
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 16 November 2022
Sec. Alloimmunity and Transplantation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1012042
 Tara K. Sigdel1
Tara K. Sigdel1 Paul A. Fields2
Paul A. Fields2 Juliane Liberto1Izabella Damm1Maggie Kerwin1Jill Hood2Parhom Towfighi1
Juliane Liberto1Izabella Damm1Maggie Kerwin1Jill Hood2Parhom Towfighi1 Marina Sirota1Harlan S. Robins2
Marina Sirota1Harlan S. Robins2 Minnie M. Sarwal1*, on behalf of CMV Systems Immunobiology Group
Minnie M. Sarwal1*, on behalf of CMV Systems Immunobiology GroupIn this cross-sectional and longitudinal analysis of mapping the T-cell repertoire in kidney transplant recipients, we have investigated and validated T-cell clonality, immune repertoire chronology at rejection, and contemporaneous allograft biopsy quantitative tissue injury, to better understand the pathobiology of acute T-cell fraction, T-cell repertoire and antibody-mediated kidney transplant rejection. To follow the dynamic evolution of T-cell repertoire changes before and after engraftment and during biopsy-confirmed acute rejection, we sequenced 323 peripheral blood samples from 200 unique kidney transplant recipients, with (n=100) and without (n=100) biopsy-confirmed acute rejection. We report that patients who develop acute allograft rejection, have lower (p=0.01) T-cell fraction even before transplantation, followed by its rise after transplantation and at the time of acute rejection accompanied by high TCR repertoire turnover (p=0.004). Acute rejection episodes occurring after the first 6 months post-transplantation, and those with a component of antibody-mediated rejection, had the highest turnover; p=0.0016) of their T-cell repertoire. In conclusion, we validated that detecting repertoire changes in kidney transplantation correlates with post-transplant rejection episodes suggesting that T-cell receptor sequencing may provide recipient pre-transplant and post-transplant predictors of rejection risk.
Transplanted kidneys fail due to both immune and nonimmune causes including primarily anti-donor alloimmunity via recruitment of activated T cells, but also due to other contributing factors such as activation of innate immunity by triggers such as cold ischemia time, donor co-morbidities, heterologous immunity from infections, and drug toxicities (1). Recent developments in T-cell receptor (TCR) sequencing allow for analysis of alloreactive human T-cell populations both before and after engraftment (2–4). Accurate and high-throughput sequencing of the third complementarity-determining region (CDR3) of the TCRβ chain, which is the crucial segment for antigen specificity, allowed us to profile the T-cell repertoire in peripheral blood samples, coincident with the occurrence of acute renal transplant rejection on a paired allograft biopsy, and to evaluate if rejection could be predicted prior to histological evaluation by peripheral blood sampling before transplantation and if specific changes in the TCR repertoire can define different phenotypes of acute rejection, such as antibody mediated rejection (4).
To assess the evolution of the T-cell immune repertoire in peripheral blood samples and their patterns in the context of allograft phenotypes, we compared peripheral blood samples from demographically matched renal transplant recipients who had either protocol or clinically indicated biopsies and paired blood samples for immune repertoire analysis; group comparisons were conducted between patients with histologically clean protocol biopsies (designated as the stable group (STA)) and histologically confirmed acute rejection as graded by the Banff classification on either protocol or indicated biopsies (designated as the acute rejection group (AR)) (5, 6). Recent exploratory studies tracking peripheral blood T cells using TCR sequencing after kidney transplantation (5, 7–10) have observed low-frequency immune repertoires alterations with small sample sizes (11, 12). In children and young infants, a diverse B-cell pre-transplant repertoire correlated with post-transplant rejection risk, but no differences were found in the TCR immune repertoire (13). Having found no significant changes in the TCR repertoire in acute rejection in pediatric recipients of renal allografts, in this study, we evaluated the TCR immune repertoires in a large cohort of adult renal transplant patients so as to be able to discern low frequency changes between T-cell clones and transplant time, histologically confirmed acute rejection episodes, and any specific variations with T cell or antibody mediated rejections.
The objective was to assess the evolution of the T-cell immune repertoire in peripheral blood samples and their patterns in the context of allograft phenotypes. For this, the study included biobanked biopsy-matched total blood samples (n=323) collected by an IRB approved research protocol at the University of California San Francisco (Study ID- #14-13573) and selected from a biobank of over 3000 blood samples collected from kidney transplant recipients. The blood samples selected for this study included pre-transplant baseline samples from 100 renal allograft recipients who had biopsy-confirmed AR, inclusive of both T cell-mediated rejection (TCMR) and antibody-mediated rejection (ABMR); 100 renal allograft recipients had STA biopsies and graft function. Study subjects were chosen who had their 1st kidney transplantation. All blood samples were submitted for sequencing using the ImmunoSEQ Assay (Adaptive Biotechnologies, Seattle, WA). For STA patients, 50 subjects had a 6-month post-transplant sample at the time of management (protocol) biopsy and none of them went on to develop AR over the next year of follow-up. For AR patients, 50 subjects had a blood sample at the time of AR, and 39 of those patients had an additional 6-month management biopsy blood draw. All subjects were enrolled following IRB approval and had informed consent. Study subjects’ baseline characteristics are summarized in Table 1.

Table 1 Demographic and baseline characteristics.
The matching allograft biopsy at the time of blood sampling was read by a single pathologist using semi-quantitative histological scores. Clinical AR was defined as an AR episode, associated with graft dysfunction, based on a greater than 20% rise in serum creatinine from baseline values, and confirmed through central pathological reading of the biopsies according to the updated Banff classification with semi-quantitative scoring for tubulitis (0, t1, t2), inflammation (0, i1, i2) and interstitial fibrosis and tubular atrophy (IFTA; 0, 1=<10% IFTA, 2 = 10-50% IFTA, 3= >50% IFTA) (14). All samples were collected at UCSF under IRB-approved protocols approved by The Human Research Protection Program (HRPP) of the University of California, San Francisco (UCSF) to allow analysis of bio-banked samples. CMV IgG status was measured on donor and recipient pairs and CMV PCR at 6 months post-transplant and with clinical suspicion in all the participants. All study subjects received antivirus prophylaxis until 6 months post-transplant. All patients or their guardians provided informed consent to participate in the research in full adherence to the Declaration of Helsinki. The clinical and research activities being reported are consistent with the Principles of the Declaration of Istanbul as outlined in the Declaration of Istanbul on Organ Trafficking and Transplant Tourism.
Blood samples (4.5 mL) were collected into a 5 mL plain glass Vacutainer® tubes, gently inverted, and incubated at room temperature for 30 min until the clot was formed. The sample was then centrifuged at 2000 × g for 5 min, the upper layer of serum was then transferred to a cryotube, and the remaining clot was stored in the original tube at −80 °C until use. Genomic DNA from whole-blood clot was extracted using the QIAsymphony DSP DNA Midi Kit (Qiagen, Valencia, CA). The DNA was quantified with NanoDrop and the extracted DNA was stored in -80°C until use for sequencing of the CDR3 regions of human TCRβ locus using the immunoSEQ assay. Extracted genomic DNA was amplified in a bias-controlled multiplex PCR with a pool of primer pairs targeting the V and J genes, as well as primers targeting reference genes to quantitate the total nucleated cells in each sample. PCR products were sequenced on an Illumina NextSeq System. Sequences were collapsed and filtered in order to identify and quantitate the absolute abundance of each unique TCRβ CDR3 region for further analysis as previously described (2, 3, 15–18). Twelve samples that had less than 500 total T cells were excluded from analysis due to insufficient DNA yields, resulting in 327 samples being included in the analyses (STA: 98 at baseline, 49 at 6M, AR: 92 at baseline, 43 at<6M, 35 at 6M, 49 at >6M AR time post-transplantation) (Table 2).
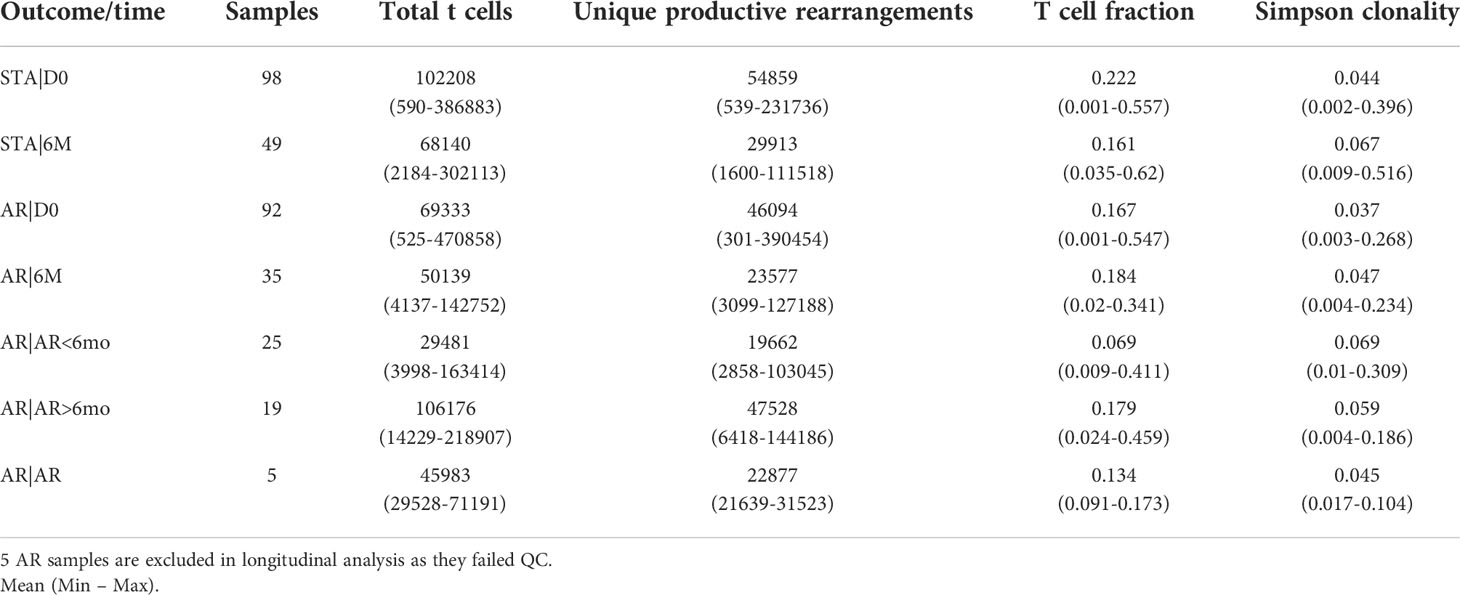
Table 2 Sequencing statistics.
TCRβ sequencing data that support the findings of this study have been deposited at the publicly available immuneACCESS platform at: https://clients.adaptivebiotech.com/pub/ DETERMINED ON ACCEPTANCE.
We compared TCRβ sequencing data from demographically matched renal transplant recipients who had either protocol or clinically indicated biopsies and paired blood samples for immune repertoire analysis; group comparisons were conducted between patients with histologically clean protocol biopsies (designated as the stable group (STA)) and histologically confirmed acute rejection as graded by the Banff classification on either protocol or indicated biopsies (designated as the acute rejection group (AR)).
Simpson clonality was calculated on productive rearrangements using the following equation: where pi is the proportional abundance of rearrangement i and N is the total number of rearrangements (19). Clonality values range from 0 to 1 and describe the shape of the frequency distribution: clonality values approaching 0 indicate a very even distribution of frequencies, whereas values approaching 1 indicate an increasingly asymmetric distribution in which a few clones are present at high frequencies.
TCFr, or the proportion of nucleated cells that are T cells, was computed using the number of T cells as determined by sequencing of productive TCRs and the number of nucleated cells by simultaneously amplifying a panel of reference genes present in all nucleated cells (19). We determine both the total number of T cells and the total number of nucleated cells using our bias controlled PCR methodology (18). Morisita Index was used to compare repertoires between longitudinal samples from the same individual. Morisita Index was calculated with the following formula: MI = ai equals the frequency of clone i in sample a, and bi equals the frequency of clone i in sample b. Morisita index takes into account sample overlap and change in clone frequencies with values that range from 1 (identical repertoires) to 0 (completely disparate repertoires) (20).
All statistical analysis was performed using standard packages in R version 3.6. Associations between groups were tested with either a Wilcoxon Rank Sum Test (two categorical groups) or a Kruskal-Wallis Test (three or more categorical groups). Pairwise comparisons after Kruskal-Wallis Tests were conducted with a Post-Hoc Dunn Test. Associations between two continuous variables were tested using Spearman’s Rank-Order Correlation. Associations between pairs of categorical groups were tested with a Fisher Exact Test.
The study cohort included a carefully selected set of peripheral blood samples obtained from demographically matched renal allograft patient groups with and without biopsy-confirmed acute renal allograft rejection (14), and with a contemporaneously obtained peripheral blood sample obtained prior to treatment intensification of graft rejection. These samples were selected from our larger biobank of over 3000 blood samples; we included 100 patients with that met definition of the STA group and 100 patients that met the definitions of the AR group, as described above. All patients had blood samples profiled prior to transplantation with the aim of evaluating changes if changes in the TCR immune repertoire could predict acute rejection after transplantation. In 50% of the patients, paired blood samples were also collected and profiled at the time of the post-transplant biopsy (STA or AR), to also evaluate if changes in the TCR immune repertoire persisted or evolved after engraftment and at acute rejection. The patient characteristics are summarized in Table 1. The study design is summarized in Figure 1. The recipients’ average age was 35±19 yrs. There were 117 males and 83 females. There were 21.5% living related donors, 26% living unrelated donors, and 52.5% deceased donors. All patients received induction with either thymoglobulin (52%) or simulect (48%), and maintenance immunosuppression was low dose maintenance steroids (5mg/day), tacrolimus (target maintenance trough levels after 6 months at 5-8 ng/ml), and mycophenolate mofetil.
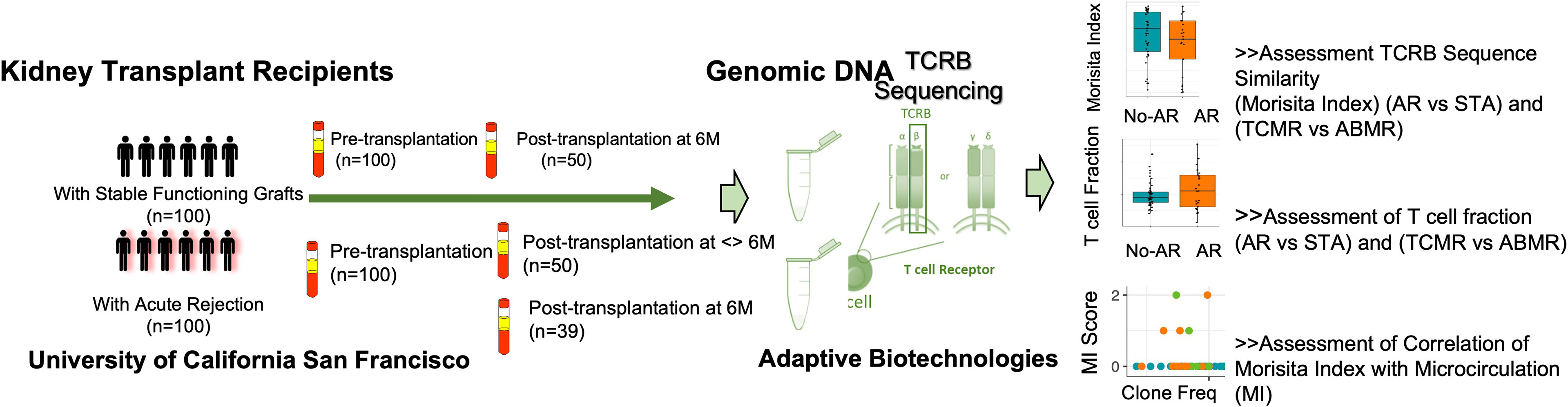
Figure 1 Study schematics. Validation of repertoire turnover and T cell fraction on post-transplant paired samples with and without acute rejection. Ninety-two AR samples and 98 STA transplant samples passed QC (>500 T cells) with sufficient T cell-derived DNA yield for analysis.
At pre-transplant phase, a greater diversity of the T-cell repertoire was observed in peripheral blood samples collected from subjects who developed acute rejection after transplant (Figure 2A). Using a previously published method (21), we inferred the CMV status of the subjects at baseline; however it was not able to differentiate between latent versus active infection. A significantly larger number of patients in the AR group were CMV naïve when compared to the STA group (51% vs.26%; Fisher exact P=0.0005). Also, a higher T cell clonality was seen in patients that were inferred CMV PCR positive (n=116) after transplant. (Figure 2B). We observed that there is an increase in the CMV positivity rate in the AR group (57% CMV positivity at the time of acute rejection vs 32% CMV positivity in the same patient’s pre-transplant (p= 0.03).
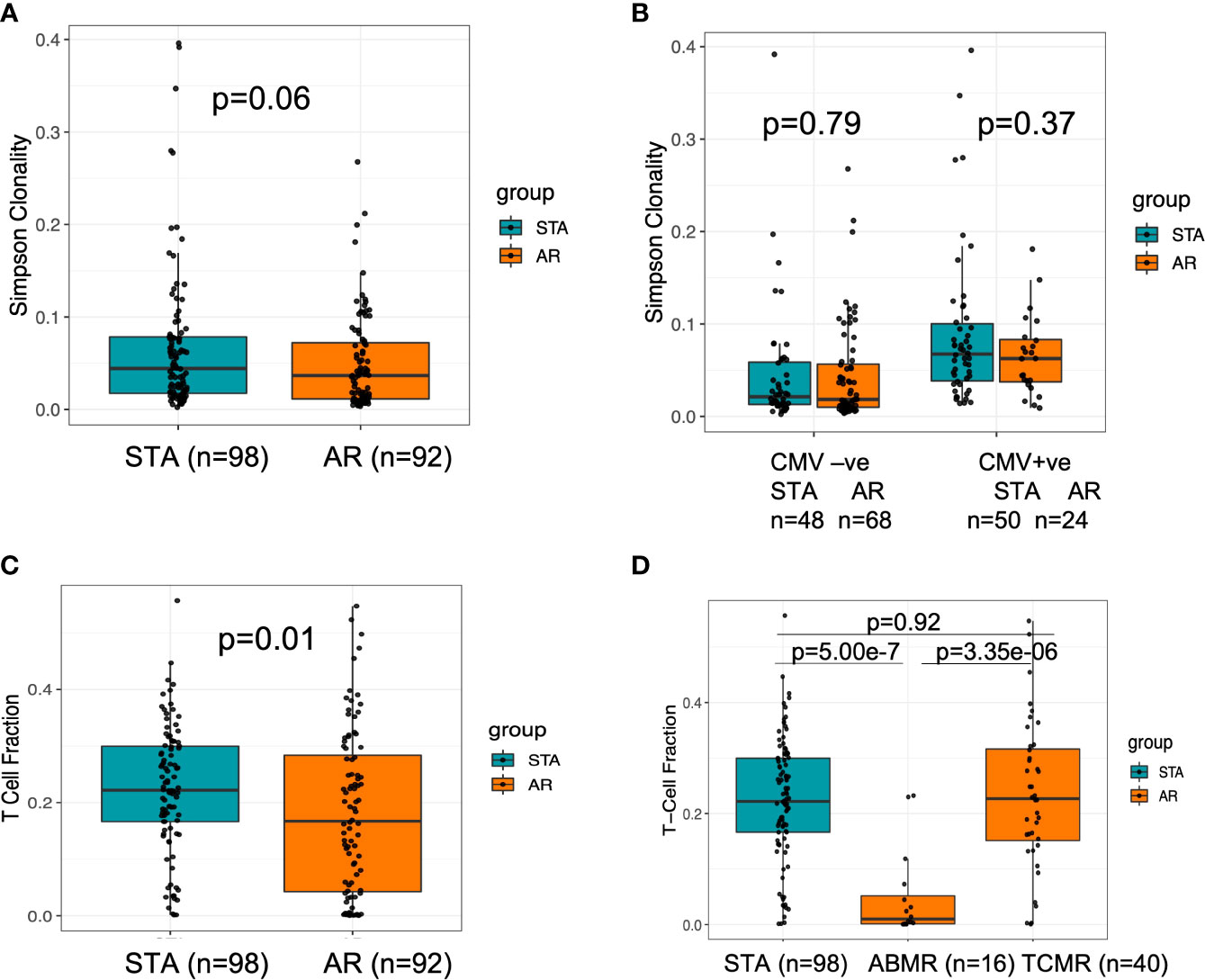
Figure 2 Baseline characteristics of TCR clonality and T cell fraction at baseline for transplant recipients who have future rejection and no rejection. (A) There was a trend towards higher clonality in stable subjects, which could indicate a more diverse repertoire at baseline in subjects who will experience acute rejection. (B) There was no difference in baseline repertoire clonality between the groups with or without CMV positivity. (C) When assessed the baseline T cell fraction in stable compared to acute rejection subjects, subjects with lower T cell fractions at baseline are at increased risk of rejection (p=0.01). (D) When we analyzed for T-cell fraction among clean TCMR and ABMR cases, we observed a significant difference between the two types of rejection cohorts (Kruskal Wallis p=4.03e-06) with a lower value in ABMR relative to TCMR using a post-hoc Dunn test p=3.35e-6.
We further assessed the patterns of V and J TCR gene usage within the baseline samples to identify differential gene usage, which may be associated with increased risk of AR (Supplemental Figures 1A, B). We observed increased use of TCRBV01 and TCRBJ01-02 in subjects with AR (p<0.05, Wilcoxon rank sum test). Overall, the magnitude of the difference may not be sufficient alone to be predictive of outcomes, as it may also reflect variations in HLA types among individuals in this data set enriched on patients who reside on the US pacific west coast, this observation requires further validation.
T-cell fraction (TCFr), the proportion of nucleated cells that are T cells, was determined as the number of T cells out of the total number of nucleated cells in the sample (similar in concept to an estimation of CD3+ T cells by flow sorting) (19); this denotes the percentage of T cells among all nucleated cells in the blood. We found that subjects with lower TCFr at baseline were at increased risk of rejection and enriched in the AR cohort (p=0.01) (Figure 2C). Within the subjects in the AR cohort, no correlation between baseline TCFr and time to rejection was observed (spearman correlation, rho=-0.1 p=0.34). When we analyzed the pre-transplant T-cell fraction among patients who had biopsy-confirmed acute rejection classified by Banff (14) as either T cell-mediated rejection (TCMR) or antibody-mediated rejection (ABMR) cases, we observed a significant difference between the two types of rejection cohorts (Kruskal Wallis p=4.03e-06) with a lower TCFr value in ABMR using a post-hoc Dunn test p=3.35e-6 (Figure 2D).
To compare for possible confounders, we compared whether baseline T-cell fraction varied by sex, age or race. We did not observe significant differences between sex (M vs. F) or age (<=37 vs. 38+), p>0.05 wilcox rank sum test. We observed a sharp rise in TCFr in the AR cohort, specifically for patients who had late acute rejections, after the first 6 months post-transplantation (log2-fold change median STA: - 0.34, median<6 months AR: 0.59, median >6 months AR: 3.52; post-hoc Dunn test, adjusted P=0.0037 vs. AR<6mo, P=7.4e-5 vs STA) (Figure 3A). When we further stratified rejection patients into ABMR and non-ABMR, irrespective of the time to rejection, TCFr was significantly increased in the ABMR group (AR ABMR vs. STA, Wilcoxon P=0.04, vs. AR non-ABMR vs. STA Wilcoxon p=0.56) (Figure 3B). Overall, 70.5% of AR patients had an increase in TCFr post-transplant, compared to 46.9% in STA patients (Fisher exact, p=0.03) (Figure 3C). In fact, this is because many AR cohort patients had very low baseline TCFr that sharply increased at an average of >10 fold at time of biopsy confirmed rejection. In contrast to TCFr, when we performed a similar analysis for TCR repertoire clonality, we observed no difference between subjects in the AR and STA cohorts (Supplemental Figure 2), suggesting that the expansion in TCFr is likely due to an overall increase in the T-cell pool rather than just an expansion of the highest-frequency clones.
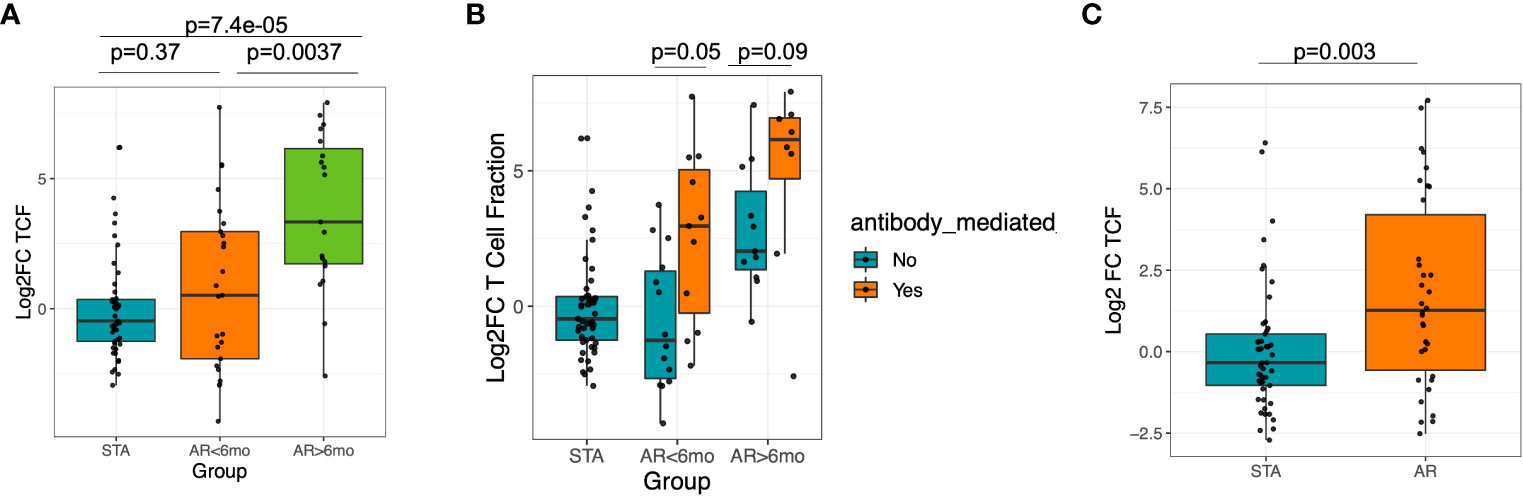
Figure 3 Significant increase in T-cell fraction at late rejection and in ABMR. (A) Increase of T-cell fraction is significant in late rejection cases >6 mo post-transplantation. (B) There is increase in T-cell fraction in ABMR compared to non-ABMR samples. (C) There was an increased peripheral T-cell fraction among AR subjects compared to STA among AR samples collected at 6 mo post-tx.
T-cell repertoire turnover was measured using Morisita Index (22), which is based on comparing the number and frequency of clones shared between the two samples. We assessed the evolution of TCR repertoire turnover by comparing paired values from the baseline samples and samples collected post-transplant for both STA patients and AR patients, where both samples had greater than 500 T cells. Because repertoire turnover can be influenced by time, we further divided the AR group based on whether their AR event occurred before or after 6 months post-transplant. Increased repertoire turnover was highest in the AR cohort (R=-0.33, p=0.029) (Supplemental Figure 3), with highest values for those patients with late rejections after 6 months post -transplant (median Morisita Index for STA: 0.73, median Morisita Index for AR less than 6 months post transplantation: 0.61, median MI for AR post 6 months post transplantation: 0.31, Kruskal-Wallis p=0.004) (Figure 4A). To further investigate whether there were clinical characteristics associated with patients that had the highest turnover, we subdivided patients that had ABMR, and found no statistical significance with rejection type (Figure 4B). This suggests that high repertoire turnover is generally associated with rejection and not just in patients with antibody-mediated rejection, irrespective of the time to acute rejection (p = 0.0016, adjusted p, post-hoc Dunn test) (Figure 4C).

Figure 4 Morisita Index which measures similarity based on the number of shared sequences between two populations as well as how well represented those overlapping sequences are within the two populations was low in AR and in antibody mediated rejection. (A) The T cell repertoire turnover is higher (with low Morisita Index) in patients with AR at > 6 mo post transplantation. (B) The turnover of TCR was more pronounced in ABMR compared with patients with STA and TCMR. (C) There was a greater repertoire turnover at AR event compared to STA at matching post-tx timepoint at 6 mo.
Comparing V and J gene usage post-transplant we observed a slightly greater usage of TCRBV18 in STA patients; however, this was not significant when correcting for multiple testing. No other TCRβ V gene showed differential enrichment (Supplemental Figures 4A, B). Together these findings suggest that measuring the TCR immune repertoire changes in an isolated post-transplant sample will likely be insufficient to predict rejection and integrating changes between the pre-transplant or baseline blood sample and a post-transplant blood sample will be more valuable to to evaluate the clinical impact of the repertoire dynamics.
Microcirculation Inflammation (MI), which is a cumulative score that includes glomerulitis (gs) and peritubular capillaritis (ptc), has been associated with worse outcomes in kidney transplantation (23). A significant correlation was observed between the MI score and Morisita Index in samples taken at post-transplant (spearman’s Rho=-0.27, p=0.0078, Figure 5). Of the post-transplant samples with a Morisita index less than 0.3, 43.5% of patients had a MI>0 compared to 15.7% of patients with an MI=0 (Fisher Exact Test, p=0.009). This suggests that greater repertoire turnover might be associated with more severe rejection.
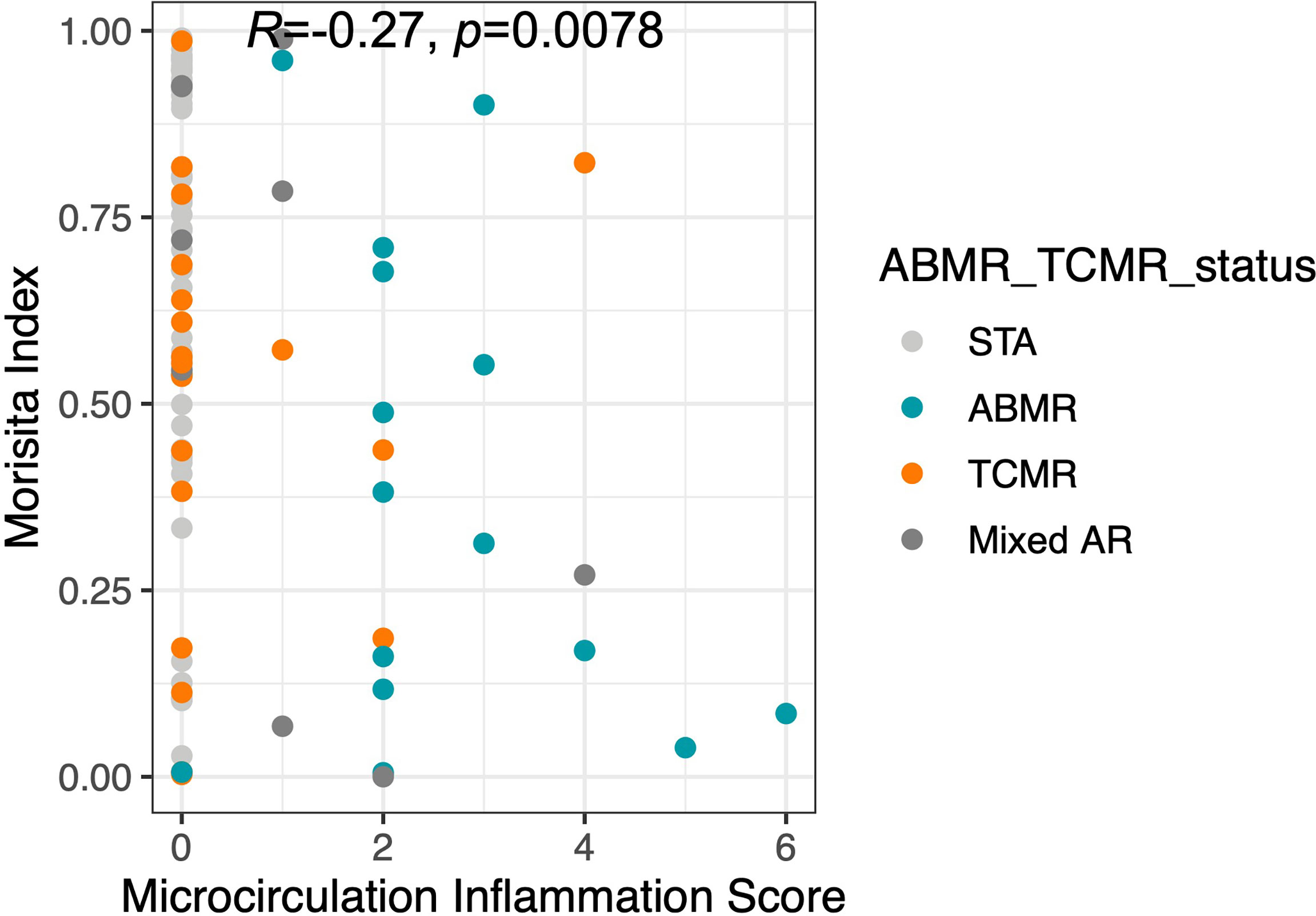
Figure 5 The Morisita Index inversely proportional to microcirculation inflammation. The finding of increased TCR turnover in terms of low Morisita Index among AR (ABMR, TCMR, Mixed AR) patients was further demonstrated by a significant correlation.
This study provides data on TCR immune repertoire sequencing on the largest cohort of kidney transplant recipients to date, to evaluate the changes in TCR before and after transplantation, by analysis of peripheral blood samples paired with transplant biopsies, and paired peripheral blood samples from the same transplant patients, before and after engraftment, using highly validated and demographically matched STA and AR cohorts. Using sequencing of the third complementarity-determining region (CDR3) of the TCRβ chain of the T-cell receptor from 323 blood samples collected from 200 kidney transplant recipients, we report multiple significant observations including associations between AR and Morisita Index and TCFr. Patients with acute rejection had lower (TCFr) before transplantation, followed by greater repertoire turnover and increased TCFr at the time of acute rejection after transplantation. Repertoire clonality is largely driven by the highest frequency clones, thus while there is significant repertoire turnover in patients with rejection, the observed lack of change in clonality indicates the acute rejection is driven by global changes in the TCR repertoire and not specifically by an increase in the highest frequency clones, which are most likely donor reactive. We observe that same repertoire of immunoreactive clones appear to continue to be immunodominant during the post-transplant rejection, even though there is repertoire turnover with regards to clone frequency. Given this observation, one of the reasons for the lower TCFr association with higher risk of post-transplant rejection can be hypothesized to be due to heterologous immunity where cross reactivity with pre-transplant auto-antigens results in increased reactivity to donor allo-specific antigens after transplant, and the evolution of rejection.
Our cohort had a an almost two-fold higher proportion of CMV-ve recipients pre-transplant in the rejection group (51% vs.26%), as predicted by TCRSeq. We recognize that CMV-ve recipients overall have a higher risk of CMV infection after transplant, and that there is an increase in the CMV positivity rate in the AR group. As there are known associations between clinical (24) and sub-clinical (25) CMV infection and acute rejection, these observations are relevant. We hypothesize that recipient CMV serostatus may be an independent factor that can influence acute rejection outcomes through sub-clinical CMV viral replication. Association analysis on baseline serostatus on this and a previous study showed an association with computationally predicted CMV status (21).
TCFr was significantly increased in late rejection cases >6 months post-transplantation and in ABMR. We did not observe significant differences in baseline or post-transplant metrics as single time point metrics, demonstrating the importance of longitudinal tracking. The most significant dynamic trends are observed in ABMR patients with low baseline TCFr that undergo large increases in TCFr and high repertoire turnover post-transplant. This might result from an expansion of CD4+ T cells, otherwise observed in ABMR (26–28), but confirmation of this will require further investigation, such as fluorescence-activated cell sorting (FACS) or CyTOF to evaluate the relative contributions of helper and cytotoxic T cells in these rejection episodes with sharp increase in TCFr. The Morisita Index was inversely proportional to MI, and had the ability to predict the mechanism of rejection, i.e. T cell versus antibody-mediated rejection, though this association was expected. These observed associations of TCR immune repertoire changes and late rejection and ABMR, may be explained by the chronicity of allo-immune exposure, the reduction in immunosuppression over time with reduction of immunosuppression target trough levels after 6 months post-transplant, as well as greater intensity of alloimmune injury in ABMR.
Despite the enormous amount of knowledge and data gained form this study, there are some intrinsic limitations as the data was generated on peripheral blood, and we did not have access to profiling paired kidney tissue and/or the draining lymphoid tissue where the immune response could be different or more amplified. Further studies will be required to evaluate changes in the immune repertoire specific to the recovery of T cells following T cell depleting induction such as thymoglobulin, and the inter-individual variability of T cell recovery and TCFr. Further independent validation studies with prospective and serial immune repertoire analysis of the TCR are warranted to validate the clinical utility of serial TCRSeq for ABMR and late onset acute rejection.
In conclusion, this study validated that detecting repertoire changes correlate with post-transplant rejection episodes suggesting that T-cell receptor sequencing (10) may provide recipient pre-transplant and post-transplant predictors of rejection risk. This assay has the potential to be utilized in immunosuppression management decisions at and after engraftment, based on dramatic increases in TCRf and/or repertoire turnover, where the identification of high-cell repertoire turnover post-transplant suggests the expansion of donor antigen-restricted, alloreactive T cells. Additional work is underway to independently validate these results in new patient sets to further decipher T-cell antigen recognition donor-stimulated proliferation of recipient cells by TCR Seq as well as by flow cytometry to further understand the clonotypic and turnover states that will help to identify dominant epitopes for prediction of renal transplant rejection risk prior to clinical deterioration of graft function. In addition, we are working on evaluating if any difference in TCFr exists in between the recipients with pre-emptive transplants compared to those who are receiving dialysis therapy.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by University of California San Francisco (Study ID- #14-13573). The patients/participants provided their written informed consent to participate in this study.
CMV Systems Immunobiology Group: Richard Ahn, Janice Arakawa-Hoyt, Patrick Boada, Jenny Brook, Suphamai Bunnapradist, Izabella Damm, Nakul Datta, Mario Deng, Don J. Diamond, Janette Gadzhyan, David Elashoff, David Gjertson, Alexander Hoffmann, Kenichi Ishiyama, Maggie Kerwin, Lewis L. Lanier, Megan Llmas, Erik Lum, Tariq Mukatash, Harry Pickering, Zach Qian, Michelle Ramirez, Rodney Rodgers, Elaine F. Reed, Minnie M. Sarwal, Maura Rossetti, Dmitri Rychov, Marina Sirota, Joanna Schaenman, Swastika Sur, Subha Sen, Tara Sigdel, Danielle Sim, Praveena Velperusiva, Otto O. Yang.
TS, JH, HR, and MS designed the study, PF, JL, ID, MK, and TS generated the data, TS, PF, MS and MS analyzed the data. All authors participated in manuscript writing. All authors contributed to the article and approved the submitted version.
This study was supported by a National Institutes of Health grant U19 AI128913 and 3U19AI128913-03S3 to MS.
We acknowledge help from Stephanie Bien in manuscript revision. We acknowledge the kidney transplant recipients who consented to participate in this study. We acknowledge Dr. Zoltan Laszik (UCSF) for pathology scores and Dr. Priyanka Rashmi for critically reading the manuscript.
Authors PF, JH, and HR were employed by Adaptive Biotechnologies.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1012042/full#supplementary-material
1. Nankivell BJ, Alexander SI. Rejection of the kidney allograft. N Engl J Med (2010) 363:1451–62. doi: 10.1056/NEJMra0902927
2. Robins HS, Campregher PV, Srivastava SK, Wacher A, Turtle CJ, Kahsai O, et al. Comprehensive assessment of T-cell receptor beta-chain diversity in alphabeta T cells. Blood (2009) 114:4099–107. doi: 10.1182/blood-2009-04-217604
3. Robins H, Desmarais C, Matthis J, Livingston R, Andriesen J, Reijonen H, et al. Ultra-sensitive detection of rare T cell clones. J Immunol Methods (2012) 375:14–9. doi: 10.1016/j.jim.2011.09.001
4. Miqueu P, Degauque N, Guillet M, Giral M, Ruiz C, Pallier A, et al. Analysis of the peripheral T-cell repertoire in kidney transplant patients. Eur J Immunol (2010) 40:3280–90. doi: 10.1002/eji.201040301
5. Alachkar H, Mutonga M, Kato T, Kalluri S, Kakuta Y, Uemura M, et al. Quantitative characterization of T-cell repertoire and biomarkers in kidney transplant rejection. BMC Nephrol (2016) 17:181. doi: 10.1186/s12882-016-0395-3
6. Guillet M, Brouard S, Gagne K, Sebille F, Cuturi MC, Delsuc MA, et al. Different qualitative and quantitative regulation of V beta TCR transcripts during early acute allograft rejection and tolerance induction. J Immunol (2002) 168:5088–95. doi: 10.4049/jimmunol.168.10.5088
7. Morris H, DeWolf S, Robins H, Sprangers B, LoCascio SA, Shonts BA, et al. Tracking donor-reactive T cells: Evidence for clonal deletion in tolerant kidney transplant patients. Sci Trans Med (2015) 7:272ra210. doi: 10.1126/scitranslmed.3010760
8. Dziubianau M, Hecht J, Kuchenbecker L, Sattler A, Stervbo U, Rodelsperger C, et al. TCR repertoire analysis by next generation sequencing allows complex differential diagnosis of T cell-related pathology. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surgeons (2013) 13:2842–54. doi: 10.1111/ajt.12431
9. Lai L, Wang L, Chen H, Zhang J, Yan Q, Ou M, et al. T Cell repertoire following kidney transplantation revealed by high-throughput sequencing. Transplant Immunol (2016) 39:34–45. doi: 10.1016/j.trim.2016.08.006
10. Aschauer C, Jelencsics K, Hu K, Heinzel A, Vetter J, Fraunhofer T, et al. Next generation sequencing based assessment of the alloreactive T cell receptor repertoire in kidney transplant patients during rejection: A prospective cohort study. BMC Nephrol (2019) 20:346. doi: 10.1186/s12882-019-1541-5
11. DeWolf S, Grinshpun B, Savage T, Lau SP, Obradovic A, Shonts B, et al. Quantifying size and diversity of the human T cell alloresponse. JCI Insight (2018) 3(15):1–17. doi: 10.1172/jci.insight.121256
12. Aschauer C, Jelencsics K, Hu K, Heinzel A, Gregorich MG, Vetter J, et al. Prospective tracking of donor-reactive T-cell clones in the circulation and rejecting human kidney allografts. Front Immunol (2021) 12:750005. doi: 10.3389/fimmu.2021.750005
13. Pineda S, Sigdel TK, Liberto JM, Vincenti F, Sirota M, Sarwal MM. Characterizing pre-transplant and post-transplant kidney rejection risk by b cell immune repertoire sequencing. Nat Commun (2019) 10:1906. doi: 10.1038/s41467-019-09930-3
14. Roufosse C, Simmonds N, Clahsen-van Groningen M, Haas M, Henriksen KJ, Horsfield C, et al. A 2018 reference guide to the banff classification of renal allograft pathology. Transplantation (2018) 102:1795–814. doi: 10.1097/TP.0000000000002366
15. Rosati E, Dowds CM, Liaskou E, Henriksen EKK, Karlsen TH, Franke A. Overview of methodologies for T-cell receptor repertoire analysis. BMC Biotechnol (2017) 17:61. doi: 10.1186/s12896-017-0379-9
16. Thome JJ, Grinshpun B, Kumar BV, Kubota M, Ohmura Y, Lerner H, et al. Longterm maintenance of human naive T cells through in situ homeostasis in lymphoid tissue sites. Sci Immunol (2016) 1(6):1–11. doi: 10.1126/sciimmunol.aah6506
17. Hsu M, Sedighim S, Wang T, Antonios JP, Everson RG, Tucker AM, et al. TCR sequencing can identify and track glioma-infiltrating T cells after DC vaccination. Cancer Immunol Res (2016) 4:412–8. doi: 10.1158/2326-6066.CIR-15-0240
18. Carlson CS, Emerson RO, Sherwood AM, Desmarais C, Chung MW, Parsons JM, et al. Using synthetic templates to design an unbiased multiplex PCR assay. Nat Commun (2013) 4:2680. doi: 10.1038/ncomms3680
19. Pruessmann W, Rytlewski J, Wilmott J, Mihm MC Jr, Attrill GH, Dyring-Andersen B, et al. Molecular analysis of primary melanoma T cells identifies patients at risk for metastatic recurrence. Nat Cancer (2020) 1:197–209. doi: 10.1038/s43018-019-0019-5
20. Reuben A, Gittelman R, Gao J, Zhang J, Yusko EC, Wu CJ, et al. TCR repertoire intratumor heterogeneity in localized lung adenocarcinomas: An association with predicted neoantigen heterogeneity and postsurgical recurrence. Cancer Discovery (2017) 7:1088–97. doi: 10.1158/2159-8290.CD-17-0256
21. Emerson RO, DeWitt WS, Vignali M, Gravley J, Hu JK, Osborne EJ, et al. Immunosequencing identifies signatures of cytomegalovirus exposure history and HLA-mediated effects on the T cell repertoire. Nat Genet (2017) 49:659–65. doi: 10.1038/ng.3822
22. Morisita M. Measuring of the Dispersion and Analysis of Distribution Patterns: Kyushu University. Series E: Biology (1959) 2, 215–35.
23. de Kort H, Willicombe M, Brookes P, Dominy KM, Santos-Nunez E, Galliford JW, et al. Microcirculation inflammation associates with outcome in renal transplant patients with de novo donor-specific antibodies. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surgeons (2013) 13:485–92. doi: 10.1111/j.1600-6143.2012.04325.x
24. Toupance O, Bouedjoro-Camus MC, Carquin J, Novella JL, Lavaud S, Wynckel A, et al. Cytomegalovirus-related disease and risk of acute rejection in renal transplant recipients: a cohort study with case-control analyses. Transpl Int (2000) 13:413–9. doi: 10.1111/j.1432-2277.2000.tb01019.x
25. Li L, Chaudhuri A, Weintraub LA, Hsieh F, Shah S, Alexander S, et al. Subclinical cytomegalovirus and Epstein-Barr virus viremia are associated with adverse outcomes in pediatric renal transplantation. Pediatr Transplant (2007) 11:187–95. doi: 10.1111/j.1399-3046.2006.00641.x
26. Walters GD, Vinuesa CG. T Follicular helper cells in transplantation. Transplantation (2016) 100:1650–5. doi: 10.1097/TP.0000000000001217
27. Susal C, Slavcev A, Pham L, Zeier M, Morath C. The possible critical role of T-cell help in DSA-mediated graft loss. Transpl Int (2018) 31:577–84. doi: 10.1111/tri.13126
Keywords: kidney transplantation, TCR sequencing, acute rejection, immune repertoire, T cell-mediated rejection, antibody-mediated rejection
Citation: Sigdel TK, Fields PA, Liberto J, Damm I, Kerwin M, Hood J, Towfighi P, Sirota M, Robins HS and Sarwal MM (2022) Perturbations of the T-cell immune repertoire in kidney transplant rejection. Front. Immunol. 13:1012042. doi: 10.3389/fimmu.2022.1012042
Received: 05 August 2022; Accepted: 26 October 2022;
Published: 16 November 2022.
Edited by:
Lin Zhong, Shanghai General Hospital, ChinaReviewed by:
Jonathan Scott Maltzman, Stanford University, United StatesCopyright © 2022 Sigdel, Fields, Liberto, Damm, Kerwin, Hood, Towfighi, Sirota, Robins and Sarwal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Minnie M. Sarwal, bWlubmllLnNhcndhbEB1Y3NmLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.