
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 04 October 2021
Sec. Autoimmune and Autoinflammatory Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.715053
 Grégoire Martin de Frémont1
Grégoire Martin de Frémont1 Pierre Hirsch2†Santiago Gimenez de Mestral3†Philippe Moguelet4Yoan Ditchi3Jean-François Emile5Patricia Senet6
Pierre Hirsch2†Santiago Gimenez de Mestral3†Philippe Moguelet4Yoan Ditchi3Jean-François Emile5Patricia Senet6 Sophie Georgin-Lavialle7Thomas Hanslik8François Maurier9Amir Adedjouma1Noémie Abisror1Thibault Mahevas1Florent Malard10Lionel Adès11Pierre Fenaux11Olivier Fain1François Chasset6†
Sophie Georgin-Lavialle7Thomas Hanslik8François Maurier9Amir Adedjouma1Noémie Abisror1Thibault Mahevas1Florent Malard10Lionel Adès11Pierre Fenaux11Olivier Fain1François Chasset6† Arsène Mekinian1*† on behalf of MINHEMON (French Network of Dysimmune Disorders Associated With Hemopathies)
Arsène Mekinian1*† on behalf of MINHEMON (French Network of Dysimmune Disorders Associated With Hemopathies)Background: Myelodysplastic syndromes (MDS) and chronic myelomonocytic leukemia (CMML) are associated with cutaneous manifestations. Next-generation sequencing (NGS) is a tool capable of identifying clonal myeloid cells in the skin infiltrate and thus better characterize the link between hematological diseases and skin lesions.
Objective: To assess whether skin lesions of MDS/CMML are clonally related to blood or bone marrow cells using NGS.
Methods: Comparisons of blood or bone marrow and skin samples NGS findings from patients presenting with MDS/CMML and skin lesions in three French hospitals.
Results: Among the 14 patients recruited, 12 patients (86%) had mutations in the skin lesions biopsied, 12 patients (86%) had a globally similar mutational profile between blood/bone marrow and skin, and 10 patients (71%) had mutations with a high variant allele frequency (>10%) found in the myeloid skin infiltrate. Mutations in TET2 and DNMT3A, both in four patients, were the most frequent. Two patients harbored a UBA1 mutation on hematopoietic samples.
Limitations: Limited number of patients and retrospective collection of the data. Blood and skin sampling were not performed at the exact same time point for two patients.
Conclusion: Skin lesions in the setting of MDS/CMML are characterized by a clonal myeloid infiltrate in most cases.
Myelodysplastic syndromes (MDS) are defined as clonal hematopoietic disorders with ineffective hematopoiesis resulting in dysplasia, bone marrow failure, and peripheral cytopenias. Chronic myelomonocytic leukemia (CMML) is closely related to MDS and characterized by persistent monocytosis with medullar dysplastic features (1). During the last years, the diagnosis, prognosis staging, and therapeutical management of MDS/CMML have been modified by the emergence of next-generation sequencing (NGS), which allows the screening of mutations in multiple genes. Blood and/or bone marrow NGS allows to identify somatic mutations in more than 90% of patients suffering from MDS/CMML (2). In the setting of MDS/CMML, systemic inflammatory and autoimmune diseases (SIADs) occur in 10 to 30% patients, mostly neutrophilic diseases, connective tissue disorders, arthritis, and vasculitis (3–7). More than half of patients with SIADs have skin involvement, consisting in neutrophilic dermatosis and skin vasculitis, less frequently cutaneous granulomatosis (8–10). Other skin lesions including cutaneous infections, drug adverse reactions, and leukemia cutis (blastic myeloid cell infiltration of the skin) can be observed and must be distinguished from SIADs (11). Moreover, using fluorescent in situ hybridization (FISH) analyses, some studies suggested the skin infiltrate of neutrophilic dermatoses that arise in the context of myeloid malignancies have differentiated from the malignant clone (12). This has been shown particularly for histiocytoid Sweet’s syndrome (H-SS) (13). Similarly, a recent study using NGS demonstrated a clonal relationship between malignant cells of myeloid neoplasm and neutrophil infiltrate of Sweet’s syndrome (14). However, these findings were restricted to neutrophilic dermatoses and included a limited number of MDS/CMML patients. Interestingly, a case of NGS identifying a clonal infiltrate in myelodysplasia cutis, consisting in an immature myeloid histiocytoid non-blastic infiltrate in the setting of MDS, was recently reported, as defined by Osio et al. (15, 16). Given these preliminary data, we sought to better characterize skin lesions of patients with MDS/CMML using NGS, hypothesizing that a majority of skin lesions could be related to a clonal myeloid infiltrate of the skin and thus share common mutations with the hematological MDS/CMML clone found in blood and marrow.
All consecutive patients with MDS or CMML referred to our department of internal medicine or dermatology in university tertiary centers between 2015 and 2020 for skin eruptions were enrolled in the study if a skin biopsy and NGS on at least one skin specimen were available. Skin lesions with a specific myelomonocytic infiltrate in pathology were referred as CMML cutis. Histiocytoid Sweet Syndrome (H-SS) was defined as a dermal infiltrate composed mostly of immature myeloid cells with histiocytic appearance as previously described (17). We decided to use the term myelodysplasia cutis only if lesions strictly corresponding to Osio et al.’s clinical and histological description were sampled (16). CMML/Erdheim Chester disease (ECD) was defined as a clonal cutaneous CMML infiltrate fulfilling ECD criteria (18). Of note, some biopsies did not have extensive immunohistochemical studies. Leukemia cutis was defined as a blastic infiltrate with CD34+, CD117+, or CD56+ cells. Skin biopsies of other patients addressed to our hospitals for leukemia cutis also underwent NGS to compare mutations and variant allele frequency (VAF) with those of non-blastic skin lesions. Three patients included in our case-series had previously been reported (18, 19).
DNA was extracted from total bone marrow or blood samples using QIAsymphony (Qiagen) method, and from fresh or formalin-fixed paraffin-embedded (FFPE) tissue for skin samples (18). For a majority of samples, libraries were obtained from 112.5 ng of DNA using HaloPlex Target Enrichment System® (Agilent technologies), using a gene panel including main genes implied in myeloid malignancies as already described (20). For three samples (patients 9, 13, and 14) without enough DNA sample available for a second technique, other similar gene panels designed for myeloid malignancies diagnosis were used. Libraries were sequenced on a MiSeq® sequencer (IlluminaINC). Read alignment, variant calling, and annotation were performed using Sophia DDM® software version 5.0.12 (Sophia genetics). The sensitivity was 1%. All variants were checked using Integrative Genomics Viewer (IGV) software v2.3.
Sanger sequencing was performed for UBA1 gene exon 3 for 12 patients with available hematopoietic samples (all patients but 8 and 12) and for one patient on skin sample (patient 8), as it was not included in the original gene panel.
The study was conducted according to the French CNIL methodology reference and in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patients unless dead at the time of the study.
The patients are described in Tables 1, 2. The median age of the 14 patients was 70 years old at MDS/CMML diagnosis (ranging 62–81) and was 69 years old at the time of cutaneous manifestations (ranging 30–82). The MDS subtypes were MDS with multilineage dysplasia (n=3, including one with myelofibrosis), MDS with excess blasts (n=1), MDS with unilineage dysplasia (n=1), MDS/myeloproliferative neoplasm (MPN) (n=2), and CMML (n=7). Karyotype was normal in eight patients, abnormalities were found in five patients [del(20)(q11q13) in patient 5; iso(X)(p10) and t(3,12)(p2?2;q24) in patient 6; trisomy 18 in patient 11; trisomy 8, del(1)(p?3?4), and del(5) (q?3?1q35) in patient 13; and del(4)(q?23q?26) in patient 14], and the karyotype could not be performed for one patient (patient 7). The MDS were low or intermediate-1 risk in 93% cases with median IPSS at 0.5 (0–2) and very-low, low, or intermediate risk in 93% cases with median IPSS-R at 2.3 (0.6–5.1).
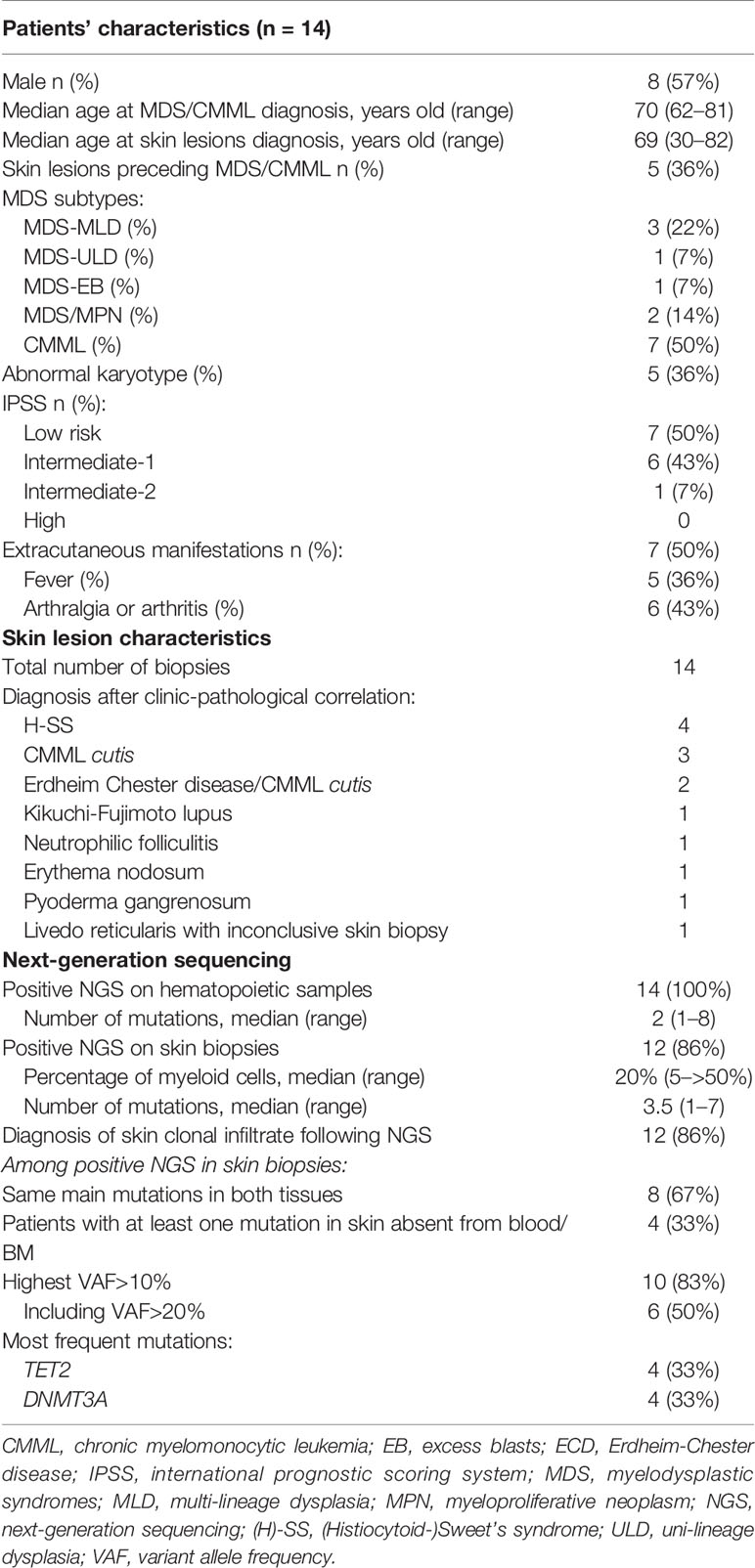
Table 1 Patients and skin lesion characteristics.
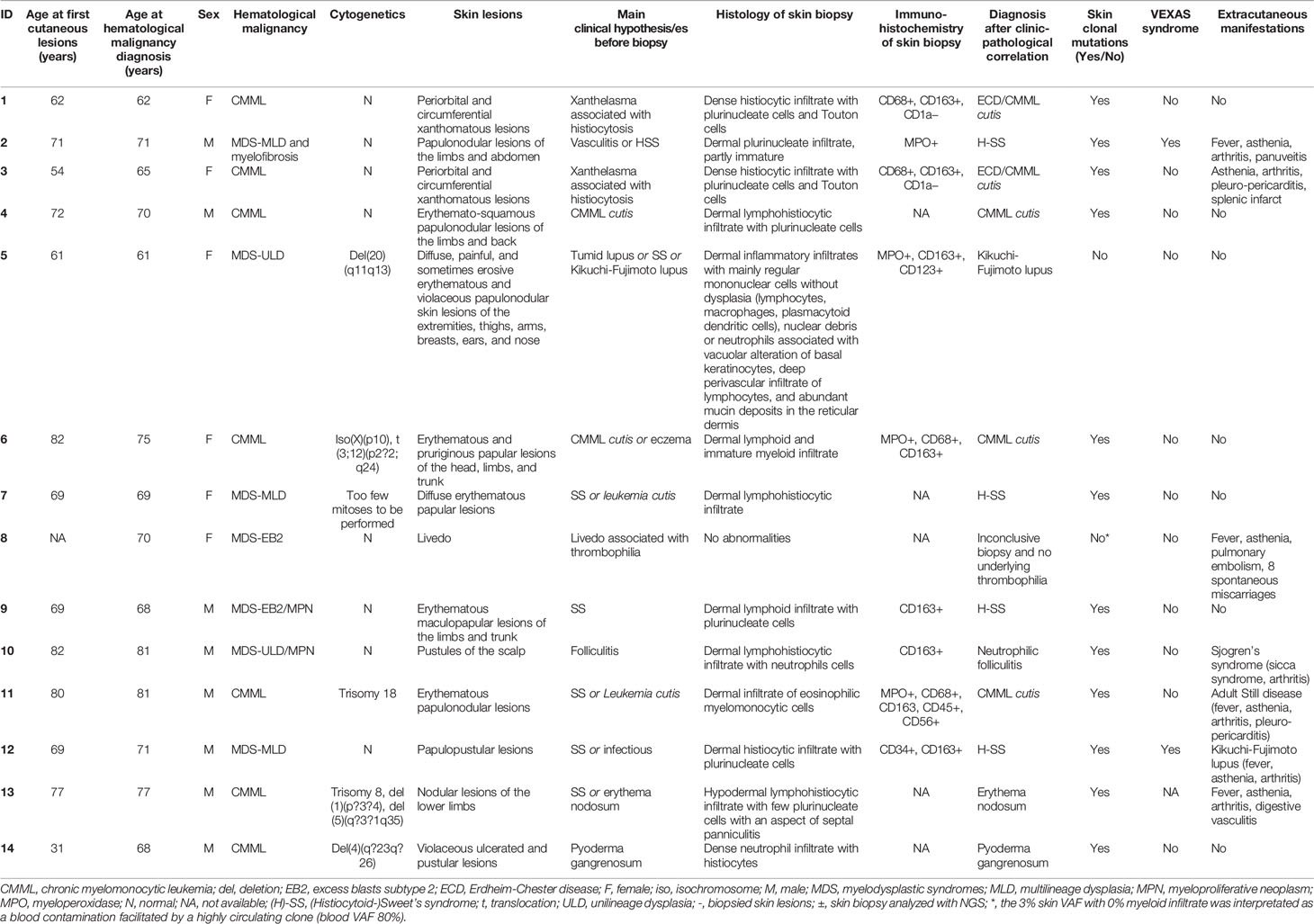
Table 2 Detailed patients’ characteristics.
Skin lesions preceded the MDS/CMML diagnosis in 5 (36%) patients. In 7 (50%) cases, extracutaneous symptoms were associated; fever (n=5; 36%) and arthralgia and/or arthritis (n=6; 43%) were the most prevalent.
Based on clinical, histological, and immunohistochemical findings and before NGS results, skin lesions have been classified as H-SS in four cases (patients 2, 7, 9, and 12), CMML cutis in three cases (patients 4, 6, and 11), and ECD associated with CMML cutis in two cases (patients 1 and 3) (18), Kikuchi-Fujimoto disease in one case (patient 5), neutrophilic folliculitis in one case (patient 10), erythema nodosum in one case (patient 13), pyoderma gangrenosum in one case (patient 14), and extensive livedo reticularis with non-specific findings on skin biopsy in one case (patient 8) (Tables 1, 2). Clinical and histological lesions are shown for patients 6, 7, and 14 (Figure 1).
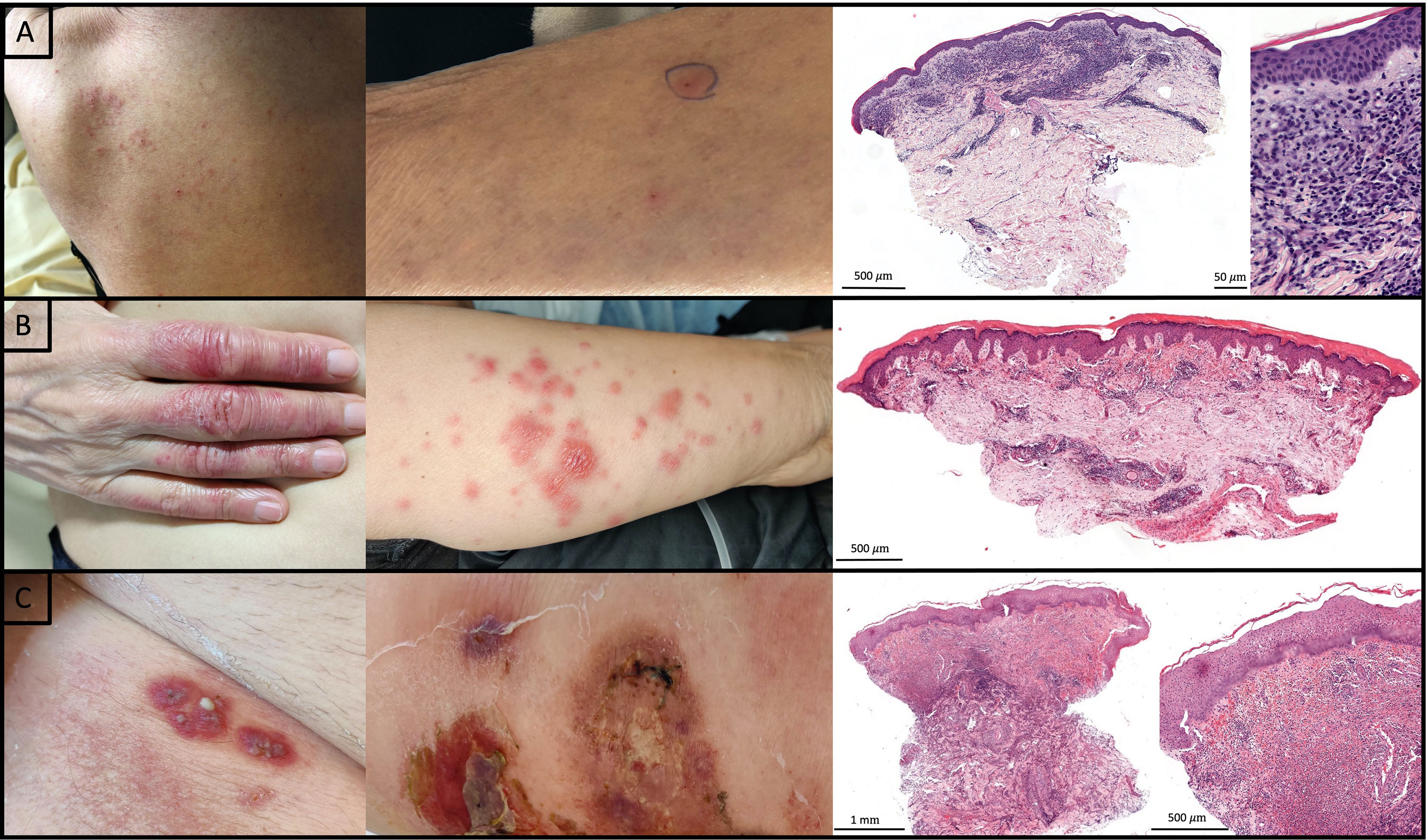
Figure 1 Clinical and histological features of patient 6, 7, and 14. (A) Patient 6, from left to right: Erythematous excoriated papules of the back; Erythematous crusty papule of the arm in which was performed skin biopsy; Dense superficial dermal infiltrate of myeloid cells (CD68+ monocytes and rare MPO+ cells) associated with lymphocytes compatible with CMML cutis (Hematoxylin-eosin-saffron; Original magnification respectively ×30 and ×400). (B) Patient 7, from left to right: papulonodular lesions of the hand and forearm; Dermal lymphohistiocytic infiltrate (Hematoxylin-eosin-saffron; Original magnification ×25). (C) Patient 14, from left to right: violaceous pustular and ulcerated lesions; Dense dermal neutrophilic infiltrate with histiocytes (Hematoxylin-eosin-saffron; Original magnification respectively ×25 and ×150).
Patients all had concomitant blood/marrow and skin sampling apart from patient 2 (skin biopsy performed 1 year before blood analysis with NGS) and patient 13 (skin biopsy performed 2 years before bone marrow analysis with NGS). At least one mutation was identified using NGS in blood/bone marrow in all patients with a median number of two mutations (ranging 1–8) and in skin biopsies in 12 patients with a median number of 3.5 mutations (ranging 1–7). Patient 5 was considered negative on skin owing to a very low skin VAF (<1%). Patient 8 was considered as a blood contamination as the weakly positive skin NGS (3% VAF) was not associated with a cutaneous myeloid infiltrate. Median VAF in skin was 12% (ranging from 1 to 76%) (Table 1). The same main mutation between blood/bone marrow and skin was found in eight patients (67% of patients with mutations in the skin). Six patients had paired mutations in blood/marrow and skin lesions (patients 1, 2, 3, 4, 11, 12 with respectively ECD/CMML cutis, H-SS, ECCD/CMML cutis, CMML cutis, CMML cutis, and H-SS). For the six other patients, three had more mutations on blood/marrow than skin (patients 6, 10, and 14, with respectively CMML cutis, neutrophilic folliculitis, and pyoderma gangrenosum), and three had more mutations on skin than blood/marrow (patients 7, 9, and 13, with respectively H-SS, H-SS, and erythema nodosum). Patient 7 had one extra-mutation in skin (in TP53, VAF 2%), patient 9 had two extra-mutations in skin (in SETBP1, VAF 4%, and in KMT2D/MLL2, VAF 3%), and patient 13 had two extra-mutations in skin (in KRAS, VAF 11%, and in RUNX1, VAF 6%) and one extra-mutation in blood (in ZRSR2, VAF 7%) with a bone marrow analysis performed 2 years after skin sampling (Tables 2, 3). Regarding VAF, 10 patients had at least one mutation in skin with VAF >10% (patients 1, 3, 4, 6, 7, 9, 10, 11, 13, 14, with respectively ECD/CMML cutis, ECD/CMML cutis, CMML cutis, CMML cutis, H-SS, H-SS, neutrophilic folliculitis, CMML cutis, erythema nodosum, and pyoderma gangrenosum), of whom six had at least one mutation with VAF >20% (patients 4, 7, 10, 11, 13, 14, with respectively CMML cutis, H-SS, neutrophilic folliculitis, CMML cutis, erythema nodosum, and pyoderma gangrenosum), and two patients had detectable mutation with VAF <10% (patients 2 and 12 with 40 and 20% myeloid cells in the infiltrate, respectively, both diagnosed with H-SS). The myeloid infiltrate was of only 5% in three patients, but all of them had VAF >10% (patients 4, 7, and 9) (Tables 2, 3). The most frequent mutations were in DNMT3A and TET2 both found in four patients. Two patients harbored the recently identified mutations in UBA1 (2 and 12) (21), both having H-SS associated with a febrile polyarthritis.
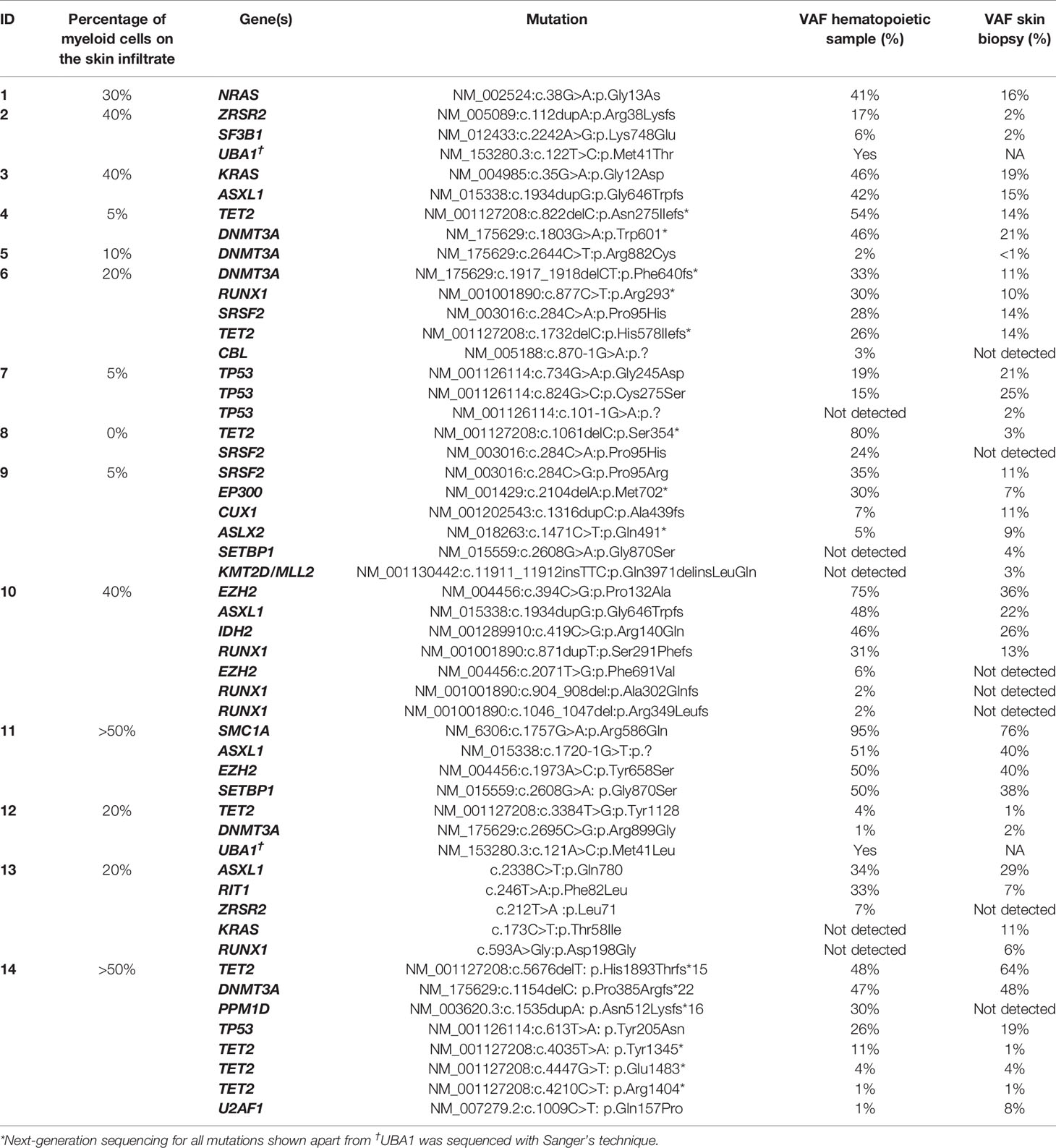
Table 3 Mutations in hematopoietic and skin samples.
Eleven patients have been treated and received oral steroids (n=8), hydroxychloroquine (n=2), immunosuppressive therapies (dapsone n=1), biological-targeted therapy (anakinra n=2, low-dose interleukin-2 n=1), or azacytidine as the hematological therapy (n=7). Azacytidine was associated with complete skin disease remission in three patients (two H-SS and one CMML cutis), partial in two (H-SS and pyoderma gangrenosum), and did not improve skin lesions in two (xanthelasma and folliculitis) (Table 4).
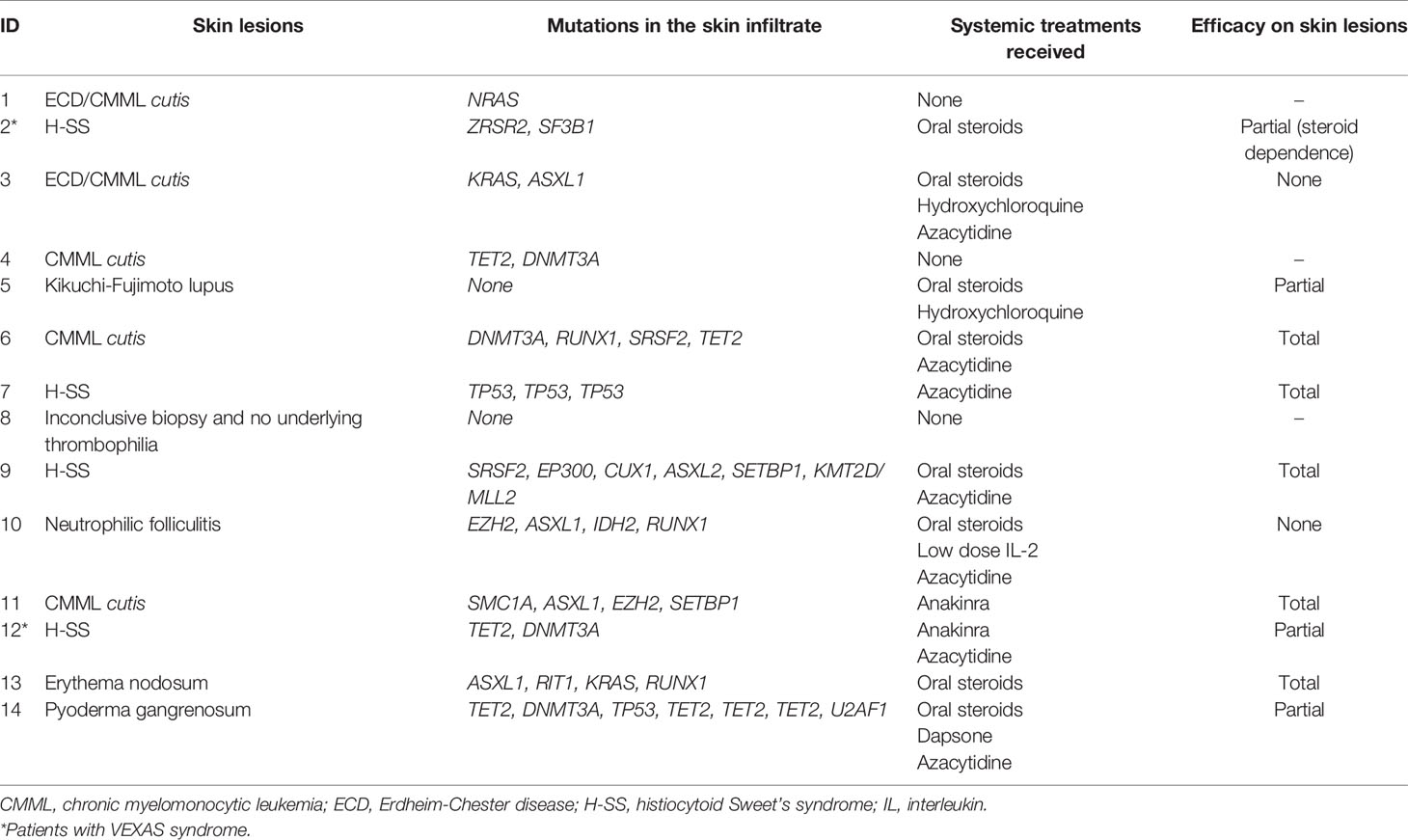
Table 4 Treatment outcome in skin lesions associated to MDS/CMML.
Two out of the 14 patients were dead by the end of data collection. One of them died of central nervous system infection (patient 11), and the other one of acute myeloid leukemia (patient 13).
It is known that leukemia cutis is characterized by a skin infiltrate of blastic cells directly related to the myeloid leukemia. Therefore, NGS mutational profile of blood and skin lesions should be similar, and these patients could be used as “positive controls.” We aimed to compare the results of our MDS/CMML patients with patients having leukemia cutis focusing on the “VAF/percentage of myeloid cells in the skin infiltrate” ratio. Four patients referred for cutaneous lesions compatible with leukemia cutis had NGS on skin samples. Two had AML and two had CMML evolving to AML. Skin symptoms were prominent with nodular lesions diagnosed in three patients and erythroderma in one. Leukemia cutis NGS found a median number of mutations of 4 (versus 4,5 in blood or marrow for the same patients). The median VAF was of 22% (ranging from 2 to 71%) in leukemia cutis (with a median percentage of myeloid cells in the infiltrate of >50%) compared with 12% (ranging from 1 to 76%) in the skin samples analyzed in our study (with a median percentage of myeloid cells in the infiltrate of 20%). The “VAF/percentage of myeloid cells in the skin infiltrate” ratio was similar between leukemia cutis and our skin samples (p=0.265 using Mann-Whitney test), supporting that mutations detected in skin biopsies of our MDS/CMML patients were related to a significant clonal myeloid infiltrate.
This case-series study highlights that despite heterogeneous clinical phenotypes of cutaneous lesions associated with MDS/CMML, a significant clonal skin infiltrate of MDS/CMML cells is found in most cases.
Recently, it has been shown using FISH in four patients and NGS in one patient followed for MDS that cutaneous lesions infiltrated by immature myeloid non-blastic cells were clonally related to the myeloid malignancy, and some authors suggested that they should be classified as myelodysplasia cutis (15, 16). Similarly, studying skin biopsies of patients with SS in the setting of MDS/CMML or acute myeloid leukemia, Passet et al. found a clonal infiltrate on the biopsies of 4/4 patients with a neutrophilic-SS associated with MDS/CMML (14). Our results confirmed these findings as all four patients diagnosed as H-SS before NGS had a clonal infiltrate related to the MDS and highlighted that other histiocytic or neutrophilic cutaneous disorders such as neutrophilic pustules, adult-xanthogranuloma, and pyoderma gangrenosum may also be characterized by a clonal infiltrate that shares a common clonal progenitor with MDS/CMML. Most patients had shared common mutations between paired blood/marrow and skin samples. Indeed, half of patients had identical paired mutations in blood/marrow and skin lesions, whereas some patients had additional mutations in skin or blood/bone marrows (n=3 each). This could be explained by a dissociated clonal evolution between hematopoietic tissue and skin once the original clone has spread to the skin.
Caution must, however, be exercised when interpreting VAF, which must be correlated to the percentage of myeloid cells infiltrating the skin to determine its significance and rule out a blood contamination, as in patient 8. Low VAF can be hard to interpret as in patient 5, considered negative but who also had a low circulating clonal burden, the low skin VAF thus did not strictly rule out a specific cutaneous localization of the myelodysplastic syndrome in this case.
The clinical diversity observed in our study is consistent with previous data in MDS/CMML-associated inflammatory manifestations. Despite efforts to classify these SIADs, they sometimes remain unlabeled. Apart from trisomy 8 associated with Behçet’s-like disease, no specific chromosomal abnormality has been associated with a particular clinical phenotype until now (7). Interestingly, an adult-onset autoinflammatory disease associated to UBA1 somatic mutations was recently described in 25 patients, 24% showing MDS and 88% having skin involvement with lesions such as nodules and plaques (compatible with neutrophilic dermatosis or cutaneous vasculitis), periorbital swelling, and severe cutaneous reaction to anakinra injection (21). In our study, we describe two new cases of VEXAS syndrome in patients with MDS associated to H-SS and extracutaneous symptoms. Furthermore, mutations in TET2 and DNMT3A were the two most prevalent (four patients each) but are also among the most frequent mutations associated with MDS. On the contrary, mutations in SF3B1, found in approximately 20% patients with MDS, was only found in one patient with low cutaneous VAF in our study (22). Given the small number of patients and the clinical diversity, no mutation could be associated with a particular cutaneous phenotype, and whether some mutations are associated with particular skin lesions still needs to be clarified.
The demonstration of a common clonal progenitor between myeloid neoplasms and neutrophilic and H-SS (12, 14–16, 23) as well as clonal association between L-Group histiocytosis and MDS/CMML (18, 24) supports a role of blood cells in the development of extramedullary expression of MDS/CMML and enlightens the pathophysiology of these manifestations, what may guide treatment. Indeed, azacytidine seems to have a potential effect on MDS/CMML-associated SIADs in a retrospective study (25). In our series, hematological treatment proved at least partly efficient on skin lesions in five patients. NGS positivity did not seem associated with treatment response as the two non-responders had a cutaneous clonal infiltrate. Beyond extramedullary hematopoiesis, the upregulation of inflammatory pathways in the clonal cells could also explain the occurrence of skin lesions. Indeed, monocytes in CMML have highly pro-inflammatory features (26), and mutations commonly seen in MDS/CMML happen to be associated with higher inflammation (27). Interestingly, the case of a patient with CMML and CMML cutis was reported in an IL-10 pilot trial with marked improvement of skin lesions under treatment (28). The dysregulation of pro-inflammatory pathways could explain the efficacy of immunosuppressive treatments in some patients.
Our study has several limitations. First, we enrolled a limited number of patient due to the rarity of the condition studied and the enrollment in only three hospitals. Second, two patients did not have a concomitant blood/marrow and skin sampling, limiting the comparability of mutations in blood/marrow versus skin. Third, some data were collected retrospectively as patients were enrolled at the time skin lesions appeared. Fourth, concurrent treatment administration was frequent, limiting outcome interpretation. At last, our study design does not allow to assess the overall prevalence of cutaneous lesions among MDS/CMML patients and to assess differences between patients with or without cutaneous lesions in terms of molecular profile and prognosis.
Our data need further investigation including a genetic study of the other organs involved in SIADs associated with MDS/CMML and of the incidence of extramedullary clonal infiltration over survival.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
GF: conceptualization, data curation, formal analysis, methodology, and writing original draft. PH, SGM, FC, and AM: conceptualization, methodology, supervision, validation, and writing review and editing. Other authors: writing review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 Revision to the World Health Organization Classification of Myeloid Neoplasms and Acute Leukemia. Blood (2016) 127(20):2391–405. doi: 10.1182/blood-2016-03-643544
2. Bacher U, Shumilov E, Flach J, Porret N, Joncourt R, Wiedemann G, et al. Challenges in the Introduction of Next-Generation Sequencing (NGS) for Diagnostics of Myeloid Malignancies Into Clinical Routine Use. Blood Cancer J (2018) 8(11):113. doi: 10.1038/s41408-018-0148-6
3. Braun T, Fenaux P. Myelodysplastic Syndromes (MDS) and Autoimmune Disorders (AD): Cause or Consequence? Best Pract Res Clin Haematol (2013) 26(4):327–36. doi: 10.1016/j.beha.2013.09.003
4. Castro M, Conn DL, Su WP, Garton JP. Rheumatic Manifestations in Myelodysplastic Syndromes. J Rheumatol (1991) 18(5):721–7.
5. Fain O, Braun T, Stirnemann J, Fenaux P. Manifestations Systémiques Et Auto-Immunes Des Syndromes Myélodysplasiques. Rev Méd Interne (2011) 32(9):552–9. doi: 10.1016/j.revmed.2010.08.005
6. Ustwani OA, Ford LA, Sait SJN, Block AMW, Barcos M, Vigil CE, et al. Myelodysplastic Syndromes and Autoimmune Diseases—Case Series and Review of Literature. Leuk Res (2013) 37(8):894–9. doi: 10.1016/j.leukres.2013.04.007
7. Wesner N, Drevon L, Guedon A, Fraison JB, Terrier B, Trad S, et al. Gastrointestinal Behcet’s-Like Disease With Myelodysplastic Neoplasms With Trisomy 8: A French Case Series and Literature Review. Leuk Lymphoma (2019) 60(7):1782–8. doi: 10.1080/10428194.2018.1542152
8. Yoneta K, Fujimoto N, Teramura K, Takayama S, Tanaka T. Disseminated Granulomatous Skin Lesions Associated With Myelodysplastic Syndrome Treated Successfully With Tranilast: A Case Report and Review of the Literature. Eur J Dermatol (2016) 26(4):398–400. doi: 10.1684/ejd.2016.2812
9. Balin SJ, Wetter DA, Kurtin PJ, Letendre L, Pittelkow MR. Myelodysplastic Syndrome Presenting as Generalized Granulomatous Dermatitis. Arch Dermatol (2011) 147(3):331. doi: 10.1001/archdermatol.2011.39
10. Farah C, Bulai Livideanu C, Jegu J, Paul C, Viraben R, Lamant L, et al. Prevalence and Prognostic Value of Cutaneous Manifestations in Patients With Myelodysplastic Syndrome: Skin Manifestations and Myelodysplasia. J Eur Acad Dermatol Venereol (2010) 24(10):1171–5. doi: 10.1111/j.1468-3083.2010.03614.x
11. Mekinian A, Grignano E, Braun T, Decaux O, Liozon E, Costedoat-Chalumeau N, et al. Systemic Inflammatory and Autoimmune Manifestations Associated With Myelodysplastic Syndromes and Chronic Myelomonocytic Leukaemia: A French Multicentre Retrospective Study. Rheumatology (2016) 55(2):291–300. doi: 10.1093/rheumatology/kev294
12. Sujobert P, Cuccuini W, Vignon-Pennamen D, Martin-Garcia N, Albertini AF, Uzunov M, et al. Evidence of Differentiation in Myeloid Malignancies Associated Neutrophilic Dermatosis: A Fluorescent In Situ Hybridization Study of 14 Patients. J Invest Dermatol (2013) 133(4):1111–4. doi: 10.1038/jid.2012.408
13. Chavan RN, Cappel MA, Ketterling RP, Wada DA, Rochet NM, Knudson R, et al. Histiocytoid Sweet Syndrome may Indicate Leukemia Cutis: A Novel Application of Fluorescence In Situ Hybridization. J Am Acad Dermatol (2014) 70(6):1021–7. doi: 10.1016/j.jaad.2014.01.874
14. Passet M, Lepelletier C, Vignon-Pennamen M-D, Chasset F, Hirsch P, Battistella M, et al. Next-Generation Sequencing in Myeloid Neoplasm-Associated Sweet’s Syndrome Demonstrates Clonal Relation Between Malignant Cells and Skin-Infiltrating Neutrophils. J Invest Dermatol (2020) 140(9):1873–6.e5. doi: 10.1016/j.jid.2019.12.040
15. Delaleu J, Battistella M, Rathana K, Vignon-Pennamen M -D., Laurent C, Ram-Wolff C, et al. Identification of Clonal Skin Myeloid Cells by Next Generation Sequencing in Myelodysplasia Cutis. Br J Dermatol (2020) 184(2):367–9. doi: 10.1111/bjd.19547
16. Osio A, Battistella M, Feugeas J-P, Cuccuini W, Noguera M-E, Petrella T, et al. Myelodysplasia Cutis Versus Leukemia Cutis. J Invest Dermatol (2015) 135(9):2321–4. doi: 10.1038/jid.2015.146
17. Requena L, Kutzner H, Palmedo G, Pascual M, Fernández-Herrera J, Fraga J, et al. Histiocytoid Sweet Syndrome: A Dermal Infiltration of Immature Neutrophilic Granulocytes. Arch Dermatol (2005) 141(7):834–42. doi: 10.1001/archderm.141.7.834
18. Bonnet P, Chasset F, Moguelet P, Abisror N, Itzykson R, Bouaziz J-D, et al. Erdheim-Chester Disease Associated With Chronic Myelomonocytic Leukemia Harboring the Same Clonal Mutation. Haematologica (2019) 104(11):e530–3. doi: 10.3324/haematol.2019.223552
19. Delplanque M, Chasset F, Hirsch P, Malard F, Ditchi Y, Fain O, et al. Cutaneous Lupus With Kikuchi Disease-Like Inflammatory Pattern Associated With Myelodysplastic Syndrome. Rheumatology (2019) 58(3):554–6. doi: 10.1093/rheumatology/key413
20. Guermouche H, Ravalet N, Gallay N, Deswarte C, Foucault A, Beaud J, et al. High Prevalence of Clonal Hematopoiesis in the Blood and Bone Marrow of Healthy Volunteers. Blood Adv (2020) 4(15):3550–7. doi: 10.1182/bloodadvances.2020001582
21. Beck DB, Ferrada MA, Sikora KA, Ombrello AK, Collins JC, Pei W, et al. Somatic Mutations in UBA1 and Severe Adult-Onset Autoinflammatory Disease. N Engl J Med (2020) 383(27):2628–38. doi: 10.1056/NEJMoa2026834
22. Spaulding TP, Stockton SS, Savona MR. The Evolving Role of Next Generation Sequencing in Myelodysplastic Syndromes. Br J Haematol (2020) 188(2):224–39. doi: 10.1111/bjh.16212
23. Van Loon K, Gill RM, McMahon P, Chigurupati R, Siddiqi I, Fox L, et al. 20q– Clonality in a Case of Oral Sweet Syndrome and Myelodysplasia. Am J Clin Pathol (2012) 137(2):310–5. doi: 10.1309/AJCP9I7NRWYLTJHV
24. Papo M, Diamond EL, Cohen-Aubart F, Emile J-F, Roos-Weil D, Gupta N, et al. High Prevalence of Myeloid Neoplasms in Adults With Non–Langerhans Cell Histiocytosis. Blood (2017) 130(8):1007–13. doi: 10.1182/blood-2017-01-761718
25. Fraison J-B, Mekinian A, Grignano E, Kahn J-E, Arlet J-B, Decaux O, et al. Efficacy of Azacitidine in Autoimmune and Inflammatory Disorders Associated With Myelodysplastic Syndromes and Chronic Myelomonocytic Leukemia. Leuk Res (2016) 43:13–7. doi: 10.1016/j.leukres.2016.02.005
26. Franzini A, Pomicter AD, Yan D, Khorashad JS, Tantravahi SK, Than H, et al. The Transcriptome of CMML Monocytes Is Highly Inflammatory and Reflects Leukemia-Specific and Age-Related Alterations. Blood Adv (2019) 3(20):2949–61. doi: 10.1182/bloodadvances.2019000585
27. Cull AH, Snetsinger B, Buckstein R, Wells RA, Rauh MJ. Tet2 Restrains Inflammatory Gene Expression in Macrophages. Exp Hematol (2017) 55:56–70.e13. doi: 10.1016/j.exphem.2017.08.001
Keywords: myelodysplastic syndrome, chronic myelomonocytic leukemia, skin, next-generation sequencing, clonal hematopoiesis
Citation: Martin de Frémont G, Hirsch P, Gimenez de Mestral S, Moguelet P, Ditchi Y, Emile J-F, Senet P, Georgin-Lavialle S, Hanslik T, Maurier F, Adedjouma A, Abisror N, Mahevas T, Malard F, Adès L, Fenaux P, Fain O, Chasset F and Mekinian A (2021) Myeloid Clonal Infiltrate Identified With Next-Generation Sequencing in Skin Lesions Associated With Myelodysplastic Syndromes and Chronic Myelomonocytic Leukemia: A Case Series. Front. Immunol. 12:715053. doi: 10.3389/fimmu.2021.715053
Received: 26 May 2021; Accepted: 02 September 2021;
Published: 04 October 2021.
Edited by:
Anna Shcherbina, Dmitry Rogachev National Research Center of Pediatric Hematology, Oncology and Immunology, RussiaReviewed by:
Jillian M. Richmond, University of Massachusetts Medical School, United StatesCopyright © 2021 Martin de Frémont, Hirsch, Gimenez de Mestral, Moguelet, Ditchi, Emile, Senet, Georgin-Lavialle, Hanslik, Maurier, Adedjouma, Abisror, Mahevas, Malard, Adès, Fenaux, Fain, Chasset and Mekinian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arsène Mekinian, YXJzZW5lLm1la2luaWFuQGFwaHAuZnI=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.