doi: 10.4103/jcrt.JCRT_775_17
59. Leuchte K, Staib E, Thelen M, Godel P, Lechner A, Zentis P, et al. Microwave ablation enhances tumor-specific immune response in patients with hepatocellular carcinoma. Cancer Immunol Immunother (2021) 70(4):893–907. doi: 10.1007/s00262-020-02734-1
60. Dai Z, Wang Z, Lei K, Liao J, Peng Z, Lin M, et al. Irreversible electroporation induces CD8(+) T cell immune response against post-ablation hepatocellular carcinoma growth. Cancer Lett (2021) 503:1–10. doi: 10.1016/j.canlet.2021.01.001
61. Gao X, Mi Y, Guo N, Xu H, Xu L, Gou X, et al. Cytokine-induced killer cells as pharmacological tools for cancer immunotherapy. Front Immunol (2017) 8:774. doi: 10.3389/fimmu.2017.00774
62. Ma H, Zhang Y, Wang Q, Li Y, He J, Wang H, et al. Therapeutic safety and effects of adjuvant autologous RetroNectin activated killer cell immunotherapy for patients with primary hepatocellular carcinoma after radiofrequency ablation. Cancer Biol Ther (2010) 9(11):903–7. doi: 10.4161/cbt.9.11.11697
63. Weng DS, Zhou J, Zhou QM, Zhao M, Wang QJ, Huang LX, et al. Minimally invasive treatment combined with cytokine-induced killer cells therapy lower the short-term recurrence rates of hepatocellular carcinomas. J Immunother (2008) 31(1):63–71. doi: 10.1097/CJI.0b013e31815a121b
64. Lee JH, Lee JH, Lim YS, Yeon JE, Song TJ, Yu SJ, et al. Adjuvant immunotherapy with autologous cytokine-induced killer cells for hepatocellular carcinoma. Gastroenterology (2015), 148:1383–91.e6. doi: 10.1053/j.gastro.2015.02.055
65. Cui J, Wang N, Zhao H, Jin H, Wang G, Niu C, et al. Combination of radiofrequency ablation and sequential cellular immunotherapy improves progression-free survival for patients with hepatocellular carcinoma. Int J Cancer (2014) 134(2):342–51. doi: 10.1002/ijc.28372
66. Yoon JS, Song BG, Lee JH, Lee HY, Kim SW, Chang Y, et al. Adjuvant cytokine-induced killer cell immunotherapy for hepatocellular carcinoma: A propensity score-matched analysis of real-world data. BMC Cancer (2019) 19(1):523. doi: 10.1186/s12885-019-5740-z
67. Peng S, Chen S, Hu W, Mei J, Zeng X, Su T, et al. Combination neoantigen-based dendritic cell vaccination and adoptive T-cell transfer induces antitumor responses against recurrence of hepatocellular carcinoma. Cancer Immunol Res (2022) 10(6):728–44. doi: 10.1158/2326-6066.CIR-21-0931
68. Bagchi S, Yuan R, Engleman EG. Immune checkpoint inhibitors for the treatment of cancer: Clinical impact and mechanisms of response and resistance. Annu Rev Pathol (2021) 16:223–49. doi: 10.1146/annurev-pathol-042020-042741
69. Duffy AG, Ulahannan SV, Makorova-Rusher O, Rahma O, Wedemeyer H, Pratt D, et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J Hepatol (2017) 66(3):545–51. doi: 10.1016/j.jhep.2016.10.029
70. den Brok MH, Sutmuller RP, van der Voort R, Bennink EJ, Figdor CG, Ruers TJ, et al. In situ tumor ablation creates an antigen source for the generation of antitumor immunity. Cancer Res (2004) 64(11):4024–9. doi: 10.1158/0008-5472.CAN-03-3949
71. Lyu N, Kong Y, Li X, Mu L, Deng H, Chen H, et al. Ablation reboots the response in advanced hepatocellular carcinoma with stable or atypical response during PD-1 therapy: A proof-of-Concept study. Front Oncol (2020) 10:580241. doi: 10.3389/fonc.2020.580241
72. Huang S, Li T, Chen Y, Liu J, Wang Y, Yang C, et al. Microwave ablation combined with anti-PD-1 therapy enhances systemic antitumor immunity in a multitumor murine model of Hepa1-6. Int J Hyperthermia (2022) 39(1):278–86. doi: 10.1080/02656736.2022.2032406
73. Behm B, Di Fazio P, Michl P, Neureiter D, Kemmerling R, Hahn EG, et al. Additive antitumour response to the rabbit VX2 hepatoma by combined radio frequency ablation and toll like receptor 9 stimulation. Gut (2016) 65(1):134–43. doi: 10.1136/gutjnl-2014-308286
74. Iida N, Nakamoto Y, Baba T, Nakagawa H, Mizukoshi E, Naito M, et al. Antitumor effect after radiofrequency ablation of murine hepatoma is augmented by an active variant of CC chemokine ligand 3/macrophage inflammatory protein-1alpha. Cancer Res (2010) 70(16):6556–65. doi: 10.1158/0008-5472.CAN-10-0096
75. Han JW, Yoon SK. Immune responses following locoregional treatment for hepatocellular carcinoma: Possible roles of adjuvant immunotherapy. Pharmaceutics (2021) 13(9):1387. doi: 10.3390/pharmaceutics13091387
76. Kole C, Charalampakis N, Tsakatikas S, Vailas M, Moris D, Gkotsis E, et al. Immunotherapy for hepatocellular carcinoma: A 2021 update. Cancers (Basel) (2020) 12(10):2859–2886. doi: 10.3390/cancers12102859
Keywords: ablation, tumor immune microenvironment, immunotherapy, HCC, combination therapy
Citation: Chen S, Zeng X, Su T, Xiao H, Lin M, Peng Z, Peng S and Kuang M (2022) Combinatory local ablation and immunotherapies for hepatocellular carcinoma: Rationale, efficacy, and perspective. Front. Immunol. 13:1033000. doi: 10.3389/fimmu.2022.1033000
Received: 31 August 2022; Accepted: 25 October 2022;
Published: 23 November 2022.
Edited by:
Sukh Mahendra Singh, Banaras Hindu University, IndiaReviewed by:
Liyong Pu, Nanjing Medical University, ChinaCopyright © 2022 Chen, Zeng, Su, Xiao, Lin, Peng, Peng and Kuang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Kuang, a3VhbmdtQG1haWwuc3lzdS5lZHUuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.