 Hugo L. Corrêa1Lysleine A. Deus1Thaís B. Araújo1Andrea L. Reis1Carlos E. N. Amorim2André B. Gadelha1,5,6Rafael L. Santos1Fernando S. Honorato1Daisy Motta-Santos3Carmen Tzanno-Martins4Rodrigo V. P. Neves1Thiago S. Rosa1*†
Hugo L. Corrêa1Lysleine A. Deus1Thaís B. Araújo1Andrea L. Reis1Carlos E. N. Amorim2André B. Gadelha1,5,6Rafael L. Santos1Fernando S. Honorato1Daisy Motta-Santos3Carmen Tzanno-Martins4Rodrigo V. P. Neves1Thiago S. Rosa1*†- 1Department of Physical Education, Catholic University of Brasília, Brasília, DF, Brazil
- 2Physical Education Department, Federal University of Maranhão, Maranhão, Brazil
- 3Pontifical Catholic University of Minas Gerais and Sports Department, EEFFTO, UFMG, Belo, Horizonte, Brazil
- 4Clinical Group Home Dialysis Center and RenalClass, São Paulo, Brazil
- 5Serviço de Preparação Física/COPSA/COSAU/DIGEP/SA/SG/Presidência da República, Brasília, Brazil
- 6Seção de Educação Física do Colégio Militar de Brasília, Brasília, Brazil
Background: The global burden of persistent COVID-19 in hemodialysis (HD) patients is a worrisome scenario worth of investigation for the critical care of chronic kidney disease (CKD). We performed an exploratory post-hoc study from the trial U1111-1237-8231 with two specific aims: i) to investigate the prevalence of COVID-19 infection and long COVID symptoms from our Cohort of 178 Brazilians HD patients. ii) to identify whether baseline characteristics should predict long COVID in this sample.
Methods: 247 community-dwelling older (>60 years) patients (Men and women) undergoing HD (glomerular filtration rate < 15 mL/min/1.73m2) with arteriovenous fistula volunteered for this study. All patients presented hypertension and diabetes. Patients were divided in two groups: without long-COVID and with long-COVID. Body composition, handgrip strength, functional performance, iron metabolism, phosphate, and inflammatory profile were assessed. Patients were screened for 11-months after COVID-19 infection. Results were considered significant at P < 0.05.
Results: We found that more than 85% of the COVID-19 infected patients presented a severe condition during the infection. In our sample, the mortality rate over 11-month follow was relatively low (8.4%) when compared to worldwide (approximately 36%). Long COVID was highly prevalent in COVID-19 survivors representing more than 80% of all cases. Phosphate and IL-10 were higher in the long COVID group, but only phosphate higher than 5.35 mg/dL appears to present an increased prevalence of long COVID, dyspnea, and fatigue.
Conclusion: There was a high prevalence of COVID-19 infection and long COVID in HD patients from the Brazilian trial ‘U1111-1237-8231’. HD clinics should be aware with phosphate range in HD patients as a possible target for adverse post-COVID events.
Introduction
Coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has impacted worldwide public health (1, 2). More than 6 million deaths were registered by May 2022, being more evident in Europe and Americas (https://covid19.who.int/; assessed 30 May 2022). Recent studies suggest that are several risk factors for severe or fatal COVID-19 that differs according to pre-existing diseases status (1, 3).
Chronic kidney disease (CKD) has emerged as an independent risk factor for the severeness of COVID-19 illness (1, 3–5). Such adverse condition appears to be related with impaired immune function, low-grade chronic inflammation, cardiovascular diseases, frailty, and endothelial dysfunction, which are enhanced according to the severity of CKD, especially in patients undergoing maintenance hemodialysis (HD) (6–8). The Centre for the Mathematical Modeling of Infectious Diseases COVID-19 working group (1) suggested CKD as an important risk factor for severe COVID-19. Furthermore, the ERA-EDTA Council (European Renal Association and European Dialysis and Transplantation Association) and the ERACODA Working Group demonstrated that HD (2021) (9), organ transplantation, and low renal function (estimated glomerular filtration rate < 30 mL/min/1.73m2) are associated with highest mortality risk from COVID-19. Carriazo et al. (7) showed that the increased mortality rate persists during the one-year after COVID-19 diagnosis in HD patients. Therefore, it is recommended that patients undergoing HD that were infected with COVID-19 should be monitored continuously to avoid future complications, especially in the first three months (8).
The long-term of new, returning, or ongoing health issues after the first infection with SARS-CoV-2 is recognized as post-acute COVID-19 syndrome conditions or long COVID (10–12). This scenario can last ranging from weeks to years. Post-COVID symptoms mostly reported are fatigue, fever, shortness of breath, cough, body aches, heart palpitations, neurological symptoms, diarrhea, stomach pain, and body aches (13). Noteworthy, subjects with underlying health conditions, including HD patients are likely to develop long-COVID (8, 11–14). Considering the global interest on how COVID-19 symptoms might persist in HD patients, as well as possible targets to avoid this condition, we performed an exploratory post-hoc study from the trial U1111-1237-8231 (15) with two specific aims: i) to characterize COVID-19 infection and long COVID symptoms from our Cohort of 178 Brazilians HD patients. ii) to identify whether baseline characteristics should predict long COVID in this sample. This study provides relevant information regarding the prevalence of COVID-19 and long COVID in HD patients and suggested phosphate and interleukin (IL-10) as possible targets associated with post-COVID conditions.
Methods
This study is a follow-up study of data from the trial U1111-1237-8231. This study has been conducted prospectively in hemodialysis clinics from Brazil and has been previous described (15). It is worth to state that this manuscript presents additional data from the study of 15. Briefly, this study covered 247 (two hundred and forty-seven) community-dwelling older patients undergoing HD (glomerular filtration rate < 15 mL/min/1.73m2) with arteriovenous fistula who volunteered for this study. All patients presented hypertension and diabetes. Eligibility criteria for participants were: (i) age equal to or older than 60 years; (ii) hemodialysis for at least 3 months; (iii) dialysis at least three times per week; and (iv) no significant medical complications in the last 3 months, except for vascular access correction. Exclusion criteria were: (i) systemic lupus erythematosus; (ii) congenital kidney malformation or some auto-immune disease that affects the kidneys; (iii) severe decompensated diabetes. Participants were informed about the procedures and possible risks of participation in the study. Before participation in the research project, each participant completed a medical history questionnaire and voluntarily signed a written informed consent form. The study was conducted according to the Declaration of Helsinki (1975). All methods and procedures were approved by the Local Human Research Ethics Committee, Brazil (no 08856012.6.0000.5505 and updated 23007319.0.0000.0029). Furthermore, a new protocol register number was made and approved for conducting the study with COVID-19 patients (no 47011221.2.0000.5086). After 11-month follow-up only 178 patients were analyzed for COVID-19 and long-COVID. All patients’ selection can be found in Figure 1.
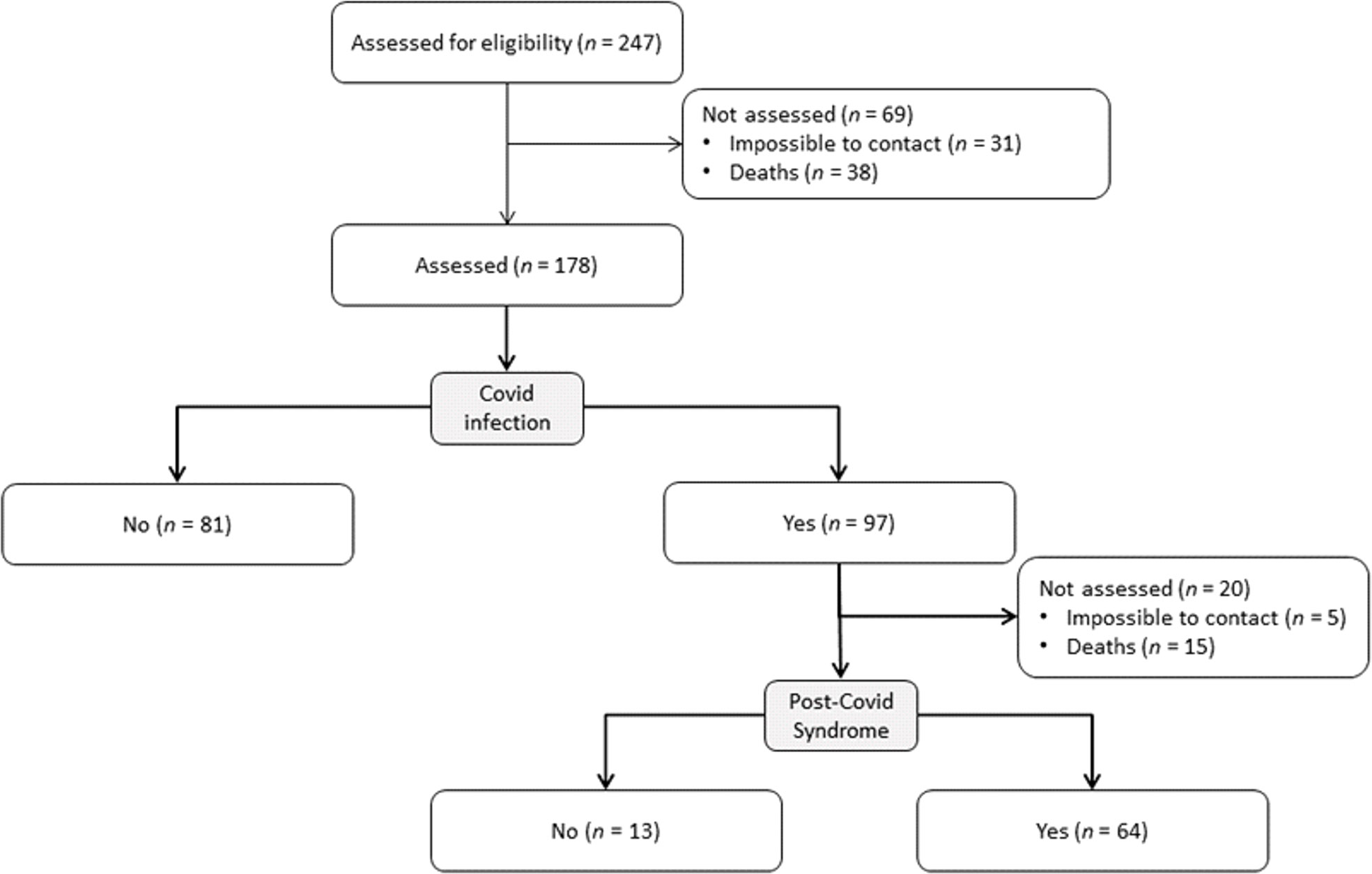
Figure 1 Participant’s flow-chart.
Anthropometric assessment
All subjects were weighed on a mechanical scale (Filizola®, São Paulo, Brazil), and height was measured with a stadiometer built into the scale (precision: 0.5 cm). Waist circumference was assessed at the level of umbilicus using an anthropometric tape (Sanny®, São Paulo, Brazil). Body composition was measured using a Prodigy Advance Plus (LUNAR,Corp/General Electric; Madison, Wisconsin, USA) dual-energy X-ray absorptiometry (DXA) according to previously specified procedures (16). All measurements were carried out by the same experienced researcher.
Handgrip strength and functional performance
Handgrip strength was measured with a hydraulic hand dynamometer (Jamar® - Sammons Preston, Bolingbrook, USA). According to the recommendations of the American Society of Hand Therapists, measurements were performed with participants in a sitting position, elbow joint at 90°, forearm in a neutral position, and wrist between 0° and 30° of extension. The best performance of three trials in the contralateral arm to the arteriovenous fistula was recorded and used for the present analyses (17, 18). Functional performance was evaluated by the Timed Up-and-Go (TUG) test and six-minute walking test (6MWT). Procedures were fully explained before the assessment, followed by a familiarization attempt as described elsewhere (19).
Medications in use
All patients had similar medication regimen. Briefly, for glucose control the most common treatment was long-acting insulin. Erythropoietin was administered raging from 50 to 100 UI/kg three times/week with constant adjustments for anemia control. Simvastatin, Pravastatin, Fluvastatin, and Rosuvastatin with the following doses/day: 5 – 20mg, 10 – 40mg, 80mg, 10 – 20mg, respectively. Phosphate binder Sevelamer was administered 800mg three times/day to control phosphate levels between 5.5 and 7.5mg/dL.
Blood collection
Venous blood samples were obtained from all patients to measure biochemical variables using dry and EDTA containing tubes. All blood was obtained before COVID infection. Samples were obtained in the morning (8 to 12 h of fasting) and all patients were instructed not to practice any physical activity for 48 h before. Samples were centrifuged at 1500 x g for 15 min; after processing, the specimens were aliquoted into cryovials and stored at -80° C.
Inflammatory profile
The systemic TNF-α, IL-6, and IL-10 levels were measured in triplicate by enzyme-linked immunosorbent assay (ELISA) kits from R&D Systems (Minneapolis, MN, USA) according to the manufacturer’s instructions. The detectable limits for TNF-α, IL-6, and IL-10 were 10, 18, and 0.2 pg,mL-1, respectively. The overall intra- and inter-assay CVs for inflammatory markers and hepcidin were in a range from 2.3 to 10%.
COVID and post-acute COVID-19 syndrome assessment
Covid diagnostic by PCR and severity, including hospitalizations, deaths, nursery, intensive care unit, and supplementary O2 was obtained through the 11-months follow-up by checking the medical records from the HD clinic. Long COVID symptoms were recorded by performing a semi-structured telephone call, conducted through all 11-months follow-up. During the interviews patients were asked if they are feeling dyspnea, dizziness, headache, myalgia, cognitive deficits, and fatigue. After that, the interviewer checked with the responsible person for the patient if all the symptoms are corrected recorded and if they were not evident before COVID infection. At least ten contact attempts were made to each volunteer with missed calls. All telephone calls were made by the same person, who had experience with telephone interviews (20). The long-term of new, returning, or ongoing health issues after the first infection with SARS-CoV-2 recognized as post-acute COVID-19 syndrome conditions or long COVID (10–12).
Statistical analysis
Descriptive characteristics are presented as means and standard deviations unless otherwise noted. The Shapiro–Wilk test and Levene were used to verify data distribution nature and homogeneity, respectively. X2 tests were performed to compare categorical variables, while continuous variables were tested for significance by performing a student t test to compare groups (with and without post-covid syndrome. The Receiver Operating Characteristic (ROC) curve was generated plotting sensitivity (y-axis) as a function of 1-specificity (x-axis). Sensitivity or true-positive points to the individual that was correctly diagnosed with the outcome by an indicator. 1-specificity or true-negative refers to the subjects that were wrongly diagnosed with the outcome by an indicator. In the present study, to be considered an indicator, the area under the ROC curve should be higher than 0.50 and lower than 1.00. Therefore, a larger area indicates a greater discriminatory power of the respective indicator. Herein the two elected indicators were phosphate and IL-10. To establish the cut-off point, was considered the closest value between sensitivity and 1-specificity not lower than 0.60. Furthermore, the odds ratio (95% confidence interval [CI]) were obtained for phosphate and IL-10 to verify the likelihood to present post-covid syndrome according to the cut-off points established for both variables.
After performing the aforementioned analysis, phosphate was elected as a possible predictor of the post-covid syndrome. Therefore, the subjects were subgrouped according to the cut-off points established by the ROC curve (group 1: phosphate <5.35; group 2: phosphate >5.35). For that purpose, the groups were than compared using a chi-squared test. Results were considered significant at P < 0.05, and all analysis were performed using IBM Corp. Released 2013. IBM SPSS Statistics for Windows, version 22.0. Armonk, NY: IBM Corp. And GraphPad Prism version 8.0.0 to Windows, GraphPad Software, San Diego, california, EUA, www.graphpad.com “.
Results
COVID infection occurs raging from April to December of 2020. The prevalence of COVID-19 in our Cohort was 54.5%. 87% were hospitalized, 91.6% needed nursery, 98.8% used supplementary O2, and 91.6% were hospitalized in an intensive care unit. Time of hospitalization ranged from 1 to 11 days (mean ± SD: 5.95 ± 3). Furthermore, patients were not vaccinated yet. As observed on Figure 1, there were 15 deaths (8.4%) from the patients infected with COVID-19 in an eleven-months follow-up. From the 77 survivors (79.38%), 64 developed long covid (83.12%). Approximately 30% of the patients presented at least four post-covid symptoms, which the most prevalent were dyspnea and fatigue (78 and 77%, respectively). No differences were found between men and women related to post-covid syndrome (P > 0.05). See Figure 2
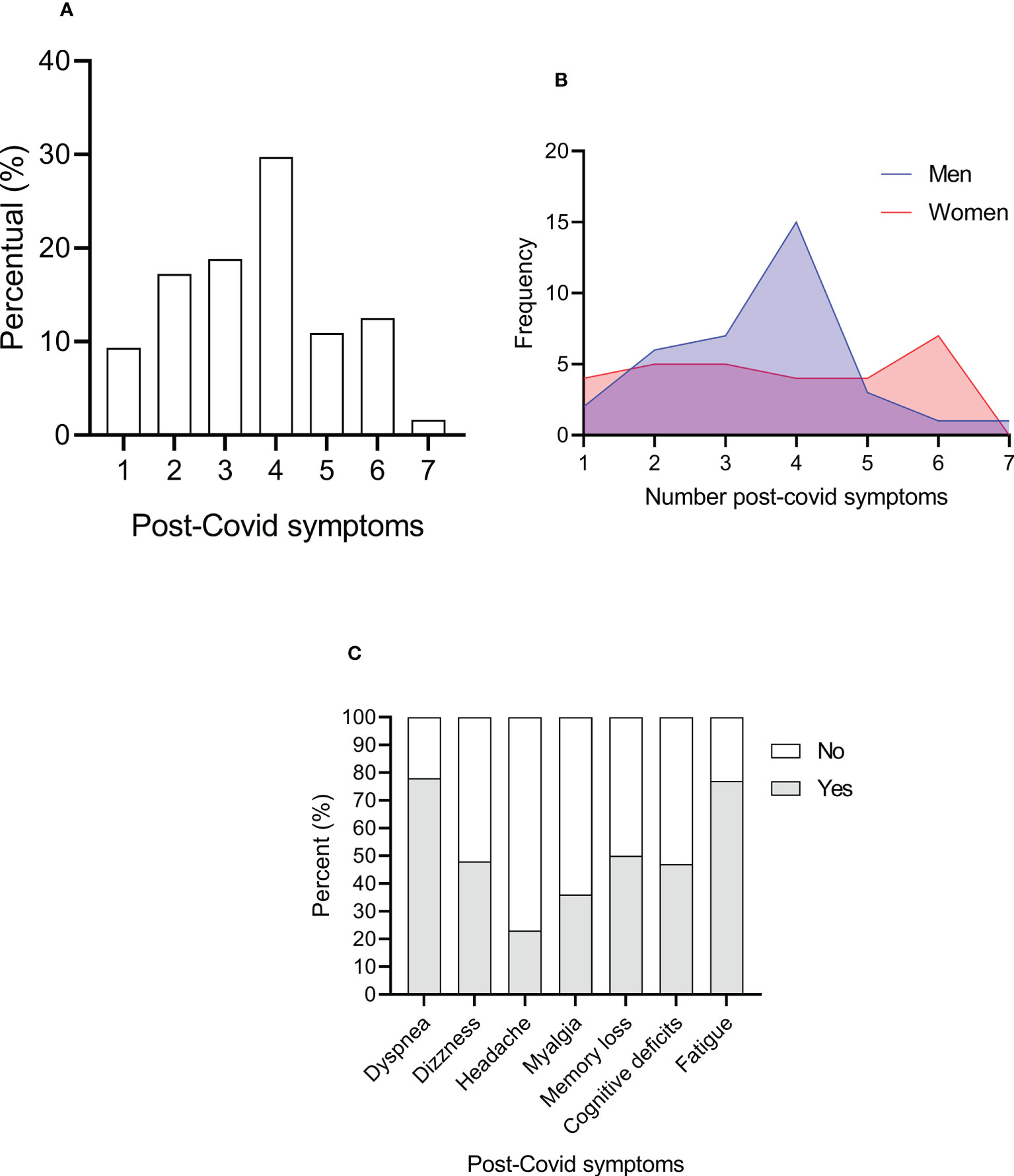
Figure 2 Percent of long covid symptoms (A), frequency of men and women for each number of post-covid symptoms, and frequency of each symptom in hemodialysis patients (B). Percent of each post-covid symptoms (C) .
Baselines characteristics stratified by the long covid diagnosis are described on Table 1. Patients that developed long covid demonstrated higher values of phosphate and IL-10 when compared to patients without long covid. In this context, a ROC curve was generated to verify the cut-off points of the aforementioned variables as possible risk factors for long covid (Table 2).
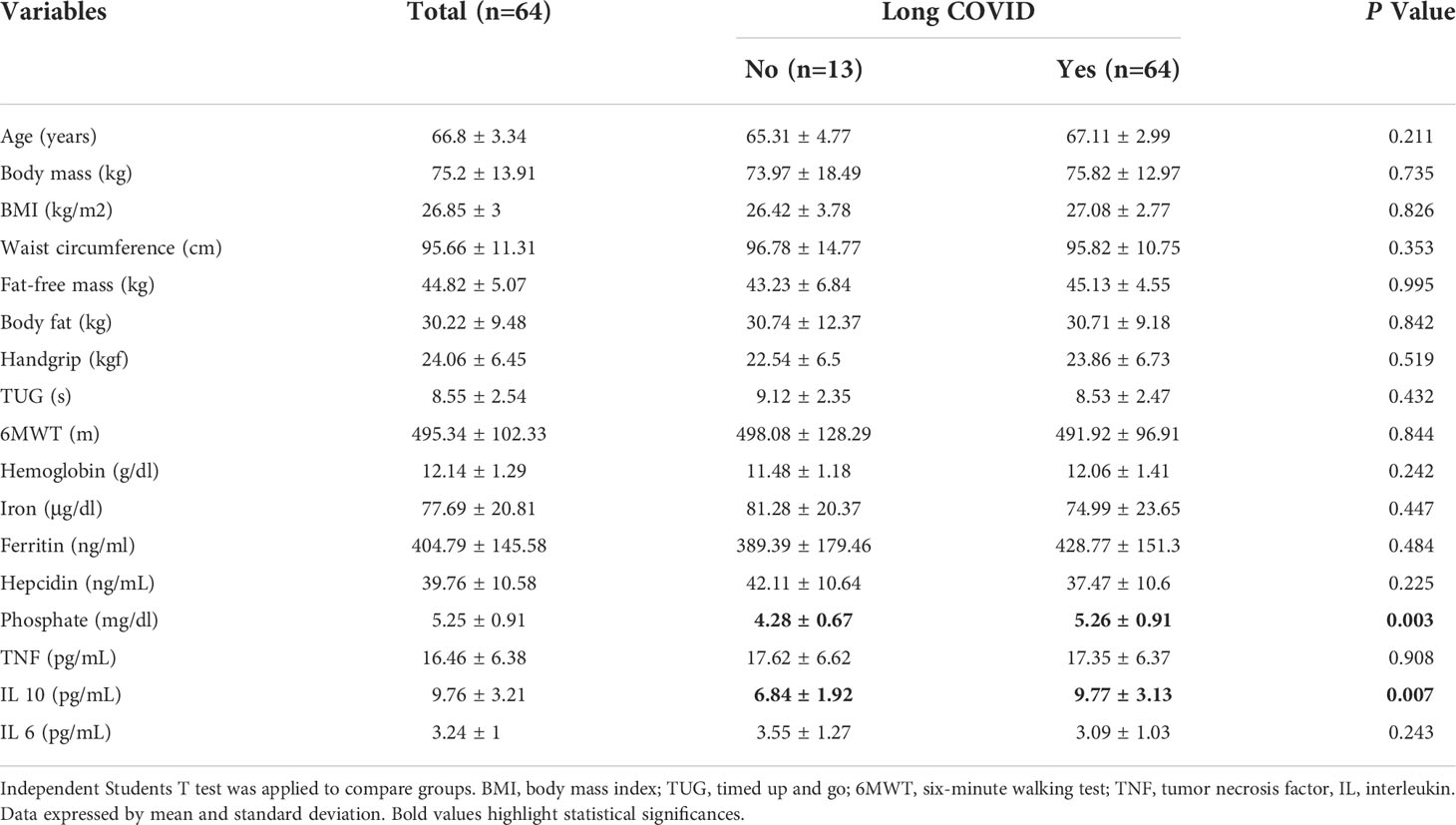
Table 1 Baseline characteristics stratified by the presence of long COVID.

Table 2 Area under the ROC curve and odds ratio in presenting post-covid syndrome.
The cut-off point stablished by the ROC curve for phosphate and IL-10 was 5.35 mg/dL and 9.75 pg/mL, respectively. Both variables seem to predict long covid in maintenance HD patients (area under the ROC curve higher than 0.50 and lower than 1.00). However, only phosphate presented a significant odds ratio (11.118%CI: 1.279 – 96.661). See Table 2. Noteworthy, IL-10 and phosphate levels from patients who did not survive were higher than the cut points proposed in the study: 11.25 ± 3.73 and 5.63 ± 0.87, respectively.
Patients with phosphate ≥ 5.35 mg/dL presented higher prevalence of long covid. Analyzing every symptom separately, it seems that subjects with higher values of phosphate are likely to present a higher prevalence of dyspnea and fatigue. See Table 3 and Figure 3. Correlation matrix between these variables is presented on Figure 2.

Table 3 Long COVID according with phosphate concentrations.
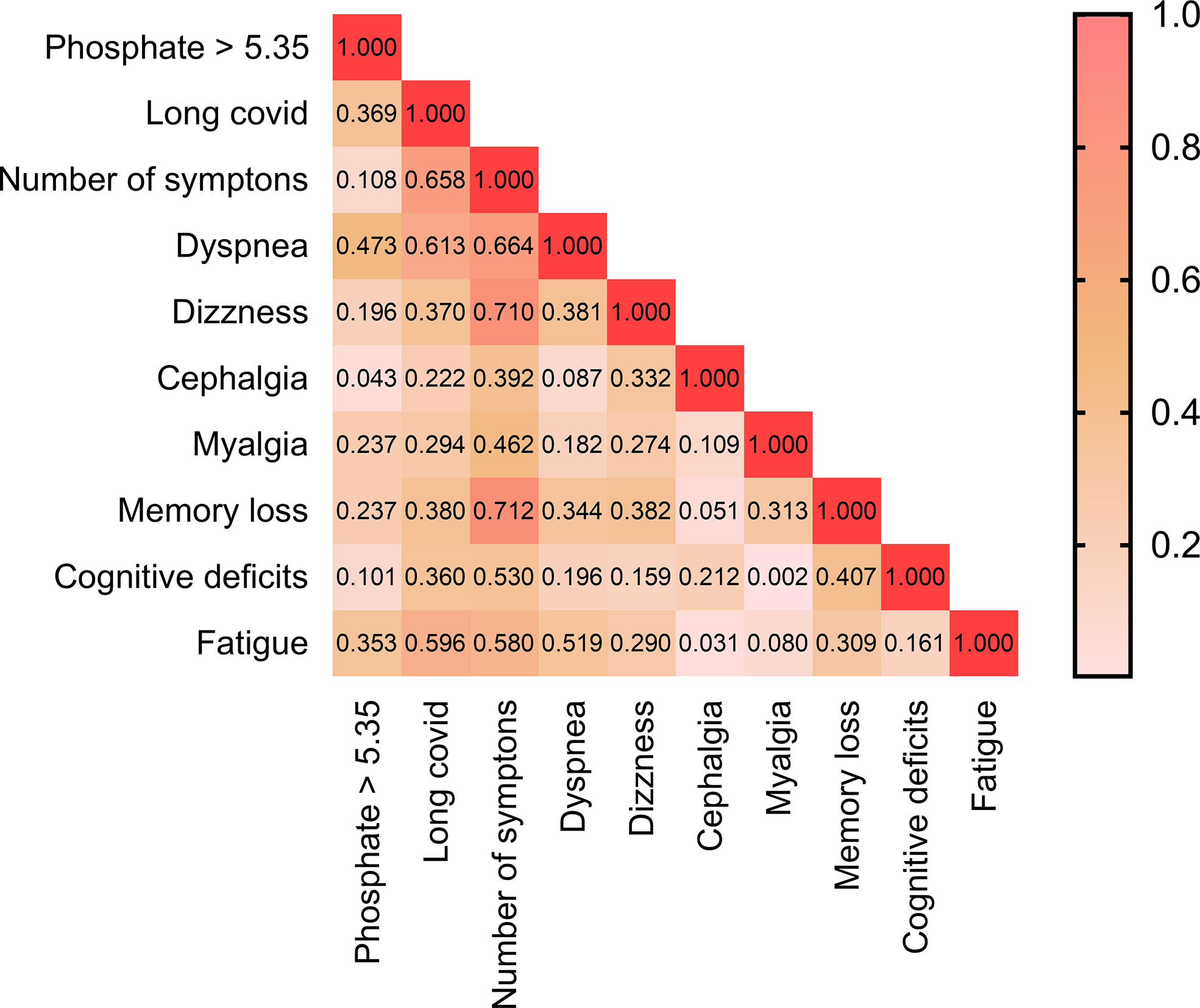
Figure 3 Heat map of the correlation matrix between phosphate ≥ 5.35 with each post COVID symptoms.
Discussion
This study sought to characterize COVID-19 infection and long COVID symptoms from our cohort of 178 Brazilians HD patients, and to identify whether baseline characteristics should predict long COVID in this sample. We found that more than 85% of the COVID-19 infected patients presented a severe condition during the infection (hospitalized, needed supplementary O2, nursery or hospitalized in an intensity unit care). In our sample, the mortality rate over 11-month follow was relatively low (8.4%) when compared to the present literature (approximately 36%) (7). However, long COVID was highly prevalent in COVID-19 survivors representing more than 80% of all cases. A key finding of the study was the association of baseline phosphate and IL-10 with long COVID, demonstrating that higher levels of these two variables might be a risk factor for post-COVID complications. We suggested that patients with phosphate higher than 5.35 mg/dL may present an increased prevalence of long COVID, dyspnea, and fatigue. Although our sample size was not robust, these results may motivate further prospective and randomized trial to investigate deepest this relation between increased phosphate and long COVID.
In COVID-19-infected patients without CKD, higher levels of phosphate appear to be a protective factor against pulmonary damage, COVID severity, and mortality (21–24). Javdani et al. (25) suggests that hypophosphatemia is associated with severe lung injures, while increased serum phosphate may be associated with better CT scan of lung outcomes. Wang et al. (24) verified that hypophosphatemia at admission may be associated with increased mortality. Xue et al. (22) indicated that the severity of COVID-19 might be linked with lower phosphate levels. By this scenario, it would be rationale to infer those higher levels of phosphate would protect HD patients from long COVID since post-covid symptoms are likely related to COVID severity and organ damage (1, 4, 12). However, due to the decreased number of nephrons, CKD patients develop a compensate mechanism for phosphate balance characterized by the increase of fibroblast growth factor – 23 (FGF-23), parathormone, and decreased Vitamin D (Kuro-o, 2013; 26, 27). This mechanism precedes a hyperphosphatemia since the residual renal function are insufficient to excrete phosphate, leading to bone mineral disorders, inflammation, and interstitial fibrosis in HD patients (Kuro-o, 2013; 26, 27).
McGovern et al. (28) verified that higher serum phosphate concentrations (>1.5 mmol/L or >4.65 mg/dL) is associated with increased cardiovascular risk in CKD stages 3-5 (odds ratio = 2.34; 95% confidence interval = 1.64 – 3.32). This same study demonstrated that subjects without CKD could also present increased cardiovascular risk related to phosphate. Furthermore, even in normal ranges, greater serum phosphate is associated with vascular and valvular calcification in CKD patients (29). Noteworthy, HD patients hospitalized with COVID-19 seems to present hyperphosphatemia (30). Taken together, all this evidence underpins the results of the present study, suggesting higher serum phosphate as a possible predictors of persistence COVID symptoms. In this regard, further studies should address the impact of phosphate on COVID-19 prognosis, and long COVID prevalence among HD patients. Although our study did not present mechanistic insights, the role of phosphate in a worst prognosis of COVID patients with HD, might be related to an increased systemic inflammation (21, 31).
A striking feature of COVID-19 severity is the ‘citokine storm’ (32, 33). This phenomenon has been attributed as a clinical condition caused by an hyperactivation of immune system associated with several diseases (32). It is known that some cytokines are elevated on cytokine storm, including IL-10, TNF, and IL-6 (32, 33). Furthermore, these cytokines appear to be higher on patients infected with COVID-19 hospitalized in intensive care units (2). Although IL-10 acts as an anti-inflammatory cytokine inhibiting TNF and IL-6, it increased concentrations in cytokine storm might be likely due to insufficient counterregulatory action to the proinflammatory proteins (32). However, another hypothesis was made based on recent studies rising IL-10 as a possible proinflammatory cytokine in COVID-19 burden, but this concept must be further tested in detail (34, 35). These findings support the elevated concentrations of serum IL-10 in patients that developed long COVID presented in the present study. Suggesting that baseline IL-10 levels might be associated with post COVID symptoms. These results should encourage further researchers in identifying whether IL-10 levels could predict COVID-19 complications and long COVID.
This study presents several limitations that should be considered: first, this is a follow-up study which were not designed to analyze COVID-19 or long COVID a priori. However, considering the global burden of persistent COVID-19 in HD patients, this is a topic worth of investigation in the critical care of CKD patients. Second, the small sample size limits our inference in the general population with HD. Third, the lack of more time points of analysis limits our observation of the phenomenon. Finally, the lack of nutrition control limit our results, and we encourage further studies to control this variable. Nonetheless, to our knowledge, this is the first study that screened COVID and long COVID in HD patients and identified two possible targets (phosphate and IL10) of post-covid symptoms in this population.
In sum, there was a high prevalence of COVID-19 infection and long COVID in HD patients from the Brazilian trial ‘U1111-1237-8231’. Further studies should give a special look on serum phosphate and IL-10 levels in HD patients as possible targets of persistent COVID symptoms and severity.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethic committee of Catholic University of Brasília. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HC, RN, LD, TA, AG, AR, RS, and TR: Conceptualization; HC, RN, LD, TA, AG, AR, RS, and TR: Data curation; HC: Formal analysis; CT-M and TR: Funding acquisition; HC, FH, RS, TA, DM-S, and TR: Investigation; Project administration; HC, DM-S, CT-M, CA, and TR: Roles/Writing - original draft; HC, DM-S, CA, and TR: Writing - review and editing. All authors contributed to the article and approved the submitted version.
Funding
TSR, HLC, TBA, and LAD were supported by a grant provided by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) – Finance Code 001 and National Council for Scientific and Technological Development (CNPq).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: A modelling study. Lancet Glob Health (2020) 8:e1003–17. doi: 10.1016/S2214-109X(20)30264-3
2. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
3. Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature (2020) 584:430–6. doi: 10.1038/s41586-020-2521-4
4. Cai R, Zhang J, Zhu Y, Liu L, Liu Y, He Q. Mortality in chronic kidney disease patients with COVID-19: A systematic review and meta-analysis. Int Urol Nephrol (2021) 53:1623–9. doi: 10.1007/s11255-020-02740-3
5. Flythe JE, Assimon MM, Tugman MJ, Chang EH, Gupta S, Shah J, et al. Characteristics and outcomes of individuals with pre-existing kidney disease and COVID-19 admitted to intensive care units in the United States. Am J Kidney Dis (2021) 77:190–203.e191. doi: 10.1053/j.ajkd.2020.09.003
6. Wang R, Liao C, He H, Hu C, Wei Z, Hong Z, et al. COVID-19 in hemodialysis patients: A report of 5 cases. Am J Kidney Dis (2020) 76:141–3. doi: 10.1053/j.ajkd.2020.03.009
7. Carriazo S, Mas-Fontao S, Seghers C, Cano J, Goma E, Avello A, et al. Increased 1-year mortality in haemodialysis patients with COVID-19: A prospective, observational study. Clin Kidney J (2022) 15:432–41. doi: 10.1093/ckj/sfab248
8. Demiray A, Kanbay A, Kanbay M. Long-term effect of COVID-19 infection on hemodialysis patients: Should we follow hemodialysis patients more closely? Clin Kidney J (2022) 15:369–71. doi: 10.1093/ckj/sfab265
9. Ortiz A, Cozzolino M, Fliser D, Fouque D, Goumenos D, Massy ZA, et al. Chronic kidney disease is a key risk factor for severe COVID-19: A call to action by the ERA-EDTA. Nephrol Dial Transplant (2021) 36:87–94. doi: 10.1093/ndt/gfaa314
10. Maestre-Muñiz MM, Arias Á., Mata-Vázquez E, Martín-Toledano M, López-Larramona G, Ruiz-Chicote AM, et al. Long-term outcomes of patients with coronavirus disease 2019 at one year after hospital discharge. J Clin Med (2021) 10:1–15. doi: 10.3390/jcm10132945
11. Och A, Tylicki P, Polewska K, Puchalska-Reglińska E, Parczewska A, Szabat K, et al. Persistent post-COVID-19 syndrome in hemodialyzed patients-a longitudinal cohort study from the north of Poland. J Clin Med (2021) 10:1–10. doi: 10.3390/jcm10194451
12. Willi S, Lüthold R, Hunt A, Hänggi NV, Sejdiu D, Scaff C, et al. COVID-19 sequelae in adults aged less than 50 years: A systematic review. Travel Med Infect Dis (2021) 40:101995. doi: 10.1016/j.tmaid.2021.101995
13. Shah W, Hillman T, Playford ED, Hishmeh L. Managing the long term effects of covid-19: Summary of NICE, SIGN, and RCGP rapid guideline. Bmj (2021) 372:n136. doi: 10.1136/bmj.n136
14. Ozturk S, Turgutalp K, Arici M, Gorgulu N, Tonbul HZ, Eren N, et al. The longitudinal evolution of post-COVID-19 outcomes among hemodialysis patients in Turkey. Kidney Int Rep (2022) 7, 1393–1405. doi: 10.1016/j.ekir.2022.03.017
15. Gadelha AB, Cesari M, Corrêa HL, Neves RVP, Sousa CV, Deus LA, et al. Effects of pre-dialysis resistance training on sarcopenia, inflammatory profile, and anemia biomarkers in older community-dwelling patients with chronic kidney disease: a randomized controlled trial. Int Urol Nephrol (2021) 53:2137–47. doi: 10.1007/s11255-021-02799-6
16. Neves RVP, Corrêa HL, Deus LA, Reis AL, Souza MK, Simões HG, et al. Dynamic not isometric training blunts osteo-renal disease and improves the sclerostin/FGF23/Klotho axis in maintenance hemodialysis patients: a randomized clinical trial. J Appl Physiol (1985) (2021) 130:508–16. doi: 10.1152/japplphysiol.00416.2020
17. Mathiowetz V, Weber K, Volland G, Kashman N. Reliability and validity of grip and pinch strength evaluations. J Handb Surg Am (1984) 9:222–6. doi: 10.1016/S0363-5023(84)80146-X
18. Corrêa HL, Rosa TDS, Dutra MT, Sales MM, Noll M, Deus LA, et al. Association between dynapenic abdominal obesity and inflammatory profile in diabetic older community-dwelling patients with end-stage renal disease. Exp Gerontol (2021) 146:111243. doi: 10.1016/j.exger.2021.111243
19. De Luca Corrêa H, Neves RVP, Deus LA, Reis AL, Raab ATO, Rodrigues-Silva PL, et al. MicroRNA levels in hemodialysis patients following resistance training: Associations with functional performance, inflammatory profile, sestrins-2, and nitric oxide. Exp Gerontol (2022) 162:111761. doi: 10.1016/j.exger.2022.111761
20. Frontera JA, Yang D, Lewis A, Patel P, Medicherla C, Arena V, et al. A prospective study of long-term outcomes among hospitalized COVID-19 patients with and without neurological complications. J Neurol Sci (2021) 426:117486. doi: 10.1016/j.jns.2021.117486
21. Yamada S, Tokumoto M, Tatsumoto N, Taniguchi M, Noguchi H, Nakano T, et al. Phosphate overload directly induces systemic inflammation and malnutrition as well as vascular calcification in uremia. Am J Physiol Renal Physiol (2014) 306:F1418–1428. doi: 10.1152/ajprenal.00633.2013
22. Xue X, Ma J, Zhao Y, Zhao A, Liu X, Guo W, et al. Correlation between hypophosphatemia and the severity of corona virus disease 2019 patients. MedRxiv. (2020). doi: 10.1101/2020.03.27.20040816
23. Van Kempen T, Deixler E. SARS-CoV-2: influence of phosphate and magnesium, moderated by vitamin d, on energy (ATP) metabolism and on severity of COVID-19. Am J Physiol Endocrinol Metab (2021) 320:E2–e6. doi: 10.1152/ajpendo.00474.2020
24. Wang R, He M, Kang Y. Hypophosphatemia at admission is associated with increased mortality in COVID-19 patients. Int J Gen Med (2021) 14:5313–22. doi: 10.2147/IJGM.S319717
25. Javdani F, Parsa S, Shakeri H, Hatami N, Kalani N, Haghbeen M, et al. Phosphate levels and pulmonary damage in COVID-19 patients based on CO-RADS scheme: Is there any link between parathyroid gland and COVID-19? MedRxiv. (2020). doi: 10.1101/2020.08.25.20181453
26. Kuro OM. The klotho proteins in health and disease. Nat Rev Nephrol (2019) 15:27–44. doi: 10.1038/s41581-018-0078-3
27. Kuro-O M. Klotho, phosphate and FGF-23 in ageing and disturbed mineral metabolism. Nat Rev Nephrol (2013) 9:650–60. doi: 10.1038/nrneph.2013.111
28. Mcgovern AP, De Lusignan S, Van Vlymen J, Liyanage H, Tomson CR, Gallagher H, et al. Serum phosphate as a risk factor for cardiovascular events in people with and without chronic kidney disease: A large community based cohort study. PloS One (2013) 8:e74996. doi: 10.1371/journal.pone.0074996
29. Adeney KL, Siscovick DS, Ix JH, Seliger SL, Shlipak MG, Jenny NS, et al. Association of serum phosphate with vascular and valvular calcification in moderate CKD. J Am Soc Nephrol (2009) 20:381–7. doi: 10.1681/ASN.2008040349
30. Malieckal DA, Uppal NN, Ng JH, Jhaveri KD, Hirsch JS. Electrolyte abnormalities in patients hospitalized with COVID-19. Clin Kidney J (2021) 14:1704–7. doi: 10.1093/ckj/sfab060
31. Komaba H, Fukagawa M. Phosphate-A poison for humans? Kidney Int (2016) 90:753–63. doi: 10.1016/j.kint.2016.03.039
32. Fajgenbaum DC, June CH. Cytokine storm. N Engl J Med (2020) 383:2255–73. doi: 10.1056/NEJMra2026131
33. Karki R, Kanneganti TD. The ‘cytokine storm’: Molecular mechanisms and therapeutic prospects. Trends Immunol (2021) 42:681–705. doi: 10.1016/j.it.2021.06.001
34. Lu L, Zhang H, Zhan M, Jiang J, Yin H, Dauphars DJ, et al. Preventing mortality in COVID-19 patients: Which cytokine to target in a raging storm? Front Cell Dev Biol (2020) 8:677. doi: 10.3389/fcell.2020.00677
Keywords: inflammation, phosphate, post-COVID, nephrology, hemodialysis
Citation: Corrêa HL, Deus LA, Araújo TB, Reis AL, Amorim CEN, Gadelha AB, Santos RL, Honorato FS, Motta-Santos D, Tzanno-Martins C, Neves RVP and Rosa TS (2022) Phosphate and IL-10 concentration as predictors of long-covid in hemodialysis patients: A Brazilian study. Front. Immunol. 13:1006076. doi: 10.3389/fimmu.2022.1006076
Received: 28 July 2022; Accepted: 15 September 2022;
Published: 30 September 2022.
Edited by:
Martijn van Griensven, Maastricht University, NetherlandsReviewed by:
Pedro Paulo Gattai Gomes, University of São Paulo, BrazilFernando Mafra, University of Mogi das Cruzes, Brazil
Copyright © 2022 Corrêa, Deus, Araújo, Reis, Amorim, Gadelha, Santos, Honorato, Motta-Santos, Tzanno-Martins, Neves and Rosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thiago S. Rosa, thiagoacsdkp@yahoo.com.br
†ORCID: Thiago S. Rosa, orcid.org/0000-0003-0418-0945