 Caroline Vinit1,2*
Caroline Vinit1,2* Sophie Georgin-Lavialle2,3
Sophie Georgin-Lavialle2,3 Aikaterini Theodoropoulou4,5
Aikaterini Theodoropoulou4,5 Catherine Barbier6
Catherine Barbier6 Alexandre Belot7,8Manel Mejbri4,5
Alexandre Belot7,8Manel Mejbri4,5 Pascal Pillet9
Pascal Pillet9 Jana Pachlopnik10Sylvaine Poignant11Charlotte Rebelle9
Jana Pachlopnik10Sylvaine Poignant11Charlotte Rebelle9 Andreas Woerner12
Andreas Woerner12 Isabelle Koné-Paut2,13†
Isabelle Koné-Paut2,13† Véronique Hentgen1,2
Véronique Hentgen1,2- 1General Pediatrics, Versailles Hospital, Versailles, France
- 2CEREMAIA (French reference center for auto-inflammatory diseases and inflammatory amyloidosis), Kremlin-Bicêtre, France
- 3Department of Internal Medicine, Sorbonne University, Tenon Hospital (APHP), Paris, France
- 4Pediatric Immuno-Rheumatology of Western Switzerland, Department Women-Mother-Child, Lausanne University Hospital, Lausanne, Switzerland
- 5Pediatric Immuno-Rheumatology Department, University Hospital, Geneva, Switzerland
- 6Pediatric Immunology, Albert Michallon Hospital, Grenoble, France
- 7Pediatric Nephrology Rheumatology and Dermatology, CHU Lyon, Lyon, France
- 8RAISE (Centre de référence des rhumatismes inflammatoires et maladies auto-immunes systémiques de l’enfant), Paris, France
- 9Pediatrics and Immunology, CHU Pellegrin, Bordeaux, France
- 10Pediatric Immunology, Kinderspital, Zurich, Switzerland
- 11General Pediatrics, CHU Nantes, Nantes, France
- 12Pediatric Cardiology and Rheumatology, UKBB Hospital, Bâle, Switzerland
- 13Pediatric Rheumatology Department, Bicêtre Hospital, APHP, University of Paris Saclay, Kremlin Bicêtre, France
Background: Interleukin (IL)-1 inhibitors represent the main treatment in patients with colchicine-resistant/intolerant familial Mediterranean fever (crFMF), mevalonate kinase deficiency (MKD), and tumor necrosis factor receptor-associated periodic syndrome (TRAPS). However, the reasons for the use of IL-1 inhibitors in these diseases are still not completely clarified.
Objective: Identify real-life situations that led to initiating anakinra or canakinumab treatment in hereditary recurrent fevers (HRFs), combining data from an international registry and an up-to-date literature review.
Patients and Methods: Data were extracted from the JIRcohort, in which clinical information (demographic data, treatment, disease activity, and quality of life) on patients with FMF, MKD, and TRAPS was retrospectively collected. A literature search was conducted using Medline, EMBASE, and Cochrane databases.
Results: Complete data of 93 patients with HRF (53.8% FMF, 31.2% MKD, and 15.1% TRAPS) were analyzed. Data from both the registry and the literature review confirmed that the main reasons for use of IL-1 blockers were the following: failure of previous treatment (n = 57, 61.3% and n = 964, 75.3%, respectively), persistence of disease activity with frequent attacks (n = 44, 47.3% and n = 1,023, 79.9%) and/or uncontrolled inflammatory syndrome (n = 46, 49.5% and n = 398, 31.1%), severe disease complication or associated comorbidities (n = 38, 40.9% and n = 390, 30.4%), and worsening of patients’ quality of life (n = 36, 38.7% and n = 100, 7,8%). No reasons were specified for 12 (16.4%) JIRcohort patients and 154 (12%) patients in the literature.
Conclusion: In the absence of standardized indications for IL-1 inhibitors in crFMF, MKD, and TRAPS, these results could serve as a basis for developing a treat-to-target strategy that would help clinicians codify the therapeutic escalation with IL-1 inhibitors.
Introduction
Hereditary recurrent fevers (HRFs) belong to the large group of autoinflammatory diseases (AIDs), whose name was first proposed by McDermott et al. in 1999 (1). This term describes inflammatory febrile attacks, with minimal involvement of the adaptive immune system in opposition to so-called autoimmune diseases.
Advances in the pathophysiological knowledge on HRFs have led to targeted therapies to improve patients’ quality of life, reduce the inflammatory response, and prevent amyloidosis. Based on the excess production of interleukin (IL)-1, the first patients with cryopyrin-associated periodic syndrome (CAPS) effectively treated with the IL-1 receptor antagonist anakinra were described in 2003 (2). The benefit of IL-1-blocking agents has subsequently been reported in the four prototypic monogenic AIDs (3–7). Anakinra received the market authorization (MA) for CAPS in 2013 and colchicine-resistant/intolerant familial Mediterranean fever (crFMF) in April 2020 in Europe (8). In addition, several studies reported its efficacy also in mevalonate kinase deficiency (MKD) and tumor necrosis factor (TNF) receptor-associated periodic syndrome (TRAPS) patients (9–11). Canakinumab is licensed in adults and children from 2 years of age in the European Union (i) for first-line maintenance treatment in CAPS since 2009 and (ii) for familial Mediterranean fever (FMF), MKD, and TRAPS since 2017 (12). However, regulatory authorities’ indications may vary across countries.
IL-1 inhibitors are indicated for patients with (i) severe clinical manifestations, (ii) failure or severe side effects of treatment in MKD and TRAPS attacks, or (iii) crFMF (13). However, the precise clinical and biological criteria leading to the use of IL-1 inhibitors in these diseases are still unclear.
The main objective of our study was to identify actual criteria for the use of IL-1-blocking agents (anakinra and canakinumab) in patients with crFMF, MKD, or TRAPS using data from the Juvenile Inflammatory Rheumatism (JIR)cohort and an updated literature review.
Patients and Methods
JIRcohort
The JIRcohort is an observational and multicenter international registry created in 2013 to collect data on patients with juvenile inflammatory rheumatic diseases. The cohort operates in specific modules; the module on AID has been running since April 2016. The participating centers can record both retrospective and prospective data, especially during follow-up visits. Patients are included in the JIRcohort after information and verification that they (or their legal guardian) are not opposed to the study and storage of their data. The JIRcohort protocol was approved by the French Ethics Committee (CCTIRS) on April 21, 2015 (decision number 14.302). The electronic form of the JIRcohort was approved by the National Commission of data processing and liberties (CNIL) on March 27, 2015 (decision number DR-2015-218).
Our survey collected only data from patients with FMF, MKD, and TRAPS treated with IL-1 inhibitors (anakinra and/or canakinumab). Selected patients came from 12 different centers in France and Switzerland. Since the HRFs Genoa criteria (14) were not available for all patients, the diagnosis of FMF, MKD, or TRAPS was established by the examining physician and investigator. Demographic data (age at diagnosis, genetics, comorbidities), therapeutic data, and data assessing disease activity and quality of life were collected at the last visit before starting IL-1 therapy. The presence of likely pathogens or pathogenic variants defined a confirmatory genotype according to the International Study Group for Systemic Autoinflammatory Diseases classification rules described elsewhere (15). Data evaluating disease activity included (i) biological features [C-reactive protein (CRP) and serum amyloid A protein (SAA) levels], (ii) flares’ characteristics (duration and frequency defined as more than three in 6 months), and (iii) the visual analog scale (VAS). The patient and physician rated this tool from 0 to 10, and an active disease was defined by a median VAS ≥ 3/10. The Auto-Inflammatory Diseases Activity Index (AIDAI) score validated and used in clinical practice was not, at this time, recorded in the JIRcohort. Data evaluating the quality of life included (i) number of hospitalizations or consultations, (ii) school or work impact (number of missing days, stress of exams triggering an attack, reduction of working times), (iii) severe daily asthenia and ongoing symptoms, and (iv) psychosocial impact (disease-related anxiety/depression). Therapeutic data included previous treatment(s), efficiency, and toxicity. Anakinra was prescribed continuously with daily injections or as on-demand treatment at the time of an attack. Patients without a follow-up visit recorded in the JIRcohort were excluded. The data extraction took place on May 15, 2020.
Literature Review
A literature search on the indications for IL-1 inhibitors in HRFs was performed using Medline, EMBASE, and Cochrane databases with mesh terms (Ilaris OR Canakinumab)/(Kineret OR Anakinra)/(IL-1 inhibitors) AND (familial Mediterranean fever OR FMF)/(mevalonate kinase deficiency OR MKD OR HIDS)/(periodic tumor necrosis factor receptor-related syndrome OR TRAPS). Additional research was conducted within the references of the retrieved papers. We identified 359 publications through this research before May 2020. We assessed all titles, abstracts, and full-length articles identified. Publications were eligible if they contained either data on anakinra and/or canakinumab in patients with FMF, MKD, or TRAPS as defined by the Tel Hashomer criteria (16) or a genetic analysis or a mevalonic aciduria dosage. After removing duplications, we excluded articles (i) that were not published in English nor French, (ii) with unavailable abstract or full text, and (iii) without data on canakinumab nor anakinra. After this process, 112 articles (randomized controlled trials, non-randomized trials, cohort studies, case reports, and case series) remained for analysis and were included in the study. Possible indications for IL-1 inhibitors were identified with data evaluating comorbidities, complications, disease activity, previous treatment(s), and tolerance.
Results
Patients
JIRcohort
At extraction date, 613 HRF patients were included in the JIRcohort: 524 FMF patients, 45 MKD patients, and 44 TRAPS patients. Ninety-three patients, male-to-female ratio 40/53, were treated with IL-1 inhibitors and had a follow-up in French (N = 71, 76.3%) and Swiss (N = 22, 30.1%) centers. Fifty (53.8%) had a diagnosis of FMF, 29 (30.9%) of MKD, and 14 (14.9%) of TRAPS. First symptoms appeared at a median age of 3.5 (2–35) years for FMF, 0.4 (5–40) years for MKD, and 2 (1–17) years for TRAPS. The median delay to diagnosis was the longest for patients with TRAPS [14.5 (0.2–47) years]. The median time of follow-up was 9 (1–60) years for all patients. Sixteen (17.2%) patients had associated secondary amyloidosis, mainly adults with FMF.
For FMF, 31 patients (62%) had a confirmatory genotype, five patients (10%) had a non-confirmatory genotype, 10 patients (20%) were not tested, and the genotype was not specified in four patients (8%). For MKD, 18 patients (62.1%) had a confirmatory genotype, three patients (10.3%) had a non-confirmatory genotype, four patients (13.8%) were not tested, and the genotype was not specified in four patients (13.8%). For TRAPS, seven patients (50%) had a confirmatory genotype, four patients (28.6%) had a non-confirmatory genotype, two patients (14.3%) were not tested, and the genotype was not specified in one patient (7.1%). The main clinical characteristics are detailed in Table 1.
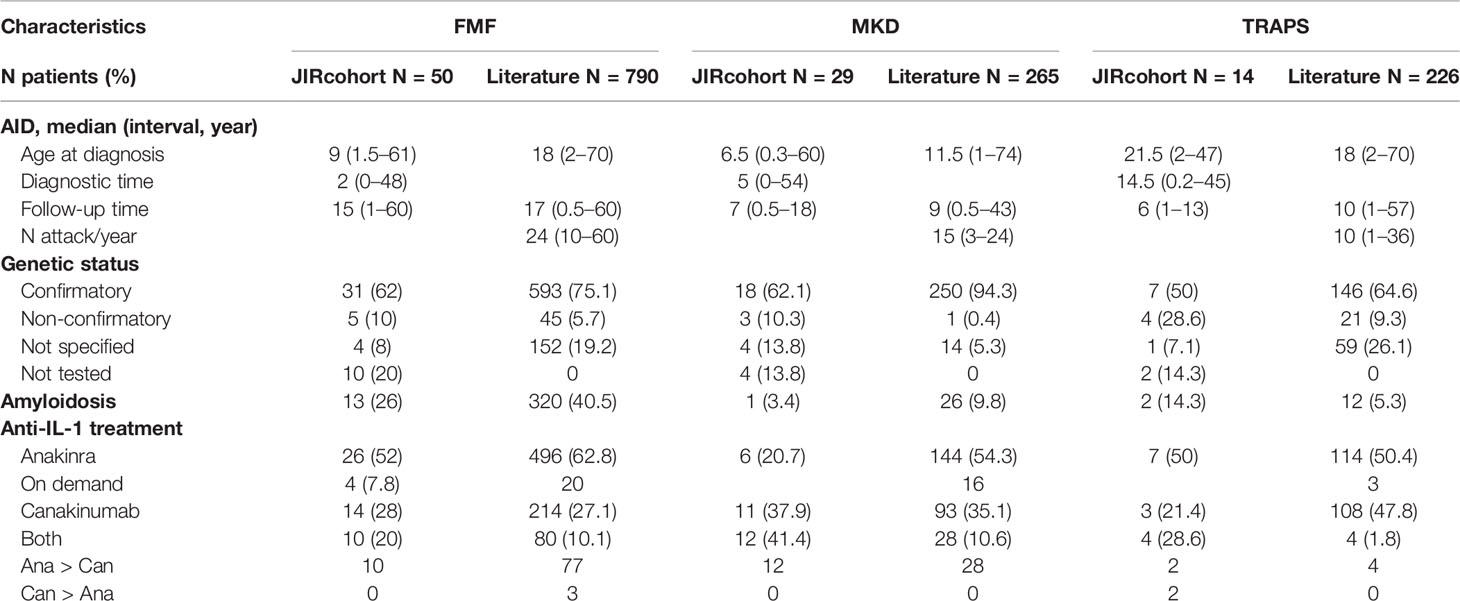
Table 1 Main characteristics: JIRcohort and literature review. IL, interleukin; FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome.
Literature Review
One thousand two hundred eighty-one patients were identified in 112 articles, including 75 case reports and case series (11, 11, 17–88), 31 cohort studies (10, 89–119), four phase II trials (99, 120–122), and two randomized placebo-controlled trials (9, 12). Seven hundred ninety patients (61.7%) were diagnosed with FMF, 265 (20.7%) with MKD, and 226 (17.6%) with TRAPS. Five hundred sixty-nine came from central Europe (44.4%), 520 from the Eastern Mediterranean area (Israel, Turkey, 40.6%), six from Asia (China, Japan, 0.5%), three from the United States and Australia (0.2%), and 185 from an international registry (Eurofever, 14.4%). Three hundred fifty-eight patients (27.9%) had secondary amyloidosis, mostly FMF (n = 320/790).
For FMF, 593 patients (75.1%) had a confirmatory genotype, 45 patients (5.7%) had a non-confirmatory genotype, and the genotype was not specified in 152 patients (19.2%). For MKD, 250 patients (94.3%) had a confirmatory genotype, one patient (0.4%) had a non-confirmatory genotype, and the genotype was not specified in 14 patients (5.3%). For TRAPS, 146 patients (64.6%) had a confirmatory genotype, 21 patients (9.3%) had a non-confirmatory genotype, and the genotype was not specified in 59 patients (26.1%). All patients were tested in the literature review for FMF, MKD, and TRAPS. The main characteristics are reported in Table 1.
Interleukin-1-Blocking Agents
Anakinra was the principal IL-1-blocking agent reported in the literature (n = 754, 58.9%), sometimes used as on-demand therapy (n = 39/754 patients in the literature and 39/93 in the JIRcohort). Patients who received both IL-1 inhibitors were almost exclusively treated with anakinra before canakinumab (n = 109/112 patients in the literature and 24/26 in the JIRcohort). In the JIRcohort, IL-1 inhibitors were mainly used off-label for 87.1% of patients (n = 81/93), including 95.8% in France (n = 68/71) and 59.1% in Switzerland (n = 13/22). Median age at the first use of an IL-1 inhibitor occurred later for FMF patients [30 (4–82) years] than for MKD [11.5 (0.7–57) years] or TRAPS [13 (3–51) years] patients. Reasons for use of IL-1 inhibitors could be classified into four main categories and were similar in both JIRcohort and literature, i.e., failure of previous treatment, serious complications or comorbidities, the persistence of clinical and/or biological activity, and decreased quality of life (Tables 2, 3).
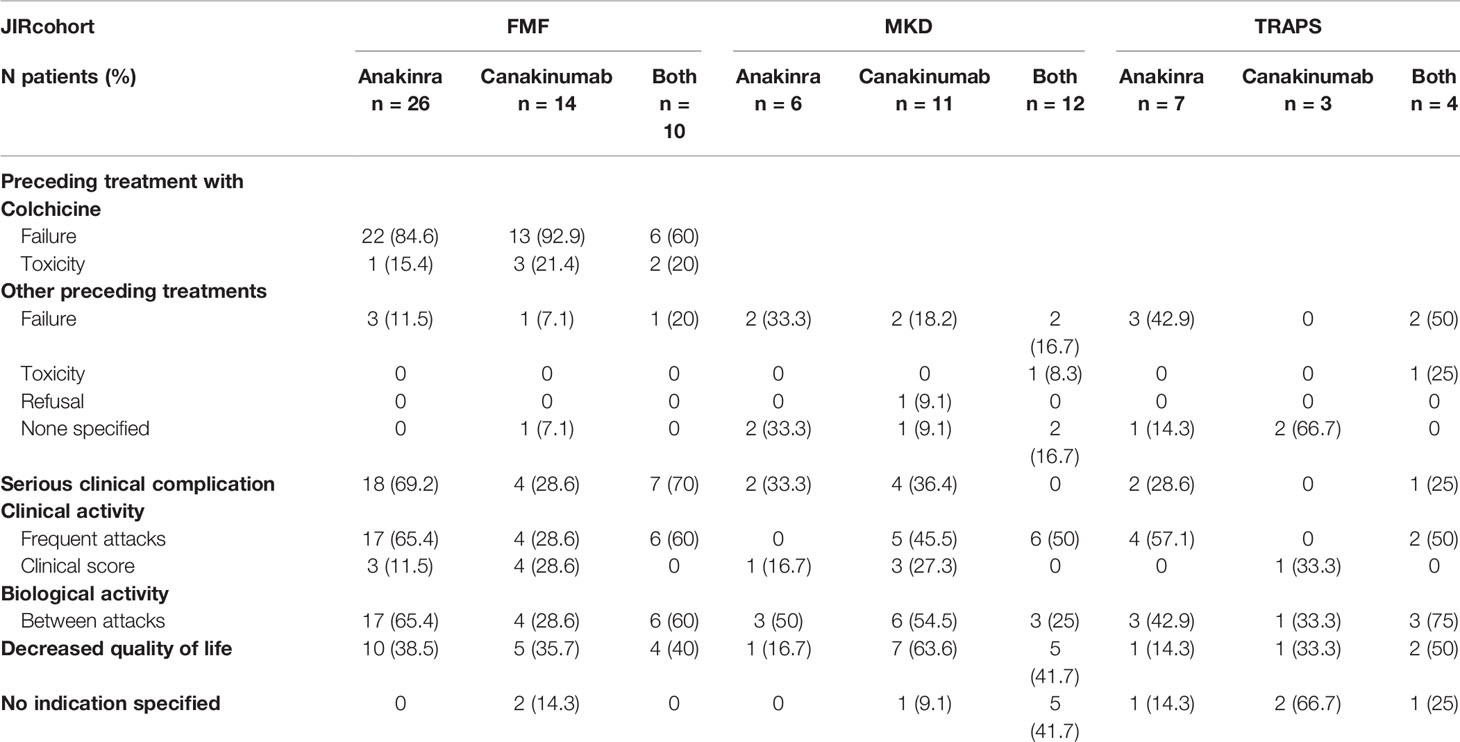
Table 2 IL-1 blockers’ indications: JIRcohort (population N = 73). IL, interleukin; FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome.
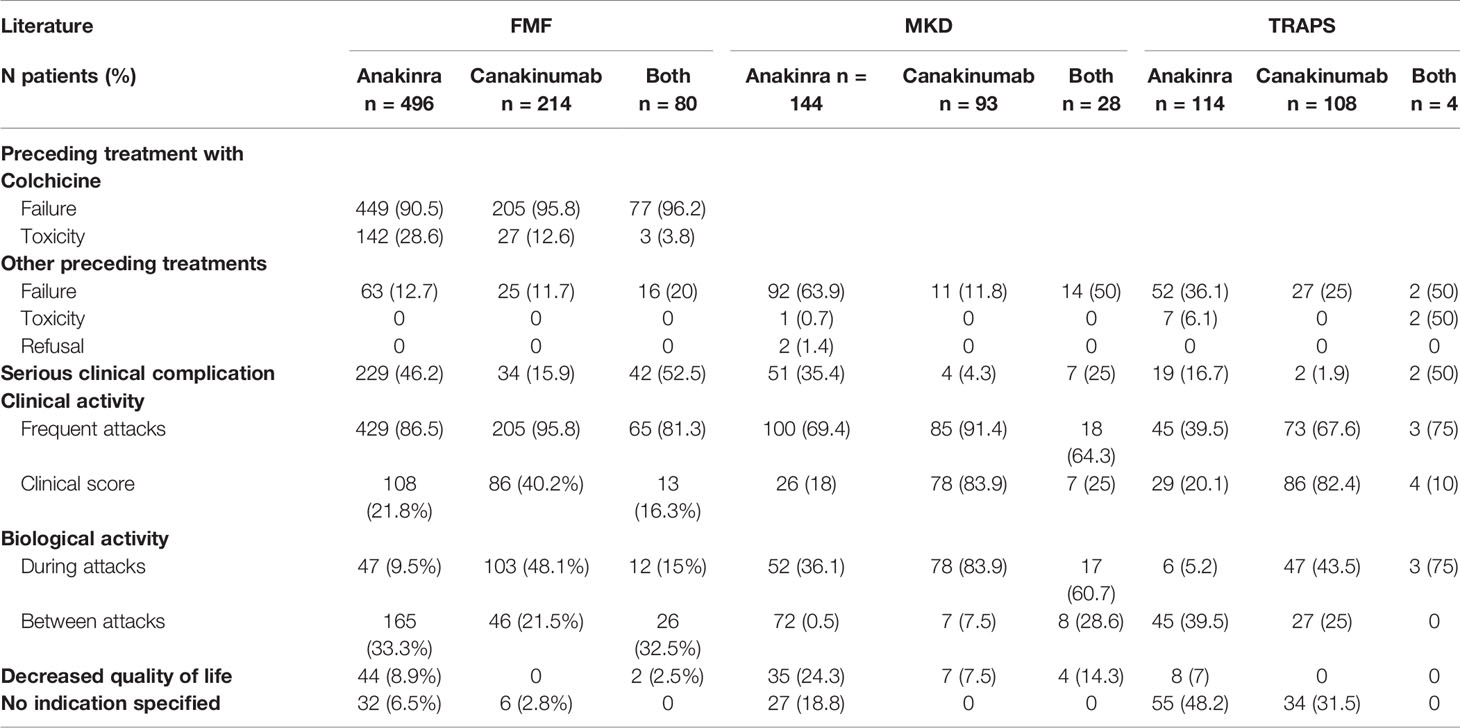
Table 3 IL-1 blockers’ indications: literature review (population N = 1,210). IL, interleukin; FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome.
Previous Treatments
Colchicine and Familial Mediterranean Fever
JIRcohort
Forty-one FMF patients (82%) were identified as colchicine-resistant, even if this characteristic was not explained in detail in the JIRcohort. Twenty-seven patients (54%) had frequent attacks according to their treating physician, of whom eight had 0.25–1 attack/month, eight patients had 1–3 attacks/month, and three had ≥4 attacks/month. Colchicine was continued in combination with the IL-1 inhibitors in almost all patients (n = 46, 92%). Colchicine toxicity was reported in five (10%) patients (diarrhea, n = 2; polyneuropathy, n = 2; and rhabdomyolysis, n = 1).
Literature Review
Seven hundred thirty-one FMF patients (93.5%) were identified as colchicine-resistant. The frequency of febrile attacks, the maximum tolerated dose (1–3 mg/day), and patient adherence to treatment (Figure 1A) characterized colchicine resistance. The frequency of attacks was defined in n = 399 (54.6%) patients: ≥1/month (n = 67), ≥2/month (n = 24), ≥3/month (n = 228), ≥4/month (n = 19), ≥6/month (n = 7), and ≥12/month (n = 1). Colchicine toxicity was reported in 172 patients (21.8%), mainly diarrhea, neuromyositis, neutropenia, cardiomyopathy, myopathy, hepatic cytolysis, and asthenozoospermia.
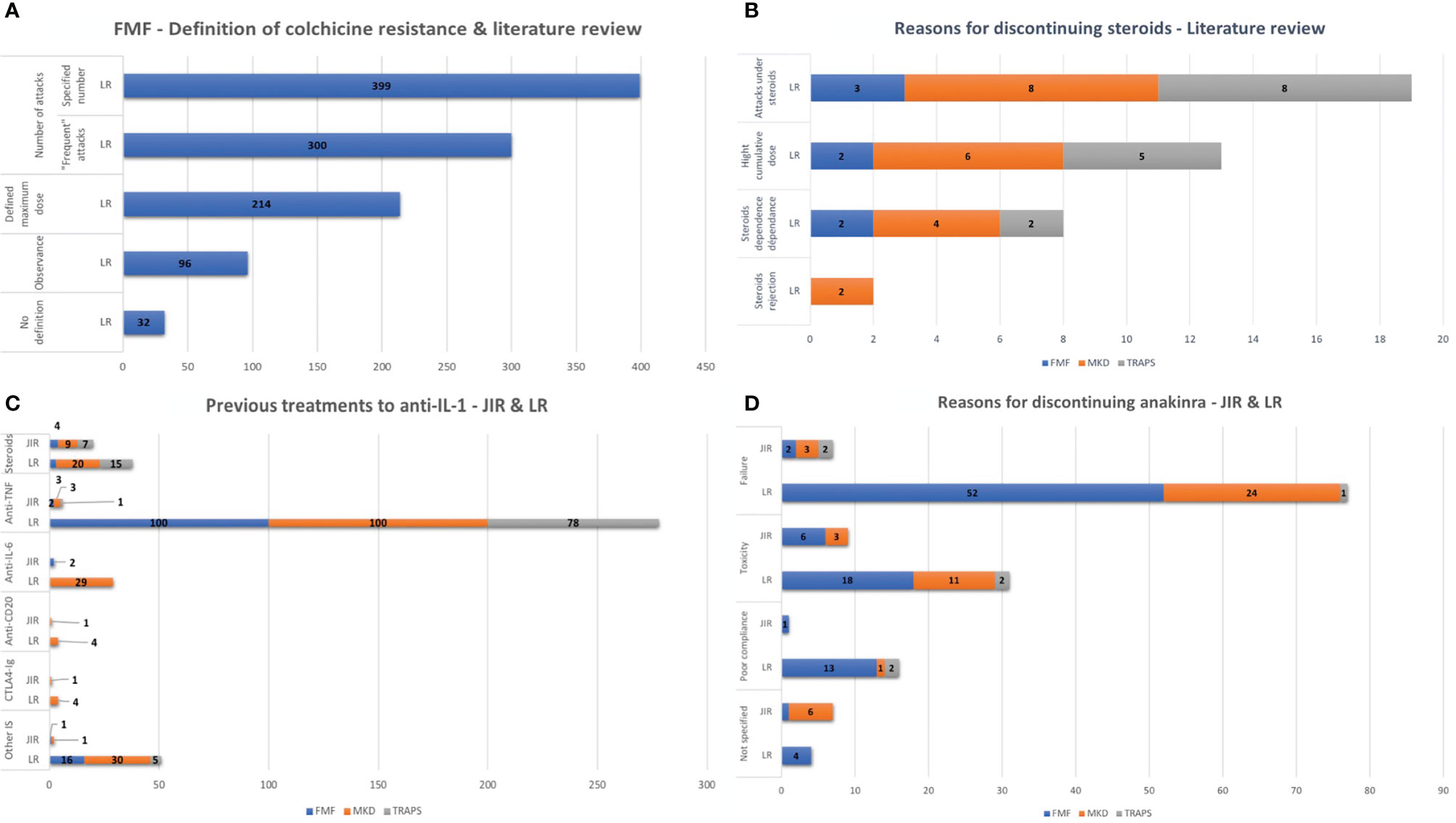
Figure 1 (A) FMF–Definition of colchicine resistance and literature review. (B) Previous treatments to IL-1 inhibitors. (C) Reasons for discontinuing steroids–Literature review. (D) Reasons for discontinuing anakinra. IL, interleukin; FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome; LR, literature review.
Other Previous Treatments
JIRcohort
Seven FMF patients (14%), 12 MKD patients (41.4%), and eight TRAPS patients (57.1%) were treated with immunosuppressive drugs and/or biological disease-modifying antirheumatic drugs (DMARDs) before IL-1 inhibitors, as detailed in Figure 1B. Reasons for discontinuation of previous treatments were ineffectiveness according to the treating physician (n = 16, 17.2%), a severe side effect (n = 2 for corticosteroids in an MKD and a TRAPS patient), or patient’s refusal (n = 1 MKD patient for corticosteroids). Reasons for discontinuation were not specified for nine patients (12.3%).
Literature Review
One hundred four FMF patients (13.2%), 117 MKD patients (44.2%), and 81 TRAPS patients (35.8%) were treated with immunosuppressive drugs and/or biotherapy before IL-1 inhibitors, as detailed in Figure 1B. Previous treatment was mainly stopped for therapeutic failure (n = 104 for FMF, n = 117 for MKD, and n = 81 for TRAPS). Nine patients (TRAPS, n = 8; MKD, n = 1) experienced a severe generalized urticarial rash, believed to be related to etanercept. Reasons for discontinuing steroid therapy are detailed in Figure 1C.
Reasons for Discontinuing Anakinra
Reasons for discontinuing anakinra are detailed in Figure 1D and were not specified for 7/24 patients (29.2%) in the JIRcohort. In the literature, the most common side effect was painful reactions at the injection site.
Severe Clinical Complications
JIRcohort
Severe clinical complications or comorbidities prompted the introduction of IL-1 inhibitors in 29 FMF patients (58%), six MKD patients (20.7%), and three TRAPS patients (21.4%) in the JIRcohort (Figure 2A). Gastroenterological complications found in FMF were peritonitis (n = 7), severe chronic diarrhea (n = 2), ulcerative colitis (n = 1), and cirrhosis (n = 2). Cerebellar ataxia has been found in one MKD patient. Three FMF patients had active spondylitis, three had severe vasculitis (Henoch–Schönlein purpura or polyarteritis nodosa), one had Still’s disease, and two others had active inflammatory bowel disease.
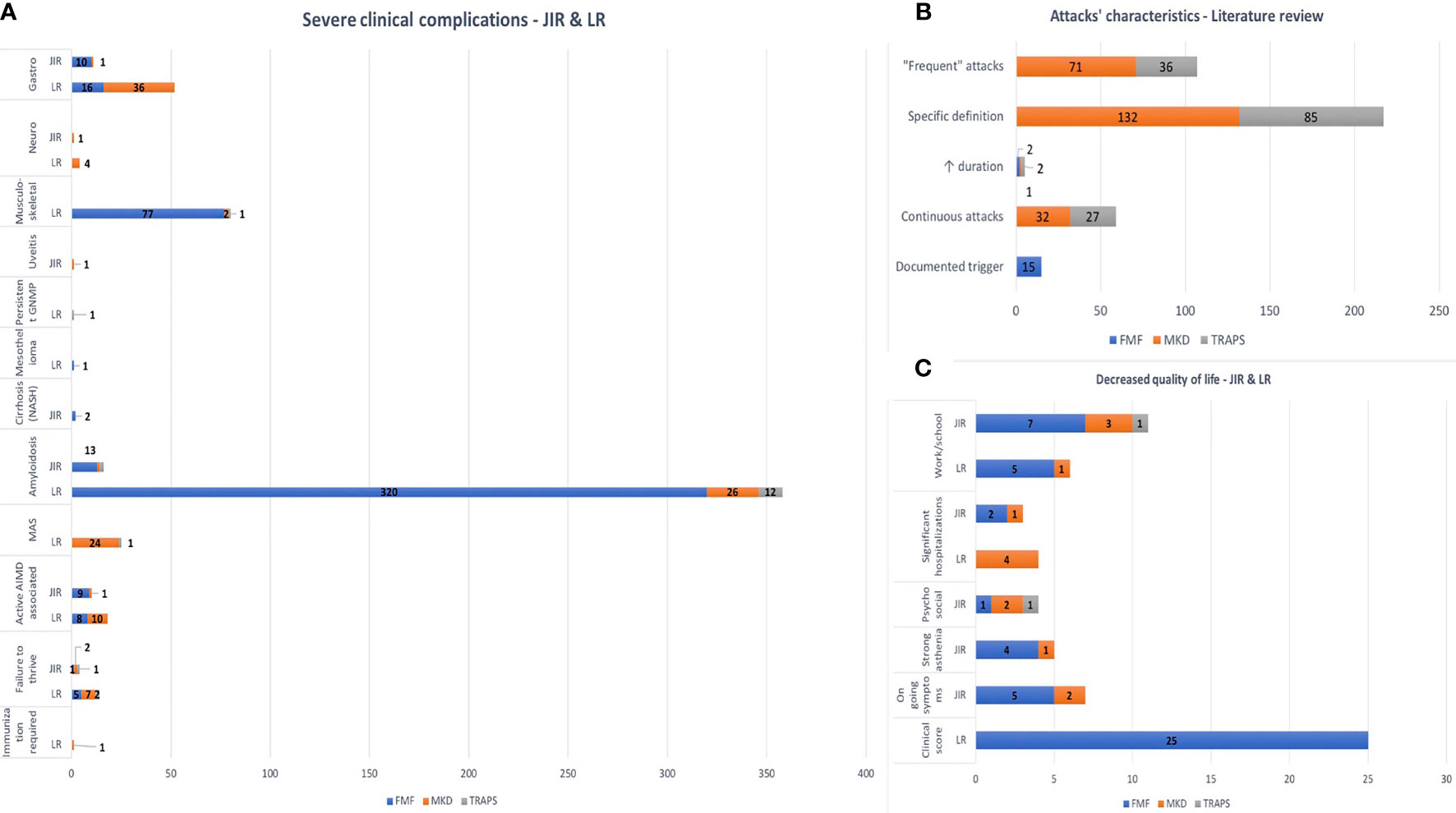
Figure 2 (A) Severe clinical complications. (B) Attacks’ characteristics–literature review. (C) Decreased quality of life. FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome; LR, literature review; GNMP, membrano-proliferative glomerulonephritis; MAS, macrophage activation syndrome; AIMD, auto-immune disease.
Literature Review
Severe clinical complications or comorbidities prompted the introduction of IL-1 inhibitors in 305 FMF patients (38.6%), 62 MKD patients (23.4%), and 23 TRAPS patients (10.2%) (Figure 2A). Gastroenterological complications found in MKD were recurrent anal abscesses (n = 1), intestinal fistula and/or necrosis (n = 33), severe colitis (n = 4), and refractory ascites (n = 1). In FMF, severe colitis was found in 16 patients. Musculoskeletal symptoms were mainly reported in FMF patients, arthritis (n = 55) or protracted febrile myalgia (n = 22). Eighteen patients (1.5%) had an associated active inflammatory disease, leading to the introduction of IL-1 inhibitors: spondylitis (n = 1), Behçet syndrome (n = 6), and Henoch–Schönlein purpura (n = 1) for FMF patients and destructive polyarthritis (n = 10) for MKD patients. On-demand anakinra was used in one MKD patient to prevent a severe attack triggered by immunization.
Biological Characteristics
JIRcohort
Persistent biological inflammation in-between attacks was reported in 46 patients (49.5%) including 27 FMF patients, 12 MKD patients, and seven TRAPS patients, mainly assessed by CRP levels >10 mg/L (Figure 3A).
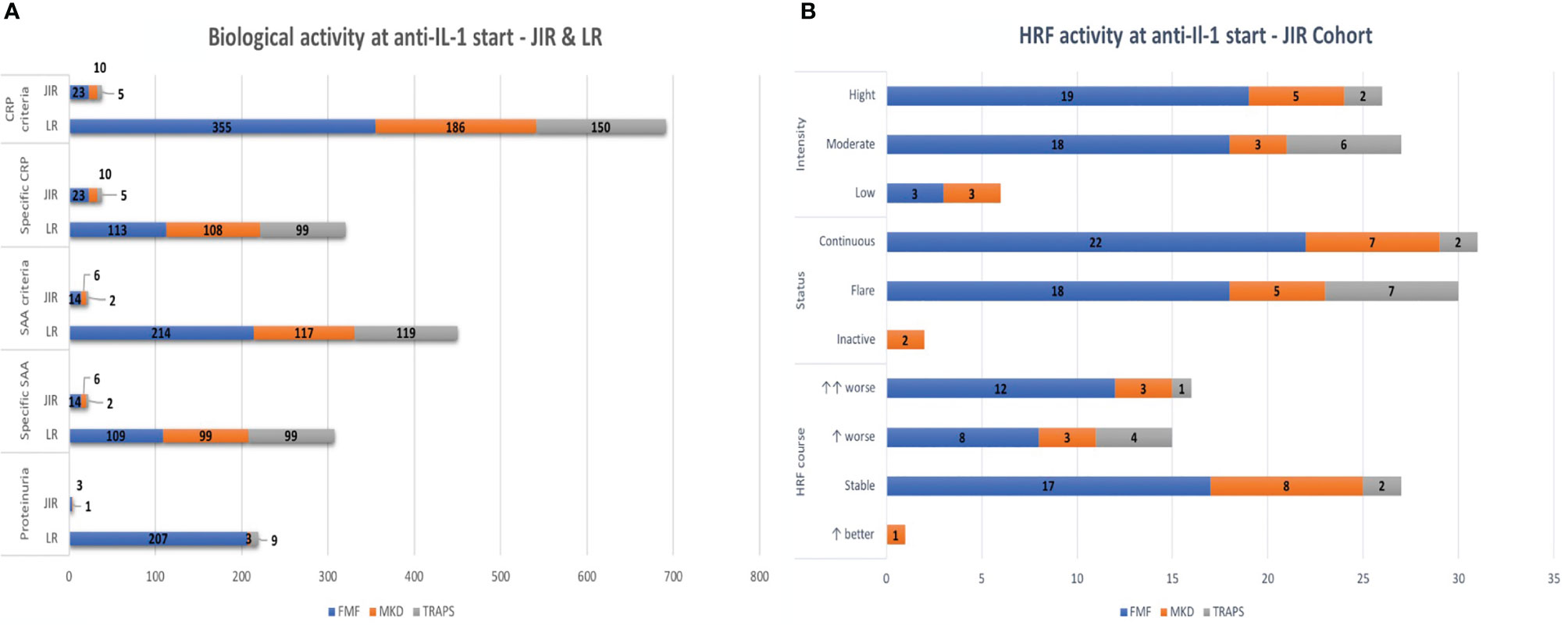
Figure 3 (A) Biological activity at IL-1 inhibitors’ start. (B) HRF activity at IL-1 inhibitors’ start. IL, interleukin; HRF, hereditary recurrent fever; FMF, familial Mediterranean fever; MKD, mevalonate kinase deficiency; TRAPS, tumor necrosis factor receptor-associated periodic syndrome; LR, literature review; CRP, C-reactive protein; SAA, serum amyloid A protein.
Literature Review
The persistence of biological inflammation in-between attacks (n = 396, 30.9%) or its significant elevation during attacks (n = 363, 28.3%) led to the introduction of IL-1 inhibitors. Inflammation levels could be specific according to papers (CRP or SAA >10, 20, 25, or 30 mg/L) or any increased CRP/SAA level was sufficient (Figure 3A).
Disease Activity
JIRcohort
Reported for only 19 patients (20.3% of the cohort), the VAS was >3/10 in seven FMF patients (14%), five MKD patients (17.2%), and one TRAPS patient (7.1%). Disease status, intensity, and time course were also assessed by the physician as described in Figure 3B.
Literature Review
The Physician Global Assessment (PGA) scale—used in most studies—was ≥2 for n = 190 patients (14.8%), and the VAS was reported for n = 118 patients (9.2%). The AIDAI score was exploited in 29 FMF and two TRAPS, and HRF activity was evaluated for 86 patients with a non-standardized score, which was different from one paper to another. These scores were consistently high but could not be compared with one another, as they were not standardized.
Inflammatory Flares’ Characteristics
In the literature, a documented trigger (n = 15, FMF), continuous attacks (n = 32, MKD and n = 27, TRAPS), prolonged (n = 1, MKD and n = 2, TRAPS) or frequent (n = 203, MKD and n = 121, TRAPS) attacks could justify the introduction of anakinra or canakinumab (Figure 2B).
Quality of Life Assessment
JIRcohort
In 36 patients (38.7%; 19 FMF, 13 MKD, and four TRAPS), decreased quality of life contributed to the use of IL-1 inhibitors (Figure 2C). Two patients received on-demand anakinra to support school exams.
Literature Review
Decreased quality of life led to the start of IL-1 inhibitors in 100 patients (7.8%; 46 FMF, 46 MKD, and eight TRAPS) (Figure 2C). Different scores were used to evaluate the improvement of quality of life with IL-1 inhibitors: Short-Form 36 (SF36; n = 104 patients), Child Health Questionnaire-Parent Form 50 (CHQ-PF50; n = 32 patients), Health Assessment Questionnaire (HAQ; n = 13 patients), VAS (n = 30 patients), and social development (n = 71 patients).
Discussion
To the best of our knowledge, this is the first paper describing extensively the criteria that lead in daily clinical practice to an indication of IL-1 blockers for adult and pediatric patients with FMF, MKD, and TRAPS. This work confirms that the reasons leading to the choice of treatment are considerably heterogeneous. However, four main categories seem to be consensual in both the JIRcohort and the literature: failure of previous treatment, a severe complication of the disease or associated comorbidity, persistent clinical and/or biological inflammation, and decrease in patients’ quality of life.
Persistent elevation of inflammatory markers and frequent attacks were the most common arguments for introducing IL-1 inhibitors. Inflammation was mainly judged on CRP levels, whose duration and severity depended on each prescriber or study. A clear definition of “frequent attacks” was rarely available, and when it did exist, the number of flares, duration, intensity, and time of onset were very heterogeneous. Recommendations for the management of MKD and TRAPS are also imprecise, as IL-1 inhibitors are required for “frequent attacks and/or subclinical inflammation between attacks” (123–125).
For FMF, IL-1 blockers are indicated only for colchicine resistance or intolerance; however, there is currently no consensus in the literature for a clear definition of crFMF. According to the Franco-Israeli consortium, crFMF is defined as the occurrence of six or more typical attacks in 1 year or three in 4–6 months associated with an increase in inflammatory markers between attacks (126); according to European Alliance of Associations for Rheumatology (EULAR) definition, as at least one flare per month in the last 6 months with full compliance to treatment (127) and as more than six attacks per year or more than four attacks in the last 6 months with persistent biological inflammation (128). Recently, Ozen et al. (129) agreed that crFMF included recurrent attacks (one or more attacks per month over 3 months) or persistent laboratory inflammation in-between attacks. Eighty-two percent of patients receiving IL1 inhibitors were considered crFMF in our study, similar to results (89%) of Kacar et al. (130). However, many factors could contribute to insufficient response to colchicine: lack of compliance, the occurrence of side effects, drug interactions, genetic factors, and environmental factors (infections, stress, and diet) (131). All studies and definitions agree that a maximum tolerated dosing of colchicine (132) and the assessment of compliance are the prerequisites before discussing crFMF (133), but finding a standardized way is challenging (134). Missing tablet count, Morisky score (135), and colchicine dosage in the hair were rarely reported in our study. Hair colchicine testing was recently proposed (136) to assess objectively and non-invasively adherence from 2 to 6 months before the sampling. Toxicity of colchicine is rare in our study, as approved by experts in the literature (129).
Our study showed that only a proportion of patients appear to require IL-1 inhibition. Unfortunately, it was not feasible to estimate the exact ratio of patients requiring these treatments because we did not have the opportunity to verify that all patients from participating centers were included in the cohort. However, IL-1 inhibitors do not appear to be offered as first-line therapy to all patients in daily practice. One reason could be that at the time of the persistent HRF activity, IL-1 inhibitors were not always available in all centers. Steroids and TNF-α blockers were mainly used before IL-1 inhibitors in our study. Steroids can be used shortly for flares’ treatment but may only have partial efficacy in MKD (10, 100) and a declining efficacy in TRAPS, requiring a higher dose for an equivalent response with many side effects (125). Efficacy of etanercept in TRAPS patients appears transient and decreases over time (137, 138), confirmed in our study with the reappearance of inflammatory flares. A better clinical and biological response also has been described by Ozen et al. (96) with an IL-1 rather than a TNFα inhibitor in TRAPS patients on first-line therapy, which also represent by far the most frequently employed biologics in the Auto-Inflammatory Diseases Alliance (AIDA) network (139). IL-1 inhibitors could be recommended as first-line therapy and for cortisone sparing in severe phenotypes (96).
A severe phenotype of HRF justified IL-1 inhibitors in about 30% of patients in the JIRcohort and the literature. Active inflammatory comorbidities found in our study have been known to be associated with FMF, vasculitis [Behçet’s disease (140), Henoch–Schönlein purpura, periarteritis nodosa (141)], spondylitis (142), and suppurative hidradenitis (143), whereas inflammatory bowel diseases (144) and multiple sclerosis (145) are still controversial. As recommended (127), intensified treatment with biological DMARDs was given in 26% of FMF patients with secondary amyloidosis in the JIRcohort. Similar results (20%) were found in the study by Corsia et al. (128). Such a therapeutic strategy has proven its effectiveness, as shown by a recent study, in which treatment with canakinumab was significantly associated with decreased proteinuria in secondary amyloidosis patients (111). In TRAPS patients complicated with amyloidosis, especially in the case of structural mutation involving cysteine (124), IL-1 inhibitors also appeared to be the most effective treatment (41, 146–148). The majority of patients in our cohort as well as those in the literature requiring IL-1 inhibition had a confirmatory genotype according to the International Study Group for Systemic Autoinflammatory Diseases (INSAID) rules. The need for this type of treatment in patients with a non-confirmatory genotype [heterozygous FMF or MKD without mevalonic aciduria, presence of a variant of uncertain significance (VOUS) in TRAPS] seems much more uncommon. The few patients classified in our cohort as having “no mutation” concern patients (i) for whom the diagnosis was made before the generalization of genetic testing and who were never tested afterward or (ii) for whom genetics was missing data.
Several (sometimes non-standardized) scores were recorded to measure disease activity and lead to IL-1 inhibitor treatment. VAS, the most frequently used score in the JIRcohort, has the disadvantage of trying to assign a single value to a complex and subjective perception of the disease, causing disparate therapeutic decisions depending on the prescriber. The FMF50, which defines non-responders to colchicine (149), and adult (150, 151) or pediatric (152) severity scores such as the International Severity Score for FMF (ISSF) are not very sensitive (153). With a sensitivity and specificity of more than 80%, the AIDAI score differentiates patients with active disease (score >9) from those with inactive disease (score <9) (154). Despite its validation and possible use in daily practice, it seems difficult to have it completed daily by patients. Furthermore, the AIDAI score has not yet been validated in a treat-to-target approach: the maximal cutoff value and the specificity of the score for the inflammatory manifestations are still unknown.
There is currently no score evaluating disease activity from both physician’s and patient’s perspective, taking into account the quality of life, which was a strong argument in our study for introducing IL-1 inhibitors. Several authors confirmed a poorer quality of life in children and adults with FMF (155–158) and a higher incidence of anxiety and depression (159–161) that may lead to more frequent attacks with higher rates of CRP and SAA (159, 161, 162). Van der Hilst et al. (10) also described lower autonomy and social development in MKD patients. Estimating quality of life in HRF is complex, involved disease activity and severity, and would require a standardized assessment to justify therapeutic escalation and improve management.
Even if canakinumab is today the only IL-1 inhibitor to have MA in Europe for treatment of MKD and TRAPS, nearly two-thirds of patients in our cohort were treated with anakinra as a first-line. There is so far no data comparing the two drugs that both seem to be effective in these HRFs (9–12, 32, 46, 54, 55, 60, 100, 104, 105, 133, 163, 164), but their costs differ. Anakinra has a shorter half-life, limiting drug overdosing in patients with renal impairment (94, 113, 165), and the French–Israeli expert committee recommends its use for crFMF patients before considering a long-half-life IL-1 inhibitor (126). Canakinumab is an alternative in case of poor tolerance of daily anakinra injections. The efficacy of anakinra prescribed on demand has been described in cases of known triggers [stress of an examination or vaccinations (56)] or rare inflammatory flares (78, 84, 103). On-demand prescribing may limit local reactions to injections, decrease the use of steroids and the risk of infection, but there are currently no studies comparing anakinra on-demand vs. continuous use. However, experts recommend continuous treatment for persistent inflammatory syndrome between attacks or the use of anakinra on demand more than once a month (123, 124). Considering its benefits and efficacy, anakinra may also soon be granted MA for MKD and TRAPS.
The major flaw of our study is its retrospective design. Since the collection of data in the JIRcohort began in April 2016, the clinical, biological, and quality of life characteristics of patients treated with IL-1 inhibitors before this date were not captured. The heterogeneity of experience in managing HRF patients among different centers and the lack of follow-up tools in the JIRcohort are also part of the limitations of our study. The strengths of our study are the large sample of both children and adults and its multicentric dimension, including countries with different market authorizations.
Conclusion
Our study has shown that the indications in real life for the use of IL-1 inhibitors in crFMF, MKD, and TRAPS are still not standardized and poorly defined. The choice for treatment with IL-1 inhibitors is based on the habits of expert clinicians that may vary from one center to another. Furthermore, the availability of the drugs may vary from country to country. Several prerequisites will be necessary to harmonize clinical care: (i) a formalization of the different criteria that clinicians use to set the indication for IL-1 inhibition in HRFs, (ii) validated composite activity scores that will eventually help to define treat-to-target treatment plans, (iii) a comparison of the different treat-to-target strategies on the actual long-term outcome of the patients, and (iv) a medico-economic analysis of the different possible treatment plans. We recently launched a European-wide survey to collect treatment plans and outcome measures applied to patients with HRF. We will hence provide a snapshot of current care and clinical practice strategies in Europe. In the long term, comparing the different strategies used will guarantee the patients with autoinflammatory diseases to be offered the optimal treatment available in their country.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Author Contributions
All authors participated in the preparation of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
Michael Hofer, Pierre Quartier, Isabelle Melki, Dallel Benazzouz, François Hofer, Sabrina Atmane, Rim Bourguiba, RES Foundation.
References
1. McDermott MF, Aksentijevich I, Galon J, McDermott EM, Ogunkolade BW, Centola M, et al. Germline Mutations in the Extracellular Domains of the 55 kDa TNF Receptor, TNFR1, Define a Family of Dominantly Inherited Autoinflammatory Syndromes. Cell (1999) 97(1):133–44. doi: 10.1016/S0092-8674(00)80721-7
2. Hawkins PN, Lachmann HJ, McDermott MF. Interleukin-1-Receptor Antagonist in the Muckle-Wells Syndrome. N Engl J Med (2003) 348(25):2583–4. doi: 10.1056/NEJM200306193482523
3. Jesus AA, Goldbach-Mansky R. IL-1 Blockade in Autoinflammatory Syndromes. Annu Rev Med (2014) 65:223–44. doi: 10.1146/annurev-med-061512-150641
4. Sota J, Vitale A, Insalaco A, Sfriso P, Lopalco G, Emmi G, et al. Safety Profile of the Interleukin-1 Inhibitors Anakinra and Canakinumab in Real-Life Clinical Practice: A Nationwide Multicenter Retrospective Observational Study. Clin Rheumatol (2018) 37(8):2233–40. doi: 10.1007/s10067-018-4119-x
5. Malcova H, Strizova Z, Milota T, Striz I, Sediva A, Cebecauerova D, et al. IL-1 Inhibitors in the Treatment of Monogenic Periodic Fever Syndromes: From the Past to the Future Perspectives. Front Immunol (2020) 11:619257. doi: 10.3389/fimmu.2020.619257
6. Marko L, Shemer A, Lidar M, Grossman C, Druyan A, Livneh A, et al. Anakinra for Colchicine Refractory Familial Mediterranean Fever: A Cohort of 44 Patients. Rheumatol Oxf Engl (2021) 60(6):2878–83. doi: 10.1093/rheumatology/keaa728
7. Atas N, Eroglu GA, Sodan HN, Ozturk BO, Babaoglu H, Satis H, et al. Long-Term Safety and Efficacy of Anakinra and Canakinumab in Patients With Familial Mediterranean Fever: A Single-Centre Real-Life Study With 101 Patients. Clin Exp Rheumatol (2021) 39 Suppl 132(5):30–6.
8. PNDS - Syndromes Périodiques Associés a La Cryopyrine (CAPS), Vol. 73 (2013). Available at: https://www.has-sante.fr/upload/docs/application/pdf/2013-05/pnds_-_syndromes_periodiques_associes_a_la_cryopyrine_caps_2013-05-15_15-23-40_118.pdf.
9. Ben-Zvi I, Kukuy O, Giat E, Pras E, Feld O, Kivity S, et al. Anakinra for Colchicine-Resistant Familial Mediterranean Fever: A Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Rheumatol Hoboken NJ (2017) 69(4):854–62. doi: 10.1002/art.39995
10. van der Hilst JCH, Bodar EJ, Barron KS, Frenkel J, Drenth JPH, van der Meer JWM, et al. Long-Term Follow-Up, Clinical Features, and Quality of Life in a Series of 103 Patients With Hyperimmunoglobulinemia D Syndrome. Med (Baltimore) (2008) 87(6):301–10. doi: 10.1097/MD.0b013e318190cfb7
11. Gattorno M, Pelagatti MA, Meini A, Obici L, Barcellona R, Federici S, et al. Persistent Efficacy of Anakinra in Patients With Tumor Necrosis Factor Receptor-Associated Periodic Syndrome. Arthritis Rheumatol (2008) 58(5):1516–20. doi: 10.1002/art.23475
12. De Benedetti F, Gattorno M, Anton J, Ben-Chetrit E, Frenkel J, Hoffman HM, et al. Canakinumab for the Treatment of Autoinflammatory Recurrent Fever Syndromes. N Engl J Med (2018) 378(20):1908–19. doi: 10.1056/NEJMoa1706314
13. Ozen S, Demir S. Monogenic Periodic Fever Syndromes: Treatment Options for the Pediatric Patient. Paediatr Drugs (2017) 19(4):303–11. doi: 10.1007/s40272-017-0232-6
14. Gattorno M, Hofer M, Federici S, Vanoni F, Bovis F, Aksentijevich I, et al. Classification Criteria for Autoinflammatory Recurrent Fevers. Ann Rheum Dis (2019) 78(8):1025–32. doi: 10.1136/annrheumdis-2019-215048
15. Van Gijn ME, Ceccherini I, Shinar Y, Carbo EC, Slofstra M, Arostegui JI, et al. New Workflow for Classification of Genetic Variants’ Pathogenicity Applied to Hereditary Recurrent Fevers by the International Study Group for Systemic Autoinflammatory Diseases (INSAID). J Med Genet (2018) 55(8):530–7. doi: 10.1136/jmedgenet-2017-105216
16. Yalçinkaya F, Ozen S, Ozçakar ZB, Aktay N, Cakar N, Düzova A, et al. A New Set of Criteria for the Diagnosis of Familial Mediterranean Fever in Childhood. Rheumatol Oxf Engl (2009) 48(4):395–8. doi: 10.1093/rheumatology/ken509
17. Hennig S, Bayegan K, Uffmann M, Thalhammer F, Winkler S. Pneumonia in a Patient With Familial Mediterranean Fever Successfully Treated With Anakinra–Case Report and Review. Rheumatol Int (2012) 32(6):1801–4. doi: 10.1007/s00296-010-1429-y
18. Bilginer Y, Ayaz NA, Ozen S. Anti-IL-1 Treatment for Secondary Amyloidosis in an Adolescent With FMF and Behçet’s Disease. Clin Rheumatol (2010) 29(2):209–10. doi: 10.1007/s10067-009-1279-8
19. Alpay N, Sumnu A, Calışkan Y, Yazıcı H, Türkmen A, Gül A. Efficacy of Anakinra Treatment in a Patient With Colchicine-Resistant Familial Mediterranean Fever. Rheumatol Int (2012) 32(10):3277–9. doi: 10.1007/s00296-010-1474-6
20. Moser C, Pohl G, Haslinger I, Knapp S, Rowczenio D, Russel T, et al. Successful Treatment of Familial Mediterranean Fever With Anakinra and Outcome After Renal Transplantation. Nephrol Dial Transplant (2009) 24(2):676–8. doi: 10.1093/ndt/gfn646
21. Roldan R, Ruiz AM, Miranda MD, Collantes E. Anakinra: New Therapeutic Approach in Children With Familial Mediterranean Fever Resistant to Colchicine. Jt Bone Spine Rev Rhum (2008) 75(4):504–5. doi: 10.1016/j.jbspin.2008.04.001
22. Mitroulis I, Papadopoulos VP, Konstantinidis T, Ritis K. Anakinra Suppresses Familial Mediterranean Fever Crises in a Colchicine-Resistant Patient. Neth J Med (2008) 66(11):489–91.
23. Calligaris L, Marchetti F, Tommasini A, Ventura A. The Efficacy of Anakinra in an Adolescent With Colchicine-Resistant Familial Mediterranean Fever. Eur J Pediatr (2008) 167(6):695–6. doi: 10.1007/s00431-007-0547-3
24. Belkhir R, Moulonguet-Doleris L, Hachulla E, Prinseau J, Baglin A, Hanslik T. Treatment of Familial Mediterranean Fever With Anakinra. Ann Intern Med (2007) 146(11):825–6. doi: 10.7326/0003-4819-146-11-200706050-00023
25. Kuijk LM, Govers AMAP, Frenkel J, Hofhuis WJD. Effective Treatment of a Colchicine-Resistant Familial Mediterranean Fever Patient With Anakinra. Ann Rheum Dis (2007) 66(11):1545–6. doi: 10.1136/ard.2007.071498
26. Gattringer R, Lagler H, Gattringer KB, Knapp S, Burgmann H, Winkler S, et al. Anakinra in Two Adolescent Female Patients Suffering From Colchicine-Resistant Familial Mediterranean Fever: Effective But Risky. Eur J Clin Invest (2007) 37(11):912–4. doi: 10.1111/j.1365-2362.2007.01868.x
27. Chae JJ, Wood G, Masters SL, Richard K, Park G, Smith BJ, et al. The B30.2 Domain of Pyrin, the Familial Mediterranean Fever Protein, Interacts Directly With Caspase-1 to Modulate IL-1beta Production. Proc Natl Acad Sci USA (2006) 103(26):9982–7. doi: 10.1073/pnas.0602081103
28. Petropoulou AD, Robin M, Socié G, Galicier L. Transmission of Familial Mediterranean Fever Mutation After Bone Marrow Transplantation and Successful Treatment With Anakinra. Transplantation (2010) 90(1):102–3. doi: 10.1097/TP.0b013e3181d84cc3
29. Estublier C, Stankovic Stojanovic K, Bergerot J-F, Broussolle C, Sève P. Myositis in a Patient With Familial Mediterranean Fever and Spondyloarthritis Successfully Treated With Anakinra. Jt Bone Spine Rev Rhum (2013) 80(6):645–9. doi: 10.1016/j.jbspin.2013.03.004
30. Soriano A, Verecchia E, Afeltra A, Landolfi R, Manna R. IL-1β Biological Treatment of Familial Mediterranean Fever. Clin Rev Allergy Immunol (2013) 45(1):117–30. doi: 10.1007/s12016-013-8358-y
31. Celebi ZK, Kucuksahin O, Sengul S, Tuzuner A, Keven K. Colchicine-Resistant Familial Mediterranean Fever in a Renal Transplantation Patient: Successful Treatment With Anakinra. Clin Kidney J (2014) 7(2):219–20. doi: 10.1093/ckj/sft164
32. Mercan R, Turan A, Bitik B, Tufan A, Haznedaroglu S, Goker B. Rapid Resolution of Protracted Febrile Myalgia Syndrome With Anakinra: Report of Two Cases. Mod Rheumatol (2016) 26(3):458–9. doi: 10.3109/14397595.2014.882221
33. Sevillano ÁM, Hernandez E, Gonzalez E, Mateo I, Gutierrez E, Morales E, et al. Anakinra Induces Complete Remission of Nephrotic Syndrome in a Patient With Familial Mediterranean Fever and Amyloidosis. Nefrol Publicacion Of Soc Espanola Nefrol (2016) 36(1):63–6. doi: 10.1016/j.nefroe.2015.10.005
34. Alpa M, Roccatello D. Canakinumab as Rescue Therapy in Familial Mediterranean Fever Refractory to Conventional Treatment. Drug Des Devel Ther (2015) 9:1983–7. doi: 10.2147/DDDT.S69117
35. Jesenak M, Hrubiskova K, Kapustova L, Kostkova M, Banovcin P. Canakinumab as Monotherapy for Treatment of Familial Mediterranean Fever - First Report in Central and Eastern Europe Region. Bratisl Lek Listy (2018) 119(4):198–200. doi: 10.4149/BLL_2018_036
36. Sozeri B, Gulez N, Ergin M, Serdaroglu E. The Experience of Canakinumab in Renal Amyloidosis Secondary to Familial Mediterranean Fever. Mol Cell Pediatr (2016) 3(1):33. doi: 10.1186/s40348-016-0058-2
37. Hacihamdioglu DO, Ozen S. Canakinumab Induces Remission in a Patient With Resistant Familial Mediterranean Fever. Rheumatol Oxf Engl (2012) 51(6):1041. doi: 10.1093/rheumatology/kes021
38. Georgin-Lavialle S, Stankovic Stojanovic K, Bachmeyer C, Sellam J, Abbara S, Awad F, et al. Spondyloarthritis Associated With Familial Mediterranean Fever: Successful Treatment With Anakinra. Rheumatol Oxf Engl (2017) 56(1):167–9. doi: 10.1093/rheumatology/kew290
39. Abbara S, Georgin-Lavialle S, Stankovic Stojanovic K, Bachmeyer C, Senet P, Buob D, et al. Association of Hidradenitis Suppurativa and Familial Mediterranean Fever: A Case Series of 6 Patients. Jt Bone Spine Rev Rhum (2017) 84(2):159–62. doi: 10.1016/j.jbspin.2016.02.021
40. Espíldora-Hernández J, Abarca-Costalago M. Familial Mediterranean Fever Treated With Anakinra: A Case Report. Reumatol Clin (2017) 13(2):120–1. doi: 10.1016/j.reuma.2016.06.001
41. Gentileschi S, Rigante D, Vitale A, Sota J, Frediani B, Galeazzi M, et al. Efficacy and Safety of Anakinra in Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) Complicated by Severe Renal Failure: A Report After Long-Term Follow-Up and Review of the Literature. Clin Rheumatol (2017) 36(7):1687–90. doi: 10.1007/s10067-017-3688-4
42. Camprubí D, Mitjavila F, Arostegui JI, Corbella X. Efficacy of Anakinra in an Adult Patient With Recurrent Pericarditis and Cardiac Tamponade as Initial Manifestations of Tumor Necrosis Factor Receptor-Associated Periodic Syndrome Due to the R92Q TNFRSF1A Variant. Int J Rheum Dis (2017) 20(4):510–4. doi: 10.1111/1756-185X.13029
43. Cattalini M, Meini A, Monari P, Gualdi G, Arisi M, Pelucchi F, et al. Recurrent Migratory Angioedema as Cutaneous Manifestation in a Familiar Case of TRAPS: Dramatic Response to Anakinra. Dermatol Online J (2013) 19(11):20405.
44. Lopalco G, Rigante D, Vitale A, Frediani B, Iannone F, Cantarini L. Tumor Necrosis Factor Receptor-Associated Periodic Syndrome Managed With the Couple Canakinumab-Alendronate. Clin Rheumatol (2015) 34(4):807–9. doi: 10.1007/s10067-014-2556-8
45. La Torre F, Muratore M, Vitale A, Moramarco F, Quarta L, Cantarini L. Canakinumab Efficacy and Long-Term Tocilizumab Administration in Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS). Rheumatol Int (2015) 35(11):1943–7. doi: 10.1007/s00296-015-3305-2
46. Simon A, Bodar EJ, van der Hilst JCH, van der Meer JWM, Fiselier TJW, Cuppen MPJM, et al. Beneficial Response to Interleukin 1 Receptor Antagonist in Traps. Am J Med (2004) 117(3):208–10. doi: 10.1016/j.amjmed.2004.02.039
47. Andrés M, Pascual E. Anakinra for a Refractory Case of Intermittent Hydrarthrosis With a TRAPS-Related Gene Mutation. Ann Rheum Dis (2013) 72(1):155. doi: 10.1136/annrheumdis-2012-202087
48. Sacré K, Brihaye B, Lidove O, Papo T, Pocidalo MA, Cuisset L, et al. Dramatic Improvement Following Interleukin 1beta Blockade in Tumor Necrosis Factor Receptor-1-Associated Syndrome (TRAPS) Resistant to Anti-TNF-Alpha Therapy. J Rheumatol (2008) 35(2):357–8.
49. Brizi MG, Galeazzi M, Lucherini OM, Cantarini L, Cimaz R. Successful Treatment of Tumor Necrosis Factor Receptor-Associated Periodic Syndrome With Canakinumab. Ann Intern Med (2012) 156(12):907–8. doi: 10.7326/0003-4819-156-12-201206190-00027
50. Arad U, Niv E, Caspi D, Elkayam O. “Trap” the Diagnosis: A Man With Recurrent Episodes of Febrile Peritonitis, Not Just Familial Mediterranean Fever. Isr Med Assoc J (2012) 14(4):229–31.
51. Horneff G, Rhouma A, Weber C, Lohse P. Macrophage Activation Syndrome as the Initial Manifestation of Tumour Necrosis Factor Receptor 1-Associated Periodic Syndrome (TRAPS). Clin Exp Rheumatol (2013) 31(3 Suppl 77):99–102.
52. Quillinan N, Mannion G, Mohammad A, Coughlan R, Dickie LJ, McDermott MF, et al. Failure of Sustained Response to Etanercept and Refractoriness to Anakinra in Patients With T50M TNF-Receptor-Associated Periodic Syndrome. Ann Rheum Dis (2011) 70(9):1692–3. doi: 10.1136/ard.2010.144279
53. Cantarini L, Lopalco G, Vitale A, Caso F, Lapadula G, Iannone F, et al. Delights and Let-Downs in the Management of Tumor Necrosis Factor Receptor-Associated Periodic Syndrome: The Canakinumab Experience in a Patient With a High-Penetrance T50M TNFRSF1A Variant. Int J Rheum Dis (2015) 18(4):473–5. doi: 10.1111/1756-185X.12521
54. Nevyjel M, Pontillo A, Calligaris L, Tommasini A, D’Osualdo A, Waterham HR, et al. Diagnostics and Therapeutic Insights in a Severe Case of Mevalonate Kinase Deficiency. Pediatrics (2007) 119(2):e523–7. doi: 10.1542/peds.2006-2015
55. Lequerré T, Vittecoq O, Pouplin S, Klemmer N, Mejjad O, Daragon A, et al. Mevalonate Kinase Deficiency Syndrome With Structural Damage Responsive to Anakinra. Rheumatol Oxf Engl (2007) 46(12):1860–2. doi: 10.1093/rheumatology/kem258
56. Bodar EJ, van der Hilst JCH, Drenth JPH, van der Meer JWM, Simon A. Effect of Etanercept and Anakinra on Inflammatory Attacks in the Hyper-IgD Syndrome: Introducing a Vaccination Provocation Model. Neth J Med (2005) 63(7):260–4.
57. Rigante D, Capoluongo E, Bertoni B, Ansuini V, Chiaretti A, Piastra M, et al. First Report of Macrophage Activation Syndrome in Hyperimmunoglobulinemia D With Periodic Fever Syndrome. Arthritis Rheumatol (2007) 56(2):658–61. doi: 10.1002/art.22409
58. Korppi M, Van Gijn ME, Antila K. Hyperimmunoglobulinemia D and Periodic Fever Syndrome in Children. Review on Therapy with Biological Drugs and Case Report. Acta Paediatr (2011) 100(1):21–5. doi: 10.1111/j.1651-2227.2010.01974.x
59. Ruiz Gomez A, Couce ML, Garcia-Villoria J, Torres A, Baña Souto A, Yagüe J, et al. Clinical, Genetic, and Therapeutic Diversity in 2 Patients With Severe Mevalonate Kinase Deficiency. Pediatrics (2012) 129(2):e535–9. doi: 10.1542/peds.2010-2192
60. Cailliez M, Garaix F, Rousset-Rouvière C, Bruno D, Kone-Paut I, Sarles J, et al. Anakinra is Safe and Effective in Controlling Hyperimmunoglobulinaemia D Syndrome-Associated Febrile Crisis. J Inherit Metab Dis (2006) 29(6):763. doi: 10.1007/s10545-006-0408-7
61. Levy M, Arion A, Berrebi D, Cuisset L, Jeanne-Pasquier C, Bader-Meunier B, et al. Severe Early-Onset Colitis Revealing Mevalonate Kinase Deficiency. Pediatrics (2013) 132(3):e779–83. doi: 10.1542/peds.2012-3344
62. Shendi HM, Walsh D, Edgar JDM. Etanercept and Anakinra can Prolong Febrile Episodes in Patients With Hyperimmunoglobulin D and Periodic Fever Syndrome. Rheumatol Int (2012) 32(1):249–51. doi: 10.1007/s00296-009-1322-8
63. Schulert GS, Bove K, McMasters R, Campbell K, Leslie N, Grom AA. 11-Month-Old Infant With Periodic Fevers, Recurrent Liver Dysfunction, and Perforin Gene Polymorphism. Arthritis Care Res (2015) 67(8):1173–9. doi: 10.1002/acr.22527
64. Campanilho-Marques R, Brogan PA. Mevalonate Kinase Deficiency in Two Sisters With Therapeutic Response to Anakinra: Case Report and Review of the Literature. Clin Rheumatol (2014) 33(11):1681–4. doi: 10.1007/s10067-014-2523-4
65. Kostjukovits S, Kalliokoski L, Antila K, Korppi M. Treatment of Hyperimmunoglobulinemia D Syndrome With Biologics in Children: Review of the Literature and Finnish Experience. Eur J Pediatr (2015) 174(6):707–14. doi: 10.1007/s00431-015-2505-9
66. Thors VS, Vastert SJ, Wulffraat N, van Royen A, Frenkel J, de Sain-van der Velden M, et al. Periodic Fever in MVK Deficiency: A Patient Initially Diagnosed With Incomplete Kawasaki Disease. Pediatrics (2014) 133(2):e461–465. doi: 10.1542/peds.2012-1372
67. Santos JA, Aróstegui JI, Brito MJ, Neves C, Conde M. Hyper-IgD and Periodic Fever Syndrome: A New MVK Mutation (P.R277G) Associated With a Severe Phenotype. Gene (2014) 542(2):217–20. doi: 10.1016/j.gene.2014.03.031
68. Curtis CD, Fox CC. Treatment of Adult Hyper-IgD Syndrome With Canakinumab. J Allergy Clin Immunol Pract (2015) 3(5):817–8. doi: 10.1016/j.jaip.2015.05.020
69. Kallianidis AF, Ray A, Goudkade D, de Fijter JW. Amyloid A Amyloidosis Secondary to Hyper IgD Syndrome and Response to IL-1 Blockage Therapy. Neth J Med (2016) 74(1):43–6.
70. Peciuliene S, Burnyte B, Gudaitiene R, Rusoniene S, Drazdiene N, Liubsys A, et al. Perinatal Manifestation of Mevalonate Kinase Deficiency and Efficacy of Anakinra. Pediatr Rheumatol Online J (2016) 14(1):19. doi: 10.1186/s12969-016-0081-9
71. Li Cavoli G, Passantino D, Tortorici C, Bono L, Ferrantelli A, Giammarresi C, et al. Renal Amyloidosis Due to Hyper-IgD Syndrome. Nefrologia (2012) 32(6):865–6. doi: 10.3265/Nefrologia.pre2012.Aug.11660
72. Lachmann HJ, Goodman HJB, Andrews PA, Gallagher H, Marsh J, Breuer S, et al. AA Amyloidosis Complicating Hyperimmunoglobulinemia D With Periodic Fever Syndrome: A Report of Two Cases. Arthritis Rheumatol (2006) 54(6):2010–4. doi: 10.1002/art.21901
73. Erdol S, Cekic S, Kılıc SC, Saglam H, Kılıc SS. Massive Ascites in a Canakinumab Resistant Case With MVA Leading to Bone Marrow Transplantation. Rheumatol Int (2016) 36(7):1011–3. doi: 10.1007/s00296-016-3456-9
74. Tsitsami E, Papadopoulou C, Speletas M. A Case of Hyperimmunoglobulinemia D Syndrome Successfully Treated With Canakinumab. Case Rep Rheumatol (2013) 2013:795027. doi: 10.1155/2013/795027
75. Dunn K, Pasternak B, Kelsen JR, Sullivan KE, Dawany N, Wright BL. Mevalonate Kinase Deficiency Presenting as Recurrent Rectal Abscesses and Perianal Fistulae. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol (2018) 120(2):214–5. doi: 10.1016/j.anai.2017.11.011
76. Laccetta G, Tutera M, Miccoli M, Consolini R. Effects of Anakinra on Health-Related Quality of Life in a Patient With 1129G>A/928G>A Mutations in MVK Gene and Heterozygosity for the Mutation 2107c>A in CIAS1 Gene. Front Pediatr (2017) 5:128. doi: 10.3389/fped.2017.00128
77. Tanaka T, Yoshioka K, Nishikomori R, Sakai H, Abe J, Yamashita Y, et al. National Survey of Japanese Patients With Mevalonate Kinase Deficiency Reveals Distinctive Genetic and Clinical Characteristics. Mod Rheumatol (2019) 29(1):181–7. doi: 10.1080/14397595.2018.1442639
78. Grimwood C, Despert V, Jeru I, Hentgen V. On-Demand Treatment With Anakinra: A Treatment Option for Selected TRAPS Patients. Rheumatol Oxf Engl (2015) 54(9):1749–51. doi: 10.1093/rheumatology/kev111
79. Yildirim T, Yilmaz R, Uzerk Kibar M, Erdem Y. Canakinumab Treatment in Renal Transplant Recipients With Familial Mediterranean Fever. J Nephrol (2018) 31(3):453–5. doi: 10.1007/s40620-018-0475-5
80. Cakan M, Karadag SG, Ayaz NA. Corticosteroid-Resistant Anakinra-Responsive Protracted Febrile Myalgia Syndrome as the First Manifestation of Familial Mediterranean Fever. North Clin Istanb (2019) 7(1):78–80. doi: 10.14744/nci.2019.38243
81. Kaly L, Rozenbaum M, Rimar D, Slobodin G, Boulman N, Awisat A, et al. Ulcerative Colitis and Familial Mediterranean Fever: Can Anakinra Treat Both? ACG Case Rep J (2019) 6(7):e00143. doi: 10.14309/crj.0000000000000143
82. Coppola T, Becken B, Van Mater H, McDonald MT, Panayotti GM. A Case Report of Mevalonate Kinase Deficiency in a 14-Month-Old Female With Fevers and Lower Extremity Weakness. BMC Pediatr (2019) 19(1):245. doi: 10.1186/s12887-019-1617-1
83. Maggio MC, Ceccherini I, Grossi A, Gattorno M, Corsello G. PAPA and FMF in Two Siblings: Possible Amplification of Clinical Presentation? A Case Report. Ital J Pediatr (2019) 45(1):111. doi: 10.1186/s13052-019-0705-z
84. Meinzer U, Quartier P, Alexandra J-F, Hentgen V, Retornaz F, Koné-Paut I. Interleukin-1 Targeting Drugs in Familial Mediterranean Fever: A Case Series and a Review of the Literature. Semin Arthritis Rheumatol (2011) 41(2):265–71. doi: 10.1016/j.semarthrit.2010.11.003
85. Ozen S, Bilginer Y, Aktay Ayaz N, Calguneri M. Anti-Interleukin 1 Treatment for Patients With Familial Mediterranean Fever Resistant to Colchicine. J Rheumatol (2011) 38(3):516–8. doi: 10.3899/jrheum.100718
86. Stankovic Stojanovic K, Delmas Y, Torres PU, Peltier J, Pelle G, Jéru I, et al. Dramatic Beneficial Effect of Interleukin-1 Inhibitor Treatment in Patients With Familial Mediterranean Fever Complicated With Amyloidosis and Renal Failure. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc - Eur Ren Assoc (2012) 27(5):1898–901. doi: 10.1093/ndt/gfr528
87. Pelagatti MA, Meini A, Caorsi R, Cattalini M, Federici S, Zulian F, et al. Long-Term Clinical Profile of Children With the Low-Penetrance R92Q Mutation of the TNFRSF1A Gene. Arthritis Rheumatol (2011) 63(4):1141–50. doi: 10.1002/art.30237
88. Talerico R, Cardillo C, De Vito F, Schinzari F, Soldato M, Giustiniani MC, et al. Mesothelioma in Familial Mediterranean Fever With Colchicine Intolerance: A Case Report and Literature Review. Front Immunol (2020) 0:889/full. doi: 10.3389/fimmu.2020.00889/full
89. Özçakar ZB, Özdel S, Yılmaz S, Kurt-Şükür ED, Ekim M, Yalçınkaya F. Anti-IL-1 Treatment in Familial Mediterranean Fever and Related Amyloidosis. Clin Rheumatol (2016) 35(2):441–6. doi: 10.1007/s10067-014-2772-2
90. Özçakar ZB, Keven K, Çakar N, Yalçınkaya F. Transplantation Within the Era of Anti-IL-1 Therapy: Case Series of Five Patients With Familial Mediterranean Fever-Related Amyloidosis. Transpl Int (2018) 31(10):1181–4. doi: 10.1111/tri.13312
91. Cetin P, Sari I, Sozeri B, Cam O, Birlik M, Akkoc N, et al. Efficacy of Interleukin-1 Targeting Treatments in Patients With Familial Mediterranean Fever. Inflammation (2015) 38(1):27–31. doi: 10.1007/s10753-014-0004-1
92. Eroglu FK, Beşbaş N, Topaloglu R, Ozen S. Treatment of Colchicine-Resistant Familial Mediterranean Fever in Children and Adolescents. Rheumatol Int (2015) 35(10):1733–7. doi: 10.1007/s00296-015-3293-2
93. Yazılıtaş F, Aydoğ Ö, Özlü SG, Çakıcı EK, Güngör T, Eroğlu FK, et al. Canakinumab Treatment in Children With Familial Mediterranean Fever: Report From a Single Center. Rheumatol Int (2018) 38(5):879–85. doi: 10.1007/s00296-018-3993-5
94. Kucuksahin O, Yildizgoren MT, Ilgen U, Ates A, Kinikli G, Turgay M, et al. Anti-Interleukin-1 Treatment in 26 Patients With Refractory Familial Mediterranean Fever. Mod Rheumatol (2017) 27(2):350–5. doi: 10.1080/14397595.2016.1194510
95. Rossi-Semerano L, Fautrel B, Wendling D, Hachulla E, Galeotti C, Semerano L, et al. Tolerance and Efficacy of Off-Label Anti-Interleukin-1 Treatments in France: A Nationwide Survey. Orphanet J Rare Dis (2015) 10:19. doi: 10.1186/s13023-015-0228-7
96. Ozen S, Kuemmerle-Deschner JB, Cimaz R, Livneh A, Quartier P, Kone-Paut I, et al. International Retrospective Chart Review of Treatment Patterns in Severe Familial Mediterranean Fever, Tumor Necrosis Factor Receptor-Associated Periodic Syndrome, and Mevalonate Kinase Deficiency/Hyperimmunoglobulinemia D Syndrome. Arthritis Care Res (2017) 69(4):578–86. doi: 10.1002/acr.23120
97. Laskari K, Boura P, Dalekos GN, Garyfallos A, Karokis D, Pikazis D, et al. Longterm Beneficial Effect of Canakinumab in Colchicine-Resistant Familial Mediterranean Fever. J Rheumatol (2017) 44(1):102–9. doi: 10.3899/jrheum.160518
98. Vitale A, Insalaco A, Sfriso P, Lopalco G, Emmi G, Cattalini M, et al. A Snapshot on the On-Label and Off-Label Use of the Interleukin-1 Inhibitors in Italy Among Rheumatologists and Pediatric Rheumatologists: A Nationwide Multi-Center Retrospective Observational Study. Front Pharmacol (2016) 7:380. doi: 10.3389/fphar.2016.00380
99. Gattorno M, Obici L, Cattalini M, Tormey V, Abrams K, Davis N, et al. Canakinumab Treatment for Patients With Active Recurrent or Chronic TNF Receptor-Associated Periodic Syndrome (TRAPS): An Open-Label, Phase II Study. Ann Rheum Dis (2017) 76(1):173–8. doi: 10.1136/annrheumdis-2015-209031
100. Ter Haar N, Lachmann H, Özen S, Woo P, Uziel Y, Modesto C, et al. Treatment of Autoinflammatory Diseases: Results From the Eurofever Registry and a Literature Review. Ann Rheum Dis (2013) 72(5):678–85. doi: 10.1136/annrheumdis-2011-201268
101. Gattorno M, Obici L, Meini A, Tormey V, Abrams K, Davis N, et al. THU0396 Efficacy and Safety of Canakinumab in Patients With TNF Receptor Associated Periodic Syndrome (TRAPS). Ann Rheum Dis (2013) 71(Suppl 3):289–9. doi: 10.1136/annrheumdis-2012-eular.2361
102. Ugurlu S, Seyahi E, Hatemi G, Hacioglu A, Akkoc NF, Ozdogan H. THU0402 Canakinumab Therapy in Patients With Familial Mediterranean Fever. Ann Rheum Dis (2014) 73(Suppl 2):320–1. doi: 10.1136/annrheumdis-2014-eular.5654
103. Bodar EJ, Kuijk LM, Drenth JPH, van der Meer JWM, Simon A, Frenkel J. On-Demand Anakinra Treatment is Effective in Mevalonate Kinase Deficiency. Ann Rheum Dis (2011) 70(12):2155–8. doi: 10.1136/ard.2011.149922
104. Galeotti C, Meinzer U, Quartier P, Rossi-Semerano L, Bader-Meunier B, Pillet P, et al. Efficacy of Interleukin-1-Targeting Drugs in Mevalonate Kinase Deficiency. Rheumatol Oxf Engl (2012) 51(10):1855–9. doi: 10.1093/rheumatology/kes097
105. Bader-Meunier B, Florkin B, Sibilia J, Acquaviva C, Hachulla E, Grateau G, et al. Mevalonate Kinase Deficiency: A Survey of 50 Patients. Pediatrics (2011) 128(1):e152–159. doi: 10.1542/peds.2010-3639
106. Deshayes S, Georgin-Lavialle S, Hot A, Durel C-A, Hachulla E, Rouanes N, et al. Efficacy of Continuous Interleukin 1 Blockade in Mevalonate Kinase Deficiency: A Multicenter Retrospective Study in 13 Adult Patients and Literature Review. J Rheumatol (2018) 45(3):425–9. doi: 10.3899/jrheum.170684
107. Ter Haar NM, Jeyaratnam J, Lachmann HJ, Simon A, Brogan PA, Doglio M, et al. The Phenotype and Genotype of Mevalonate Kinase Deficiency: A Series of 114 Cases From the Eurofever Registry. Arthritis Rheumatol Hoboken NJ (2016) 68(11):2795–805. doi: 10.1002/art.39763
108. Ergezen B, Ugurlu S, Ozdogan H. FRI0596 Anakinra Treatment in Patients With Familial Mediterranean Fever: A Single-Center Experience (Case Series). Ann Rheum Dis (2017) 76(Suppl 2):714–5. doi: 10.1136/annrheumdis-2017-eular.5436
109. Köhler BM, Lorenz H-M, Blank N. IL1-Blocking Therapy in Colchicine-Resistant Familial Mediterranean Fever. Eur J Rheumatol (2018) 5(4):230–4. doi: 10.5152/eurjrheum.2018.18036
110. Babaoglu H, Varan O, Kucuk H, Atas N, Satis H, Salman R, et al. Effectiveness of Canakinumab in Colchicine- and Anakinra-Resistant or -Intolerant Adult Familial Mediterranean Fever Patients: A Single-Center Real-Life Study. J Clin Rheumatol (2018) 26(1):7–13. doi: 10.1097/RHU.0000000000000873
111. Varan Ö, Kucuk H, Babaoglu H, Guven SC, Ozturk MA, Haznedaroglu S, et al. Efficacy and Safety of Interleukin-1 Inhibitors in Familial Mediterranean Fever Patients Complicated With Amyloidosis. Mod Rheumatol (2019) 29(2):363–6. doi: 10.1080/14397595.2018.1457469
112. Gülez N, Makay B, Sözeri B. Long-Term Effectiveness and Safety of Canakinumab in Pediatric Familial Mediterranean Fever Patients. Mod Rheumatol (2020) 30(1):166–71. doi: 10.1080/14397595.2018.1559488
113. Akar S, Cetin P, Kalyoncu U, Karadag O, Sari I, Cınar M, et al. Nationwide Experience With Off-Label Use of Interleukin-1 Targeting Treatment in Familial Mediterranean Fever Patients. Arthritis Care Res (2018) 70(7):1090–4. doi: 10.1002/acr.23446
114. Berdeli A, Şenol Ö, Talay G. Treatment of Familial Mediterranean Fever With Canakinumab in Patients Who are Unresponsive to Colchicine. Eur J Rheumatol (2019) 6(2):85–8. doi: 10.5152/eurjrheum.2019.18190
115. Pecher A-C, Igney-Oertel A, Kanz L, Henes J. Treatment of Familial Mediterranean Fever With Anakinra in Patients Unresponsive to Colchicine. Scand J Rheumatol (2017) 46(5):407–9. doi: 10.1080/03009742.2016.1245780
116. Trabulus S, Korkmaz M, Kaya E, Seyahi N. Canakinumab Treatment in Kidney Transplant Recipients With AA Amyloidosis Due to Familial Mediterranean Fever. Clin Transplant (2018) 32(8):e13345. doi: 10.1111/ctr.13345
117. Başaran Ö, Uncu N, Çelikel BA, Taktak A, Gür G, Cakar N. Interleukin-1 Targeting Treatment in Familial Mediterranean Fever: An Experience of Pediatric Patients. Mod Rheumatol (2015) 25(4):621–4. doi: 10.3109/14397595.2014.987437
118. Obici L, Meini A, Cattalini M, Chicca S, Galliani M, Donadei S, et al. Favourable and Sustained Response to Anakinra in Tumour Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) With or Without AA Amyloidosis. Ann Rheum Dis (2011) 70(8):1511–2. doi: 10.1136/ard.2010.143438
119. Gaggiano C, Vitale A, Obici L, Merlini G, Soriano A, Viapiana O, et al. Clinical Features at Onset and Genetic Characterization of Pediatric and Adult Patients With TNF-α Receptor-Associated Periodic Syndrome (TRAPS): A Series of 80 Cases From the AIDA Network. Mediators Inflammation (2020) 2020:8562485. doi: 10.1155/2020/8562485
120. Gül A, Ozdogan H, Erer B, Ugurlu S, Kasapcopur O, Davis N, et al. Efficacy and Safety of Canakinumab in Adolescents and Adults With Colchicine-Resistant Familial Mediterranean Fever. Arthritis Res Ther (2015) 17:243. doi: 10.1186/s13075-015-0765-4
121. Brik R, Butbul-Aviel Y, Lubin S, Ben Dayan E, Rachmilewitz-Minei T, Tseng L, et al. Canakinumab for the Treatment of Children With Colchicine-Resistant Familial Mediterranean Fever: A 6-Month Open-Label, Single-Arm Pilot Study. Arthritis Rheumatol Hoboken NJ (2014) 66(11):3241–3. doi: 10.1002/art.38777
122. Arostegui JI, Anton J, Calvo I, Robles A, Iglesias E, López-Montesinos B, et al. Open-Label, Phase II Study to Assess the Efficacy and Safety of Canakinumab Treatment in Active Hyperimmunoglobulinemia D With Periodic Fever Syndrome. Arthritis Rheumatol Hoboken NJ (2017) 69(8):1679–88. doi: 10.1002/art.40146
123. PNDS - Déficit En Mévalonate Kinase (MKD), Vol. 47. Available at: https://www.has-sante.fr/upload/docs/application/pdf/2015-07/pnds_-_deficit_en_mevalonate_kinase_mkd.pdf
124. Pnds_-_Traps_Tumor_Necrosis_Factor-Receptor-Associated_Periodic_Syndrome_Ou_Syndrome_De_Fievre_Recurrente_Lie_Au_Recepteur_D.Pdf. Available at: https://www.has-sante.fr/portail/upload/docs/application/pdf/2018-07/pnds_-_traps_tumor_necrosis_factor-receptor-associated_periodic_syndrome_ou_syndrome_de_fievre_recurrente_lie_au_recepteur_d.pdf.
125. ter Haar NM, Oswald M, Jeyaratnam J, Anton J, Barron KS, Brogan PA, et al. Recommendations for the Management of Autoinflammatory Diseases. Ann Rheum Dis (2015) 74(9):1636–44. doi: 10.1136/annrheumdis-2015-207546
126. Hentgen V, Grateau G, Kone-Paut I, Livneh A, Padeh S, Rozenbaum M, et al. Evidence-Based Recommendations for the Practical Management of Familial Mediterranean Fever. Semin Arthritis Rheumatol (2013) 43(3):387–91. doi: 10.1016/j.semarthrit.2013.04.011
127. Ozen S, Demirkaya E, Erer B, Livneh A, Ben-Chetrit E, Giancane G, et al. EULAR Recommendations for the Management of Familial Mediterranean Fever. Ann Rheum Dis (2016) 75(4):644–51. doi: 10.1136/annrheumdis-2015-208690
128. Corsia A, Georgin-Lavialle S, Hentgen V, Hachulla E, Grateau G, Faye A, et al. A Survey of Resistance to Colchicine Treatment for French Patients With Familial Mediterranean Fever. Orphanet J Rare Dis (2017) 12(1):54. doi: 10.1186/s13023-017-0609-1
129. Özen S, Sag E, Ben-Chetrit E, Gattorno M, Gül A, Hashkes PJ, et al. Defining Colchicine Resistance/Intolerance in Patients With Familial Mediterranean Fever: A Modified-Delphi Consensus Approach. Rheumatology (Oxford) (2021) 60(8):3799–808. doi: 10.1093/rheumatology/keaa863
130. Kacar M, Savic S, van der Hilst JCH. The Efficacy, Safety and Tolerability of Canakinumab in the Treatment of Familial Mediterranean Fever: A Systematic Review of the Literature. J Inflamm Res (2020) 13:141–9. doi: 10.2147/JIR.S206204
131. Gül A. Treatment of Familial Mediterranean Fever: Colchicine and Beyond. Isr Med Assoc J (2014) 16(5):281–4.
132. Bustaffa M, Mazza F, Sutera D, Carrabba MD, Alessio M, Cantarini L, et al. Persistence of Disease Flares is Associated With an Inadequate Colchicine Dose in Familial Mediterranean Fever: A National Multicenter Longitudinal Study. J Allergy Clin Immunol Pract (2021) 9(8):3218–20. doi: 10.1016/j.jaip.2021.03.048
133. Ozen S, Kone-Paut I, Gül A. Colchicine Resistance and Intolerance in Familial Mediterranean Fever: Definition, Causes, and Alternative Treatments. Semin Arthritis Rheum (2017) 47(1):115–20. doi: 10.1016/j.semarthrit.2017.03.006
134. Tekgöz E, Çolak S, Çinar FI, Yilmaz S, Çinar M. Non-Adherence to Colchicine Treatment Is a Common Misevaluation in Familial Mediterranean Fever. Turk J Med Sci (2021) 51(5):2357–63. doi: 10.3906/sag-2102-328
135. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive Validity of A Medication Adherence Measure in an Outpatient Setting. J Clin Hypertens Greenwich Conn (2008) 10(5):348–54. doi: 10.1111/j.1751-7176.2008.07572.x
136. Georgin-Lavialle S, Abe E, Larabi A, Savey L, Ducharme-Bénard S, Hentgen V, et al. Could We Measure Hair Colchicine to Assess Colchicine Observance in Familial Mediterranean Fever? Rheumatol Oxf Engl (2021) 60(3):1563–4. doi: 10.1093/rheumatology/keaa811
137. Bulua AC, Mogul DB, Aksentijevich I, Singh H, He DY, Muenz LR, et al. Efficacy of Etanercept in the Tumor Necrosis Factor Receptor-Associated Periodic Syndrome: A Prospective, Open-Label, Dose-Escalation Study. Arthritis Rheumatol (2012) 64(3):908–13. doi: 10.1002/art.33416
138. Jacobelli S, André M, Alexandra J-F, Dodé C, Papo T. Failure of Anti-TNF Therapy in TNF Receptor 1-Associated Periodic Syndrome (TRAPS). Rheumatol Oxf Engl (2007) 46(7):1211–2. doi: 10.1093/rheumatology/kel298
139. Vitale A, Obici L, Cattalini M, Lopalco G, Merlini G, Ricco N, et al. Biotechnological Agents for Patients With Tumor Necrosis Factor Receptor Associated Periodic Syndrome-Therapeutic Outcome and Predictors of Response: Real-Life Data From the AIDA Network. Front Med (2021) 8:668173. doi: 10.3389/fmed.2021.668173
140. Watad A, Tiosano S, Yahav D, Comaneshter D, Shoenfeld Y, Cohen AD, et al. Behçet’s Disease and Familial Mediterranean Fever: Two Sides of the Same Coin or Just an Association? A Cross-Sectional Study. Eur J Intern Med (2017) 39:75–8. doi: 10.1016/j.ejim.2016.10.011
141. Ozdogan H, Arisoy N, Kasapçapur O, Sever L, Calişkan S, Tuzuner N, et al. Vasculitis in Familial Mediterranean Fever. J Rheumatol (1997) 24(2):323–7.
142. Akar S, Soysal O, Balci A, Solmaz D, Gerdan V, Onen F, et al. High Prevalence of Spondyloarthritis and Ankylosing Spondylitis Among Familial Mediterranean Fever Patients and Their First-Degree Relatives: Further Evidence for the Connection. Arthritis Res Ther (2013) 15(1):R21. doi: 10.1186/ar4154
143. Hodak E, Atzmony L, Pavlovsky L, Comaneshter D, Cohen AD. Hidradenitis Suppurativa Is Associated With Familial Mediterranean Fever-A Population-Based Study. J Invest Dermatol (2017) 137(9):2019–21. doi: 10.1016/j.jid.2017.04.024
144. Villani A-C, Lemire M, Louis E, Silverberg MS, Collette C, Fortin G, et al. Genetic Variation in the Familial Mediterranean Fever Gene (MEFV) and Risk for Crohn’s Disease and Ulcerative Colitis. PloS One (2009) 4(9):e7154. doi: 10.1371/journal.pone.0007154
145. Yahalom G, Kivity S, Lidar M, Vaknin-Dembinsky A, Karussis D, Flechter S, et al. Familial Mediterranean Fever (FMF) and Multiple Sclerosis: An Association Study in One of the World’s Largest FMF Cohorts. Eur J Neurol (2011) 18(9):1146–50. doi: 10.1111/j.1468-1331.2011.03356.x
146. Lane T, Loeffler JM, Rowczenio DM, Gilbertson JA, Bybee A, Russell TL, et al. AA Amyloidosis Complicating the Hereditary Periodic Fever Syndromes. Arthritis Rheumatol (2013) 65(4):1116–21. doi: 10.1002/art.37827
147. Rodziewicz N, Bhushan S, Avasia A, Singh N. Kidney Transplant in a Patient With Tumor Necrosis Factor Receptor-1 Syndrome (TRAPS): Case Report and Review of the Literature. Transplant Proc (2016) 48(1):265–6. doi: 10.1016/j.transproceed.2015.11.006
148. Delaleu J, Deshayes S, Rodrigues F, Savey L, Rivière E, Martin Silva N, et al. Tumor Necrosis Factor Receptor-1 Assciated Periodic Syndrome (TRAPS) Related AA Amyloidosis: A National Case Series and Systematic Review. Rheumatology (Oxford) (2021) keab252. doi: 10.1093/rheumatology/keab252
149. Ozen S, Demirkaya E, Duzova A, Erdogan O, Erken E, Gul A, et al. FMF50: A Score for Assessing Outcome in Familial Mediterranean Fever. Ann Rheum Dis (2014) 73(5):897–901. doi: 10.1136/annrheumdis-2013-204719
150. Pras E, Livneh A, Balow JE, Pras E, Kastner DL, Pras M, et al. Clinical Differences Between North African and Iraqi Jews With Familial Mediterranean Fever. Am J Med Genet (1998) 75(2):216–9. doi: 10.1002/(SICI)1096-8628(19980113)75:2<216::AID-AJMG20>3.0.CO;2-R
151. Mor A, Shinar Y, Zaks N, Langevitz P, Chetrit A, Shtrasburg S, et al. Evaluation of Disease Severity in Familial Mediterranean Fever. Semin Arthritis Rheumatol (2005) 35(1):57–64. doi: 10.1016/j.semarthrit.2005.02.002
152. Ozen S, Aktay N, Lainka E, Duzova A, Bakkaloglu A, Kallinich T. Disease Severity in Children and Adolescents With Familial Mediterranean Fever: A Comparative Study to Explore Environmental Effects on a Monogenic Disease. Ann Rheum Dis (2009) 68(2):246–8. doi: 10.1136/ard.2008.092031
153. Demirkaya E, Acikel C, Hashkes P, Gattorno M, Gul A, Ozdogan H, et al. Development and Initial Validation of International Severity Scoring System for Familial Mediterranean Fever (ISSF). Ann Rheum Dis (2016) 75(6):1051–6. doi: 10.1136/annrheumdis-2015-208671
154. Piram M, Koné-Paut I, Lachmann HJ, Frenkel J, Ozen S, Kuemmerle-Deschner J, et al. Validation of the Auto-Inflammatory Diseases Activity Index (AIDAI) for Hereditary Recurrent Fever Syndromes. Ann Rheum Dis (2014) 73(12):2168–73. doi: 10.1136/annrheumdis-2013-203666
155. Buskila D, Zaks N, Neumann L, Livneh A, Greenberg S, Pras M, et al. Quality of Life of Patients With Familial Mediterranean Fever. Clin Exp Rheumatol (1997) 15(4):355–60.
156. Giese A, Kurucay M, Kilic L, Örnek A, Şendur SN, Lainka E, et al. Quality of Life in Adult Patients With Familial Mediterranean Fever Living in Germany or Turkey Compared to Healthy Subjects: A Study Evaluating the Effect of Disease Severity and Country of Residence. Rheumatol Int (2013) 33(7):1713–9. doi: 10.1007/s00296-012-2622-y
157. Sahin S, Yalcin I, Senel S, Ataseven H, Uslu A, Yildirim O, et al. Assesment Life Quality of Familial Mediterranean Fever Patients by Short Form-36 and its Relationship With Disease Parameters. Eur Rev Med Pharmacol Sci (2013) 17(7):958–63.
158. Yildirim DG, Bakkaloglu SA, Acar ASS, Celik B, Buyan N. Evaluation of Quality of Life and Its Associations With Clinical Parameters in Pediatric Patients With Familial Mediterranean Fever. North Clin Istanb (2021) 8(3):255–60. doi: 10.14744/nci.2020.90093
159. Makay B, Unsal E, Arslan N, Varni JW. Health-Related Quality of Life of School-Age Children With Familial Mediterranean Fever. Clin Exp Rheumatol (2009) 27(2 Suppl 53):S96–101.
160. Deger SM, Ozturk MA, Demirag MD, Aslan S, Goker B, Haznedaroglu S, et al. Health-Related Quality of Life and Its Associations With Mood Condition in Familial Mediterranean Fever Patients. Rheumatol Int (2011) 31(5):623–8. doi: 10.1007/s00296-009-1334-4
161. Duruoz MT, Unal C, Bingul DK, Ulutatar F. Fatigue in Familial Mediterranean Fever and its Relations With Other Clinical Parameters. Rheumatol Int (2018) 38(1):75–81. doi: 10.1007/s00296-017-3882-3
162. Kucuksahin O, Omma A, Ozdemirel AE, Tecer D, Ulutas S, Maras Y, et al. Incidence of Sleep Disturbances in Patients With Familial Mediterranean Fever and the Relation of Sleep Quality With Disease Activity. Int J Rheum Dis (2018) 21(10):1849–56. doi: 10.1111/1756-185X.13104
163. Koga T, Migita K, Kawakami A. Biologic Therapy in Familial Mediterranean Fever. Mod Rheumatol (2016) 26(5):637–41. doi: 10.3109/14397595.2016.1162261
164. Soriano A, Soriano M, Espinosa G, Manna R, Emmi G, Cantarini L, et al. Current Therapeutic Options for the Main Monogenic Autoinflammatory Diseases and PFAPA Syndrome: Evidence-Based Approach and Proposal of a Practical Guide. Front Immunol (2020) 11:865. doi: 10.3389/fimmu.2020.00865
165. Simsek C, Karatas M, Tatar E, Yildirim AM, Alkan FT, Uslu A. The Efficacy of Interleukin-1 Antagonist Drugs in Combination With Colchicine in Patients With FMF-AA With Colchicine Resistance After Kidney Transplantation: A Study With Histopathologic Evidence. Clin Transplant (2021) 35(6):e14309. doi: 10.1111/ctr.14309
Keywords: autoinflammatory diseases, indications, treatment, hereditary recurrent fevers, interleukin-1 blockers, anakinra, canakinumab
Citation: Vinit C, Georgin-Lavialle S, Theodoropoulou A, Barbier C, Belot A, Mejbri M, Pillet P, Pachlopnik J, Poignant S, Rebelle C, Woerner A, Koné-Paut I and Hentgen V (2021) Real-Life Indications of Interleukin-1 Blocking Agents in Hereditary Recurrent Fevers: Data From the JIRcohort and a Literature Review. Front. Immunol. 12:744780. doi: 10.3389/fimmu.2021.744780
Received: 20 July 2021; Accepted: 19 October 2021;
Published: 11 November 2021.
Edited by:
Sinisa Savic, University of Leeds, United KingdomReviewed by:
Amra Adrovic, Istanbul University-Cerrahpasa, TurkeyAlessandra Soriano, Case Western Reserve University, United States
Copyright © 2021 Vinit, Georgin-Lavialle, Theodoropoulou, Barbier, Belot, Mejbri, Pillet, Pachlopnik, Poignant, Rebelle, Woerner, Koné-Paut and Hentgen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Vinit, Y2Fyb2xpbmUudmluaXRAYXBocC5mcg==
†ORCID: Isabelle Koné-Paut, orcid.org/0000-0001-8939-5763