
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 28 June 2021
Sec. Antigen Presenting Cell Biology
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.704776
This article is part of the Research Topic The Therapeutic Potential of Antigen Presenting Cells View all 13 articles
 Iris A. E. van der Hoorn1,2
Iris A. E. van der Hoorn1,2 Georgina Flórez-Grau2
Georgina Flórez-Grau2 Michel M. van den Heuvel1
Michel M. van den Heuvel1 I. Jolanda M. de Vries2*
I. Jolanda M. de Vries2* Berber Piet1
Berber Piet1Current treatment for patients with non-small-cell lung cancer (NSCLC) is suboptimal since therapy is only effective in a minority of patients and does not always induce a long-lasting response. This highlights the importance of exploring new treatment options. The clinical success of immunotherapy relies on the ability of the immune system to mount an adequate anti-tumor response. The activation of cytotoxic T cells, the effector immune cells responsible for tumor cell killing, is of paramount importance for the immunotherapy success. These cytotoxic T cells are primarily instructed by dendritic cells (DCs). DCs are the most potent antigen-presenting cells (APCs) and are capable of orchestrating a strong anti-cancer immune response. DC function is often suppressed in NSCLC. Therefore, resurrection of DC function is an interesting approach to enhance anti-cancer immune response. Recent data from DC-based treatment studies has given rise to the impression that DC-based treatment cannot induce clinical benefit in NSCLC by itself. However, these are all early-phase studies that were mainly designed to study safety and were not powered to study clinical benefit. The fact that these studies do show that DC-based therapies were well-tolerated and could induce the desired immune responses, indicates that DC-based therapy is still a promising option. Especially combination with other treatment modalities might enhance immunological response and clinical outcome. In this review, we will identify the possibilities from current DC-based treatment trials that could open up new venues to improve future treatment.
Lung cancer is the leading cause of cancer-related death worldwide (1). This type of cancer is a heterogeneous disease (2). Based on histology, lung cancer is divided into small-cell lung cancer (SCLC) and non-small-cell lung cancer (NSCLC). NSCLC is the most prevalent form, accounting for about 80-85% of the lung cancer cases (3). The five-year overall survival rate (OS) for NSCLC is around 20% in the western world, highlighting the importance to explore the current and future therapeutic approaches in this field (4, 5).
Although surgery remains the cornerstone of therapy for early-stage NSCLC, a wide range of therapeutic options for adjuvant treatment or treatment of advanced stage disease have been introduced over the last decade. Targeted therapy and immunotherapy are examples of these novel therapies (6, 7). Targeted therapy targets specific alterations in NSCLC cells that stimulate tumor growth, for example mutations in the epidermal growth factor receptor (EGFR). Many other specific targets in NSCLC have been identified over time. Targeted therapy often leads to prolonged survival and greatly enhanced quality of life in this subgroup of patients (8, 9). Most patients with NSCLC lack actionable therapy targets. Therefore, immunotherapy, with or without chemotherapy, is the first-line treatment for the majority of NSCLC patients with advanced stage disease. Although targeted therapy and immunotherapy greatly improved clinical outcome in NSCLC, not all patients respond (10). Moreover, the patients who do respond eventually develop therapy resistance. Therefore, a high clinical need for new systemic treatment modalities remains. During this review we will shine our light on the rather unexposed field of dendritic cell (DC)-based therapies, to explore whether these could be a valuable treatment option for NSCLC.
The role of the immune system in prevention of cancer development and progression has been widely recognized. Immunotherapy exploits this role by stimulating the patient’s immune system to eliminate the tumor. Different immunotherapeutic strategies are being used or currently studied for their use in cancer. These can be largely subdivided into cancer vaccines, cellular therapies, immune stimulatory agonists and immune checkpoint inhibitors (ICIs). NSCLC is a promising potential target for immunotherapeutic approaches due to its high tumor mutational burden, which enhances immunogenicity of the tumor (11). ICIs are the only currently approved immunotherapy option for NSCLC. The most frequently used ICIs are directed against programmed-death receptor 1 (PD-1), expressed on immune effector cells such as T cells and natural killer (NK) cells, or its ligand programmed-death ligand 1 (PD-L1), which is expressed on antigen-presenting cells (APCs) and tumor cells. Receptor binding of PD-1 can lead to inhibition of effector cell function and survival, while it induces T regulatory cells (Tregs) (12–14). Immune cells in tumors frequently demonstrate a non-functional or ‘exhausted’ phenotype which hampers an anti-cancer immune response. ICIs aim to revert this immunosuppressive phenotype, thereby inducing an efficient anti-cancer immune response (15).
Recently, anti-cytotoxic T-lymphocyte associated protein 4 (CTLA-4), which is another ICI, has been registered to be used in combination with a PD-1 inhibitor in the United States and is registered for the combination with a PD-1 inhibitor and chemotherapy in Europe (16, 17). CTLA-4 is expressed on T cells after activation. It is also constitutively expressed on Tregs. CTLA-4 binds CD80 and CD86 on APCs. Receptor binding transmits an inhibitory signal to the T cell. Furthermore, binding of CTLA-4 to CD80 and CD86 blocks their binding to T cell receptors thereby hampering T cell activation (18).
Nowadays, it is known that the tumor and its surrounding microenvironment (TME) can modulate anti-tumor immune responses. Recent data suggest that the low response rate to ICIs could be partly explained by the lack of immune cells in the TME or other regulatory factors that prevent an anti-tumor immune response (19). Therefore, other forms of immunotherapy to enhance the anti-tumor immune response are currently being studied, such as DC-based therapy.
DC-based therapy depends on the fundamental link that DCs form between tumor antigen recognition and an anti-tumor immune response. More specifically, DCs are highly specialized APCs that show the highest antigen-presenting potential when inducing naïve T cell activation (20). In tissue, DCs are constantly scanning their surroundings. Upon antigen encounter in the presence of pathogen-associated molecular patterns (PAMPs) or damage-associated molecular patterns (DAMP), DCs get activated, undergo maturation and secrete large amounts of pro-inflammatory cytokines to shape the local inflammatory environment (6, 21, 22). After maturation, DCs migrate to the lymph node where they activate T cells to induce an immune response directed against their presented antigen. In absence of PAMP or DAMP signals during antigen encounter, DCs remain immature, migrate to the lymph nodes and induce antigen-specific tolerance in T cells. DC-based therapies showed promising results in several malignancies such as melanoma, prostate cancer, and glioma (23–25). In NSCLC only early-phase clinical trials have been performed, which show disappointing clinical results but were not powered to evaluate clinical effect. In this review, we will analyse these studies and discuss different possibilities to optimize DC-based therapy in order to improve therapeutic effects.
The DC-based therapy in NSCLC consists of the vaccination of patients with DCs. In all studies investigating DC vaccination in NSCLC patients, monocytes derived from autologous peripheral blood mononuclear cells (PBMCs) were differentiated to moDCs ex vivo (Table 1) (26–36). These DCs were then primed with a combination of several synthetic peptides of commonly expressed tumor antigens in NSCLC or autologous tumor lysate. In the majority of studies, primed DCs were administered via multiple subcutaneous injections. In vivo, these DCs are supposed to activate cytotoxic T cells that will induce a tumor-directed immune reaction.
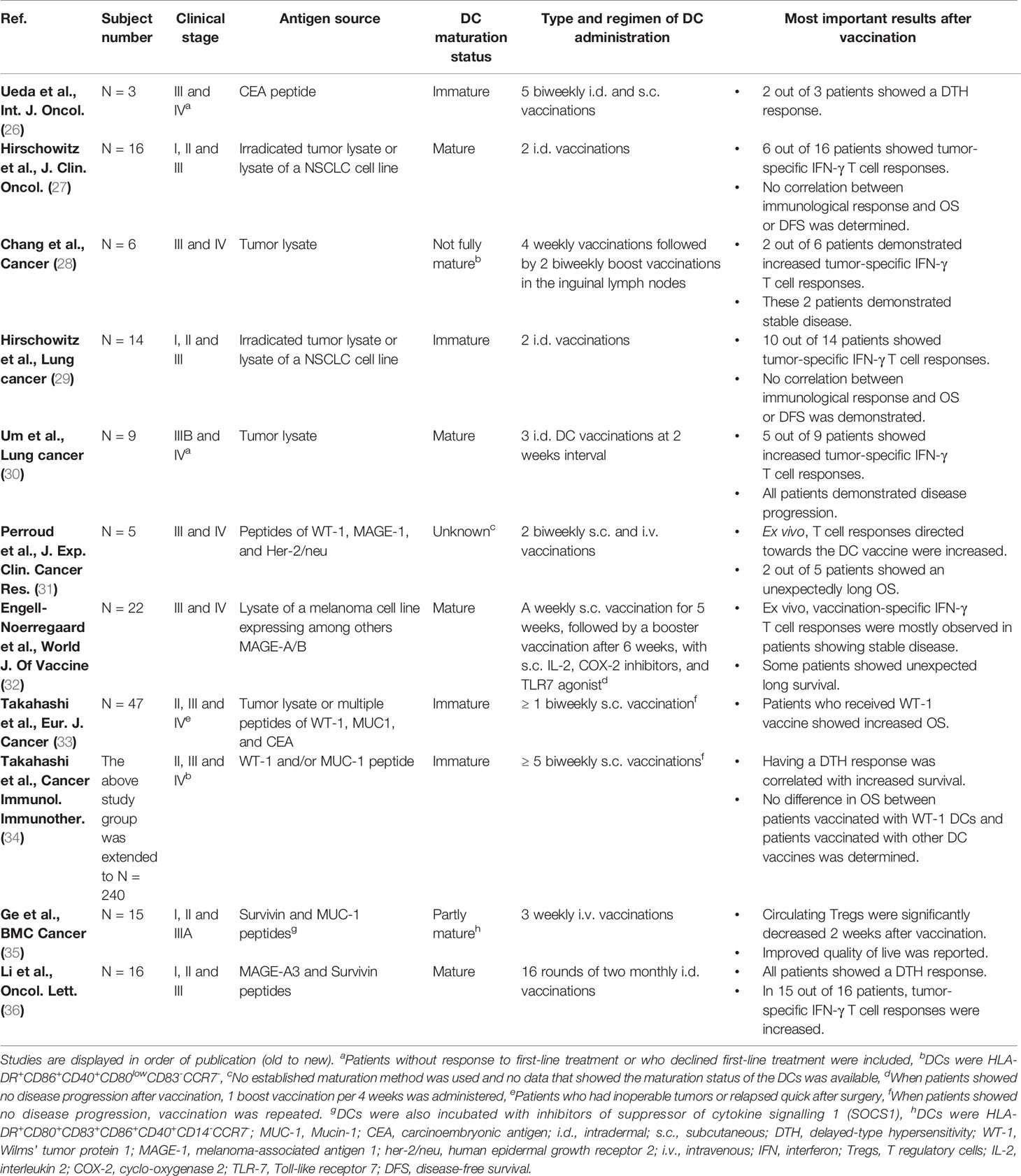
Table 1 Characteristics of studies in which DC vaccination monotherapy was performed in NSCLC.
All studies showed DC vaccination to be safe. In addition, many studies examined vaccine-specific immunological responses by determining ex vivo T cell responses directed towards the vaccine or by performing a delayed-type hypersensitivity (DTH) test. The principle of a positive DTH test is that if T cells are activated by DC vaccination, this DC vaccine will be recognized upon injection in the skin. This will cause a local immune reaction resulting in erythema. Most studies initially confirmed expression of their used tumor antigen in the tumor or used autologous tumor lysate for DC priming. Interestingly, vaccine-specific immunological responses were demonstrated in most studies after vaccination. However, this induced tumor-specific immune response was almost never linked to a radiological response or improved survival.
Investigators have also been focusing on the effect of combining DC vaccination with other therapies. For instance, chemotherapy and radiotherapy are hypothesised to enhance anti-tumor immunity and could therefore synergize with immunotherapy. A well-described effect of chemotherapy and radiotherapy is immunogenic cell death of cancer cells, exposing high levels of tumor antigen and DAMP molecules to immune cells in the TME (37–39). The superior immune-activating ability that chemotherapy and radiotherapy induce in cancer cells is highlighted in DC vaccination studies of cancer mouse models exploiting this strategy. In these studies, DC vaccination of DCs loaded with radiation-treated or chemotherapy-treated cancer cells, resulted in reduced tumor volume compared to mice vaccinated with DCs loaded with untreated tumor cells (40–43). Moreover, chemotherapy and radiotherapy were reported to stimulate human leukocyte antigen I (HLA-I) expression of the tumor, making tumor cells more sensitive to cytotoxic killing by CD8+ T cells (38). It is important to define the optimal dose of chemotherapy or radiotherapy for combination treatment with immunotherapy, as high doses of chemo- and radiotherapy can induce cell death of immune cells as well (37). The synergistic effect of chemotherapy to DC vaccination was recently validated in a human melanoma study (44). For NSCLC, this synergistic effect of both chemotherapy and radiotherapy with DC vaccination was confirmed in mouse models (45–47). In human NSCLC, only one study examined the combination of chemotherapy with DC monotherapy, but many studies investigated the combined effect of chemo- and/or radiotherapy, DC vaccination and cytokine-induced killer cells (CIK) (Table 2) (48, 50–55). CIK cells consist of a heterogeneous group of T cells, NK cells, and NKT cells. CIK cells are derived from autologous PBMCs, activated and expanded ex vivo under influence of anti-CD3 and cytokines, such as interferon γ (IFN-γ) and interleukin 2 (IL-2) (56). CIK therapy was shown to be safe and had a response rate of 39% in various tumors. Moreover, CIK treatment was associated with increased survival (57). Co-culture of CIK cells and DCs enhanced cytolytic function of CIK cells and increased both IL-12 secretion by DCs and levels of immunostimulatory receptors on DCs as well as CIK cells (58).
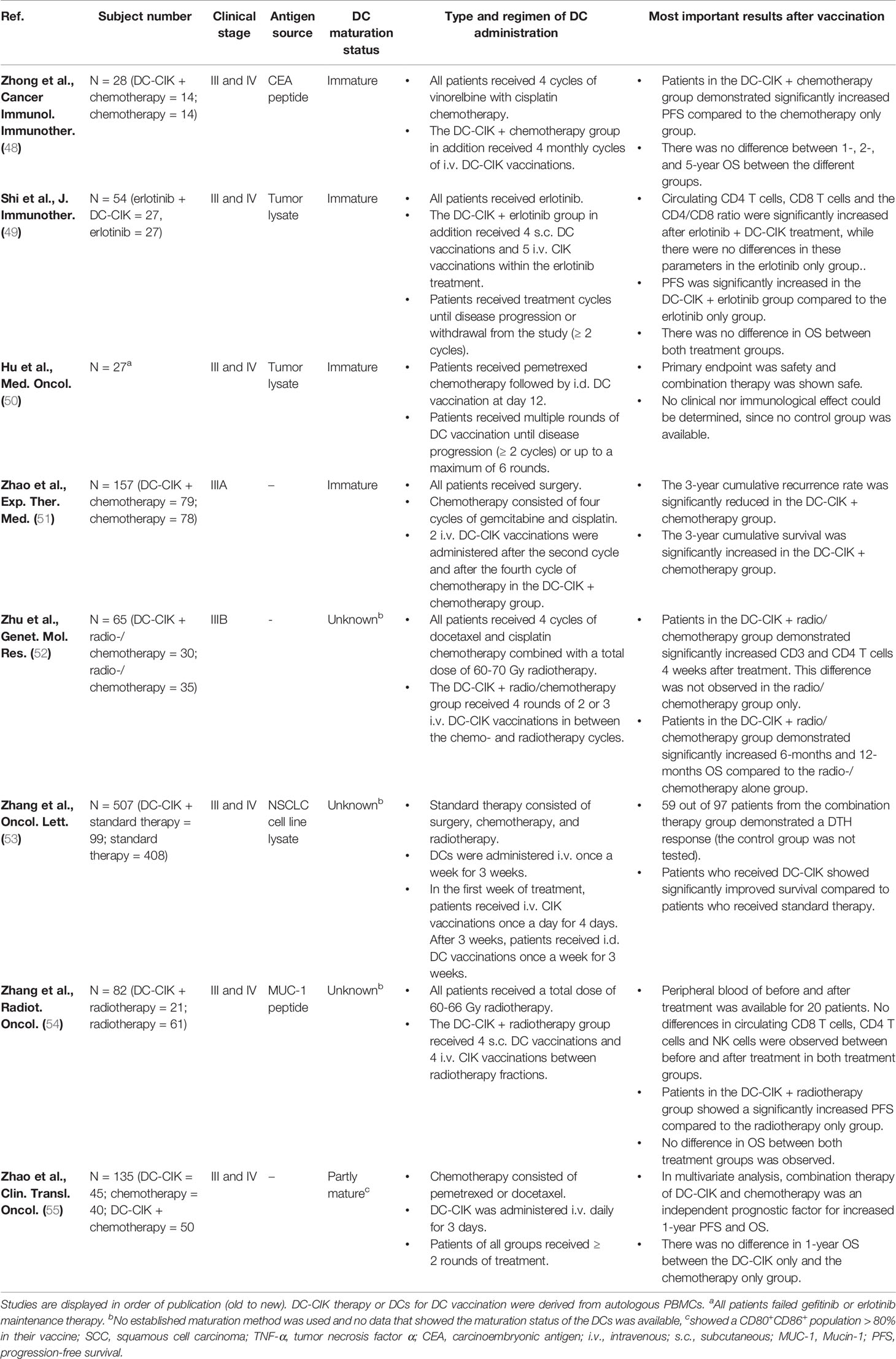
Table 2 Characteristics of studies in which DC vaccination combination therapy was performed in NSCLC.
Importantly, all studies showed that combination therapy was safe and well-tolerated. From all studies that combined DC-based therapy with radio- and/or chemotherapy in NSCLC, four out of seven demonstrated improved OS in the combination therapy group compared to radiotherapy or chemotherapy alone. Two studies of combined DC-CIK therapy that showed no differences in OS between groups, did show improved disease-free survival (DFS) in the combination therapy group. Unfortunately, the study investigating the effect of chemotherapy and DC vaccination alone included no control group to compare treatment efficiency or clinical outcome.
In addition to chemotherapy and radiotherapy, one study investigated the combination of DC-CIK and the EGFR tyrosine kinase inhibitor erlotinib in patients with advanced stage NSCLC (Table 2) (49). This study demonstrated increased progression-free survival (PFS) in the combination therapy group, while OS did not differ between the groups. This synergistic effect is particularly interesting considering that EGFR-mutated NSCLC is insensitive to anti-PD-1/anti-PD-L1 therapy (15, 59, 60). Erlotinib is normally not combined with other systemic treatment, because it shows no benefit in survival to monotherapy, while toxicity potentially increases (61, 62).
Whereas the current DC-based monotherapy studies could not show clinical benefit in NSCLC patients, combinations with chemotherapy, radiotherapy, and targeted therapy showed to improve clinical outcome. However, in almost all combination studies CIK cells were administered simultaneously with the DC vaccine. Hence, whether the observed clinical advantage of combination therapy over the standard therapy is an effect of the DC vaccine, the CIK cells, or the combination of both cannot be discerned from those studies.
A combination of therapies that was not studied in NSCLC before is DC-based therapy and other immunotherapy, such as ICIs. Several studies have pointed out that when there is no anti-tumor immune response, ‘releasing the brakes’ by checkpoint inhibition will not lead to improved clinical results. Hence, a combination with an immune strategy that actively induces an anti-tumor immune response might improve therapy response rate (63). Vice versa, therapies that actively stimulate the immune response, often result in increased expression of immune checkpoint molecules and might therefore also benefit from a combination treatment with ICIs. In addition, in single-cell RNA sequencing data from NSCLC tissue a mature DC subset with high expression of regulatory molecules, such as PD-L1, was identified which could be targeted by anti-PD-L1 therapy (64).
The potential synergistic effect of ICIs and DC vaccination is currently examined in advanced stage melanoma patients. Accordingly, two studies showed that a combination strategy of anti-CTLA-4 and DC vaccination resulted in an improved clinical response compared to similar cohorts that received anti-CTLA-4 treatment alone, without causing additional toxicity (65–68). In addition, ICI therapy was shown to be effective in advanced stage melanoma patients with recurrent disease after adjuvant DC vaccination (69). Until date, no results are available of studies that examine whether the synergistic effect of combined ICI and DC-based therapy also applies for NSCLC.
An important question is whether the current administration route for DC vaccination in NSCLC can induce a tumor-specific immune response in the lungs. The most promising results from human DC-based therapies are achieved in melanoma. In these trials, DCs were injected in the skin and migrated to cutaneous lymph nodes in which maturated DCs can initiate an anti-tumor immune response. For melanoma, this is often in close proximity to the tumor. For NSCLC this same route of administration is chosen, although the tumor is located at a large distance from the cutaneous lymph nodes. This difference in environment of T cell activation might lead to a decreased amount of T cells that reach the tumor. This is illustrated in a pancreatic cancer mouse model in which intraperitoneal administration of a DC vaccine suppressed tumor growth and inhibited tumor progression to a larger extent compared to subcutaneous injections of the same DC vaccine (70). It might therefore be interesting to study the effect of DC-based therapy that is administered into the local lymph nodes. Although this is more invasive, it might induce a more locally effective anti-tumor immune response.
The local environment during T cell activation might not be the only element causing the suggested suboptimal lung T cell infiltration. In an inflammation mouse model, it was shown, that after local immunization with the immunogenic ovalbumin protein (OVA), DCs isolated from lung-draining mediastinal lymph nodes induced increased lung homing of CD4 T cells compared to DCs isolated from muscle-draining inguinal lymph nodes (71). The authors linked this increased ability to induce lung-homing of CD4 T cells to a CD24+ DC subset that is highly expressed in the mediastinal lymph node compared to the inguinal lymph node. To induce a local immune reaction in the lung, it therefore seems pivotal to specifically target this DC subset. Interestingly, in another inflammation mouse model it was demonstrated that this specific DC subset is probably not induced in the lung-draining lymph node itself, but rather in the lungs before lymph node migration (72). This is illustrated by an experiment in which DCs isolated from lung tissue, lung-draining lymph nodes, and other lymph nodes received antigen and were co-cultured with T cells ex vivo. DCs isolated from lung were superior at inducing lung-homing T cells, while there was no difference between DCs originating from lung-draining lymph nodes and other lymph nodes. This finding that lung-derived DCs induced superior homing of T cells to the lung was also confirmed in another mouse model of viral infection. In this model, mice were intranasally challenged with viral particles after which DCs were isolated from both lung and lung-draining lymph nodes at multiple time points after infection. Their results demonstrate that at 30 minutes after infection lung DCs were superior at inducing T cell homing compared to DCs originating from lung-draining lymph nodes, while at 24 hours after infection this difference was abolished. Since transport of soluble antigen from the lung towards the local lymph node already occurs within a few minutes after infection, this experiment validates that DCs that migrated from the lung are the main stimulants for lung-homing T cells. Although these are all pre-clinical data, a lung-derived DC subset paramount for optimal local tumor-specific T cell immune response might also be present in humans. DCs used for DC vaccination in NSCLC are not lung-derived. Therefore, means to equip DCs with an optimal capacity to induce lung-homing T cells should be developed.
The clinical trials using DC-based therapy in NSCLC were performed with DCs that were earlier isolated from the patient’s peripheral blood, after which the DC vaccine was finalized in the lab. This procedure to construct DC vaccines has disadvantages: it is demanding for patients, laborious and expensive. For that reason, targeting DCs in vivo is a promising approach. Moreover, specific DC subsets in the tumor could be directly targeted when a monoclonal antibody directed against specific endocytic DC receptors would be used as guide for antigen delivery. For example, C-type lectin domain containing 9A (CLEC9A) on conventional type 1 DCs (cDC1s). Since CLEC9A is involved in cross-presentation, this specific targeting could also skew the antigen-processing towards this direction (73). This strategy of specific DC-targeting is not yet performed in humans, but some mouse studies show promising results.
In melanoma mouse models, receptors targeting among others, CLEC9A, CD11c, and DEC-205 (receptor on circulating DCs of mice and human, involved in cross-presentation) were bound to OVA (74–77). With concurrent activation, such as Polyinosinic:polycytidylic acid (poly I:C) and anti-CD40, the administered tumor antigen-receptor complex was shown to elicit effective immune responses and inhibit tumor growth. Hence, in the study using DEC-205 it was even demonstrated that in vivo vaccination showed larger inhibition of tumor growth compared to vaccination with ex vivo spleen-derived DCs which were also primed with OVA and maturated using anti-CD40 (74).
In the previous examples, antigens were chemically conjugated to a monoclonal antibody, or the DNA sequence of the antigen was genetically fused to the monoclonal antibody, while DC activation signals were injected separately. Currently, however, many studies focus on more complex manners of antigen delivery in vivo that could improve antigen uptake and DC activation efficiency. Examples are lipid vesicles or nanoparticles with surface-bound DC targeting receptors, and containing tumor antigens and DC activation signals (78). An important advantage of this technique is that the maturation signals are selectively delivered to the DCs. This is important because maturation molecules have been shown to have a tumor-supporting function when binding to other cells in the TME (79–81).
There are also studies that only focus on in vivo DC activation, without loading the DC with antigen. In a lymphoma mouse model, it is shown that intratumoral injection of TriMix mRNA, encoding costimulatory molecules CD70, CD40 ligand, and constitutively active toll-like receptor 4 (TLR4), induces systemic tumor-specific T cell responses independent of the co-delivery of tumor antigen (82). Moreover, in animal cancer models they show increased survival after injection of TriMix mRNA. The uptake of Trimix mRNA relies on the ability of DCs to rapidly and selectively internalize free RNA and avoids off-target effects. These results suggest that tumor-infiltrating DCs may have acquired antigen, and that the problem in their malfunctioning phenotype is rather the lack of sufficient activation signals in their surroundings.
Nowadays, DC-based therapy in NSCLC is still at a developmental stage. The DC vaccination studies performed are all early-phase studies that demonstrated low toxicity of the treatment, but were underpowered to show clinical benefit. However, most of these clinical trials showed that DC vaccination can induce the desired immune response. The latter highlights the potential of DC-based therapy in NSCLC and encourages further research that could advance the peripheral immunological effect to a radiological response or improved survival. In particular, studies that examine whether the anti-tumor immune response in peripheral blood or skin could also be induced in the tumor environment could provide more insight. The immune-activating ability of DC vaccination and the low toxicity of treatment make this therapy an excellent candidate for combination with other anti-cancer treatment. Clinical success of combination therapies is illustrated by the results of combination studies of chemotherapy and/or radiotherapy and even targeted therapy with DC-CIK vaccination in NSCLC. Likewise, studies in melanoma demonstrated the synergizing effect of DC-based therapy and ICIs. Especially this latter combination with ICIs, which inhibit the immunosuppressive TME, could allow the optimal immune-activating potential of DC based therapy to be revealed in NSCLC.
IAEvdH wrote the manuscript. GFG and BP wrote and reviewed the manuscript. IJMdV and MMvdH reviewed the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. WHO Cancer. Geneva, Switzerland: WHO (2018). Available at: https://www.who.int/health-topics/cancer#tab=tab_1.
2. de Sousa VML, Carvalho L. Heterogeneity in Lung Cancer. Pathobiology (2018) 85(1–2):96–107. doi: 10.1159/000487440
3. Society, A. C Lung Cancer (2020). Available at: https://www.cancer.org/cancer/lung-cancer/about/key-statistics.html.
4. Society, A. C Lung Cancer Survival Rates (2020). Available at: https://www.cancer.org/cancer/lung-cancer/detection-diagnosis-staging/survival-rates.html.
5. NKR Cijfers - IKNL. (n.d). Available at: https://iknl.nl/nkr-cijfers?fs%7Cepidemiologie_id=506&fs%7Ctumor_id=1&fs%7Cregio_id=530&fs%7Cperiode_id=545%2C546%2C547%2C548%2C549%2C550%2C551%2C552%2C553%2C554%2C555%2C556%2C557%2C558%2C559%2C560%2C561%2C562%2C563%2C564%2C565%2C566%2C567%2C568%2C569%2C570%2C571%2C572%2C544%2C543%2C542%2C541&fs%7Cgeslacht_id=622&fs%7Cleeftijdsgroep_id=655&fs%7Cjaren_na_diagnose_id=665&fs%7Ceenheid_id=681&cs%7Ctype=line&cs%7CxAxis=periode_id&cs%7Cseries=epidemiologie_id&ts%7CrowDimensions=periode_id&ts%7CcolumnDimensions=&lang%7Clanguage=nl.
6. Wang JB, Huang X, Li FR. Impaired Dendritic Cell Functions in Lung Cancer: A Review of Recent Advances and Future Perspectives. Cancer Commun (Lond) (2019) 39(1):43. doi: 10.1186/s40880-019-0387-3
7. Brierley J, Wittekind C, Gospodarowicz MK. Tnm Classification of Malignant Tumours. 8th edition. Chichester, UK: Union for International Cancer Control (UICC) (2016) p. 1–241.
8. Larsen JE, Cascone T, Gerber DE, Heymach JV, Minna JD. Targeted Therapies for Lung Cancer: Clinical Experience and Novel Agents. Cancer J (2011) 17(6):512–27. doi: 10.1097/PPO.0b013e31823e701a
9. Asao T, Takahashi F, Takahashi K. Resistance to Molecularly Targeted Therapy in Non-Small-Cell Lung Cancer. Respir Invest (2019) 57(1):20–6. doi: 10.1016/j.resinv.2018.09.001
10. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. N Engl J Med (2015) 372(12):2018–28. doi: 10.1056/nejmoa1501824
11. Lawrence MS, Stojanov P, Polak P, Kryukov GV, Cibulskis K, Sivachenko A, et al. Mutational Heterogeneity in Cancer and the Search for New Cancer-Associated Genes. Nature (2013) 499(7457):214–8. doi: 10.1038/nature12213
12. Riley JL. PD-1 Signaling in Primary T Cells. Immunol Rev (2009) 229(1):114–25. doi: 10.1111/j.1600-065X.2009.00767.x
13. Pesce S, Greppi M, Grossi F, Del Zotto G, Moretta L, Sivori S, et al. PD/1-PD-Ls Checkpoint: Insight on the Potential Role of NK Cells. Front Immunol (2019) 10:1242. doi: 10.3389/fimmu.2019.01242
14. Francisco LM, Salinas VH, Brown KE, Vanguri VK, Freeman GJ, Kuchroo VK, et al. PD-L1 Regulates the Development, Maintenance, and Function of Induced Regulatory T Cells. J Exp Med (2009) 206(13):3015–29. doi: 10.1084/jem.20090847
15. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Pembrolizumab Versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2016) 375(19):1823–33. doi: 10.1056/NEJMoa1606774
16. FDA. FDA Approves Nivolumab Plus Ipilimumab for First-Line mNSCLC (PD-L1 Tumor Expression ≥1%). Silver Spring, USA: FDA (2020). Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-nivolumab-plus-ipilimumab-first-line-mnsclc-pd-l1-tumor-expression-1.
17. EMA. Annex I Summary of Product Characteristics (2020). Available at: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf.
19. Nowicki TS, Hu-Lieskovan S, Ribas A. Mechanisms of Resistance to PD-1 and PD-L1 Blockade. Cancer J (United States) (2018) 24(1):47–53. doi: 10.1097/PPO.0000000000000303
20. Steinman RM. The Dendritic Cell System and Its Role in Immunogenicity. Annu Rev Immunol (1991) 9:271–96. doi: 10.1146/annurev.iy.09.040191.001415
21. Condon TV, Sawyer RT, Fenton MJ, Riches DW. Lung Dendritic Cells at the Innate-Adaptive Immune Interface. J Leukoc Biol (2011) 90(5):883–95. doi: 10.1189/jlb.0311134
22. Cook PC, MacDonald AS. Dendritic Cells in Lung Immunopathology. Semin Immunopathol (2016) 38(4):449–60. doi: 10.1007/s00281-016-0571-3
23. Cheever MA, Higano CS. Provenge (Sipuleucel-T) in Prostate Cancer: The First FDA-approved Therapeutic Cancer Vaccine. Clin Cancer Res (2011) 17(11):3520–6. doi: 10.1158/1078-0432.CCR-10-3126
24. Dillman RO, Cornforth AN, Depriest C, McClay EF, Amatruda TT, de Leon C, et al. Tumor Stem Cell Antigens as Consolidative Active Specific Immunotherapy: A Randomized Phase II Trial of Dendritic Cells Versus Tumor Cells in Patients With Metastatic Melanoma. J Immunother (2012) 35(8):641–9. doi: 10.1097/CJI.0b013e31826f79c8
25. Liau LM, Ashkan K, Tran DD, Campian JL, Trusheim JE, Cobbs CS, et al. First Results on Survival From a Large Phase 3 Clinical Trial of an Autologous Dendritic Cell Vaccine in Newly Diagnosed Glioblastoma. J Transl Med (2018) 16(1):142. doi: 10.1186/s12967-018-1507-6
26. Ueda Y, Itoh T, Nukaya I, Kawashima I, Okugawa K, Yano Y, et al. Dendritic Cell-Based Immunotherapy of Cancer With Carcinoembryonic Antigen-Derived, HLA-A24-Restricted CTL Epitope: Clinical Outcomes of 18 Patients With Metastatic Gastrointestinal or Lung Adenocarcinomas. Int J Oncol (2004) 24(4):909–17. doi: 10.3892/ijo.24.4.909
27. Hirschowitz EA, Foody T, Kryscio R, Dickson L, Sturgill J, Yannelli J. Autologous Dendritic Cell Vaccines for Non-Small-Cell Lung Cancer. J Clin Oncol (2004) 22(14):2808–15. doi: 10.1200/JCO.2004.01.074
28. Chang GC, Lan HC, Juang SH, Wu YC, Lee HC, Hung YM, et al. A Pilot Clinical Trial of Vaccination With Dendritic Cells Pulsed With Autologous Tumor Cells Derived From Malignant Pleural Effusion in Patients With Late-Stage Lung Carcinoma. Cancer (2005) 103(4):763–71. doi: 10.1002/cncr.20843
29. Hirschowitz EA, Foody T, Hidalgo GE, Yannelli JR. Immunization of NSCLC Patients With Antigen-Pulsed Immature Autologous Dendritic Cells. Lung Cancer (2007) 57(3):365–72. doi: 10.1016/j.lungcan.2007.04.002
30. Um SJ, Choi YJ, Shin HJ, Son CH, Park YS, Roh MS, et al. Phase I Study of Autologous Dendritic Cell Tumor Vaccine in Patients With Non-Small Cell Lung Cancer. Lung Cancer (2010) 70(2):188–94. doi: 10.1016/j.lungcan.2010.02.006
31. Perroud MW Jr., Honma HN, Barbeiro AS, Gilli SC, Almeida MT, Vassallo J, et al. Mature Autologous Dendritic Cell Vaccines in Advanced Non-Small Cell Lung Cancer: A Phase I Pilot Study. J Exp Clin Cancer Res (2011) 30:65. doi: 10.1186/1756-9966-30-65
32. Engell-Noerregaard L, Kvistborg P, Zocca M-B, Pedersen AW, Claesson MH, Mellemgaard A. Clinical and Immunological Effects in Patients With Advanced Non-Small Cell Lung-Cancer After Vaccination With Dendritic Cells Exposed to an Allogeneic Tumor Cell Lysate. World J Vaccines (2013) 03(02):68–76. doi: 10.4236/wjv.2013.32011
33. Takahashi H, Okamoto M, Shimodaira S, Tsujitani S, Nagaya M, Ishidao T, et al. Impact of Dendritic Cell Vaccines Pulsed With Wilms’ Tumour-1 Peptide Antigen on the Survival of Patients With Advanced Non-Small Cell Lung Cancers. Eur J Cancer (2013) 49(4):852–9. doi: 10.1016/j.ejca.2012.11.005
34. Takahashi H, Shimodaira S, Ogasawara M, Ota S, Kobayashi M, Abe H, et al. Lung Adenocarcinoma may be a More Susceptive Subtype to a Dendritic Cell-Based Cancer Vaccine Than Other Subtypes of Non-Small Cell Lung Cancers: A Multicenter Retrospective Analysis. Cancer Immunol Immunother (2016) 65(9):1099–111. doi: 10.1007/s00262-016-1872-z
35. Ge C, Li R, Song H, Geng T, Yang J, Tan Q, et al. Phase I Clinical Trial of a Novel Autologous Modified-DC Vaccine in Patients With Resected NSCLC. BMC Cancer (2017) 17(1):884. doi: 10.1186/s12885-017-3859-3
36. Li D, He S. MAGE3 and Survivin Activated Dendritic Cell Immunotherapy for the Treatment of Non-Small Cell Lung Cancer. Oncol Lett (2018) 15(6):8777–83. doi: 10.3892/ol.2018.8362
37. Emens LA, Middleton G. The Interplay of Immunotherapy and Chemotherapy: Harnessing Potential Synergies. Cancer Immunol Res (2015) 3(5):436–43. doi: 10.1158/2326-6066.CIR-15-0064
38. Reits EA, Hodge JW, Herberts CA, Groothuis TA, Chakraborty M, Wansley EK, et al. Radiation Modulates the Peptide Repertoire, Enhances MHC Class I Expression, and Induces Successful Antitumor Immunotherapy. J Exp Med (2006) 203(5):1259–71. doi: 10.1084/jem.20052494
39. Di Blasio S, Wortel IM, van Bladel DA, de Vries LE, Duiveman-de Boer T, Worah K, et al. Human CD1c(+) DCs Are Critical Cellular Mediators of Immune Responses Induced by Immunogenic Cell Death. Oncoimmunology (2016) 5(8):e1192739. doi: 10.1080/2162402X.2016.1192739
40. Strome SE, Voss S, Wilcox R, Wakefield TL, Tamada K, Flies D, et al. Strategies for Antigen Loading of Dendritic Cells to Enhance the Antitumor Immune Response. Cancer Res (2002) 62(6):1884–9.
41. Goldszmid RS, Idoyaga J, Bravo AI, Steinman R, Mordoh J, Wainstok R. Dendritic Cells Charged With Apoptotic Tumor Cells Induce Long-Lived Protective CD4 + and CD8 + T Cell Immunity Against B16 Melanoma. J Immunol (2003) 171(11):5940–7. doi: 10.4049/jimmunol.171.11.5940
42. Komorowski M, Tisonczyk J, Kolakowska A, Drozdz R, Kozbor D. Modulation of the Tumor Microenvironment by CXCR4 Antagonist-Armed Viral Oncotherapy Enhances the Antitumor Efficacy of Dendritic Cell Vaccines Against Neuroblastoma in Syngeneic Mice. Viruses (2018) 10(9):455. doi: 10.3390/v10090455
43. Lamberti MJ, Nigro A, Mentucci FM, Vittar NBR, Casolaro V, Col JD. Dendritic Cells and Immunogenic Cancer Cell Death: A Combination for Improving Antitumor Immunity. Pharmaceutics (2020) 12(3):256. doi: 10.3390/pharmaceutics12030256
44. Eisendle K, Weinlich G, Ebner S, Forstner M, Reider D, Zelle-Rieser C, et al. Combining Chemotherapy and Autologous Peptide-Pulsed Dendritic Cells Provides Survival Benefit in Stage IV Melanoma Patients. JDDG - J German Soc Dermatol (2020) 18(11):1270–7. doi: 10.1111/ddg.14334
45. Flieswasser T, Van Loenhout J, Freire Boullosa L, Van den Eynde A, De Waele J, Van Audenaerde J, et al. Clinically Relevant Chemotherapeutics Have the Ability to Induce Immunogenic Cell Death in Non-Small Cell Lung Cancer. Cells (2020) 9(6):1474. doi: 10.3390/cells9061474
46. Zhong H, Han B, Tourkova IL, Lokshin A, Rosenbloom A, Shurin MR, et al. Low-Dose Paclitaxel Prior to Intratumoral Dendritic Cell Vaccine Modulates Intratumoral Cytokine Network and Lung Cancer Growth. Clin Cancer Res (2007) 13(18 Pt 1):5455–62. doi: 10.1158/1078-0432.CCR-07-0517
47. Choi CW, Jeong MH, Park YS, Son CH, Lee HR, Koh EK. Combination Treatment of Stereotactic Body Radiation Therapy and Immature Dendritic Cell Vaccination for Augmentation of Local and Systemic Effects. Cancer Res Treat (2019) 51(2):464–73. doi: 10.4143/crt.2018.186
48. Zhong R, Teng J, Han B, Zhong H. Dendritic Cells Combining With Cytokine-Induced Killer Cells Synergize Chemotherapy in Patients With Late-Stage Non-Small Cell Lung Cancer. Cancer Immunol Immunother (2011) 60(10):1497–502. doi: 10.1007/s00262-011-1060-0
49. Shi SB, Tang XY, Tian J, Chang CX, Li P, Qi JL. Efficacy of Erlotinib Plus Dendritic Cells and Cytokine-Induced Killer Cells in Maintenance Therapy of Advanced Non-Small Cell Lung Cancer. J Immunother (2014) 37(4):250–5. doi: 10.1097/CJI.0000000000000015
50. Hu RH, Shi SB, Qi JL, Tian J, Tang XY, Liu GF, et al. Pemetrexed Plus Dendritic Cells as Second-Line Treatment for Patients With Stage IIIB/IV Non-Small Cell Lung Cancer Who had Treatment With TKI. Med Oncol (2014) 31(8):63. doi: 10.1007/s12032-014-0063-z
51. Zhao M, Li H, Li L, Zhang Y. Effects of a Gemcitabine Plus Platinum Regimen Combined With a Dendritic Cell-Cytokine Induced Killer Immunotherapy on Recurrence and Survival Rate of Non-Small Cell Lung Cancer Patients. Exp Ther Med (2014) 7(5):1403–7. doi: 10.3892/etm.2014.1574
52. Zhu XP, Xu YH, Zhou J, Pan XF. A Clinical Study Evaluating Dendritic and Cytokine-Induced Killer Cells Combined With Concurrent Radiochemotherapy for Stage IIIB Non-Small Cell Lung Cancer. Genet Mol Res (2015) 14(3):10228–35. doi: 10.4238/2015.August.28.6
53. Zhang L, Yang X, Sun Z, Li J, Zhu H, Li J, et al. Dendritic Cell Vaccine and Cytokine-Induced Killer Cell Therapy for the Treatment of Advanced Non-Small Cell Lung Cancer. Oncol Lett (2016) 11(4):2605–10. doi: 10.3892/ol.2016.4273
54. Zhang L, Xu Y, Shen J, He F, Zhang D, Chen Z, et al. Feasibility Study of DCs/CIKs Combined With Thoracic Radiotherapy for Patients With Locally Advanced or Metastatic Non-Small-Cell Lung Cancer. Radiat Oncol (2016) 11:60. doi: 10.1186/s13014-016-0635-5
55. Zhao Y, Qiao G, Wang X, Song Y, Zhou X, Jiang N, et al. Combination of DC/CIK Adoptive T Cell Immunotherapy With Chemotherapy in Advanced Non-Small-Cell Lung Cancer (NSCLC) Patients: A Prospective Patients’ Preference-Based Study (PPPS). Clin Transl Oncol (2019) 21(6):721–8. doi: 10.1007/s12094-018-1968-3
56. Wang S, Wang X, Zhou X, Lyerly HK, Morse MA, Ren J. DC-CIK as a Widely Applicable Cancer Immunotherapy. Expert Opin Biol Ther (2020) 20(6):601–7. doi: 10.1080/14712598.2020.1728250
57. Schmeel LC, Schmeel FC, Coch C, Schmidt-Wolf IG. Cytokine-Induced Killer (CIK) Cells in Cancer Immunotherapy: Report of the International Registry on CIK Cells (IRCC). J Cancer Res Clin Oncol (2015) 141(5):839–49. doi: 10.1007/s00432-014-1864-3
58. Marten A, Ziske C, Schottker B, Renoth S, Weineck S, Buttgereit P, et al. Interactions Between Dendritic Cells and Cytokine-Induced Killer Cells Lead to an Activation of Both Populations. J Immunother (2001) 24(6):502–10. doi: 10.1097/00002371-200111000-00007
59. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab Versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N Engl J Med (2015) 373(17):1627–39. doi: 10.1056/nejmoa1507643
60. Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab Versus Docetaxel in Patients With Previously Treated Non-Small-Cell Lung Cancer (OAK): A Phase 3, Open-Label, Multicentre Randomised Controlled Trial. Lancet (2017) 389(10066):255–65. doi: 10.1016/S0140-6736(16)32517-X
61. Herbst RS, Prager D, Hermann R, Fehrenbacher L, Johnson BE, Sandler A, et al. Tribute: A Phase III Trial of Erlotinib Hydrochloride (OSI-774) Combined With Carboplatin and Paclitaxel Chemotherapy in Advanced Non-Small-Cell Lung Cancer. J Clin Oncol (2005) 23(25):5892–9. doi: 10.1200/JCO.2005.02.840
62. Gatzemeier U, Pluzanska A, Szczesna A, Kaukel E, Roubec J, De Rosa F, et al. Phase III Study of Erlotinib in Combination With Cisplatin and Gemcitabine in Advanced Non-Small-Cell Lung Cancer: The Tarceva Lung Cancer Investigation Trial. J Clin Oncol (2007) 25(12):1545–52. doi: 10.1200/JCO.2005.05.1474
63. Saxena M, Bhardwaj N. Re-Emergence of Dendritic Cell Vaccines for Cancer Treatment. Trends Cancer (2018) 4(2):119–37. doi: 10.1016/j.trecan.2017.12.007
64. Maier B, Leader AM, Chen ST, Tung N, Chang C, LeBerichel J, et al. A Conserved Dendritic-Cell Regulatory Program Limits Antitumour Immunity. Nature (2020) 580(7802):257–62. doi: 10.1038/s41586-020-2134-y
65. Ribas A, Comin-Anduix B, Chmielowski B, Jalil J, de la Rocha P, McCannel TA, et al. Dendritic Cell Vaccination Combined With CTLA4 Blockade in Patients With Metastatic Melanoma. Clin Cancer Res (2009) 15(19):6267–76. doi: 10.1158/1078-0432.CCR-09-1254
66. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved Survival With Ipilimumab in Patients With Metastatic Melanoma. N Engl J Med (2010) 363(8):711–23. doi: 10.1056/NEJMoa1003466
67. Wilgenhof S, Corthals J, Heirman C, van Baren N, Lucas S, Kvistborg P, et al. Phase II Study of Autologous Monocyte-Derived mRNA Electroporated Dendritic Cells (TriMixDC-MEL) Plus Ipilimumab in Patients With Pretreated Advanced Melanoma. J Clin Oncol (2016) 34(12):1330–8. doi: 10.1200/JCO.2015.63.4121
68. Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD, Schmidt H, et al. Adjuvant Ipilimumab Versus Placebo After Complete Resection of High-Risk Stage III Melanoma (EORTC 18071): A Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol (2015) 16(5):522–30. doi: 10.1016/S1470-2045(15)70122-1
69. van Willigen WW, Bloemendal M, Boers-Sonderen MJ, de Groot JWB, Koornstra RHT, van der Veldt AAM, et al. Response and Survival of Metastatic Melanoma Patients Treated With Immune Checkpoint Inhibition for Recurrent Disease on Adjuvant Dendritic Cell Vaccination. OncoImmunology (2020) 9(1):1738814. doi: 10.1080/2162402X.2020.1738814
70. Yang J, Eresen A, Shangguan J, Ma Q, Zhang Z, Yaghmai V. Effect of Route of Administration on the Efficacy of Dendritic Cell Vaccine in PDAC Mice. Am J Cancer Res (2020) 10(11):3911–9.
71. Pejoski D, Ballester M, Auderset F, Vono M, Christensen D, Andersen P, et al. Site-Specific DC Surface Signatures Influence CD4+ T Cell Co-Stimulation and Lung-Homing. Front Immunol (2019) 10:1650. doi: 10.3389/fimmu.2019.01650
72. Mikhak Z, Strassner JP, Luster AD. Lung Dendritic Cells Imprint T Cell Lung Homing and Promote Lung Immunity Through the Chemokine Receptor CCR4. J Exp Med (2013) 210(9):1855–69. doi: 10.1084/jem.20130091
73. Schreibelt G, Klinkenberg LJJ, Cruz LJ, Tacken PJ, Tel J, Kreutz M, et al. The C-type Lectin Receptor CLEC9A Mediates Antigen Uptake and (Cross-)Presentation by Human Blood BDCA3+ Myeloid Dendritic Cells. Blood (2012) 119(10):2284–92. doi: 10.1182/blood-2011-08-373944
74. Bonifaz LC, Bonnyay DP, Charalambous A, Darguste DI, Fujii S, Soares H, et al. In Vivo Targeting of Antigens to Maturing Dendritic Cells Via the DEC-205 Receptor Improves T Cell Vaccination. J Exp Med (2004) 199(6):815–24. doi: 10.1084/jem.20032220
75. Sancho D, Mourao-Sa D, Joffre OP, Schulz O, Rogers NC, Pennington DJ, et al. Tumor Therapy in Mice Via Antigen Targeting to a Novel, DC-Restricted C-Type Lectin. J Clin Invest (2008) 118(6):2098–110. doi: 10.1172/JCI34584
76. Wei H, Wang S, Zhang D, Hou S, Qian W, Li B, et al. Targeted Delivery of Tumor Antigens to Activated Dendritic Cells Via CD11c Molecules Induces Potent Antitumor Immunity in Mice. Clin Cancer Res (2009) 15(14):4612–21. doi: 10.1158/1078-0432.CCR-08-3321
77. Kato M, McDonald KJ, Khan S, Ross IL, Vuckovic S, Chen K, et al. Expression of Human DEC-205 (CD205) Multilectin Receptor on Leukocytes. Int Immunol (2006) 18(6):857–69. doi: 10.1093/intimm/dxl022
78. Caminschi I, Maraskovsky E, Heath WR. Targeting Dendritic Cells In Vivo for Cancer Therapy. Front Immunol (2012) 3:13. doi: 10.3389/fimmu.2012.00013
79. Huang B, Zhao J, Li H, He KL, Chen Y, Chen SH, et al. Toll-Like Receptors on Tumor Cells Facilitate Evasion of Immune Surveillance. Cancer Res (2005) 65(12):5009–14. doi: 10.1158/0008-5472.CAN-05-0784
80. Chiodoni C, Iezzi M, Guiducci C, Sangaletti S, Alessandrini I, Ratti C, et al. Triggering CD40 on Endothelial Cells Contributes to Tumor Growth. J Exp Med (2006) 203(11):2441–50. doi: 10.1084/jem.20060844
81. Dölen Y, Gileadi U, Chen J-L, Valente M, Creemers JHA, Van Dinther EAW, et al. PLGA Nanoparticles Co-Encapsulating NY-ESO-1 Peptides and IMM60 Induce Robust CD8 and CD4 T Cell and B Cell Responses. Front Immunol (2021) 12:641703. doi: 10.3389/fimmu.2021.641703
Keywords: dendritic cells, lung cancer, immunotherapy, immunology and lung cancer, non-small cell lung cancer
Citation: van der Hoorn IAE, Flórez-Grau G, van den Heuvel MM, de Vries IJM and Piet B (2021) Recent Advances and Future Perspective of DC-Based Therapy in NSCLC. Front. Immunol. 12:704776. doi: 10.3389/fimmu.2021.704776
Received: 03 May 2021; Accepted: 15 June 2021;
Published: 28 June 2021.
Edited by:
Fabienne Anjuère, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Jessica Dal Col, University of Salerno, ItalyCopyright © 2021 van der Hoorn, Flórez-Grau, van den Heuvel, de Vries and Piet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: I. Jolanda M. de Vries, Sm9sYW5kYS5kZVZyaWVzQHJhZGJvdWR1bWMubmw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.